CHRONIC PAIN in adolescents final
27
Running head: ADOLESCENT CHRONIC PAIN MANAGEMENT 1 Management of Chronic Pain in Adolescents Juliann M. Trumpower Clemson University
-
Upload
juliann-trumpower -
Category
Documents
-
view
13 -
download
0
Transcript of CHRONIC PAIN in adolescents final

Running head: Adolescent chronic pain management 1
Management of Chronic Pain in Adolescents
Juliann M. Trumpower
Clemson University

Adolescent chronic pain management 2
Abstract
Purpose: Although frequently under-recognized, chronic pain in adolescents is widespread and
is often the result of a dynamic integration of biological, psychological and sociocultural factors
existing within a unique developmental path. The purpose of this systematic literature review is
to describe the characteristics of adolescents with chronic pain, determine the most efficacious
management of chronic pain in this population and discuss the implications for nursing
education, practice and research.
Methods: A thorough and exhaustive search of multiple electronic databases produced hundreds
of articles but a limited number of research studies published from 2000 to 2016 written in
English. The databases searched were CINAHL, MEDLINE, PubMed, Psych Info and the
Cochrane Central Register of Controlled Trials.
Results: A relatively limited number of studies were found related to the topic despite searches
of multiple databases and expanding years from publication. Ultimately, seventeen studies were
chosen based on relevancy to the topic. There was little to no evidence found for the safe and
effective use of medications, as evidenced by, a lack of high-grade research for this treatment
strategy. In contrast, the vast majority of studies advocated a multidisciplinary approach
consisting of care providers from specialties including medicine, psychology, nursing, and
psychiatry. The strongest evidence base exists for the use of psychological interventions
(relaxation, cognitive-behavioral therapy and acceptance and commitment therapy).
Keywords: Chronic pain, management, pharmaceutical, multidisciplinary, adolescents

Adolescent chronic pain management 3
Management of Chronic Pain in Adolescents
Chronic pain is defined as persistent and recurrent pain lasting longer than 3
months. (Dobe, Hartman, Kriszi. Hechler, Behlert, & Zernikow, 2013). Chronic pain in children
has been recognized as a major health concern around the world. Conservative estimates are 20-
35% of children and adolescents worldwide suffer from some form of chronic pain (WHO,
2012). In the United States (US), prevalence rates of chronic pain in children are estimated at
15-25% with an annual cost of more than 19.5 billion dollars (Groenewald, Essner, Wright,
Fesinmeyer, & Palermo, 2014). The most common types of chronic pain are musculoskeletal,
headache and abdominal pain. Chronic pain can be further categorized as ongoing and episodic
in children with chronic health conditions, such as arthritis and sickle cell disease, and pain that
is a disorder itself, such as, migraines and complex regional pain syndrome (Suresh, & Shah,
2011). The highest rates of chronic pain occur in females 12-14 years old and 30% of chronic
pain sufferers have had pain lasting over 2 years. Quality of life is impacted by pain that may
make them unable to socialize with peers, participate in sports or hobbies or attend school
(Voerman et al., 2012). In addition, chronic pain may result in sleep disturbances, loss of
appetite and depression (Gupta, 2014). Adolescents with chronic pain and depression are at
increased risk for thinking about and committing suicide (Tilburg, Spence, Whitehead,
Bangdiwala, & Goldston, 2011).
The treatment and management of chronic pain in children and adolescents is a challenge
for health care professionals, especially when the exact cause of pain in not clear (Voerman, et
al., 2012). Children often feel they are not believed and parents grow frustrated and distrustful
of healthcare professionals, as they are sent from one specialist to another for diagnostic testing,
while pain is not adequately managed (Wojtowicz & Banez, 2014). Providers are often

Adolescent chronic pain management 4
uncomfortable with prescribing effective pain medications, especially opiates, due to fear of drug
addiction and abuse. Negative attitudes and poor knowledge of pain assessment and
management are barriers to pain management in children (Tseng, Weiss, Harrison, Hansen, &
Bruce, 2014). Advanced practice nurses will encounter adolescents with chronic pain and can be
instrumental in guiding treatment. The most effective approach for chronic pain management in
adolescents has been shown to follow a biopsychosocial model utilizing a multi-disciplinary
approach (Wojtowicz & Banez, 2014). This integrative review will examine the characteristics
of youth who suffer from chronic pain, explore the most current and effective treatments for
management and discuss the implications for nursing education, practice and research.
Methods
A systematic review of the literature was performed to locate studies associated
with the management of chronic non-malignant pain in adolescents. The search method was an
in-depth assessment of multiple electronic databases to find related studies published from 2000
to 2016 written in English. The searched databases were CINAHL, MEDLINE, PubMed, Psych
Info and the Cochrane Central Register of Controlled Trials. Keywords used during this
exploration included chronic pain, management, pharmaceutical, multidisciplinary and
adolescents.
Results
Biopsychosocial Characteristics of Adolescents with Chronic Pain
The biopsychosocial model provides a useful theoretical framework for understanding
the relationship between chronic pain and psychiatric symptoms. It accounts for the complex
interplay of biological, psychological, social, environmental and individual factors that
contribute to and maintain chronic pain and subsequent disability (Odell & Logan, 2013).

Adolescent chronic pain management 5
Skrove, Romundstad and Indredavik (2015) conducted a large cross-sectional population based
study in Norway (Young-Hunt study) of over 7,000 adolescents (50.9% girls, 49.1% boys) which
sought to assess the prevalence of chronic pain with high disability in relation to emotional and
behavioral problems and resilience factors. The prevalence of chronic pain with high disability
increased with increasing scores of anxiety, depression, social anxiety and behavioral problems
(p<0.001). In contrast, both girls and boys with increased scores for resilience factors including
family cohesion, personal competence, social competence, community resources and self-
esteem, had significantly lower prevalence of pain (6.5% vs. 17.6%). A smaller study
(Wojtowicz & Banez, 2015) found the seven pain-associated factors identified in previous
research (Hyman et. al., 2002) were common. These include dependent coping style, chronic
illness in a parent, alexithymic personality, family problems, early pain experiences,
learning/developmental difficulties and perfectionist personality. In a phenomenological,
qualitative study of adolescents with cerebral palsy and severe chronic pain by Castle, Imms and
Howie, (2013), common themes included presence of unrelenting pain, frustration, loneliness,
despair, hopelessness, resentfulness of their dependence and feeling pain consumed their
thoughts, time, and energy. These studies provide further support of the biopsychosocial model
of chronic pain and related functional disability.
Multidisciplinary Management
The primary goal of chronic pain management is to improve all areas of functioning and
quality of life. This is best achieved through a multidisciplinary approach that incorporates
cognitive behavioral therapy (CBT) and other psychological therapies into rehabilitation
programs of functional restoration through physical and occupational treatments along with
standard medical care (i.e. treatment of any underlying conditions) and pharmaceutical

Adolescent chronic pain management 6
interventions (Odell & Logan, 2013). In addition, school reintegration and addressing significant
sleep disturbances are important aspects of care (Rajapakse, Liossi & Howard, 2014). A study
by Valrie, Bromberg, Palermo and Schanberg (2013) found that not only did pain lead to sleep
disturbances, but poor sleep related to increased pain, poor mood and increased disability.
Members of a multidisciplinary pain team may include physicians (typically
anesthesiologists or physiatrists), nurses, psychologists, physical therapists, occupational
therapists, recreational therapist, pharmacists, social workers, music therapists, and child life
specialists, among others. (Gregoire & Finley, 2013) An exploratory retrospective cohort study
of 70 children treated at an inpatient multidisciplinary pain management program (Blecourt et
al., 2008) showed improved overall level of functioning (including improved motor activities and
ability to assist with activities of daily living), as well as, increased participation in social
activities (p value Chi Square; ADL <0.001). Although it was not a primary outcome, pain
scores were significantly decreased both at discharge and at follow up (p <0.001). These results
mirror a newer retrospective study (Roessler et al., 2016) of consecutive patients admitted to a
functional rehabilitation center between 2010 and 2014 with chronic pain and significant
disability. Utilizing a multidisciplinary approach, 65.5% were treated inpatient and 34.5%
outpatient. Pain improved significantly in 89.7% (95% CI [0.73-0.98]) and pain medication
consumption decreased significantly in 72.4% (95% CI [0.53-0.87]). Patients who had stopped
walking could ambulate again in 91.7% of cases (95% CI [0.73-0.99]) and 86.4% who had
stopped going to school were back full time (95% CI [0.65-0.97]. There were no significant
differences in results between inpatients and outpatients and improvements were maintained at 3-
6 months after discharge in 83.3% of participants. In a larger study by Hechler, Wager &
Zernikow (2014), researchers compared treatment outcomes using three domains (pain intensity,

Adolescent chronic pain management 7
disability and school absence) between outpatients versus inpatients treated at a multidisciplinary
treatment center and who returned for follow up within a year. Both inpatients and outpatients
reported relatively low levels of pain intensity (NRS 0-10, mean =4 SD =2.7) and disability
(Pediatric Pain Disability Index PPDI: [12-60] mean = 24; SD= 10) at return visit. Compared to
outpatients, more inpatients achieved significant changes in pain intensity (52% vs. 45%) and
disability (46% vs. 31%). Both groups showed significantly reduced school absenteeism with
80% attending school regularly.
Psychological Therapies
Psychological interventions are the most evidence-based treatments and are an integral
component of the multidisciplinary pain treatment model. The primary goal of cognitive-
behavioral therapy (CBT) treatment is to teach the child self-regulation techniques through the
use of such strategies as relaxation, biofeedback, and guided imagery, as well as, cognitive
restructuring to help the patient perceive pain as less debilitating (Odell & Logan, 2013).
Psychological therapies, delivered to children and families, significantly reduce pain and
disability in children (Clinch & Eccleston, 2008). However, many adolescents do not receive
treatments due to lack of providers, expense and geographical distance to treatment centers.
(Palermo et. al, 2009). New and innovative technology has utilized computer-based programs
and smartphone applications to deliver psychological therapies remotely. A Cochrane Database
System Review by Fisher, Law, Palermo and Eccleston (2009), reviewed 8 randomized
controlled trials of adolescents (N=371 participants) with chronic pain who received remotely
delivered psychological therapies and found them to reduce pain severity across pain types but
showed no beneficial effect on improving disability. In addition, a meta-analysis of CBT
treatment (Velleman, Stallard and Richardson, 2010) identified four studies that all reported

Adolescent chronic pain management 8
significant post-treatment improvements in pain frequency, duration and intensity (50% from
baseline to post-treatment).
Acceptance and Commitment Therapy (ACT) is a new CBT approach that does not focus
on symptom control (reduced pain or depression) but rather aims to help individuals encounter
pain openly and without resistance. This can liberate an individual to focus on living a
personally meaningful and valued life, despite distress. Two studies of ACT therapy (Weiss et
al., 2013 and Gauntlett et al, 2012) found this treatment to significantly increase acceptance and
decrease depression, catastrophizing and functional disability.
Pharmaceutical Management
The World Health Organization (WHO) has the only guidelines on the pharmacological
treatment of persisting pain in children with medical illnesses and advocates a two-step approach
of acetaminophen and NSAIDS initially, followed by morphine or other opiate equivalents as
needed (WHO, 2012). In the United States, the Center for Disease Control (CDC) has issued
guidelines for the pharmacological management of chronic pain in adults but these specifically
exclude use for anyone under eighteen (Dowell, Haegerich & Chou, 2016). While the use of
opiates in chronic pain is rarely recommended in adolescents, they have been shown effective in
certain known disorders such as neurodegenerative diseases, juvenile arthritis and sickle cell
(Gregoire & Finley, 2013). This was demonstrated by a small practice study (Slater et al, 2010)
that found patients had better pain control and improved function while on opioid therapy. Many
of the medications currently used to treat chronic pain in children (i.e. amitriptyline, gabapentin,
and pregablin) are being used without evidence of safety and efficacy in children but rather on
findings extrapolated from adult trials (Walker, 2008).

Adolescent chronic pain management 9
Ketamine, an N-methyl-D-aspartate receptor antagonist, has been shown to improve pain
and decrease opioid use in the adult population and may be used as an adjunct for refractory pain
(Sheehy, et al, 2015). A longitudinal cohort study of consecutive pediatric patients (Sheehy, et
al, 2015), found that ketamine significantly reduced pain intensity (p<0.001). Pain reduction was
greatest in patients who suffered from trauma, complex regional pain syndrome (CRPS) and
postural orthostatic tachycardia syndrome (POTS) and was smallest in patients with chronic
headache. Similarly, a retrospective review by Mooney, Pagel and Kundu (2014), on the
efficacy of intravenous lidocaine infusions, found them to be well tolerated in adolescents, with
few side effects and significant pain relief. Interestingly, maximum pain reduction occurred in
patients with the highest reported intensity of pain (Mooney, Pagel & Kundu, 2014).
Complementary and Alternative Medicine (CAM) use in adolescents with chronic pain is
on the rise as methods for relief of pain are sought. This may encompass a group of diverse
medical practices and products that are not generally considered to be a part of conventional
medicine. Examples are herbal supplements, essential oils, massage, hypnotherapy, acupuncture
and yoga. In a study on CAM use by Vinson, Yeh, Davis and Deirdre (2014), a multivariable
model found that female gender, parental education, greater pain intensity and higher disability
were independently associated with CAM use. In addition, CAM use was found to have a
significant correlation with accommodative coping skills (B 0.2, p value 0=.003).
Implications for Nursing Education, Practice and Research
Pain assessment and management should by an integral part of all healthcare provided by
practitioners who care for children and adolescents. It is widely accepted that healthcare
providers are seeing a significant number of adolescents with chronic pain which is effecting
their development and quality of life. A multidisciplinary approach based on a biopsychosocial

Adolescent chronic pain management 10
framework has proven to be the most effective treatment strategy for adolescents with chronic
pain, however, most healthcare providers have limited understanding of this and instead refer
patients from specialist to specialist for diagnosis without adequately treating pain.
Unfortunately, there is limited information to guide clinical practice and a significant lack of
scientific data for the safety and efficacy of pharmaceuticals for the treatment of chronic pain.
There are enormous gaps in research on the pharmacological treatment of chronic and complex
pain in children and adolescents. Future research is desperately needed in the pharmacokinetics
and pharmacodynamics of drugs currently used in the treatment of chronic pain in children to
ensure safe and effective drug dosage. In addition, some classes of medications including
anticonvulsants and antidepressants being used in select pediatric pain conditions have not been
studied in this population and can have dramatically different results amongst users.
Conclusion
In the course of this research, a very limited amount of research was found related to the
treatment of chronic pain in children and adolescents. The majority of studies found, were small
in size and many had significant limitations identified. Most advocate a multidisciplinary
approach utilizing a biopsychosocial framework. The gaps in research on pharmacological
interventions are profound and the scientific community should be called upon to invest in
research on the safety and efficacy of pain-relieving medications, specifically in children with
persistent pain related to medical illnesses. Any findings measured in future studies should
include both positive (pain relief, improved quality of life, etc.) and negative (prevalence,
severity of adverse effects, etc.) outcomes. Finally, healthcare professionals, who will most
certainly encounter adolescents with chronic pain, are implored to validate the patient’s

Adolescent chronic pain management 11
complaints and work with them, their family members and other members of the healthcare team
to bring relief and improved quality of life.

Adolescent chronic pain management 12
References
Blécourt, A. C., Preuper, H. R., Schans, C. P., Groothoff, J. W., & Reneman, M. F. (2008).
Preliminary evaluation of a multidisciplinary pain management program for children and
adolescents with chronic musculoskeletal pain. Disability and Rehabilitation, 30(1), 13-
20. doi:10.1080/09638280601178816
Castle, K., Imms, C., & Howie, L. (2007). Being in pain: A phenomenological study of young
people with cerebral palsy. Developmental Medicine & Child Neurology, 49(6),
445-449. doi:10.1111/j.1469-8749.2007.00445.x
Clinch, J., & Eccleston, C. (2008). Chronic musculoskeletal pain in children: Assessment and
management. Rheumatology, 48(5), 466-474. doi:10.1093/rheumatology/kep001
Dobe, M., Hartmann, R., Kriszio, H., Hechler, T., Behlert, J., & Zernikow, B. (2013). Pain
Therapy in Childhood and Adolescent Chronic Pain. Practical Treatment Options for
Chronic Pain in Children and Adolescents, 75-184. doi:10.1007/978-3-642-37816-4_6
Dowell, D., Haegerich, T. M., & Chou, R. (2016). CDC Guideline for Prescribing Opioids for
Chronic Pain—United States, 2016. Jama, 315(15), 1624. doi:10.1001/jama.2016.1464
Fisher, E., Law, E., Palermo, T. M., & Eccleston, C. (2014). Psychological therapies (remotely
delivered) for the management of chronic and recurrent pain in children and adolescents.
Cochrane Database of Systematic Reviews Reviews. doi:10.1002/14651858.cd011118
Gauntlett-Gilbert, J., Connell, H., Clinch, J., & Mccracken, L. M. (2012). Acceptance and
Values-Based Treatment of Adolescents With Chronic Pain: Outcomes and Their
Relationship to Acceptance. Journal of Pediatric Psychology, 38(1), 72-81.
doi:10.1093/jpepsy/jss098
Groenewald, C. B., Essner, B. S., Wright, D., Fesinmeyer, M. D., & Palermo, T. M. (2014). The

Adolescent chronic pain management 13
Economic Costs of Chronic Pain Among a Cohort of Treatment-Seeking Adolescents in
the United States. The Journal of Pain, 15(9), 925-933. doi:10.1016/j.jpain.2014.06.002
Grégoire, M., & Finley, G. A. (2013). Drugs for Chronic Pain in Children: A Commentary on
Clinical Practice and the Absence of Evidence. Pain Research and Management, 18(1),
47-50. doi:10.1155/2013/402863
Gupta, R. (2014). Psychological Assessment of Chronic Pain. Pain Management, 19-20.
doi:10.1007/978-3-642-55061-4_7
Hechler, T., Wager, J., & Zernikow, B. (2014). Chronic pain treatment in children and
adolescents: Less is good, more is sometimes better. BMC Pediatrics BMC Pediatr,
14(1). doi:10.1186/1471-2431-14-262
Mooney, J. J., Pagel, P. S., & Kundu, A. (2014). Safety, Tolerability, and Short-Term Efficacy of
Intravenous Lidocaine Infusions for the Treatment of Chronic Pain in Adolescents and
Young Adults: A Preliminary Report. Pain Med Pain Medicine, 15(5), 820-825.
doi:10.1111/pme.12333
Odell, S., & Logan, D. (2013). Pediatric pain management: The multidisciplinary approach. JPR
Journal of Pain Research, 785. doi:10.2147/jpr.s37434
Palermo, T. M., Wilson, A. C., Peters, M., Lewandowski, A., & Somhegyi, H. (2009).
Randomized controlled trial of an Internet-delivered family cognitive–behavioral
therapy intervention for children and adolescents with chronic pain. Pain, 146(1), 205-
213. doi:10.1016/j.pain.2009.07.034
Rajapakse, D., Liossi, C., & Howard, R. F. (2014). Presentation and management of chronic
pain. Archives of Disease in Childhood, 99(5), 474-480. doi:10.1136/archdischild-2013-
304207

Adolescent chronic pain management 14
Sheehy, K. A., Muller, E. A., Lippold, C., Nouraie, M., Finkel, J. C., & Quezado, Z. M. (2015).
Subanesthetic ketamine infusions for the treatment of children and adolescents with
chronic pain: A longitudinal study. BMC Pediatrics BMC Pediatr, 15(1).
doi:10.1186/s12887-015-0515-4
Skrove, M., Romundstad, P., & Indredavik, M. S. (2014). Chronic multisite pain in adolescent
girls and boys with emotional and behavioral problems: The Young-HUNT study.
European Child & Adolescent Psychiatry Eur Child Adolesc Psychiatry, 24(5),
503-515. doi:10.1007/s00787-014-0601-4
Slater, M., Lima, J. D., Campbell, K., Lane, L., & Collins, J. (2010). Opioids for the
Management of Severe Chronic Nonmalignant Pain in Children: A Retrospective 1-Year
Practice Survey in a Children's Hospital. Pain Med Pain Medicine, 11(2), 207-214.
doi:10.1111/j.1526-4637.2009.00754.x
Suresh, S., & Shah, R. (2011). Chronic pain management in children and adolescents. Essentials
of Pain Medicine, 403-408. doi:10.1016/b978-1-4377-2242-0.00066-3
Tilburg, M. A., Spence, N. J., Whitehead, W. E., Bangdiwala, S., & Goldston, D. B. (2011).
Chronic Pain in Adolescents Is Associated With Suicidal Thoughts and Behaviors. The
Journal of Pain, 12(10), 1032-1039. doi:10.1016/j.jpain.2011.03.004
Tseng, A. S., Weiss, K., Harrison, T., Hansen, D., & Bruce, B. (2014). Pain Relief as a Primary
Treatment Goal: At What Point does Functioning and Well-Being Become more
Important? a Case Study of an Adolescent with Debilitating Chronic Pain. Pain
Research and Management, 19(4), 219-223. doi:10.1155/2014/745458
Valrie, C. R., Bromberg, M. H., Palermo, T., & Schanberg, L. E. (2013). A Systematic Review of
Sleep in Pediatric Pain Populations. Journal of Developmental & Behavioral

Adolescent chronic pain management 15
Pediatrics, 34(2), 120-128. doi:10.1097/dbp.0b013e31827d5848
Velleman, S., Stallard, P., & Richardson, T. (2010). A review and meta-analysis of computerized
cognitive behaviour therapy for the treatment of pain in children and adolescents. Child:
Care, Health and Development, 36(4), 465-472. doi:10.1111/j.1365-2214.2010.01088.x
Vinson, R., Yeh, G., Davis, R. B., & Logan, D. (2014). Correlates of Complementary and
Alternative Medicine Use in a Pediatric Tertiary Pain Center. Academic Pediatrics,
14(5), 491-496. doi:10.1016/j.acap.2014.04.003
Voerman, J. S., Remerie, S., Graaf, L. D., Looij-Jansen, P. V., Westendorp, T., Elderen, I. V., . . .
Klerk, C. D. (2012). Early signaling, referral, and treatment of adolescent chronic pain:
A study protocol. BMC Pediatrics BMC Pediatr, 12(1), 66. doi:10.1186/1471-2431-12-
66
Walker, S. M. (2008). Pain in children: Recent advances and ongoing challenges. British Journal
of Anaesthesia, 101(1), 101-110. doi:10.1093/bja/aen097
Weiss, K. E., Hahn, A., Wallace, D. P., Biggs, B., Bruce, B. K., & Harrison, T. E. (2013).
Acceptance of Pain: Associations With Depression, Catastrophizing, and Functional
Disability Among Children and Adolescents in an Interdisciplinary Chronic Pain
Rehabilitation Program. Journal of Pediatric Psychology, 38(7), 756-765.
doi:10.1093/jpepsy/jst028
WHO Guidelines on the Pharmacological Treatment of … (n.d.). Retrieved May 14th, 2016,
from http://www.ncbi.nlm.nih.gov/pubmed/23720867
Wojtowicz, A. A., & Banez, G. A. (2014). Adolescents with chronic pain and associated
functional disability: A descriptive analysis. Journal of Child Health Care, 19(4), 478-484.
doi:10.1177/1367493514523157

Adolescent chronic pain management 16
Tables
Table 1. Domains of clinical evaluation of chronic pain at presentation
Biological Psychological Social
Pain characteristics Mood School attendance
Site/sites Anxiety Social functioning (peer/family)
Time features- onset, frequency, etc.
Depression Parental behaviors (protective responsiveness, overbearing, minimization
Descriptors Cognitions (attitudes, beliefs) pain catastrophizing
Parent characteristics- age, educational level, economic status
Intensity (0-10) NRS Sleep Cognitions (catastrophizing, expectancies
Radiation Behavioral problems Isolation
Precipitating factors Social isolation Inability to participate in sports and hobbies
Relieving factors loneliness Chronic illness in parent-Parent with chronic pain
Physical functioning hopelessness Community resources available
Level of disability Resilience factors Ability to participate in activities- outings, Band, support groups
*Note- areas for Provider assessment

Adolescent chronic pain management 17
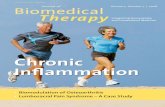
Figures
Figure 1. Proposed Management Algorithm of chronic pain in adolescents
Chronic Pain
Clear Diagnosis
medlDddDiagnosis
Unknown cause
Optimize Disease Specific
TREATMENT
Pain persists
NO YES
MANAGEMENT WITHIN
BIOPSYCHOSOCIAL
FRAMEWORK
Continue disease
specific Management
Pain education
Psychological TxSLEEP Medications
INTERVENTIONS
AS APPROPRIATE
PT/OTCAM- herbs,
hypnosis, yoga, etc.
Pain persists
Pediatric Pain
SpecialistInpatient or
outpatient pain rehab

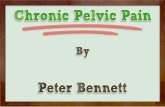
Adolescent chronic pain management 18
Figure 2. Experience of 17 year old with chronic pain and disability
SS
Pain
ananand
Family “My
mom/dad worry about me,
dad had change jobs to
stay home with me”
Fitness
“I used to be able to
walk with a walker, now I
only use my wheelchair.
Even swimming makes my
pain worse”
Independence “my
mom has to help me take a
shower and use the bathroom… I
used to be able to dress myself
It’s not fair… I’m 17”
Appetite
“I can’t eat when
the pain is bad, my meds make
my stomach hurt, I’m just not
hungry and sometimes the
pain is so bad I throw up’
Moods
“I get angry and
frustrated. I just go to my
room. I say mean things to my
family. I don’t want to talk to
anyone. I cry at night when I
can’t sleep”
Social Life
“I don’t see my
friends much, Mostly, I lay
in bed and watch TV- I used
to play in the school band”
Education
“I used to love school,
but have missed 85% of school
this year. I can’t concentrate
when my pain is bad”
Sleep
“I go to bed early but
wake up and can’t go back to
sleep, when I don’t sleep my pain
is worse”