Chronic Joint Pain
28
Volume 2, Number 2 ) 2008 Therapy Biomedical Chronic Inflammation • Biomodulation of Osteoarthritis • Lumbosacral Pain Syndrome – A Case Study Integrating Homeopathy and Conventional Medicine d 2.00 • US $ 2.00 • CAN $ 3.00 Journal of
-
Upload
ganesh-kumar -
Category
Documents
-
view
243 -
download
2
Transcript of Chronic Joint Pain

Volume 2, Number 2 ) 2008
TherapyBiomedical
Chronic Inflammation
• BiomodulationofOsteoarthritis• LumbosacralPainSyndrome–ACaseStudy
IntegratingHomeopathyandConventionalMedicine
d 2.00 • US $ 2.00 • CAN $ 3.00
Journal of

I n Fo c u sBiomodulation of Osteoarthritis . . . . . . . . . . . . . . . . . . . . . . . 4
Wh a t E l s e I s N e w ? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
S p e c i a l i z e d Ap p l i c a t i o n s Biopuncture Protocols for the Treatment of Chronic Inflammatory Disorders . . . . . . . . . . . . . . . . . . . . . 10
Re f r e s h Yo u r H o m o t ox i c o l o g y Movement and the Matrix: The Importance of Biomechanical Signals in Matrix Remodeling . . . . . . . . . . . . . 13
A r o u n d t h e G l o b eEvidence-Based Homeopathy – More Than Results of Double-Blind Studies! . . . . . . . . . . . . . .16
M a r ke t i n g Yo u r P ra c t i c eGetting Organized . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
N e w Pe r s p e c t i v e sSulfur in Health and Disease: A Hypothesis on Sulfur Intoxication . . . . . . . . . . . . . . . . . . . . 20
Fr o m t h e P ra c t i c eWhiplash – Acute Inflammation Becomes Chronic . . . . . . . . 24 Lumbosacral Pain Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
M a k i n g o f . . .Suis-Organ Products in Antihomotoxic Medicine . . . . . . . . . 26
)
) 2
Contents
Published by/Verlegt durch: International Academy for Homotoxicology GmbH, Bahnackerstraße 16, 76532 Baden-Baden, Germany, e-mail: [email protected] Editor in charge/verantwortlicher Redakteur: Dr. Alta A. SmitPrint/Druck: VVA Konkordia GmbH, Dr.-Rudolf-Eberle-Straße 15, 76534 Baden-Baden, Germany© 2008 International Academy for Homotoxicology GmbH, Baden-Baden, Germany
Cover photograph © 2008 bilderlounge media

A Holistic Approach to Chronic Inflammation
)
There is no longer any question that chronic inflammation is
the common denominator in almost all chronic illnesses, including sys-temic diseases such as arteriosclero-sis and metabolic syndrome.1 In this issue, though, we examine chronic inflammation’s role in disorders of the structured connective tissue of the musculoskeletal system. Such disorders fall into the next to last column of the Disease Evolution Table, i.e., the degeneration phase.We cannot embark on this journey without venturing into the fascinat-ing world of the extracellular ma-trix. Although long known to prac-titioners of biological medicine as the crux of cell and organ health, it is now also being recognized by mainstream medicine. In particular, the molecular basis of matrix re-modeling – after injury and as a normal physiological process – is under increasing scrutiny. This ana-
bolic/catabolic balance depends on delicate interactions among the im-mune, endocrine, vascular, and ner-vous systems, so the complex multi-target interventions available to bioregulatory medicine are especial-ly suited to restoring the balance. Dr. Martin Plotkin, an orthopedic surgeon and co-author of the focus article, uses such medications exten-sively in his practice. The focus ar-ticle concentrates on the modern pathophysiology of cartilage degen-eration, but as connective tissue uses the same mechanisms in both struc-tured and nonstructured matrix, the story becomes fascinating once we examine the effects of mechanical forces on matrix remodeling (see Refresh Your Homotoxicology).Antihomotoxic medicines offer a holistic approach to disorders of the musculoskeletal system, and case studies and protocols demonstrate the practical applications. Dr. Den-
nis van Aswegen, D.C. speaks out of long experience with such disorders in two cases from his practice. Dr. Edgar Estrada introduces the con-cept of sulfur “intoxication” and highlights a form of suppression that has not yet been widely recog-nized. Dr. Peter Smith reports from the LIGA conference in Oostend, Belgium. Lastly, Dr. Wilfried Stock continues the Making of … series with the suis organs, part 2 – an ar-ticle that is well-placed in this issue, given that organ support is one of the main pillars of antihomotoxic treatment in the degeneration phase.
Alta A. Smit, MD
Dr. Alta A. Smit
Reference:
1. Edwards T. Inflammation, pain, and chronic disease: an integrative approach to treat-ment and prevention. Altern Ther Health Med 2005;11(6):20-27.
) 3
Journal of Biomedical Therapy 2008)Vol.2,No.2

Journal of Biomedical Therapy 2008)Vol.2,No.2
Biomodulation of Osteoarthritis By Martin Plotkin, MD, and Alta A. Smit, MD
Introduction
Osteoarthritis (OA) is a chronic, dis-abling condition that affects synovial joints. Its pathogenesis involves mul-tiple etiologies, including mechani-cal, genetic, and biochemical factors. OA is generally described as “nonin-flammatory” arthritis in contrast to rheumatoid arthritis, but this is in-creasingly recognized as a misno-mer, since inflammation does indeed contribute to both the symptoms and the progression of OA.1 Morn-ing or inactivity stiffness is a com-mon symptom in OA, but acute in-flammatory flares with all the clinical signs (redness, warmth, swelling, and further loss of function) are also common in OA patients.
From the homotoxicological per-spective, OA falls into the degenera-tion phase on the Disease Evolution Table and shares many of the char-acteristics of degenerative disease processes, namely, chronic inflam-mation accompanied by the release of dangerous free radicals such as peroxynitrite, disturbance of the normal cycle of degeneration and repair, and disturbance of angiogen-ic balance in the direction of inap-propriate vascularization.
Inflammation in osteoarthritis
The effects of subclinical chronic in-flammation in OA are now increas-ingly being recognized.2 The onset of acute inflammation is generally sudden, with the above-mentioned symptoms developing in a matter of minutes or hours. Neutrophils are
the most abundant cells and proin-flammatory cytokines such as IL-1, TNF-α, and IL-8 are the most prominent. In contrast, chronic in-flammation develops over a longer period of time and may persist for weeks, months, or years. Markers of chronic inflammation such as C-re-active protein (CRP) may be elevat-ed in patients with OA and may be mediated by IL-6, which is the ma-jor cytokine secreted by macrophag-es. IL-6 may also play a role in an-giogenesis, which is another factor contributing to the pathology of OA (see below).The outcome of acute inflammation is elimination of the irritation, fol-lowed by restoration of the tissues to their original state. In chronic in-flammation, on the other hand, in-flammation and repair occur concur-rently, and the joints remain
) I n Fo c u s
) 4
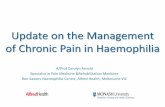
Figure 1: Degradation and repair in the matrix. In osteoarthritis, the catabolic/anabolic rhythm is disturbed.
Interleukin-1Interleukin-6
TumorNecrosisFactor
BoneMorphogeneticProteins(Transforming
GrowthFactorβ)Chondrocyte
MeTALLOPrOTeINASeS
TISSueINFLAMMATIONANddeGrAdATION
(Freeradicals)
Osteoarthritis
ANTIMeTALLOPrOTeINASeS
TISSuerePAIr
Tissuehealing

Journal of Biomedical Therapy 2008)Vol.2,No.2
abnormal even after the inflamma-tion subsides. In chronic inflamma-tion, the cells that predominate are macrophages and often lymphocytic infiltrates. Chronic inflammation can therefore be seen as a misguided at-tempt on the part of chondrocytes and other cells to eliminate damaged tissue and to effect repair.
Anabolic/catabolic imbalance
Oscillation between degradation and repair is a normal occurrence in the matrix. Although the extracellu-lar matrix is the functional unit in this process, homeostasis is affected by chondrocytes. Matrix metallo-proteinases (MMPs) are stimulated by inflammatory cytokines and ma-trix degradation products to induce degradation of older or damaged tissues and are counterbalanced by a number of growth factors, notably also members of the TGF-β family, Bone Morphogenetic Proteins
(BMPs), which reciprocally inhibit the actions of the MMPs and there-fore induce tissue healing. This cata-bolic/anabolic oscillation is of vital importance in normal tissue integri-ty.3,4 When the process is disturbed (due to continuous tissue damage, either by mechanical stressors or toxins) or the body’s ability to trig-ger repair reduced (due to either a deficiency of growth factors or an inability to respond to them, as is seen in old age), an overactive cata-bolic/anabolic cycle results (see Fig-ure 1). To better understand cartilage de-struction, at least inasmuch as it is mediated by chondrocytes them-selves (sometimes called chondro-cytic chondrolysis), we must study the molecular mechanisms that dis-rupt the balance between chondro-cyte catabolic and anabolic activity. Since chondrocytes are lost to cell death at some point in the process of cartilage destruction, it is also im-
portant to know whether these mo-lecular factors also contribute to cell death.The cause of chronic synovitis in OA is not well understood. Debris or parts of cartilage may be found in the synovium, where they provoke typical responses to foreign bodies. Mechanical injury can also lead to the secretion of free radicals or reac-tive oxygen species (ROS).
ROS and chronic cartilage destruction
The role of ROS in cartilage damage remains controversial. Recently, Green et al. added to the literature describing the role of ROS release after mechanical injury in the pro-gression of cartilage destruction.5 Nitric oxide in particular is impli-cated in this process and may com-bine with other ROS to form the highly toxic compound peroxyni-trite.
) 5
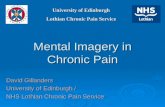
Figure 2: Molecular pathophysiology of osteoarthritis (adapted from Loeser1)
ExCESSIvE MECHAnICAL fORCE
damagedmatrixIncreasedrOSproduction
Activationofcatabolicsignalingpathwaysandinhibitionof
anabolicpathways
Chronicinflammation
Activation of signaling pathwaysand ROS production
AGED CELL
PoorresponsetogrowthfactorsdegradativepathwaysstayonContinuedmatrixdestruction
UnBALAnCED CHOnDROCyTE METABOLIC ACTIvITy
Catabolic > Anabolic
AngiogenesisVeGF,FGF
OsteophytesPain
Matrix Growthfactorrelease
degradedamagedmatrix
Cytokines,chemokines,growthfactorsandproteolyticenzymes
Matrix fragments

Journal of Biomedical Therapy 2008)Vol.2,No.2
) I n Fo c u s
ROS also will induce inflammatory mediators, such as NF-κB, IL-1, and IL-6. ROS have been implicated in chondrocyte senescence.6 ROS may also have a direct influence on the production of Vascular Endothelial Growth Factor (VEGF), a powerful stimulator of angiogenesis and chronic inflammation.7
Angiogenesis and chronic inflammation
The formation of new blood vessels is essential during fetal development but rarely occurs in adults except in overzealous attempts at remodeling and regeneration, as in OA. Inflam-matory mediators can stimulate an-giogenesis either directly or indi-rectly. Inflammatory cells that pro duce this effect include mac-rophages and mast cells, which are present in the OA synovium. Mac-rophages are generally found wher-ever abnormal angiogenesis occurs, as in synovitis and tumors. Angio-genesis may be important in poten-tiating or perpetuating inflamma-tion, rather than initiating it. On the other hand, angiogenesis may be in-directly self-perpetuating because it increases inflammatory cell infiltra-tion and thus increases the cells that secrete angiogenic factors such as VEGF and Fibroblast Growth Factor (FGF-1).8
Vascularization of normally avascu-lar cartilage and at the osteochon-dral junction is a feature of OA. In growing individuals, angiogenesis is required for normal endochondral ossification to close long bones. This process is mediated by VEGF from hypertrophic chondrocytes. In OA, however, growth through osteo-phytes at the joint margin also oc-curs through osteochondral ossifica-tion. Cartilaginous extensions of the articular surface become invaded by blood vessels, and bone extends from the subchondral structures.
Neoinnervation also follows angio-genesis and may contribute to pain in chronic synovitis (see Figure 2).Targeting these aspects could lead to novel approaches to treating OA. The fact that Zeel, a homeopathic combination medication, is formu-lated to address these aspects, along with its excellent tolerability, makes it an ideal option for treating the chronic inflammation seen in OA.
Bioregulatory treatment of OA
We have seen in the previous section that OA is characterized by chronic, low grade inflammation with fre-quent flare-ups of acute inflamma-tion. Conventional treatments (NSAIDs, paracetamol/acetamino-phen, and/or intra-articular corti-costeroids) act to suppress only cer-tain aspects of the inflammation and have significant side effects.Intra-articular administration of hya luronic acid attempts to supply the cartilage with proteoglycan sup-port.9 Combinations of chondroitin sulfate and glucosamine have long been used for this purpose in treat-ing OA, with variable evidence of efficacy.10,11,12 Some promising new treatments use autologous serum.13 The use of antioxidants in OA has not been proven to be beneficial and remains controversial.14
In view of the pathogenesis outlined above, the use of low-concentration antigens with a multi-target regula-tion such as is seen in the antihomo-toxic repertoire becomes interest-ing.
Traumeel and Zeel as combination therapy in OA
Traumeel has been shown in studies to be both clinically efficacious and an immune-modulating medica-tion15-21 and should be considered for its immune-regulating proper-ties, which promote repair while
permitting a certain level of inflam-mation so that degradation of debris can occur. Zeel has been used for degenerative arthritis for many years; empirical evidence indicates that it is as effec-tive as Cox-1 and Cox-2 inhibitors in treating OA.22 However, it may have a special role to play with re-gard to the pathophysiology of chronic inflammation. Many of its ingredients, such as Rhus tox, con-tain flavonoids, known for their an-tioxidant effects.23 Rhus tox and Ar-nica also have been shown to have effects on IL-6, which is secreted by macrophages and may play a central role in chronic inflammation and an-giogenesis. In an animal study, Stančíková demonstrated that when rabbits with experimentally induced arthritis were treated with either Zeel or a solvent (reference sub-stance), the Zeel group developed far fewer erosions and less hypertro-phic cartilage than the solvent group.24 Histochemical analysis also revealed significant vascularization of the deeper layers of cartilage in the animals treated with the solvent, whereas the Zeel group developed only a few capillaries. (In view of the central role that angiogenesis appears to play in the pathophysiol-ogy of OA, this is a very important finding.) And finally, the arrange-ment of chondrocytes was also much more structured in the verum group. It is interesting to note that the alka-loid sanguinarine, found in Sangui-naria canadensis (one of Zeel’s in-gredients), has been shown to inhibit VEGF.25,26
Conclusion
Ongoing research is clarifying the complex pathophysiology of OA. Disruption of the catabolic/anabolic cycle of the cartilaginous matrix ap-pears paramount. New evidence
) 6

Journal of Biomedical Therapy 2008)Vol.2,No.2
) I n Fo c u s
suggests that both the generation of ROS (through mechanical pressure) and angiogenesis contribute signifi-cantly to the development of chron-ic inflammation, tissue destruction, and pain. Standard treatment with NSAIDs aims primarily to reduce inflammation and control pain. Sub-stances that inhibit MMPs are cur-rently deemed too toxic to be of any use in OA. Viscosupplements, chon-droitin sulfate and glucosamine, and some other novel treatments are also used, with variable evidence of effi-cacy.Due to the different effects of the two antihomotoxic medications Traumeel and Zeel on acute and chronic inflammation, it is feasible to administer these two products in combination: Zeel for long-term treatment, Traumeel at the begin-ning of treatment and for acute flare-ups. Both of these medications have been shown to have excellent tolerability profiles. Further research is warranted to clarify the exact ef-fect of Zeel on angiogenesis and the effect of the medication on ROS in chronic inflammation.|
References
1. Loeser RF. Molecular mechanisms of carti-lage destruction: mechanics, inflammatory mediators, and aging collide. Arthritis Rheum 2006;54(5):1357-1360.
2. Bonnet CS, Walsh DA. Osteoarthritis, an-giogenesis and inflammation. Rheumatology 2005;44:7-16.
3. Aigner T, Soeder S, Haag J. IL-1ß and BMPs – interactive players of cartilage matrix deg-radation and regeneration. Eur Cell Mater 2006;12:49-56.
4. Yasuda T, Poole AR. A fibronectin fragment induces type II collagen degradation by col-lagenase through an interleukin-1-mediated pathway. Arthritis Rheum 2002;46:138-148.
5. Green DM, Noble PC, Ahuero JS, Birdsall HH. Cellular events leading to chondrocyte death after cartilage impact injury. Arthritis Rheum 2006;54:1509-1517.
6. Yudoh K, Nguyen T, Nakamura H, Hongo-Masuko K, Kato T, Nishioka K. Potential involvement of oxidative stress in cartilage senescence and development of osteoar-thritis: oxidative stress induces chondrocyte telomere instability and downregulation of chondrocyte function. Arthritis Res Ther 2005;7(2):R380-R391.
7. Fay J, Varoga D, Wruck CJ, Kurz B, Gol-dring MB, Pufe T. Reactive oxygen species induce expression of vascular endothelial growth factor in chondrocytes and human articular cartilage explants. Arthritis Res Ther 2006;8(6):R189.
8. Mentlein R, Pufe T. New functions of angio-genic peptides in osteoarthritic cartilage. Curr Rheumatol Rev 2005;1:37-43.
9. Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G. Viscosupplementa-tion for the treatment of osteoarthritis of the knee. Cochrane Database Syst Rev 2006; 19;(2):CD005321.
10. Barnhill JG, Fye CL, Williams DW, Reda DJ, Harris CL, Clegg DO. Chondroitin product selection for the glucosamine/chondroitin arthritis intervention trial. J Am Pharm Assoc 2006;46(1):14-24.
11. Clegg DO, Reda DJ, Harris CL, et al. Glu-cosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med 2006;354(8):795-808.
12. Hochberg MC. Nutritional supplements for knee osteoarthritis – still no resolution. N Engl J Med 2006;354:858-859.
13. Wehling P, Moser C, Frisbie D, et al. Autolo-gous conditioned serum in the treatment of orthopedic diseases: the orthokine therapy. BioDrugs 2007;21(5):323-332.
14. Henrotin Y, Kurz B. Antioxidant to treat os-teoarthritis: dream or reality? Curr Drug Tar-gets 2007;8(2):347-357. ) 7
15. Heine H, Schmolz M. Induction of the im-munological bystander reaction by plant ex-tracts. Biomed Ther 1998;16(3):224-226.
16. Porozov S, Cahalon L, Weiser M, Branski D, Lider O, Oberbaum M. Inhibition of IL-1β and TNF-α secretion from resting and ac-tivated human immunocytes by the homeo-pathic medication Traumeel® S. Clin Dev Im-munol 2004;11(2):143-149.
17. Lyss G, Knorre A, Schmidt TJ, Pahl HL, Mer-fort I. The anti-inflammatory sesquiterpene lactone helenalin inhibits the transcription factor NF-kappaB by directly targeting p65. J Biol Chem 1998;273(50):33508-33516.
18. Zell J, Connert W-D, Mau J et al. Treat-ment of acute sprains of the ankle. Biol Ther 1989;7(1):1-6.
19. Schneider C, Klein P, Stolt P, Oberbaum M. A homeopathic ointment preparation com-pared with 1% diclofenac gel for acute symp-tomatic treatment of tendinopathy. Explore 2005;1(6):446-452.
20. Birnesser H, Oberbaum M, Klein P, Weiser M. The homeopathic preparation Traumeel S compared with NSAIDs for symptomatic treatment of epicondylitis. J Musculosekelet Res 2004;8(2-3):119-128.
21. Singer SR, Amit-Kohn M, Weiss S, Rosen-blum J, Lukasiewicz E, Itzchaki M, Oberbaum M. Efficacy of a homeopathic preparation in control of post-operative pain – A pilot clini-cal trial. Acute Pain 2007;9(1):7-12.
22. Birnesser H, Stolt P. The homeopathic an-tiarthritic preparation Zeel comp. N: a re-view of molecular and clinical data. Explore 2007;3(1):16-22.
23. Mersch-Sundermann V, Kassie F, Böhmer S, et al. Extract of Toxicodendron quercifolium caused genotoxicity and antigenotoxicity in bone marrow cells of CD1 mice. Food Chem Toxicol 2004;42(10):1611-1617.
24. Stančíková M, Bély M, Metelmann HW, et al. Effects of Zeel comp. on experimental osteoarthritis in rabbit knee. Rheumatologia 1999;13:101-108.
25. Basini G, Bussolati S, Santini SE, Grasselli F. Sanguinarine inhibits VEGF-induced an-giogenesis in a fibrin gel matrix. Biofactors 2007;29(1):11-18.
26. Basini G, Santini SE, Bussolati S, Gras-selli F. Sanguinarine inhibits VEGF-induced Akt phosphorylation. Ann N Y Acad Sci 2007;1095:371-376.
Osteoarthritis is generally described as “non-inflammatory” arthritis, but acute flare-ups with clinical signs of inflammation such as redness, warmth, swelling, pain, and loss of function are common in OA patients (here: inflamed elbow joint).

Journal of Biomedical Therapy 2008)Vol.2,No.2
) W h a t E l s e I s N e w ?
) 8
Myths in medicine
Even western medicine is not always strictly rational, and little headway has been made against its unfounded myths and preconceptions. For ex-ample, the claim that only 10 per-cent of the human brain is utilized is demonstrably false. There is also no scientific evidence to support the re-peatedly postulated health-promot-ing effects of drinking a daily mini-mum of eight glasses of water. Hair and fingernails do not continue to grow after death, nor does shaving make hair grow back faster and thicker. Ophthalmologists agree that reading by flashlight under the cov-ers at night will not ruin your eyes, and eating turkey will not make you sleepy any faster than other, simi-larly fatty or heavy foods. Forbid-ding the use of cell phones in hospi-tals may be conducive to patients’ recovery, but to date there is no proof that radiation emitted by the phones makes medical equipment malfunction. In tests, interference has been noted only in rare instanc-es when mobile phones and medical electronic devices were in very ex-tremely close proximity.
BMJ 2007;335:1288-1289
Honey for coughs
Honey relieves coughs in children, according to a randomized study in which 105 children with upper re-spiratory infections were given hon-ey, a cough suppressant, or no medi-cation at night before going to bed. The children who received honey fared the best not only in terms of frequency and severity of coughing but also with regard to quality of sleep (both their own and their par-ents’).
Arch Pediatr Adolesc Med 2007;161(12):1140-1146
Mozart as medicine
Not only is Mozart’s music beauti-ful, it also has its uses in the ICU. In one study, 10 patients on artificial respiration listened to slow move-ments from Mozart’s piano sonatas through earphones for one hour on the first day after surgery, with as-tonishing effects. In comparison to the control group, the patients who received “Mozart therapy” experi-enced decreases in heart rate and blood pressure and required signifi-cantly less sedation.
Crit Care Med 2007;35(12):2709-2713
Children who are given honey before going to bed cough less than those who receive a cough suppressant or no medication at all.
Couch potatoes age faster
It has long been known that regular exercise has positive effects on health, but now a study conducted at King’s College in London has shown that physically active people also seem to be biologically younger than their nonathletic age peers. Scientists used leukocyte telomere lengths to determine the biological age of more than 2,400 subjects ranging in age from 18 to 81. Te-lomeres are the terminal sections of DNA that protect chromosomes from destruction. Over the course of a lifetime, telomeres become shorter, leaving the chromosomes more sus-ceptible to damage and disease. Sci-entists found that older but more active subjects had the same telo-mere lengths as younger people who were inactive. It seems, therefore, that lack of physical exercise accel-erates the aging process. An active lifestyle that includes ade-quate exercise is both “good medi-cine” and a cost-effective anti-aging strategy. Science has now provided couch potatoes with one more bit of motivation to become active.
Arch Intern Med 2008;168(2):154-158

Journal of Biomedical Therapy 2008)Vol.2,No.2
) W h a t E l s e I s N e w ?
Plush bacilli and huggable microbes
There’s nothing new under the sun: Stuffed animals are now available in the shape of viruses, microbes, and other germs. The selection of 15 cm-long “GIANTmicrobes,” as the American manufacturer calls its cud-dly bacilli, includes Helicobacter pylori, the syphilis germ, and the AIDS virus (complete with its own red AIDS ribbon) – to name just a few. Prices for these monster mi-crobes begin at $7.95 US (7 euros). The real items are usually free, but they’re harder to get rid of than stuffed animals.
www.giantmicrobes.com
Taciturn or talkative?
Gender has no bearing on how much a person talks, according to a study conducted by Texas scientists who recorded snippets of students’ conversations. They found that in the course of a day, men talk just as much as women – roughly 16,000 words, on average, although there were significant variations within each gender. Taciturn men and women alike got by on approxi-mately 8,000 words per day, while chatterboxes of either sex let loose 24,000 words during the same time period.
New Scientist 2007;195(2612);18
) 9
F O R P R O F E S S I O N A L U S E O N L Y
The information contained in this journal is meant for professional use only, is meant to convey general and/or specific worldwide scientific information relating to the products or ingredients referred to for informational purposes only, is not intended to be a recommendation with respect to the use of or benefits derived from the products and/or ingredients (which may be different depending on the regulatory environment in your country), and is not intended to diagnose any illness, nor is it intended to replace competent medical advice and practice. IAH or anyone connected to, or participating in this publication does not accept nor will it be liable for any medical or legal responsibility for the reliance upon or the misinterpretation or misuse of the scientific, informational and educational content of the articles in this journal.The purpose of the Journal of Biomedical Therapy is to share worldwide scientific information about successful protocols from orthodox and complementary practi-tioners. The intent of the scientific information contained in this journal is not to “dispense recipes” but to provide practitioners with “practice information” for a better understanding of the possibilities and limits of complementary and integrative therapies.Some of the products referred to in articles may not be available in all countries in which the journal is made available, with the formulation described in any article or available for sale with the conditions of use and/or claims indicated in the articles. It is the practitioner’s responsibility to use this information as applicable and in a manner that is permitted in his or her respective jurisdiction based on the applicable regulatory environment. We encourage our readers to share their complementary therapies, as the purpose of the Journal of Biomedical Therapy is to join together like-minded practitioners from around the globe.Written permission is required to reproduce any of the enclosed material. The articles contained herein are not independently verified for accuracy or truth. They have been provided to the Journal of Biomedical Therapy by the author and represent the thoughts, views and opinions of the article’s author.
Contrary to popular belief, women do not talk more than men. However, there are significant variations within each gender.
Fear increases sensory acuity
Being afraid heightens your sense of smell. That was the admittedly over-simplified conclusion of an Ameri-can study that investigated the con-nection between olfactory acuity and emotional stress in 12 young adults. Subjects were asked to iden-tify the non-matching substance in a series of three chemicals that smelled very similar. Results improved sig-nificantly during the second round of smell testing, when the partici-pants were exposed to stress in the form of mild electric shocks. The in-vestigators interpreted this mecha-nism as a survival strategy that helps humans sort out dangerous “mes-sages” from an overabundance of sensory stimuli.
Science 2008;319(5871):1842-1845
New scientific findings show that regular physical exercise slows down the aging process.

) 10
Journal of Biomedical Therapy 2008)Vol.2,No.2
Introduction
Biopuncture is the injection of bio-therapeutics into indication or tis-sue-related zones or points on the body, as determined through clinical and functional diagnosis.1 The ther-apeutic agents may be administered subcutaneously or injected into joints, muscles, or ligaments.2 Ad-ministering the medications in the right spots or in the relevant body zone enhances the clinical effect. In-creasing numbers of physicians are realizing that such injections can ex-pand the scope of their practice.3
Biopuncturists use both antihomo-toxic medications and hyaluronic acid.4,5,6 Lymphomyosot is used for lymphatic drainage and matrix de-toxification and Traumeel is used to regulate the inflammatory response. Spascupreel is injected for muscular
spasms and Coenzyme compositum for tissue repair (damage on the cel-lular level). Zeel and hyaluronic acid are used for chronic joint pain in the elderly and for degenerative joint disease (cartilage damage). Many doctors combine several ampoules in a single injection to achieve better results (see Table 1).Local anesthetics can be added as modulators of neural information and to make the injections less pain-ful. Biopuncturists use low concen-trations of local anesthetics such as 0.5 percent procaine or 0.25 percent lidocaine.7 Hypertonic dextrose can also be added to stimulate healing of injured connective tissues such as capsules, fascia, ligaments, and pe-riosteum.
Frequency and location of injections
Biotherapeutic agents are adminis-tered once weekly by injection into zones or points related to the indi-cation or affected tissue. In selecting injection sites, we opt for either lo-cal injections (e.g., in the pain zone) or distant injections (e.g., in trigger points) and select one of four tissue types for injection:
1. subcutaneous, 2. intramuscular, 3. soft tissues (e.g., a bursa or around a tendon), 4. a ligament, enthesis, or periosteum.
Different steps of local injections
When dealing with chronic inflam-matory disorders, a step-by-step procedure enhances clinical results.1 We begin, for example, with local administration of a lymphatic drain-age agent to cleanse the local matrix. For this purpose, we use local subcu-taneous injections with Lymphomy-osot (phase 1 product). Traumeel is then used for local immunomodula-
) S p e c i a l i z e d A p p l i c a t i o n s
Biopuncture Protocols for the Treatment of Chronic Inflammatory Disorders By Jan Kersschot, MD
For subcutaneous injections Lymphomyosot + Traumeel
For soft tissue injections (e.g., tendon) Lymphomyosot + Traumeel
For intramuscular injections (overuse/posttraumatic)
Lymphomyosot + Traumeel
For intramuscular injections (spasms) Lymphomyosot + Spascupreel
For ligament injections Traumeel + dextrose
For chronic inflammation (cellular) Traumeel + Coenzyme compositum
For chronic inflammation ( joint degeneration) Traumeel + Zeel
Table 1: Examples of standard combinations commonly used by biopuncturists
Phase 1 product: Lymphomyosot
Phase 2 product: Traumeel
Phase 3 products: Spascupreel or a Homaccord ampoule
Phase 4 products: Coenzyme compositum or other compositum or Zeel
Step 1: Once weekly for two weeks: Subcutaneous or soft-tissue injections of Lymphomyosot and Traumeel in the pain zone
Step 2: Once weekly for two weeks: Intramuscular injection of Traumeel (or Lymphomyosot + Spascupreel) into myofascial pain points or trigger points. Alternatively, injection of Traumeel and dextrose into ligaments
Step 3: Once weekly for two weeks: Deeper injections of Traumeel + Coenzyme compositum into the above-mentioned points

) 11
Journal of Biomedical Therapy 2008)Vol.2,No.2
tion (phase 2 product). At a later stage, we can inject more specific, symptom-related medications such as Spascupreel or a Homaccord am-poule if available (phase 3 products). Finally, we work on a deeper (cellu-lar) level with injections of medica-tions such as Coenzyme composi-tum, Zeel, or Discus compositum (phase 4 products). (See table 2).
The step-by-step strategy is not set in stone but can be adapted to each patient’s specific situation. Begin-ning with Lymphomyosot is espe-cially important for hyper-respond-ers (sensitive patients). The three steps and six weekly sessions shown in Table 3 are a typical example of step-by-step biopuncture treatment of chronic inflammatory disorders. In the first step, which combines
phase 1 and phase 2 products, a mixture of Lymphomyosot and Traumeel is administered once weekly for two weeks. These medi-cations are usually injected either subcutaneously or into the soft tis-sues surrounding the site of chronic inflammation. In step 2, Traumeel (or Lymphomyosot and Spascupreel) can then be injected into the myo-fascial pain points or myofascial trigger points. When painful spots are found in ligaments, Traumeel and dextrose are injected into these spots. In step 3, a mixture of Traumeel and Coenzyme composi-tum or Zeel and Coenzyme com-positum is used.
Clinical applications of biopuncture in treating chronic inflammatory disorders
In cases of chronic inflammatory disorders, we usually administer six weekly injections and then give the body six weeks to respond and achieve bioregulation and complete healing. If necessary, the whole pro-cess (another series of 6 injections) may be repeated.
Phase 1 product: Lymphomyosot
Phase 2 product: Traumeel
Phase 3 products: Spascupreel or a Homaccord ampoule
Phase 4 products: Coenzyme compositum or other compositum or Zeel
Table 2: Phase products used in biopuncture
Step 1: Once weekly for two weeks: Subcutaneous or soft-tissue injections of Lymphomyosot and Traumeel in the pain zone
Step 2: Once weekly for two weeks: Intramuscular injection of Traumeel (or Lymphomyosot + Spascupreel) into myofascial pain points or trigger points. Alternatively, injection of Traumeel and dextrose into ligaments
Step 3: Once weekly for two weeks: Deeper injections of Traumeel + Coenzyme compositum into the above-mentioned points
Table 3: Example of a standard step-by-step biopuncture treatment for chronic inflammatory disorders
Zeel is used to treat chronic joint pain in elderly patients and for degenerative joint disease with cartilage damage.

) S p e c i a l i z e d A p p l i c a t i o n s
) 12
Journal of Biomedical Therapy 2008)Vol.2,No.2
Here are three examples of chronic disorders: in the shoulder, in the knee, and in the Achilles tendon.
Chronic shoulder pain
We begin by injecting Traumeel and Lymphomyosot subcutaneously into the pain zone (step 1). If the biceps tendon is tender upon clinical ex-amination, we also administer an-other injection near the tendon. This treatment is repeated one week later. In the third and fourth sessions (step 2), Lymphomyosot and Traumeel (or Spascupreel) may be injected into several different muscles (e.g., pectoral, trapezius, infraspinatus: see Figure 1, deltoid) and/or Traumeel and dextrose may be injected into the shoulder ligaments (e.g., AC lig-ament, coraco-clavicular ligament) or into the joint capsule. In the fifth and sixth sessions (step 3), injections of Coenzyme compositum (or Zeel, in the case of degeneration of the shoulder joint) may be administered on several different levels per ses-
sion: subcutaneously in the shoulder pain zone, into muscles or near ten-dons, and/or into ligaments.
Chronic knee pain
We usually begin with two sessions of subcutaneous injections of Traumeel and Lymphomyosot in the pain zone (step 1). If the patellar tendon is tender, the same combina-tion is also injected near the tendon. In the third and fourth sessions (step 2), Lymphomyosot plus Traumeel or Spascupreel may be injected i.m. (e.g., into the quadriceps) and/or Traumeel and dextrose may be in-jected into the collateral ligaments or the pes anserinus (see Figure 2). In the fifth and sixth sessions (step 3), Coenzyme compositum (or Zeel in elderly patients or in cases of de-
generative joint disease) may be in-jected into the above-mentioned sites.
Chronic Achilles tendinosis
Step 1 consists of two sessions of injections of Traumeel plus Lym-phomyosot administered s.c. and around the tendon (Figure 3). In the third and fourth sessions, Traumeel may be injected into soft tissue clos-er to the tendon while Lymphomyo-sot plus Traumeel (or Spascupreel) is injected into the calf muscle (step 2). In the fifth and sixth sessions, Coen-zyme compositum may be injected near the tendon and into the calf muscle (step 3).|
Chronic shoulder pain Chronic knee pain Chronic Achilles tendinosis
References
1. Kersschot J. Biopuncture – A New Clinical Guide. Aartselaar, Belgium: Inspiration Pub-lishing; in press.
2. Kersschot J. Biopuncture and the Manage-ment of Sports Injuries. Albuquerque, NM: Jaysea Press; 2008.
3. Barkauskas D. Biopuncture in Family Prac-tice. Paper presented at: HSA Congress 2008; June 8, 2008; Drakensberg Mountains, South Africa.
4. Smit A, O’Byrne A, Van Brandt B, Bianchi I, Küstermann K. Introduction to Bioregulatory Medicine. Stuttgart, Germany: Thieme Pub-lishers; in press.
5. Kersschot J. Biopuncture in General Practice. Aartselaar, Belgium: Inspiration Publishing; 2004: 56-57.
6. Arnold W, Fullerton DS, Holder S, May CS. Viscosupplementation: managed care issues for osteoarthritis of the knee. J Manag Care Pharm 2007;13(4)(suppl):3-19.
7. Iwama H, Akama Y. The superiority of water-diluted 0.25% to neat 1% lidocaine for trigger-point injections in myofascial pain syndrome: a prospective, randomized, double-blinded trial. Anesth Analg 2000;91(2):408-409.

) Re f r e s h Yo u r H o m o t ox i c o l o g y
Movement and the Matrix The Importance of Biomechanical Signals in Matrix Remodeling By Alta A. Smit, MD
) 13
Journal of Biomedical Therapy 2008)Vol.2,No.2
The role of the connective tissue as a body-wide signaling net-
work has been recognized by the ancient cultures and has been re-cently revisited by authors such as Langevin.2 She also makes the con-nection between the connective tis-sue planes and the meridians, there-by offering an explanation of phenomena observed in daily prac-tice when working with acupunc-ture points.3
The role of mechanical forces on the ECM is also becoming clearer, al-though the exact mechanism of ac-tion is still not completely known. In the past two decades, research has determined that many cells are sen-sitive to mechanical forces and can change their phenotype as well as the structure of the surrounding connective tissue. Of even greater interest, cells that share a common ECM may alter their mechanical en-
vironment by inducing other cells to remodel the ECM, as happens in lung tissue where fibrosis is the out-come, even if there is no inflamma-tion in the environment.4
According to Langevin and others, a number of possibilities emerge when looking for possible signals sensitive to mechanical forces:
1. Electrical signals
Szent-Györgyi used the term “bio-energetics” to refer to energy not confined in biomolecules but emit-ted or absorbed directly by tissue. As early as 1941, Szent-Györgyi proposed that electrons can propa-gate through crystalline structures both within and between molecules, forming semiconducting currents entirely separate from the movement of ions, previously assumed to be the only possible basis for bioelec-
tricity.5 This is the working mecha-nism postulated to explain the recent discovery that rotational field quan-tum magnetic resonance (RFQMR) can be used to regenerate cartilage in osteoarthritis of the knee joint.6 The major stimulus for bone and cartilage formation is a piezoelectric signal generated when the bone or cartilage is subjected to tension or compression. This knowledge is widely used today in orthopedics, where it is known that bone atro-phies, as during space travel or when immobilized or not used. In these cases, therefore, movement is en-couraged to support better healing, and ultrasound or other devices may be used to simulate the piezoelectric signal. Transmission of this piezo-electric signal is also impaired fol-lowing joint injury and trauma or in diseases such as osteoarthritis.7
2. Cellular signals
Connective tissue fibroblasts have been shown to become active after mechanical stretching,8 and sports medicine has documented the effect of stretching on healing tendons and other structures.9,10 Even ionic membrane pumps and cytoplasmic enzyme reactions have been shown to respond to mechanical stimuli. Recent evidence suggests that stretching may even attenuate in-flammatory signals in osteoarthritis joints.
To stay healthy, the extracellular matrix (ECM) must
renew itself constantly. The anabolic/catabolic cycle of
tissues is one of the body’s homeostatic mechanisms that
follow a biorhythm. All such processes involve close
orchestration among different systems, namely the
immune system, hormonal system, and local mediators.
Various triggers for remodeling have been postulated,
ranging from denatured tissue to mechanical forces.1

) 14
Journal of Biomedical Therapy 2008)Vol.2,No.2
) Re f r e s h Yo u r H o m o t ox i c o l o g y
Data suggest that constant applica-tion of cyclic tensile strain (CTS) blocks IL-1β-induced proinflamma-tory genes at the transcriptional level. The signals generated by CTS are sustained after its removal, with their persistence dependent on the length of CTS exposure. Further-more, the sustained effects of me-chanical signals are also reflected in their ability to induce aggrecan syn-thesis. These effects were seen on transcription factors of inflammato-ry mediators on chondrocyte stretch in vivo. These findings, extrapolated to human chondrocytes, may pro-vide the insight needed to achieve optimal sustained effects of physical therapies in the management of ar-thritic joints.11
3. Plasticity signals
Structural change of an organism is closely related to the cell’s ability to modulate its pericellular environ-ment, whether in the normal process of growth, in maintaining homeo-stasis, or as part of a disease process. This response of connective tissue to mechanical stress is well-known. According to Langevin, it takes place over days or weeks following a change in posture or a new activi-ty. It follows remodeling of the ECM with changes in the collagen matrix as well as viscoelasticity. Matrix re-modeling is an example of a cata-bolic/anabolic cycle: Proteolytic
enzymes stimulated by tissue dam-age or inflammatory mediators are counteracted by antiproteases acti-vated by substances such as TGF-β.12 To date, these effects had been not-ed only in specialized connective tissue. The possibility that they will also be found in loose connective tissue suggests an overall plasticity reflecting an individual’s overall movement patterns and would also explain the effect of local inflamma-tory foci on the entire body, known empirically to practitioners of bio-logical medicine. Oschman also ex-amines this phenomenon in an arti-cle reviewing the role of free electrons and their antioxidant ac-tivity.13
In conclusion, movement of the ma-trix plays an important role in its remodeling and regeneration. We would do well to include stretching or even aerobic exercise as part of our patients’ treatment.14 The need is especially great in cases of tissue damage that require remodeling, as in fractures, osteoporosis, and even tendon injury.
Supportive bioregulation
As mentioned above, matrix remod-eling is a complex process relying on multiple factors: the immune sys-tem for controlled inflammation and repair, the action of amino acid-de-pendent proteases and metallopro-teinases, normal cortisol diurnal
rhythm, and normal angiogenic bal-ance. The three pillars of antihomo-toxic therapy (detoxification and drainage, immunomodulation, and organ regulation) are essential to en-sure matrix health.It can be postulated that many envi-ronmental toxins carry electrical or chemical charges that may disrupt subtle piezoelectric signals and af-fect transcription of mediators, thus affecting plasticity. The example of the zebra fish tail, which regener-ates completely after being severed, shows that adult zebra fish have the capacity to regenerate the caudal fin, a process that is inhibited by expo-sure to the ubiquitous environmen-tal contaminant 2,3,7,8-tetrachloro-dibenzo-p-dioxin (TCDD). Fin re ge neration is a complex process re-quiring precise regulation of several processes including wound healing, ECM production, revascularization, innervation, and bone formation. TCDD, a persistent organic pesti-cide, directly inhibits this process.15
The practice of advanced supportive detoxification with subsequent drainage is thus recommended for matrix health. Antihomotoxic medi-cine combined with proper nutrition can support this process. Medica-tions such as Thyreoidea composi-tum and Pulsatilla compositum are especially suitable for supporting the matrix biorhythm. Immune modulation that down-regulates in-flammatory mediators and secretion
Microscopic view of the extracellular matrix

) 15
Journal of Biomedical Therapy 2008)Vol.2,No.2
) Re f r e s h Yo u r H o m o t ox i c o l o g y
of TGF-β (part of the working mechanism of Traumeel) is also of benefit. These interventions support matrix remodeling and form the backbone of treatment of many chronic diseases. Together with ad-equate movement and nutrition and restoration of sleep/wake cycles, they may ensure normal matrix plas-ticity and restore anabolic/catabolic cycles.|
References
1. Abraham LC, Dice JF, Lee K, Kaplan DL. Phagocytosis and remodeling of collagen matrices. Exp Cell Res 2007;313(5):1045-1055.
2. Langevin HM. Connective tissue: a body-wide signaling network? Med Hypotheses 2006;66(6):1074-1077.
3. Langevin HM, Yandow JA. Relationship of acupuncture points and meridians to connec-tive tissue planes. Anat Rec 2002;269(6):257-265.
4. Swartz MA, Tschumperlin DJ, Kamm RD, Drazen JM. Mechanical stress is communi-cated between different cell types to elicit matrix remodeling. Proc Natl Acad Sci U S A 2001;98(11):6180-6185.
5. Szent-Györgyi A. The study of energy-levels in biochemistry. Nature 1941;148:157-159.
6. Vasishta VG; Kumar RV; Pinto LJ. Rotational field quantum magnetic resonance (RFQMR) in treatment of osteoarthritis of the knee joint. Ind J Aerospace Med 2004;48(2):1-7.
7. Gierse H, Breul R, Faensen M, Markoll R. Pulsed Signal Therapy (PST) stimulates mi-tosis of human chondrocytes in culture. In: Proceedings of the Tenth International Conference on Biomedical Engineering. Singapore: Humani-tas Press, 2000:473-474.
8. Langevin HM, Cornbrooks CJ, Taatjes DJ. Fi-broblasts form a body-wide cellular network. Histochem Cell Biol 2004;122(1):7-15.
9. Zeichen J, van Griensven M, Bosch U. The proliferative response of isolated human ten-don fibroblasts to cyclic biaxial mechanical strain. Am J Sports Med 2000;28(6):888-892.
10. Timmons JA, Jansson E, Fischer H, et al. Modulation of extracellular matrix genes re-flects the magnitude of physiological adapta-tion to aerobic exercise training in humans. BMC Biol 2005;3:19.
11. Madhavan S, Anghelina M, Rath-Deschner B, et al. Biomechanical signals exert sus-tained attenuation of proinflammatory gene induction in articular chondrocytes. Osteoar-thritis Cartilage 2006;14(10):1023-1032.
12. Holmbeck K, Szabova L. Aspects of extra-cellular matrix remodeling in development and disease. Birth Defects Res C Embryo Today 2006;78(1):11-23.
13. Oschman JL. Perspective: Assume a spheri-cal cow: The role of free or mobile elec-trons in bodywork, energetic and movement therapies. J Bodywork Movement Ther 2008; 12:40-57.
14. Carmeli E, Moas M, Lennon S, Powers SK. High intensity exercise increases expression of matrix metalloproteinases in fast skeletal mus-cle fibres. Exp Physiol 2005;90(4):613-619.
15. Andreasen EA, Mathew LK, Tanguay RL. Regenerative growth is impacted by TCDD: gene expression analysis reveals extracellular matrix modulation. Toxicol Sci 2006;92(1):254-269.
Structure of the extracellular matrix
Phot
o by
Wbe
nsm
ith; l
icen
sed
unde
r the
Cre
ativ
e Co
mm
ons
Attr
ibut
ion
3.0
Unp
orte
d (h
ttp:
//cr
eativ
ecom
mon
s.org
/lic
ense
s/by
/3.0
/), h
ttp:
//co
mm
ons.w
ikim
edia
.org
/wik
i/Im
age:
WVS
OM
_Su
bman
dibu
lar_
Gla
nd.JP
G

The lovely seaside resort of Ost-end is tailor-made for such
gatherings. The Kursaal conference center, where the lectures were held, is located right on the beach, mid-way along the broad promenade that stretches for several kilometers in either direction – an ideal site for walking, jogging, cycling, or roller-blading. The conference also coin-cided with a four-day gathering of sailing ships from all over Europe.
A long tradition
Belgium has a long homeopathic tradition and has hosted no less than five LMHI (“Liga”) conferences in the past. The 2008 event, organized to celebrate the 20th anniversary of
the Unio Homoeopathica Belgica (the Belgian professional organiza-tion for medical homeopathy), was truly international in content and at-tendance. The conference aimed to give an overview of effective ho-meopathic methodologies and strat-egies that have stood the test of time. Well-known specialists (in-cluding university professors) gave presentations on provings, clinical cases, clinical studies, and pharma-co-epidemiological studies. There were always five or six different con-current sessions to choose from, forcing the delegates to make some difficult choices. Feedback reporting
sessions at the end of each day pro-vided a useful overview of the prog-ress of the conference.
Opening ceremony
Liga president Dr. Ulrich Fischer gave the opening remarks, followed by a moving tribute by David Owen to the many great British homeo-paths and administrators who died in a plane crash in 1972 on the way to the last LMHI conference held in Belgium. Jacques Imberechts inau-gurated a commemorative plaque to George Jahr, the great Belgian ho-meopath and student of Hahne-mann. Ton Nicolai, President of the European Committee of Homeopa-thy, then awarded the “Globular Politics Award” to Michel Van Was-senhoven, the Chairperson for the 63rd congress. This is given to “phy-sicians who, in addition to their day-to-day work as a homeopathic doctor, have been instrumental in the social-political area and apply the homeopathic principles in all areas of their lives.”
) A r o u n d t h e G l o b e
) 16
From May 20-24, 2008, some 800 delegates met in
Ostend, Belgium, to participate in the 63rd conference
of the Liga Medicorum Homeopathica Internationalis
(LMHI). The overall theme of this years’ conference was
“Evidence-based homeopathy – more than results of
double-blind studies.”
Queen Paola of Belgium and her physician, Dr. Maurice Jenaer (to her left), surrounded by participants at the Liga congress.
Evidence-Based Homeopathy More Than Results of Double-Blind Studies! 63rd Congress of the Liga Medicorum Homeopathica Internationalis By Peter Rae Smith, MD

) A r o u n d t h e G l o b e
To the surprise and delight of the participants, Queen Paola of Bel-gium paid an unannounced visit to the conference, sitting in the audi-ence and listening intently to an in-teresting presentation by her ho-meopathic physician, Dr. Maurice Jenaer, on microimmunotherapy. A report of her visit aired on local television that evening. What a won-derful show of support for home-opathy!A variety of intriguing workshops dealt with different clinical methods such as the Masi method, Sankaran’s “Bombay method,” the Vithoulkas method, etc., while others looked at actual provings of a broad range of new (and old) substances. Jan Schol-ten led a number of sessions on his work with the Lanthanide remedies. The provings of this series of 15 “rare earth” elements appear to show affinity for the immune system.
Dr. Ulrike Keim’s satellite sympo-sium, “Is there a synergy between classical homeopathy and homeo-pathic combination preparations?” was well attended. Dr. Keim, known to BT readers as a specialist on met-abolic syndrome (see BT issue 1/2008), skillfully interwove the principles of classical homeopathy, such as miasmatic theory, with the practical applications of antihomo-toxic combination medicines.Dr. Robbert van Haselen, Head of Research at Biologische Heilmittel Heel GmbH, Baden-Baden, gave an interesting talk entitled “Detoxifica-tion and drainage – historical per-spectives and the current scientific state of the art,” which was well re-ceived by the audience. Although the Liga is predominantly a classical homeopathic organiza-tion, presentations dealing with ho-motoxicology were well received by the delegates. The next congress will be held in Warsaw, Poland, in Sep-tember 2009.|
) 17
Journal of Biomedical Therapy 2008)Vol.2,No.2
This year’s Liga congress took place at the Kursaal conference center in Ostend, Belgium.
Dr. Michel Van Wassenhoven, chairman of the 63rd Liga congress, received the “Globular Politics Award.”
Dr. Ulrike Keim gave a satellite symposium on the synergy between classical homeopathy and homotoxicology.
Some highlights of the conference
Among the many highlights of this conference, here are a few of special interest: The first plenary session, on the “Politics, History and Econom-ics of Homeopathy,” included Ton Nicolai’s talk on the current status of complementary and alternative medicine (CAM) in the European healthcare system and Christian Boiron’s “Homeopathy is a lan-guage.” In another plenary session on “Re-search – from proving to double-blind,” Prof. Claudia Witt presented an important paper on the treatment of atopic eczema in children. Dr. Witt is the first person to hold the Chair for Research in Complemen-tary/Alternative Medicine, recently endowed by the Karl and Veronica Carstens Foundation, at the Charité University Medical Center in Ber-lin.

) 18
Journal of Biomedical Therapy 2008)Vol.2,No.2
) M a r k e t i n g Yo u r P r a c t i c e
Getting Organized Professional file management and returning phone calls By Marc Deschler Marketing specialist
Learn to manage files proactively
At some point, all of us have made very quick decisions about questions with significant financial impact, such as buying a car or hiring staff. On the other hand, we often put off making much less important deci-sions for days or even weeks, and the stack of unanswered mail keeps on growing. What things do you leave lying around to deal with later – a whole newspaper with a single interesting article in it? A letter from a patient that you want to discuss with your team?These steps will help you get the problem under control:
1. Confront your procrastination consciously and note what types of things you tend to leave for later.
2. Set a time to tackle your entire “to do” pile and don’t stop until you have made all necessary de-cisions.
In this issue, we’ll deal with two topics: how to use
professional file management to aid in efficient decision-
making in your practice and how to deal with constant,
annoying phone interruptions during office hours.
Do not allow yourself to be interrupted by patient phone calls during an appointment. Patients deserve your undivided attention, whether in person or on the phone.
© 2
008
Blen
d Im
ages

) 19
Journal of Biomedical Therapy 2008)Vol.2,No.2
) M a r k e t i n g Yo u r P r a c t i c e
A professional filing system will help you in your daily decision-making process.
3. On each piece of mail, note what action it requires: Do you need to make an appointment, place an order, discuss it in a team meeting, file it for future refer-ence?
4. Starting right now, make all such decisions immediately.
Organized decision-making requires an appropriate filing system. Estab-lish folders for interesting topics you want to be sure not to forget, such as:• itemsforyournextteammeeting
(for example, discuss this col-umn!)
• taxtipstobringupatyournextmeeting with your tax advisor
• patients’ complaints that youneed to address
Set deadlines for dealing with the contents of these folders so nothing gets forgotten.Of course there are some decisions that cannot be made on the spot. For example, you receive informa-tion about some very interesting new electroacupuncture technology, but there’s no place for it in your in-vestment plan at the moment. Make a habit of saving such materials in a file cabinet that is located as far from your desk as possible and that only you use, so simply filing or retriev-
ing the information will take enough time to allow you to think about your indecision. If you then go through the file at regular intervals, you’ll find that most of these materi-als can simply be thrown out.
I’ll call you back!
Many practitioners accept calls from patients even during office visits. This practice has at least three dis-tinct disadvantages:
1. You may need to interrupt the patient you’re with in the middle of a very personal conversation.
2. The patient you’re with may overhear confidential informa-tion about the patient on the phone.
3. Your work flow is disrupted.
As a general rule, do not allow your-self to be interrupted by patient phone calls during office hours. This is especially important during ap-pointments because an interrupted conversation is much less satisfying to the patient than even a brief con-sultation in which he or she can count on your undivided attention. Furthermore, privacy of information is very high on most patients’ prior-ity list, so it should be preserved at all costs.
The solution? Institute an efficient system for returning calls. Your of-fice staff notes all incoming calls and pulls those patients’ charts so they are immediately available when you have fifteen minutes free to return calls. If you don’t have to search for missing information, you’ll spend less of your precious time on the phone. Another plus: You get to de-cide whom you talk to, what you talk about, and when. Here are some general rules:• To avoid scheduling conflicts,
make a habit of returning calls at certain set times. Note these times in your daily calendar.
• Make sure your employees tellpatients when your call-back time is so they will be available when you call.
• Your office staff shouldmake alist that includes each caller’s name and phone number and the time and subject of the call.
• Ifnoone is available toanswerthe phone during office hours, record an appropriate message on your answering machine.
If you follow these guidelines, you will always be able to give each patient the attention they de-serve, whether in person or on the phone. |

Sulfur is a non-metal, lemon yel-low in color, with atomic num-
ber 16 in the periodic table of the chemical elements. Its symbol is S and it is situated next to phosphorus (P, atomic number 15) to its left and chlorine (Cl, atomic number 17) to its right. The element immediately above it is oxygen (O, atomic num-ber 8) and the element immediately below it is selenium (Se, atomic number 34). It is characterized by high electro-negativity and consequently gains electrons more easily than it loses them. Its oxides are acidic and tend to form anions and oxyanions in aqueous solution. Solutions in water are acidic (pK
a1 = 7.00).
The essential amino acid methion-ine, which is apolar and hydropho-bic, contains a sulfur atom in its side chain. It is converted to homo-
cysteine and combines with the nonessential hydrophilic amino acid serine to form cysteine, a special nonessential amino acid. The side chain of cysteine contains a sulfhy-dryl (-SH) group, also known as a thiol group, which can undergo oxi-dation to form a covalent disulfide bond (-S-S-) with a second cysteine from the same or a different poly-peptide chain.The disulfide bonds form in the lu-men of the rough endoplasmic re-ticulum (RER) of the cell in which oxidizing conditions predominate, unlike in the cytosol where the pre-vailing reducing conditions main-tain cysteine residues in the reduced state (-SH). Disulfide bonds (S-S) are essentially found only in secre-tory proteins and in the exoplasmic domains of membrane proteins. The RER is also the site of synthesis of
proteins that subsequently go on to form part of various cell membrane receptors.The efficient formation of disulfide bonds in the lumen of the RER de-pends on the enzyme protein disul-fide isomerase (PDI). This enzyme catalyzes the formation of disulfide bonds, which catalyze the protein folding of many proteins. In this process, PDI catalyzes the cleavage of some disulfide bonds and the for-mation of others, which implies an interchange between pairs of disul-fide bonds in the polypeptide chain. PDI is found in all eukaryotic cells, particularly in organs such as the liver and pancreas.Glutathione and the enzyme gluta-thione reductase are other enzymes involved in the formation of the ap-propriate disulfide bonds in many proteins and polypeptide hormones. Similarly, they have been shown to be involved in the metabolism of xe-nobiotics. Thus the disulfide bonds of cysteine contribute to the forma-tion of the three-dimensional struc-ture of the various protein chains. The sulfate present in urine thus comes entirely from oxidation of L-cysteine. The following list shows where sul-fur is found in bodily metabolism:• inthestructureoftheamino
acids methionine, cysteine, homocysteine, and taurine
• inthestructureofproteins
) N e w P e r s p e c t i v e s
Sulfur in Health and Disease A Hypothesis on Sulfur Intoxication By Edgar Estrada Serrato, MD Orthopedist – Traumatologist Biological Medicine
) 20
Journal of Biomedical Therapy 2008)Vol.2,No.2
Since antiquity, sulfur has been used as a homeopathic
medicine in various conditions. Its use has been empirical
in nature, it being given in accordance with its various
homeopathic effects when administered to sick patients.
Advances in the study of basic sciences now enable us to
understand many of these empirical applications, giving
them new-found scientific validity. Sulfur plays an active
role in numerous metabolic processes in the healthy
human body.

) 21
• invariousrolesintheimmunesystem (immunoglobulins, cytokines)
• inadhesionmolecules (cellular = CAM and intercellular = ICAM)
• inmembranereceptors, such as insulin
• inleukotrienes,suchasLTD4
and LTE4
• inthestructureofgrowthhormone, calcitonin, dehydro-epiandrosterone, insulin, pro lac-tin, somatomedin, somatostatin, synthesis of T
3 and T
4
• inthepeptidesactivin,inhibins,atrial natriuretic peptide, brain natriuretic peptide, C peptide, relaxin, arginine-vasopressin, oxytocin
• epidermalgrowthfactor,nervegrowth factor, platelet-derived growth factor, erythropoietin
• leptin,cholecystokinin• inthestructureofcollagen
fibers, desmosine, elastin, fibrillin, fibronectin, integrin, laminin, osteonectin, keratin
• inthestructureofarticularcartilage and glycosaminogly-cans, chondroitin 4-sulfate and 6-sulfate, keratan sulfate I and II, heparin, heparan sulfate, dermatan sulfate
• constituentofthestructureofthe vascular wall, endothelins
• inthecoagulationcascade,structure of fibrinogen
• asacatalystintherespiratorychain of the citric acid cycle
• incellularapoptosis(caspaseenzymes)
• S-adenosylmethionine,synthesisof epinephrine, creatinine, melatonin
• hepaticmetabolismofcyto-chromes and action on xeno-biotics
• ingastricfluidandpancreaticfluid
• vitamins,suchasthiamine,biotin
• Shigellatoxin,diphtheriatoxin,immunotoxin
• inthepharmaceuticalandfoodindustry and in agriculture
The sources of the sulfur entering the body are diverse, and the ab-sorption occurs via a number of car-riers, including food and the envi-ronment. Indirectly, we ingest sulfur in the form of toxic by-products of fuels derived from coal and petro-leum, which on combustion produce sulfur dioxide. Direct ingestion of sulfur occurs primarily in our daily diet with the consumption of foods rich in the sulfites used in the food industry as preservatives and color-ing agents to improve shelf life and color fixation, or with the ingestion of refined sugar, which is found in a high percentage of the food and drink that we consume each day, or with foods contaminated with pesti-cides.The principles of Rudolf Arndt and Hugo Schulz, which demonstrate the linear pharmacological relation between dose and effect, give rise to
the basic biological rule which states that the physiological action of a cell increases or decreases in relation to the intensity of the stimulus: Weak stimuli stimulate the life func-tions, moderately strong stimuli ac-celerate them, strong stimuli act as inhibitors, and the strongest stimuli suspend the life functions. The high consumption of sulfur en-tering the body is probably trans-formed into an intense stimulus that displaces the equilibrium of the ma-trix and the membrane receptors, a phenomenon leading to modifica-tions in the network of information received and transported through the matrix in the intranuclear, intra-cytoplasmic, and extracellular spac-es. A cascade effect then ensues that leads to a change in biochemical, immunological, and hormonal re-sponses. This also destabilizes the three-dimensional structure of pro-teins, which, as we have already seen, need the presence of the disul-fide bonds to maintain their stereo-chemical presentation and recogni-tion at the cell membrane. Similarly, changes are produced in the assembly of collagen and elastin fibers. Destabilization of the proteo- and aminoglycans that form the hy-drated fibrous framework for the extracellular matrix results in com-petition between the H+ ions of the weak acid of H
2O and the hydrogen
ions of the strong acids SO42- of sul-
furic acid H2SO
4 and HPO
42- of
Journal of Biomedical Therapy 2008)Vol.2,No.2
) N e w P e r s p e c t i v e s
Sulfur, in its native form, is a yellow crystalline substance.

phosphoric acid H3PO
4. Proteogly-
cans and aminoglycans are substanc-es that readily undergo electrolytic exchange. Their alteration destroys their capacity to retain water in the cartilage and extracellular matrix, changing their state of fluidity to a state of desiccation or gel formation; the end result of this alteration is a loss of the ability of the body to ex-change information between differ-ent compartments, leading to loss of the state of systemic equilibrium. These alterations predispose the pa-tient to chronic conditions such as diabetes, rheumatic disease, osteo-porosis, and arthritis.What happens in this information exchange? We do not know exactly, but can postulate one of the follow-ing:• AchangeinbodypHaltersthe
behavior of the disulfide bonds, making them more rigid, the re-sult being that the protein chain loses its capacity to adjust to the membrane receptor.
• Anincreaseinthesebondscauseschanges in the three-dimensional structure of the protein chain.
• A loss of the capacity to formdisulfide bonds causes the pro-tein chains to break.
• Alossofcohesivestrengthofthedisulfide bonds makes them cleave easily.
We do not know exactly how this destructive process occurs, but we are familiar with the catastrophic ef-fect of sulfur consumption on the body. Within a few years, research will surely reveal to us in detail how the destructive effect of excessive in-take of sulfur on bodily metabolism occurs.
Contrast this with the pharmaco-logical viewpoint and therapeutic indication of allopathic medicine, in which the damage caused by an ex-cess of sulfur is treated with sulfur-based drugs that the patient takes in high doses, causing a high degree of intoxication and consequent wors-ening of the disease. Although there may be a relative improvement due to an initial mechanism, what is seen long-term is a worsening of symp-toms and a chronification of the ini-tial disease process, each time neces-sitating more combinations of medicines. We can take as an exam-ple the profile and timescale of a chronic condition such as diabetes. For chronic diabetic illness, treat-ment is commenced with sulfonyl-ureas, which are briefly effective. However, in time the body ceases to respond to these drugs, making it necessary to add another oral antidi-abetic such as metformin or rosigli-tazone, with the patient ultimately becoming dependent on insulin in order to manage symptoms and without this curing the disease. We return then to the patient as a chron-ic consumer of pharmacological substances that provide no cure but continually exacerbate the disease course and the permanent sulfur intoxication. |
References
1. Cooper GM, Hausman RE. La Célula. 4th ed. Madrid, Spain: Marbán; 2008.
2. Esteller M. Epigenetics in cancer. N Engl J Med 2008;358(11):1148-1159.
3. Etezad-Razavi M, Mahmoudi M, Hefazi M, Balali-Mood M. Delayed ocular complica-tions of mustard gas poisoning and the re-lationship with respiratory and cutaneous complications. Clin Experiment Ophthalmol 2006;34(4):342-346.
4. Fessenden R, Fessenden J. Química Orgánica. 2nd ed. Mexico City, Mexico: Grupo Edito-rial Iberoamericana; 1984.
5. Foye WO. Principios de Química farmacéutica. Barcelona, Spain: Reverté; 1984.
6. Ganong WF. Fisiología médica. 19th ed. Mexi-co City, Mexico: Manual Moderno; 2004.
7. Goldsby RA, Kindt TJ, Osborne BA, Kuby J. Inmunología. 5th ed. McGraw Hill; 2004.
8. Lodish H, Berk A, Matsudaira P, et al. Biolo-gia Celular Y Molecular. 5th ed. México City, Mexico: Editorial Medica Panamericana; 2005.
9. Meyers F, Jawetz E, Goldfien A. Farmacología Clínica. 3rd ed. Mexico City, Mexico: Manual Moderno; 1977.
10. Murray RK, Granner DK, Mayes PA, Rodwell VW. Bioquímica de Harper. 15th ed. Mexico City, Mexico: Manual Moderno; 2001.
11. Nussey SS, Whitehead SA. Endocrinology: an integrated approach. Oxford, UK: BIOS Scien-tific Publishers Ltd; 2001.
12. Reckeweg H-H. Materia Medica – Homoeo-pathia Antihomotoxica. 4th ed. Baden-Baden, Germany: Aurelia; 2002.
13. Schmid F, Rimpler M, Wemmer U. Medicina antihomotóxica. Vol. I – Principios – clinica – práctica. Baden-Baden, Germany: Aurelia; 2004:51-88.
14. Scientific opinion of the Panel on Food Ad-ditives, Flavourings, Processing Aids and Food Contact Materials (AFC) on a request from the Commission on the results of the study by McCann et al. (2007) on the ef-fect of some colours and sodium benzoate on children’s behaviour. The EFSA Journal 2008;660:1-54.
15. Vannier L. Compendio de Materia Médica Ho-meopática. 4th ed. México City, Mexico: Por-rúa, 1998.
16. World Cancer Research Fund/American In-stitute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. Washington, DC: AICR; 2007:35-37.
) 22
Journal of Biomedical Therapy 2008)Vol.2,No.2
) N e w P e r s p e c t i v e s

For MDs and licensed healthcare practitioners only
Free of charge
www.iah-online.com
1 Access the IAH website at www.iah-online.com. Select your language.
2 Click on Login and register.
3 Go to Education Program.
4 Click on The IAH abbreviated course.
5 When you have finished the course, click on Examination. After completing it successfully, you will receive your certificate by mail.
An e-learning course leading to
certification in homotoxicology
from the International Academy for
Homotoxicology in just 40 hours.
IAH Abbreviated Course

Journal of Biomedical Therapy 2008)Vol.2,No.2
) F r o m t h e P r a c t i c e
) 24
ness) that varied in frequency, some-times appearing daily, sometimes with symptom-free intervals of up to a month. Several months ago, however, the pain became more pro-nounced and the pain-free intervals less frequent. Because the pain pre-vented her from sleeping, she also suffered from severe fatigue and ir-ritation.
Examination
An initial examination revealed: • decreasedrangeofmotioninthe
cervical spine• swellingand inflammation in the
cervical and surrounding muscula-ture
• tenderness and pain around thecervical facet joints
• activemyofascialtriggerpoints• cervicogenicheadacheUpper cervical evaluation revealed an upper neck injury that had not been addressed by previous practi-tioners. Jackson’s Compression Test and the Valsalva maneuver were positive. An MRI revealed a small hernia between C5 and C6, poste-riolateral to right. X-rays showed early-stage degeneration of the facet joints.
Treatment regimen
Treatment required a combination of chiropractic (to restore normal joint mobility and range of motion) and physical therapy (to restore muscle flexibility and movement). In addition, several antihomotoxic medications were administered: • SpascupreelandZeelwereinject-
ed twice weekly into trigger points along the lumbar vertebrae to im-prove paraspinal muscular spasms and myofascial trigger points.
• Gelsemium-HomaccordandLym-phomyosot were injected twice weekly into the painful area to re-lieve cervical pain and inflamma-tion and cervicogenic headache.
• OralGelsemium-Homaccordwasalso prescribed (10-15 drops 3-4 times per day).
The patient initially reported an in-crease in pain (possibly due to a re-action phase) but then reported gradual improvement in the pain and other symptoms from the 2nd to 3rd week. With less pain and irrita-tion, she was able to relax, and her sleep pattern improved. Upon con-clusion of treatment, she felt ener-getic, was no longer experiencing mood swings, and reported excel-lent concentration at work. Her quality of life has greatly improved, as has her family life.|
This patient, referred to me by a local family physician, present-
ed with secondary whiplash symp-toms presumably due to an automo-bile accident several years ago. After the accident, treatment with NSAIDs and physical therapy adequately re-lieved the acute pain of the patient’s whiplash, but she remained con-stantly aware of discomfort in her neck. As time passed, she continued to take medication for this chronic pain, but her symptoms gradually worsened and eventually became unmanageable.
History
Fifteen years ago, this female patient, now 48 years old, had been involved in an auto accident without wearing her seat belt and suffered whiplash and minor cuts and bruises as a re-sult. After the accident, she com-plained of severe headache and nau-sea and was hospitalized for two days. She was given a neck brace to wear for a minimum of 4-6 weeks and medication to address possible inflammation.She was left with chronic symptoms (pain in her neck, shoulder, and arms; stiffness; headaches; restless-
Whiplash – Acute Inflammation Becomes Chronic By Dennis van Aswegen, DC
Whiplash is a term used to describe an injury to the soft
tissues – the muscles, ligaments, and nerves – of the neck.
Many people fail to relate their symptoms to a car
accident because the symptoms often begin days, months,
or even years after the accident.

) 25
Journal of Biomedical Therapy 2008)Vol.2,No.2
Treatment regimen
Treatment required a combination of chiropractic and physical therapy. In addition, several antihomotoxic medications were prescribed: • Spascupreel was injected twice
weekly into trigger points along the lumbar vertebrae.
• AmixtureofZeelandDiscuscom-positum was injected twice weekly into the paravertebral muscles to relieve chronic inflammation and degeneration of the facet joints and intervertebral disc.
• Colocynthis-Homaccord (whichcould also be mixed with Zeel and Discus compositum) was injected twice weekly into sites along the paraspinal muscles to relieve symptoms of sciatica and neural-gia.
• Traumeel tablets were prescribedfor general inflammation and pain (1 tablet 3 times per day for six weeks).
The patient reported a 60 percent improvement in both pain and range of motion after four weeks of treat-ment and an additional ten percent improvement after six weeks. He has been able to resume his day-to-day activities and looks forward to tak-ing up some of his previous sporting and outdoor pursuits again in the near future.|
) F r o m t h e P r a c t i c e
chanical movements triggered pain-ful symptoms. The patient described the pain as burning, sharp, shooting, or “pins and needles.” It intensified with long periods of activity such as walking or cycling. Additional symptoms included pain-related insomnia and a painful sensation when bearing down during bowel movements.
Examination
On initial physical examination, the following orthopedic tests were po-si tive, suggesting an L4/5 disc lesion:• decreasedrangeofmotioninac-
tive flexion/extension and rota-tion
• straightlegraising(especiallytheright leg, above 70 degrees)
• Bragard’stest• ValsalvamaneuverX-ray and MRI studies of the lum-bar spine revealed:• disc herniation at the levels of L4
and L5 (more pronounced at the L5 level and on the right, but with minimal pressure on the thecal sac)
• early facet degeneration fromL2to L5, both left and right
• activemyofascialtriggerpointsinthe lumbar paraspinal and gluteal muscles
• flatteningofthelumbarlordosis• irritationandinflammationofthe
lumbar facet joints
The patient, who suffered from longstanding back pain and
had consulted numerous specialists, had decided to endure his condition with the help of medication for as long as possible before resorting to surgical intervention. As a result, he became a walking illustration of the well-known statistic: Back pain is second only to the common cold as a cause of lost work time and results in more lost productivity than any other medical condition. His condi-tion was interfering not only with his work but also with his general day-to-day activities and family life and even forced him to give up most of his sporting/outdoor interests.
History
The patient is a 43-year-old male with a long history of lower back pain, which began at a very young age after various childhood mis-haps and enthusiastic participation in contact sports. Treatment with NSAIDs was initially effective in combination with physical therapy, but as the years passed, the pain be-gan to move into his legs, although it rarely radiated below the knees. As a result, treatment became less effec-tive, and the symptom-free intervals between bouts of pain/restricted movement became shorter. At a later stage, even slight abnormal biome-
Lumbosacral Pain Syndrome By Dennis van Aswegen, DC
“Treatment for lower back pain is not a single therapy but
rather an integration of several therapies.”
©
200
8 Ju
pite
rImag
es C
orpo
ratio
n

) 26
Journal of Biomedical Therapy 2008)Vol.2,No.2
) M a k i n g o f …
The manufacturing of suis-organ preparations is strictly regulat-
ed to ensure their safety. Before pro-duction of the mother tincture be-gins, the identity of the raw material of animal origin is first confirmed by a veterinarian. A number of tests are then performed, including a his-tological examination. Additional tests for zoonoses are conducted in specialized laboratories to ensure that the animal tissues contain no pathogens that infect humans. All of the test results are documented and archived and must be available be-fore the animal material is processed further.
Homeopathic extracts
Production of homeopathic extracts from freshly slaughtered animals or their organs follows manufacturing methods 42a or 42b of the Ger-man Homeopathic Pharmacopoeia (HAB).1 In accordance with the 2007 HAB, one part of the animal ingredient is diluted with nine parts of 85 percent glycerol (Method 42a). The initial mixture is allowed to stand for at least five days, after which the coarsest particles are fil-
tered out. The resulting filtrate is the mother tincture used in the produc-tion of further dilutions. Method 42b applies specifically to the production of injectable medica-tions (as defined in HAB 2007, Method 11) and eye drops (Method 15). The manufacturing process dif-fers from that described in Method 42b only in that one part of the finely ground raw material is first mixed with 2.1 parts of 85 percent glycerol and succussed; for injection purposes, the first decimal (D1) di-lution is then produced using three parts of this mother tincture and seven parts water, while the D2 di-lution uses one part D1 and nine parts water. In accordance with Method 42a, potentization stages up to and in-cluding D2 always involve a 1:10 mix with either 85 percent glycerol or 15 percent ethanol; beginning with D3, the carrier is 15 percent ethanol. The potentized suis-organ
Suis-Organ Products in Antihomotoxic Medicine Part 2: Production and Quality Control By Wilfried Stock, PhD
Suis-organ preparations, an important component of
antihomotoxic therapy, are administered especially to
patients with chronic diseases to stimulate and reactivate
the homologous human organs or tissues. Homeopathi-
cally prepared extracts of more than seventy different
organs are available for specific organ support.
“Isoelectric focusing,” a technique for separating different molecules according to electric charge differences, is used to confirm the identity of suis-organ mother tinctures. The photograph shows a flatbed system for horizontal applications with integrated cooling plate and an external power supply unit.

) M a k i n g o f …
) 27
extracts are then further processed into antihomotoxic medications in accordance with the relevant manu-facturing guideline of the HAB.
Quality assurance
In addition to the above-mentioned microscopic histological examina-tion of the animal raw material, ad-ditional analytical testing of finished mother tinctures takes place in Heel’s quality control lab. In particular, the identity of the mother tincture is confirmed through “isoelectric fo-cusing,” a specialized electrophore-sis technique applied in accordance with the European Pharmacopoeia.2 Isoelectric focusing makes it possible to identify the various components of a biological material as shown on an electropherogram. Com parison to previous production runs then ensures the uniformity of the current batch of mother tincture. Other physical characteristics (color, opalescence, relative density) of the mother tincture are also tested.
Viral and bacterial safety
The special conditions under which donor animals are raised (see Part 1: Breeding and Raising the Donor Pigs,“ BT 1/2008, pp. 24-25) and extensive testing of the animal tis-sues for zoonoses ensures that the quality of the suis-organ extracts meets modern standards of safety. The European Pharmacopoeia’s general monograph on homeopathic preparations requires that animal in-gredients be free of viral and bac-terial agents to avoid infecting patients. An assessment report, re-gularly updated, evaluates the viral safety of the hog tissue.
Because the animal tissues used in the manufacture of suis-organ medi-cations are derived exclusively from hogs, which have no known suscep-tibility to spongiform encephalopa-thy (BSE), there is no danger of transmitting the disease. Thus the suis-organ preparations manufac-tured and marketed by Heel meet all the requirements of the law and the pharmacopoeia with regard to bio-logical materials of this type.|
References
1. Homöopathisches Arzneibuch 2007. Stuttgart, Germany: Deutscher Apotheker Verlag, 2007.
2. European Pharmacopoeia. 6th ed. Strasbourg, France: Council of Europe, 2007.
A lab assistant positions a precast polyacrylamide gel on the cooling plate.
Electropherogram of splen suis mother tincture. Proteins appear as distinct, sharp zones. The resulting pattern is unique to a given substance, thus permitting unambiguous identification.

Hans-Heinrich Reckeweg Award 2009 Join in – get your experience rewarded
Outstanding scientific research deserves to be acknowledged, and rapid international distribution
of the results provides a useful service to both researchers and potential consumers. In the field of
homotoxicology, Biologische Heilmittel Heel GmbH offers such support in the form of the annual
Hans-Heinrich Reckeweg award.
The main award
valued at € 10,000, will be given for completed scientific work of fundamental theoretical and/
or practical significance in antihomotoxic medicine in the related fields of human and veterinary
medicine (no research involving animal testing).
The incentive award
valued at € 5,000, will be given for results arising from clinical, case based or fundamental research
in antihomotoxic medicine in the related fields of human and veterinary medicine that invite further
investigation (no research involving animal testing). The prize monies are intended to be invested in
ongoing research into the particular research subject.
The prize will be awarded for results arising from research carried out in a registered practice or
in a laboratory. In either case the results have to be new, not published before and convincing.
Homotoxicology is one of medicine‘s great success stories. Originally conceived as a model to explain
the outstanding efficacy of a distinct class of homeopathic medications, homotoxicology has grown
into a comprehensive theory of disease.
The deadline for submissions is May 31. An independent panel of reviewers will allocate the awards.
The review panel maintains the right to allocate either of the awards to any of the entries. The review
panel‘s decision is final.
Interested parties are welcome to ask for entry details and conditions:
Biologische Heilmittel Heel GmbH, Department of Research,76532 Baden-Baden, Germany
Phone +49 7221 501-227, Fax +49 7221 501-660, [email protected], www.heel.com