
Outcome of zirconia single crowns made by predoctoral ... · complications were chipping of...
6
CLINICAL SCIENCE Outcome of zirconia single crowns made by predoctoral dental students: A clinical retrospective study after 2 to 6 years of clinical service Ritva Näpänkangas, DDS, PhD, a Juha Pihlaja, DDS, b and Aune Raustia, DDS, PhD c Zirconia has been established as a reliable ceramic material for fixed prostheses in several follow-up studies. 1-11 The survival rate of zirconia has been shown to be similar to that of metal ceramics for both crowns 12 and partial fixed dental prostheses (FDPs). 13-18 Traditional metal ceramic res- torations are still the safest option in patients with bruxism, because studies have shown that the veneering porcelain of ceramic restora- tions has a higher rate of fracture than that of metal ceramic restorations. 19-21 Zirconia has better mechanical properties than other ceramics, including alumina, glass ceramics, and lithium disilicate. 22 Zirconia is biocompatible and esthetic, and can withstand both tensile and compressive stress. 22,23 The strength of zirconia allows its use in anterior, premolar, and molar areas. 6 Some studies have shown a higher risk of complications for ceramic crowns in the molar area than in anterior or premolar teeth, 24 but in other studies no difference was seen. 5-7 Compared with lithium disilicate, the bond between the resin cement and the zirconia may be weaker. 25 A phosphate monomer is beneficial in bonding. 26 The retention and resistance of zirconia crowns have to be ensured with adequate prep- aration of the abutment tooth. Another disadvantage of zirconia is a high prevalence of chipping fractures in the veneering porcelain, 20,21,27 even though the techniques and materials of veneers have been improved. 28-30 One option for restorations is to use monolithic a Senior Lecturer, Department of Prosthetic Dentistry and Stomatognathic Physiology, Institute of Dentistry, University of Oulu; and Medical Research Center, Oulu, Oulu University Hospital and University of Oulu, Finland. b Research Assistant, Department of Prosthetic Dentistry and Stomatognathic Physiology, Institute of Dentistry, University of Oulu; and Medical Research Center, Oulu, Oulu University Hospital and University of Oulu, Finland. c Professor, Department of Prosthetic Dentistry and Stomatognathic Physiology, Institute of Dentistry, University of Oulu; and Medical Research Center, Oulu, Oulu University Hospital and University of Oulu, Finland. ABSTRACT Statement of problem. Zirconia has established its role as a reliable ceramic material for fixed prostheses. Purpose. The purpose of this retrospective study was to evaluate the outcome of zirconia single crowns made by predoctoral students after 2 to 6 years of clinical service. Material and methods. A cohort of 88 patients treated with zirconia single crowns (mean 3 crowns per patient, range 1 to 12 crowns) from 2007 to 2010 by predoctoral dental students was identified. The patients were invited to attend a clinical examination. Results. Sixty-six participants (75%) took part in the clinical follow-up (30 women and 36 men; mean age 60.4 years, range 19 to 81 years). Altogether, 190 teeth with single crowns were examined, and the mean follow-up time was 3.88 years (1.85 to 6.04 years). The most common complications were chipping of veneering porcelain (4%) and loss of cementation (4%). The success rate of the zirconia single crowns after 2 to 6 years was 80% and the survival rate 89%. Conclusions. Zirconia crowns can be successfully used in predoctoral dental education. The success rate of zirconia single crowns after 2 to 6 years was 80% and the survival rate was 89%, in accordance with previous studies. (J Prosthet Dent 2015;113:289-294) THE JOURNAL OF PROSTHETIC DENTISTRY 289
Transcript of Outcome of zirconia single crowns made by predoctoral ... · complications were chipping of...

CLINICAL SCIENCE
aSenior LectuOulu UniversbResearch AOulu UniverscProfessor, DOulu Univers
THE JOURNA
Outcome of zirconia single crowns made by predoctoral dentalstudents: A clinical retrospective study after 2 to 6 years of
clinical service
Ritva Näpänkangas, DDS, PhD,a Juha Pihlaja, DDS,b and Aune Raustia, DDS, PhDcABSTRACTStatement of problem. Zirconia has established its role as a reliable ceramic material for fixedprostheses.
Purpose. The purpose of this retrospective study was to evaluate the outcome of zirconia singlecrowns made by predoctoral students after 2 to 6 years of clinical service.
Material and methods. A cohort of 88 patients treated with zirconia single crowns (mean 3 crownsper patient, range 1 to 12 crowns) from 2007 to 2010 by predoctoral dental students was identified.The patients were invited to attend a clinical examination.
Results. Sixty-six participants (75%) took part in the clinical follow-up (30 women and 36 men;mean age 60.4 years, range 19 to 81 years). Altogether, 190 teeth with single crowns wereexamined, and the mean follow-up time was 3.88 years (1.85 to 6.04 years). The most commoncomplications were chipping of veneering porcelain (4%) and loss of cementation (4%). Thesuccess rate of the zirconia single crowns after 2 to 6 years was 80% and the survival rate 89%.
Conclusions. Zirconia crowns can be successfully used in predoctoral dental education. The successrate of zirconia single crowns after 2 to 6 years was 80% and the survival rate was 89%, inaccordance with previous studies. (J Prosthet Dent 2015;113:289-294)
Zirconia has been establishedas a reliable ceramic materialfor fixed prostheses in severalfollow-up studies.1-11 Thesurvival rate of zirconia hasbeen shown to be similar tothat of metal ceramics for bothcrowns12 and partial fixeddental prostheses (FDPs).13-18
Traditional metal ceramic res-torations are still the safestoption in patients withbruxism, because studies haveshown that the veneeringporcelain of ceramic restora-tions has a higher rate offracture than that of metal
ceramic restorations.19-21Zirconia has better mechanical properties than otherceramics, including alumina, glass ceramics, and lithiumdisilicate.22 Zirconia is biocompatible and esthetic, andcan withstand both tensile and compressive stress.22,23
The strength of zirconia allows its use in anterior,premolar, and molar areas.6 Some studies have shown ahigher risk of complications for ceramic crowns inthe molar area than in anterior or premolar teeth,24 but inother studies no difference was seen.5-7 Compared with
rer, Department of Prosthetic Dentistry and Stomatognathic Physiology, Inity Hospital and University of Oulu, Finland.ssistant, Department of Prosthetic Dentistry and Stomatognathic Physiologity Hospital and University of Oulu, Finland.epartment of Prosthetic Dentistry and Stomatognathic Physiology, Instituteity Hospital and University of Oulu, Finland.
L OF PROSTHETIC DENTISTRY
lithium disilicate, the bond between the resin cement andthe zirconia may be weaker.25 A phosphate monomer isbeneficial in bonding.26 The retention and resistance ofzirconia crowns have to be ensured with adequate prep-aration of the abutment tooth. Another disadvantage ofzirconia is a high prevalence of chipping fractures in theveneering porcelain,20,21,27 even though the techniquesand materials of veneers have been improved.28-30
One option for restorations is to use monolithic
stitute of Dentistry, University of Oulu; and Medical Research Center, Oulu,
y, Institute of Dentistry, University of Oulu; and Medical Research Center, Oulu,
of Dentistry, University of Oulu; and Medical Research Center, Oulu,
289

Figure 1. Zirconia single crowns restoring maxillary incisors and canineteeth.
Clinical ImplicationsZirconia single crowns can be used with adequatesurvival and success in the predoctoral dentalstudent clinic.
290 Volume 113 Issue 4
anatomic-contour zirconia without veneering porcelain.31
A framework fracture is a less frequent complication inzirconia restorations.32,33
The marginal gap of zirconia restorations has beenshown to be equal to that of metal ceramics.34,35 Themarginal gap has varied amongdifferent zirconiamaterialsbut has always been clinically acceptable.36-39 Anotherissue concerning zirconia restorations is the wear of bothzirconia and the antagonist enamel. However, zirconiawith adequate surface finish (polishing, glazing) resultedin the least wear of the antagonist enamel among thevarious dental materials; a smooth surface of zirconia canbe obtained with adequate polishing.40
In predoctoral dental education, the techniques andmaterials need to be reliable, because teaching the basicprinciples of preparation and procedures of prosthetictreatment should be the focus. In addition to the strengthof zirconia, the willingness to use metal-free, moreesthetic, and less expensive material than metal ceramicsalso encourages its use in predoctoral dental educationalongside metal ceramics. The hypothesis of the studywas that zirconia is also suitable for fixed prostheses inpredoctoral dental education. The aim of the study was toevaluate the outcome of zirconia single crowns in a 4-year clinical retrospective follow-up study.
MATERIAL AND METHODS
The study protocol was approved by the Ethical Com-mittee of the Northern Ostrobothnia Hospital District(100/2013). A total of 88 patients were treated with 268zirconia single crowns (mean 2.9 crowns per patient,range 1 to 12 crowns) between 2007 and 2010 by pre-doctoral dental students (Fig. 1). All patients were invitedto a clinical examination, and 66 patients (75%) took partin the study. Nine patients did not attend and did notcontact us, 11 patients had moved away (not invited),and 1 patient had died.
Before prosthodontic treatment, the patients receivedperiodontal treatment, caries control, and endodontictreatment, as well as occlusal adjustment if needed. Allthe preparations were made in accordance with inter-national treatment guidelines.41 Composite resin (Z250;3M ESPE) was used for foundation restorations whenneeded, and a fiber post (RelyX Fiber Post; 3M ESPE) wasused in endodontically treated teeth. All the treatmentprocedures were performed under the supervision ofprosthodontists.
THE JOURNAL OF PROSTHETIC DENTISTRY
Before the definitive cementation of the zirconiasingle crowns, their esthetic appearance and occlusionwere evaluated. The clinical instructor evaluated the fit ofthe restoration, and the patients were asked whetherthey were satisfied with the color and esthetics. Therestorations were bonded with dual-polymerizing, self-adhesive universal resin cement (RelyX Unicem; 3MESPE), according to the manufacturer’s instructions.
The zirconia frameworks in the single crowns werefabricated from Zirkonzahn Zirconia (Zirkonzahn),NobelProcera Zirconia (Nobel Biocare), or Prettau Zir-conia (Zirkonzahn). With Zirkonzahn Zirconia and Pre-ttau Zirconia, the frameworks were fabricated by manualmilling and designed for uniform thickness of theveneering porcelain layer. The minimal thickness of theframework was 0.4 mm, and the veneering porcelain (GCInitial Zr; GC Europe) was layered on the frameworks.For NobelProcera Zirconia, the frameworks were fabri-cated with computer-aided design/computer-aidedmanufacture (CAD/CAM) and designed for uniformthickness of the veneering porcelain layer. The minimalthickness of the frameworks in the single crowns was 0.4mm in the anterior area and 0.7 mm in the posterior area.The veneering porcelain (VITA VM 9; VITA Zahnfabrik)was hand layered on the frameworks.
All the follow-up examinations were carried out bythe same prosthodontist (R.N.). The participants wereasked their opinions about esthetics, color match, con-tour, gloss, hypersensitivity to cold or heat, gingivalbleeding, pain related to the single crowns, and whetherthey noticed bruxism. At the clinical examination, theperiodontal condition (plaque accumulation/plaque indexand bleeding on probing/sulcus bleeding index accordingto Silness and Löe42and Mombelli et al43), the location ofthe crown margins related to the gingival margins, caries,or restorations in the crown margin, the presence ofendodontic treatment through the prosthetic crown, andthe status of the contralateral tooth were evaluated. Thedifference between the plaque accumulation and
Näpänkangas et al

Table 1. Indications for 204 single zirconia crowns
Indication n %
Large restoration 81 40
Poor esthetics 31 15
Unstable occlusion 26 13
Fractured restoration or tooth 22 11
Occlusal wear 13 6
Abutment tooth for PRDP 13 6
Old crown 12 6
Periodontal reasons 6 3
TOTAL 204 100
PRDP, partial removable dental prosthesis.
18 17
45
40
35
30
25
20
15
10
5
0
0
5
10
15
20
25
30
35
40
45
16 15 14 13 12 11 21 22 23 24 25 26 27 28
48 47 46 45 44 43 42 41 31 32 33 34 35 36 37 38
PonticsAbutments
PonticsAbutments
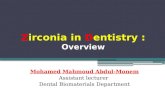
Figure 2. Distribution of single zirconia crowns in dentition.
April 2015 291
bleeding on probing in the abutment teeth and contra-lateral teeth were analyzed with the Fisher exact test(a=.05). Porcelain fractures were recorded and classifiedaccording to Anusavice.44 Any dental treatment per-formed at the Institute of Dentistry after the prosthetictreatment was determined from the patient records(Effica; Tieto).
The longevity of the single zirconia crowns wasmeasured from the day the crown was cemented to theday of a complication, or, if no complications occurred, tothe day of the clinical examination. A Kaplan-Meiersurvival analysis was performed on the basis of thesefacts and the survival percentage was counted at thepoint of 4 years because of the low number of singlecrowns after that time. A successful single crown wasdefined as a crown that had remained unchanged overthe observation period (according to Tan et al45). A sur-vived single crown was defined as a crown that was insitu at the examination visit, regardless of its rece-mentation or porcelain fractures (according to Tanet al45).
RESULTS
Altogether, 30 women and 36 men were examined. Meanage was 60.4 years (19 to 81 years). Mean follow-up was3.88 years (1.85 to 6.04 years). Altogether, 204 teeth wereprepared for crowns – Zirkonzahn 164 crowns (80%),Procera 21 crowns (21%), and Prettau 19 crowns (9%).The mean number of crowns was 2.9 crowns per patient(range 1 to 10 crowns).
The most common indication for a zirconia singlecrownwas a large existing restoration in the tooth (81/204,40%) (Table 1). Other common indications were pooresthetics (31/204, 15%) and unstable occlusion (26/204,13%). The distribution of zirconia single crowns is pre-sented in Figure 2. The opposing dentition was the pa-tient’s own teeth in 82% of restorations, a crown or partialFDP in 12%, a complete denture in 4%, and a partialremovable dental prosthesis in 2% of the restorations.
One participant had lost all 6 zirconia crowns becauseof loss of cementation (1 crown), because of root fracture
Näpänkangas et al
(2 crowns), and because of a change in the treatmentplan for the removable prosthesis (3 crowns). Oneparticipant lost 1 molar tooth with a crown because ofroot fracture, and thereafter 3 other adjacent teeth withcrowns were prepared for the abutment teeth of a partialfixed dental prosthesis. The number of individuals in theclinical examination remained at 64. In addition, 2 lostcrowns were attributed to cementation and 2 to peri-apical endodontic infections. The number of crowns inthe clinical follow-up remained 190.
Most of the participants were satisfied with the es-thetics (63/64 participants), color-match (61/64), contour(61/64), and gloss (64/64) of the zirconia single crowns.Three participants suffered from hypersensitivity to cold,and 3 of 64 participants noticed gingival bleeding. Oneparticipant experienced pain. Self-reported bruxism wasreported by 26 of 64 participants.
More plaque was seen in contralateral teeth than inteeth with zirconia crowns, but the difference was notstatistically significant (P=.376) (Table 2). Morebleeding on probing was seen in teeth with zirconiacrowns than in contralateral teeth (P=.012) (Table 3).
THE JOURNAL OF PROSTHETIC DENTISTRY

Table 3. Bleeding on probing (sulcus bleeding index) around abutmentteeth (n=190) and contralateral teeth
Bleeding on ProbingAbutmentTeeth (%)
ContralateralTeeth (%)
No bleeding when a periodontal probe is passedalong the gingival margin
49 39
Isolated bleeding when a periodontal probe ispassed along the gingival margin
40 60
Confluent bleeding when a periodontal probe ispassed along the gingival margin
11 1
P=.012; Fisher exact test.
Figure 3. Porcelain fracture in zirconia single crown for maxillary leftcanine (Grade 1 according to Anusavice43). Fracture did not affectfunction or esthetics and surface has been polished. Figure 4. Porcelain fracture in zirconia single crown for maxillary right
incisor (Grade 1 according to Anusavice43). Fracture did not affectfunction or esthetics and surface has been polished. Bleeding on prob-ing was seen in abutment tooth; location of crown margin wassubgingival.
Table 2. Plaque accumulation (Plaque index) in abutment teeth (n=190)and in contralateral teeth
Plaque IndexAbutmentTeeth (%)
ContralateralTeeth (%)
No detection of plaque 77 41
Plaque only recognized by running a probeacross the marginal surface of the crown
17 56
Plaque can be seen by the naked eye 6 3
P=.376; Fisher exact test.
292 Volume 113 Issue 4
The location of the crown margin was subgingival in43% of the single crown, marginal in 53%, andsupragingival in 4%.
Caries were not found and endodontic treatment wasnot performed through the prosthetic crown in any of theteeth with zirconia single crowns examined at follow-up.The most common complications were chipping of theveneering porcelain (4%) (Figs. 3, 4) and loss of cemen-tation (4%) (Table 4). According to Anusavice,44 3 por-celain fractures were grade 3 (severe chipping fracturesrequiring replacement of single crowns) and 6 porcelainfractures were grade 1 (fracture surfaces were polished;fractures did not affect function or esthetics). The successrate was 80%, and the survival rate was 89% after 4 years(Fig. 5).
DISCUSSION
The survival rate of zirconia single crowns made bypredoctoral dental students in the present study was89%, in accordance with previous clinical follow-upstudies, which found survival rates of 97.3% (5 years,ceramic restorations),5 98.1% (5 years),10 88.8% (5years),7 and 98.2% (3 years).9 The success rate (80%)here was lower than that reported earlier by Monacoet al10 (94.3% after 5 years). The limitation of the studywas that the zirconia crowns were performed bypredoctoral dental students and this may affect the sur-vival of the single crowns. Parafunctional habits andendodontically treated teeth pose a greater risk for fail-ures.5,10,20 Thus, complications may accumulate in the
THE JOURNAL OF PROSTHETIC DENTISTRY
same individuals and, in the case of complication in 1crown, the risk for a complication in another crown mayincrease in an individual with multiple crowns. Earlyrepairable chipping of veneering porcelain may increasethe risk for unrepairable porcelain damage later.13,14 Theindications for choosing a material between ceramics,metal ceramics, or high-gold alloys must be well indi-cated in individual situations.
Several attempts have been made to improve thefracture rate of veneering porcelain in zirconia restora-tions. Anatomically designed frameworks have beenshown to result in a lower rate of porcelain fractures.28,31
Guess et al29 showed in an in vitro study that anatomi-cally shaped monolithic lithium disilicate crowns (IPS e-max CAD) resulted in fatigue-resistant crowns comparedwith hand-layer, veneered zirconia crowns (IPS e-maxZir-CAD/Ceram). The tooth should be adequatelyreduced to provide sufficient thickness of the veneeringporcelain. Occlusion must be evaluated properly, becausethe number and distribution of occlusal contact pointshave been shown to significantly influence the stressesinduced by occlusal forces in ceramic restorations.19 Inaddition, parafunctional habits have to be taken intoconsideration in treatment planning.20
It has been shown that biofilm formation on varioustypes of dental ceramics differ significantly; in particular,
Näpänkangas et al

~~
~~Cu
mul
ativ
e Su
rviv
al (%
)
100
80
60
0
0 2 4Time (y)
Figure 5. Survival rate in 204 zirconia single crowns was 89% after 4years.
Table 4. Complications in 204 zirconia single crowns
Complication
ZirkonzahnZirconia
NobelProceraZirconia
PrettauZirconia Total
n % n % n % n %
No complication 138 84 17 82 18 95 173 85
Porcelain fracture 7 4 2 9 0 0 9 4
Loss of cementation 5 3 2 9 1 5 8 4
Loss of crown
loss of cementation 3 2 0 0 0 0 3 2
root fracture 3 2 0 0 0 0 3 2
periapical endodontic infections 2 1 0 0 0 0 2 1
change in treatment plan 6 4 0 0 0 0 6 3
Total 164 100 21 100 19 100 204 100
April 2015 293
zirconia exhibited low plaque accumulation compared toglass-ceramic and a lithium disilicate glass-ceramic.46
Studies have also shown variations in plaque formationamong enamel and restorative materials, but it has beenconcluded that instructing the patient to maintain properoral hygiene and home care is more important than thechoice of restorative material.47
On the contrary, the difference between teeth withcrowns and contralateral teeth in terms of gingival bleedingwas not as clear as the amount of plaque would show.Plaque and gingivitis is obviously one reason for gingivalbleeding, but a subgingival crown margin can also causegingival bleeding, especially when the biological width hasbeen disturbed. Ideally the restoration margin should beplaced no more than 0.5 mm subgingivally to prevent theencroachment of biological width and the chronic peri-odontal inflammation.48 In addition, localized gingival irri-tation can be caused by excess cement, whichwas shown tobe a common early complication of single crowns.49
Some differences were seen in the number of compli-cations between the zirconia systems, but the number ofZirkonzahn Zirconia and Prettau Zirconia was quite low in
Näpänkangas et al
this study, and no comparison between the systems wasdone. However, zirconia systems may exhibit differences,particularly in terms of mechanical failures, marginaladaptation, and color matching,36,39 although zirconiafabricated by CAD/CAM demonstrated a similar andacceptable marginal fit when compared with metal ce-ramics.34 It is important to record the manufacturers ofmaterials in patient files, because in the case of a compli-cation or a possible warranty issue, the material must beidentified.
CONCLUSIONS
Zirconia can be successfully used in predoctoral dentaleducation. The success rate of the zirconia single crownsafter 4 years was 80%, and the survival rate was 89%, inaccordance with previous studies.
REFERENCES
1. Conrad HJ, Seong WJ, Pesun IJ. Current ceramic materials and systems withclinical recommendations: A systematic review. J Prosthet Dent 2007;98:389-404.
2. Della Bona A, Kelly JR. The clinical success of all-ceramic restorations. J AmDent Assoc 2008;139:8-13.
3. Groten M, Huttig F. The performance of zirconium dioxide crowns: a clinicalfollow-up. Int J Prosthodont 2010;23:429-31.
4. Shenoy A, Shenoy N. Dental ceramics: An update. J Conserv Dent 2010;13:195-203.
5. Beier US, Kapferer I, Dumfahrt H. Clinical long-term evaluation and failurecharacteristics of 1,335 all-ceramic restorations. Int J Prosthodont 2012;25:70-8.
6. Ortorp A, Kihl ML, Carlsson GE. A 3-year retrospective and clinical follow-up study of zirconia single crowns performed in a private practice. J Dent2009;37:731-6.
7. Ortorp A, Kihl ML, Carlsson GE. A 5-year retrospective study of survival ofzirconia single crowns fitted in a private clinical setting. J Dent 2012;40:527-30.
8. Poggio CE, Dosoli R, Ercoli C. A retrospective analysis of 102 zirconia singlecrowns with knife-edge margins. J Prosthet Dent 2012;107:317-21.
9. Tartaglia GM, Sidoti E, Sforza C. A 3-year follow-up study of all-ceramicsingle and multiple crowns performed in a private practice: a prospective caseseries. Clinics (Sao Paulo) 2011;66:2063-70.
10. Monaco C, Caldari M, Scotti R. Clinical evaluation of 1,132 zirconia-basedsingle crowns: a retrospective cohort study from the AIOP Clinical ResearchGroup. Int J Prosthodont 2013;26:435-42.
11. Raigrodski AJ, Hillstead MB, Meng GK, Chung KH. Survival and complica-tions of zirconia-based fixed dental prostheses: a systematic review.J Prosthet Dent 2012;107:170-7.
12. Näpänkangas R, Raustia AM. A 20-year follow-up study of fixed metalceramic single crowns. Int J Prosthodont 2008;21:307-11.
THE JOURNAL OF PROSTHETIC DENTISTRY

294 Volume 113 Issue 4
13. De Backer H, Van Maele G, De Moor N, Van den Berghe L, De Boever J. An18-year retrospective survival study of full crowns with or without posts. Int JProsthodont 2006;19:136-42.
14. De Backer H, Van Maele G, De Moor N, Van den Berghe L, De Boever J.A 20-year retrospective survival study of fixed partial dentures. Int JProsthodont 2006;19:143-53.
15. Lops D, Mosca D, Casentini P, Ghisolfi M, Romeo E. Prognosis of zirconiaceramic fixed partial dentures: a 7-year prospective study. Int J Prosthodont2012;25:21-3.
16. Pelaez J, Cogolludo PG, Serrano B, Serrano JF, Suarez MJ. A four-yearprospective clinical evaluation of zirconia and metal-ceramic posterior fixeddental prostheses. Int J Prosthodont 2012;25:451-8.
17. Vigolo P, Mutinelli S. Evaluation of zirconium-oxide-based ceramic single-unit posterior fixed dental prostheses (FDPs) generated with two CAD/CAMsystems compared to porcelain-fused-to-metal single-unit posterior FDPs: a5-year clinical prospective study. J Prosthodont 2012;21:265-9.
18. Näpänkangas R, Raustia AM. A 18-year follow-up study of fixed metalceramic partial dentures. Int J Prosthodont 2011;24:314-9.
19. Dittmer MP, Kohorst P, Borchers L, Schwestka-Polly R, Stiesch M. Stressanalysis of an all-ceramic FDP loaded according to different occlusal con-cepts. J Oral Rehabil 2011;38:278-85.
20. van Dijken JW, Hasselrot L. A prospective 15-year evaluation of extensivedentin-enamel-bonded pressed ceramic coverages. Dent Mater 2010;26:929-39.
21. Augstin-Panadero R, Fons-Font A, Roman-Rodriguez JL, Granell-Ruiz M,del Rio-Highsmith J, Sola-Ruiz MF. Zirconia versus metal: a preliminarycomparative analysis of ceramic veneer behavior. Int J Prosthodont 2012;25:294-300.
22. Manicone PF, Rossi Iommetti P, Raffaelli L. An overview of zirconia ceramics:Basic properties and clinical applications. J Dent 2007;35:819-26.
23. Kelly JR, Denry I. Stabilized zirconia as a structural ceramic: an overview.Dent Mater 2008;24:289-98.
24. Wang X, Fan D, Swain MV, Zhao K. A systematic review of all-ceramiccrowns: clinical fracture rates in relation to restored tooth type. Int J Pros-thodont 2012;25:441-50.
25. Piascik JR, Smith R, Stoner BR, Thompson JY. Adhesion/cementation tozirconia and other non-silicate ceramics: Where are we now? Dent Mater2011;27:71-82.
26. Aboushelib MN, Kleverlaan CJ, Feilzer AJ. Selective infiltration-etchingtechnique for a strong and durable bond of resin cements to zirconia-basedmaterials. J Prosthet Dent 2007;98:379-88.
27. Heintze SD, Rousson V. Fracture rates of IPS Empress all-ceramic crownseasystematic review. Int J Prosthodont 2010;23:129-33.
28. Rosentritt M, Steiger D, Behr M, Handel G, Kolbeck C. Influence of sub-structure design and spacer settings on the in vitro performance of molarzirconia crowns. J Dent 2009;37:978-83.
29. Guess PC, Zavanelli RA, Silva NR, Bonfante EA, Coelho PG, Thompson VP.Monolithic CAD/CAM lithium disilicate versus veneered Y-TZP crowns:comparison of failure modes and reliability after fatigue. Int J Prosthodont2010;23:434-42.
30. Guess PC, Bonfante EA, Silva NR, Coelho PG, Thompson VP. Effect of coredesign and veneering technique on damage and reliability of Y-TZP-supported crowns. Dent Mater 2013;29:307-16.
31. Guess PC, Bonfante EA, Coelho P, Ferencz JL, Silva NR. All ceramic systems.Laboratory and clinical performance. Dent Clin North Am 2011;55:333-52.
32. Sax C, Hämmerle CH, Sailer I. 10-year clinical outcomes of fixed dentalprostheses with zirconia frameworks. Int J Comput Dent 2011;14:183-202.
33. Al-Amleh B, Lyons K, Swain M. Clinical trials in zirconia: a systematic re-view. J Oral Rehabil 2010;37:641-52.
THE JOURNAL OF PROSTHETIC DENTISTRY
34. Biscaro L, Bonfiglioli R, Soattin M, Vigolo P. An in vivo evaluation of fit ofzirconium-oxide based ceramic single crowns, generated with two CAD/CAM systems, in comparison to metal ceramic single crowns. J Prosthodont2013;22:36-41.
35. Song TJ, Kwon TK, Yang JH, Han JS, Lee JB, Kim SH, et al. Marginal fit ofanterior 3-unit fixed partial zirconia restorations using different CAD/CAMsystems. J Adv Prosthodont 2013;5:219-25.
36. Sagirkaya E, Arikan S, Sadik B, Kara C, Karasoy D, Cehreli M. A ran-domized, prospective, open-ended clinical trial of zirconia fixed partialdentures on teeth and implants: interim results. Int J Prosthodont 2012;25:221-31.
37. Rinke S, Fornefett D, Gersdorff N, Lange K, Roediger M. Multifactorialanalysis of the impact of different manufacturing processes on the marginalfit of zirconia copings. Dent Mater J 2012;31:601-9.
38. Brawek PK, Wolfart S, Endres L, Kirsten A, Reich S. The clinical accuracy ofsingle crowns exclusively fabricated by digital workflow-the comparison oftwo systems. Clin Oral Investig 2013;17:2119-25.
39. Contrepois M, Soenen A, Bartala M, Laviole O. Marginal adaptation ofceramic crowns: A systematic review. J Prosthet Dent 2013;110:447-54.
40. Miyazaki T, Nakamura T, Matsumura H, Ban S, Kobayashi T. Current statusof zirconia restoration. J Prosthodont Res 2013;57:236-61.
41. Shillingburg HT, Staher DA, Wilson EL, Cain JR, Mitchell DL, Blanco LJ, et al.Fundamentals of fixed prosthodontics. 4th ed. Chicago: Quintessence Pub-lishing Co; 2012. p. 131-48, 161-2.
42. Silness J, Löe H. Periodontal disease in pregnancy. II. Correlationbetween oral hygiene and periodontal condition. Acta Odontol Scand1964;22:121-35.
43. Mombelli A, van Oosten MA, Schurch E Jr, Land NP. The microbiotaassociated with successful or failing osseointegrated titanium implants. OralMicrobiol Immunol 1987;2:145-51.
44. Anusavice KJ. Standardizing failure, success, and survival decisions in clinicalstudies of ceramic and metal-ceramic fixed dental prostheses. Dent Mater2012;28:102-11.
45. Tan K, Pjetursson BE, Lang NP, Chan ES. A systematic review of the survivaland complication rates of fixed partial dentures (FPDs) after an observationperiod of at least 5 years. Clin Oral Implants Res 2004;15:654-66.
46. Bremer F, Grade S, Kohorst P, Stiesch M. In vivo biofilm formation ondifferent dental ceramics. Quintessence Int 2011;42:565-74.
47. Litonjua LA, Cabanilla LL, Abbott LJ. Plaque formation and marginalgingivitis associated with restorative materials. Compend Contin Educ Dent2012;33:e6-10.
48. Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM. Current concepts on themanagement of tooth wear: part 4. An overview of the restorative techniquesand dental materials commonly applied for the management of tooth wear.Br Dent J 2012;212:169-77.
49. Pihlaja J, Näpänkangas R. Raustia Early complications and short-term failuresof zirconia single crowns and partial fixed dental prostheses. J Prosthet Dent2014;112:778-83.
Corresponding author:Dr Ritva NäpänkangasUniversity of OuluBox 5281, FIN-90014 OuluFINLANDEmail: [email protected]
Copyright © 2015 by the Editorial Council for The Journal of Prosthetic Dentistry.
Näpänkangas et al










![Archived: Predoctoral Interdisciplinary Research …€¦ · Web viewTitle Archived: Predoctoral Interdisciplinary Research Training Program in the Education Sciences [MS Word] Author](https://static.fdocuments.us/doc/165x107/5f08093a7e708231d4200257/archived-predoctoral-interdisciplinary-research-web-view-title-archived-predoctoral.jpg)




