Orthodontic Minor surgery
57
-
Upload
sanutom -
Category
Health & Medicine
-
view
225 -
download
19
Transcript of Orthodontic Minor surgery


Surgical procedures carried out as an adjunct to or in
conjunction with orthodontic treatment are termed as
surgical orthodontics.

These surgical procedures are usually carried out to eliminate
an etiologic factor or to correct severe dentofacial
abnormalities that cannot be satisfactorily treated by growth
modification procedures or orthodontic camouflage.
Retained deciduous teeth misplaced tooththe eruption of permanent central incisor.

Surgical orthodontic procedures are broadly classified as
a) minor surgical procedures
b) major surgical procedures .
Most minor surgical procedures are an integral part of
orthodontic therapy
The major procedures are aimed at treatment of severe
skeletal malocclusion or dentofacial deformities that cannot
be satisfactorily treated by orthodontic treatment alone.
There should be good co-ordination between oral surgeon and
orthodontist when undertaking such procedures
• Extraction
• Surgical uncovering of teeth
• Frenectomy
• Pericision
• Transplantation of teeth
• Corticotomy

Extractions are the most commonly undertaken minor
surgical procedures in conjunction with orthodontic therapy.

Extraction procedures carried out are :
Therapeutic extraction
Serial extraction
Extraction of carious teeth
Extraction of malformed teeth
Extraction of supernumerary teeth
Extraction of impacted teeth

Therapeutic extraction is undertaken as a part of full fledged
orthodontic treatment mainly to gain space.
• Prior to therapeutic extraction a thorough diagnostic exercise
is essential.
• Preoperative radiographs are a valuable aid in planning and
execution of extraction.

Features
Extraction should be as atraumatic as possible
Care should be taken to preserve the integrity of the alveolus.
Any break or loss of either buccal or lingual bony plates may
prevent ideal positioning of the teeth during orthodontic
therapy

Serial extraction is an interceptive orthodontic procedure
Usually initiated in the early mixed dentition period

Corrected by a procedure that includes the planned extraction
of certain deciduous teeth and later specific permanent teeth
in an orderly sequence and pre determined pattern to guide
the erupting permanent teeth in to a , more favorable
position.


Premature loss
Arch length –tooth material discrepancy
Lingual eruption of laterals
Canines erupting mesialy over laterals
Mesial drift of buccal segments
Flaring
Ectopic eruption
Labial stripping or gingival l recession usually of lower incisors

The most common teeth to be impacted other than third
molars are maxillary canine followed by premolars, and
maxillary second molars
Ectopically erupted
Adjacent teeth are in good contact
Any pathology associated with it
Causing pressure on root of standing tooth
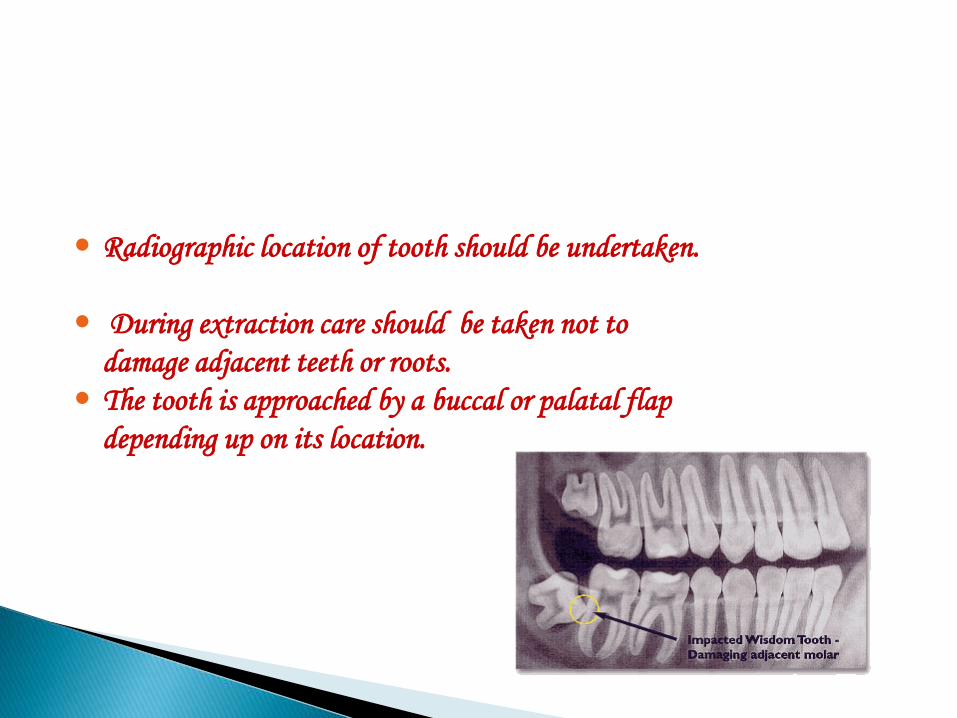
Radiographic location of tooth should be undertaken.
During extraction care should be taken not to
damage adjacent teeth or roots.
The tooth is approached by a buccal or palatal flap
depending up on its location.

Supernumerary
odontomes

Supernumeraries should be extracted when:
in anterior maxillary region, it prevents eruption of the permanent incisors
Cause malpositioning of adjacent tooth
If erupted causing crowding and periodontal complications
Cyst associated with it

After careful elevation of flap , adequate amount of bone is
removed using rotary cutting instruments
.The impacted or supernumerary tooth is removed and the
extraction socket inspected for any pathological tissue.
The flap is repositioned and sutures are placed for a week.

The presence of impacted teeth in dental arch can cause minor
dental irregularities due to deflection of adjacent teeth.
Impaction of teeth usually occur as a result of arch length
discrepancy or presence of mucosal and bony barriers that
prevent their eruption

The most commonly impacted tooth is the maxillary
permanent canine.
In many cases it is possible for the orthodontist to guide the
impacted canine in to normal location in the dental arch after
adequate surgical exposure.

An un erupted canine may be a candidate for surgical exposure
if :
No sign of tooth even after 12 years of age
Adequate room in the arch
Un obstructed path of eruption
Radio graphically root is not dilacerated

Location of the tooth
Evaluation of favorability
Evaluation of space adequacy
Surgical excision and bone removal
Fixing orthodontic attachments

Exact location of impacted tooth has to be determined .
This can be done using tube shift or right angle technique.
Most impacted teeth present as a bulge corresponding to their location which should be examined clinically by inspection and palpation

In many cases the orientation of impacted teeth may be such
that surgical orthodontic guidance of tooth in to the arch
may not be possible.
The favorability should be examined prior to the procedure, it
is considered favorable whenever the apex of canine is closer
to its normal position.

When impacted tooth is guided in to dental arch adequate space
should be present for their normal alignment .
In many cases involving the impaction of permanent canine the
deciduous canines are over retained .
These teeth have to be extracted to accommodate the permanent
canine.

The crown of impacted tooth is exposed by excision of the
overlying soft tissue and removal of bone covering .
The bone should be removed up to maximum height of
contour.

In most cases of favorably impacted canines, once the soft tissue and bony tissue is removed , the canine erupt on its own.
In some cases orthodontic guidance for eruption of the teeth in to the arch may be required.
Attachments are placed on the impacted tooth to guide the erupting tooth in to the arch

A metal crown with a hook
A celluloid crown with an attachment bonded to it.
Bondable orthodontic brackets or button

A ligature wire is wound around the attachment and the other end is tied to a removable or fixed orthodontic appliance.
The wire is gradually tightened at regular intervals to guide the erupting tooth.

Frenectomy is a surgical procedure performed to excise the
frenum and remove the deeply embedded fibrous tissue.
It may be a labial frenectomy and lingual frenectomy.

Two school of thoughts are :
i. it should be performed before orthodontic treatment
ii. It should be done after orthodontic treatment as it reduces
risk of scar tissue that prevents the closure of diastema

Indications: when a median diastema is being caused or held open by a thick, short and fibrous labial frenum which is attached to the incisive papilla.
Sometimes this frenum may insert in the inter maxillary suture area on the palatal aspect. When tension is applied to the frenum , incisive papilla should blanch.

Frenectomy usually done only after eruption of permanent
lateral incisors and canines fails to close the midline diastema
.
It can be done either before or after appliance therapy has
approximated central incisors.

The purpose of frenectomy is to eliminate the fibrous tissue
between the roots of the central incisors so that there is no
obstruction to approximation of these teeth by appliance
therapy.
Local anesthetic is infiltrated on either side of the frenum and
an assistant holds the lip outwards and forward while exerting
pressure on the lateral aspect , there by reducing the resultant
bleeding.

With no: 15 knife , incisions down to the bone are made on either side of the frenum , going in between the teeth and joined around the incisive papilla.
With a periosteal elevator ,underlying fibrous tissue is detached from the palatal bone and in between the teeth, This releases the frenum , which is left attached to the lip at its anterior end.


The band of tissue connecting the tongue to the floor of the mouth is called the lingual frenum or frenulum.
Occasionally this frenum might be congenitally short, thick, or tight , or may extend too far down along the tongue or the gum.

An unusually thick , large, or tight lingual frenum can
seriously constrict the movement of the tongue and this
condition called
“ tongue tie” or ankyloglossia.

Children may have difficulty breast feeding as infants and may
later develop lisping.
The patient is unable to clear away food from the roof of the
palate and from labiobuccal sulci
Occasionally , irregularity
of the lower incisors may develop .

Some patients may develop an open bite because of the pull
of the frenum on the jaw and tongue thrusting.
In edentulous patients the frenum may interfere with the fit
of the lower denture causing its displacement every time the
tongue moves.
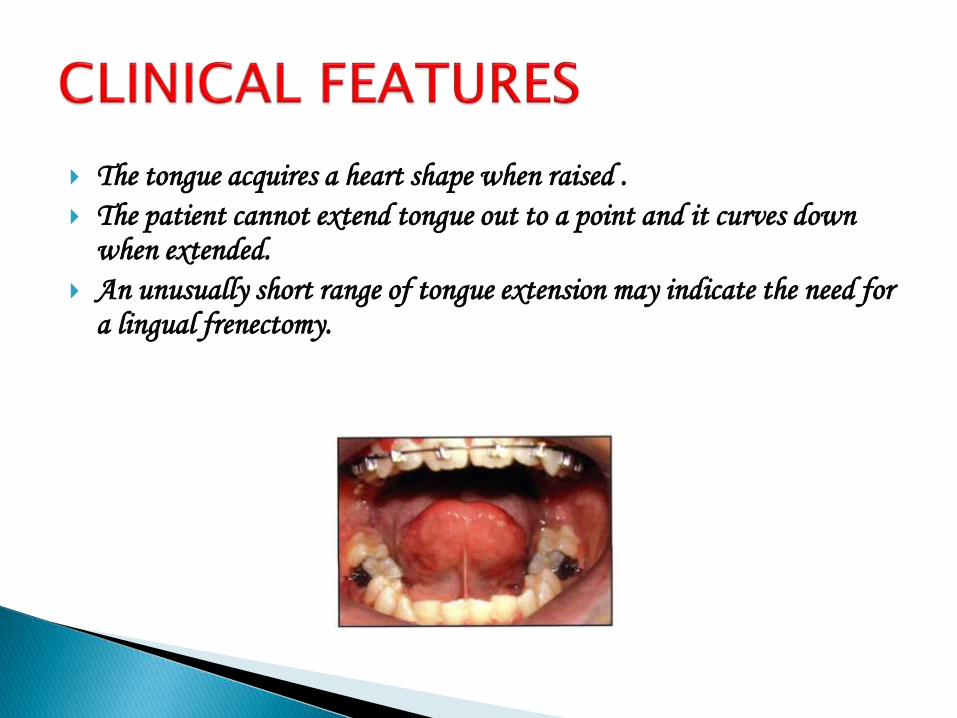
The tongue acquires a heart shape when raised .
The patient cannot extend tongue out to a point and it curves down when extended.
An unusually short range of tongue extension may indicate the need for a lingual frenectomy.

A frenectomy is performed using either scalpel or a carbon
dioxide laser .
The surgeon excises the frenum or performs a
Z – plasty in order to
mobilize the tongue.

Pericision or circumferential supracrestal fibrotomy as it is
often called a minor surgical procedure that is undertaken to
counter the relapse tendency of the stretched gingival fibers.

Pericision involves surgical sectioning of these fibers by
passing a sharp narrow scalpel through the gingival sulcus
around the tooth to a depth of 2 mm apical to the alveolar
crest.
Pericision is generally undertaken as an adjunctive retention
procedure after the correction of rotations.

Under LA a no 11 knife is passed through gingival sulcus up to
crest alveolar bone
Cuts are made inter proximally on each side of a rotated tooth
and along the labial or lingual gingival margin

Transplantation of teeth has been advocated as an alternative
to other methods of treatment of impacted teeth.
It may be a good alternative for the adult patient who cannot
undergo conventional orthodontic movement of an impacted
tooth.
The advocated technique is a careful wide exposure of the
impacted tooth. .

The tooth is then moved in to its position with in the dental
arch and is stabilized with a segmental orthodontic
appliance.
Endodontic treatment ,if necessary is rendered 6 to 8 weeks
after the surgical procedure initially using a calcium
hydroxide paste.

Then a conventional root canal filling is done 1 year later.
Teeth may be transplanted from one position to another in
the dental arch .

Corticotomy is a surgical procedure usually undertaken in
patients having dental proclination with spacing .
This technique involves the sectioning of the dentoalveolar
region in to multiple small units to fasten orthodontic tooth
movement.
Labial flaps are raised and interdental bony cuts are made
parallel to the long axis of teeth
Done in young adults to reduce the duration of appliance
therapy
Rapid movement of one or more teeth

These cuts may be joined together by a horizontal bony cut above the apices of the roots.
Care should be taken not to totally separates the individual units.
Following the surgery ; orthodontic tooth movement is initiated using fixed appliance.


Adults with skeletal maxillary constriction
RME is not possible in this patients because of fusion of mid
palatal sutures

A jackscrew expansion device is cemented before surgery
followed by corticotomies are performed
Mid palatal sutures are osteotomized
Activate jackscrew
Expansion carried out in small increments
A stabilization period of 6 weeks for bony consolidation to
occur


Only through team effort that the multifaceted problems can
be successfully controlled.
To accomplish optimal orthodontic treatment a combined
effort of oral and maxillofacial surgeon and orthodontist is
essential