Minor oral surgery.
8
Minor Oral Surgery Thilanka Umesh Sugathadasa
-
Upload
faculty-of-dental-sciences-university-of-peradeniya -
Category
Education
-
view
132 -
download
6
Transcript of Minor oral surgery.
Minor Oral
Surgery
Thilanka Umesh Sugathadasa
Thilanka Umesh Sugathadasa Page 1
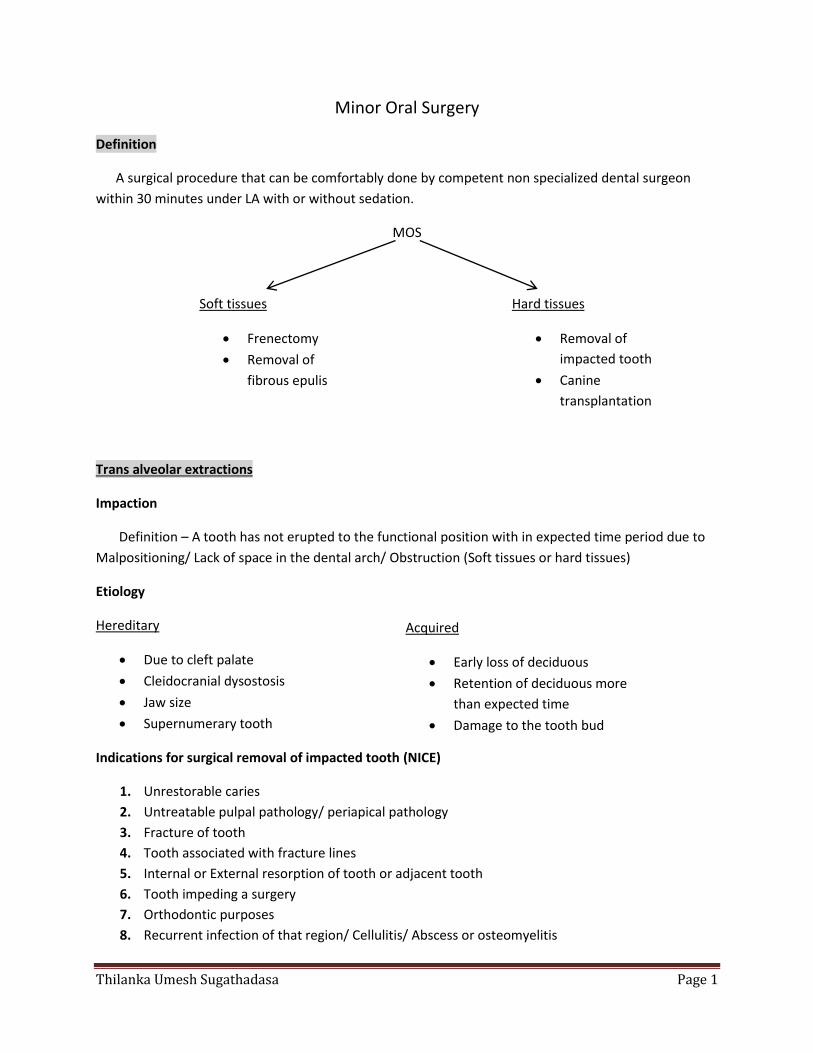
Minor Oral Surgery
Definition
A surgical procedure that can be comfortably done by competent non specialized dental surgeon
within 30 minutes under LA with or without sedation.
MOS
Trans alveolar extractions
Impaction
Definition – A tooth has not erupted to the functional position with in expected time period due to
Malpositioning/ Lack of space in the dental arch/ Obstruction (Soft tissues or hard tissues)
Etiology
Hereditary
Due to cleft palate
Cleidocranial dysostosis
Jaw size
Supernumerary tooth
Indications for surgical removal of impacted tooth (NICE)
1. Unrestorable caries
2. Untreatable pulpal pathology/ periapical pathology
3. Fracture of tooth
4. Tooth associated with fracture lines
5. Internal or External resorption of tooth or adjacent tooth
6. Tooth impeding a surgery
7. Orthodontic purposes
8. Recurrent infection of that region/ Cellulitis/ Abscess or osteomyelitis
Soft tissues
Frenectomy
Removal of
fibrous epulis
Hard tissues
Removal of
impacted tooth
Canine
transplantation
Acquired
Early loss of deciduous
Retention of deciduous more
than expected time
Damage to the tooth bud
Thilanka Umesh Sugathadasa Page 2
9. Cyst or tumor
10. Prophylactic removal or in combine surgeries.
Contraindications
1. Extremes of Ages(Higher ages the bone become highly calcified though less flexible & less likely
to be bend also post-operative problems more in the elderly persons)
2. Compromised medical status
3. Excessive damage to the adjacent structures.
Classifications(Extraction difficulty indices)
1. Pell & Gregory classification.
2. Winter’s line
3. Penderson scale
4. Parents scale
5. WHARFE scale
6. Classify according to angulation of the tooth.
- Mesio angular
- Disto angular
- Horizontal
- Vertical
- Transverse
- Inverted
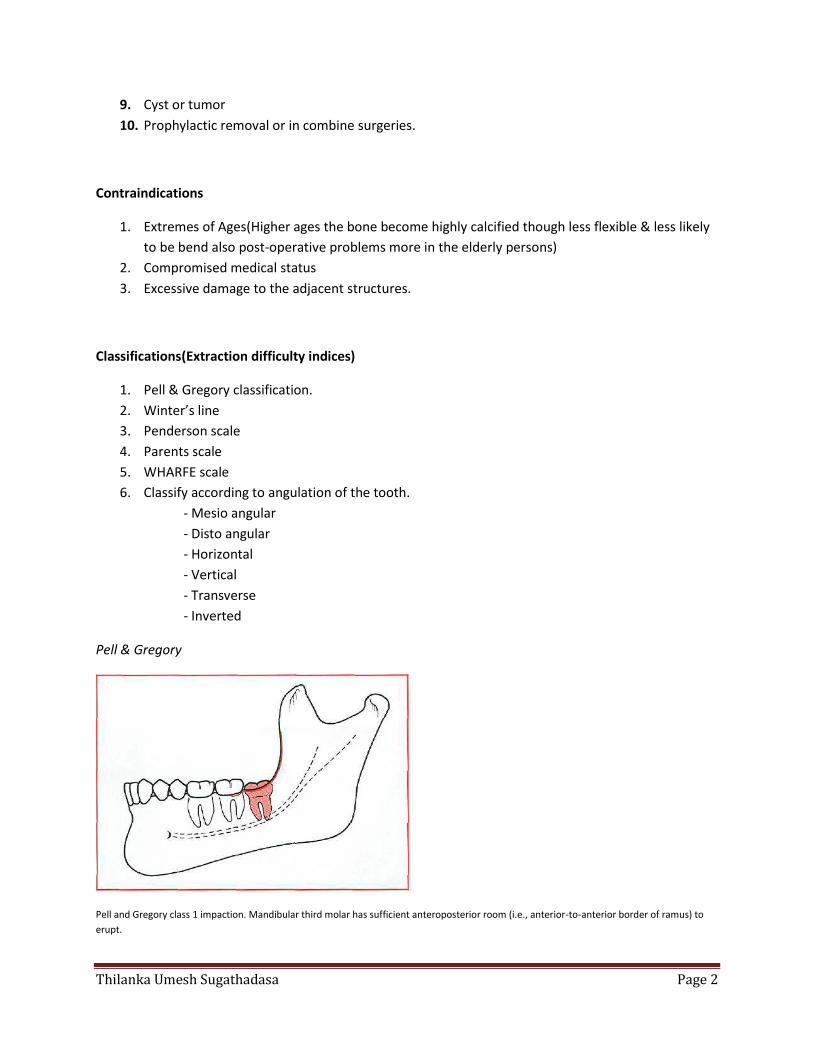
Pell & Gregory
Pell and Gregory class 1 impaction. Mandibular third molar has sufficient anteroposterior room (i.e., anterior-to-anterior border of ramus) to
erupt.
Thilanka Umesh Sugathadasa Page 3
.
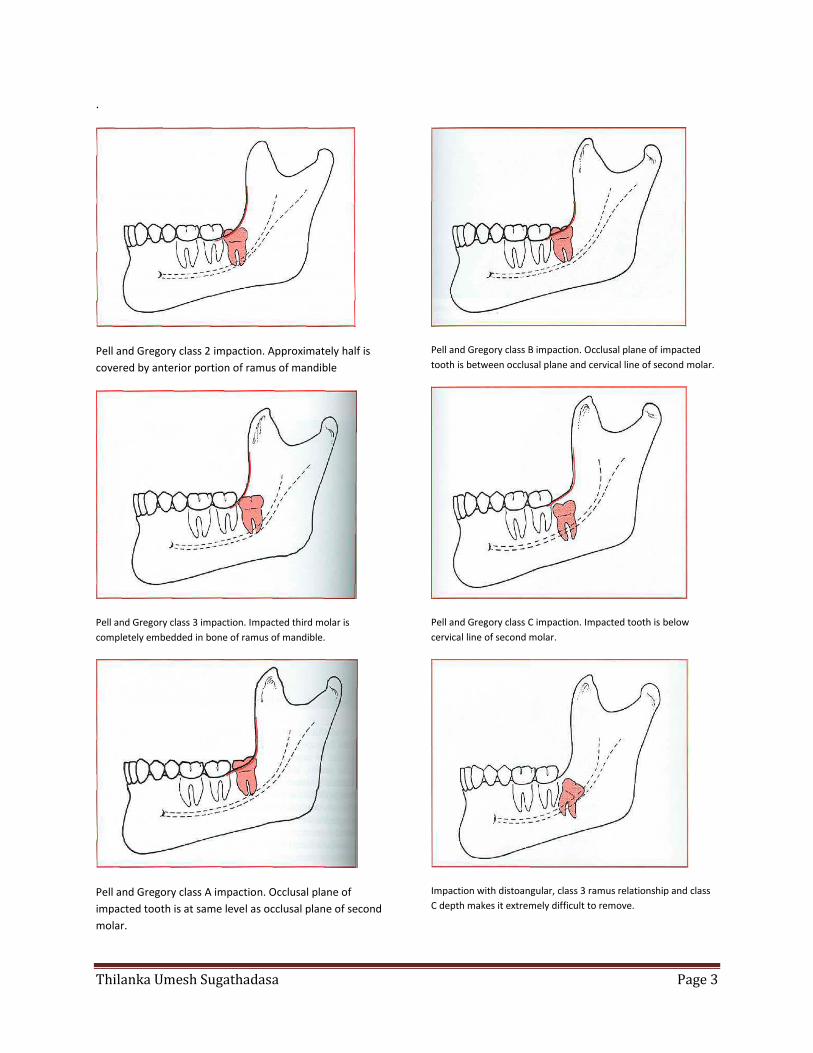
Pell and Gregory class 2 impaction. Approximately half is
covered by anterior portion of ramus of mandible
Pell and Gregory class 3 impaction. Impacted third molar is
completely embedded in bone of ramus of mandible.
Pell and Gregory class A impaction. Occlusal plane of
impacted tooth is at same level as occlusal plane of second
molar.
Pell and Gregory class B impaction. Occlusal plane of impacted
tooth is between occlusal plane and cervical line of second molar.
Pell and Gregory class C impaction. Impacted tooth is below
cervical line of second molar.
Impaction with distoangular, class 3 ramus relationship and class
C depth makes it extremely difficult to remove.
Thilanka Umesh Sugathadasa Page 4
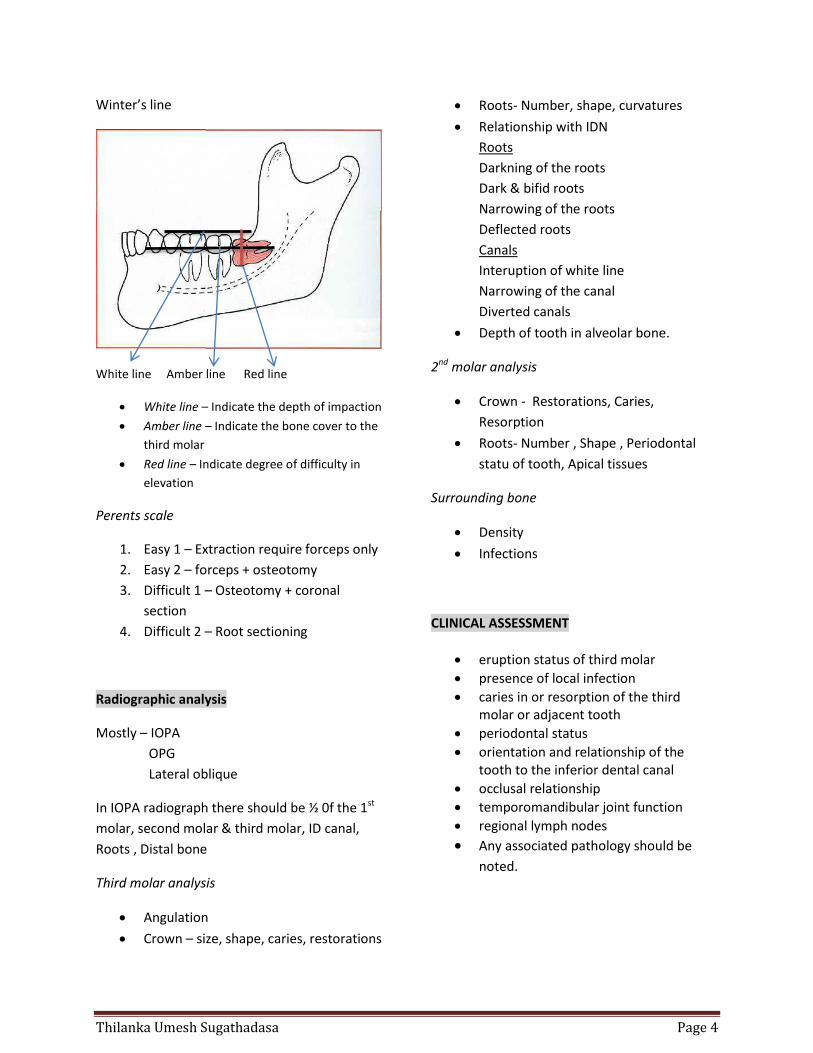
Winter’s line
White line Amber line Red line
White line – Indicate the depth of impaction
Amber line – Indicate the bone cover to the
third molar
Red line – Indicate degree of difficulty in
elevation
Perents scale
1. Easy 1 – Extraction require forceps only
2. Easy 2 – forceps + osteotomy
3. Difficult 1 – Osteotomy + coronal
section
4. Difficult 2 – Root sectioning
Radiographic analysis
Mostly – IOPA
OPG
Lateral oblique
In IOPA radiograph there should be ½ 0f the 1st
molar, second molar & third molar, ID canal,
Roots , Distal bone
Third molar analysis
Angulation
Crown – size, shape, caries, restorations
Roots- Number, shape, curvatures
Relationship with IDN
Roots
Darkning of the roots
Dark & bifid roots
Narrowing of the roots
Deflected roots
Canals
Interuption of white line
Narrowing of the canal
Diverted canals
Depth of tooth in alveolar bone.
2nd molar analysis
Crown - Restorations, Caries,
Resorption
Roots- Number , Shape , Periodontal
statu of tooth, Apical tissues
Surrounding bone
Density
Infections
CLINICAL ASSESSMENT
eruption status of third molar
presence of local infection
caries in or resorption of the third molar or adjacent tooth
periodontal status
orientation and relationship of the tooth to the inferior dental canal
occlusal relationship
temporomandibular joint function
regional lymph nodes
Any associated pathology should be
noted.
Thilanka Umesh Sugathadasa Page 5
SERIOUS COMPLICATIONS
Fracture of the mandible or maxilla: Treat at time of surgery or arrange immediate referral.
Oro-antral communication: Repair at time of surgery, usually with a buccal advancement flap. Antibiotic therapy is advisable and the patient should avoid nose blowing.
Broken instrument: Remove at time of surgery. If not retrievable, inform the patient and record in notes
.
Nerve damage: For complete transection of lingual or inferior dental nerves, arrange immediate nerve repair by experienced surgeon. For partial damage, debride gently
and maintain good apposition of the
ends
COMMON COMPLICATIONS
Haemorrhage: Control at time of surgery. Soft tissue bleeding may require haemostatic agents, bipolar diathermy and/or sutures.
Bruising: Patients should be informed that bruising is common and will usually resolve within two weeks
Displacement: Appropriate instruments should be in place prior to elevation to help prevent displacement. Recover any displaced tooth at time of surgery if possible, or arrange referral to a specialist centre
Wound dehiscence: If no pain or infection, advise patients to continue wound toilet (e.g. hot salty mouthwashes, socket syringing).
Damage to adjacent teeth: Inform patient at time of surgery (or when fully conscious). Record in notes and arrange repair if required.
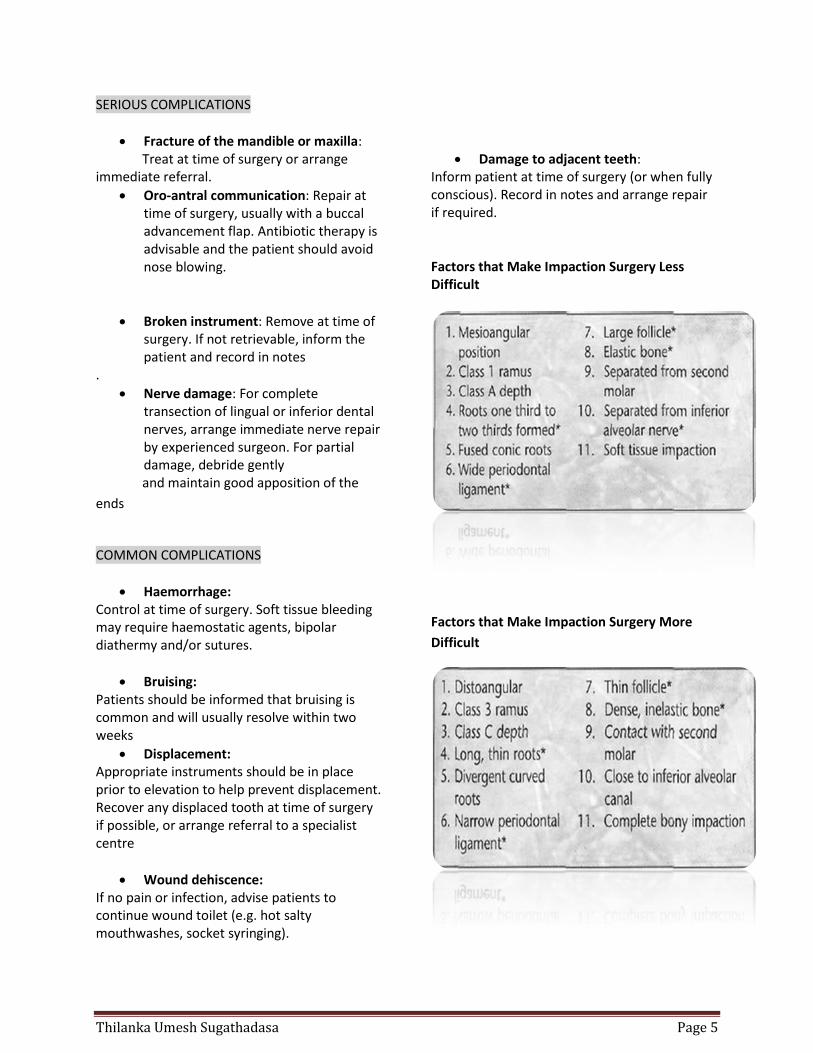
Factors that Make Impaction Surgery Less Difficult
Factors that Make Impaction Surgery More
Difficult
Thilanka Umesh Sugathadasa Page 6
Prophylaxis doses
Amoxicillin(Oral) Adults - 2g Childs - 50mg/kg
Amphicillin(IV) Adults – 2g Childs – 50mg/kg
Clindamycin Adults – 600mg Childs – 20mg/kg
Clarythromycin Adults – 500mg Childs – 15mg/kg
Indications 1. Heart transplantation 2. Prosthetic heart valves 3. Previous Hx of IE 4. Cyanotic heart diseases.
Flap Definition ; A unit of skin & Subcutaneous tissues that transferred from donor site to the recipient site, while surviving it’s own intravascular circulation. Graft Does not carry it’s own blood supply survive by the blood supply of the recipient site. Mucoperiosteal flap Definition : A unit of mucosa & periosteal elevated by surgical incision for exposure of an underlying pathology of bone (jaws) Main principles
1. Preserve blood supply 2. Good accessibility 3. Easy to repositioning 4. Margins should be lying on the intact
bone 5. Prevent damage to the vital structures
In 3rd molar removal surgery when
suturing the suture distal to the 2nd molar should be very tight. Otherwise it causes post-operative sensitivity.
Also most of the time when raising flap in the edentulous mandible we have to take extra precautions to not to damage the periosteum, Because due to no teeth ID artery blood supply reduced though most of the time edentulous arch depend on the periosteal blood supply. So we have to raise supraperiosteal flap.
Effect of root morphology in impaction surgery
Root morphology plays a major role in deter-mining the degree of difficulty of the impacted tooth's removal
The first consideration is the length of
the root when the root is one third to two thirds formed, the ends of the roots are blunt and almost never fracture
If the tooth is not removed during the
formative stage and the entire length of the root develops, the possibility increases for abnormal root morphology and for fracture of the root tips during extraction.
If the root development is insufficient
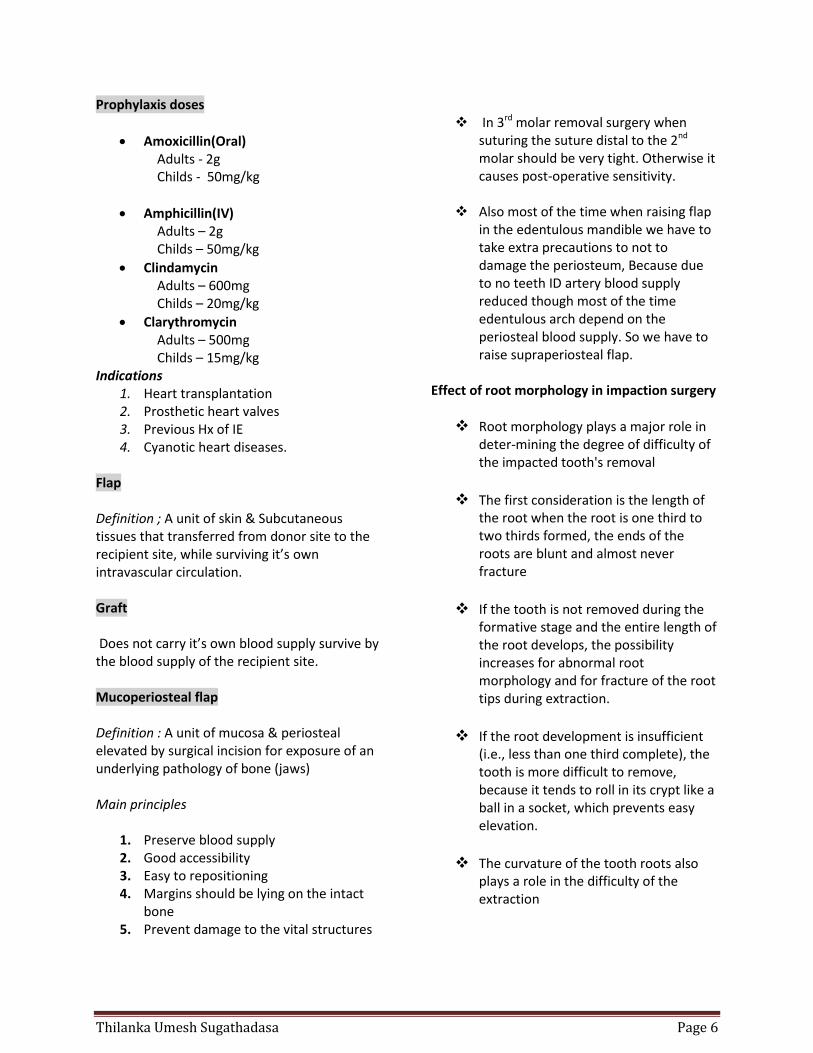
(i.e., less than one third complete), the tooth is more difficult to remove, because it tends to roll in its crypt like a ball in a socket, which prevents easy elevation.
The curvature of the tooth roots also
plays a role in the difficulty of the extraction
Thilanka Umesh Sugathadasa Page 7
Lack of root development. If extraction is attempted, crown will roll around in crypt, which makes it difficult to remove.
Finally, the surgeon should assess the
periodontal ligament space. older
patients, especially those over age 40,
tend to have a much narrower
periodontal ligament space, which
thereby increases the difficulty of the
extraction.
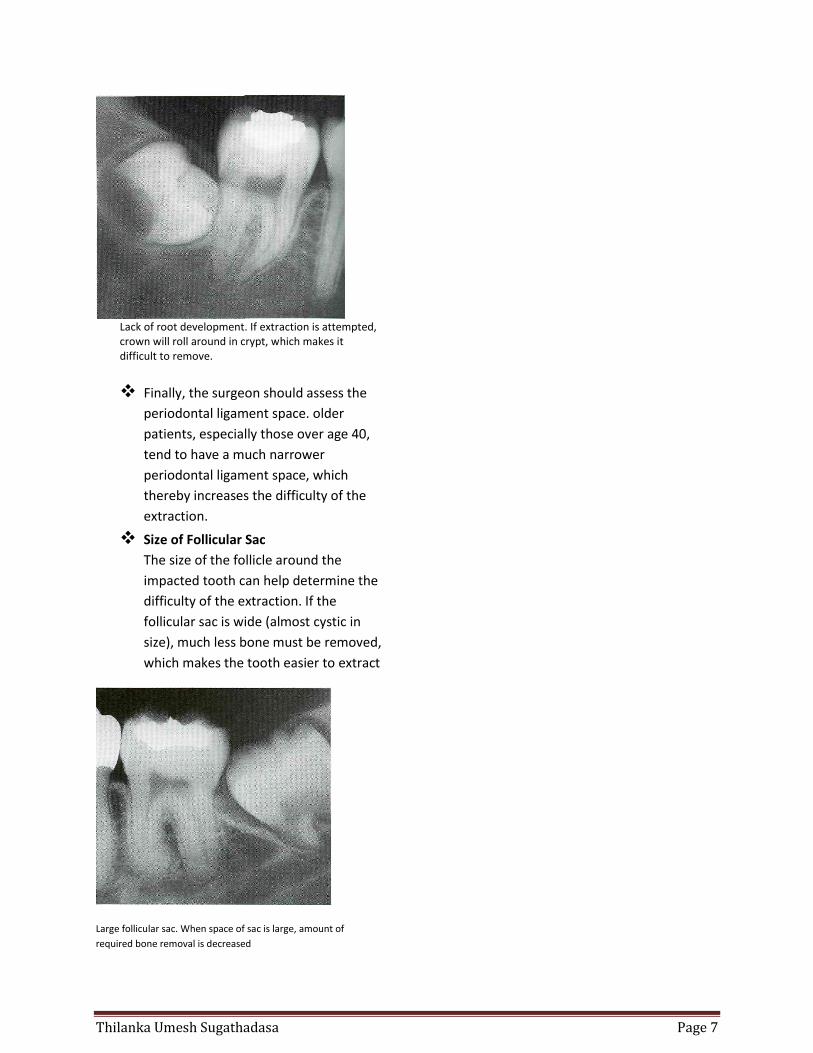
Size of Follicular Sac
The size of the follicle around the
impacted tooth can help determine the
difficulty of the extraction. If the
follicular sac is wide (almost cystic in
size), much less bone must be removed,
which makes the tooth easier to extract
Large follicular sac. When space of sac is large, amount of
required bone removal is decreased