Original Research ajog - Losing Lucy and Finding Hope
9
OBSTETRICS M281, an anti-FcRn antibody, inhibits IgG transfer in a human ex vivo placental perfusion model Sucharita Roy, PhD; Tatiana Nanovskaya, PhD; Svetlana Patrikeeva, MS; Edward Cochran; Viraj Parge, MS; Jamey Guess, MS; John Schaeck, PhD; Amit Choudhury, PhD; Mahmoud Ahmed, PhD; Leona E. Ling, PhD BACKGROUND: The transfer of pathogenic immunoglobulin G anti- bodies from mother to fetus is a critical step in the pathophysiology of alloimmune and autoimmune diseases of the fetus and neonate. Immu- noglobulin G transfer across the human placenta to the fetus is mediated by the neonatal Fc receptor, and blockade of the neonatal Fc receptor may provide a therapeutic strategy to prevent or minimize pathological events associated with immune-mediated diseases of pregnancy. M281 is a fully human, aglycosylated monoclonal immunoglobulin G1 antineonatal Fc receptor antibody that has been shown to block the neonatal Fc receptor with high affinity in nonclinical studies and in a phase 1 study in healthy volunteers. OBJECTIVE: The objective of the study was to determine the trans- placental transfer of M281 and its potential to inhibit transfer of immu- noglobulin G from maternal to fetal circulation. STUDY DESIGN: To determine the concentration of M281 required for rapid cellular uptake and complete saturation of the neonatal Fc receptor in placental trophoblasts, primary human villous trophoblasts were incu- bated with various concentrations of M281 in a receptor occupancy assay. The placental transfer of M281, immunoglobulin G, and immunoglobulin G in the presence of M281 was studied using the dually perfused human placental lobule model. Immunoglobulin G transfer was established using a representative immunoglobulin G molecule, adalimumab, a human immunoglobulin G1 monoclonal antibody, at a concentration of 270 mg/ mL. Inhibition of immunoglobulin G transfer by M281 was determined by cotransfusing 270 mg/mL of adalimumab with 10 mg/mL or 300 mg/mL of M281. Concentrations of adalimumab and M281 in sample aliquots from maternal and fetal circuits were analyzed using a sandwich enzyme-linked immunosorbent assay and Meso Scale Discovery assay, respectively. RESULTS: In primary human villous trophoblasts, the saturation of the neonatal Fc receptor by M281 was observed within 30e60 minutes at 0.15e5.0 mg/mL, suggesting rapid blockade of neonatal Fc receptor in placental cells. The transfer rate of adalimumab (0.23% 0.21%) across dually perfused human placental lobule was significantly decreased by 10 mg/mL and 300 mg/mL of M281 to 0.07 0.01% and 0.06 0.01%, respectively. Furthermore, the transfer rate of M281 was 0.002% 0.02%, approximately 100-fold lower than that of adalimumab. CONCLUSION: The significant inhibition of immunoglobulin G transfer across the human placental lobule by M281 and the minimal transfer of M281 supports the development of M281 as a novel agent for the treatment of fetal and neonatal diseases caused by transplacental transfer of alloimmune and autoimmune pathogenic immunoglobulin G antibodies. Key words: autoimmune disease, fetal transfer, monoclonal antibodies, M281, neonate, placental perfusion model A lloimmune and autoimmune dis- eases of the fetus and newborn result from maternal development of potent pathogenic immunoglobulin G (IgG) antibodies that are transferred from mother to fetus. 1 For example, hemolytic disease of the fetus and newborn, fetal neonatal autoimmune thrombocytopenia, and autoimmune congenital heart block result from development of maternal IgG antibodies against fetal red blood cell antigens, platelets, or the developing fetal AV node, respectively. 1e3 With elevated maternal titers and, importantly, patho- genic IgG potency, the exposure of the fetus to these alloantibodies or autoantibodies through the increasing placental transfer of IgG from the second to third trimester results in damage to fetal tissues and disease development. 4,5 The neonatal Fc receptor (FcRn) me- diates the passage of IgG from mother to fetus in addition to maintaining the long half-life of IgG by IgG recycling in vascular endothelial cells. 6 These mech- anisms suggest that an inhibitor of FcRn- IgG interaction may prevent or mini- mize gestational transfer of pathogenic IgG from mother to fetus as well as decrease pathogenic antibody titers in maternal circulation. M281 is a mono- clonal anti-FcRn antibody that binds with high affinity to the IgG binding site on FcRn and blocks IgG binding to FcRn. In a phase 1 normal healthy volunteer study, M281 was observed to rapidly saturate systemic FcRn upon intravenous administration and decrease circulating IgG consistent with inhibi- tion of IgG recycling. 7 The aims of the current study were to determine the potential of M281 to inhibit transplacental IgG transfer using adalimumab as a representative IgG molecule and to determine whether M281 itself is transferred across the hu- man placenta using the dually perfused human placental model. Materials and Methods Test agents and reagents Adalimumab (Humira; AbbVie Inc, North Chicago, IL) and IVIg (Car- immune, lyophilized preparation; CSL Behring, Bern, Switzerland) were ob- tained from commercial sources. M281 was produced and manufactured by Momenta Pharmaceuticals Inc (Cam- bridge, MA). Dextran 40, gentamicin sulfate, heparin, sodium bicarbonate, Cite this article as: Roy S, Nanovskaya T, Patrikeeva S, et al. M281, an anti-FcRn antibody, inhibits IgG transfer in a human ex vivo placental perfusion model. Am J Obstet Gynecol 2019;220:498.e1-9. 0002-9378 ª 2019 The Author(s). Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http:// creativecommons.org/licenses/by-nc-nd/4.0/). https://doi.org/10.1016/j.ajog.2019.02.058 498.e1 American Journal of Obstetrics & Gynecology MAY 2019 Original Research ajog.org
Transcript of Original Research ajog - Losing Lucy and Finding Hope

Original Research ajog.org
OBSTETRICS
M281, an anti-FcRn antibody, inhibits IgG transfer in ahuman ex vivo placental perfusion model
Sucharita Roy, PhD; Tatiana Nanovskaya, PhD; Svetlana Patrikeeva, MS; Edward Cochran; Viraj Parge, MS;Jamey Guess, MS; John Schaeck, PhD; Amit Choudhury, PhD; Mahmoud Ahmed, PhD; Leona E. Ling, PhDBACKGROUND: The transfer of pathogenic immunoglobulin G anti- immunoglobulin G1 monoclonal antibody, at a concentration of 270 mg/
bodies from mother to fetus is a critical step in the pathophysiology ofalloimmune and autoimmune diseases of the fetus and neonate. Immu-
noglobulin G transfer across the human placenta to the fetus is mediated
by the neonatal Fc receptor, and blockade of the neonatal Fc receptor may
provide a therapeutic strategy to prevent or minimize pathological events
associated with immune-mediated diseases of pregnancy. M281 is a fully
human, aglycosylated monoclonal immunoglobulin G1 antineonatal Fc
receptor antibody that has been shown to block the neonatal Fc receptor
with high affinity in nonclinical studies and in a phase 1 study in healthy
volunteers.
OBJECTIVE: The objective of the study was to determine the trans-
placental transfer of M281 and its potential to inhibit transfer of immu-
noglobulin G from maternal to fetal circulation.
STUDYDESIGN: To determine the concentration of M281 required forrapid cellular uptake and complete saturation of the neonatal Fc receptor
in placental trophoblasts, primary human villous trophoblasts were incu-
bated with various concentrations of M281 in a receptor occupancy assay.
The placental transfer of M281, immunoglobulin G, and immunoglobulin G
in the presence of M281 was studied using the dually perfused human
placental lobule model. Immunoglobulin G transfer was established using
a representative immunoglobulin G molecule, adalimumab, a human
Cite this article as: Roy S, Nanovskaya T, Patrikeeva S,et al. M281, an anti-FcRn antibody, inhibits IgG transfer in
a human ex vivo placental perfusion model. Am J Obstet
Gynecol 2019;220:498.e1-9.
0002-9378ª 2019 The Author(s). Published by Elsevier Inc. This is an
open access article under the CC BY-NC-ND license (http://
creativecommons.org/licenses/by-nc-nd/4.0/).https://doi.org/10.1016/j.ajog.2019.02.058
498.e1 American Journal of Obstetrics & Gynecology MAY 2019
mL. Inhibition of immunoglobulin G transfer by M281 was determined by
cotransfusing 270 mg/mL of adalimumab with 10 mg/mL or 300 mg/mL ofM281. Concentrations of adalimumab and M281 in sample aliquots from
maternal and fetal circuits were analyzed using a sandwich enzyme-linked
immunosorbent assay and Meso Scale Discovery assay, respectively.
RESULTS: In primary human villous trophoblasts, the saturation of theneonatal Fc receptor by M281 was observed within 30e60 minutes at
0.15e5.0 mg/mL, suggesting rapid blockade of neonatal Fc receptor in
placental cells. The transfer rate of adalimumab (0.23%� 0.21%) across
dually perfused human placental lobule was significantly decreased by 10
mg/mL and 300 mg/mL of M281 to 0.07 � 0.01% and 0.06 � 0.01%,
respectively. Furthermore, the transfer rate of M281 was 0.002% �0.02%, approximately 100-fold lower than that of adalimumab.
CONCLUSION: The significant inhibition of immunoglobulin G transfer
across the human placental lobule by M281 and the minimal transfer of
M281 supports the development of M281 as a novel agent for the
treatment of fetal and neonatal diseases caused by transplacental transfer
of alloimmune and autoimmune pathogenic immunoglobulin G antibodies.
Keywords: autoimmune disease, fetal transfer, monoclonal antibodies,M281, neonate, placental perfusion model
lloimmune and autoimmune dis-
A eases of the fetus and newbornresult from maternal development ofpotent pathogenic immunoglobulin G(IgG) antibodies that are transferredfrom mother to fetus.1 For example,hemolytic disease of the fetus andnewborn, fetal neonatal autoimmunethrombocytopenia, and autoimmunecongenital heart block result fromdevelopment of maternal IgG antibodiesagainst fetal red blood cell antigens,platelets, or the developing fetal AVnode, respectively.1e3 With elevatedmaternal titers and, importantly, patho-genic IgG potency, the exposure ofthe fetus to these alloantibodies orautoantibodies through the increasingplacental transfer of IgG from thesecond to third trimester results indamage to fetal tissues and diseasedevelopment.4,5
The neonatal Fc receptor (FcRn) me-diates the passage of IgG frommother tofetus in addition to maintaining the longhalf-life of IgG by IgG recycling invascular endothelial cells.6 These mech-anisms suggest that an inhibitor of FcRn-IgG interaction may prevent or mini-mize gestational transfer of pathogenicIgG from mother to fetus as well asdecrease pathogenic antibody titers inmaternal circulation. M281 is a mono-clonal anti-FcRn antibody that bindswith high affinity to the IgG binding siteon FcRn and blocks IgG binding toFcRn. In a phase 1 normal healthyvolunteer study, M281 was observed to
rapidly saturate systemic FcRn uponintravenous administration and decreasecirculating IgG consistent with inhibi-tion of IgG recycling.7
The aims of the current study were todetermine the potential of M281 toinhibit transplacental IgG transfer usingadalimumab as a representative IgGmolecule and to determine whetherM281 itself is transferred across the hu-man placenta using the dually perfusedhuman placental model.
Materials and MethodsTest agents and reagentsAdalimumab (Humira; AbbVie Inc,North Chicago, IL) and IVIg (Car-immune, lyophilized preparation; CSLBehring, Bern, Switzerland) were ob-tained from commercial sources. M281was produced and manufactured byMomenta Pharmaceuticals Inc (Cam-bridge, MA). Dextran 40, gentamicinsulfate, heparin, sodium bicarbonate,

AJOG at a Glance
Why was this study conducted?This study was conducted to evaluate the transplacental transfer of M281, amonoclonal anti-FcRn antibody and its potential to inhibit the transfer ofimmunoglobulin G from maternal to fetal circulation.
Key findingsM281 significantly inhibits the maternal-to-fetal transfer of a representativeimmuoglobulin G molecule (adalimumab) in the ex vivo dually perfused humanplacental lobule model. However, M281 itself shows insignificant transfer frommaternal to fetal circulation.
What does this add to what is known?M281, a novel anti-FcRn antibody, may reduce the transfer of pathogenicimmunoglobulin G frommaternal to fetal circulation. These data support furtherinvestigation of M281 in the management of alloimmune or autoimmune dis-eases of the fetus and newborn.
ajog.org OBSTETRICS Original Research
antipyrine, phenacetin, and methanolwere purchased from Sigma-Aldrich (StLouis, MO). Gibco M199 media wasobtained from ThermoFisher Scientific(Waltham, MA).
Clinical materialPlacentas were collected immediatelyfollowing cesarean-sectioned abdom-inal deliveries from the labor anddelivery ward of the John Sealy Hos-pital, the teaching hospital of theUniversity of Texas Medical Branch(Galveston, TX) according to a pro-tocol approved by the institutionalreview board. Only placentas deter-mined by macroscopic examination tobe of normal morphology and fromuncomplicated term (38e40 weeks)singleton pregnancies were includedto the study. Placentas from womenwith multiple gestation, hypertension,evidence of infection, systemic dis-ease, drug or alcohol abuse, intra-uterine growth restriction, and knownfetal congenital abnormalities wereexcluded.
FcRn receptor occupancy assayA receptor occupancy assay (detailedmethods in Supplementary Material)was used to determine the concentrationand time required for M281 to fullyoccupy FcRn in primary human villoustrophoblasts (HVTs). M281 was testedover a range of concentrations
(0.015e5.0 mg/mL) and incubationtimes (5e120 minutes). Receptor occu-pancy was assessed as the percentage ofunoccupied (free) FcRn per cell afterincubation with unlabeled M281 forvarious periods of time. Briefly, primaryHVT monolayers were incubated withmedia alone, M281, or isotype-matched(IgG1) control antibody (SouthernBiotech, Birmingham, AL) for the indi-cated times. At each time point, cellswere detached, subjected to ice-coldfixation, and permeabilized at pH 7.4(Cytofix/Cytoperm; BD Biosciences, SanJose, CA) and then incubated for 30minutes on ice in the dark with a VT645-labeled M281 for binding to cell-associated, unoccupied FcRn. Cellswere washed in ice-cold buffer andanalyzed for geometric mean fluores-cence index of cell-associated VT645-labeled M281. M281 label in cells incu-bated with media alone represented themeasure of 100% unoccupied receptors.Full FcRn saturation was defined as<10% unoccupied receptors.
Placental perfusion studiesThe transfer of test compounds M281and adalimumab from the maternal-to-fetal circulation was studied usingthe ex vivo technique of dual perfusionof placental lobule as previouslydescribed by Nanovskaya et al.8-10
Briefly, each placenta was examinedfor tears, and 2 chorionic vessels (1
MAY 2019 Ameri
artery and 1 vein) supplying a singleintact peripheral cotyledon were can-nulated with 3F and 5F umbilicalcatheters, respectively. The cotyledonwas trimmed and placed in the perfu-sion chamber with the maternal sur-face upward. The intervillous space onthe maternal side was perfused by 2catheters piercing the basal plate. Theflow rate of medium in the fetal andmaternal circuits was maintained at 3.0and 12 mL/min, respectively. Thematernal perfusate was equilibratedwith a gas mixture made of 95% oxy-gen/5% carbon dioxide and the fetalperfusate with a mixture of 95% ni-trogen/5% carbon dioxide.
Each placental cotyledonwas perfusedfor an initial period of 1 hour in theabsence of test compounds (controlperiod) to evaluate the physical integrityof the tissue. During the control period,the perfusion system was used in open-open configuration (ie, without recir-culation of the perfusate). The perfusionwas terminated, and experiment was notinitiated if 1 or more of the followingcriteria were observed during the controlperiod: fetal volume loss of >2 mL/hand/or a difference between partialpressure of oxygen in fetal vein and ar-tery < 60 mm Hg.
Following the control period,maternal and fetal perfusates werereplaced with fresh medium contain-ing 3 mg/mL of bovine serum albu-min. The experimental period wasperformed using closed-closed config-uration of the system (ie, with recir-culation of the perfusates). Theexperimental period was initiated afterthe addition to the maternal reservoirof tests substances. The nonionizable,lipophilic marker compound antipy-rine (100 mg/mL) was cotransfusedwith test substance(s) to assure that allstudies maintained an adequate level ofperfusion overlap (ie, transfer of anti-pyrine to the fetal circuit within 120minutes) was >35%.11,12
In a first set of experiments, theextent of M281 transfer (concentra-tions between 300 and 20,000 mg/mL)across dually perfused humanplacental lobule was carried out for 4or 6 hours. In a second set of
can Journal of Obstetrics & Gynecology 498.e2

FIGURE 1Rapid uptake and saturation of FcRn by M281
FcRn saturation is indicated by a decrease in unoccupied receptors detectable following cell per-meabilization and incubation with fluor-labeled M281. Primary HVTs were incubated for differentperiods of time with various concentrations of unlabeled M281 or isotype-matched control antibody.At each time point, cells were detached, washed, fixed/permeabilized, and incubated with VT645-labeled M281. Flow cytometry was used to quantitate cell-associated mean fluorescence index.Values are mean � standard deviation, representative graph of n ¼ 2 experiments.HVT, human villous trophoblast.
Roy et al. M281 inhibits IgG transplacental transfer. Am J Obstet Gynecol 2019.
Original Research OBSTETRICS ajog.org
experiments, the extent of trans-placental transfer of adalimumab (270mg/mL) during 6 hours of perfusion13
was established. A third set of experi-ments was then performed wherein theinhibitory effect of M281 on thetransplacental transfer of adalimumab(270 mg/mL) was studied. In theseexperiments, M281 concentrations of10 and 300 mg/mL were investigated.These concentrations of M281 repre-sent serum levels of M281 observed inthe phase 1 study of M281.7
Samples from maternal artery andfetal vein (in 0.5 mL aliquots) were takenat 0, 30, 60, 120, 180, 240, 270, 300, 330,and 360 minutes during the experi-mental period and frozen ate80�C untilanalysis.
Sample and data analysisQuantitation of the antipyrineConcentrations of antipyrine inmaternal and fetal aliquots weremeasured using a modified high-performance liquid chromatography(HPLC) method previously described byMorck et al.14 Briefly, protein wasprecipitated by the addition of 200 mL ofice-cold acetonitrile containing 10 mL/mL of internal standard phenacetin toeach 200 mL sample. Samples werecentrifuged at 8000 rpm, and superna-tants were run on an Agilent 1200 HPLCsystem equipped with a G1315D DADdetector (Agilent Technologies, SantaClara, CA).
Antipyrine was analyzed using anHPLC method with a lower limit ofquantification of 5 mg/mL. The HPLCanalysis was performed at room tem-perature (22e25�C) using a reverse-phase, C18-based column (WatersAtlantis T3, Atlantis T3 Column, 100Å,3 mm, 3 mm � 150 mm [WatersCorporation, Milford, MA]) fitted witha guard cartridge (Waters T3, 3 mm,2.1 mm � 150 mm [Waters Corpora-tion]). The samples were run with alinear gradient ranging from 25% to95% methanol water over 14 minutesat a flow rate of 0.3 mL/min; the in-jection volume was 10 mL and detec-tion was performed using absorbanceat 260 nm.
498.e3 American Journal of Obstetrics & Gynecol
Quantitation of adalimumabThe concentrations of adalimumab in allmaternal and fetal sample aliquots weremeasured using a sandwich enzyme-linked immunosorbent assay (MomentaPharmaceuticals) with a lower limit ofquantitation of approximately 1 ng/mL.Briefly, 96-well plates were coated withrecombinant human tumor necrosis fac-tor alpha overnight, followed by incuba-tion with adalimumab-containingsamples and standards at room tempera-ture. Adalimumab was detected by acolorimetric method using peroxidase-conjugated donkey antihuman IgG sec-ondary antibody in the presence of chro-mogenic substrate TMB (ThermoFisherScientific, Waltham, MA), which allowedan absorbance readout at 450 nm. Testsubstance levels were interpolated fromthe calibration standards plotted using a4-parameter logistic curve fit.
ogy MAY 2019
Quantitation of M281M281 concentrations in all the maternaland fetal perfusate sample aliquots weredetermined using a Meso Scale Discoveryelectrochemiluminescence assay (Bio-Agilytix, Durham, NC) with a lower limitof quantification of 5 ng/mL. Briefly,plates coated with a mouse anti-M281idiotype capture antibody and blockedwith enzyme-linked immunosorbentassay blocking buffer E104 (Bethyl Lab-oratories, Montgomery, TX) were incu-bated with test samples for 1 hour atroom temperature. After washing, plateswere incubated for 1 hour with a secondbiotinylated mouse anti-M281 idiotypedetection antibody, followed by detectionwith Sulfo-Tag Streptavidin, and analyzedon aMeso QuickPlex SQ 120 (Meso ScaleDiscovery, Rockville, MD). Data wereanalyzed using MSD Workbench 4.0(Meso Scale Discovery).
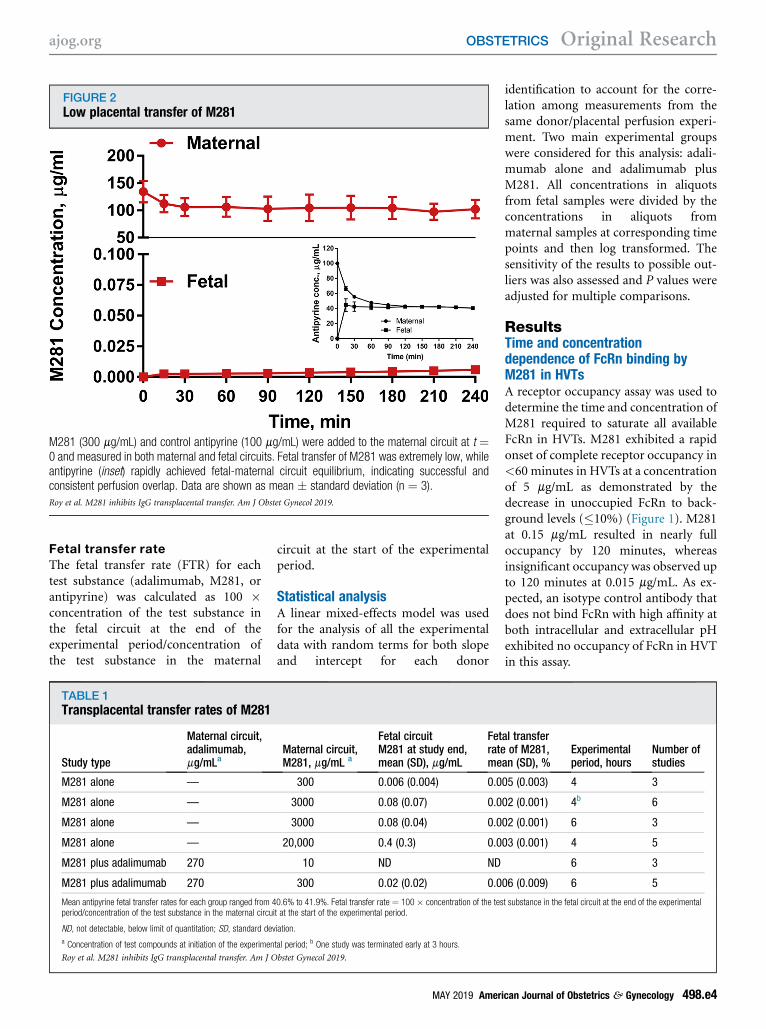
FIGURE 2Low placental transfer of M281
M281 (300 mg/mL) and control antipyrine (100 mg/mL) were added to the maternal circuit at t ¼0 and measured in both maternal and fetal circuits. Fetal transfer of M281 was extremely low, whileantipyrine (inset) rapidly achieved fetal-maternal circuit equilibrium, indicating successful andconsistent perfusion overlap. Data are shown as mean � standard deviation (n ¼ 3).
Roy et al. M281 inhibits IgG transplacental transfer. Am J Obstet Gynecol 2019.
ajog.org OBSTETRICS Original Research
Fetal transfer rateThe fetal transfer rate (FTR) for eachtest substance (adalimumab, M281, orantipyrine) was calculated as 100 �concentration of the test substance inthe fetal circuit at the end of theexperimental period/concentration ofthe test substance in the maternal
TABLE 1Transplacental transfer rates of M281
Study type
Maternal circuit,adalimumab,mg/mLa
M281 alone —
M281 alone —
M281 alone —
M281 alone —
M281 plus adalimumab 270
M281 plus adalimumab 270
Mean antipyrine fetal transfer rates for each group ranged from 4period/concentration of the test substance in the maternal circu
ND, not detectable, below limit of quantitation; SD, standard dev
a Concentration of test compounds at initiation of the experimen
Roy et al. M281 inhibits IgG transplacental transfer. Am J O
circuit at the start of the experimentalperiod.
Statistical analysisA linear mixed-effects model was usedfor the analysis of all the experimentaldata with random terms for both slopeand intercept for each donor
Maternal circuit,M281, mg/mL a
Fetal circuitM281 at study end,mean (SD), mg/mL
Fetrateme
300 0.006 (0.004) 0.0
3000 0.08 (0.07) 0.0
3000 0.08 (0.04) 0.0
20,000 0.4 (0.3) 0.0
10 ND ND
300 0.02 (0.02) 0.0
0.6% to 41.9%. Fetal transfer rate ¼ 100� concentration of the tesit at the start of the experimental period.
iation.
tal period; b One study was terminated early at 3 hours.
bstet Gynecol 2019.
MAY 2019 Ameri
identification to account for the corre-lation among measurements from thesame donor/placental perfusion experi-ment. Two main experimental groupswere considered for this analysis: adali-mumab alone and adalimumab plusM281. All concentrations in aliquotsfrom fetal samples were divided by theconcentrations in aliquots frommaternal samples at corresponding timepoints and then log transformed. Thesensitivity of the results to possible out-liers was also assessed and P values wereadjusted for multiple comparisons.
ResultsTime and concentrationdependence of FcRn binding byM281 in HVTsA receptor occupancy assay was used todetermine the time and concentration ofM281 required to saturate all availableFcRn in HVTs. M281 exhibited a rapidonset of complete receptor occupancy in<60 minutes in HVTs at a concentrationof 5 mg/mL as demonstrated by thedecrease in unoccupied FcRn to back-ground levels (�10%) (Figure 1). M281at 0.15 mg/mL resulted in nearly fulloccupancy by 120 minutes, whereasinsignificant occupancy was observed upto 120 minutes at 0.015 mg/mL. As ex-pected, an isotype control antibody thatdoes not bind FcRn with high affinity atboth intracellular and extracellular pHexhibited no occupancy of FcRn in HVTin this assay.
al transferof M281,
an (SD), %Experimentalperiod, hours
Number ofstudies
05 (0.003) 4 3
02 (0.001) 4b 6
02 (0.001) 6 3
03 (0.001) 4 5
6 3
06 (0.009) 6 5
t substance in the fetal circuit at the end of the experimental
can Journal of Obstetrics & Gynecology 498.e4

FIGURE 3Placental transfer of adalimumab
Adalimumab (270 mg/mL) and control antipyrine (100 mg/mL) were added to the maternal circuit att¼ 0 and measured in both maternal and fetal circuits during the experimental period. Fetal transferof adalimumab increased significantly after 60 minutes. Successful, consistent perfusion overlapwas achieved in these studies because antipyrine (inset) transfer rapidly reached equilibrium be-tween maternal and fetal circuits. Data are shown as mean � standard deviation (n ¼ 8).
Roy et al. M281 inhibits IgG transplacental transfer. Am J Obstet Gynecol 2019.
Original Research OBSTETRICS ajog.org
Transfer of control compound,antipyrine, across the duallyperfused human placental lobuleAntipyrine, a widely used controlmolecule in perfusion studies, is ex-pected to transfer rapidly and equili-brate between the fetal and maternalcircuits in a successful perfusion.11 Inall experiments reported here,maternal-fetal circuit equilibration wasachieved within the expected time-frame. The FTR of antipyrine coper-fused with M281 was 41% � 0.5%,with adalimumab, 42% � 2.7%, andwith a combination of M281 and ada-limumab, 43% � 2.8%, indicating asimilar degree of perfusion overlapamong different sets of experimentsand thus enabling comparability be-tween studies reported.
498.e5 American Journal of Obstetrics & Gynecol
Transfer of test compounds acrossthe dually perfused humanplacental lobuleVery low concentrations of M281 weredetected in the fetal circuit throughoutthe experimental period (Figure 2 andTable 1). The low amount of M281transferred to the fetal circuit increasedsteadily and in proportion with the con-centration added to the maternal circuit,suggesting transfer by a nonsaturableprocess. The average FTR of M281 overthe concentrations tested (300 mg/mL,3000 mg/mL, 20,000 mg/mL) ranged from0.002e0.006% (Table 1) indicated anextremely low transfer rate, even at thehighest concentration tested.The transfer of the representative IgG
(adalimumab) showed an initial declinein concentration in the maternal
ogy MAY 2019
circulation during the initial 30 minutes,which can be attributed to the distribu-tion of the adalimumab in the perfusedlobule. Adalimumab appeared in the fetalcircuit after 60 minutes, and its transferincreased substantially through the end ofthe experimental period (Figure 3). At theend of 6 hours of perfusion, the averageFTR of adalimumab was 0.23% � 0.21%(range, 0.05e 0.65%, n ¼ 8, Table 2).
The effect of M281 ontransplacental transfer ofadalimumabIn the presence of M281, the detect-able transfer of adalimumab across theplacental lobule was delayed (>120minutes vs >60 minutes), and fetaltransfer rates were decreased, irre-spective of the concentrations of M281tested (Figure 4 and Table 2). How-ever, the FTR of M281 was notaffected by the presence of adalimu-mab (Table 1).
CommentThe ability of M281 to inhibit IgG1transfer across the human placenta wasevaluated using the dual-perfusion termplacental lobule model under conditionsintended to represent the highest effi-ciency transfer of pathogenic IgG. Ahuman IgG1 monoclonal antibody,adalimumab, was used as a representa-tive IgG molecule. IgG1 and IgG3comprise the 2 subclasses of pathogenicIgG in the majority of alloimmune andautoimmune diseases of the fetus andnewborn, with IgG1 being the predom-inant subclass.13,15e18 IgG1 is also themost efficiently transferred IgG subclassin both human pregnancy and theplacental perfusion model.4,13 Becausethe transfer of IgG increases with theprogression of gestational age,4,5 we usedhuman term placentas representingthe period for the highest IgG transfer.Additionally, the adalimumab concen-tration in the maternal circuit iswithin the range of concentrationsobserved for pathogenic alloantibodiesand autoantibodies.19e22
The FTR of the representative IgG,adalimumab (0.23% � 0.21%), in theabsence of M281 was similar to previ-ously reported IgG transfer rates

TABLE 2M281 inhibition of IgG transfer from maternal to fetal circulation
Maternal circuitM281, mg/mLa
Maternal circuitadalimumab, mg/mLa
Fetal circuitadalimumab at studyend, mean (SD), mg/mL
Fetal transfer rateAdalimumab,mean (SD), % P valueb
Number ofstudies
Experimentalperiod, hours
0 270 0.50 (0.5) 0.23 (0.21) NA 8 6
10 270 0.12 (0.02) 0.07 (0.01) < .001 3 6
300 270 0.12 (0.01) 0.06 (0.01) < .001 5 6
Mean antipyrine fetal transfer rate for these studies was 41.7%� 2.7% for adalimumab alone and 43.8%� 4.2% for all adalimumab plus M281 studies. Fetal transfer rate¼ 100� concentration ofthe test substance in the fetal circuit at the end of the experimental period/concentration of the test substance in the maternal circuit at the start of the experimental period.
NA, not applicable.
a Concentration of test compounds in the maternal perfusate at initiation of the experimental period; b P values were calculated compared with no M281 using a linear mixed-effects model withrandom slope and intercept.
Roy et al. M281 inhibits IgG transplacental transfer. Am J Obstet Gynecol 2019.
ajog.org OBSTETRICS Original Research
(0.08e0.5%) in this model.13,23e26 Thehigh variability in the extent of adali-mumab transfer across the placenta
FIGURE 4Placental transfer of adalimumab is in
Adalimumab (270 mg/mL), M281 (10 mg/mL, n ¼(100 mg/mL) were added to the maternal circuit atcircuits over the experimental period. M281, irrdecreased adalimumab transfer compared with itsare shown as mean � standard deviation.
Roy et al. M281 inhibits IgG transplacental transfer. Am J Obst
lobule may be explained in part by fac-tors such as individual variability in IgGuptake by pinocytosis, expression of
hibited by M281
3, or 300 mg/mL, n ¼ 5) and control antipyrinet ¼ 0 and measured in both maternal and fetalespective of concentration tested, significantlytransfer in the absence of M281 (Figure 3). Data
et Gynecol 2019.
MAY 2019 Ameri
IgG-binding Fc gamma receptors, orvesicular trafficking. No association wasfound between FcRn expression andadalimumab FTR in these studies (datanot shown).
In the presence of M281, the adali-mumab transfer rate decreased byapproximately 3- to 4-fold (Table 2) andremained at 0.06e0.07%, irrespective ofthe M281 concentration tested (10 or300 mg/mL). It should be noted thatthe diminished transfer rate of adali-mumab in the presence of M281 issimilar to the previously reportedtransfer rate for immunoglobulin A,26
an immunoglobulin isotype known totransfer extremely poorly across thehuman placenta in pregnancy. Further-more, IVIg, which at high concentra-tions acts as a competitive inhibitor atthe FcRn IgG binding site, was used as apositive control. The inhibitory effect of6700 mg/mL of IVIg on adalimumabtransfer to the fetal circuit (FTR 0.07%�0.03%; Supplemental Table 1) wassimilar to the inhibitory effect of M281at 10 ug/mL (FTR 0.07% � 0.01%,Table 2).
These data suggest that the transfer ofIgG in the presence of M281 may benegligible in vivo. Both 10 and 300 mg/mL of M281 resulted in similar de-creases in adalimumab transfer rates,suggesting that the inhibitory activity ofM281 on IgG transport was saturated.These ex vivo model results are consis-tent with the rapid uptake and receptoroccupancy of FcRn by M281 in HVTs atconcentrations as low as 5 mg/mL.
can Journal of Obstetrics & Gynecology 498.e6

Original Research OBSTETRICS ajog.org
Because concentrations of M281 greaterthan 10 mg/mL were maintained alongwith FcRn receptor occupancy withweekly 30 mg/kg dosing of healthyvolunteers in the phase 1 study, a sus-tained blockade of IgG transfer acrossthe human placenta may be achievablein clinical studies.7
The transfer rate of M281 itself acrossthe perfused placenta lobule was 0.002%� 0.002%, which is nearly 100-foldlower than the transfer rate for therepresentative IgG, adalimumab alone.This low transfer rate of M281 is unlikelyto maintain active drug concentrationsin the fetal circulation in vivo becauseconcentrations in the fetal circuit weresubstantially below active M281 con-centrations observed in HVTs in vitro.
The extremely poor placental transferof M281 may be explained by the high-affinity binding of M281 to FcRn atboth intracellular and extracellular pH,which prevents its release from FcRnduring any step of the transfer process.6
The low transfer of M281 across thehuman placenta is significant becausethe potential for a low or negligentexposure of the developing fetus andneonate is an important safety consid-eration in the future clinical develop-ment of M281.
The results of this investigationdemonstrate that M281, a direct andpotent inhibitor of FcRn, decreasedtransfer of IgG across term placenta.These data together with the rapidFcRn occupancy and reduction incirculating IgG observed on M281administration in nonpregnant healthyvolunteers in the phase 1 study7 and inchronic, reproductive, and immuno-logical toxicology studies in nonhumanprimates (data not shown) suggest thatmaternal administration of M281 couldpotentially lower alloantibody or auto-antibody titers and prevent their pas-sage into the fetus to potentially delay,minimize, or prevent fetal and neonataldisease development.
While M281 is expected to inhibittransplacental transfer and increasematernal clearance of both pathogenicand beneficial IgG, a single maternalIVIg infusion just prior to birth wouldprovide passive immunity to the neonate
498.e7 American Journal of Obstetrics & Gynecol
and recovery of maternal circulating IgGin clinical settings. A favorable risk-benefit may be achievable for initialevaluation of M281 safety and efficacy inan indication such as severe early-onsetantenatal hemolytic disease of the fetus,an indication with predictably pooroutcomes, noninvasive disease moni-toring, and potential for standard-of-care rescue therapy.27-29 Other poten-tial indications include pregnancies witha history of autoimmune congenitalheart block,3 fetal neonatal alloimmunethrombocytopenia with intracranialhemorrhage,30 or neonatalthyrotoxicosis.31
In summary, these human placentalperfusion studies together with theadditional M281 nonclinical and clinicalstudies support further clinical researchto evaluate the safety and efficacy ofM281 in severe pregnancy-associatedalloimmune and autoimmune diseasesof the fetus and newborn. n
AcknowledgmentsWe thank Dr Victor Farutin for guidance in sta-tistical analysis, Drs Anthony M. Manning andSantiago Arroyo for their review and helpfuldiscussion and guidance for this study, andAgnes Costello for help in preparation of thismanuscript. Momenta Pharmaceuticalscontributed to the study design, research, datainterpretation, and the writing, review, andapproval of the manuscript. We also thank Ste-phanie E. Tedford, PhD, and Lamara D. Shrode,PhD, ISMPP, CMPP�, of J. B. Ashtin, whoprovided editorial support during the preparationof the manuscript. Drs Roy and Nanovskayawere involved in the concept/design of the studyand the data acquisition and interpretation.S. Patrikeeva and Dr Schaeck were involved inthe data acquisition. Dr Choudhury, E. Cochran,and V. Parge were involved in the data acquisi-tion and interpretation. J. Guess was involved inthe statistical analysis. Drs Ahmedand Lingwereinvolved in the concept/design of the study anddata interpretation. All authors critically reviewedthe manuscript and provided final approval forsubmission. All authors agree to be accountablefor all aspects of thework, ensuring the accuracyand integrity of the publication.
Data requests from any qualified researcherswho engage in rigorous, independent scientificresearch will be considered if the trials are notpart of an ongoing or planned regulatory sub-mission (this includes requests for data on unli-censed products and indications). Data will beprovided following review and approval of aresearch proposal, statistical analysis plan,confirmation that the requested data can be
ogy MAY 2019
shared under applicable privacy laws, andexecution of a data-sharing agreement. Datarequests can be submitted at any time, and thedata will be accessible for 12 months, withpossible extensions considered. Requests canbe sent to [email protected].
References
1. Hadley A, Soothhill P. Alloimmune disordersof pregnancy: anaemia, thrombocytopenia andneutropenia in the fetus and newborn. Cam-bridge, United Kingdom: Cambridge UniversityPress; 2002.2. Bordachar P, Zachary W, Ploux S,Labrousse L, Haissaguerre M, Thambo JB.Pathophysiology, clinical course, and manage-ment of congenital complete atrioventricularblock. Heart Rhythm 2013;10:760–6.3. Izmirly PM, Buyon JP, Saxena A. Neonatallupus: advances in understanding pathogenesisand identifying treatments of cardiac disease.Curr Opin Rheumatol 2012;24:466–72.4. Palmeira P, Quinello C, Silveira-Lessa AL,Zago CA, Carneiro-Sampaio M. IgG placentaltransfer in healthy and pathological pregnancies.Clin Dev Immunol 2012;2012:985646.5. Palfi M, Hilden JO, Gottvall T, Selbing A.Placental transport of maternal immunoglobulinG in pregnancies at risk of Rh (D) hemolyticdisease of the newborn. Am J Reprod Immunol1998;39:323–8.6. Roopenian DC, Akilesh S. FcRn: the neonatalFc receptor comes of age. Nat Rev Immunol2007;7:715–25.7. Ling LE, Hillson JL, Tiessen RG, et al. M281,an anti-FcRn antibody: pharmacodynamics,pharmacokinetics, and safety across the fullrange of IgG reduction in a first-in-human study.Clin Pharmacol Ther 2018;105:1031–9.8. Nanovskaya T, Deshmukh S, Brooks M,Ahmed MS. Transplacental transfer and meta-bolism of buprenorphine. J Pharmacol Exp Ther2002;300:26–33.9. Nanovskaya T, Patrikeeva S, Zhan Y,Fokina V, Hankins GD, Ahmed MS. Trans-placental transfer of vancomycin and telavancin.Am J Obstet Gynecol 2012;207:331.e1–6.10. Nanovskaya TN, Patrikeeva SL, Paul J,Costantine MM, Hankins GD, Ahmed MS.Transplacental transfer and distribution of pra-vastatin. Am J Obstet Gynecol 2013;209:373.e1–5.11. Mathiesen L,Mose T,Morck TJ, et al. Qualityassessment of a placental perfusion protocol.Reprod Toxicol 2010;30:138–46.12. Schneider H. Techniques: in vitro perfusionof human placenta. In: Sastry BVR, ed. Placentaltoxicology. Boca Raton (FL): CRC Press; 1995.13. Malek A. Ex vivo human placenta models:transport of immunoglobulin G and its sub-classes. Vaccine 2003;21:3362–4.14. Morck TJ, Sorda G, Bechi N, et al. Placentaltransport and in vitro effects of Bisphenol A.Reprod Toxicol 2010;30:131–7.15. Frohlich E, Wahl R. Thyroid autoimmunity:role of anti-thyroid antibodies in thyroid and extra-thyroidal diseases. Front Immunol 2017;8:521.

ajog.org OBSTETRICS Original Research
16. Pollock JM, Bowman JM. Anti-Rh(D) IgGsubclasses and severity of Rh hemolytic diseaseof the newborn. Vox Sang 1990;59:176–9.17. Sonneveld ME, Natunen S, Sainio S, et al.Glycosylation pattern of anti-platelet IgG is sta-ble during pregnancy and predicts clinicaloutcome in alloimmune thrombocytopenia. Br JHaematol 2016;174:310–20.18. Tseng CE, Caldwell K, Feit S, Chan EK,Buyon JP. Subclass distribution of maternal andneonatal anti-Ro(SSA) and La(SSB) antibodies incongenital heart block. J Rheumatol 1996;23:925–32.19. Garberg H, Jonsson R, Brokstad KA. Theserological pattern of autoantibodies to theRo52, Ro60, and La48 autoantigens in primarySjogren’s syndrome patients and healthy con-trols. Scand J Rheumatol 2005;34:49–55.20. Hilden JO, Backteman K, Nilsson J,Ernerudh J. Flow-cytometric quantitation of anti-D antibodies. Vox Sang 1997;72:172–6.21. Nakatake N, Sanders J, Richards T, et al.Estimation of serum TSH receptor autoantibodyconcentration and affinity. Thyroid 2006;16:1077–84.22. Tunks RD, Clowse ME, Miller SG,Brancazio LR, Barker PC. Maternal autoanti-body levels in congenital heart block and po-tential prophylaxis with antiinflammatory agents.Am J Obstet Gynecol 2013;208:64.e1–7.23. Morgan CL, Cannell GR, Addison RS,Minchinton RM. The effect of intravenous
immunoglobulin on placental transfer of aplatelet-specific antibody: anti-P1A1. TransfusMed 1991;1:209–16.24. Porter C, Armstrong-Fisher S, Kopotsha T,et al. Certolizumab pegol does not bind theneonatal Fc receptor (FcRn): consequences forFcRn-mediated in vitro transcytosis and ex vivohuman placental transfer. J Reprod Immunol2016;116:7–12.25. Urbaniak SJ, Duncan JI, Armstrong-Fisher SS, AbramovichDR, Page KR. Transfer ofanti-D antibodies across the isolated perfusedhuman placental lobule and inhibition by high-dose intravenous immunoglobulin: a possiblemechanism of action. Br J Haematol 1997;96:186–93.26. Malek A, Sager R, Lang AB, Schneider H.Protein transport across the in vitro perfusedhuman placenta. Am J Reprod Immunol1997;38:263–71.27. Lindenburg IT, Van Kamp IL, Van Zwet EW,Middeldorp JM, Klumper FJ, Oepkes D.Increased perinatal loss after intrauterine trans-fusion for alloimmune anaemia before 20 weeksof gestation. BJOG 2013;120:847–52.28. LobatoG, Soncini CS. Relationship betweenobstetric history and Rh(D) alloimmunizationseverity. Arch Gynecol Obstet 2008;277:245–8.29. Moise KJ Jr, Argoti PS. Management andprevention of red cell alloimmunization inpregnancy: a systematic review. Obstet Gynecol2012;120:1132–9.
MAY 2019 Ameri
30. Bussel JB, Berkowitz RL, Hung C, et al.Intracranial hemorrhage in alloimmune throm-bocytopenia: stratified management to preventrecurrence in the subsequent affected fetus. AmJ Obstet Gynecol 2010;203:135.e1–14.31. Ogilvy-Stuart AL. Neonatal thyroid disor-ders. Arch Dis Child Fetal Neonatal Ed 2002;87:F165–71.
Author and article informationFrom Momenta Pharmaceuticals, Cambridge, MA
(Authors Roy, Cochran, Parge, Guess, Schaeck,
Choudhury, and Ling); and the Maternal-Fetal Pharma-
cology and Bio-Development Laboratories, Department of
Obstetrics and Gynecology, University of Texas Medical
Branch, Galveston, TX (Authors Nanovskaya, Patrikeeva,
and Ahmed).
Received Nov. 10, 2018; revised Feb. 22, 2019;
accepted Feb. 27, 2019.
This work was supported by Momenta Pharmaceuti-
cals, Inc.
Authors Nanovskaya and Ahmed have received grant/
research support from the Eunice Kennedy Shriver Na-
tional Institute of Child Health and Human Development.
Authors Roy, Cochran, Parge, Guess, Schaeck, Choud-
hury, and Ling are or were full-time employees of
Momenta Pharmaceuticals, Inc and may own company
stock and/or stock options. S. Patrikeeva reports no
conflict of interest.
Corresponding author: Leona E. Ling, PhD. lling@
momentapharma.com
can Journal of Obstetrics & Gynecology 498.e8

Original Research OBSTETRICS ajog.org
SupplementaryMaterialsFcRn receptor occupancy assay
Primary human villous trophoblasts(HVTs) (ScienCell, Carlsbad, CA) werecultured in complete trophoblast media(ScienCell) on plates coated with poly-L-lysine (ScienCell). For receptor oc-cupancy studies, HVTs were seeded inpoly-L-lysine-coated, 6-well plates andcultured until 80% confluence. Mediaalone, M281, or an immunoglobulinG1 isotype-matched control antibody
SUPPLEMENTAL TABLE 1IVIg inhibition of IgG transfer from ma
Maternalcircuit IVIg,mg/mL a
Maternal circuitadalimumab, mg/mLa
Fetadaend
6700 270 0.1
Mean antipyrine fetal transfer rate for these studies was 41.7%�the test substance in the fetal circuit at the end of the experime
a Concentration of test articles in the maternal perfusate at therandom slope and intercept; c One study was terminated early
Roy et al. M281 inhibits IgG transplacental transfer. Am J O
498.e9 American Journal of Obstetrics & Gynecol
(Southern Biotech, Birmingham, AL) introphoblast media media alone wasadded to HVT at time 0 and incubatedat 37�C in a tissue culture incubator forvarious times. At indicated times, plateswere placed on ice. The media wasaspirated, and cell monolayers wererinsed once with ice-cold Dulbecco’sphosphate-buffered saline (MilliporeSigma, St Louis, MO) and then de-tached with room-temperatureHyQTase (ScienCell). After centrifuga-tion at 400 � g, cells were resuspendedin Cytofix/Cytoperm solution (BD
ternal to fetal circulation
al circuitlimumab at study, mean (SD), mg/mL
Fetal transferrate adalimumab,mean (SD), % P
2 (0.05) 0.07 (0.03) <
2.7% for adalimumab alone and 43.8%� 4.2% for all adalimumab pluntal period/concentration of the test substance in the maternal circuit
initiation of the experimental period; b P values were calculated compat 5.5 hours.
bstet Gynecol 2019.
ogy MAY 2019
Biosciences, San Jose, CA) at 4�C for 20minutes, washed twice with ice-cold1 � Perm buffer (BD Biosciences),and resuspended in Perm buffer with10% fetal bovine serum (ScienCell)with 7.5 mg/mL VT645-labeled M281for 30 minutes. Following incubation,cells were washed twice with ice-coldPerm buffer, resuspended in FACSbuffer (BD Biosciences), and filteredprior to FACS analysis (FACSCanto, BDBiosciences).
Roy. M281 inhibits IgG transplacentaltransfer. Am J Obstet Gynecol 2019.
valuebNumber ofstudies
Experi-mentalperiod, hours
.001 5 6c
s M281 studies. Fetal transfer rate¼ 100� concentration ofat the start of the experimental period.
ared with no M281 using a linear mixed-effects model with