Opportunistic Mycoses 06-07
35
OPPORTUNISTIC MYCOSES
-
Upload
api-3699361 -
Category
Documents
-
view
129 -
download
7
Transcript of Opportunistic Mycoses 06-07

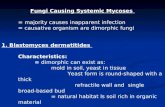
OPPORTUNISTIC MYCOSES

OPPORTUNISTIC MYCOSESGeneral features
CAUSATIVE AGENTSSaprophyte in nature/found in normal flora
HOST Immunosupressed /other risk factors

• Candidiasis• Cryptococcosis (discussed)• Aspergillosis• Zygomycosis• Other: Trichosporonosis, fusariosis,
penicillosis……***ANY fungus found in nature may give
rise to opportunistic mycoses ***
OPPORTUNISTIC MYCOSES

• Most commonly encountered opportunistic mycoses worldwide
• Cellular immunity protects against mucocutaneous candidiasis, neutrophiles protect against invasive candidiasis
• Endogenous infection. • Etiology: Candida spp. Most common:
1. C. albicans 2. C. tropicalis 3. C. glabrata
CANDIDIASIS

Candida
MORPHOLOGICAL FEATURES
• Micr. Budding yeast cells Pseudohyphae, true hyphae
• Macr. Creamy yeast colonies (SDA)• Germ tube (C. albicans, C.
dubliniensis)• Chlamydospore (C. albicans, C.
dubliniensis)• Identification Germ tube, fermentation

Macroscopic Morphology Yeast colony. Sabouraud Dextrose agar (DSA)
Candida albicans

Candida albicans Microscopic Morphology
Yeast cells and pseudohyphae in material from the oral cavity, KOH
preparation, phase-contrast microscopy

Candida
PATHOGENICITY • Attachment (Germ tube is more
adhesive than yeast cell)• Adherence to plastic surfaces
(catheter, prosthetic valve..)• Protease• Phospholipase

CANDIDIASISRisk factors
• Physiological. Pregnancy, elderly, infancy
• Traumatic. Burn, infection• • Hematological. Cellular immune deficiency, AIDS, chronic
granulamatous disease, aplastic anemia, leukemia, lymphoma...
• Endocrinological. DM
• Iatrogenic. Oral contraceptives, antibiotics, steroid, chemotherapy, catheter...

CANDIDIASISClinical manifestations-I
1. CUTANEOUS and SUBCUTANEOUS• Oral• Vaginal • Onychomycosis• Dermatitis• Diaper rash

Candida albicans Clinical Presentation
The white material are masses of the yeast

The presence of satellite lesions help makes the
diagnosis of diaper rash.

CANDIDIASISClinical manifestations-II
• Esophagitis• Pulmonary inf.• Cystitis• Pyelonephritis• Endocarditis• Myocarditis
• Peritonitis• Hepatosplenic• Endophthalmitis • Osteomyelitis• Menengitis• Skin lesions
2. SYSTEMIC

CANDIDIASISClinical manifestations-III
3. CHRONIC MUCOCUTANEOUS• Candida inf. of skin and mucous
membranes • Verrucose lesions• Impaired cellular immunit• Hypoparathyroidism, iron
deficiency

Candida albicans Granulomatous lesions involving the hands.

CANDIDIASISDiagnosis
• Direct micr.ic examination Yeast cells, pseudohyphae, true hyphae• Culture SDA, routine bacteriological media• Serology Detection of mannan antigen (ELISA, RIA, IF, latex agglutination)

CANDIDIASISTreatment
• CUTANEOUSTopical antifungal: Ketoconazole, miconazole, nystatin• SYSTEMIC Amphotericin B Fluconazole, itraconazole• CHRONIC MUCOCUTANEOUSAmphotericin BFluconazole, itraconazoleTransfer factor

Causative Agent• Aspergillus fumigatus• Aspergillus flavus• Aspergillus niger- mostly local infection;
otomycosis• Are molds that have septate hyphae with V-
shaped branches (Fruiting body of Aspergillus)
Source of infection• Widely distributed in environment• Transmitted by air-borne light spores• High environmental load is associated with sick
building syndrome & contaminated AC system
Aspergillosis
Systemic infection

Aspergillus

Pathogenesis & Clinical featuresAspergillus can colonize and invade:• Lungs • Wounds, burns • Cornea• External ear • Paranasal sinuses
Aspergillosis

In lungs can cause:a) Hypersensitivity Reaction: Spores colonise RT without invasion and lead toallergic asthma, rhinitis, bronchopulmonary aspergillosis
b) Aspergilloma (fungus ball): the spores colonise paranasal sinuses or a pre-existing cavity in lung (TB cavity)The radiological appearance may be similar to malignancy.
c) Invasive AspergillosisIn immunocompromised can invade lungs causing hemoptysis & granuloma and disseminate to other organs Fatality rate 100% if not diagnosed and treated promptly.
Aspergillosis

Lab DiagnosisSpecimens : sputum, BM aspirate, biopsyDirect Microscopy• Shows branching septate hyphaeCultures : Microscopy shows radiating chains of sporesSerology• In allergic condition: high levels of specific IgE• Galactomannan in invasive aspergillosisTreatment• Invasive aspergillosis
Amphotericin B• Allergic conditions
Steroids & antifungals
Aspergillosis

ZygomycosisMucormycosis
• Causative agents; saprophtic molds• Rhizopus, Mucor & Absidia• Have broad, aseptate hyphae• Have large no. of asexual spores inside a sporangium
• Risk factors Diabetic ketoacidosis, immunosuppression
• Pathogenesis Inhalation of sporangiospores
• Infected tissue vascular invasion, thrombus, infarct,

ZYGOMYCOSISClinical manifestations
I. RHINOCEREBRAL• Nose, paranasal sinuses, eye, brain and meninges are
involved• Orbital cellulitis II. THORACIC• Pulmonary lesions, parenchymal necrosisIII. LOCAL• Posttraumatic kidney inf.• Skin inf. following burn or surgery



ZYGOMYCOSIS Diagnosis
• Samples Sputum, BAL, biopsy of paranasal sinuses..
• Direct exam. Nonseptate, ribbon-like hyphae which branch at right angles, sporangium
• Culture SDA (cotton candy appearence)

Rhizopus

Diseases• Rhinocerebral zygomycosis
o Extensive cellulitis of nasal mucosa, paranasal sinuses, orbit & brain
o Rapidly fatal• Pulmonary & disseminated infectionsTreatment• Surgical debridement
• Amphotericin B
***High mortality rate
ZygomycosisMucormycosis

Fusariosis
• Fusarium species, have been increasingly recognized as lethal pathogens
• ~50 different species of the Fusarium • Only a few human pathogens• The skin and respiratory tract are the
primary portals of entry for Fusarium infection
• Fusarium spp. are angiotropic and angioinvasive molds that lead to hemorrhagic infarction, low tissue perfusion, and resultant tissue necrosis

Fusariosis
Infections in normal hosts• Are typically localized like skin, eye infections and
osteomyelitis • Frequently do not require systemic therapy
Infections in immunocompromised patients
Manifest in four major patterns: • Refractory PUO • Pulmonary infection or pneumonia • Disseminated infection• A variety of focal single-organ infections

• Fusarium is one of the most resistant fungi to the arsenal of modern antifungal agents
• The mainstay in the treatment is Ampho-B
• In vitro susceptibility of Fusarium spp. to Ampho-B is, at best, mediocre
Fusariosis

Invasion of the cornea by a Fusarium species

Endophthalmitis due to a Fusarium species

Macroscopic Morphology of Fusarium species