
Systemic mycoses - bpums.ac.ir
35
Systemic mycoses • True pathogenic fungi 1.Histoplasma 2.Coccidioides 3. Blastomyses 4. paracoccidiodes • Opportunistic fungi • 1. Candida 2.Aspergillus • 3. Zygomycet 4. cryptococcous: 1
Transcript of Systemic mycoses - bpums.ac.ir

Systemic mycoses
• True pathogenic fungi1.Histoplasma 2.Coccidioides3. Blastomyses 4. paracoccidiodes
• Opportunistic fungi• 1. Candida 2.Aspergillus• 3. Zygomycet 4. cryptococcous:
1

Cryptococcosis
• The causal organism: Cryptococcus• Basidiomycete• Sexual form is: Filobasidiella
• Pathogenesis: Inhalation of ?• Size ?• Natural reservoir ? Worldwide, Soil, Bird dropping
• Macr. Cramy, mucoid colonies (SDA)• Micr. Encapsulated yeast (India ink)
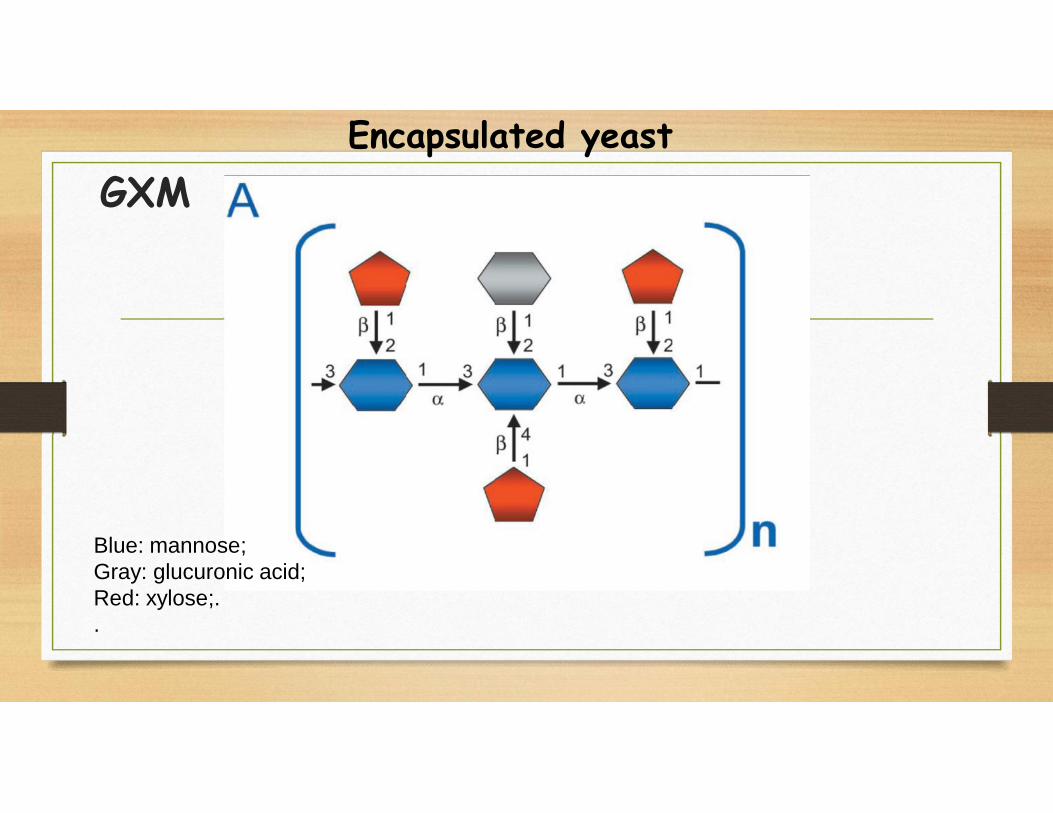
GXM
Blue: mannose;Gray: glucuronic acid;Red: xylose;..
Encapsulated yeast

GalXM
Blue: mannose;Red: xylose;Green: galactose.
Encapsulated yeastGalxm

MP: Mannoprotein.
These mannoproteins have been the focus of immunologic studies. Why?
Involved in the induction of cell-mediated immunity and cytokineproduction, both critical functions for clearing the fungus.
Encapsulated yeast

Subclassified into 5 serotypes and 2 varieties:
Five serotypes: A, B, C, D, AD
Serotypes A, D, AD var. neoformans
Serotypes B, C var. gattii
(Serotype A now classified as var. grubii)

• What are the sources of causative agents?
• Serotypes A and D: soil contaminated with pigeon or other bird droppings.
• var. neoformans in individuals with T- cell mediated immunological defects
• serotypes B and C: wood of eucalyptus trees.
• Environmental exposure appears to be the major risk factor for infection with C.neoformans var. gattii

Cryptococcosis: European blastomycosis, torulosis
• C. neoformans/C. gattii/albidus/laurentii
• How do we become sick from these yeasts?• Depends on three main factors:
• The state of the host defense mechanisms
• The virulence of the infecting strain
• The inoculum count
• Inhalation OR transmission OR inoculation

• After inhalation what happened?
• First line of defense:
• Nonspecific phagocytic effector cells phagocytosis the yeasts
• Processed antigen with class II and present it to CD4+ T cells
• Eliminate the infection
• By consequence a large inoculum can overcome this defense mechanism allowing fungalmultiplication and dissemination

Clinical manifestationsPulmonary cryptococcosis in immunocompetent persons
Up to 30% of patients develop no symptomsmay be presented by remainder
FeverCough sputum production chest painweight loss The most frequent radiological findings arenodular lesions

Pulmonary cryptococcosis in immunocompromised persons
Most patients develop symptoms
Chest radiographs reveal diffuse
Interstitial or alveolar infiltrates
High mortality have presented in up to 14% of AIDS patients with
pulmonary cryptococcosis

The most common clinical form
The most common disseminated form
The most common Life-threatening meningitis in AIDS
Neurotropism?
CNS Cryptoccosis

CNS Cryptococcosis
Meningitis (85%)
Meningoencephalitis
Cryptococcoma• A wide range of CNS symptoms can be present, headache and
fever (38-39 °C) being the most prominent
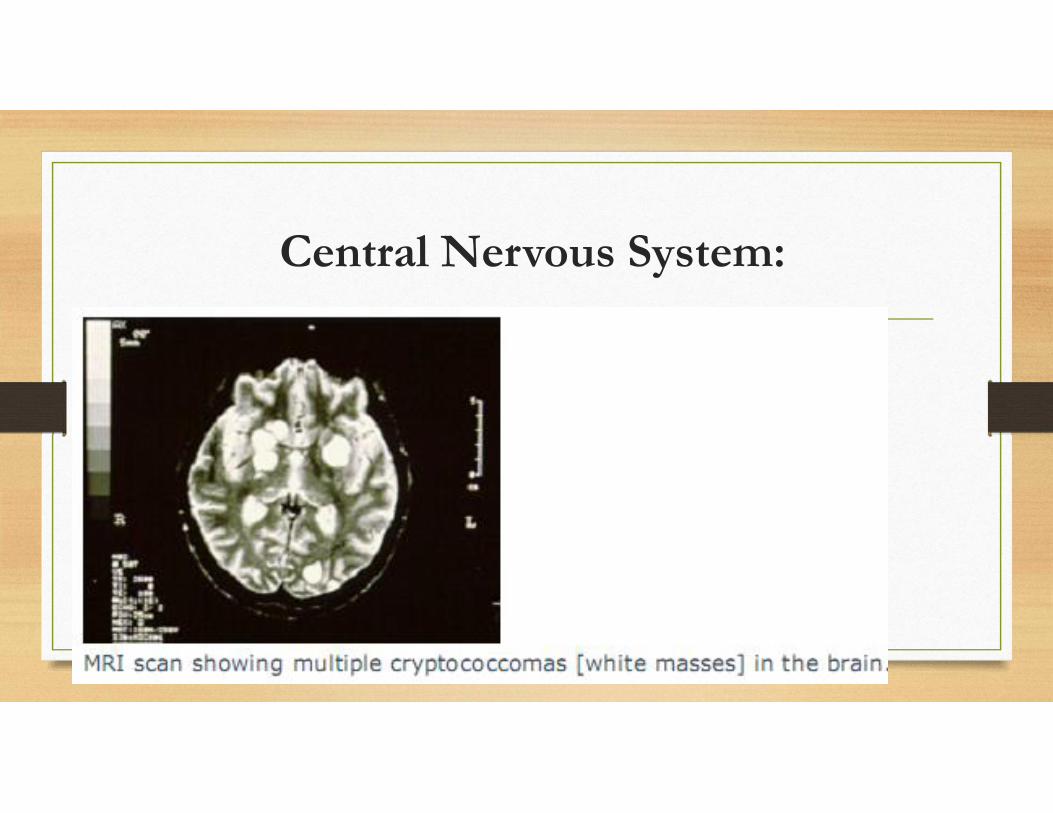
Central Nervous System:

Cutaneous cryptococcosis• 10-15% of disseminated cryptococcosis
• Common in HIV-infected persons
• Small papules that subsequently ulcerate
Osteomyelitis• 5-10% of patients with disseminated cryptococcosis
Genitourinary cryptococcosis• Common in HIV-infected persons• An important reservoir for relapse



115Molluscum contagiosum" like lesions

Laboratory diagnosis of cryptococcosis
• Direct microscopy examination
• Histopathological study
• Culture methods
• Detection of capsular antigen

Indian ink
Positive in more than 80% of patients with AIDS and approximately 50% in other
patients with cryptococcal meningitis.
• Yeast cells can be confused with? lymphocytes, fat droplets or other artifacts
• A positive smear must always be confirmed by culture


Culture•Definitive diagnosis can be obtained by culture
•C. neoformans can be isolated from the CSF in 75-90%of cases of C. meningrtis

Culture• Culture media incubated at 37oC
• Colonies usually appear within 2-5 days
• C. neoformans produce a white colony with a pink hallo
• Growth may be delayed in samples with few organism
• Cultures should be retained for 4-6 weeks

Niger seed agar can be used to distinguish Cryptococcus spp. (brown colonies) from Candida spp.(whitecolonies).

Histopathology
• Two basic histologic patterns may occur (gelatinous & granulomatus)
• The size of the yeast cells vary from less than one micron to 60µm
• The number of yeasts in granulomatous lesions is much fewer than thegelatinous type lesions

Organism is almost difficult to see with H&E

GMS

PAS

Mayer’s mucicarmine stain

Serological test
• Either serum of CSF has >95% sensitivity and specificity in the diagnosis ofinvasive cryptococcal infection
• Indicative of systemic disease
• Latex particle agglutination (LPA) and enzyme-linked immunosorbent assay(ELISA) tests

False-negative results ?
Can occur if the organism load is low or if the
organisms are not well encapsulated

False positive tests ?
May occur from contamination with loap or
detergents
Titers of most false positive results are 1:8
or less

Cross-reactive antigens?
In disseminated infections with
Trichosporon beigelii

TreatmentBased on anatomic site of disease and immune status of the patient.
Pulmonary disease: fluconazole is effective therapy in most patients.
Cryptococcal meningitis: amphotericin B with or without flu-cytosine, followed by aprolonged course of fluconazole.
• HIV-infected patients: Chronic maintenance therapy with fluconazole


















