
Obesity and metabolic syndrome 2
99
Obesity & Metabolic Syndrome By: Dr Madhumita Sen
-
Upload
madhumita-sen -
Category
Health & Medicine
-
view
452 -
download
2
Transcript of Obesity and metabolic syndrome 2

Obesity & Metabolic
Syndrome
By:
Dr Madhumita Sen

Learning Objectives
After this lesson, the audience are expected to know
- The causes of obesity
- The prevalence of obesity worldwide and in Malaysia
- Pathophysiology of Obesity- Regional fat distribution and its relationship to the
obesity health consequences
- Appetite regulation
- The role of gut hormones in obesity
- The endocrine function of the adipose tissue
- Clinical complications of obesity

Factors affecting Health

Rise of obesity
The recent rise in obesity and type 2 diabetes rates has reached disturbing levels.
This has occurred despite the fact that our knowledge about the importance and effects of diet and exercise are at an all time high.
Overweight and obesity lead to adverse metabolic effects on blood pressure, cholesterol, triglycerides and insulin resistance.
Risks of coronary heart disease, ischemic stroke and type 2 diabetes mellitus increase steadily.

Raised body mass index also increases the risk of cancer of the breast, colon, prostate, endometrium, kidney and gall bladder.

http://www.healthworks.my/malaysians
“Malaysia is ranked sixth in the Asia-Pacific region for obesity and tops the list in South-East Asia for both obesity and diabetes,” stated Prof Dr. Mohd Ismail Noor, the president of Malaysian Society for the Study of Obesity.
Malaysians diagnosed with diabetes has increased by two folds, from 1.5 million in 2006 to about three million in 2011.

What causes obesity? The thrifty gene hypothesis
The central premise of this theory is that through
natural selection we evolved to be efficient at
food storage and utilization.

Feast and FaminePaleolithic Era > 25,000 years ago
The thrifty gene hypothesis theorizes that if a person was more efficient at storing energy during the feasting portion of the cycle, he would be more likely to survive during the famine portion.
Physical activity-rest cycle is just as important as the feast-famine cycle.
In the hunter-gatherer society, food was obtained largely through physical activity.
Men hunted 1 to 4 non-consecutive days per week, while women gathered food 2 to 3 days per week.

Combining exercise into the thrifty gene hypothesis means that we likely did not evolve just to survive feast or famine, but also to be able to have enough fitness to survive the procurement of food.
This brings us to our current environment which consists of low activity levels, high calorie diets, and positive energy balance.
How does obesity occur? The formula is simple:
Food eaten – Exercise = Weight Gained

Other Causes: Social factors
Social factors play a major role in weight gain. adolescence, pregnancy, mid-life in women, and following marriage in men. Persons who emigrate to a more urbanized culture
tend to gain weight. Behavioural or environmental changes in life, such
as smoking cessation, are associated with weight gain.
Weight gained during holiday periods and festivals is more than at other times of the year and tends not to be lost.

Family Matters
Among pairs of adult siblings, if one sibling becomes obese, the chance that the other becomes obese increases by 40%.
If one spouse becomes obese, the likelihood that the other spouse becomes obese increases by 37%.

Sitting for Too Long At one time or another, we all end up spending
too much time at our desk staring at the computer screen.
Research shows that extended periods of sitting can increase our risk of heart disease, diabetes, depression, and certain types of cancer.
What we may not know is that even an adequate amount of exercise cannot reverse the unhealthy effects of sitting for eight hours.

Drinking Sugary Soft Drinks
People who drink a can of soda a day increase their risk of suffering a heart attack by 20 percent according to a recent Harvard University study.
The amount of sugar in a single can of soda, 10 teaspoons, or 100 percent of our daily recommended intake, can also increase our risk of pulmonary complications such as asthma and chronic obstructive pulmonary disorder (COPD).

Appetite Regulation

Appetite
Appetite is the amount of food one eats, feltas hunger.
Appetite exists in all higher life-forms, and serves to regulate adequate energy intake to maintain metabolic needs.
It is regulated by a close interplay between the digestive tract, adipose tissue and the brain.

The Main Hormones of Appetite Regulation
OREXIGENIC MOLECUES ANOREXIGENIC MOLECULES
Neuropeptide Y
Agouti Related Peptide
Melanin Concentrating Hormone
(MCH)
Orexins 1 & 2
Galanin
Ghrelin
Insulin
Endocannabinoids
Glutamate
Endorphins
Catecholamines (adrenaline,
noradrenaline, dopamine)
Alpha MSH
Cocaine and Amphetamine related
Transcript (CART)
Corticotrophin releasing hormone
(CRH)
Leptin
Serotonin
Peptide YY
GABA
Glucagon Like Peptide 1 (GLP1)
Cholecystokinin
Estrogen
Neurotensin

Hormones in Appetite Regulation
Amylin A partner hormone to insulin, released
after meals
Secreted by the pancreas
It slows the emptying of our stomach
and suppresses glucagon

GLP-1 Released when blood glucose levels are
above the norm
Secreted by cells of the gut in
proportion to the amount of energy
ingested
Stimulates insulin secretion, may assist
in signalling the brain to stop eating
GLP-1 is secreted from L cells in the
gastrointestinal tract and is induced by
sugars, amino acids, and long-chain
fatty acids. Short-chain fatty acids also
increase GLP-1 secretion

Leptin Released with low calorie intake and low body fat levels. Secreted by fat cells
Low leptin means a slower metabolism
and drive to increase food consumption.
Administering leptin analogs in humans
is ineffective for appetite suppression.
Leptin exists to prevent starvation, not
to lose weight.

Gastrin Released when food enters stomach,
protein dense foods are the
most potent stimulator of gastrin
Secreted by cells in
stomach/small intestine
Initiates the digestion process

Secretin Released when acids reach small
intestine
Secreted by cells in small intestine
Produces pancreatic fluid, inhibits
gastrin release, and enhances effects
of cholescystokinin

Cholecysto
kinin
(CCK)
Released when protein and fat enter
the small intestine
Secreted by cells in small intestine
Signals pancreas to produce
enzymes, inhibits gastrin, stimulates
gallbladder contraction, and triggers
satiety in the brain
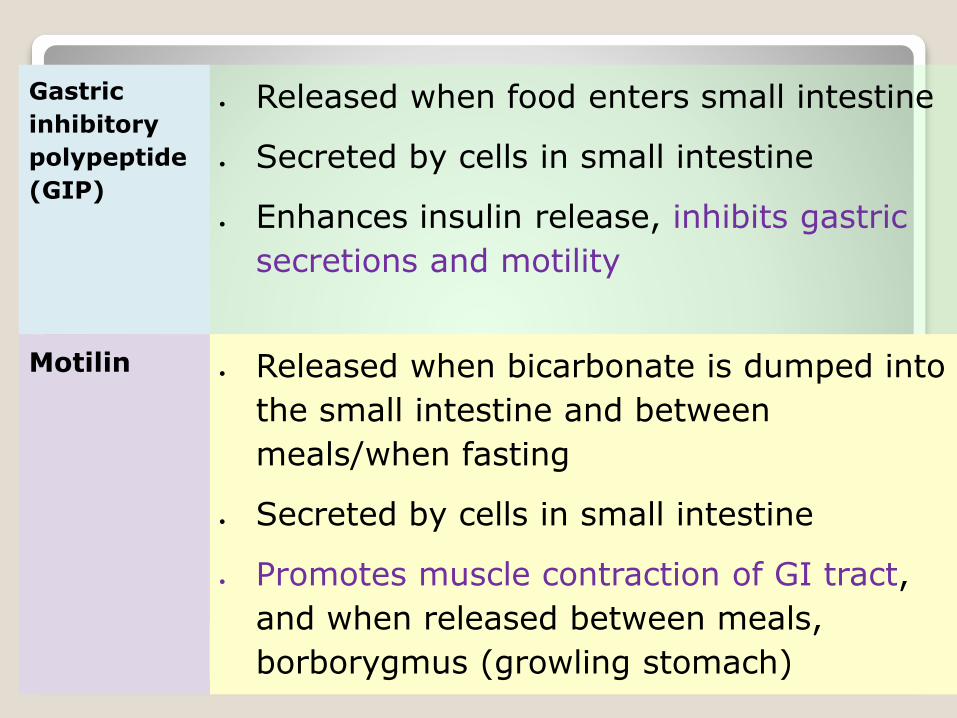
Gastric
inhibitory
polypeptide
(GIP)
Released when food enters small intestine
Secreted by cells in small intestine
Enhances insulin release, inhibits gastric
secretions and motility
Motilin Released when bicarbonate is dumped into
the small intestine and between
meals/when fasting
Secreted by cells in small intestine
Promotes muscle contraction of GI tract,
and when released between meals,
borborygmus (growling stomach)

Ghrelin Released in response to low food
intake/fasting
Secreted by cells of the stomach,
pancreas, placenta, kidney, pituitary
and hypothalamus
Stimulates release of growth hormone
to encourage eating and acts to
regulate energy balance.


Adiponectin
Adiponectin, is a 244-amino acid protein secreted from adipose tissue.
The plasma concentration of adiponectin is inversely correlated with adiposity in humans.
Studies show that treatment with adiponectincan reduce body weight gain, increase insulin sensitivity, and decrease lipid levels.
Thus adiponectin, as well as increasing energy expenditure, may also provide protection against insulin resistance and atherogenesis.


Recent data have suggested that brain reward pathways that are involved in alcohol and drug addiction are also essential elements of the ghrelin responsive circuit. And ghrelin has been shown to both signal hunger and increase food intake.
A subgroup of obese patients indeed show 'addictive-like' properties with regard to overeating.
Binge eating disorder (BED) is part of the recently published fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5)Oct 2013

Hypothalamic Lipid Metabolism and Energy Homeostasis
Within the central nervous system the metabolism of fatty acids is primarily for the purposes of membrane function and the central regulation of energy metabolism.
Fats do not serve as a major source of energy within the brain.
Fatty acids, specifically long-chain fatty acids via the formation of long-chain fatty acyl-CoAs, have very recently been shown to exert anorexigenic effects via the hypothalamus.

Zinc:
Leptin levels decrease in response to zinc depletion and increases after zinc supplementation.
Importantly, the magnitude of leptin level changes were proportional to the changes of cellular zinc.
Adequate zinc levels reduce appetite, possibly by increasing brain sensitivity to leptin.

Probiotics:
Recently, a potential link between gut microbiotaand obesity has emerged.
The study by Cani et al. [2011] evaluated the effect of prebiotics on plasma levels of gut hormones in healthy subjects.
After two weeks of probiotic treatment, they observed increased gut microbiota fermentation, decreased appetite, and improved postprandial glucose responses.
Furthermore plasma levels of GLP-1 was increasedin subjects following probiotic treatment.

Estrogen deficiency might result in a higher energy intake and increased body weight. Food intake varies across the menstrual cycle. Women tend to eat more in the luteal phase (the premenstrual period) compared with the follicular phase.
Testosterone (directly) seems to have little effect on food intake, although many people supplementing anabolic doses of testosterone (e.g. bodybuilders) do report increased appetite.
Including a balanced intake of omega-6:omega-3 fats can help with appetite regulation.
A high protein diet can reduce appetite.

Fibre seem to help control appetite.
Refined carbohydrates, on the other hand, appear to increase appetite.
Dietary fat has mixed results; when combined with refined carbohydrate it seems to increase appetite while on its own or combined with protein, it typically decreases appetite.
Elderly people have less appetite than young people from not only decreased energy expenditure but also from mechanisms potentially involving sex–steroid balance as well as altered CNS signalling to and from peripheral organs.

Don’t forget sleep!

Appetite regulation has so many factors!!!!
Dietary changes can manage weight as well as appetite.

Pathology of fats

Adipose Tissue as an Endocrine Organ
Adipose tissue is an important endocrine organ that secretes numerous protein hormones, collectively called Adipokines.
These hormones generally influence energy metabolism, which is of great interest to the understanding and treatment of type 2 diabetes and obesity.
Their relative roles in modifying appetite, insulin resistance and atherosclerosis are the subjects of intense research.

Obesity and Inflammation
Obesity is associated with a state of chronic, low-grade inflammation.
There is associated chronic inflammatory response characterized by abnormal cytokine production, increased acute-phase reactants, and activation of inflammatory signalling pathways.
A feature of this inflammatory response is that it appears to be triggered, and to reside predominantly, in abdominal adipose tissue, and not in subcutaneous fat.

Growth and angiogenic factors: Fibroblast growth factors (FGFs), insulin-like growth factor-1 (IGF-1), hepatocyte growth factor (HGF), nerve growth factor (NGF), vascular endothelial cell growth factor (VEGF), transforming growth factor-β (TGFβ), angiopoietin-1, angiopoietin-2, tissue factor (TF, factor 3).
Cytokines: IL-1β, IL-4, IL-6, IL-8, IL-10, IL-18, TNFα, macrophage migration inhibitory factor (MIF)
Complement-like factors: adipsin, adiponectin,
acylation stimulating protein (ASP)

Adhesion molecules and ECM components: α2-macroglobulin, vascular cell adhesion molecule-1 (VCAM-1), intercellular adhesion molecule-1 (ICAM-1), fibronectin, lysyloxidase.
Acute phase proteins: C-reactive protein (CRP), serum amyloid A3 (SAA3), plasminogen activator inhibitor-1 (PAI-1), haptoglobin
Chemokines: chemerin, monocyte chemotactic protein-1 (MCP-1), macrophage inhibitory protein-1 alpha (MIP-1α)-regulated upon activation, normally T cell expressed and secreted (RANTES)

Metabolic processes: adipocyte fatty acid binding protein (aP2), apolipoprotein E (apoE), resistin, omentin, vaspin, apelin, retinol binding protein 4 (RBP4), visfatin, leptin
Other processes: COX pathway products PGE2 and PGI2 (prostacyclin), nitric oxide synthase pathway, renin-angiotensin system

The proinflammatory state in the adipose tissue also leads to a local insulin resistance including an impaired inhibitory effect of insulin on FFA release.
The insulin resistance further supports the pro-inflammatory state because insulin, by itself, is antilipolytic.
Although energy restriction leading to weight loss is the primary dietary intervention to reverse these obesity-associated metabolic disorders, other interventions targeted at alleviating adipose tissue inflammation have not been explored in detail.

Omega-3 Fatty Acids Alleviate Adipose Tissue Inflammation and Insulin Resistance
There are studies showing that adipose tissue inflammation can be reduced without changing adipose mass.
EPA reverses high-fat–induced metabolic disorders and adipose inflammation.
In one study, EPA supplementation reversed high-saturated fat diet-induced insulin resistance and hepatic steatosis.
Omega 3 fatty acids are known to increase fatty acid oxidation in liver, adipose tissue, and small intestine


Syndrome - X or Metabolic syndrome
What is it?
Is it important?
How common is it?
What should be done about it?

What is it?
Metabolic syndrome is a combination of medicaldisorders that, when occurring together, increase the risk of developing cardiovascular disease and diabetes.
It affects about 20% of the Malaysian population and prevalence increases with age.
There are slight differences in the criteria of diagnosis - depending on which authority is quoted.
Regardless, the concept of a clustering of risks factors leading to cardiovascular disease is well accepted.

The cluster
Hypertension Hypertriglyceridemia Low HDL-cholesterol
Obesity (central) Impaired Glucose Handling
(Insulin Resistance) Microalbuninuria
(WHO)

American Heart Association1. Elevated waist circumference:
◦ Men — greater than 40 inches (102 cm)
◦ Women — greater than 35 inches (88 cm)
2. Elevated triglycerides: Equal to or greater than 150 mg/dL (1.7 mmol/L)
3. Reduced HDL (“good”) cholesterol:
◦ Men — Less than 40 mg/dL (1.03 mmol/L)
◦ Women — Less than 50 mg/dL (1.29 mmol/L)
4. Elevated blood pressure: Equal to or greater than 130/85 mm Hg or use of medication for hypertension
5. Elevated fasting glucose: Equal to or greater than 100 mg/dL (5.6 mmol/L) or use of medication for hyperglycemia


Other names used
Syndrome X
Cardio-metabolic Syndrome
Cardiovascular Dysmetabolic Syndrome
Insulin-Resistance Syndrome
Metabolic Syndrome
Beer Belly Syndrome
Reaven’s Syndrome

Risk Factors
Several associated risk factors include:
1. Genetic Factors: (inherited component):
◦ Family history of type 2 diabetes;
◦ Being Black, Hispanic, American Indian or Asian.
South Asians in urban and migrant environments may be at a higher risk of CHD due to the confluence of
1. genetic factors that predispose to higher cholesterol levels, and a possible "thrifty gene" effect, with
2. environmental influences that lead to weight gain

2. Particular physiological conditions and environmental factors:
> 40–45 years of age
obesity
the body storing fat predominantly in the abdomen, as opposed to storing it in hips and thighs.
lack of physical exercise
hypertension

3. Pre-diabetes:
sugar levels in the blood have been too high in the past, i.e. the body has previously shown slight problems with its production and usage of insulin ("previous evidence of impaired glucose homeostasis");
having developed gestational diabetes during past pregnancies;
giving birth to a baby weighing more than 9 pounds (a bit over 4 kilograms).

More risk factors
• Urban populations have higher levels of risk factors related to diet and physical activity (overweight, hypertension, dyslipidaemia and diabetes)
• Tobacco consumption is more widely prevalent in rural population
• The social gradient will reverse as the epidemic populations mature. The poor will become progressively vulnerable to the ravages of these diseases.

Environmental toxins
Xenobiotic and dietary compounds with hormone-like activity (obesogens) can disrupt endocrine signaling pathways that play important roles during perinatal differentiation and result in alterations that are not apparent until later in life.
Environmental obesogens: organotins and endocrine disruption via nuclear receptor signaling. Grün F, Blumberg B Endocrinology. 2006 Jun; 147(6 Suppl):S50-5.

History
The term "metabolic syndrome" dates back to at least the late 1950s.
The Marseilles physician Dr. Jean Vague, in 1947, observed that upper body obesity appeared to predispose to diabetes,atherosclerosis, gout and renal calculi.
In 1988, in his Banting lecture, Gerald M. Reavenproposed insulin resistance as the underlying factor and named the constellation of abnormalities Syndrome X.

INSULIN RESISTANCE IS THE MAIN PATHOLOGY BEHIND SYNDROME X

How Insulin Acts
• Any food or drink containing glucose (or any digestible carbohydrates) causes blood glucose levels to increase.
• In normal metabolism, the elevated blood glucose level and intestinal incretin makes beta (β) cells in the Islets of Langerhans, release insulin into the blood.

Insulin attaches to glucose-insulin receptors on cell membranes to allow glucose to be taken into the cell.
GLUT4 is the insulin-regulated glucose transporter that is responsible for insulin-regulated glucose translocation into the cell.

Glucose Transporter 4 Receptor
The GLUT4 protein is expressed primarily in muscle and fat cells, the major tissues in the body that respond to insulin.
Under conditions of low insulin, GLUT4 is sequestered in intracellular vesicles in muscle and fat cells.
Insulin induces the translocation of GLUT4 from these vesicles to the plasma membrane.
As the vesicles fuse with the plasma membrane, GLUT4 transporters are inserted and become available for transporting glucose.

• If the cell phospholipid membrane is not “fluid” enough (i.e. its composition does not have enough PUFA), insulin receptors are disrupted.
• The insulin cannot act and glucose cannot enter the cells, and thereby lower the blood glucose level.

• Without insulin, the liver is unable to use glucose, and therefore secretes glucagon, which further increases blood sugar by converting liver glycogen into glucose.
• The beta cells reduce insulin output only if the blood glucose level falls.
• In IR states, insulin levels remain high, and this promotes lipogenesis.

Factors influencing Insulin Resistance

Diet It is well known that insulin
resistance commonly coexists with obesity.
Saturated fat appears to be the most effective at producing IR.
Being insensitive to insulin is positively correlated with fat intake, and negatively correlated with dietary fibre intake.

CIS PUFA
In the long term, poor diet has the potential to change the ratio of CIS polyunsaturated fats to trans phospholipids in cell membranes, correspondingly changing cell membrane fluidity.
It is hypothesized that increasing cell membrane fluidity by increasing healthy PUFA concentration might result in an enhanced number of insulin receptors and reduced insulin resistance.

ADVANCED GLYCATION END PRODUCTS
AGE: Elevated blood levels of glucose – regardless of cause – lead to increased glycation of proteins and lipids with changes in their function throughout the body.
These are called Advanced Glycation End productsand contribute to the end organ damages of T2DM

Visceral fat
Unlike subcutaneous adipose tissue, visceral adipose cells produce significant amounts of pro-inflammatory cytokines such as tumour necrosis factor-alpha (TNF-a), Interleukins-1 and -6, etc.
These pro-inflammatory cytokines disrupt normal insulin action in fat and muscle cells.

Role of leptin
Yet another problem in metabolic syndrome involves the phenomenon known as leptinresistance.
An important role of leptin is long-term inhibition of appetite in response to formation of body fat.

Once leptinsignalling has been disrupted, the individual becomes prone to further overeating, weight gain, and insulin resistance.

Glycemic index
Integrated blood glucose response to a fixed quantity of carbohydrates in a meal is known as glycemicindex.
Complex carbs and foods high in fiber cause a slower rise in sugar, and reduced insulin resistance.

Signs and symptoms of insulin resistance
These depend on poorly understood variations in individual biology and consequently may not be found with all people diagnosed with insulin resistance.
1. Fatigue.
2. Brain fogginess and inability to focus.
3. High blood sugar.
4. Intestinal bloating – most intestinal gas is produced from simple carbohydrates in the diet.

5. Sleepiness, especially after meals.
6. Weight gain, fat storage, difficulty losing weight – for most people, excess weight is from high fat storage; the fat in IR is generally stored in and around abdominal organs in both males and females.
7. Increased blood triglyceride levels.
8. Increased blood pressure. One of insulin's effects is to control arterial wall tension throughout the body.

9. Increased pro-inflammatory cytokines associated with cardiovascular disease.
10. Depression. Due to the deranged metabolism resulting from insulin resistance, psychological effects, including depression, are not uncommon.
11. Acanthosis nigricans.
12. Increased hunger.

MANAGEMENT

Multiple risk factor management
Goals: Minimize Risk of Type 2 Diabetes and Cardiovascular Disease
Obesity
Glucose Intolerance
Insulin Resistance
Lipid Disorders
Hypertension

Treating Insulin Resistance
The primary treatment for insulin resistance is exercise and weight loss.
Low-glycemic index diet has also been shown to help.
Low salt diet helps reduce blood pressure and improves insulin sensitivity.
Both metformin and the thiazolidinediones improve insulin resistance.

Diabetes control For every 1% rise in Hb A1c there is an 18% rise in risk of
cardiovascular events & a 28% increase in peripheral arterial disease.
Goals: FBS = premeal 90-130,
postmeal <180.
Hgb A1c = 6.5 - 7%

Hypertension control
BP >130/85 or on Rx for previously diagnosed hypertension.
Goal: B.P.<130/85

DYSLIPIDEMIA
Goals: HDL >40 mg% (>1.1 mmol /l)
LDL <100 mg/dL (<3.0 mmol /l)
TG <150 mg% (<1.7 mmol /l)
Multiple major studies show 24 - 37% reductions in cardiovascular disease risk with the control of hyperlipidemia.
Increased HDL cholesterol can be achieved with increase in marine omega 3 fats intake.

SURGERY
Recent research has shown that weight reducing surgeries like gastric banding and roux-en-y gastric bypass can cure T2DM and IR, irrespective of associated weight loss.
The mechanisms of this effect are still being studied (? Incretin effect).
Type 2 diabetes has long been regarded as inevitably progressive, requiring increasing numbers of oral hypoglycemic agents and eventually insulin, but it is now certain that the disease process can be halted with restoration of normal carbohydrate and fat metabolism.
Type 2 diabetes can be understood as a potentially reversible metabolic state precipitated by the single cause of chronic excess intra-organ fat.
Roy Taylor, MD, FRCP, Diabetes Care.
2013;36(4):1047-1055.

Betatrophin
Researchers at Harvard University discovered that a hormone, called betatrophin, promotes the growth of Beta cells in the pancreas of mice.
Rather than having to take daily injections of insulin, patients would need to take this new hormone just weekly or even monthly, according to the researchers.
Dr Melton added, however, that the work was still in the early stages.
Cell. 2013 May 9;153(4):747-58. doi:10.1016/j.cell.2013.04.008. Epub 2013 Apr 25.

Testostorone
Testosterone replacement reverses insulin resistance in hypogonadal men with type 2 diabetes, preliminary data suggest.
The findings, from a randomized trial in 81 men, were reported by Paresh Dandona, MD, PhD, head of the division of endocrinology, diabetes, and metabolism at the University of Buffalo, State University of New York.
American Association of Clinical Endocrinologists 2013 Scientific & Clinical Congress Abstract 280, presented May 2, 2013.


Prevention
There is an urgent need to increase awareness of the CVD burden, and develop preventive strategies.
Prevention and treatment strategies that have been proven to be effective in developed countries should be adapted for developing countries.
Prevention is the best option as an approach to reduce CVD burden.

Diabetes and CVD – end points to avoid

Screening
1. Public Education
2. Screening for at risk individuals:
◦ Blood Sugar/ HbA1c
◦ Lipids
◦ Blood pressure
◦ Tobacco use
◦ Body habitus
◦ Family history

Public education
DIET
Carbohydrates:1.Eat according to energy requirements and as per
energy expended.2.Eat complex carbohydrates and fibre. Proteins1.Choose a wide variety of sources, both
Vegetarian and Non-vegetarian over the week2.Restrict intake to 30 gms per meal (size of a
deck of cards) Fats1.Choose vegetable fats2.Eat 1 helping of oily fish at least 2 -3 days a
week3.Snack on nuts

Life-Style Modification
Exercise◦ Improves CV fitness, weight control, sensitivity to insulin, reduces incidence of diabetes
◦ Goal: Brisk walking - 30 min./day/5 days a week
Weight loss◦ Improves lipids, insulin sensitivity, BP levels,reduces incidence of diabetes
◦ Goal: 10% reduction in body wt.

SMOKING CESSATION Both passive and active exposure harmful
A major risk factor for:◦ insulin resistance and metabolic syndrome
◦ Macro-vascular disease (PVD, MI, Stroke)◦ Micro-vascular complications of diabetes◦ pulmonary disease, etc.◦ Cancers

SLEEP
People who go to bed late and sleep in late typically have a greater degree of "circadian misalignment" between their actual sleep-wake pattern and their natural body clock.
Studies have linked such misalignment with a host of ailments, including coronary artery disease, metabolic syndrome, and impaired glucose tolerance.
Diabetes Care. Published online May 1, 2013.

Note: Obesity Paradox
The original description of the obesity paradox was published in 1999 using data from >1300 patients with chronic kidney disease undergoing haemodialysis.
The obesity paradox suggests that a BMI of ~25–35 kg/m2 carries benefit in patients with chronic disease possibly because excess fat serves as an energy depot in times of need.

The available studies, together with previously published study data, permit the conclusion that weight loss in patients with chronic illness and a BMI <40 kg/m2 is bad, and in fact not a single study exists to suggest that weight loss in chronic illness makes patients live longer.
This statement, however, should not be extrapolated to healthy individuals.
In summary, the most obvious seems to be most confusing in understanding the obesity paradox: healthy people and patients with chronic diseases are quite different.

Obesity may carry benefit up to a certain degree, and it should be recognized that obesity is not necessarily associated with abnormal metabolic function.
Eur Heart J. 2013;34(5):330-332. © 2013 Oxford
University Press

Key Points
• There is an urgent need to increase awareness of the
obesity, CVD and T2DM burden, and develop
preventive strategies.
• Prevention and treatment strategies that have been
proven to be effective in developed countries should
be adapted for developing countries.
• Prevention is the best option.

Thank you
Any questions?
Ref: http://www.medscape.com/viewarticle/851929?src=wnl_edit_tpal&uac=130781BG


















