Noura AlAyedh Abeer AlGhamdi Doha Marenga. OVERVIEW Definition Epidemology Etiology Pathophysiology...
22
Noura AlAyedh Abeer AlGhamdi Doha Marenga PENETRATING NECK TRAUMA
Transcript of Noura AlAyedh Abeer AlGhamdi Doha Marenga. OVERVIEW Definition Epidemology Etiology Pathophysiology...
Noura AlAyedh
Abeer AlGhamdi
Doha Marenga
PENETRATING NECK TRAUMA

OVERVIEW
•Definition•Epidemology•Etiology•Pathophysiology•Presentaion•Hard signs of air way injury•Evalaution•Indication of surgical evaluation•Investigation•Managment

Penetrating neck trauma involves a missile or sharp object penetrating the skin and violating the platysma layer of the
neck. This includes gunshot wounds, stab or puncture wounds, and impalement injuries
DEFINITION

ANATOMY ZONES
Anatomy: Zones I – III
Zone I: sternal notch > cricothyroid membrane
Zone II: cricothyroid membrane > angle of mandible
Zone III: angle of mandible > skull base
*Zone I is treated like thoracic injury
Penetrating neck trauma represents approximately 5-10% of all trauma cases that present to the emergency
department. About 30% of these cases are accompanied by injury outside of the neck zones as well.
EPIDEMIOLOGY
1.Gun shot (GSW): 45%
2. Stab (SW) 40%
*Structures injured: (40% no significant damage)
Major vein 15-25%
Major artery 10-15%
Digestive tract (pharynx, esophagus) 5-15%
Respiratory tract (larynx, trachea) 4-12%
Major nerves 3-8%

Penetrating neck injuries, like any trauma, may be classified as intentional or nonintentional.
The objects causing these injuries can be divided into:
1. stabbing instruments
(eg, knives, cutting instruments, puncturing objects, impaling objects)
2. shooting instruments
(eg, missiles, projectiles).
ETIOLOGY

Two factors in the mechanism of injury in penetrating neck trauma determine the extent of damage to the tissue:
Weapon characteristics
The amount of kinetic energy delivered by the wounding agent has to be considered together with its interaction with the
involved tissue.
Location of injury and human tissues involved
Tissue injury results from either a direct impact by the penetrating projectile or tissue displacement from temporary
cavitation.
Wound sites and, if present, the wounding agent in the neck provide an indication of the likely injury complex.
PATHOPHYSIOLOGY
Evidence of significant injury to vital structures of the neck may be indicated by the following clinical manifestations:
1. Dysphagia –> Tracheal and/or esophageal injury
2. Hoarseness –> Tracheal and/or esophageal injury (especially recurrent laryngeal nerve)
3. Oronasopharyngeal bleeding –> Vascular, tracheal, or esophageal injury Neurologic deficit – Vascular and/or spinal cord injury
4. Hypotension –> Nonspecific; may be related to the neck injury or may indicate trauma elsewhere
PRESENTATION
• Subcutaneous emphysema –> Tracheal, esophageal, or pulmonary injury
• Air bubbling through the wound
• Stridor or respiratory distress –> Laryngeal and/or esophageal injury
HARD SIGNS OF AIRWAY INJURY
1. Hematoma (expanding) –> Vascular injury
2. Active external hemorrhage from the wound site –> Arterial vascular injury
3. Bruit/thrill –> Arteriovenous fistula
4. Pulselessness/pulse deficit ->Distal ischemia (neurologic deficit in this case)
HARD SIGNS THAT STRONGLY INDICATE VASCULAR INJURY

1. (ABC).
2. secondary survey (complete history & physical examination).
• Mechanism of injury?
• Which zone?
• Depth of the wound (through platysma)?
• Transcervical
3. Workup (next slides)
EVALUATION
Investigation
Hemoglobin concentration:
is useful to evaluate for the immediate need for transfusion and to document the starting point for future comparison.
A toxicologic screen:
is indicated for the patient with an altered sensorium. This is important to help differentiate the altered sensorium of intoxication from a neurologic etiology following penetrating neck trauma with an arterial injury component.
LABORATORY STUDIES
• Cervical anteroposterior and lateral radiography
(evaluate for vertebral bony injury; retained foreign bodies; and foreign body deformity, location, size, and number.)
• Four-vessel cerebral angiography
(Indicated with clinical evidence of significant vascular injury (ie, hard signs) in zone I and zone III, as well as in selectively managed zone II injuries)
• CT / CT angiography
• MRI
IMAGING STUDIES

Direct laryngoscopy : For evaluation of oropharyngeal and tracheal injuries
Flexible bronchoscopy : For delineation of tracheal and bronchial injuries
Esophagoscopy:Flexible esophagoscopy can be used to detect an esophageal injury with less risk of procedure-related complications than rigid esophagoscopy
DIAGNOSTIC PROCEDURES
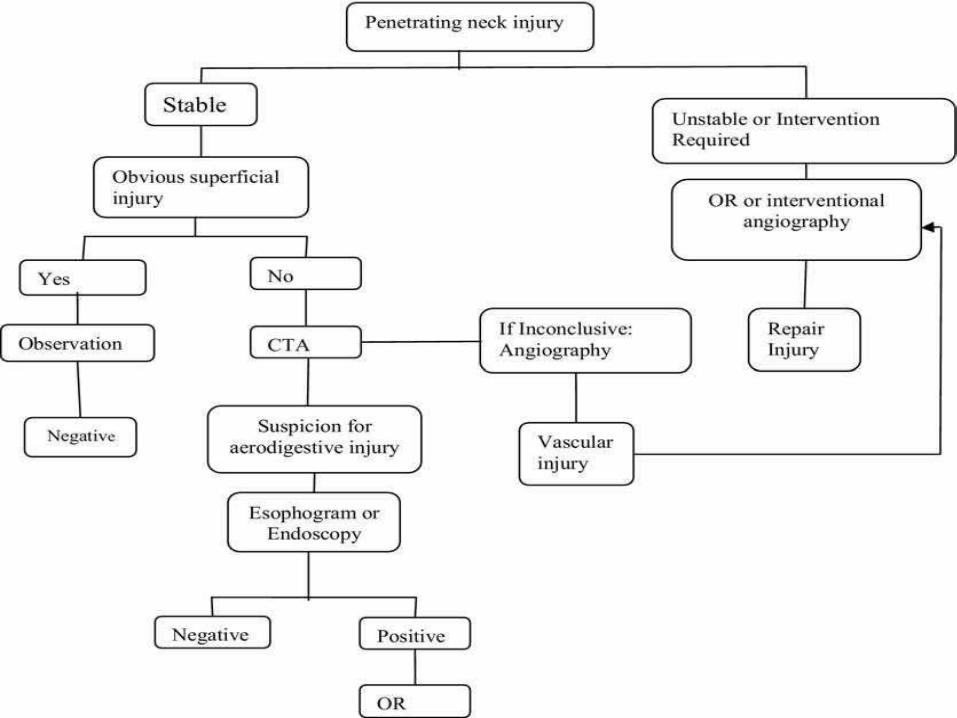
1. Unstable:
Airway injury , Hemodynamic instability, uncontrolled bleeding, evolving CVA
>>> Mandatory Exploration
MANAGEMENT

2.Stable w/ Symptoms:Hematoma, hemoptysis, hematemesis, dysphagia, dysphonia, peripeheral neuro deficit, subcutaneous air
>>> CTA in allSelective testing: endoscopy, esophagraphy, arteriography zones 1&3
Mandatroy exploration?
CONT.
3. Stable w/out symptoms:
observe >12hCTA in all
Artiography & Esophagraphy in zone 1
Exploration?
patients who present with signs and symptoms of shock and continuous hemorrhage from the neck wound.
The type of incision depends on the neck zone and the structures at risk for injury.
INDICATIONS OF SURGICAL EXPLORATION

The following specific injuries must be confirmed and treated during neck exploration:
1. Carotid artery injuries
2. Vertebral artery injuries
3. Jugular vein injury
4. Laryngotracheal injuries
5. Esophageal injuries
6. Nerve injuries
7. Thoracic duct injuries
8. Thyroid injuries
CONT..
Thank You!!