
Nottinghamshire STP Estates Workbook 21 October 2016 ... · Estates Workbook 21st October 2016...
22
1 Nottinghamshire STP Estates Workbook 21 st October 2016 Submission
-
Upload
truonghuong -
Category
Documents
-
view
217 -
download
0
Transcript of Nottinghamshire STP Estates Workbook 21 October 2016 ... · Estates Workbook 21st October 2016...
1
Nottinghamshire STP Estates Workbook
21st October 2016 Submission
2
• The options set out in this document are for discussion purposes. The involved NHS bodies understand and will comply with their statutory obligations when seeking to make decisions over estate strategies which impact on the provision of care to patients and the public. The options set out do not represent a commitment to any particular course of action on the part of the organisations involved.
• In respect of any request for disclosure under the FoIA: This is a confidential document for discussion purposes and any application for disclosure under the Freedom of Information Act 2000 should be considered against the potential exemptions contained in s.22 (Information intended for future publication), s.36 (Prejudice to effective conduct of public affairs) and s.43 (Commercial Interests). Prior to any disclosure under the FoIA the parties should discuss the potential impact of releasing such information as is requested.
STP Estates Workbook - Disclaimer
3
3. Contents
4/5. STP Service Strategy and Implications
6. Performance Indicators
7/8. Summary of Existing Projects
9. Sustainability & Transformation Initiatives
10/11. Implementation Priorities
12. Headline Financial Impacts – Investment and Disposal
13. Critical Decisions
14-22 Annex 1: Carter Metrics (Acute), NUH Programme & Basic Estates
Data
STP Estates Workbook - Contents
4
STP Service Strategy & ImplicationsKey STP Service Strategy Themes:
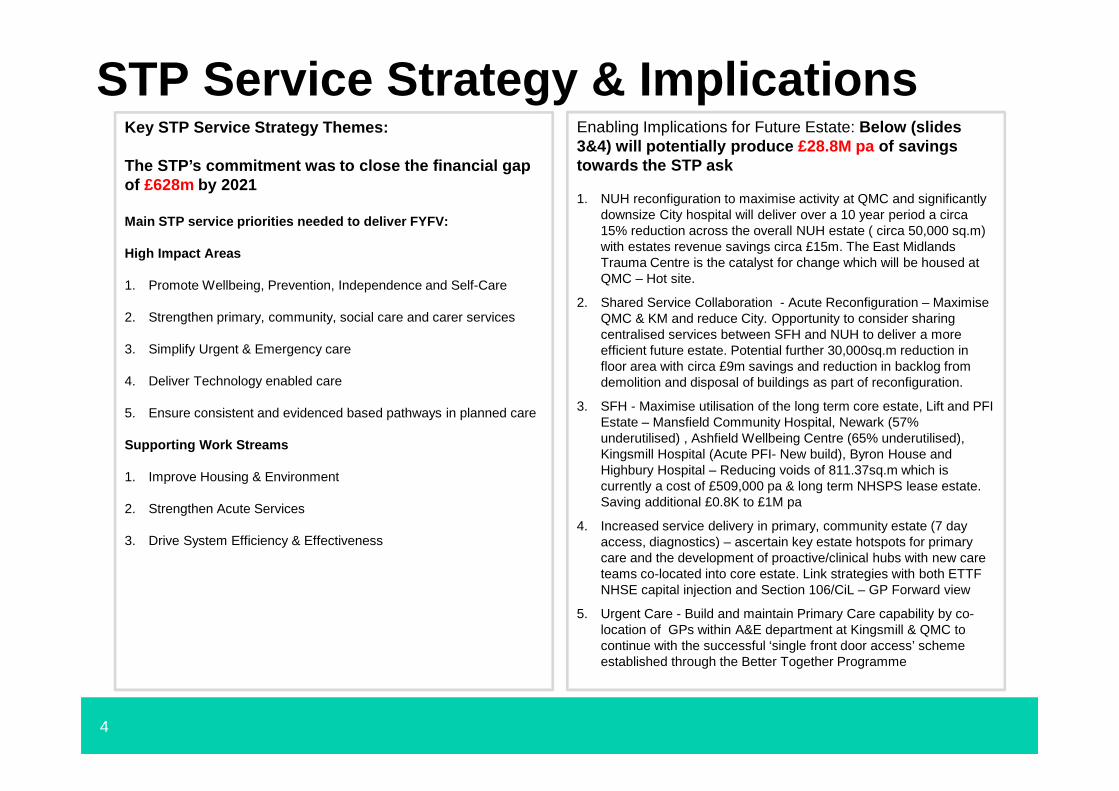
The STP’s commitment was to close the financial gap of £628m by 2021
Main STP service priorities needed to deliver FYFV:
High Impact Areas
1. Promote Wellbeing, Prevention, Independence and Self-Care
2. Strengthen primary, community, social care and carer services
3. Simplify Urgent & Emergency care
4. Deliver Technology enabled care
5. Ensure consistent and evidenced based pathways in planned care
Supporting Work Streams
1. Improve Housing & Environment
2. Strengthen Acute Services
3. Drive System Efficiency & Effectiveness
Enabling Implications for Future Estate: Below (slides 3&4) will potentially produce £28.8M pa of savings towards the STP ask
1. NUH reconfiguration to maximise activity at QMC and significantly downsize City hospital will deliver over a 10 year period a circa 15% reduction across the overall NUH estate ( circa 50,000 sq.m) with estates revenue savings circa £15m. The East Midlands Trauma Centre is the catalyst for change which will be housed at QMC – Hot site.
2. Shared Service Collaboration - Acute Reconfiguration – Maximise QMC & KM and reduce City. Opportunity to consider sharing centralised services between SFH and NUH to deliver a more efficient future estate. Potential further 30,000sq.m reduction in floor area with circa £9m savings and reduction in backlog from demolition and disposal of buildings as part of reconfiguration.
3. SFH - Maximise utilisation of the long term core estate, Lift and PFI Estate – Mansfield Community Hospital, Newark (57% underutilised) , Ashfield Wellbeing Centre (65% underutilised), Kingsmill Hospital (Acute PFI- New build), Byron House and Highbury Hospital – Reducing voids of 811.37sq.m which is currently a cost of £509,000 pa & long term NHSPS lease estate. Saving additional £0.8K to £1M pa
4. Increased service delivery in primary, community estate (7 day access, diagnostics) – ascertain key estate hotspots for primary care and the development of proactive/clinical hubs with new care teams co-located into core estate. Link strategies with both ETTF NHSE capital injection and Section 106/CiL – GP Forward view
5. Urgent Care - Build and maintain Primary Care capability by co-location of GPs within A&E department at Kingsmill & QMC to continue with the successful ‘single front door access’ scheme established through the Better Together Programme

5
STP Service Strategy & ImplicationsKey STP Service Strategy Themes:
Main STP service priorities needed to deliver FYFV:
Enablers
1. Workforce & Organisational development
2. Commissioning and System Governance
3. Estates Utilisation - accompanying slide
4. Communication & Engagement
Enabling Implications for Future Estate:
Priority areas to address are….
1. The acute reconfiguration work will also reduce outpatients departments in the acute & bed space to align with the shift of activity into the community
2. Further opportunities to reduce the footprint of estate through system wide disposals approx. £6.3m
3. Integrated primary, community, social care and mental health multidisciplinary teams (MDTs) working in formal network arrangements within a local clusters of practices to facilitate estate utilisation and 7 day working, maximisation of technological enablers and remote work will enable a reduction in non-priority estate through co-location
4. Respond to the Carter review and corporate services consolidation to support a potential reduction in floor area of administrative estate by 2,500 sqm. – 3,500 sqm . or between 70% and 100% of total floor area. Potential to reduce running costs by £1.3m – £1.5m , with required capital expenditure. Known schemes include the retraction from rented accommodation as Trust HQ within the Mid Notts footprint £0.8 to 1.0m
5. Working with the Health and Wellbeing Board, an engagement process is ongoing to help Local Authority Planners familiarise themselves with each Local Estates Forum to ensure that housing/business growth is captured through capital monies to support ongoing health infrastructure development – Mid-Notts CCG for Newark South have agreed £1.7m over 5 phases with developers for existing infrastructure upgrades
6
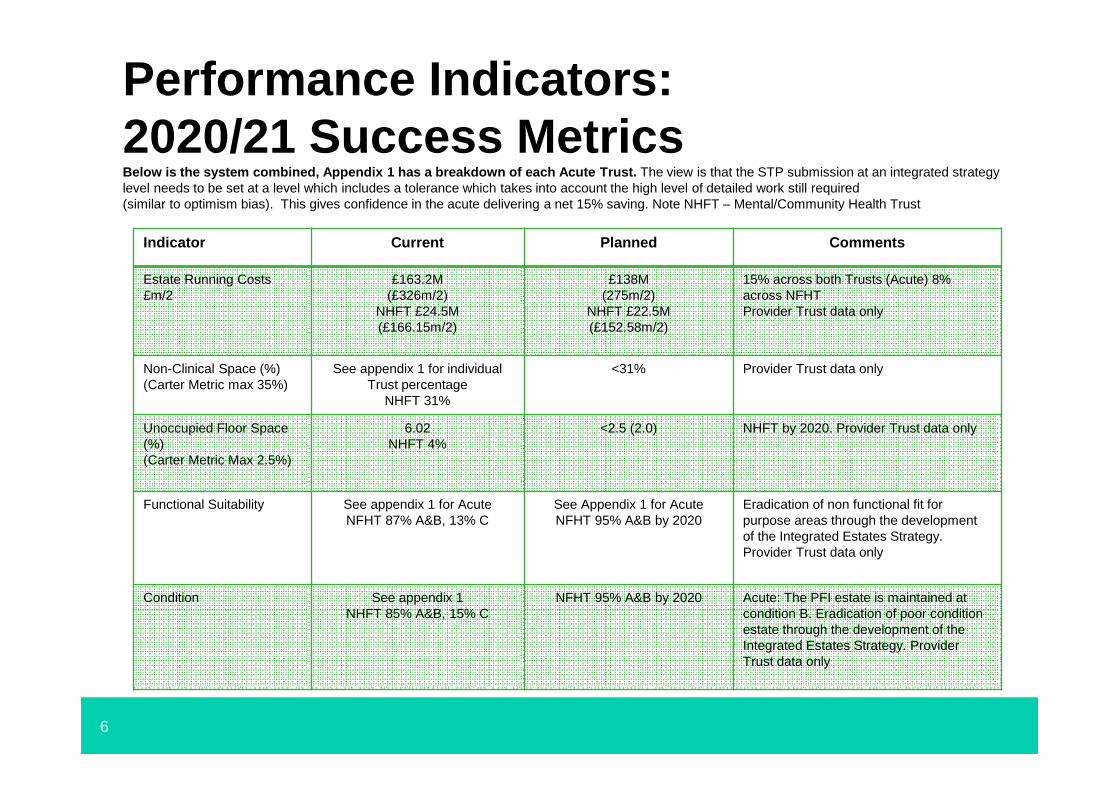
Performance Indicators: 2020/21 Success Metrics Below is the system combined, Appendix 1 has a brea kdown of each Acute Trust. The view is that the STP submission at an integrated strategy level needs to be set at a level which includes a tolerance which takes into account the high level of detailed work still required (similar to optimism bias). This gives confidence in the acute delivering a net 15% saving. Note NHFT – Mental/Community Health Trust
Indicator Current Planned Comments
Estate Running Costs£m/2
£163.2M(£326m/2)
NHFT £24.5M(£166.15m/2)
£138M(275m/2)
NHFT £22.5M(£152.58m/2)
15% across both Trusts (Acute) 8% across NFHT Provider Trust data only
Non-Clinical Space (%)(Carter Metric max 35%)
See appendix 1 for individual Trust percentage
NHFT 31%
<31% Provider Trust data only
Unoccupied Floor Space (%)(Carter Metric Max 2.5%)
6.02NHFT 4%
<2.5 (2.0) NHFT by 2020. Provider Trust data only
Functional Suitability See appendix 1 for Acute NFHT 87% A&B, 13% C
See Appendix 1 for Acute NFHT 95% A&B by 2020
Eradication of non functional fit for purpose areas through the development of the Integrated Estates Strategy. Provider Trust data only
Condition See appendix 1NHFT 85% A&B, 15% C
NFHT 95% A&B by 2020 Acute: The PFI estate is maintained at condition B. Eradication of poor condition estate through the development of the Integrated Estates Strategy. Provider Trust data only
7
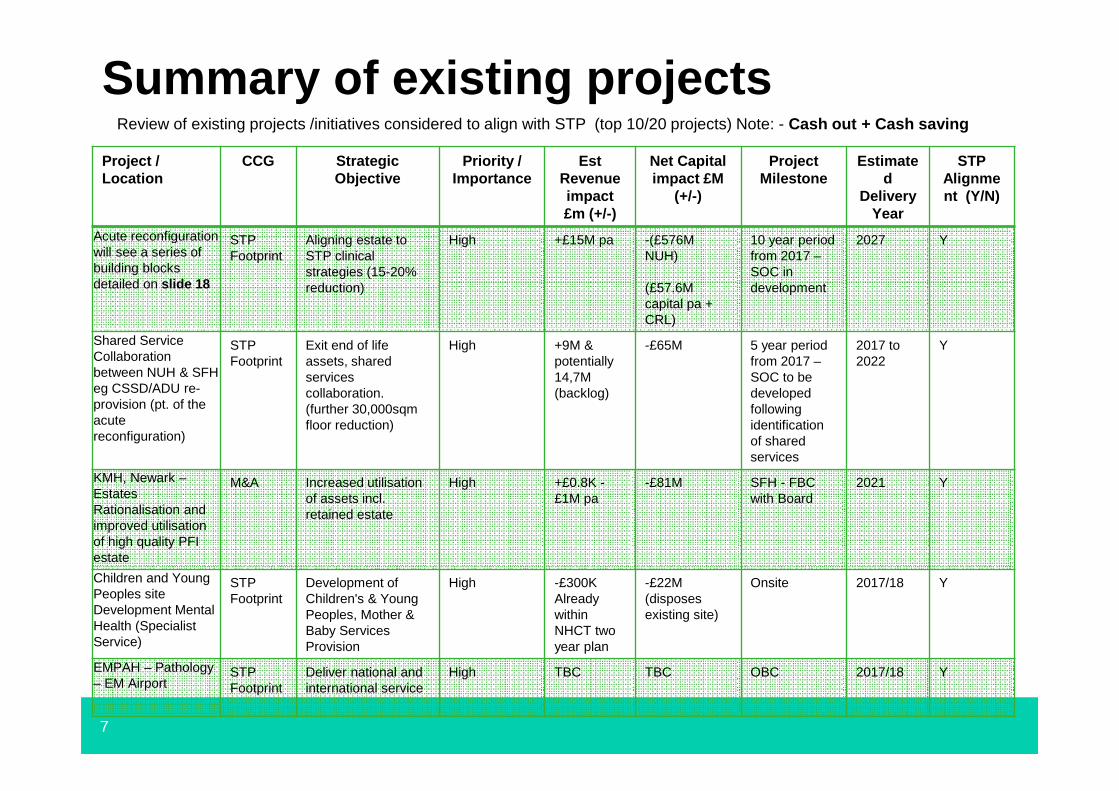
Summary of existing projectsReview of existing projects /initiatives considered to align with STP (top 10/20 projects) Note: - Cash out + Cash saving
Project / Location
CCG StrategicObjective
Priority / Importance
Est Revenue impact£m (+/-)
Net Capitalimpact £M
(+/-)
Project Milestone
Estimated
DeliveryYear
STP Alignment (Y/N)
Acute reconfiguration will see a series of building blocks detailed on slide 18
STP Footprint
Aligning estate to STP clinical strategies (15-20% reduction)
High +£15M pa -(£576MNUH)
(£57.6M capital pa + CRL)
10 year period from 2017 –SOC in development
2027 Y
Shared ServiceCollaboration between NUH & SFH eg CSSD/ADU re-provision (pt. of the acute reconfiguration)
STP Footprint
Exit end of life assets, shared services collaboration. (further 30,000sqm floor reduction)
High +9M & potentially 14,7M (backlog)
-£65M 5 year period from 2017 –SOC to be developed following identification of sharedservices
2017 to 2022
Y
KMH, Newark –Estates Rationalisation and improved utilisation of high quality PFI estate
M&A Increased utilisationof assets incl. retained estate
High +£0.8K -£1M pa
-£81M SFH - FBC with Board
2021 Y
Children and Young Peoples site Development Mental Health (Specialist Service)
STP Footprint
Development of Children's & Young Peoples, Mother & Baby Services Provision
High -£300KAlready within NHCT two year plan
-£22M(disposes existing site)
Onsite 2017/18 Y
EMPAH – Pathology – EM Airport
STPFootprint
Deliver national and international service
High TBC TBC OBC 2017/18 Y
8
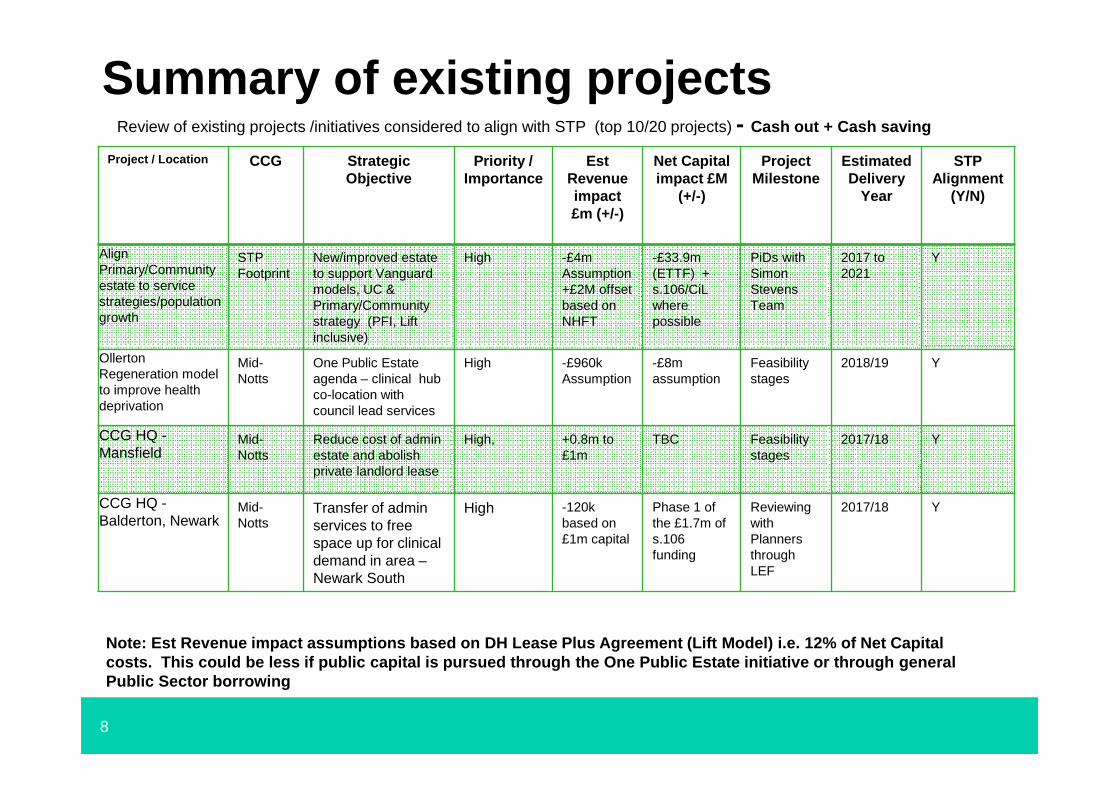
Summary of existing projectsReview of existing projects /initiatives considered to align with STP (top 10/20 projects) - Cash out + Cash saving
Project / Location CCG StrategicObjective
Priority / Importance
Est Revenue impact£m (+/-)
Net Capitalimpact £M
(+/-)
Project Milestone
Estimated Delivery
Year
STP Alignment
(Y/N)
AlignPrimary/Community estate to service strategies/population growth
STP Footprint
New/improved estate to support Vanguard models, UC & Primary/Community strategy (PFI, Lift inclusive)
High -£4m Assumption+£2M offset based on NHFT
-£33.9m (ETTF) +s.106/CiLwhere possible
PiDs with Simon Stevens Team
2017 to 2021
Y
OllertonRegeneration model to improve health deprivation
Mid-Notts
One Public Estate agenda – clinical hub co-location with council lead services
High -£960kAssumption
-£8m assumption
Feasibilitystages
2018/19 Y
CCG HQ -Mansfield
Mid-Notts
Reduce cost of admin estate and abolish private landlord lease
High, +0.8m to£1m
TBC Feasibilitystages
2017/18 Y
CCG HQ -Balderton, Newark
Mid-Notts
Transfer of admin services to free space up for clinical demand in area –Newark South
High -120k based on £1m capital
Phase 1 of the £1.7m of s.106funding
Reviewing with Planners through LEF
2017/18 Y
Note: Est Revenue impact assumptions based on DH Lease Plus Agreement (Lift Model) i.e. 12% of Net Capital costs. This could be less if public capital is pursued through the One Public Estate initiative or through general Public Sector borrowing
9
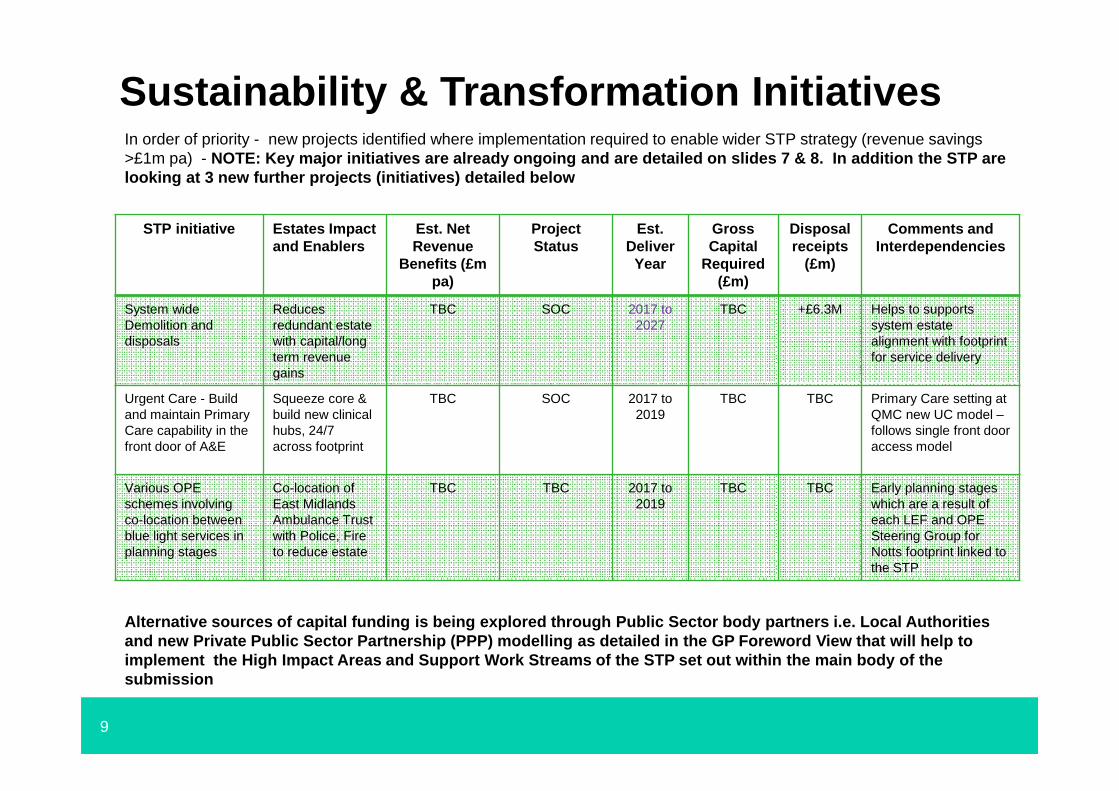
In order of priority - new projects identified where implementation required to enable wider STP strategy (revenue savings >£1m pa) - NOTE: Key major initiatives are already ongoing and are detailed on slides 7 & 8. In addition the STP are looking at 3 new further projects (initiatives) det ailed below
STP initiative Estates Impact and Enablers
Est. Net Revenue
Benefits (£m pa)
Project Status
Est. Deliver
Year
GrossCapital
Required (£m)
Disposalreceipts
(£m)
Comments and Interdependencies
System wide Demolition and disposals
Reduces redundant estate with capital/long term revenue gains
TBC SOC 2017 to 2027
TBC +£6.3M Helps to supportssystem estate alignment with footprint for service delivery
Urgent Care - Build and maintain PrimaryCare capability in the front door of A&E
Squeeze core &build new clinical hubs, 24/7 across footprint
TBC SOC 2017 to 2019
TBC TBC Primary Care setting at QMC new UC model –follows single front door access model
Various OPE schemes involving co-location between blue light services in planning stages
Co-location of East Midlands Ambulance Trust with Police, Fire to reduce estate
TBC TBC 2017 to 2019
TBC TBC Early planning stages which are a result of each LEF and OPE Steering Group for Notts footprint linked to the STP
Sustainability & Transformation Initiatives
Alternative sources of capital funding is being explored through Public Sector body partners i.e. Local Authorities and new Private Public Sector Partnership (PPP) modelling as detailed in the GP Foreword View that will help to implement the High Impact Areas and Support Work Streams of the STP set out within the main body of the submission
10
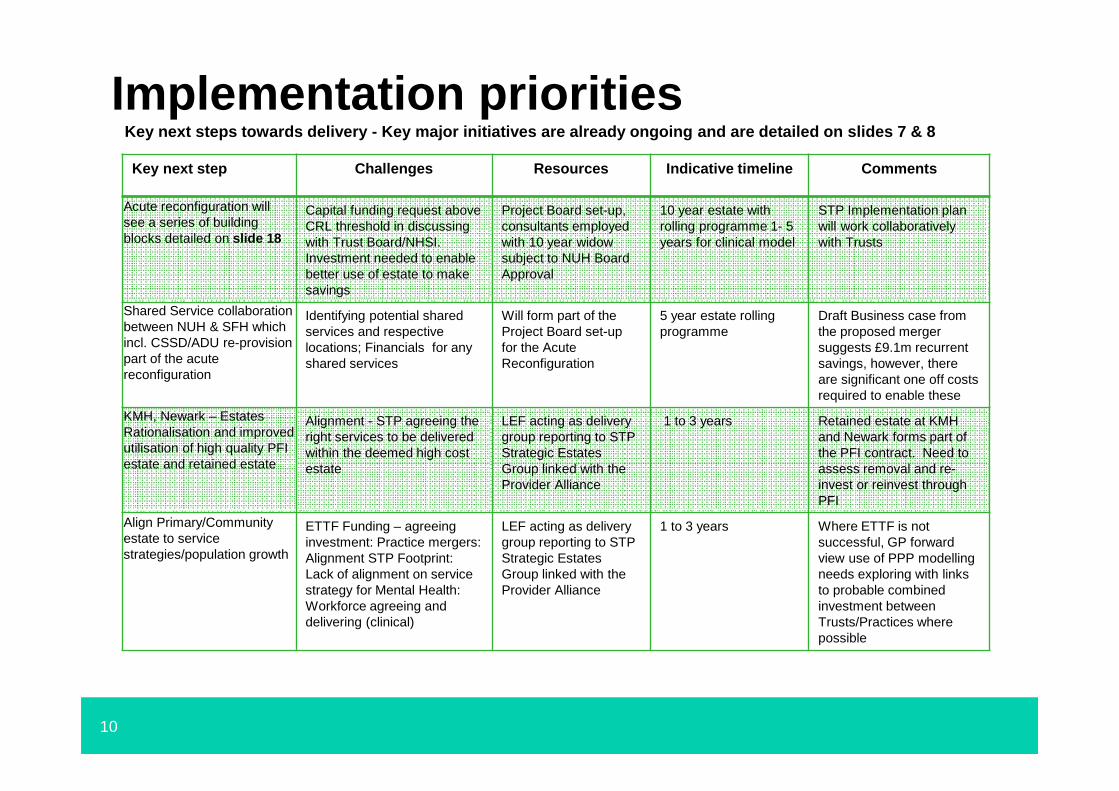
Implementation prioritiesKey next steps towards delivery - Key major initiati ves are already ongoing and are detailed on slides 7 & 8
Key next step Challenges Resources Indicative timeline Comments
Acute reconfiguration will see a series of building blocks detailed on slide 18
Capital funding request above CRL threshold in discussing with Trust Board/NHSI. Investment needed to enable better use of estate to make savings
Project Board set-up, consultants employed with 10 year widow subject to NUH Board Approval
10 year estate with rolling programme 1- 5 years for clinical model
STP Implementation plan will work collaboratively with Trusts
Shared Service collaboration between NUH & SFH which incl. CSSD/ADU re-provision part of the acute reconfiguration
Identifying potential shared services and respective locations; Financials for any shared services
Will form part of the Project Board set-up for the Acute Reconfiguration
5 year estate rolling programme
Draft Business case from the proposed merger suggests £9.1m recurrent savings, however, there are significant one off costs required to enable these
KMH, Newark – Estates Rationalisation and improved utilisation of high quality PFI estate and retained estate
Alignment - STP agreeing the right services to be delivered within the deemed high cost estate
LEF acting as delivery group reporting to STPStrategic Estates Group linked with the Provider Alliance
1 to 3 years Retained estate at KMH and Newark forms part of the PFI contract. Need to assess removal and re-invest or reinvest through PFI
Align Primary/Community estate to service strategies/population growth
ETTF Funding – agreeing investment: Practice mergers: Alignment STP Footprint:Lack of alignment on service strategy for Mental Health: Workforce agreeing and delivering (clinical)
LEF acting as delivery group reporting to STPStrategic Estates Group linked with the Provider Alliance
1 to 3 years Where ETTF is not successful, GP forward view use of PPP modelling needs exploring with links to probable combined investment between Trusts/Practices where possible
11
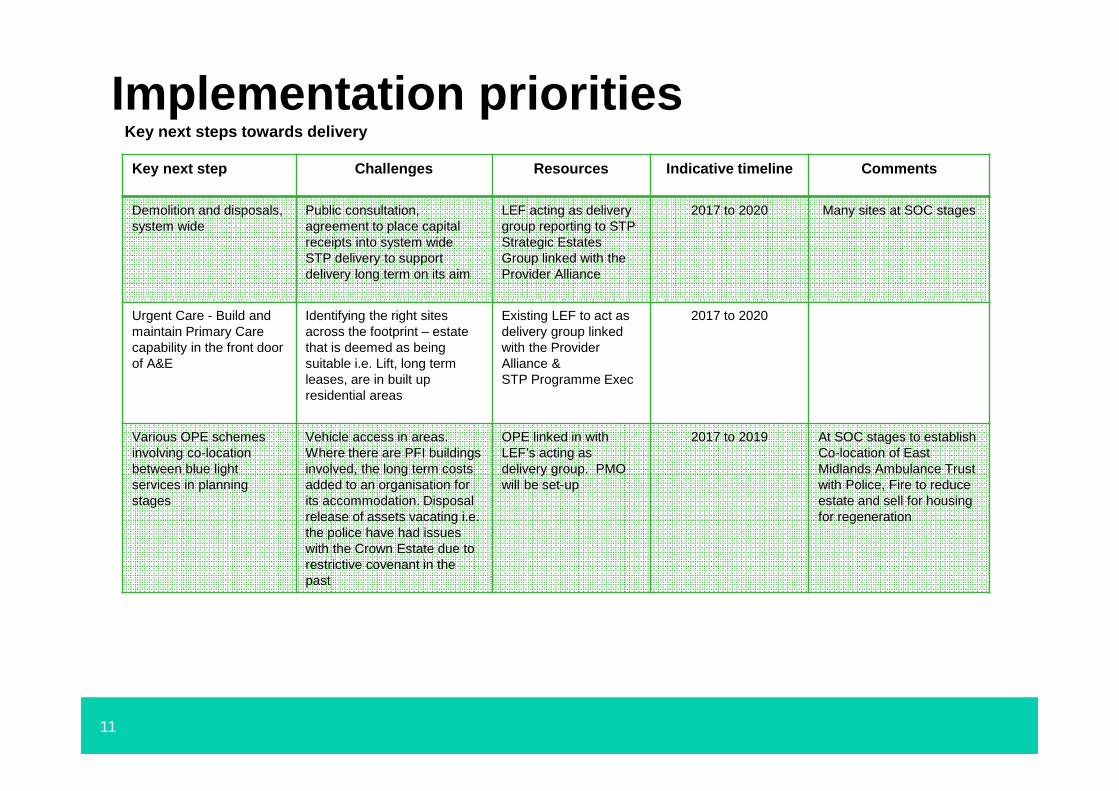
Implementation prioritiesKey next steps towards delivery
Key next step Challenges Resources Indicative timeline Comments
Demolition and disposals, system wide
Public consultation,agreement to place capital receipts into system wide STP delivery to support delivery long term on its aim
LEF acting as delivery group reporting to STPStrategic Estates Group linked with the Provider Alliance
2017 to 2020 Many sites at SOC stages
Urgent Care - Build and maintain Primary Care capability in the front door of A&E
Identifying the right sites across the footprint – estate that is deemed as being suitable i.e. Lift, long term leases, are in built up residential areas
Existing LEF to act as delivery group linked with the Provider Alliance &STP Programme Exec
2017 to 2020
Various OPE schemes involving co-location between blue light services in planning stages
Vehicle access in areas. Where there are PFI buildings involved, the long term costs added to an organisation for its accommodation. Disposal release of assets vacating i.e. the police have had issues with the Crown Estate due to restrictive covenant in the past
OPE linked in with LEF’s acting as delivery group. PMO will be set-up
2017 to 2019 At SOC stages to establish Co-location of EastMidlands Ambulance Trust with Police, Fire to reduce estate and sell for housing for regeneration
12
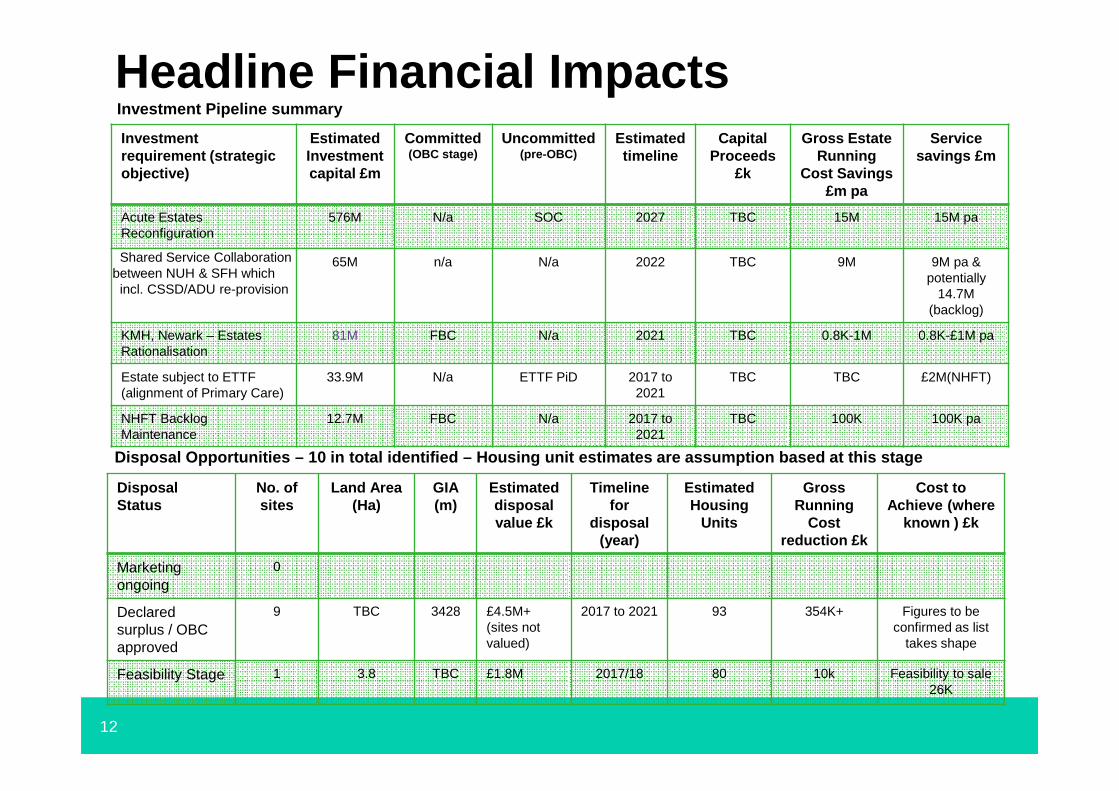
Headline Financial ImpactsInvestment Pipeline summary
Disposal Opportunities – 10 in total identified – Housing unit estimates are assumption based at this stage
Investment requirement (strategic objective)
Estimated Investment capital £m
Committed(OBC stage)
Uncommitted(pre-OBC)
Estimated timeline
Capital Proceeds
£k
Gross Estate Running
Cost Savings £m pa
Service savings £m
Acute Estates Reconfiguration
576M N/a SOC 2027 TBC 15M 15M pa
Shared Service Collaboration between NUH & SFH which incl. CSSD/ADU re-provision
65M n/a N/a 2022 TBC 9M 9M pa & potentially
14.7M (backlog)
KMH, Newark – Estates Rationalisation
81M FBC N/a 2021 TBC 0.8K-1M 0.8K-£1M pa
Estate subject to ETTF (alignment of Primary Care)
33.9M N/a ETTF PiD 2017 to 2021
TBC TBC £2M(NHFT)
NHFT Backlog Maintenance
12.7M FBC N/a 2017 to 2021
TBC 100K 100K pa
Disposal Status
No. of sites
Land Area (Ha)
GIA(m)
Estimated disposal value £k
Timeline for
disposal (year)
Estimated Housing
Units
Gross Running
Costreduction £k
Cost to Achieve (where
known ) £k
Marketing ongoing
0
Declared surplus / OBC approved
9 TBC 3428 £4.5M+ (sites not valued)
2017 to 2021 93 354K+ Figures to be confirmed as list
takes shape
Feasibility Stage 1 3.8 TBC £1.8M 2017/18 80 10k Feasibility to sale26K
13
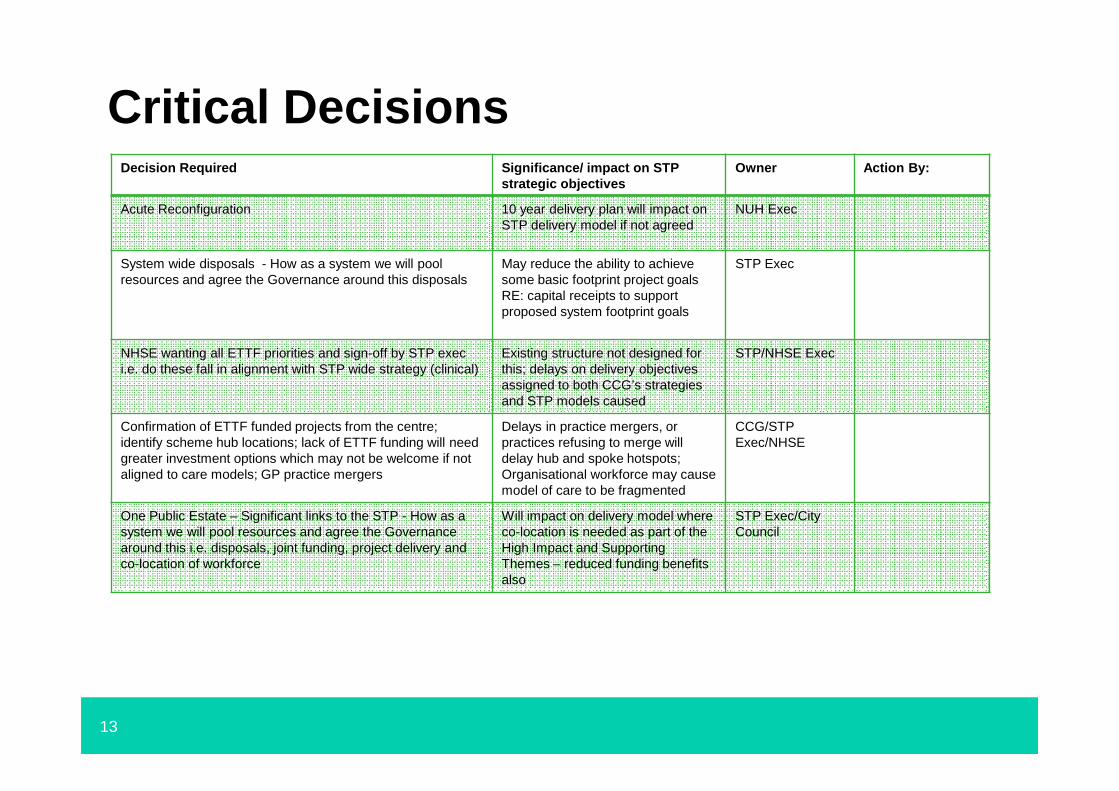
Critical DecisionsDecision Required Significance/ impact on STP
strategic objectivesOwner Action By:
Acute Reconfiguration 10 year delivery plan will impact on STP delivery model if not agreed
NUH Exec
System wide disposals - How as a system we will pool resources and agree the Governance around this disposals
May reduce the ability to achieve some basic footprint project goals RE: capital receipts to support proposed system footprint goals
STP Exec
NHSE wanting all ETTF priorities and sign-off by STP exec i.e. do these fall in alignment with STP wide strategy (clinical)
Existing structure not designed for this; delays on delivery objectives assigned to both CCG’s strategies and STP models caused
STP/NHSE Exec
Confirmation of ETTF funded projects from the centre;identify scheme hub locations; lack of ETTF funding will need greater investment options which may not be welcome if not aligned to care models; GP practice mergers
Delays in practice mergers, or practices refusing to merge will delay hub and spoke hotspots;Organisational workforce may cause model of care to be fragmented
CCG/STPExec/NHSE
One Public Estate – Significant links to the STP - How as a system we will pool resources and agree the Governance around this i.e. disposals, joint funding, project delivery and co-location of workforce
Will impact on delivery model where co-location is needed as part of the High Impact and Supporting Themes – reduced funding benefits also
STP Exec/City Council
14
Annex 1: Carter Metrics (Acute), NUH Programme & Basic Estates Data
15
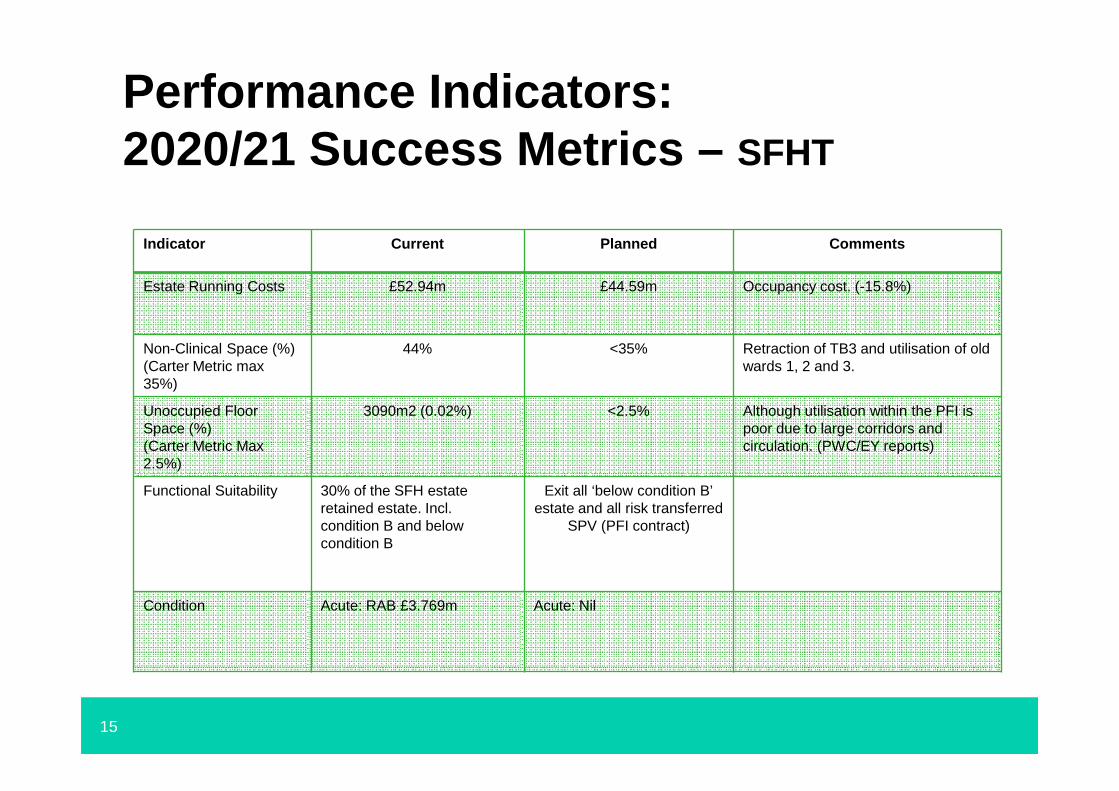
Performance Indicators: 2020/21 Success Metrics – SFHT
Indicator Current Planned Comments
Estate Running Costs £52.94m £44.59m Occupancy cost. (-15.8%)
Non-Clinical Space (%)(Carter Metric max35%)
44% <35% Retraction of TB3 and utilisation of old wards 1, 2 and 3.
Unoccupied Floor Space (%)(Carter Metric Max 2.5%)
3090m2 (0.02%) <2.5% Although utilisation within the PFI is poor due to large corridors and circulation. (PWC/EY reports)
Functional Suitability 30% of the SFH estate retained estate. Incl. condition B and below condition B
Exit all ‘below condition B’ estate and all risk transferred
SPV (PFI contract)
Condition Acute: RAB £3.769m Acute: Nil
16
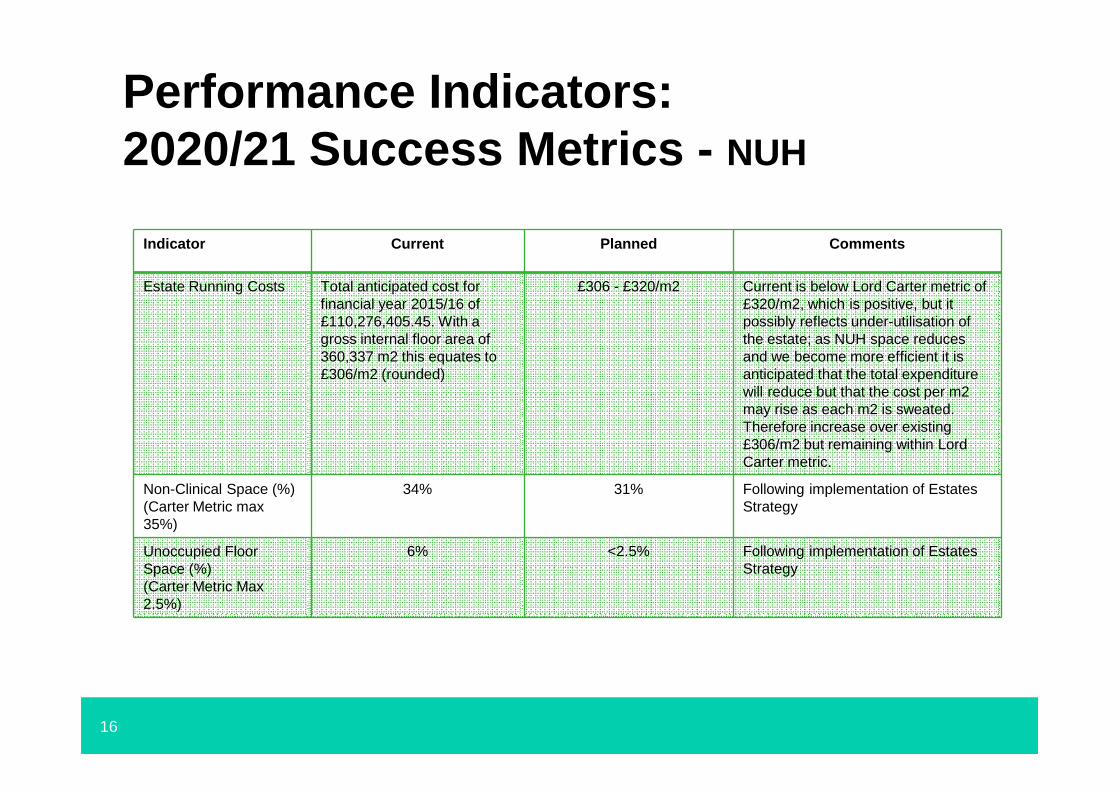
Performance Indicators: 2020/21 Success Metrics - NUH
Indicator Current Planned Comments
Estate Running Costs Total anticipated cost for financial year 2015/16 of £110,276,405.45. With a gross internal floor area of 360,337 m2 this equates to £306/m2 (rounded)
£306 - £320/m2 Current is below Lord Carter metric of £320/m2, which is positive, but it possibly reflects under-utilisation of the estate; as NUH space reduces and we become more efficient it is anticipated that the total expenditure will reduce but that the cost per m2 may rise as each m2 is sweated. Therefore increase over existing £306/m2 but remaining within Lord Carter metric.
Non-Clinical Space (%)(Carter Metric max35%)
34% 31% Following implementation of Estates Strategy
Unoccupied Floor Space (%)(Carter Metric Max 2.5%)
6% <2.5% Following implementation of Estates Strategy
17
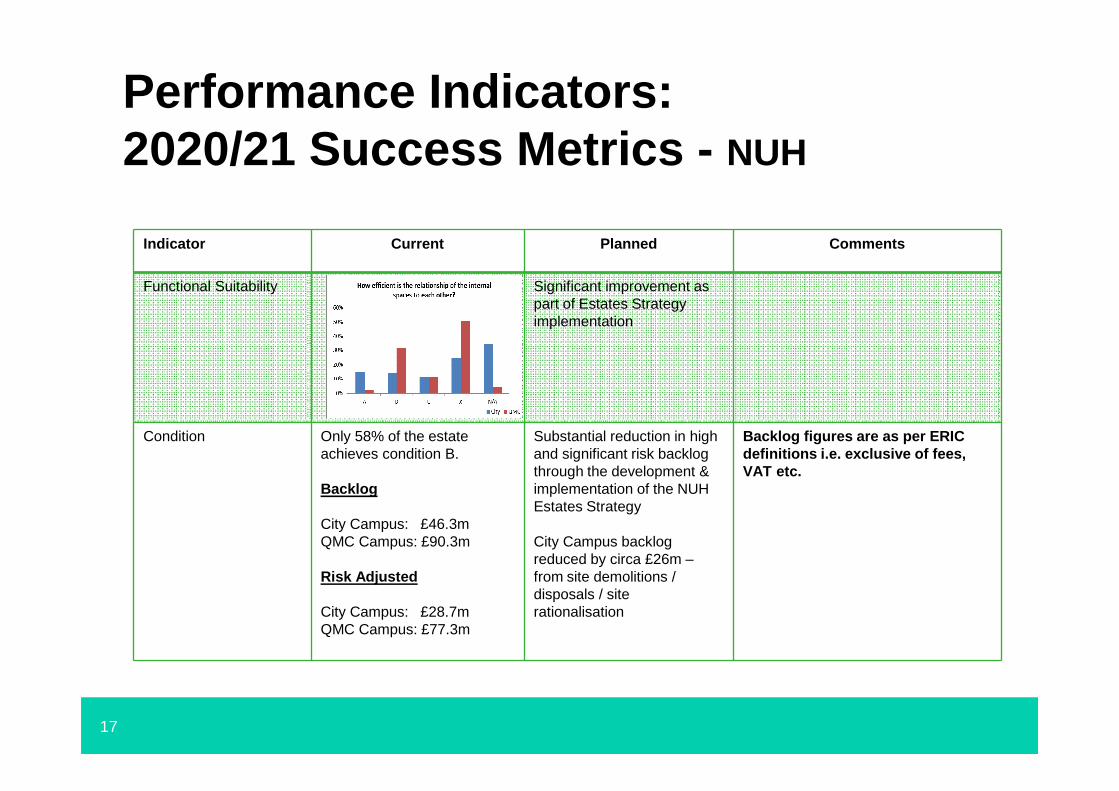
Performance Indicators: 2020/21 Success Metrics - NUH
Indicator Current Planned Comments
Functional Suitability Significant improvement aspart of Estates Strategy implementation
Condition Only 58% of the estate achieves condition B.
Backlog
City Campus: £46.3mQMC Campus: £90.3m
Risk Adjusted
City Campus: £28.7mQMC Campus: £77.3m
Substantial reduction in high and significant risk backlog through the development & implementation of the NUH Estates Strategy
City Campus backlog reduced by circa £26m –from site demolitions / disposals / site rationalisation
Backlog figures are as per ERIC definitions i.e. exclusive of fees, VAT etc.
18
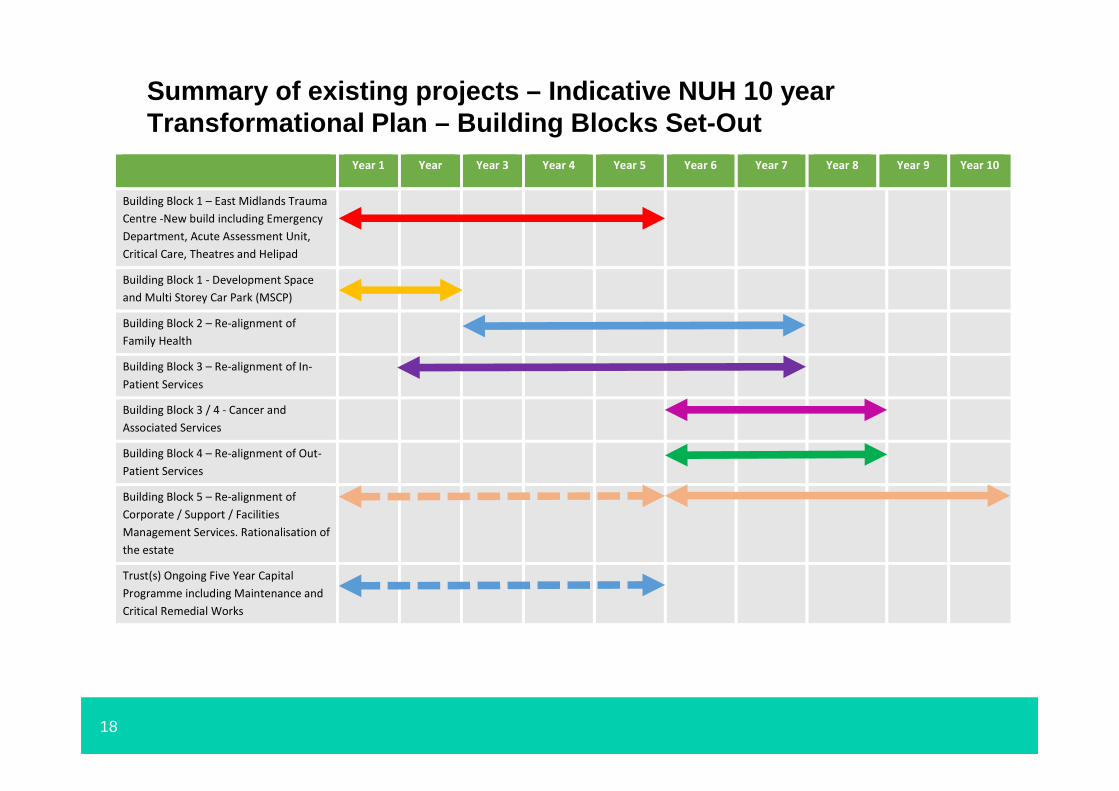
Summary of existing projects – Indicative NUH 10 yea rTransformational Plan – Building Blocks Set-Out
Year 1 Year Year 3 Year 4 Year 5 Year 6 Year 7 Year 8 Year 9 Year 10
Building Block 1 – East Midlands Trauma
Centre -New build including Emergency
Department, Acute Assessment Unit,
Critical Care, Theatres and Helipad
Building Block 1 - Development Space
and Multi Storey Car Park (MSCP)
Building Block 2 – Re-alignment of
Family Health
Building Block 3 – Re-alignment of In-
Patient Services
Building Block 3 / 4 - Cancer and
Associated Services
Building Block 4 – Re-alignment of Out-
Patient Services
Building Block 5 – Re-alignment of
Corporate / Support / Facilities
Management Services. Rationalisation of
the estate
Trust(s) Ongoing Five Year Capital
Programme including Maintenance and
Critical Remedial Works

19
Estates Composition (1 of 3)
Portfolio No. Properties
FootprintSize (Ha)
Size GIA (sqm)
Percentage Tenure split Freehold /
Leasehold
Estate Running costs pa (£m)
(rent, s’charge, FM)
Back-logMaintenance
£m
GP owned 194 TBC TBC TBC 11.1M TBC
NHS PS 59 TBC 85,060.74 44%FH, 44%LH, 2%PFI & 10% licence
21.1M TBC
CHP 12 TBC 43,649 Lift 14.1M £0
Provider estate (Acute) 5 71.87 501,153 SFHT PFI (140k) 163.2M 255.4M
Mental/Community HT 120 TBC 153,996 Freehold 24.5M 12.7M
Other 5,324 TBC TBC TBC TBC TBC
Totals 5,714 71.87 783,858.74 n/a 234M 268.5M
Functional Uses No. Properties
FootprintSize (Ha)
Size GIA (sqm)
Percentage Tenure split Freehold /
Leasehold
Estate Running costs pa (£m)
Back-logMaintenance
£m
Community FT Non Clinical TBC TBC 45983 Freehold 10.42 Non Clinical
Community FT Clinical TBC TBC 108103 Freehold 14.07 Clinical
Back Office (self contained unit)
8 TBC 8,800.11 Leasehold/Licence 3.16 None
Totals TBC TBC 162,886.11 n/a 27.6M n/a
Portfolio Summary – Other is assets known through One Public Estate programme, does not Incl. NHS. GP premises data has been extracted using NHS Premises 2015/16 data (SHAPE) - Data is a known issue that is in working progress – NHSPS Backlog is “subject to condition survey and ratification at present” – Provider data has been provided directly with sources i.e. Ha taken from SHAPE
Functional Use Summary – Offices based on NHS Proper ty Services data only which CCG’s rent/lease
20
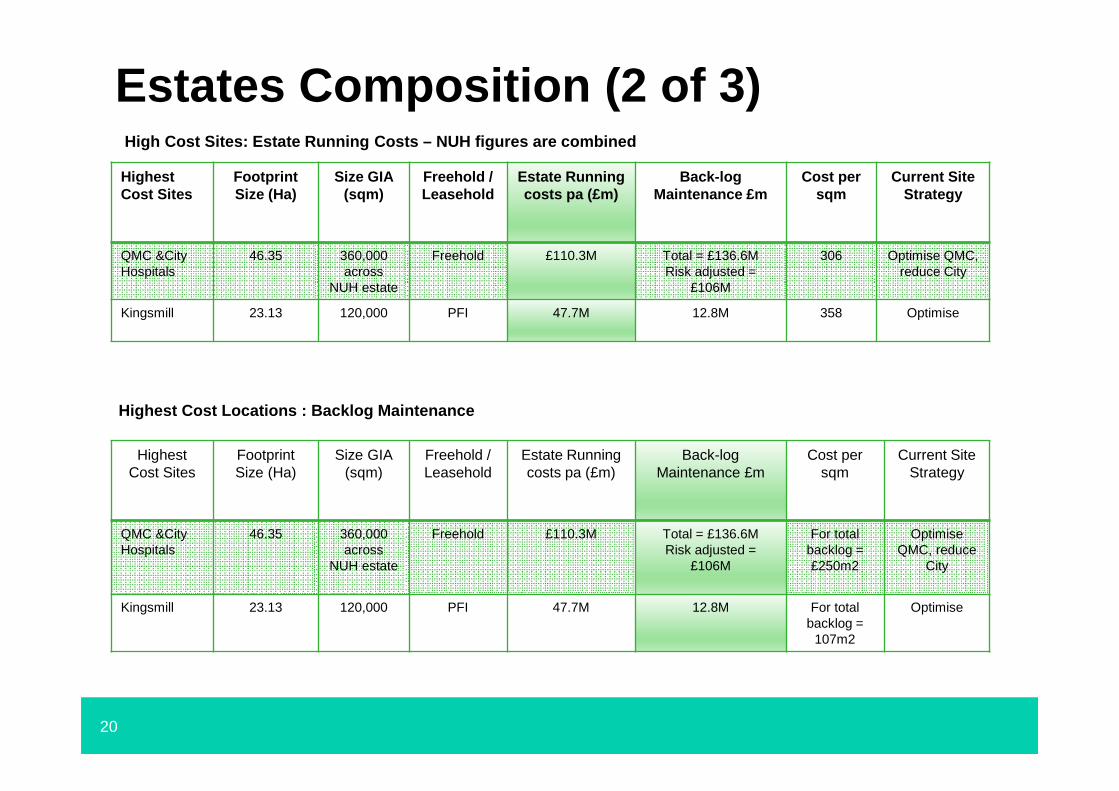
Estates Composition (2 of 3)
Highest Cost Sites
FootprintSize (Ha)
Size GIA (sqm)
Freehold / Leasehold
Estate Running costs pa (£m)
Back-logMaintenance £m
Cost per sqm
Current Site Strategy
QMC &City Hospitals
46.35 360,000 across
NUH estate
Freehold £110.3M Total = £136.6MRisk adjusted =
£106M
306 Optimise QMC, reduce City
Kingsmill 23.13 120,000 PFI 47.7M 12.8M 358 Optimise
High Cost Sites: Estate Running Costs – NUH figures are combined
Highest Cost Sites
Footprint Size (Ha)
Size GIA (sqm)
Freehold / Leasehold
Estate Running costs pa (£m)
Back-log Maintenance £m
Cost per sqm
Current Site Strategy
QMC &City Hospitals
46.35 360,000 across
NUH estate
Freehold £110.3M Total = £136.6MRisk adjusted =
£106M
For total backlog = £250m2
Optimise QMC, reduce
City
Kingsmill 23.13 120,000 PFI 47.7M 12.8M For totalbacklog =
107m2
Optimise
Highest Cost Locations : Backlog Maintenance
21
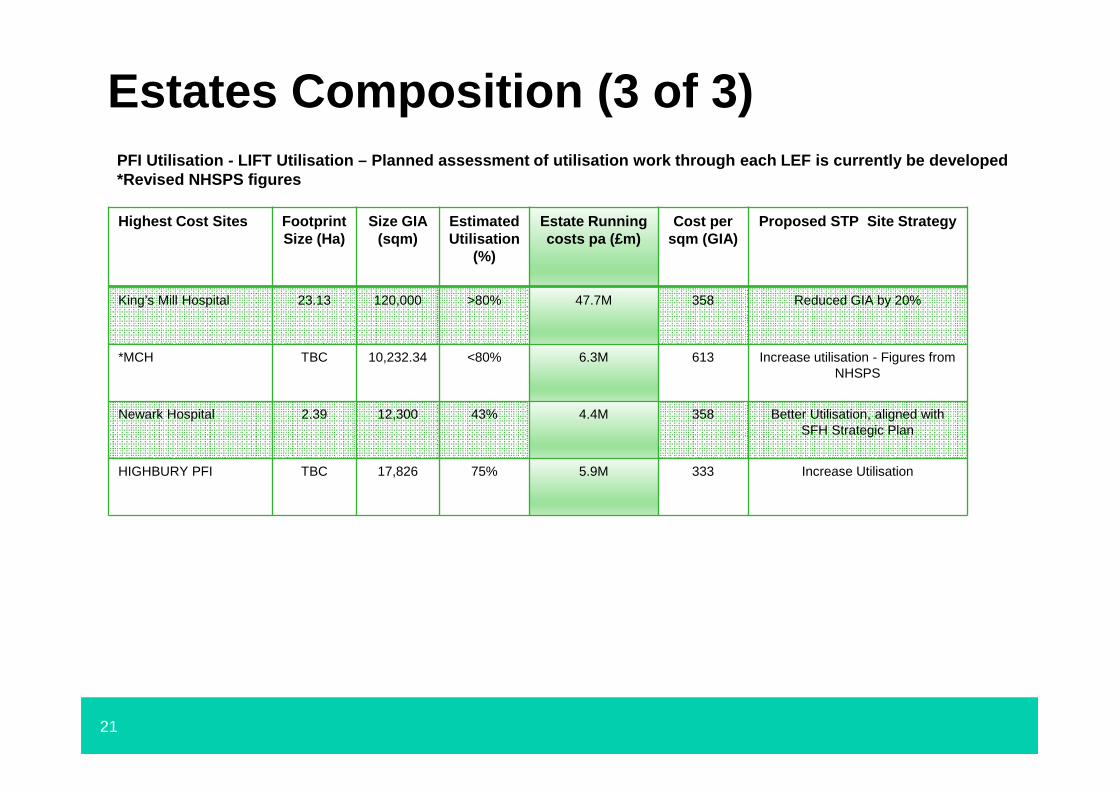
Estates Composition (3 of 3)
Highest Cost Sites FootprintSize (Ha)
Size GIA (sqm)
Estimated Utilisation
(%)
Estate Running costs pa (£m)
Cost per sqm (GIA)
Proposed STP Site Strategy
King’s Mill Hospital 23.13 120,000 >80% 47.7M 358 Reduced GIA by 20%
*MCH TBC 10,232.34 <80% 6.3M 613 Increase utilisation - Figures from NHSPS
Newark Hospital 2.39 12,300 43% 4.4M 358 Better Utilisation, aligned with SFH Strategic Plan
HIGHBURY PFI TBC 17,826 75% 5.9M 333 Increase Utilisation
PFI Utilisation - LIFT Utilisation – Planned assessme nt of utilisation work through each LEF is currentl y be developed*Revised NHSPS figures
22
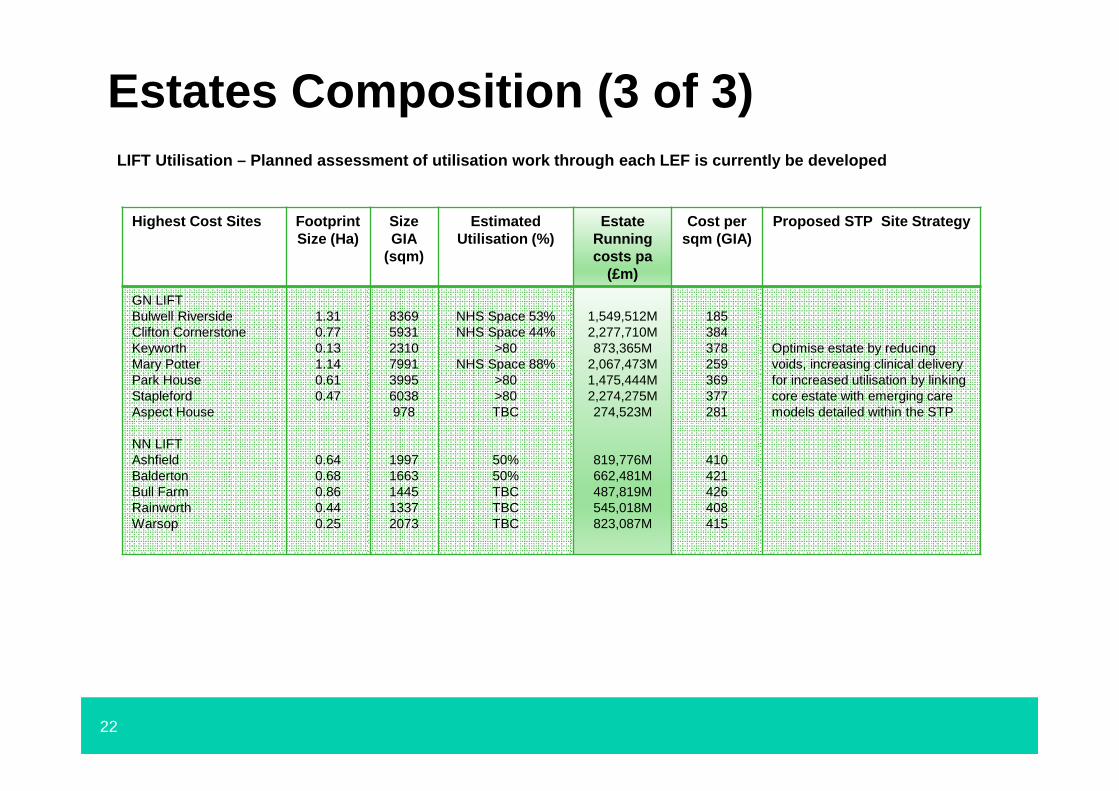
Estates Composition (3 of 3)LIFT Utilisation – Planned assessment of utilisation work through each LEF is currently be developed
Highest Cost Sites FootprintSize (Ha)
Size GIA
(sqm)
Estimated Utilisation (%)
Estate Running costs pa
(£m)
Cost per sqm (GIA)
Proposed STP Site Strategy
GN LIFTBulwell RiversideClifton CornerstoneKeyworthMary PotterPark HouseStaplefordAspect House
NN LIFTAshfieldBaldertonBull FarmRainworthWarsop
1.310.770.131.140.610.47
0.640.680.860.440.25
836959312310799139956038978
19971663144513372073
NHS Space 53%NHS Space 44%
>80NHS Space 88%
>80>80TBC
50%50%TBCTBCTBC
1,549,512M2,277,710M873,365M
2,067,473M1,475,444M2,274,275M274,523M
819,776M662,481M487,819M545,018M823,087M
185384378259369377281
410421426408415
Optimise estate by reducing voids, increasing clinical delivery for increased utilisation by linking core estate with emerging care models detailed within the STP


















