Not Simply an Ulcer. A 67-year-old woman experienced a sudden onset of right lower abdominal pain...
24
Not Simply an Ulcer
-
Upload
bernice-rose -
Category
Documents
-
view
214 -
download
0
Transcript of Not Simply an Ulcer. A 67-year-old woman experienced a sudden onset of right lower abdominal pain...

Not Simply an Ulcer

• A 67-year-old woman experienced a sudden onset of right lower abdominal pain without other associated symptoms.

• She contacted her physician who did not identify a clear etiology and referred her to a surgeon.

• The physical examination, laboratory tests and a CT scan did not demonstrate obvious abnormalities.

• The patient underwent a laparoscopy with incidental appendectomy. Her abdominal pain subsided and she returned to work.

One week later, she developed bilateral leg pain.
She described the pain as "pins and needles" that often started when she was sitting or lying down and occasionally improved when she walked slowly. She underwent a non-invasive work up of her peripheral vasculature demonstrated slightly decreased flow through the left iliac artery.
She received symptomatic therapy with naproxen and propoxyphene.

One month later, she developed intense mid-abdominal pain, nausea and low-grade fever.
She again contacted her local physician who admitted her because of partial small bowel obstruction with the diagnosis of diverticulitis.
She improved gradually with conservative management and was discharged.
Soon after discharge, she developed bilateral leg swelling and persistent fatigue.
After additional two weeks, she presented for further evaluation.
prior medical history
Her prior medical history was remarkable for recurrent bronchopulmonary problems that had been attributed to her long smoking history.

physical examination• On physical examination she was thin, but not emaci
ated. • There was no peripheral lymphadenopathy. • Bilateral wheezing became prominent during forced
expiration. • The abdominal exam revealed slight tenderness with
out guarding or rebound. • There was a large mass in the mid-abdomen and righ
t flank, measuring about 10 cm. • Normal bowel sounds were present. She had bilatera
l pitting edema up to the knees.

• The pedal pulses were palpable and strong.
• Active mobility,
• reflexes and epicritic sensory testing were normal.
laboratory tests
• The laboratory tests showed a normochromic, normocytic anemia with a hemoglobin of 10.6 g/dl,
• LDH 355 U/l,• AST 56 U/l, • alkaline phosphatase 176 U/l,• albumin of 3.1 g/dl• ++ protein in the urine.

CT
Based on her history and physical examination with a palpable mass, a computerized tomography was performed.
• This demonstrated a large mass in the epigastric area that had not been seen 2 months earlier .
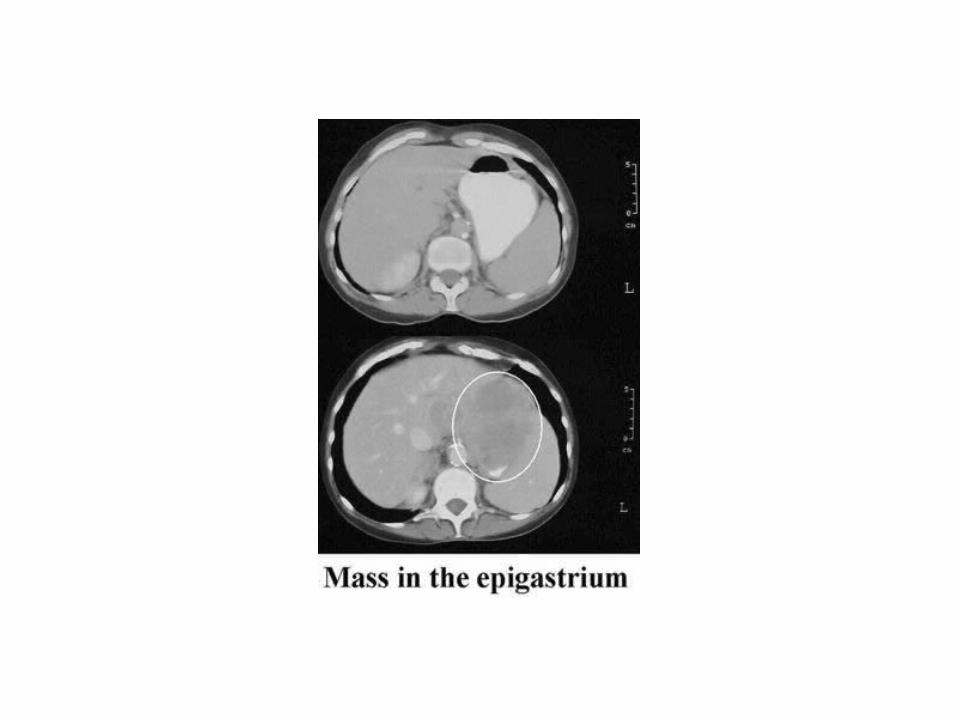

The gastric wall was thickened and irregular

• In addition, a large mass involving the lower pole of the kidney was found, which was also new compare to her prior examination . The appearance suggested a neoplasm.

upper endoscopy
In view of the abnormalities of the gastric wall, an upper endoscopy was performed.
• A small bolus was encountered right at the GE junction , which was narrow but could be passed with the endoscope.

• Immediately distal of the GE junction, an ulcerated, exophytic mass was seen .


DIAGNOSIS
• Considering the rapid growth, a lymphoma was the most likely etiology.
• Biopsies obtained from the margins revealed a high-grade lymphoma infiltrating the gastric wall.
• Similarly, tissue aspirated from the renal mass demonstrated a large cell lymphoma of the B-cell line (CD19+, lambda+).
Discussion
• Gastric lymphomas are the most commonly gastrointestinal manifestation of this group of neoplasms with nearly 50 % of primary and secondary intestinal lymphomas involving the stomach.
• Conversely, up to 5 % of gastric malignancies are lymphomas.
• H.pylori infection is associated with low-grade lymphomas (MALT lymphoma), and successful eradication may lead to a remission of the disease.
• However, a similar association has not been found for high-grade lymphomas.
• Even in patients with more localized disease, systemic chemotherapy plays the central role in the treatment.
• With modern combination therapies, complete remission rates exceeding 80 % can be achieved.
• Surgery, which certainly was not an option in the patient presented, does not significantly improve survival compared to conservative treatment.
• The patient is currently undergoing further evaluation for chemotherapy with cyclophosphamide, vincristine, doxorubicin and prednisone.