New Approaches to Care for Underserved Adolescents: The Enhanced Medical Home Seth Ammerman, M.D....
58
New Approaches to Care for Underserved Adolescents: The Enhanced Medical Home Seth Ammerman, M.D. Clinical Associate Professor Division of Adolescent Medicine Department of Pediatrics Stanford University Lucile Packard Children’s Hospital
-
Upload
archibald-moore -
Category
Documents
-
view
216 -
download
0
Transcript of New Approaches to Care for Underserved Adolescents: The Enhanced Medical Home Seth Ammerman, M.D....

New Approaches to Care for Underserved Adolescents:
The Enhanced Medical Home
Seth Ammerman, M.D.Clinical Associate Professor
Division of Adolescent MedicineDepartment of Pediatrics
Stanford UniversityLucile Packard Children’s Hospital

Goals
• Definitions and current stats for underserved youth in USA
• Key concepts of the Medical Home and the Enhanced Medical Home
• Common barriers to care• Pros and Cons of typical school-based,
community, and mobile clinic programs• Adolescent Outreach Program Lucile Packard
Children’s Hospital as a Model That Works

Definitions of Adolescents
• American Academy of Pediatrics: ages 12-21.
• Society for Adolescent Medicine and the World Health Organization: ages 10-25– Developmentally (bio-psycho-social-cognitive)
this age range makes a lot of sense.

Definitions of Underserved Adolescents
• Common Descriptive Terms: “At-Risk,” “High-Risk,” “Vulnerable,” “Underserved,” “Marginalized”
• Homeless youth (terms also include: street youth, couch surfers, street-connected, runaway, throwaway, curb-siders,) are the most disadvantaged of these youth
• Homelessness means an unstable housing situation, and ranges from living with relatives to living on the streets

Uninsured Youth USA
• Approximately 12% (5 million) adolescents do not have health insurance
• Medicaid and S-CHIP (State Child Health Insurance Programs) main programs for the poor
• Numbers of uninsured increasing

Definitions of Homelessness
• U.S. Government: Homelessness means an unstable housing situation
• Homelessness ranges from living with relatives to living on the streets
• Poverty is a common denominator for being homeless

The Latest Homeless Youth Numbers: USA
• > 1,000,000 adolescents experience homelessness in the United States each year
• Numbers increasing
• Demographics vary by region, city, and neighborhood– Minority youth over-represented – LGBTQ –I – Two Spirit youth over-represented
The Latest Homeless Youth Numbers: Local
• In San Francisco: ~2,000-3,000 homeless adolescents
• In San Mateo, ~500 homeless adolescents
• In San Jose, ~1,500 homeless adolescents



What is A “Medical Home?”
For optimal health care, a medical home provides
• Access
• Health Care, broadly defined

What is “Access?”
• “Access” is getting provider and patient together:– in the same place– at the same time – in a straightforward and easy manner

What is “Health Care?”
“Health care” broadly defined is:
• Comprehensive
• Continuous
• Youth-centered
• Affordable

What is “Health Care?” cont.
• Care provided or coordinated by a qualified primary care practitioner
• Care includes health screening, preventive care, and management of acute and chronic conditions – including organizing and f/u of sub-specialty
needs

A Medical Home is not:
• Emergency room visits
• Episodic sick care clinic visits
• Urgent care clinic visits
• Clinics not ensuring medication provision

A Medical Home is not (cont.):
• Clinics focusing on a specific problem, e.g., – STD clinics– Family Planning Clinics– Mammography Vans

A Medical Home means:
• Increased opportunities for health screening
• Preventive health interventions, including immunizations
• Timely follow-up of acute illness
• Increased opportunities for health education and anticipatory guidance

A Medical Home means, cont.
• Improved management of chronic conditions like asthma or diabetes
• Increased access to critically needed specialists
• Improved functionality and decreased cost of the health care system
• Improved health and well-being of underserved youth

What is an “Enhanced Medical Home?”
• An enhanced medical home adds to the medical home model:– Mental health services– Nutrition services– Oral Health Services– Others: acupuncture, massage therapy,
yoga, etc.

The “Enhanced Medical Home”
• Ensures the most comprehensive care for at-risk youth
• Ensures the most continuous care for at-risk youth
• Is the most focused on prevention and early intervention
• Is the most cost-effective model of health care

Barriers to Care
• Lack of health insurance is major barrier, as are insurance-related issues if one has insurance– Co-Pays for visits and for medications– No coverage for “pre-existing conditions”– Carve-outs of mental health, nutrition, dental,
and other services

Barriers to Care, cont.
• Lack of transportation is major barrier– Most youth don’t have cars or easy access to
cars– Public transportation often not simple or quick– Rural areas often without local clinics– Have to get to clinic, then to lab, then to
pharmacy, etc.

Barriers to Care: Youth-Related
• Health care is not a priority
• Denial
• Shame
• Fear
• Distrust

Barriers to Care: Youth Related, cont.
• Communication problems: illiteracy or language barriers
• Limited access to telephones, showers, and laundry facilities
• Limited or unfamiliarity with available services
• Lack of skills to manage “red tape”

Barriers to Care: System Related
• Address requirements and lengthy bureaucratic processing
• Crowded waiting rooms
• Long waits
• Not youth focused

Barriers to Care: Provider Related
• Difficulty dealing with issues around confidentiality
• Usually not “youth friendly” practice• Lack of comfort working with adolescents • Lack of experience with the range of
adolescents health care needs: medical, psychosocial, mental health, nutrition, and developmental

Legal Issues: California Law for Health Care for Minors
• Minors in California (under age 18) may consent to treatment for 3 categories of services on their own without parental consent (and for free):– Reproductive health care (birth control, STI
testing and treatment, abortions)– Substance abuse (tobacco, alcohol, and other
drugs)– Mental Health (need parental consent for meds)

California Law for Health Care for Minors, cont.
• Minors in California (under age 18) may consent to treatment for all other services on their own without parental consent if they are:– Emancipated (formal court process)– “Self-sufficient”: not living at home and not
being financially supported by their parents

The Enhanced Medical Home:New Approaches
Three major types of health care models for underserved youth
• School-based clinics
• Community fixed-site clinics
• Mobile clinics

School-Based Clinics
Pros: • Setting is where youth spend many hours a
day• Teachers, counselors, administrators, and
peer leaders can:– identify youth in need– enhance health education and health promotion– Help with follow up and case management

School-Based Clinics
Cons: • Youth needs to be attending school• “Continuation Schools” often have limited
resources for neediest youth• Often limited services – not medical home
model• Often politically charged issue in the United
States

Community Clinics
Pros:
• In neighborhoods where underserved populations live
• Typically integrated into the community
• Often hooked up with other community resources

Community Clinics
Cons:
• Variable services offered, not usually medical home model
• Typically not youth-focused
• Rarely separate adolescent services

Mobile Clinic
Pros:
• Goes to where the target patients are
• Sites can change if neighborhoods or circumstances change
• Friendly, non-intimidating environment
Mobile Clinic
Cons:
• Variable services offered, not usually medical home model
• Often a specific focus (Family planning; HIV counseling; mammography)
• Typically not youth-focused

Adolescent Outreach ProgramPackard Children’s Hospital
Enhanced medical home model
• Program begun September 1996
• Mobile Clinic (36 feet long, 2 exam rooms, and mini-pharmacy)
• Specifically targets homeless and uninsured adolescents ages 10-25: unique model

Program Components
• Clinical care to the underserved• Teaching medical students, residents, fellows, etc.
– Core component of adolescent and community medicine rotations; outstanding evaluations by trainees
• Research– Projects include juvenile delinquency and
homelessness; sexual attitudes and behaviors; nutrition knowledge, behaviors, and body image; media influence and disordered eating; emergency contraception knowledge, attitudes, and beliefs.

Personnel: Multidisciplinary
• Pediatrician/adolescent medicine specialists
• Pediatric Nurse Practitioner (female)
• Medical Assistant
• Social Worker
• Registered Dietician
• Psychiatrist (with trainees) 1x/month to Van, and refers to his office as needed

Personnel, cont.
– Van driver (registration of pts. by MA and Van driver)
– Business Manager– Administrative assistant (also performs data
collection and entry) – IT services– Most providers bilingual Spanish; some
bicultural

Finances
• Funding provided by generous philanthropic individuals, foundations, corporations, and state/local programs
• Yearly budget ~$500,000 for 2 days/week Van services, plus SW and RD outreach.
• Cost-savings (conservative estimate) of $10- for every $1 spent for this program
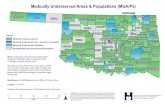
Service Sites
Services provided in Santa Clara, San Mateo, and San Francisco Counties: clinic hours correspond to site hours
• Tenderloin Recreation Center (SF) -- partners include Indochinese Development Housing Corporation and the Boys and Girls Club
• Peninsula Continuation High School (San Bruno)

Service Sites, cont.
• East Palo Alto Continuation High School (Menlo Park)
• Los Altos High School (Los Altos)
• Alta Vista Continuation High School (Mountain View)
• Emergency Housing Consortium Youth Shelter “Our House” (San Jose)

Outcomes, Teen Health Van
– Outcomes may be of 3 types, depending upon type of program• Short-term: e.g., #s of new and return
patients• Medium-term: e.g., immunization rates• Long-Term: e.g., behavior change
– Outcomes may overlap

Patient Numbers
Current statistics (through December 2008)
• > 9,000 patient visits– New patients : 31%– Return patients: 69%– Male patients: 41%– Female patients: 59%

Comprehensive & Continuous Health Services Offered
• Acute illness and injury care
• Complete history and physical exams
• Family planning
• Health education and anticipatory guidance

Comprehensive & Continuous Health Services, cont.
• HIV counseling and testing
• Immunizations
• Mental health counseling and referrals
• Nutrition counseling
• Pregnancy testing and counseling

Comprehensive & Continuous Health Services, cont.
• Referrals to collaborating agencies
• Risk reduction counseling
• Sexually transmitted infection testing and counseling
• Substance abuse counseling and referrals
• Urine, blood testing options on site for basic tests; rest to hospital lab or DPH

Components of Providing Successful Health Care
• Listen to the adolescent
• Spend time with the adolescent
• Meet the adolescent’s agenda
• Remember, you can’t do it all at once:– Continuity a must– Follow-up a must– Consistency a must
Components of Providing Successful Health Care
• Meet immediate needs first
• Then help address other aspects of their lives
• Start with clean socks, and a snack: staff and patients share the same food
• Provide clothing
Components of Providing Successful Health Care
• Provide hygiene kits
• Provide dental hygiene items
• The Human Connection: Building Trust over time is a key factor to success– We typically spend an hour with each patient– Patients typically have multiple diagnoses and
unmet health care needs: are “complex” patients

Components of Providing Successful Health Care
• Collaborate with community and neighborhood agencies that provide non-health care services and importantly that perform youth outreach and will help promote the program
• Have a formal evaluation process on a regular basis, with a designated point person: we do it Q 6 months.

Components of Providing Successful Health Care
• Collaborate with local agencies that provide health care, e.g., Juvenile Hall, Children’s Shelter
• Have all patients sign a “release of information” to ensure sharing of information with these agencies
• “Seamless” referrals; provide transportation if needed.

Components of Providing Successful Health Care
• Utilize a screening questionnaire: we have both a “Teen Questionnaire” and a “Family Planning” questionnaire.
• Explain limits of confidentiality up-front
• Let patients know you work as a team and may share information with the team as needed (with patient ok)

Components of Providing Successful Health Care
• Utilize both male and female providers• Personnel must be respectful, caring,
nonjudgmental, and enjoy adolescents• Provide comprehensive health services (“1-
stop shopping”) (pts may focus initially on only 1 service, but access others later)
• Provide medications for free at the time of the visit: significantly increases compliance

Components of Providing Successful Health Care
• Invite partners to “see you in action” – make the abstract concrete
• Steward donors
• Involve the media: newspapers, radio, and television

Components of Providing Successful Health Care
• Provide incentives: movie tickets, gift cards• Maintain privacy and confidentiality• Use peer outreach and counseling –
adolescents respond particularly well to this • Focus on the youth’s strengths and always
try to comment on successes, however small• Have ongoing youth outreach • Have fun!

References
• Brito A, Grant R, Overholt S, Aysola J, Pino I, Spalding SH, Prinz T, Redlener I. The enhanced medical home: the pediatric standard of care for medically underserved children. Adv Pediatr. 2008;55:9-28.
• Busen NH, Engebretson JC. Facilitating risk reduction among homeless and street-involved youth. J Am Acad Nurse Pract. 2008 Nov;20(11):567-75.
• Strunk JA. The effect of school-based health clinics on teenage pregnancy and parenting outcomes: an integrated literature review. J Sch Nurs. 2008 Feb;24(1):13-20.
• Fletcher CW, Slusher IL, Hauser-Whitaker M. Meeting the health care needs of medically underserved, uninsured, & underinsured Appalachians. Ky Nurse. 2006 Oct-Dec;54(4):8-9.
• Redlener I, Grant R, Krol DM. Beyond primary care: Ensuring access to subspecialists, special services, and health care systems for medically underserved children. Adv Pediatr. 2005;52:9-22.
• Forrest CB, Whelan EM. Primary care safety-net delivery sites in the United States: A comparison of community health centers, hospital outpatient departments, and physicians' offices. JAMA. 2000 Oct 25;284(16):2077-83.

Web Resources
• The Children’s Health Fund: www.chf.org• The National Health Care for the Homeless
Council: www.nhchc.org• End Homelessness:
www.endhomelessness.org• www.adolescenthealth.org• Lucile Packard Foundation for Children’s
Health: www.lpfch.org