
Neurology and the COVID-19 Pandemic
17
REVIEW Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response Brigit High*, Alison M. Hixon, PhD*, Kenneth L. Tyler, MD, Amanda L. Piquet, MD, and Victoria S. Pelak, MD Neurology: Clinical Practice April 2021 vol. 11 no. 2 e48-e63 doi:10.1212/CPJ.0000000000000908 Correspondence Dr. Pelak [email protected] Abstract Purpose of Review The current coronavirus disease 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is one of the greatest medical crises faced by our current generation of health care providers. Although much remains to be learned about the pathophysiology of SARS-CoV-2, there is both historical precedent from other coronaviruses and a growing number of case reports and series that point to neurologic consequences of COVID-19. Recent Findings Olfactory/taste disturbances and increased risk of strokes and encephalopathies have emerged as potential consequences of COVID-19 infection. Evidence regarding whether these sequelae result indirectly from systemic infection or directly from neuroinvasion by SARS-CoV-2 is emerging. Summary This review summarizes the current understanding of SARS-CoV-2 placed in context with our knowledge of other human coronaviruses. Evidence and data regarding neurologic sequelae of COVID-19 and the neuroinvasive potential of human coronaviruses are provided along with a summary of patient registries of interest to the Neurology community. Coronaviruses (CoVs) are ubiquitous pathogens and have been isolated from many animal species ranging from turkeys to bats to beluga whales. 1 CoVs belong within the taxonomic family Coronaviridae, which is further divided into 4 genera—α-, β-, γ-, and δ-CoVs. 2 There are 7 known species of human CoVs (HCoVs), and all are in the α- and β-CoV genera. 3,4 HCoVs consist of 2 α-CoVs, HCoV-NL63 and HCoV-229E, and 5 β-CoVs, HCoV-OC43, HCoV-HKU1, severe acute respiratory syndrome (SARS)-CoV-1, Middle East respiratory syndrome (MERS)-CoV, and now the recently identified SARS-CoV-2, which is responsible for the coronavirus disease 2019 (COVID-19) pandemic. 1–4 Of the 7 HCoVs, the -NL63, -229E, -OC43, and -HKU1 species are endemic worldwide and are primarily associated with mild upper respiratory disease (the common cold). 1–4 In the past 30 years, the 3 other HCoV species have now emerged to infect humans and are most well known for causing severe respiratory disease: SARS-CoV-1, MERS-CoV, and SARS-CoV-2. The modern outbreaks of these HCoVs are thought to represent bat-to-human zoonotic transmissions with the involvement of an intermediate host. Although the SARS-CoV-2 *These authors contributed equally to the manuscript. Medical Scientist Training Program (BH, AMH), Rocky Mountain Taste and Smell Center (BH), Department of Neurology (KLT, ALP, VSP), and Department of Ophthalmology (VSP), University of Colorado School of Medicine, Aurora. Funding information and disclosures are provided at the end of the article. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp. MORE ONLINE COVID-19 Resources For the latest articles, invited commentaries, and blogs from physicians around the world NPub.org/COVID19 e48 Copyright © 2020 American Academy of Neurology Copyright © 2020 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Transcript of Neurology and the COVID-19 Pandemic

REVIEW
Neurology and the COVID-19 PandemicGatheringData for an InformedResponse
Brigit High Alison M Hixon PhD Kenneth L Tyler MD Amanda L Piquet MD and Victoria S Pelak MD
Neurology Clinical Practice April 2021 vol 11 no 2 e48-e63 doi101212CPJ0000000000000908
Correspondence
Dr Pelak
victoriapelakcuanschutzedu
AbstractPurpose of ReviewThe current coronavirus disease 2019 (COVID-19) pandemic causedby the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)is one of the greatest medical crises faced by our current generation ofhealth care providers Although much remains to be learned about thepathophysiology of SARS-CoV-2 there is both historical precedent fromother coronaviruses and a growing number of case reports and series thatpoint to neurologic consequences of COVID-19
Recent FindingsOlfactorytaste disturbances and increased risk of strokes andencephalopathies have emerged as potential consequences ofCOVID-19 infection Evidence regarding whether these sequelae resultindirectly from systemic infection or directly from neuroinvasion bySARS-CoV-2 is emerging
SummaryThis review summarizes the current understanding of SARS-CoV-2 placed in context with ourknowledge of other human coronaviruses Evidence and data regarding neurologic sequelae ofCOVID-19 and the neuroinvasive potential of human coronaviruses are provided along with asummary of patient registries of interest to the Neurology community
Coronaviruses (CoVs) are ubiquitous pathogens and have been isolated from many animalspecies ranging from turkeys to bats to beluga whales1 CoVs belong within the taxonomicfamily Coronaviridae which is further divided into 4 generamdashα- β- γ- and δ-CoVs2 Thereare 7 known species of human CoVs (HCoVs) and all are in the α- and β-CoV genera34
HCoVs consist of 2 α-CoVs HCoV-NL63 and HCoV-229E and 5 β-CoVs HCoV-OC43HCoV-HKU1 severe acute respiratory syndrome (SARS)-CoV-1 Middle East respiratorysyndrome (MERS)-CoV and now the recently identified SARS-CoV-2 which is responsiblefor the coronavirus disease 2019 (COVID-19) pandemic1ndash4
Of the 7 HCoVs the -NL63 -229E -OC43 and -HKU1 species are endemic worldwide andare primarily associated with mild upper respiratory disease (the common cold)1ndash4 In the past30 years the 3 other HCoV species have now emerged to infect humans and are most wellknown for causing severe respiratory disease SARS-CoV-1 MERS-CoV and SARS-CoV-2The modern outbreaks of these HCoVs are thought to represent bat-to-human zoonotictransmissions with the involvement of an intermediate host Although the SARS-CoV-2
These authors contributed equally to the manuscript
Medical Scientist Training Program (BH AMH) Rocky Mountain Taste and Smell Center (BH) Department of Neurology (KLT ALP VSP) and Department of Ophthalmology (VSP)University of Colorado School of Medicine Aurora
Funding information and disclosures are provided at the end of the article Full disclosure form information provided by the authors is available with the full text of this article atNeurologyorgcp
MORE ONLINE
COVID-19 ResourcesFor the latest articlesinvited commentaries andblogs from physiciansaround the world
NPuborgCOVID19
e48 Copyright copy 2020 American Academy of Neurology
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
outbreak was first associated with workers at a live animalmarket in Wuhan China the exact origin and evolution ofthis virus remains to be fully delineated56
Basic VirologyCoV virions are 125 μm in diameter and are composed of ahost-derived lipid envelope surrounding a helical nucleocapsidwith a single strand of positive-sense RNA (+ssRNA) as the viralgenome47 (figure 1) CoV genome sizes range from 26 to 32 kband are the largest known +ssRNA viral genome8 These ge-nomes encode viral proteins that assist in different steps of theviral life cycle and thus are potential vaccine targets CoVs arenamed for their distinctive crown-like appearance under electronmicroscopy resulting from a radiating array of spike (S) proteinsprojecting from the viral envelope17 The S protein is critical forCoV binding to cell receptors In addition the viral genomeencodes other structural proteins including the membrane (M)protein which helps to shape the viral envelope and disrupt hostinterferons and envelope (E) protein which participates in var-ious stages of the viral life cycle and contributes to host cell death(figure 1)1910 The nucleocapsid (N) protein which surroundsthe RNA genome acts as an RNA chaperone (figure 1)179
The significance of the genomic differences betweenSARS-CoV-2 and the other modern HCoVs and the implications for diseasephenotype and tropism remains to be fully characterized Fol-lowing identification of the first case cluster inWuhan China inlate December 2019 the pathogen was isolated by January 72020 and the whole-genome sequence was shared with theWorld Health Organization only 5 days later on January 12202011 The available sequencing data indicate that the genomesize is 298 kb with 14 open reading frames encoding 27 pro-teins8 SARS-CoV-2 appears more closely related to SARS-CoV-1 (79 homology) and more distantly related to MERS-CoV(50 homology)6812 Like SARS-CoV-1 SARS-CoV-2 usesthe angiotensin-converting enzyme 2 (ACE-2) receptor andappears to have a 4- to 20-fold higher ACE-2 binding affinity
than SARS-CoV-113ndash15 SARS-CoV-2 also appears to have theability to use a host protease furin to cleave the viral Sprotein This furin cleavage site is not found in SARS-CoV-1and its exact function in the SARS-CoV-2 life cycle has yet to bedetermined15 Acquisition of mutations allowing for furincleavage has been seen in other viruses such as influenza andMERS-CoV and has been implicated in causing increasedvirulence and promoting cross-species transmission1617 Itmay function in enhancing viral fusion following receptorbinding or assist in viral exit from an infected cell
Clinical Spectrum and Transmissionof COVID-19As of May 30 2020 there have been over 59 million confirmedcases of COVID-19 worldwide with over 365000 deaths18 Theglobal case fatality rate is estimated to range from 2 to 5although testing variability between countriesmdashincluding a lackof testing formild and asymptomatic casesmdashlikely overestimatesthis range19 In most instances COVID-19 is less lethal than thedisease caused by SARS-CoV-1 which had a case fatality rate of11However the higher rate of human-to-human transmissionof SARS-CoV-2 has created a global pandemic with dire impli-cations for health care capacity SARS-CoV-2 is thought to betransmitted primarily through respiratory droplets when aninfected person coughs or sneezes (figure 2A)20 The virus canremain viable on various surfaces thus allowing potential fomitetransmission20 Finally asymptomatic carriers who tend to beyounger and healthier than those with moderate or severecourses of disease are increasingly being recognized as drivers ofdisease propagation However the exact prevalence of this groupis unclear due to gaps in testing2122
The incubation time to symptom onset following exposure canrange from2 to14 days (mean 5 days)2324 Typical COVID-19presenting symptoms include fever cough and shortness ofbreath25 Chest CT abnormalities are observed in nearly allhospitalized patients with COVID-19 and consist of ground-
Figure 1 Schematic of a SARS-CoV-2 Virion
The image depicts the severe acute respiratory syndrome coro-navirus 2 (SARS-CoV-2) virion with lipid bilayer membrane andshows the structural spike (S) membrane (M) envelope (E) andnucleocapsid (N) proteins The virion contains a single-strandpositive-sense RNA (+ssRNA) genome surrounded by its N proteinchaperone The S M E and N proteins are possible targets forvaccine development
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e49
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 2 Proposed Pathways of SARS-CoV-2 Systemic Infection and Neuroinvasion
(A) Initial infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with viral entry into the nasopharynx oropharynx larynx andlungs (B) Magnified cross-section of a lung alveolus and capillary SARS-CoV-2 is known to infect type II pneumocytes as well as endothelial cells whichexpress the angiotensin-converting enzyme 2 (ACE-2) From the lungs the virus could enter the vasculature and circulate to other organs resulting inmultiorgan infection and sepsis Inflammation of cells such as neutrophils monocytes and lymphocytes could contribute to viral access to thevasculature due capillary leakage and direct tissue damage Thismay also be an initial site for viral infection of immune cells such asmacrophages andlymphocytes which have been shown to become infected by other coronaviruses such as SARS-CoV-1 and express the ACE-2 receptor (C) Sagittalcross-section of the brain at the level of the third and fourth ventricles with surrounding structures Hematogenous spread could lead to direct viralinfection of the CNS or infection of the CNS via the circumventricular organs (CVOs) including the subfornical organs the vascular organ of the laminaterminalis (OVLT) the median eminence and the area postrema which do lack a blood-brain barrier and have been shown to express ACE-2 SARS-CoV-2 may also access the CNS via the choroid plexus depicted on the roof of the third ventricle and in the fourth ventricle Virus could infect thevasculature of these regions which expresses ACE-2 or traffic into the CNS via infected lymphocytes (D) Sagittal cross-section of the upper re-spiratory tract SARS-CoV-2 infection has been associated with hyposmia and hypogeusia in a significant number of patients ACE-2 has been found inthe non-neuronal cells of the olfactory system suggesting dysfunction damage to non-neuronal cells as a cause of anosmia Hypogeusia could becaused by viral infection of gustatory neurons of cranial nerves VII (chorda tympani of the facial nerve) CN IX and CN X all of which project to thenucleus of the solitary tract in the brainstem and are known to express ACE-2 Gustatory pathways could contribute to viral CNS access to thebrainstem that ultimately contributes to respiratory dysfunction Infection of the brainstem could worsen respiratory distress in patients with severeCOVID-19 For all panels SARS-CoV-2 virions are depicted as green dots Black or white arrows show possible directions of viral spread in each organor tissue
e50 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
glass opacities with bilateral multiple lobular and subsegmentalareas of consolidation2526 Most symptomatic individualshave a mild course that resolves without the need for hos-pitalization but infection can rapidly progress to severedisease with multiorgan failure and death2427 Severe com-plications of COVID-19 include acute respiratory distresssyndrome acute kidney injury acute cardiac disease anddisseminated intravascular coagulopathy and laboratory find-ings can include leukopenia lymphopenia or lymphocytosisabnormal liver enzymes elevated D-dimer and elevatedinflammatory markers (eg interleukin [IL]-6 ferritin andC-reactive protein)1924
The risk of developing severe COVID-19 increases pro-gressively with age Individuals gt65 years in age are more likelyto experience hospitalization intensive care unit admissionmechanical ventilation and death compared with youngerpeople252829 These epidemiologic patterns of COVID-19 aresimilar to those seen with SARS-CoV-1 and MERS-CoV3031
Although children tend to experience milder symptoms and abetter prognosis compared with adults there have beenemerging reports from Europe and North America of multi-system inflammatory conditions like that of Kawasaki diseaseand hyperinflammatory shock syndrome in children andadolescents3233 The association between SARS-CoV-2 andsevere pediatric disease is likely a reflection the size of the globaloutbreak in diverse populations rather than increased virulenceof the SARS-CoV-2 compared with other modern HCoVs
For the 3 modern HCoVsmdashSARS-CoV-1 MERS and SARS-CoV-2mdasha key feature of severe disease is a dysregulated im-mune response that damages the lungs and organs above andbeyond the direct viral damage1034 The exact mechanismsdriving this hyperinflammatory immunopathology are not wellunderstood and may be multifactorial10 Overall individualswith severe disease appear to have rapid viral replication in thelungs with increases in alveolar macrophages and proin-flammatory cytokines including tumor necrosis factor-α IL-1IL-6 and ferritin34 Seemingly paradoxically as many as 80 ofpatients with COVID-19 develop lymphopenia35 The exactcause of lymphopenia is unknown but could be due to tissueredistribution to areas of infection (lungs) direct viral infectionof lymphocytes followed by cell death or cytokine-inducedlymphotoxicity103436 Together these factors promotemassiveinflammation and cytokine storm
Health-related comorbidities also contribute to the de-velopment of severe disease with 94 of deaths occurring inpatientswith at least 1 comorbidity37 Conditions increasing therisk of severe disease include diabetes hypertension Class IIIobesity (body mass index gt40 kgm2) severe or chronic car-diac disease chronic lung disease including moderate to severeasthma and being male37 Members of racial minorities in theUnited States are at a higher risk of poor outcomes that aremost likely due to inequalities in medical care and the higherprevalence of comorbidities in this population driven by healthdisparities38 The relationship between these comorbidities and
development of cytokine storm could be driven by changes inreceptor expression and dysregulation of innate immunity andinflammation that can occur in these disease states amongother hypotheses
Neurologic Sequelae of SARS-CoV-2and COVID-19Although COVID-19 is primarily a disease of the re-spiratory tract neurologic symptoms are increasingly beingrecognized39ndash50 With a rapid rise in severely ill patients ner-vous system manifestations can be overlooked masked by se-dation during ventilation or be of lower priority when severerespiratory and cardiac compromise occur The neurologicsequelae that have been described to date are discussed withattention to available evidence for indirect direct or post-infectious mechanisms
Olfactory and Taste DisturbancesThe CDC recently expanded the COVID-19 symptom listfrom the typical fever cough and shortness of breath triad toinclude sudden onset of taste andor smell loss37 Table 1summarizes studies focusing on tastesmell dysfunction withCOVID-19 The prevalence of these symptoms among pa-tients with COVID-19 is estimated around 5273 (95confidence interval [CI] 2964ndash7523) for olfactorydysfunction and 4393 (95 CI 2046ndash6895) for gus-tatory dysfunction in a meta-analysis of published reportsbefore April 19 202051 The timing of onset of the olfactorytaste disorders presents particular interest because they mayoccur earlier than other hallmark features of COVID-19(fever or cough) which opens the possibility of using themas initial screening measures52 In a cohort of hospitalizedpatients in Milan Italy 20 experienced smell and tastedisturbance before admission whereas the remainderreported these disturbances during their hospital stay39
Taste alterations were noted to be more prevalent beforehospitalization (91) whereas taste and smell changes wereequally prevalent during hospitalization39 In other anotherreport symptoms of loss of taste smell or both have beennoted to persist for up to several weeks41 Although olfactorydisturbances are common in other upper respiratory illnessesof viral origin due to sinonasal symptoms (rhinorrhea andcongestion) these are less commonly observed in patientswith COVID-1951 The lack of sinonasal symptoms suggestsviral-mediated dysfunction of gustatory and olfactory organsrather than inflammatory damage however the exact mecha-nisms remain to be determined
Cerebrovascular DiseaseA small but growing number of reports suggest an increasedrisk of stroke as a potential complication of COVID-19 in-fection (table 2)4253ndash56 Predisposition to stroke may berelated to an infection-induced coagulopathy as indicated byelevated D-dimer elevated fibrinogen and thrombocytope-nia common in patients with severe COVID-19 disease54
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e51
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 1 Summary of Current Reports on Acute Taste and Smell Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Evaluation Reference
Multicenter questionnaire Belgium FranceSpain and Italy
417 patients mean age 369 y(range 19ndash77 y) female 263(631) male 154 (369) allwith mild COVID-19
Anosmia or hyposmia856 dysgeusia 880
Online questionnaire of OlfactoryDisordersmdashNegative Statements
Lechien et al 202041
Case report Aarhus Denmark Female patient in early 30swithmild COVID-19
Anosmia and hypogeusia Anosmia verified with Sniffin Sticks extendedtest (848) hypogeusia verified with tastespray screening (24) taste drop test (2440)and taste strips (1216)
Haldrup et al 202040
Single-center cross-sectional survey Milan Italy 59 patients median age 60 y(range 50ndash74 y) female 29(322) male 30 (678) allwere hospitalized with COVID-19 but capable of completingthe survey
Sudden onset olfactory ortaste disorder in 20patients (339)
Self-reported Giacomelli et al 202039
Case series Padua Italy 6 patients no furtherdescriptions given
Sudden-onset hyposmiaand hypogeusia as only ormain COVID-19 symptom
Suprathreshold Odor Rating Test using sixodors to confirm hyposmia
Marchese-Ragona et al202044 (note nonndashpeer-reviewed report)
Case control Tehran Iran 60 hospitalized patients withCOVID-19 median age 4655 plusmn1217 y female 40 (67) male20 (33) COVID-19 diseasemild (42) moderate (48)and severe (10)
Mild microsmia (13)moderate microsmia(27) severe microsmia(33) and anosmia (25)
University of Pennsylvania SmellIdentification Test of 40 odorants
Moein et al 202045
Retrospective observational Mulhouse France 54 (47) of 114 examined andor hospitalized patients withCOVID-19 with reportedanosmia mean age 47 plusmn 16 yfemale 36 (67)male 18 (33)
Anosmia mean duration89 plusmn 63 d anosmiadeveloped 44 plusmn 19 d afterinfection onset dysgeusiain 85
Self-reported Klopfenstein et al 2020102
Retrospective review Tehran Iran 8 patients with sudden-onsetanosmia 5 COVID-19+ agerange 22ndash44 y female 6 (75)male 2 (25)
Anosmia in 88 patientsonset between 2 and 4d after fever ageusia in 28 patients
Self-reported Gilani et al 2020103
Case report Madrid Spain 40-y-old Venezuelan femaleradiologist caring for multiplesymptomatic patients withCOVID-19
Anosmia 3 d aftersymptom onset anosmiaresolved after 14 d
Self-reported Ollarves-Carrero et al2020104
Case series Washington DC 177 pediatric and young adultpatients (25hospitalized 20critically ill) male 92 (52)female 85 (48)
Loss of taste and smell in15 (9) patients
Methods not described DeBaisi et al 2020105
Abbreviation COVID-19 = coronavirus disease 2019
e52
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
3 centersretrospective
Wuhan Hubei China 214 patients mean age527 plusmn 155 y female 127(593) male 87 (407)severe COVID-19 88(411)
Any neurologic signs orsymptoms 78 (364) CNSsigns or symptoms(dizziness headacheimpaired consciousnessacute cerebrovasculardisease ataxia and seizure)53 (248) PNS signs orsymptoms (tasteimpairment smellimpairment visionimpairment and nervepain) 19 (89)
None described Patients with severesymptoms uarr CRP D-dimer darrlymphocytes uarr BUNCr
Mao et al 202043
Single-centerretrospective
Wuhan Hubei China 221 patients mean age533 plusmn 159 y female 90(40middot7)male 131 (59middot3)severe COVID-19 94(42middot5)
AIS 11 (5) CVST 1 (0middot5)CH 1 (0middot5)
Representative brain CTsshowing new-onset AISCVST and left basalganglia CH
Blood from patients with AISCVSTCH showed uarr WBCsneutrophils CRP D-dimer darrlymphocytes
Li et al 202042
Case report Shimokato ChuoYamanashi Japan
24-y-old man withheadache fatigue andfever
Altered mental statusseizures meningitisencephalitis
Brain MRI DWI showinghyperintensities along theright lateral ventricleFLAIR showinghyperintense signals inthe mesial temporal lobeand hippocampus T2WIshowing pan-paranasalsinusitis
CSF uarr opening pressure uarrWBCs SARS-CoV-2+ by RT-PCR blood uarr WBCs uarr CRP
Moriguchi et al 202046
Case report Beijing Hebei China 56-y-old patient ofunknown sex
Viral encephalitis None CSF SARS-CoV-2+ by RT-PCR Zhou et al 202050
(note nonndashpeer-reviewedreport)
Case report Detroit MI Female patient age in late50s with 3 d of cough andfever with COVID-19 innasal swab
Altered mental status andnecrotizing hemorrhagicencephalopathy
Head CT with symmetrichypoattenuation withinbilateral medial thalamiwith normal CT angiogramand venogram brain MRIwith hemorrhagic rim-enhancing lesions withinbilateral thalami medialtemporal lobes andsubinsular regions
CSF traumatic punctureunable to test for SARS-CoV-2via RT-PCR
Poyiadji et al 202047
Retrospectivecase study
Leiden and Rotterdamthe Netherlands
Analysis of 184 COVID-19+admitted to the ICUs of 3hospitals for 1 mo 3184(16) had strokes patientcharacteristics notdescribed
COVID-19 pneumoniarequiring ICU admissionfollowed by development ofcoagulopathy and stroke
Ischemia strokediagnosed with CT
None described Klok et al 202053
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e53
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series New York NY 5 adult patients aged33ndash49 y 1 female 4 maleswith mild COVID-19
2 patients wereasymptomatic with COVID-19 3 had fever cough orfatigue all developedsymptoms of severe strokewith reducedconsciousness gaze palsydysarthria andorhemiplegia
CT CTA CTP andor MRIshowed large vesselocclusions in all patients
Blood uarr fibrinogen (60) uarr D-dimer (60)
Oxley et al 202055
Case report Barcelona CataloniaSpain
50-y-old man with severeCOVID-19
While in ICU with bilateralpneumonia developedacute-onset right facialparalysis and left limbweakness
Head CT perfusion mapshowed hypoperfusion inthe left paramedianthalamic artery head MRIshowed left medialthalamic infarct
None described Rudilosso et al 202056
Case series Wuhan Hubei China 69-y-old male 70-y-oldmale and 65-y-old femalepatients with severeCOVID-19
Presentedwith fever coughdyspnea and headache andlater developed evidencecerebral infarcts 1 patientalso had distal limbischemia
Head CT showed diffuseacute cerebral infarctionsin cerebral hemispheresin all patients 2 patientsalso had cerebellarinfarctions
Blood darr lymphocytes darrplatelets uarr D-dimer uarrfibrinogen all had positiveanticardiolipin IgA andantindashβ2-glycoprotein I IgAand IgG
Zhang et al 202058
Case report Boca Raton FL 74-y-old male patient withsevere COVID-19
Fever cough headache andaltered mental status
Head CT showed evidenceof distant posteriorcerebral artery strokeEEG described asconsistent withencephalopathy lefttemporal lobedysfunction and possibleepileptogenicity
CSF no evidence of infection Filatov et al 202059
Rome Italy 78-y-old female patientwith mild COVID-19
Focal status epilepticusfollowed by fever 12 h later
Head MRI showed noevidence of new cerebrallesions ictal EEG showedseizure activity localizedover left-fronto-centro-temporal regions
Blood darr lymphocytes darrplatelets uarr CRP
Vollono et al 202061
Case report Jingzhou China 66-y-old female patientwith moderate COVID-19
Progressive arm and legweakness with decreaseddistal sensationmdashtreatedwith IVIg
Nerve conduction studiessupporting demyelinatingneuropathy
SARS-CoV-2 in oropharyngealswab by RT-PCRlymphocytopeniathrombocytopenia normalCSF
Zhao et al 202049
Continued
e54
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

outbreak was first associated with workers at a live animalmarket in Wuhan China the exact origin and evolution ofthis virus remains to be fully delineated56
Basic VirologyCoV virions are 125 μm in diameter and are composed of ahost-derived lipid envelope surrounding a helical nucleocapsidwith a single strand of positive-sense RNA (+ssRNA) as the viralgenome47 (figure 1) CoV genome sizes range from 26 to 32 kband are the largest known +ssRNA viral genome8 These ge-nomes encode viral proteins that assist in different steps of theviral life cycle and thus are potential vaccine targets CoVs arenamed for their distinctive crown-like appearance under electronmicroscopy resulting from a radiating array of spike (S) proteinsprojecting from the viral envelope17 The S protein is critical forCoV binding to cell receptors In addition the viral genomeencodes other structural proteins including the membrane (M)protein which helps to shape the viral envelope and disrupt hostinterferons and envelope (E) protein which participates in var-ious stages of the viral life cycle and contributes to host cell death(figure 1)1910 The nucleocapsid (N) protein which surroundsthe RNA genome acts as an RNA chaperone (figure 1)179
The significance of the genomic differences betweenSARS-CoV-2 and the other modern HCoVs and the implications for diseasephenotype and tropism remains to be fully characterized Fol-lowing identification of the first case cluster inWuhan China inlate December 2019 the pathogen was isolated by January 72020 and the whole-genome sequence was shared with theWorld Health Organization only 5 days later on January 12202011 The available sequencing data indicate that the genomesize is 298 kb with 14 open reading frames encoding 27 pro-teins8 SARS-CoV-2 appears more closely related to SARS-CoV-1 (79 homology) and more distantly related to MERS-CoV(50 homology)6812 Like SARS-CoV-1 SARS-CoV-2 usesthe angiotensin-converting enzyme 2 (ACE-2) receptor andappears to have a 4- to 20-fold higher ACE-2 binding affinity
than SARS-CoV-113ndash15 SARS-CoV-2 also appears to have theability to use a host protease furin to cleave the viral Sprotein This furin cleavage site is not found in SARS-CoV-1and its exact function in the SARS-CoV-2 life cycle has yet to bedetermined15 Acquisition of mutations allowing for furincleavage has been seen in other viruses such as influenza andMERS-CoV and has been implicated in causing increasedvirulence and promoting cross-species transmission1617 Itmay function in enhancing viral fusion following receptorbinding or assist in viral exit from an infected cell
Clinical Spectrum and Transmissionof COVID-19As of May 30 2020 there have been over 59 million confirmedcases of COVID-19 worldwide with over 365000 deaths18 Theglobal case fatality rate is estimated to range from 2 to 5although testing variability between countriesmdashincluding a lackof testing formild and asymptomatic casesmdashlikely overestimatesthis range19 In most instances COVID-19 is less lethal than thedisease caused by SARS-CoV-1 which had a case fatality rate of11However the higher rate of human-to-human transmissionof SARS-CoV-2 has created a global pandemic with dire impli-cations for health care capacity SARS-CoV-2 is thought to betransmitted primarily through respiratory droplets when aninfected person coughs or sneezes (figure 2A)20 The virus canremain viable on various surfaces thus allowing potential fomitetransmission20 Finally asymptomatic carriers who tend to beyounger and healthier than those with moderate or severecourses of disease are increasingly being recognized as drivers ofdisease propagation However the exact prevalence of this groupis unclear due to gaps in testing2122
The incubation time to symptom onset following exposure canrange from2 to14 days (mean 5 days)2324 Typical COVID-19presenting symptoms include fever cough and shortness ofbreath25 Chest CT abnormalities are observed in nearly allhospitalized patients with COVID-19 and consist of ground-
Figure 1 Schematic of a SARS-CoV-2 Virion
The image depicts the severe acute respiratory syndrome coro-navirus 2 (SARS-CoV-2) virion with lipid bilayer membrane andshows the structural spike (S) membrane (M) envelope (E) andnucleocapsid (N) proteins The virion contains a single-strandpositive-sense RNA (+ssRNA) genome surrounded by its N proteinchaperone The S M E and N proteins are possible targets forvaccine development
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e49
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 2 Proposed Pathways of SARS-CoV-2 Systemic Infection and Neuroinvasion
(A) Initial infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with viral entry into the nasopharynx oropharynx larynx andlungs (B) Magnified cross-section of a lung alveolus and capillary SARS-CoV-2 is known to infect type II pneumocytes as well as endothelial cells whichexpress the angiotensin-converting enzyme 2 (ACE-2) From the lungs the virus could enter the vasculature and circulate to other organs resulting inmultiorgan infection and sepsis Inflammation of cells such as neutrophils monocytes and lymphocytes could contribute to viral access to thevasculature due capillary leakage and direct tissue damage Thismay also be an initial site for viral infection of immune cells such asmacrophages andlymphocytes which have been shown to become infected by other coronaviruses such as SARS-CoV-1 and express the ACE-2 receptor (C) Sagittalcross-section of the brain at the level of the third and fourth ventricles with surrounding structures Hematogenous spread could lead to direct viralinfection of the CNS or infection of the CNS via the circumventricular organs (CVOs) including the subfornical organs the vascular organ of the laminaterminalis (OVLT) the median eminence and the area postrema which do lack a blood-brain barrier and have been shown to express ACE-2 SARS-CoV-2 may also access the CNS via the choroid plexus depicted on the roof of the third ventricle and in the fourth ventricle Virus could infect thevasculature of these regions which expresses ACE-2 or traffic into the CNS via infected lymphocytes (D) Sagittal cross-section of the upper re-spiratory tract SARS-CoV-2 infection has been associated with hyposmia and hypogeusia in a significant number of patients ACE-2 has been found inthe non-neuronal cells of the olfactory system suggesting dysfunction damage to non-neuronal cells as a cause of anosmia Hypogeusia could becaused by viral infection of gustatory neurons of cranial nerves VII (chorda tympani of the facial nerve) CN IX and CN X all of which project to thenucleus of the solitary tract in the brainstem and are known to express ACE-2 Gustatory pathways could contribute to viral CNS access to thebrainstem that ultimately contributes to respiratory dysfunction Infection of the brainstem could worsen respiratory distress in patients with severeCOVID-19 For all panels SARS-CoV-2 virions are depicted as green dots Black or white arrows show possible directions of viral spread in each organor tissue
e50 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
glass opacities with bilateral multiple lobular and subsegmentalareas of consolidation2526 Most symptomatic individualshave a mild course that resolves without the need for hos-pitalization but infection can rapidly progress to severedisease with multiorgan failure and death2427 Severe com-plications of COVID-19 include acute respiratory distresssyndrome acute kidney injury acute cardiac disease anddisseminated intravascular coagulopathy and laboratory find-ings can include leukopenia lymphopenia or lymphocytosisabnormal liver enzymes elevated D-dimer and elevatedinflammatory markers (eg interleukin [IL]-6 ferritin andC-reactive protein)1924
The risk of developing severe COVID-19 increases pro-gressively with age Individuals gt65 years in age are more likelyto experience hospitalization intensive care unit admissionmechanical ventilation and death compared with youngerpeople252829 These epidemiologic patterns of COVID-19 aresimilar to those seen with SARS-CoV-1 and MERS-CoV3031
Although children tend to experience milder symptoms and abetter prognosis compared with adults there have beenemerging reports from Europe and North America of multi-system inflammatory conditions like that of Kawasaki diseaseand hyperinflammatory shock syndrome in children andadolescents3233 The association between SARS-CoV-2 andsevere pediatric disease is likely a reflection the size of the globaloutbreak in diverse populations rather than increased virulenceof the SARS-CoV-2 compared with other modern HCoVs
For the 3 modern HCoVsmdashSARS-CoV-1 MERS and SARS-CoV-2mdasha key feature of severe disease is a dysregulated im-mune response that damages the lungs and organs above andbeyond the direct viral damage1034 The exact mechanismsdriving this hyperinflammatory immunopathology are not wellunderstood and may be multifactorial10 Overall individualswith severe disease appear to have rapid viral replication in thelungs with increases in alveolar macrophages and proin-flammatory cytokines including tumor necrosis factor-α IL-1IL-6 and ferritin34 Seemingly paradoxically as many as 80 ofpatients with COVID-19 develop lymphopenia35 The exactcause of lymphopenia is unknown but could be due to tissueredistribution to areas of infection (lungs) direct viral infectionof lymphocytes followed by cell death or cytokine-inducedlymphotoxicity103436 Together these factors promotemassiveinflammation and cytokine storm
Health-related comorbidities also contribute to the de-velopment of severe disease with 94 of deaths occurring inpatientswith at least 1 comorbidity37 Conditions increasing therisk of severe disease include diabetes hypertension Class IIIobesity (body mass index gt40 kgm2) severe or chronic car-diac disease chronic lung disease including moderate to severeasthma and being male37 Members of racial minorities in theUnited States are at a higher risk of poor outcomes that aremost likely due to inequalities in medical care and the higherprevalence of comorbidities in this population driven by healthdisparities38 The relationship between these comorbidities and
development of cytokine storm could be driven by changes inreceptor expression and dysregulation of innate immunity andinflammation that can occur in these disease states amongother hypotheses
Neurologic Sequelae of SARS-CoV-2and COVID-19Although COVID-19 is primarily a disease of the re-spiratory tract neurologic symptoms are increasingly beingrecognized39ndash50 With a rapid rise in severely ill patients ner-vous system manifestations can be overlooked masked by se-dation during ventilation or be of lower priority when severerespiratory and cardiac compromise occur The neurologicsequelae that have been described to date are discussed withattention to available evidence for indirect direct or post-infectious mechanisms
Olfactory and Taste DisturbancesThe CDC recently expanded the COVID-19 symptom listfrom the typical fever cough and shortness of breath triad toinclude sudden onset of taste andor smell loss37 Table 1summarizes studies focusing on tastesmell dysfunction withCOVID-19 The prevalence of these symptoms among pa-tients with COVID-19 is estimated around 5273 (95confidence interval [CI] 2964ndash7523) for olfactorydysfunction and 4393 (95 CI 2046ndash6895) for gus-tatory dysfunction in a meta-analysis of published reportsbefore April 19 202051 The timing of onset of the olfactorytaste disorders presents particular interest because they mayoccur earlier than other hallmark features of COVID-19(fever or cough) which opens the possibility of using themas initial screening measures52 In a cohort of hospitalizedpatients in Milan Italy 20 experienced smell and tastedisturbance before admission whereas the remainderreported these disturbances during their hospital stay39
Taste alterations were noted to be more prevalent beforehospitalization (91) whereas taste and smell changes wereequally prevalent during hospitalization39 In other anotherreport symptoms of loss of taste smell or both have beennoted to persist for up to several weeks41 Although olfactorydisturbances are common in other upper respiratory illnessesof viral origin due to sinonasal symptoms (rhinorrhea andcongestion) these are less commonly observed in patientswith COVID-1951 The lack of sinonasal symptoms suggestsviral-mediated dysfunction of gustatory and olfactory organsrather than inflammatory damage however the exact mecha-nisms remain to be determined
Cerebrovascular DiseaseA small but growing number of reports suggest an increasedrisk of stroke as a potential complication of COVID-19 in-fection (table 2)4253ndash56 Predisposition to stroke may berelated to an infection-induced coagulopathy as indicated byelevated D-dimer elevated fibrinogen and thrombocytope-nia common in patients with severe COVID-19 disease54
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e51
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 1 Summary of Current Reports on Acute Taste and Smell Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Evaluation Reference
Multicenter questionnaire Belgium FranceSpain and Italy
417 patients mean age 369 y(range 19ndash77 y) female 263(631) male 154 (369) allwith mild COVID-19
Anosmia or hyposmia856 dysgeusia 880
Online questionnaire of OlfactoryDisordersmdashNegative Statements
Lechien et al 202041
Case report Aarhus Denmark Female patient in early 30swithmild COVID-19
Anosmia and hypogeusia Anosmia verified with Sniffin Sticks extendedtest (848) hypogeusia verified with tastespray screening (24) taste drop test (2440)and taste strips (1216)
Haldrup et al 202040
Single-center cross-sectional survey Milan Italy 59 patients median age 60 y(range 50ndash74 y) female 29(322) male 30 (678) allwere hospitalized with COVID-19 but capable of completingthe survey
Sudden onset olfactory ortaste disorder in 20patients (339)
Self-reported Giacomelli et al 202039
Case series Padua Italy 6 patients no furtherdescriptions given
Sudden-onset hyposmiaand hypogeusia as only ormain COVID-19 symptom
Suprathreshold Odor Rating Test using sixodors to confirm hyposmia
Marchese-Ragona et al202044 (note nonndashpeer-reviewed report)
Case control Tehran Iran 60 hospitalized patients withCOVID-19 median age 4655 plusmn1217 y female 40 (67) male20 (33) COVID-19 diseasemild (42) moderate (48)and severe (10)
Mild microsmia (13)moderate microsmia(27) severe microsmia(33) and anosmia (25)
University of Pennsylvania SmellIdentification Test of 40 odorants
Moein et al 202045
Retrospective observational Mulhouse France 54 (47) of 114 examined andor hospitalized patients withCOVID-19 with reportedanosmia mean age 47 plusmn 16 yfemale 36 (67)male 18 (33)
Anosmia mean duration89 plusmn 63 d anosmiadeveloped 44 plusmn 19 d afterinfection onset dysgeusiain 85
Self-reported Klopfenstein et al 2020102
Retrospective review Tehran Iran 8 patients with sudden-onsetanosmia 5 COVID-19+ agerange 22ndash44 y female 6 (75)male 2 (25)
Anosmia in 88 patientsonset between 2 and 4d after fever ageusia in 28 patients
Self-reported Gilani et al 2020103
Case report Madrid Spain 40-y-old Venezuelan femaleradiologist caring for multiplesymptomatic patients withCOVID-19
Anosmia 3 d aftersymptom onset anosmiaresolved after 14 d
Self-reported Ollarves-Carrero et al2020104
Case series Washington DC 177 pediatric and young adultpatients (25hospitalized 20critically ill) male 92 (52)female 85 (48)
Loss of taste and smell in15 (9) patients
Methods not described DeBaisi et al 2020105
Abbreviation COVID-19 = coronavirus disease 2019
e52
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
3 centersretrospective
Wuhan Hubei China 214 patients mean age527 plusmn 155 y female 127(593) male 87 (407)severe COVID-19 88(411)
Any neurologic signs orsymptoms 78 (364) CNSsigns or symptoms(dizziness headacheimpaired consciousnessacute cerebrovasculardisease ataxia and seizure)53 (248) PNS signs orsymptoms (tasteimpairment smellimpairment visionimpairment and nervepain) 19 (89)
None described Patients with severesymptoms uarr CRP D-dimer darrlymphocytes uarr BUNCr
Mao et al 202043
Single-centerretrospective
Wuhan Hubei China 221 patients mean age533 plusmn 159 y female 90(40middot7)male 131 (59middot3)severe COVID-19 94(42middot5)
AIS 11 (5) CVST 1 (0middot5)CH 1 (0middot5)
Representative brain CTsshowing new-onset AISCVST and left basalganglia CH
Blood from patients with AISCVSTCH showed uarr WBCsneutrophils CRP D-dimer darrlymphocytes
Li et al 202042
Case report Shimokato ChuoYamanashi Japan
24-y-old man withheadache fatigue andfever
Altered mental statusseizures meningitisencephalitis
Brain MRI DWI showinghyperintensities along theright lateral ventricleFLAIR showinghyperintense signals inthe mesial temporal lobeand hippocampus T2WIshowing pan-paranasalsinusitis
CSF uarr opening pressure uarrWBCs SARS-CoV-2+ by RT-PCR blood uarr WBCs uarr CRP
Moriguchi et al 202046
Case report Beijing Hebei China 56-y-old patient ofunknown sex
Viral encephalitis None CSF SARS-CoV-2+ by RT-PCR Zhou et al 202050
(note nonndashpeer-reviewedreport)
Case report Detroit MI Female patient age in late50s with 3 d of cough andfever with COVID-19 innasal swab
Altered mental status andnecrotizing hemorrhagicencephalopathy
Head CT with symmetrichypoattenuation withinbilateral medial thalamiwith normal CT angiogramand venogram brain MRIwith hemorrhagic rim-enhancing lesions withinbilateral thalami medialtemporal lobes andsubinsular regions
CSF traumatic punctureunable to test for SARS-CoV-2via RT-PCR
Poyiadji et al 202047
Retrospectivecase study
Leiden and Rotterdamthe Netherlands
Analysis of 184 COVID-19+admitted to the ICUs of 3hospitals for 1 mo 3184(16) had strokes patientcharacteristics notdescribed
COVID-19 pneumoniarequiring ICU admissionfollowed by development ofcoagulopathy and stroke
Ischemia strokediagnosed with CT
None described Klok et al 202053
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e53
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series New York NY 5 adult patients aged33ndash49 y 1 female 4 maleswith mild COVID-19
2 patients wereasymptomatic with COVID-19 3 had fever cough orfatigue all developedsymptoms of severe strokewith reducedconsciousness gaze palsydysarthria andorhemiplegia
CT CTA CTP andor MRIshowed large vesselocclusions in all patients
Blood uarr fibrinogen (60) uarr D-dimer (60)
Oxley et al 202055
Case report Barcelona CataloniaSpain
50-y-old man with severeCOVID-19
While in ICU with bilateralpneumonia developedacute-onset right facialparalysis and left limbweakness
Head CT perfusion mapshowed hypoperfusion inthe left paramedianthalamic artery head MRIshowed left medialthalamic infarct
None described Rudilosso et al 202056
Case series Wuhan Hubei China 69-y-old male 70-y-oldmale and 65-y-old femalepatients with severeCOVID-19
Presentedwith fever coughdyspnea and headache andlater developed evidencecerebral infarcts 1 patientalso had distal limbischemia
Head CT showed diffuseacute cerebral infarctionsin cerebral hemispheresin all patients 2 patientsalso had cerebellarinfarctions
Blood darr lymphocytes darrplatelets uarr D-dimer uarrfibrinogen all had positiveanticardiolipin IgA andantindashβ2-glycoprotein I IgAand IgG
Zhang et al 202058
Case report Boca Raton FL 74-y-old male patient withsevere COVID-19
Fever cough headache andaltered mental status
Head CT showed evidenceof distant posteriorcerebral artery strokeEEG described asconsistent withencephalopathy lefttemporal lobedysfunction and possibleepileptogenicity
CSF no evidence of infection Filatov et al 202059
Rome Italy 78-y-old female patientwith mild COVID-19
Focal status epilepticusfollowed by fever 12 h later
Head MRI showed noevidence of new cerebrallesions ictal EEG showedseizure activity localizedover left-fronto-centro-temporal regions
Blood darr lymphocytes darrplatelets uarr CRP
Vollono et al 202061
Case report Jingzhou China 66-y-old female patientwith moderate COVID-19
Progressive arm and legweakness with decreaseddistal sensationmdashtreatedwith IVIg
Nerve conduction studiessupporting demyelinatingneuropathy
SARS-CoV-2 in oropharyngealswab by RT-PCRlymphocytopeniathrombocytopenia normalCSF
Zhao et al 202049
Continued
e54
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Figure 2 Proposed Pathways of SARS-CoV-2 Systemic Infection and Neuroinvasion
(A) Initial infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with viral entry into the nasopharynx oropharynx larynx andlungs (B) Magnified cross-section of a lung alveolus and capillary SARS-CoV-2 is known to infect type II pneumocytes as well as endothelial cells whichexpress the angiotensin-converting enzyme 2 (ACE-2) From the lungs the virus could enter the vasculature and circulate to other organs resulting inmultiorgan infection and sepsis Inflammation of cells such as neutrophils monocytes and lymphocytes could contribute to viral access to thevasculature due capillary leakage and direct tissue damage Thismay also be an initial site for viral infection of immune cells such asmacrophages andlymphocytes which have been shown to become infected by other coronaviruses such as SARS-CoV-1 and express the ACE-2 receptor (C) Sagittalcross-section of the brain at the level of the third and fourth ventricles with surrounding structures Hematogenous spread could lead to direct viralinfection of the CNS or infection of the CNS via the circumventricular organs (CVOs) including the subfornical organs the vascular organ of the laminaterminalis (OVLT) the median eminence and the area postrema which do lack a blood-brain barrier and have been shown to express ACE-2 SARS-CoV-2 may also access the CNS via the choroid plexus depicted on the roof of the third ventricle and in the fourth ventricle Virus could infect thevasculature of these regions which expresses ACE-2 or traffic into the CNS via infected lymphocytes (D) Sagittal cross-section of the upper re-spiratory tract SARS-CoV-2 infection has been associated with hyposmia and hypogeusia in a significant number of patients ACE-2 has been found inthe non-neuronal cells of the olfactory system suggesting dysfunction damage to non-neuronal cells as a cause of anosmia Hypogeusia could becaused by viral infection of gustatory neurons of cranial nerves VII (chorda tympani of the facial nerve) CN IX and CN X all of which project to thenucleus of the solitary tract in the brainstem and are known to express ACE-2 Gustatory pathways could contribute to viral CNS access to thebrainstem that ultimately contributes to respiratory dysfunction Infection of the brainstem could worsen respiratory distress in patients with severeCOVID-19 For all panels SARS-CoV-2 virions are depicted as green dots Black or white arrows show possible directions of viral spread in each organor tissue
e50 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
glass opacities with bilateral multiple lobular and subsegmentalareas of consolidation2526 Most symptomatic individualshave a mild course that resolves without the need for hos-pitalization but infection can rapidly progress to severedisease with multiorgan failure and death2427 Severe com-plications of COVID-19 include acute respiratory distresssyndrome acute kidney injury acute cardiac disease anddisseminated intravascular coagulopathy and laboratory find-ings can include leukopenia lymphopenia or lymphocytosisabnormal liver enzymes elevated D-dimer and elevatedinflammatory markers (eg interleukin [IL]-6 ferritin andC-reactive protein)1924
The risk of developing severe COVID-19 increases pro-gressively with age Individuals gt65 years in age are more likelyto experience hospitalization intensive care unit admissionmechanical ventilation and death compared with youngerpeople252829 These epidemiologic patterns of COVID-19 aresimilar to those seen with SARS-CoV-1 and MERS-CoV3031
Although children tend to experience milder symptoms and abetter prognosis compared with adults there have beenemerging reports from Europe and North America of multi-system inflammatory conditions like that of Kawasaki diseaseand hyperinflammatory shock syndrome in children andadolescents3233 The association between SARS-CoV-2 andsevere pediatric disease is likely a reflection the size of the globaloutbreak in diverse populations rather than increased virulenceof the SARS-CoV-2 compared with other modern HCoVs
For the 3 modern HCoVsmdashSARS-CoV-1 MERS and SARS-CoV-2mdasha key feature of severe disease is a dysregulated im-mune response that damages the lungs and organs above andbeyond the direct viral damage1034 The exact mechanismsdriving this hyperinflammatory immunopathology are not wellunderstood and may be multifactorial10 Overall individualswith severe disease appear to have rapid viral replication in thelungs with increases in alveolar macrophages and proin-flammatory cytokines including tumor necrosis factor-α IL-1IL-6 and ferritin34 Seemingly paradoxically as many as 80 ofpatients with COVID-19 develop lymphopenia35 The exactcause of lymphopenia is unknown but could be due to tissueredistribution to areas of infection (lungs) direct viral infectionof lymphocytes followed by cell death or cytokine-inducedlymphotoxicity103436 Together these factors promotemassiveinflammation and cytokine storm
Health-related comorbidities also contribute to the de-velopment of severe disease with 94 of deaths occurring inpatientswith at least 1 comorbidity37 Conditions increasing therisk of severe disease include diabetes hypertension Class IIIobesity (body mass index gt40 kgm2) severe or chronic car-diac disease chronic lung disease including moderate to severeasthma and being male37 Members of racial minorities in theUnited States are at a higher risk of poor outcomes that aremost likely due to inequalities in medical care and the higherprevalence of comorbidities in this population driven by healthdisparities38 The relationship between these comorbidities and
development of cytokine storm could be driven by changes inreceptor expression and dysregulation of innate immunity andinflammation that can occur in these disease states amongother hypotheses
Neurologic Sequelae of SARS-CoV-2and COVID-19Although COVID-19 is primarily a disease of the re-spiratory tract neurologic symptoms are increasingly beingrecognized39ndash50 With a rapid rise in severely ill patients ner-vous system manifestations can be overlooked masked by se-dation during ventilation or be of lower priority when severerespiratory and cardiac compromise occur The neurologicsequelae that have been described to date are discussed withattention to available evidence for indirect direct or post-infectious mechanisms
Olfactory and Taste DisturbancesThe CDC recently expanded the COVID-19 symptom listfrom the typical fever cough and shortness of breath triad toinclude sudden onset of taste andor smell loss37 Table 1summarizes studies focusing on tastesmell dysfunction withCOVID-19 The prevalence of these symptoms among pa-tients with COVID-19 is estimated around 5273 (95confidence interval [CI] 2964ndash7523) for olfactorydysfunction and 4393 (95 CI 2046ndash6895) for gus-tatory dysfunction in a meta-analysis of published reportsbefore April 19 202051 The timing of onset of the olfactorytaste disorders presents particular interest because they mayoccur earlier than other hallmark features of COVID-19(fever or cough) which opens the possibility of using themas initial screening measures52 In a cohort of hospitalizedpatients in Milan Italy 20 experienced smell and tastedisturbance before admission whereas the remainderreported these disturbances during their hospital stay39
Taste alterations were noted to be more prevalent beforehospitalization (91) whereas taste and smell changes wereequally prevalent during hospitalization39 In other anotherreport symptoms of loss of taste smell or both have beennoted to persist for up to several weeks41 Although olfactorydisturbances are common in other upper respiratory illnessesof viral origin due to sinonasal symptoms (rhinorrhea andcongestion) these are less commonly observed in patientswith COVID-1951 The lack of sinonasal symptoms suggestsviral-mediated dysfunction of gustatory and olfactory organsrather than inflammatory damage however the exact mecha-nisms remain to be determined
Cerebrovascular DiseaseA small but growing number of reports suggest an increasedrisk of stroke as a potential complication of COVID-19 in-fection (table 2)4253ndash56 Predisposition to stroke may berelated to an infection-induced coagulopathy as indicated byelevated D-dimer elevated fibrinogen and thrombocytope-nia common in patients with severe COVID-19 disease54
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e51
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 1 Summary of Current Reports on Acute Taste and Smell Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Evaluation Reference
Multicenter questionnaire Belgium FranceSpain and Italy
417 patients mean age 369 y(range 19ndash77 y) female 263(631) male 154 (369) allwith mild COVID-19
Anosmia or hyposmia856 dysgeusia 880
Online questionnaire of OlfactoryDisordersmdashNegative Statements
Lechien et al 202041
Case report Aarhus Denmark Female patient in early 30swithmild COVID-19
Anosmia and hypogeusia Anosmia verified with Sniffin Sticks extendedtest (848) hypogeusia verified with tastespray screening (24) taste drop test (2440)and taste strips (1216)
Haldrup et al 202040
Single-center cross-sectional survey Milan Italy 59 patients median age 60 y(range 50ndash74 y) female 29(322) male 30 (678) allwere hospitalized with COVID-19 but capable of completingthe survey
Sudden onset olfactory ortaste disorder in 20patients (339)
Self-reported Giacomelli et al 202039
Case series Padua Italy 6 patients no furtherdescriptions given
Sudden-onset hyposmiaand hypogeusia as only ormain COVID-19 symptom
Suprathreshold Odor Rating Test using sixodors to confirm hyposmia
Marchese-Ragona et al202044 (note nonndashpeer-reviewed report)
Case control Tehran Iran 60 hospitalized patients withCOVID-19 median age 4655 plusmn1217 y female 40 (67) male20 (33) COVID-19 diseasemild (42) moderate (48)and severe (10)
Mild microsmia (13)moderate microsmia(27) severe microsmia(33) and anosmia (25)
University of Pennsylvania SmellIdentification Test of 40 odorants
Moein et al 202045
Retrospective observational Mulhouse France 54 (47) of 114 examined andor hospitalized patients withCOVID-19 with reportedanosmia mean age 47 plusmn 16 yfemale 36 (67)male 18 (33)
Anosmia mean duration89 plusmn 63 d anosmiadeveloped 44 plusmn 19 d afterinfection onset dysgeusiain 85
Self-reported Klopfenstein et al 2020102
Retrospective review Tehran Iran 8 patients with sudden-onsetanosmia 5 COVID-19+ agerange 22ndash44 y female 6 (75)male 2 (25)
Anosmia in 88 patientsonset between 2 and 4d after fever ageusia in 28 patients
Self-reported Gilani et al 2020103
Case report Madrid Spain 40-y-old Venezuelan femaleradiologist caring for multiplesymptomatic patients withCOVID-19
Anosmia 3 d aftersymptom onset anosmiaresolved after 14 d
Self-reported Ollarves-Carrero et al2020104
Case series Washington DC 177 pediatric and young adultpatients (25hospitalized 20critically ill) male 92 (52)female 85 (48)
Loss of taste and smell in15 (9) patients
Methods not described DeBaisi et al 2020105
Abbreviation COVID-19 = coronavirus disease 2019
e52
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
3 centersretrospective
Wuhan Hubei China 214 patients mean age527 plusmn 155 y female 127(593) male 87 (407)severe COVID-19 88(411)
Any neurologic signs orsymptoms 78 (364) CNSsigns or symptoms(dizziness headacheimpaired consciousnessacute cerebrovasculardisease ataxia and seizure)53 (248) PNS signs orsymptoms (tasteimpairment smellimpairment visionimpairment and nervepain) 19 (89)
None described Patients with severesymptoms uarr CRP D-dimer darrlymphocytes uarr BUNCr
Mao et al 202043
Single-centerretrospective
Wuhan Hubei China 221 patients mean age533 plusmn 159 y female 90(40middot7)male 131 (59middot3)severe COVID-19 94(42middot5)
AIS 11 (5) CVST 1 (0middot5)CH 1 (0middot5)
Representative brain CTsshowing new-onset AISCVST and left basalganglia CH
Blood from patients with AISCVSTCH showed uarr WBCsneutrophils CRP D-dimer darrlymphocytes
Li et al 202042
Case report Shimokato ChuoYamanashi Japan
24-y-old man withheadache fatigue andfever
Altered mental statusseizures meningitisencephalitis
Brain MRI DWI showinghyperintensities along theright lateral ventricleFLAIR showinghyperintense signals inthe mesial temporal lobeand hippocampus T2WIshowing pan-paranasalsinusitis
CSF uarr opening pressure uarrWBCs SARS-CoV-2+ by RT-PCR blood uarr WBCs uarr CRP
Moriguchi et al 202046
Case report Beijing Hebei China 56-y-old patient ofunknown sex
Viral encephalitis None CSF SARS-CoV-2+ by RT-PCR Zhou et al 202050
(note nonndashpeer-reviewedreport)
Case report Detroit MI Female patient age in late50s with 3 d of cough andfever with COVID-19 innasal swab
Altered mental status andnecrotizing hemorrhagicencephalopathy
Head CT with symmetrichypoattenuation withinbilateral medial thalamiwith normal CT angiogramand venogram brain MRIwith hemorrhagic rim-enhancing lesions withinbilateral thalami medialtemporal lobes andsubinsular regions
CSF traumatic punctureunable to test for SARS-CoV-2via RT-PCR
Poyiadji et al 202047
Retrospectivecase study
Leiden and Rotterdamthe Netherlands
Analysis of 184 COVID-19+admitted to the ICUs of 3hospitals for 1 mo 3184(16) had strokes patientcharacteristics notdescribed
COVID-19 pneumoniarequiring ICU admissionfollowed by development ofcoagulopathy and stroke
Ischemia strokediagnosed with CT
None described Klok et al 202053
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e53
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series New York NY 5 adult patients aged33ndash49 y 1 female 4 maleswith mild COVID-19
2 patients wereasymptomatic with COVID-19 3 had fever cough orfatigue all developedsymptoms of severe strokewith reducedconsciousness gaze palsydysarthria andorhemiplegia
CT CTA CTP andor MRIshowed large vesselocclusions in all patients
Blood uarr fibrinogen (60) uarr D-dimer (60)
Oxley et al 202055
Case report Barcelona CataloniaSpain
50-y-old man with severeCOVID-19
While in ICU with bilateralpneumonia developedacute-onset right facialparalysis and left limbweakness
Head CT perfusion mapshowed hypoperfusion inthe left paramedianthalamic artery head MRIshowed left medialthalamic infarct
None described Rudilosso et al 202056
Case series Wuhan Hubei China 69-y-old male 70-y-oldmale and 65-y-old femalepatients with severeCOVID-19
Presentedwith fever coughdyspnea and headache andlater developed evidencecerebral infarcts 1 patientalso had distal limbischemia
Head CT showed diffuseacute cerebral infarctionsin cerebral hemispheresin all patients 2 patientsalso had cerebellarinfarctions
Blood darr lymphocytes darrplatelets uarr D-dimer uarrfibrinogen all had positiveanticardiolipin IgA andantindashβ2-glycoprotein I IgAand IgG
Zhang et al 202058
Case report Boca Raton FL 74-y-old male patient withsevere COVID-19
Fever cough headache andaltered mental status
Head CT showed evidenceof distant posteriorcerebral artery strokeEEG described asconsistent withencephalopathy lefttemporal lobedysfunction and possibleepileptogenicity
CSF no evidence of infection Filatov et al 202059
Rome Italy 78-y-old female patientwith mild COVID-19
Focal status epilepticusfollowed by fever 12 h later
Head MRI showed noevidence of new cerebrallesions ictal EEG showedseizure activity localizedover left-fronto-centro-temporal regions
Blood darr lymphocytes darrplatelets uarr CRP
Vollono et al 202061
Case report Jingzhou China 66-y-old female patientwith moderate COVID-19
Progressive arm and legweakness with decreaseddistal sensationmdashtreatedwith IVIg
Nerve conduction studiessupporting demyelinatingneuropathy
SARS-CoV-2 in oropharyngealswab by RT-PCRlymphocytopeniathrombocytopenia normalCSF
Zhao et al 202049
Continued
e54
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

glass opacities with bilateral multiple lobular and subsegmentalareas of consolidation2526 Most symptomatic individualshave a mild course that resolves without the need for hos-pitalization but infection can rapidly progress to severedisease with multiorgan failure and death2427 Severe com-plications of COVID-19 include acute respiratory distresssyndrome acute kidney injury acute cardiac disease anddisseminated intravascular coagulopathy and laboratory find-ings can include leukopenia lymphopenia or lymphocytosisabnormal liver enzymes elevated D-dimer and elevatedinflammatory markers (eg interleukin [IL]-6 ferritin andC-reactive protein)1924
The risk of developing severe COVID-19 increases pro-gressively with age Individuals gt65 years in age are more likelyto experience hospitalization intensive care unit admissionmechanical ventilation and death compared with youngerpeople252829 These epidemiologic patterns of COVID-19 aresimilar to those seen with SARS-CoV-1 and MERS-CoV3031
Although children tend to experience milder symptoms and abetter prognosis compared with adults there have beenemerging reports from Europe and North America of multi-system inflammatory conditions like that of Kawasaki diseaseand hyperinflammatory shock syndrome in children andadolescents3233 The association between SARS-CoV-2 andsevere pediatric disease is likely a reflection the size of the globaloutbreak in diverse populations rather than increased virulenceof the SARS-CoV-2 compared with other modern HCoVs
For the 3 modern HCoVsmdashSARS-CoV-1 MERS and SARS-CoV-2mdasha key feature of severe disease is a dysregulated im-mune response that damages the lungs and organs above andbeyond the direct viral damage1034 The exact mechanismsdriving this hyperinflammatory immunopathology are not wellunderstood and may be multifactorial10 Overall individualswith severe disease appear to have rapid viral replication in thelungs with increases in alveolar macrophages and proin-flammatory cytokines including tumor necrosis factor-α IL-1IL-6 and ferritin34 Seemingly paradoxically as many as 80 ofpatients with COVID-19 develop lymphopenia35 The exactcause of lymphopenia is unknown but could be due to tissueredistribution to areas of infection (lungs) direct viral infectionof lymphocytes followed by cell death or cytokine-inducedlymphotoxicity103436 Together these factors promotemassiveinflammation and cytokine storm
Health-related comorbidities also contribute to the de-velopment of severe disease with 94 of deaths occurring inpatientswith at least 1 comorbidity37 Conditions increasing therisk of severe disease include diabetes hypertension Class IIIobesity (body mass index gt40 kgm2) severe or chronic car-diac disease chronic lung disease including moderate to severeasthma and being male37 Members of racial minorities in theUnited States are at a higher risk of poor outcomes that aremost likely due to inequalities in medical care and the higherprevalence of comorbidities in this population driven by healthdisparities38 The relationship between these comorbidities and
development of cytokine storm could be driven by changes inreceptor expression and dysregulation of innate immunity andinflammation that can occur in these disease states amongother hypotheses
Neurologic Sequelae of SARS-CoV-2and COVID-19Although COVID-19 is primarily a disease of the re-spiratory tract neurologic symptoms are increasingly beingrecognized39ndash50 With a rapid rise in severely ill patients ner-vous system manifestations can be overlooked masked by se-dation during ventilation or be of lower priority when severerespiratory and cardiac compromise occur The neurologicsequelae that have been described to date are discussed withattention to available evidence for indirect direct or post-infectious mechanisms
Olfactory and Taste DisturbancesThe CDC recently expanded the COVID-19 symptom listfrom the typical fever cough and shortness of breath triad toinclude sudden onset of taste andor smell loss37 Table 1summarizes studies focusing on tastesmell dysfunction withCOVID-19 The prevalence of these symptoms among pa-tients with COVID-19 is estimated around 5273 (95confidence interval [CI] 2964ndash7523) for olfactorydysfunction and 4393 (95 CI 2046ndash6895) for gus-tatory dysfunction in a meta-analysis of published reportsbefore April 19 202051 The timing of onset of the olfactorytaste disorders presents particular interest because they mayoccur earlier than other hallmark features of COVID-19(fever or cough) which opens the possibility of using themas initial screening measures52 In a cohort of hospitalizedpatients in Milan Italy 20 experienced smell and tastedisturbance before admission whereas the remainderreported these disturbances during their hospital stay39
Taste alterations were noted to be more prevalent beforehospitalization (91) whereas taste and smell changes wereequally prevalent during hospitalization39 In other anotherreport symptoms of loss of taste smell or both have beennoted to persist for up to several weeks41 Although olfactorydisturbances are common in other upper respiratory illnessesof viral origin due to sinonasal symptoms (rhinorrhea andcongestion) these are less commonly observed in patientswith COVID-1951 The lack of sinonasal symptoms suggestsviral-mediated dysfunction of gustatory and olfactory organsrather than inflammatory damage however the exact mecha-nisms remain to be determined
Cerebrovascular DiseaseA small but growing number of reports suggest an increasedrisk of stroke as a potential complication of COVID-19 in-fection (table 2)4253ndash56 Predisposition to stroke may berelated to an infection-induced coagulopathy as indicated byelevated D-dimer elevated fibrinogen and thrombocytope-nia common in patients with severe COVID-19 disease54
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e51
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 1 Summary of Current Reports on Acute Taste and Smell Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Evaluation Reference
Multicenter questionnaire Belgium FranceSpain and Italy
417 patients mean age 369 y(range 19ndash77 y) female 263(631) male 154 (369) allwith mild COVID-19
Anosmia or hyposmia856 dysgeusia 880
Online questionnaire of OlfactoryDisordersmdashNegative Statements
Lechien et al 202041
Case report Aarhus Denmark Female patient in early 30swithmild COVID-19
Anosmia and hypogeusia Anosmia verified with Sniffin Sticks extendedtest (848) hypogeusia verified with tastespray screening (24) taste drop test (2440)and taste strips (1216)
Haldrup et al 202040
Single-center cross-sectional survey Milan Italy 59 patients median age 60 y(range 50ndash74 y) female 29(322) male 30 (678) allwere hospitalized with COVID-19 but capable of completingthe survey
Sudden onset olfactory ortaste disorder in 20patients (339)
Self-reported Giacomelli et al 202039
Case series Padua Italy 6 patients no furtherdescriptions given
Sudden-onset hyposmiaand hypogeusia as only ormain COVID-19 symptom
Suprathreshold Odor Rating Test using sixodors to confirm hyposmia
Marchese-Ragona et al202044 (note nonndashpeer-reviewed report)
Case control Tehran Iran 60 hospitalized patients withCOVID-19 median age 4655 plusmn1217 y female 40 (67) male20 (33) COVID-19 diseasemild (42) moderate (48)and severe (10)
Mild microsmia (13)moderate microsmia(27) severe microsmia(33) and anosmia (25)
University of Pennsylvania SmellIdentification Test of 40 odorants
Moein et al 202045
Retrospective observational Mulhouse France 54 (47) of 114 examined andor hospitalized patients withCOVID-19 with reportedanosmia mean age 47 plusmn 16 yfemale 36 (67)male 18 (33)
Anosmia mean duration89 plusmn 63 d anosmiadeveloped 44 plusmn 19 d afterinfection onset dysgeusiain 85
Self-reported Klopfenstein et al 2020102
Retrospective review Tehran Iran 8 patients with sudden-onsetanosmia 5 COVID-19+ agerange 22ndash44 y female 6 (75)male 2 (25)
Anosmia in 88 patientsonset between 2 and 4d after fever ageusia in 28 patients
Self-reported Gilani et al 2020103
Case report Madrid Spain 40-y-old Venezuelan femaleradiologist caring for multiplesymptomatic patients withCOVID-19
Anosmia 3 d aftersymptom onset anosmiaresolved after 14 d
Self-reported Ollarves-Carrero et al2020104
Case series Washington DC 177 pediatric and young adultpatients (25hospitalized 20critically ill) male 92 (52)female 85 (48)
Loss of taste and smell in15 (9) patients
Methods not described DeBaisi et al 2020105
Abbreviation COVID-19 = coronavirus disease 2019
e52
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
3 centersretrospective
Wuhan Hubei China 214 patients mean age527 plusmn 155 y female 127(593) male 87 (407)severe COVID-19 88(411)
Any neurologic signs orsymptoms 78 (364) CNSsigns or symptoms(dizziness headacheimpaired consciousnessacute cerebrovasculardisease ataxia and seizure)53 (248) PNS signs orsymptoms (tasteimpairment smellimpairment visionimpairment and nervepain) 19 (89)
None described Patients with severesymptoms uarr CRP D-dimer darrlymphocytes uarr BUNCr
Mao et al 202043
Single-centerretrospective
Wuhan Hubei China 221 patients mean age533 plusmn 159 y female 90(40middot7)male 131 (59middot3)severe COVID-19 94(42middot5)
AIS 11 (5) CVST 1 (0middot5)CH 1 (0middot5)
Representative brain CTsshowing new-onset AISCVST and left basalganglia CH
Blood from patients with AISCVSTCH showed uarr WBCsneutrophils CRP D-dimer darrlymphocytes
Li et al 202042
Case report Shimokato ChuoYamanashi Japan
24-y-old man withheadache fatigue andfever
Altered mental statusseizures meningitisencephalitis
Brain MRI DWI showinghyperintensities along theright lateral ventricleFLAIR showinghyperintense signals inthe mesial temporal lobeand hippocampus T2WIshowing pan-paranasalsinusitis
CSF uarr opening pressure uarrWBCs SARS-CoV-2+ by RT-PCR blood uarr WBCs uarr CRP
Moriguchi et al 202046
Case report Beijing Hebei China 56-y-old patient ofunknown sex
Viral encephalitis None CSF SARS-CoV-2+ by RT-PCR Zhou et al 202050
(note nonndashpeer-reviewedreport)
Case report Detroit MI Female patient age in late50s with 3 d of cough andfever with COVID-19 innasal swab
Altered mental status andnecrotizing hemorrhagicencephalopathy
Head CT with symmetrichypoattenuation withinbilateral medial thalamiwith normal CT angiogramand venogram brain MRIwith hemorrhagic rim-enhancing lesions withinbilateral thalami medialtemporal lobes andsubinsular regions
CSF traumatic punctureunable to test for SARS-CoV-2via RT-PCR
Poyiadji et al 202047
Retrospectivecase study
Leiden and Rotterdamthe Netherlands
Analysis of 184 COVID-19+admitted to the ICUs of 3hospitals for 1 mo 3184(16) had strokes patientcharacteristics notdescribed
COVID-19 pneumoniarequiring ICU admissionfollowed by development ofcoagulopathy and stroke
Ischemia strokediagnosed with CT
None described Klok et al 202053
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e53
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series New York NY 5 adult patients aged33ndash49 y 1 female 4 maleswith mild COVID-19
2 patients wereasymptomatic with COVID-19 3 had fever cough orfatigue all developedsymptoms of severe strokewith reducedconsciousness gaze palsydysarthria andorhemiplegia
CT CTA CTP andor MRIshowed large vesselocclusions in all patients
Blood uarr fibrinogen (60) uarr D-dimer (60)
Oxley et al 202055
Case report Barcelona CataloniaSpain
50-y-old man with severeCOVID-19
While in ICU with bilateralpneumonia developedacute-onset right facialparalysis and left limbweakness
Head CT perfusion mapshowed hypoperfusion inthe left paramedianthalamic artery head MRIshowed left medialthalamic infarct
None described Rudilosso et al 202056
Case series Wuhan Hubei China 69-y-old male 70-y-oldmale and 65-y-old femalepatients with severeCOVID-19
Presentedwith fever coughdyspnea and headache andlater developed evidencecerebral infarcts 1 patientalso had distal limbischemia
Head CT showed diffuseacute cerebral infarctionsin cerebral hemispheresin all patients 2 patientsalso had cerebellarinfarctions
Blood darr lymphocytes darrplatelets uarr D-dimer uarrfibrinogen all had positiveanticardiolipin IgA andantindashβ2-glycoprotein I IgAand IgG
Zhang et al 202058
Case report Boca Raton FL 74-y-old male patient withsevere COVID-19
Fever cough headache andaltered mental status
Head CT showed evidenceof distant posteriorcerebral artery strokeEEG described asconsistent withencephalopathy lefttemporal lobedysfunction and possibleepileptogenicity
CSF no evidence of infection Filatov et al 202059
Rome Italy 78-y-old female patientwith mild COVID-19
Focal status epilepticusfollowed by fever 12 h later
Head MRI showed noevidence of new cerebrallesions ictal EEG showedseizure activity localizedover left-fronto-centro-temporal regions
Blood darr lymphocytes darrplatelets uarr CRP
Vollono et al 202061
Case report Jingzhou China 66-y-old female patientwith moderate COVID-19
Progressive arm and legweakness with decreaseddistal sensationmdashtreatedwith IVIg
Nerve conduction studiessupporting demyelinatingneuropathy
SARS-CoV-2 in oropharyngealswab by RT-PCRlymphocytopeniathrombocytopenia normalCSF
Zhao et al 202049
Continued
e54
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract
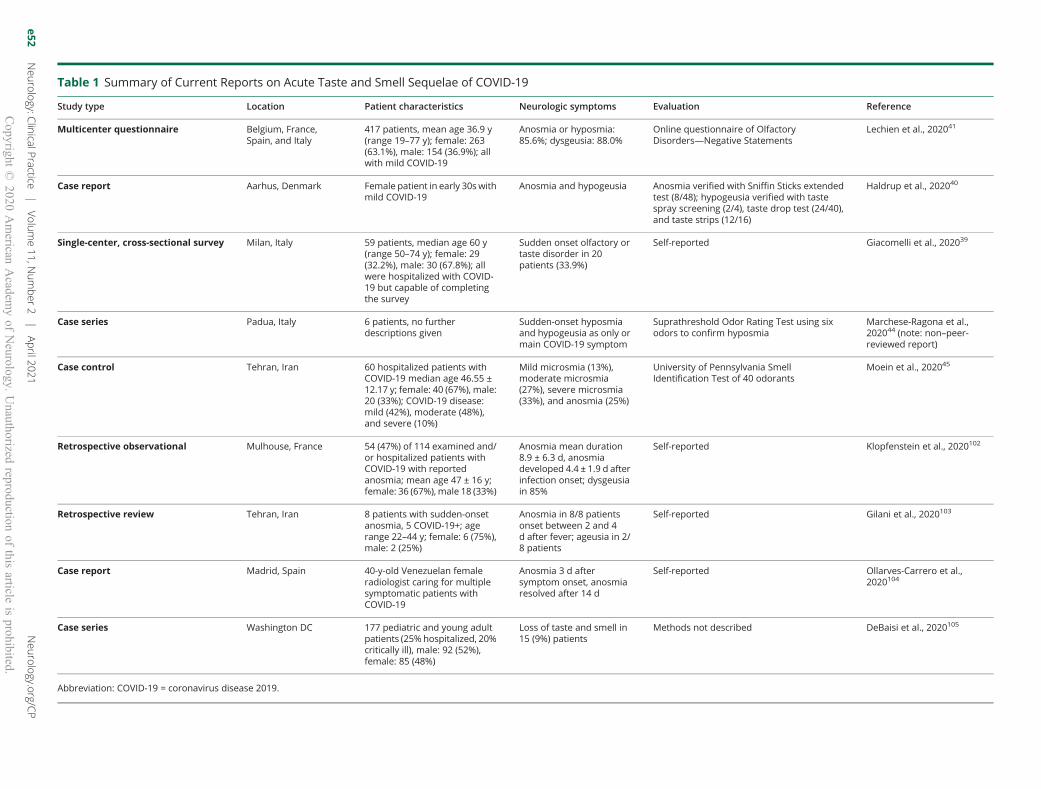
Table 1 Summary of Current Reports on Acute Taste and Smell Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Evaluation Reference
Multicenter questionnaire Belgium FranceSpain and Italy
417 patients mean age 369 y(range 19ndash77 y) female 263(631) male 154 (369) allwith mild COVID-19
Anosmia or hyposmia856 dysgeusia 880
Online questionnaire of OlfactoryDisordersmdashNegative Statements
Lechien et al 202041
Case report Aarhus Denmark Female patient in early 30swithmild COVID-19
Anosmia and hypogeusia Anosmia verified with Sniffin Sticks extendedtest (848) hypogeusia verified with tastespray screening (24) taste drop test (2440)and taste strips (1216)
Haldrup et al 202040
Single-center cross-sectional survey Milan Italy 59 patients median age 60 y(range 50ndash74 y) female 29(322) male 30 (678) allwere hospitalized with COVID-19 but capable of completingthe survey
Sudden onset olfactory ortaste disorder in 20patients (339)
Self-reported Giacomelli et al 202039
Case series Padua Italy 6 patients no furtherdescriptions given
Sudden-onset hyposmiaand hypogeusia as only ormain COVID-19 symptom
Suprathreshold Odor Rating Test using sixodors to confirm hyposmia
Marchese-Ragona et al202044 (note nonndashpeer-reviewed report)
Case control Tehran Iran 60 hospitalized patients withCOVID-19 median age 4655 plusmn1217 y female 40 (67) male20 (33) COVID-19 diseasemild (42) moderate (48)and severe (10)
Mild microsmia (13)moderate microsmia(27) severe microsmia(33) and anosmia (25)
University of Pennsylvania SmellIdentification Test of 40 odorants
Moein et al 202045
Retrospective observational Mulhouse France 54 (47) of 114 examined andor hospitalized patients withCOVID-19 with reportedanosmia mean age 47 plusmn 16 yfemale 36 (67)male 18 (33)
Anosmia mean duration89 plusmn 63 d anosmiadeveloped 44 plusmn 19 d afterinfection onset dysgeusiain 85
Self-reported Klopfenstein et al 2020102
Retrospective review Tehran Iran 8 patients with sudden-onsetanosmia 5 COVID-19+ agerange 22ndash44 y female 6 (75)male 2 (25)
Anosmia in 88 patientsonset between 2 and 4d after fever ageusia in 28 patients
Self-reported Gilani et al 2020103
Case report Madrid Spain 40-y-old Venezuelan femaleradiologist caring for multiplesymptomatic patients withCOVID-19
Anosmia 3 d aftersymptom onset anosmiaresolved after 14 d
Self-reported Ollarves-Carrero et al2020104
Case series Washington DC 177 pediatric and young adultpatients (25hospitalized 20critically ill) male 92 (52)female 85 (48)
Loss of taste and smell in15 (9) patients
Methods not described DeBaisi et al 2020105
Abbreviation COVID-19 = coronavirus disease 2019
e52
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
3 centersretrospective
Wuhan Hubei China 214 patients mean age527 plusmn 155 y female 127(593) male 87 (407)severe COVID-19 88(411)
Any neurologic signs orsymptoms 78 (364) CNSsigns or symptoms(dizziness headacheimpaired consciousnessacute cerebrovasculardisease ataxia and seizure)53 (248) PNS signs orsymptoms (tasteimpairment smellimpairment visionimpairment and nervepain) 19 (89)
None described Patients with severesymptoms uarr CRP D-dimer darrlymphocytes uarr BUNCr
Mao et al 202043
Single-centerretrospective
Wuhan Hubei China 221 patients mean age533 plusmn 159 y female 90(40middot7)male 131 (59middot3)severe COVID-19 94(42middot5)
AIS 11 (5) CVST 1 (0middot5)CH 1 (0middot5)
Representative brain CTsshowing new-onset AISCVST and left basalganglia CH
Blood from patients with AISCVSTCH showed uarr WBCsneutrophils CRP D-dimer darrlymphocytes
Li et al 202042
Case report Shimokato ChuoYamanashi Japan
24-y-old man withheadache fatigue andfever
Altered mental statusseizures meningitisencephalitis
Brain MRI DWI showinghyperintensities along theright lateral ventricleFLAIR showinghyperintense signals inthe mesial temporal lobeand hippocampus T2WIshowing pan-paranasalsinusitis
CSF uarr opening pressure uarrWBCs SARS-CoV-2+ by RT-PCR blood uarr WBCs uarr CRP
Moriguchi et al 202046
Case report Beijing Hebei China 56-y-old patient ofunknown sex
Viral encephalitis None CSF SARS-CoV-2+ by RT-PCR Zhou et al 202050
(note nonndashpeer-reviewedreport)
Case report Detroit MI Female patient age in late50s with 3 d of cough andfever with COVID-19 innasal swab
Altered mental status andnecrotizing hemorrhagicencephalopathy
Head CT with symmetrichypoattenuation withinbilateral medial thalamiwith normal CT angiogramand venogram brain MRIwith hemorrhagic rim-enhancing lesions withinbilateral thalami medialtemporal lobes andsubinsular regions
CSF traumatic punctureunable to test for SARS-CoV-2via RT-PCR
Poyiadji et al 202047
Retrospectivecase study
Leiden and Rotterdamthe Netherlands
Analysis of 184 COVID-19+admitted to the ICUs of 3hospitals for 1 mo 3184(16) had strokes patientcharacteristics notdescribed
COVID-19 pneumoniarequiring ICU admissionfollowed by development ofcoagulopathy and stroke
Ischemia strokediagnosed with CT
None described Klok et al 202053
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e53
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series New York NY 5 adult patients aged33ndash49 y 1 female 4 maleswith mild COVID-19
2 patients wereasymptomatic with COVID-19 3 had fever cough orfatigue all developedsymptoms of severe strokewith reducedconsciousness gaze palsydysarthria andorhemiplegia
CT CTA CTP andor MRIshowed large vesselocclusions in all patients
Blood uarr fibrinogen (60) uarr D-dimer (60)
Oxley et al 202055
Case report Barcelona CataloniaSpain
50-y-old man with severeCOVID-19
While in ICU with bilateralpneumonia developedacute-onset right facialparalysis and left limbweakness
Head CT perfusion mapshowed hypoperfusion inthe left paramedianthalamic artery head MRIshowed left medialthalamic infarct
None described Rudilosso et al 202056
Case series Wuhan Hubei China 69-y-old male 70-y-oldmale and 65-y-old femalepatients with severeCOVID-19
Presentedwith fever coughdyspnea and headache andlater developed evidencecerebral infarcts 1 patientalso had distal limbischemia
Head CT showed diffuseacute cerebral infarctionsin cerebral hemispheresin all patients 2 patientsalso had cerebellarinfarctions
Blood darr lymphocytes darrplatelets uarr D-dimer uarrfibrinogen all had positiveanticardiolipin IgA andantindashβ2-glycoprotein I IgAand IgG
Zhang et al 202058
Case report Boca Raton FL 74-y-old male patient withsevere COVID-19
Fever cough headache andaltered mental status
Head CT showed evidenceof distant posteriorcerebral artery strokeEEG described asconsistent withencephalopathy lefttemporal lobedysfunction and possibleepileptogenicity
CSF no evidence of infection Filatov et al 202059
Rome Italy 78-y-old female patientwith mild COVID-19
Focal status epilepticusfollowed by fever 12 h later
Head MRI showed noevidence of new cerebrallesions ictal EEG showedseizure activity localizedover left-fronto-centro-temporal regions
Blood darr lymphocytes darrplatelets uarr CRP
Vollono et al 202061
Case report Jingzhou China 66-y-old female patientwith moderate COVID-19
Progressive arm and legweakness with decreaseddistal sensationmdashtreatedwith IVIg
Nerve conduction studiessupporting demyelinatingneuropathy
SARS-CoV-2 in oropharyngealswab by RT-PCRlymphocytopeniathrombocytopenia normalCSF
Zhao et al 202049
Continued
e54
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
3 centersretrospective
Wuhan Hubei China 214 patients mean age527 plusmn 155 y female 127(593) male 87 (407)severe COVID-19 88(411)
Any neurologic signs orsymptoms 78 (364) CNSsigns or symptoms(dizziness headacheimpaired consciousnessacute cerebrovasculardisease ataxia and seizure)53 (248) PNS signs orsymptoms (tasteimpairment smellimpairment visionimpairment and nervepain) 19 (89)
None described Patients with severesymptoms uarr CRP D-dimer darrlymphocytes uarr BUNCr
Mao et al 202043
Single-centerretrospective
Wuhan Hubei China 221 patients mean age533 plusmn 159 y female 90(40middot7)male 131 (59middot3)severe COVID-19 94(42middot5)
AIS 11 (5) CVST 1 (0middot5)CH 1 (0middot5)
Representative brain CTsshowing new-onset AISCVST and left basalganglia CH
Blood from patients with AISCVSTCH showed uarr WBCsneutrophils CRP D-dimer darrlymphocytes
Li et al 202042
Case report Shimokato ChuoYamanashi Japan
24-y-old man withheadache fatigue andfever
Altered mental statusseizures meningitisencephalitis
Brain MRI DWI showinghyperintensities along theright lateral ventricleFLAIR showinghyperintense signals inthe mesial temporal lobeand hippocampus T2WIshowing pan-paranasalsinusitis
CSF uarr opening pressure uarrWBCs SARS-CoV-2+ by RT-PCR blood uarr WBCs uarr CRP
Moriguchi et al 202046
Case report Beijing Hebei China 56-y-old patient ofunknown sex
Viral encephalitis None CSF SARS-CoV-2+ by RT-PCR Zhou et al 202050
(note nonndashpeer-reviewedreport)
Case report Detroit MI Female patient age in late50s with 3 d of cough andfever with COVID-19 innasal swab
Altered mental status andnecrotizing hemorrhagicencephalopathy
Head CT with symmetrichypoattenuation withinbilateral medial thalamiwith normal CT angiogramand venogram brain MRIwith hemorrhagic rim-enhancing lesions withinbilateral thalami medialtemporal lobes andsubinsular regions
CSF traumatic punctureunable to test for SARS-CoV-2via RT-PCR
Poyiadji et al 202047
Retrospectivecase study
Leiden and Rotterdamthe Netherlands
Analysis of 184 COVID-19+admitted to the ICUs of 3hospitals for 1 mo 3184(16) had strokes patientcharacteristics notdescribed
COVID-19 pneumoniarequiring ICU admissionfollowed by development ofcoagulopathy and stroke
Ischemia strokediagnosed with CT
None described Klok et al 202053
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e53
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series New York NY 5 adult patients aged33ndash49 y 1 female 4 maleswith mild COVID-19
2 patients wereasymptomatic with COVID-19 3 had fever cough orfatigue all developedsymptoms of severe strokewith reducedconsciousness gaze palsydysarthria andorhemiplegia
CT CTA CTP andor MRIshowed large vesselocclusions in all patients
Blood uarr fibrinogen (60) uarr D-dimer (60)
Oxley et al 202055
Case report Barcelona CataloniaSpain
50-y-old man with severeCOVID-19
While in ICU with bilateralpneumonia developedacute-onset right facialparalysis and left limbweakness
Head CT perfusion mapshowed hypoperfusion inthe left paramedianthalamic artery head MRIshowed left medialthalamic infarct
None described Rudilosso et al 202056
Case series Wuhan Hubei China 69-y-old male 70-y-oldmale and 65-y-old femalepatients with severeCOVID-19
Presentedwith fever coughdyspnea and headache andlater developed evidencecerebral infarcts 1 patientalso had distal limbischemia
Head CT showed diffuseacute cerebral infarctionsin cerebral hemispheresin all patients 2 patientsalso had cerebellarinfarctions
Blood darr lymphocytes darrplatelets uarr D-dimer uarrfibrinogen all had positiveanticardiolipin IgA andantindashβ2-glycoprotein I IgAand IgG
Zhang et al 202058
Case report Boca Raton FL 74-y-old male patient withsevere COVID-19
Fever cough headache andaltered mental status
Head CT showed evidenceof distant posteriorcerebral artery strokeEEG described asconsistent withencephalopathy lefttemporal lobedysfunction and possibleepileptogenicity
CSF no evidence of infection Filatov et al 202059
Rome Italy 78-y-old female patientwith mild COVID-19
Focal status epilepticusfollowed by fever 12 h later
Head MRI showed noevidence of new cerebrallesions ictal EEG showedseizure activity localizedover left-fronto-centro-temporal regions
Blood darr lymphocytes darrplatelets uarr CRP
Vollono et al 202061
Case report Jingzhou China 66-y-old female patientwith moderate COVID-19
Progressive arm and legweakness with decreaseddistal sensationmdashtreatedwith IVIg
Nerve conduction studiessupporting demyelinatingneuropathy
SARS-CoV-2 in oropharyngealswab by RT-PCRlymphocytopeniathrombocytopenia normalCSF
Zhao et al 202049
Continued
e54
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series New York NY 5 adult patients aged33ndash49 y 1 female 4 maleswith mild COVID-19
2 patients wereasymptomatic with COVID-19 3 had fever cough orfatigue all developedsymptoms of severe strokewith reducedconsciousness gaze palsydysarthria andorhemiplegia
CT CTA CTP andor MRIshowed large vesselocclusions in all patients
Blood uarr fibrinogen (60) uarr D-dimer (60)
Oxley et al 202055
Case report Barcelona CataloniaSpain
50-y-old man with severeCOVID-19
While in ICU with bilateralpneumonia developedacute-onset right facialparalysis and left limbweakness
Head CT perfusion mapshowed hypoperfusion inthe left paramedianthalamic artery head MRIshowed left medialthalamic infarct
None described Rudilosso et al 202056
Case series Wuhan Hubei China 69-y-old male 70-y-oldmale and 65-y-old femalepatients with severeCOVID-19
Presentedwith fever coughdyspnea and headache andlater developed evidencecerebral infarcts 1 patientalso had distal limbischemia
Head CT showed diffuseacute cerebral infarctionsin cerebral hemispheresin all patients 2 patientsalso had cerebellarinfarctions
Blood darr lymphocytes darrplatelets uarr D-dimer uarrfibrinogen all had positiveanticardiolipin IgA andantindashβ2-glycoprotein I IgAand IgG
Zhang et al 202058
Case report Boca Raton FL 74-y-old male patient withsevere COVID-19
Fever cough headache andaltered mental status
Head CT showed evidenceof distant posteriorcerebral artery strokeEEG described asconsistent withencephalopathy lefttemporal lobedysfunction and possibleepileptogenicity
CSF no evidence of infection Filatov et al 202059
Rome Italy 78-y-old female patientwith mild COVID-19
Focal status epilepticusfollowed by fever 12 h later
Head MRI showed noevidence of new cerebrallesions ictal EEG showedseizure activity localizedover left-fronto-centro-temporal regions
Blood darr lymphocytes darrplatelets uarr CRP
Vollono et al 202061
Case report Jingzhou China 66-y-old female patientwith moderate COVID-19
Progressive arm and legweakness with decreaseddistal sensationmdashtreatedwith IVIg
Nerve conduction studiessupporting demyelinatingneuropathy
SARS-CoV-2 in oropharyngealswab by RT-PCRlymphocytopeniathrombocytopenia normalCSF
Zhao et al 202049
Continued
e54
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Table 2 Summary of Current Reports on Acute Neurologic Sequelae of COVID-19 (continued)
Study type Location Patient characteristics Neurologic symptoms Imaging Laboratory findings Reference
Case series Pavia Italy 5 patients aged 23ndash77 yfemale 1 (20) male 5(80) all had mild COVID-19
Flaccid tetraparesis (60)flaccid paraplegia (20)flaccid tetraplegia (20)facial diplegia (20) facialweakness (40)paresthesias (100)respiratory failure(60)mdashtreated with IVIg
MRI brain performed in 4patients with one showingfacial nerve enhancementin patient with facialdiplegia MRI spineperformed in all patientswith caudal nerve rootenhancement found in 1patient
CSF in 4 patients tested uarrprotein SARS-CoV-2 negativeby RT-PCR negativeantiganglioside antibodies in4 patients tested
Toscano et al 202048
Case report Saint-Etienne France 64-y-old male patient withfever and cough for 2 dadmitted to hospital afterrotator cuff injury foundto be SARS-CoV-2 positiveon nasal swab
Bilateral upper and lowerextremity flaccid severeparesthesia developedbeginning 11 d after initialsymptom onset swallowingdisturbancemdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCRdemyelinating pattern onEMG
Camdessanche et al202063
Case report 54-y-old Caucasian femalepatient with no precedingfever or respiratorysymptoms but withtemporary loss of tasteand smell
Progressive proximallypronounced paraparesisareflexia and sensory losswith tingling of allextremities consistent withan acute demyelinatinginflammatorypolyneuropathy beginning10 d beforeadmissionmdashtreated withIVIg
None reported SARS-CoV-2 in oropharyngealswab by RT-PCR CSF withalbuminocytologicdissociation demyelinatingpattern on EMG
Scheidl et al 202062
Abbreviations AIS = acute ischemic stroke BUN=blood urea nitrogen CH = cerebral hemorrhage COVID-19 = coronavirus disease 2019 Cr = creatinine CRP =C-reactive protein CVST = central venous sinus thrombosis DWI =diffusion-weighted imaging FLAIR = fluid-attenuated inversion recovery Ig = immunoglobulin PNS = peripheral nervous system RT-PCR = reverse transcription PCR SARS-CoV-2 = severe acute respiratory syndromecoronavirus 2 T2WI = T2-weighted imaging WBC = white blood cell
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e55
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Large vessel strokes have also been reported in relativelyhealthy individuals aged 30ndash50 years with only minorCOVID-19 symptoms55 As discussed in the next sectionsinfection of endothelial vasculature by SARS-CoV-2 couldlead to endothelial dysfunction and this dysfunction com-bined with hypercoagulability could predispose to eitherthrombotic or hemorrhagic stroke Another possiblemechanism explaining stroke-associated COVID-19 couldbe the development of prothrombotic immunoglobulinssuch as antiphospholipid antibodies and lupus anticoagu-lant that have now been reported in some patients withCOVID-19 both with and without signs of stroke (table2)545758 Procoagulant antibodies however may be tran-siently expressed in many disease states and more work isneeded to understand their prevalence and significance inCOVID-19ndashassociated stroke
Encephalitis and EncephalopathyThere have been 2 cases of viral encephalitis or meningitisencephalitis with SARS-CoV-2 RNA found in the CSF(table 2)4650 Detection of SARS-CoV-2 in the CSF the goldstandard for causal diagnosis of CNS infection suggests aneuroinvasive potential for this virus Encephalopathy may bean indirect (ie non-CNS invasion) presenting feature of severeCOVID-19 particularly in the elderly and COVID-19 shouldbe included in the differential for those presenting with signs ofillness and altered mental status (AMS)59 Acute necrotizingencephalopathy which is likely an inflammatory disorder re-lated to a viral-induced cytokine storm was described in anairline worker in her late fifties with SARS-CoV-2 infection whoexperienced AMS that rapidly progressed to coma (table 2)47
This case highlights the potential for more than 1 viral-inducedindirect (ie noninvasive) mechanism to cause encephalopathy
SeizureA retrospective study of 304 patients with no history of ep-ilepsy or seizure showed no increase in risk for developingnew-onset seizures following COVID-19 infection60 How-ever viral illnesses can lower seizure thresholds in those withepilepsy due to alterations in medication metabolism duringillness as illustrated by a case report of a patient withCOVID-19 and a history of well-controlled seizures due toremote history of herpes encephalitis who presented withfocal status epilepticus despite an absence of respiratorysymptoms (table 2)61 This case highlights the need tomonitor for changes in those with epilepsy and SARS-CoV-2exposure
Guillain-Barre SyndromeSeveral single case reports detail the emergence of Guillain-Barre syndrome (GBS) as a postinfectious complicationSARS-COV-2 (table 2)48496263 In addition 5 patients inNorthern Italy were reported to develop flaccid limb weak-ness and tingling consistent with GBS following SARS-CoV-2 infection48 Outcomes for the Italian patients were poorwith 2 patients requiring continued ventilation and 4 withsignificant weakness at 4-week follow-up despite treatment
with IV immunoglobulin4849 With time the full extent andprognosis of GBS associated with COVID-19 will be betterunderstood
Impact on Preexisting Inflammatory Disordersof the Nervous SystemThe CDC reports that immunocompromised individuals are ata higher risk of severe illness from SARS-CoV-2 infection but aspecific evidence of such and outcomes are lacking37 Beforeadvising patients to alter ongoing therapies that target theimmune system the risk of neurologic disease progressionmust be weighed against the current unknowns relatedto COVID-19 There exists a balance between suppressingthe inflammatory response and creating an environment thatpromotes viral proliferation Broadly acting agents glucocor-ticoids which suppress both innate and adaptive arms of theimmune system have been used during the severe respiratoryphase of COVID-19 although recommendations against glu-cocorticoids in COVID-19 exist64 Other agents such asalemtuzumab (targets CD52 present on T and B lymphocytes)and cladribine (depletes B and T lymphocytes) can causeprofound lymphopenia and may exacerbate the lymphopeniaand immune dysregulation already seen in severe COVID-19More narrow targeting of proinflammatory cytokines may ac-tually be beneficial in COVID-19 including drugs such asbaricitinib (inhibits Janus kinase inflammatory pathway) toci-lizumab (antindashIL-6 receptor) and siltuximab (antindashIL-6) Useof these drugs in COVID-19 has some shown some promise insmall trials but data from randomized controlled trials arepending6566 Many of the immunomodulatory or immuno-suppressive agents commonly used for inflammatory neuro-logic disorders such as rituximab ocrelizumab fingolimodnatalizumab and azathioprine have unknown impact on therisk of infection with SARS-CoV-2 and on the severity ofcomplications from COVID-19 The decision to continue onthese agents with careful monitoring for COVID-19 symptomsto prevent exacerbation of devastating neurologic disordersshould be made on a case-by-case basis until further data areavailable67
Neurologic Sequelae of Other HCoVsIt is noteworthy that neuroinvasion has been demonstrated inalmost all the other β-CoVs368ndash80 Table 3 details all studiesdescribed in this section A series of postmortem studies onindividuals who died as a result of SARS-CoV-1 in 2003 somewith neurologic symptoms before death revealed that SARS-CoV-1 can become widely disseminated during infection andcan be found within the CNS7072747980 SARS-CoV-1 viruswas identified by several different methods including by RT-PCR in CSF and brain tissue and by immunohistochemistryin cortical and hypothalamic neurons71727479 Rare casesstudies have also implicated HCoV-OC43 and -229E ascauses of encephalomyelitis encephalitis and acute flaccidparalysis in children757778 Histopathology is not availablefor any cases of MERS-CoV Neurologic symptoms of
e56 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
SARS-CoV-1 Case series Postmortem samplesfrom 4 patients withconfirmed SARS 3males aged 25ndash57 y 1female aged 62 y
1 patient had headacheno other neurologicsymptoms described
None described Cerebrum cerebellumpituitary lung lymphnode spleen heart liverkidney adrenal glandparathyroid gland bonemarrow skin esophagusgastric fundus smallintestine pancreasthyroid aorta testisovary uterus and striatedmuscle by IHC and ISH
SARS in neurons of thecerebrum by IHC and ISHpituitary lung stomachsmall intestine kidneyadrenal skin parathyroidand liver by IHC and ISH
Ding et al 200371Ding et al 200470
SARS-CoV-1 Case series Postmortem samplesfrom 8 patients withconfirmed SARS nofurther clinicaldescriptions provided
None described None described Brain by light microscopyEM RT-PCR lungstrachea esophagus smallintestines largeintestines kidneysstomach liver spleenpancreas testes heartadrenals thyroid andskeletal muscle by ISH andEM
Virus in neurons ofhypothalamus and cortexlight microscopy EM anddetectable in brain tissueby RT-PCR lungs tracheaesophagus smallintestines largeintestines and kidneys byISH and EM
Gu et al 200572
SARS-CoV-1 Case report 59-y-old woman hx ofIgA nephropathy withfevers chills coughand diarrhea
Vomiting confusionseizures and statusepilepticus
CT showed noabnormalities
Tracheal aspirate serumCSF by RT-PCR
Tracheal aspirate serumCSF by RT-PCR
Hung et al 200379
SARS-CoV-1 Case report 32-y-old woman 26-wkpregnant with feverschills myalgias andcough
Seizures MRI showed noabnormalities
CSF by RT-PCR CSF by RT-PCR Lau et al 200474
SARS-CoV-1 Case report 39-y-old man withfever and progressivepneumonia
Dysphoria vomitingdelirium and coma
CT showed broadischemia necrosis andedema
Brain tissue with IHC RT-PCR viral culture EM
Virus in glia and neuronsby IHC detectable frombrain tissue by RT-PCRviral culture EM
Xu et al 200580
HCoV-OC43 Case report 11-mo-old male withsevere combinedimmunodeficiency noprodrome noted
Irritability sleepinessfeeding problems andabnormal posturing
MRI showed volume lossand abnormal graymattersignal by T2WI
Brain biopsy by RT-PCRand IHC
Brain tissue by RT-PCRHCoV antigen in neuronsand neuropil by IHC
Morfopoulou et al 200675
HCoV-OC43and 229E
Case report 3-y-old female withURI prodrome
Acute flaccid paralysisfollowing viral URI
None Nasal swabs CSF by RT-PCR
Nasal swabs by RT-PCR Turgay et al 201577
HCoV-OC43 Case report 15-y-old male with URIprodrome
Acute disseminatedencephalomyelitis
MRI showed diffuse whitematter lesions brain andspinal cord on T2WI
Nasal swabs CSF by RT-PCR
Nasal swabs CSF by RT-PCR
Yeh et al 200478
Continued
Neurolo
gyorgC
PNeurologyC
linicalPractice|
Volume11N
umber
2|
April2021
e57
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Table 3 Summary of Studies on the Neurologic Sequelae of Human Coronaviruses Before SARS-CoV-2 (continued)
HCoV Study typePatientcharacteristics Neurologic symptoms CNS imaging Specimen examined Cellstissue CoV Reference
MERS-CoV Case series 70 patients withlaboratory-confirmedMERS 657 male343 female medianage 62 y (range 1ndash90 y)
Headache (129) andconfusion (297)
None Respiratory swabs by RT-PCR
Respiratory swabs by RT-PCR
Saad et al 201476
MERS-CoV Case series 3 adult patients aged45ndash72 y all withsymptoms ofrespiratory disease orfever
1 patient had ataxiavomiting and confusion 1patient had stroke withhemiparesis followed bycoma 1 patient had comaand encephalitis
MRI with widespreadwhite matter andsubcortical lesions onT2WI in all 3 patients
Tracheal aspirate in 3patients CSF in 2 patientsby RT-PCR
Tracheal aspirate in 3patients by RT-PCR
Arabi et al 201569
MERS-CoV Case series 2 patients 34-y-oldwoman with fever and28-y-old man withfevermyalgias coughand dizziness
A 34-y-old womandeveloped headachenausea vomiting andcoma 2 wk followingMERS a 28-y-old mandeveloped lower limbparaplegia withnumbness in stockingdistribution
34-y-old woman CTshowed frontal lobehemorrhage and edemaa 28-y-old man hadabnormal nerveconduction studies andnormal MRI
Both had respiratoryswabs by RT-PCR a 28-y-old man had CSF studies
Respiratory swabs by RT-PCR
Algahtani et al 201668
MERS-CoV Case series 2 male 2 female adultpatients aged 38ndash55 ywith symptoms ofrespiratory disease
1 patient hadhypersomnolence andweakness in all 4 limbs 1patient had tingling inhands and legs with legweakness 1 patient hadtingling in both hands andfeet 1 patient had tinglingin both hands
None described Nasal swabs in 3 patients1 patient with confirmedexposure
Nasal swabs Kim et al 201773
Abbreviations CoV = coronavirus EM = electron microscopy HCoV = human coronavirus IHC = immunohistochemistry ISH = in situ hybridization MERS = Middle East respiratory syndrome RT-PCR = reverse transcriptionPCR SARS = severe acute respiratory syndrome T2WI = T2-weighted imaging URI = upper respiratory infection
e58
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

headache and confusion were reported in 10ndash25 of pa-tients with MERS-CoV during acute infection76 There are 2reports of MERS-CoVndashassociated hemorrhagic stroke6869
MERS-CoV has been more commonly associated withpostinfectious complications such as GBS68697376 One caseseries documented diffuse subcortical gray and white matterdamage in 3 patients following severe MERS-CoV infectionpossibly due to hypoxic-ischemic injury although 1 patientmay have had acute disseminated encephalomyelitis a de-myelinating disease that attacks white matter in the brain andspinal cord69 There have also been 5 cases of patients whodeveloped GBS-like flaccid paralysis and paresthesia followingMERS-CoV infection6873
Possible Mechanisms ofHCoV NeuroinvasionGiven our knowledge of other HCoVs we describe 2 po-tential methods by which SARS-CoV-2 could invade thenervous system hematogenous and transsynaptic spread(figure 2 BndashD)
Potential for Hematogenous Spread to the CNSFor many viruses initial infection of the lungs has beendemonstrated to lead to access to the circulatory system withthe presence of virus in the blood (eg viremia) ACE-2 isexpressed on vascular endothelium of arteries and veins inhumans and could serve as a gateway to multiorgan HCoVdisease81 In addition infected monocytes and lymphocytescould carry HCoV to multiple sites throughout the body aprior study demonstrated SARS-CoV-1 infection of mono-cytes and lymphocytes in 6 out of 22 blood samples frominfected patients72 Monocytes and lymphocytes couldtherefore act as Trojan Horses for viral CNS access as hasbeen shown in coxsackie B3 virus and cytomegalovirus in-fections82 Taken together it is possible that viremia andhematogenous trafficking via infected white blood cells mayallow for SARS-CoV-2 access to the CNS via CNS capillarieswhich are particularly extensive and highly permeable withincircumventricular organs (CVOs) that localize to periven-tricular regions of the brain and lack a blood-brain barrier(BBB) (figure 2 B and C)8183 ACE-2 expression in severalCVOs are responsible for detecting compositional changesin the peripheral circulation and transmitting this in-formation to autonomic control centers in the hypothalamusand brainstem84 A study investigating ACE-2 expression inwild type mice found that ACE-2 is expressed in the sub-fornical organs the vascular organ of the lamina terminalisthe median eminence and the area postrema85 (figure 2C)The latter has projections to other ACE-2ndashexpressing re-gions of the brainstem notably the dorsal motor nucleus ofthe vagus nerve (CN X) and the nucleus of the solitary tractwhich is involved in taste processing Furthermore ACE-2 ishighly expressed in the choroid plexus of humans In-flammation produced by pathologic conditions such ashypoxic-ischemic injury that occurs with severe COVID-19
can lead to the release of proinflammatory cytokines bymicroglia and brain endothelial cells which along with ox-idative stress and increased nitric oxide productiondegrading the BBB86 and increasing susceptibility for viralentry via hematogenous spread In this pathologic state virusand leukocytes could enter the CSF via the choroid plexusand lead to infiltration of brain tissue86 (figure 2C)
Consideration of Transsynaptic Spread tothe CNSAnother potential route to the CNS is transsynaptic spreadthrough tissues innervated by nerves for taste and smell(figure 2D) particularly in light of the numerous case re-ports and emerging studies describing disturbances in tasteandor smell without rhinorrhea in patients with confirmedCOVID-19 (see table 2 for details)39ndash414445 When con-sidering transsynaptic spread via gustatory system compo-nents it is important to note that ACE-2 is crucial to sodiumhomeostasis which influences salt appetite and perceptionof salty taste ACE-2 is highly expressed in the lingual tastebuds and in the tongue epithelium of mice along with otherrenin-angiotensin aldosterone system components that areinnervated by gustatory afferents87 although the expressionof ACE-2 in human gustatory afferents has not been char-acterized Recent work describes significant expression ofACE-2 in human oral tissues in the epithelial cells includingthe tongue and palate where taste budsmdashwhich are com-prised of specialized epithelial cells innervated by gustatoryafferentsmdashreside ACE-2 receptors are also widely expressedin the human CNS and particularly widely throughout thebrainstem Renin-angiotensin system components (ACEand AngIIR) have also been detected specifically throughoutthe human nucleus of the solitary tractmdashwhere gustatoryafferents terminatemdashas well as in the dorsal motor nucleusof the vagus nerve and both the rostral and caudal ventro-lateral reticular nucleus of the human brainstem88 In addi-tion to receiving gustatory information the nucleus of thesolitary tract receives general visceral afferents from thecardiovascular pulmonary and gastrointestinal systems IfSARS-CoV-2 were capable of invasion via chemosensoryandor chemoreceptive neurons this could account for thevariety of symptoms observed in patients with COVID-19including taste disturbances hypoxia cardiac complicationsand even gastrointestinal complaints
A significant effort is being made to understand the role of theolfactory system in COVID-19 symptomatology AlthoughACE-2 is known to be expressed in the olfactory system and inthe olfactory bulbs ofmice87 the anosmia of COVID-19 is morelikely mediated through non-neuronal cell types of the olfactoryepithelium Human olfactory sensory neurons have little ex-pression or coexpression of ACE-2 whereas non-neuronal celltypes of the olfactory epithelium had high levels of expressionand coexpression of these SARS-CoV-2 entry genes89ndash91 Thesefindings suggest that disruption or loss of smell is more likely aresult of damage to or dysfunction of non-neuronal cell typesrather than infection of neuronal cells (figure 2D)
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e59
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Table 4 A Sampling of COVID-19 Reporting Databases for Neurologic Conditions and Registries Outside of Neurology
Database Location Purpose Partnersinstitutions
COVID-19 reporting databases for neurologic conditions
COVID-19 infections in MS amp Related Conditions North America Define the impact of COVID-19 on patients with MS andhow factors such as age comorbidities and MStreatments affect COVID outcomes
National MS Society Consortium of MS Centers
COVID-19 Cardiovascular Disease Registry (includes stroke) United States Aggregate data and aid research on the diseasetreatment protocols and risk factors tied to adversecardiovascular outcomes
American Heart Society
Acute Encephalopathy in Critically Ill Patients with COVID-19 France Reporting the prevalence of acute encephalopathy atinitial management in criticalintensive care orneurocritical care to report its morbidity and mortalityand to identify prognostic factors
COVID-19 registries outside of neurology
ASH RC COVID-19 Registry for Hematologic Malignancy United States Collect and disseminate surveillance data on the naturalhistory of patients with COVID-19 and hematologicmalignancies
ASH Research Collaborative
COVID-19 Dermatology Registry International Understand dermatologic manifestations of the COVID-19 virus
American Academy of Dermatology
COVID-19 in Pregnancy and Newborns United States Understand course of COVID-19 in pregnant women University of California San Francisco
ASCO Survey on COVID-19 in Oncology Registry United States Collect both baseline and follow-up data onhow the virusaffects cancer care and cancer patient outcomes duringthe COVID-19 pandemic and into 2021
The COVID-19 Global Rheumatology Alliance Registry International Create a secure deidentified international casereporting registry for cases of COVID-19 in rheumatologypatients and then curate and disseminate the outputsfrom that registry
The COVIDndash19 Global Rheumatology AllianceSteering Committee
COVID-19 Pediatric Observatory France Describe the clinical phenotypes of hospitalized pediatricpatients with COVID-19 in France according to agegroups
Centre Hospitalier Intercommunal Creteil
COVID-19 in patients with HIV United States Characterize the clinical presentation and disease courseof COVID-19 in patients with HIV
University of MissourindashColumbia
Abbreviations ASCO = American Society of Clinical Oncology ASH RC = American Society of Hematology Research Collaborative COVID-19 = coronavirus disease 2019
e60
NeurologyC
linicalPractice
|Volu
me11N
umber
2|
April2021
NeurologyorgC
P
Copyright
copy2020
American
Academ
yof
Neurology
Unauthorized
reproductionof
thisarticle
isprohibited
Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Additional gaps remain in our understanding of CNSinvasion First although it is certainly plausible that ACE-2mdashtheknown SARS-CoV-2 receptormdashplays a role in CNS infectionother receptors that remain to be discovered might better ex-plain COVID-19 CNS manifestations Second other host fac-tors may be necessary to explain pathogenesis in specific tissuesThis is most evident in tissues that have high expression ofACE-2 receptors yet appear to not be significantly affected byinfection For example ACE-2 is strongly expressed in the di-gestive system according to the Human Protein Altas92 and yetgastrointestinal symptoms are reported in a minority of patientswith COVID-1925
Long-term Neurologic Sequelae ofCoV InfectionAn important consideration for HCoVs is the evidence forpotential long-term persistence in CNS tissue Infection ofimmortalized neuronal and oligodendrocyte cells lines withHCoV-OC43 and -229E respectively revealed viral antigenand infectious particles in a small proportion of the cell pop-ulations through dozens of cell passages9394 T lymphocytesfrom patients with multiple sclerosis contain antigens thatcross-react with antigens of HCoV-229E previously suggestinga link between HCoV infection and CNS immune-relateddisease95 and mice infected intracerebrally with HCoV-OC43developed long-term behavioral deficits with chronic loss ofhippocampal neurons and viral RNA detected by RT-PCR forup to 1 year postinfection96
There has been significant interest in the link between chronicneurologic disease and infectious events and some viral infec-tions are known to cause persistent neurologic disease For ex-ample measles persistence in the CNS can cause subacutesclerosing panencephalitis to begin 1 month to 27 years afterinitial infection97 There is also growing evidence that viral in-fections could be among the many environmental factors pre-disposing individuals to development of neurodegenerativediseases West Nile virus infection in the CNS results in upre-gulation of α-synuclein which appears to have an innate immunefunction suggesting a mechanistic link between viral infectionand the development of Parkinson disease98 Varicella zostervirus (VZV) which infects gt90 of the world population canreactivate in sensory ganglia to cause shingles and other sequelaecerebrovascular infection and stroke99 VZV can increase theproduction of amylin and amyloid β and has a theoretical po-tential to be associated with the risk of Alzheimer disease99
Monitoring the long-term association of viruses with neurologicdisease has a historic precedent Between 1916 and 1927 theworld was swept with a phenomenon known as encephalitislethargica (EL)100101 This syndrome resulted in symptoms ofextreme fatigue abnormal eye movements and parkinsonian-like motor symptoms Estimates suggest that EL afflicted over 1million people to cause up to 500000 deaths100101 The mostlikely culprit for this widespread phenomenon has been thought
to be a viral infection such as the 1918 H1N1 influenza buthistorical epidemiologic and histologic examinations have beeninconclusive100 Neurologists should be prepared tomonitor forchanges and future neurologic sequelae related to the COVID-19 pandemic
Clinical Recommendationsand ResourcesTo effectively understand the neurologic consequences ofCOVID-19 and the potential for neurologic disorders andtheir therapies to be risk factors for COVID-19 complica-tions standardized and large-scale collaborative data col-lection is necessary Multiple medical specialty groups suchas the American Society of Clinical Oncology and the GlobalRheumatology Alliance have developed registries for theirrespective patient populations Recently the Consortium ofMultiple Sclerosis Centers and the National Multiple Scle-rosis Society created COViMS to capture data on clinicaloutcomendashrelated COVID-19 in patients with prior di-agnosis of MS and related disorders and to learn aboutrelative risks associated with disease-modifying treatmentsin the setting of COVID-19 As the list of registries continueto grow (table 4) we must keep in mind that the trueprevalence of disease will remain uncertain without large-scale testing in asymptomatic people and serology for an-tibodies to SARS-CoV-2 Reports of increased incidence ofdeath at home in major cities point to the lack of accuratedata and future registry data will be a biased sample withoutmore widespread testing
ConclusionsHCoVs have the capacity to be neuropathogenic There isincreasing evidence that SARS-CoV-2 can cause both directand indirect neurologic disease but much remains tobe learned For now caution must be taken in regard toattributing neurologic disease to direct neuronal infectionby SARs-CoV-2 until protocols can be developed that allowfor postmortem tissue investigations and in the absence ofthat it is prudent to view neurologic outcomes signs andsymptoms associated with COVID-19 through the lens ofprior discoveries related to other HCoVs The impact ofCOVID-19 on preexisting neurologic disorders and the impactof immunosuppressive and immunomodulatory therapies onthe course of COVID-19 are currently unknown Patient reg-istries and improved testing for acute infection and exposure toSARS-CoV-2 will improve clinical decision-making in themanagement of neurologic disorders during the COVID-19pandemic
AcknowledgmentThe authors thank Dr Thomas E Finger for his guidance andthoughts on this manuscript especially on the topics of tasteand smell
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e61
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

Study FundingBH is supported by funding from the NIH (NIDCDDC014728-04S1 to Dr Finger) AMH is supported by afellowship from the NIAID (F30 AI136403-01A1) KLT issupported by funding from the NIH (R01 NS101208) and isthe recipient of a VA Merit Award
DisclosureThe authors report no disclosures relevant to themanuscriptFull disclosure form information provided by the authors isavailable with the full text of this article at Neurologyorgcp
Publication HistoryReceived byNeurology Clinical Practice April 30 2020 Accepted in finalform June 18 2020
References1 Perlman S Netland J Coronaviruses post-SARS update on replication and
pathogenesis Nat Rev Microbiol 20097439ndash450
2 Coronaviridae Study Group of the International Committee on Taxonomy of VirusesThe species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2 Nat Microbiol 20205536ndash544
3 Desforges M Le Coupanec A Dubeau P et al Human coronaviruses and otherrespiratory viruses underestimated opportunistic pathogens of the central nervoussystem Viruses 20191214
4 Li F Receptor recognition mechanisms of coronaviruses a decade of structuralstudies J Virol 2015891954ndash1964
5 Tang X Wu C Li X et al On the origin and continuing evolution of SARS-CoV-2Natl Sci Rev 202071012ndash1023
6 Wu F Zhao S Yu B et al A new coronavirus associated with human respiratorydisease in China Nature 2020579265ndash269
7 Graham RL Baric RS Recombination reservoirs and the modular spike mech-anisms of coronavirus cross-species transmission J Virol 2010843134ndash3146
8 Wu A Peng Y Huang B et al Genome composition and divergence of the novelcoronavirus (2019-nCoV) originating in China Cell Host Microbe 202027325ndash328
9 Desforges M Le Coupanec A Stodola JK Meessen-Pinard M Talbot PJ Humancoronaviruses viral and cellular factors involved in neuroinvasiveness and neuro-pathogenesis Virus Res 2014194145ndash158
10 Channappanavar R Perlman S Pathogenic human coronavirus infections causesand consequences of cytokine storm and immunopathology Semin Immunopathol201739529ndash539
11 Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of globalhealth concern Lancet 2020395470ndash473
12 Lu R Zhao X Li J et al Genomic characterisation and epidemiology of 2019 novelcoronavirus implications for virus origins and receptor binding Lancet 2020395565ndash574
13 Hoffmann M Kleine-Weber H Schroeder S et al SARS-CoV-2 cell entry dependson ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitorCell 2020181271ndash280e8
14 Wrapp D Wang N Corbett KS et al Cryo-EM structure of the 2019-nCoV spike inthe prefusion conformation Science 20203671260ndash1263
15 Walls AC Park YJ Tortorici MA Wall A McGuire AT Veesler D Structurefunction and antigenicity of the SARS-CoV-2 spike glycoprotein Cell 2020181281ndash292e6
16 Menachery VD Dinnon KH III Yount BL Jr et al Trypsin treatment unlocksbarrier for zoonotic bat coronavirus infection J Virol 202094e01774ndash19
17 Nao N Yamagishi J Miyamoto H et al Genetic predisposition to acquire a poly-basic cleavage site for highly pathogenic avian influenza virus hemagglutinin mBio20178e02298ndash16
18 Dong E Du H Gardner L An interactive web-based dashboard to track COVID-19in real time Lancet Infect Dis 202020533ndash534
19 Phua J Weng L Ling L et al Intensive care management of coronavirus disease2019 (COVID-19) challenges and recommendations Lancet Respir Med 20208506ndash517
20 van Doremalen N Bushmaker T Morris DH et al Aerosol and surface stability ofSARS-CoV-2 as compared with SARS-CoV-1 N Engl J Med 20203821564ndash1567
21 Bai Y Yao L Wei T et al Presumed asymptomatic carrier transmission of COVID-19 JAMA 20203231406ndash1407
22 Ye F Xu S Rong Z et al Delivery of infection from asymptomatic carriers ofCOVID-19 in a familial cluster Int J Infect Dis 202094133ndash138
23 Li Q Guan X Wu P et al Early transmission dynamics in Wuhan China of novelcoronavirus-infected pneumonia N Engl J Med 20203821199ndash1207
24 Auwaerter PG Coronavirus COVID-19 (SARS-CoV-2) [online] Available athopkinsguidescomhopkinsviewJohns_Hopkins_ABX_Guide540747allCoronavirus_COVID_19__SARS_CoV_2_ Accessed April 21 2020
25 Huang C Wang Y Li X et al Clinical features of patients infected with 2019 novelcoronavirus in Wuhan China Lancet 2020395497ndash506
26 Shi H Han X Jiang N et al Radiological findings from 81 patients with COVID-19pneumonia in Wuhan China a descriptive study Lancet Infect Dis 202020425ndash434
27 World Health Organization Report of the WHO-China Joint Mission on Coro-navirus Disease 2019 (COVID-19) Geneva Switzerland WHO 2020
28 Liu K Chen Y Lin R Han K Clinical features of COVID-19 in elderly patients acomparison with young and middle-aged patients J Infect 202080e14ndashe18
29 CDC COVID-19 Response Team Severe outcomes among patients with corona-virus disease 2019 (COVID-19)mdashUnited States February 12ndashMarch 16 2020MMWR Morb Mortal Wkly Rep 202069343ndash346
30 Alghamdi IG Hussain II Almalki SS Alghamdi MS Alghamdi MM El-SheemyMAThe pattern of Middle East respiratory syndrome coronavirus in Saudi Arabia adescriptive epidemiological analysis of data from the Saudi Ministry of Health Int JGen Med 20147417ndash423
31 Chan-Yeung M Xu RH SARS epidemiology Respirology 20038(suppl 1)S9ndashS14
32 Ludvigsson JF Systematic review of COVID-19 in children shows milder cases and abetter prognosis than adults Acta Paediatr 20201091088ndash1095
33 Viner RM Whittaker E Kawasaki-like disease emerging complication during theCOVID-19 pandemic Lancet 20203951741ndash1743
34 Mehta P McAuley DF Brown M Sanchez E Tattersall RS Manson JJ COVID-19consider cytokine storm syndromes and immunosuppression Lancet 20203951033ndash1034
35 Huang G Kovalic AJ Graber CJ Prognostic value of leukocytosis and lymphopeniafor coronavirus disease severity Emerg Infect Dis 202026
36 Li G Fan Y Lai Y et al Coronavirus infections and immune responses J Med Virol202092424ndash432
37 CDC Coronavirus Disease 2019 (COVID-19) [online] Atlanta GA CDC38 Yancy CW COVID-19 and African Americans JAMA Epub 2020 Apr 1539 Giacomelli A Pezzati L Conti F et al Self-reported olfactory and taste disorders in
SARS-CoV-2 patients a cross-sectional study Clin Infect Dis Epub 2020 Mar 2640 HaldrupM JohansenMI Fjaelstad AW Lugte- og smagstab som primaeligre symptom
pa COVID-19 [online] Ugeskr Laeligger 2020182V04200205
TAKE-HOME POINTS
Human coronaviruses have been shown to beneuropathogenic
Potential mechanisms of neuropathogenesis ofSARS-CoV-2 include hematogenous and transsy-naptic spread based on viral receptor expression
Neurologic sequelae of COVID-19 involve indirectdirect and postinfectious diseasemechanisms withconsequences that include stroke encephalitisencephalopathy and Guillain-Barre syndrome
Patient registries will be useful to identify and trackneurologic sequelae of SARS-CoV-2 infection andwill improve our understanding of the impact ofCOVID-19 on the nervous system
Appendix Authors
Name Location Contribution
Brigit High University ofColorado Aurora
Wrote themanuscript andmadethe tables
AlisonM HixonPhD
University ofColorado Aurora
Wrote themanuscript made thetables and made the figures
Kenneth LTyler MD
University ofColorado Aurora
Edited the manuscript
Amanda LPiquet MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
Victoria SPelak MD
University ofColorado Aurora
Wrote themanuscript andmadethe tables
e62 Neurology Clinical Practice | Volume 11 Number 2 | April 2021 NeurologyorgCP
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

41 Lechien JR Chiesa-Estomba CM De Siati DR et al Olfactory and gustatory dys-functions as a clinical presentation of mild-to-moderate forms of the coronavirusdisease (COVID-19) a multicenter European study Eur Arch Otorhinolaryngol20202772251ndash2261
42 Li Y Wang M Zhou Y et al Acute Cerebrovascular Disease Following COVID-19A Single Center Retrospective Observational Study SSRN Scholarly PaperRochester NY Social Science Research Network 2020 Report No ID 3550025
43 Mao L Jin HWangM et al Neurologic manifestations of hospitalized patients withcoronavirus disease 2019 in Wuhan China JAMA Neurol 2020771ndash9
44 Marchese-Ragona R Ottaviano G Nicolai P Vianello A Carecchio M Suddenhyposmia as a prevalent symptom of COVID-19 infection Otolaryngology 2020Preprint 2020-04-07
45 Moein ST Hashemian SMR Mansourafshar B Khorram-Tousi A Tabarsi P DotyRL Smell dysfunction a biomarker for COVID-19 Int Forum Allergy Rhinol Epub2020 Apr 17
46 Moriguchi T Harii N Goto J et al A first case of meningitisencephalitis associatedwith SARS-coronavirus-2 Int J Infect Dis 20209455ndash58
47 Poyiadji N Shahin G Noujaim D Stone M Patel S Griffith B COVID-19-associated acute hemorrhagic necrotizing encephalopathy CT and MRI featuresRadiology 2020296E119ndashE120
48 Toscano G Palmerini F Ravaglia S et al Guillain-Barre syndrome associated withSARS-CoV-2 N Engl J Med 20203822574ndash2576
49 Zhao H Shen D Zhou H Liu J Chen S Guillain-Barre syndrome associated withSARS-CoV-2 infection causality or coincidence Lancet Neurol 202019383ndash384
50 Zhou L Zhang M Wang J Gao J Sars-Cov-2 underestimated damage to nervoussystem Travel Med Infect Dis 2020 Epub 2020 Mar 24
51 Tong JY Wong A Zhu D Fastenberg JH Tham T The prevalence of olfactory andgustatory dysfunction in COVID-19 patients a systematic review and meta-analysisOtolaryngol Head Neck Surg 20201633ndash11
52 Kaye R Chang CWD Kazahaya K Brereton J Denneny JC COVID-19 anosmiareporting tool initial findings Otolaryngol Head Neck Surg 2020163132ndash134
53 Klok FA Kruip MJHA van der Meer NJM et al Incidence of thrombotic com-plications in critically ill ICU patients with COVID-19 Thromb Res 2020191145ndash147
54 Hess DC Eldahshan W Rutkowski E COVID-19-related stroke Transl Stroke Res202011322ndash325
55 Oxley TJ Mocco J Majidi S et al Large-vessel stroke as a presenting feature ofCovid-19 in the young N Engl J Med 2020382e60
56 Rudilosso S Esteller D Urra X Chamorro A Thalamic perforating artery stroke oncomputed tomography perfusion in a patient with coronavirus disease 2019 J StrokeCerebrovasc Dis 202029104974
57 Harzallah I Debliquis A Drenou B Lupus anticoagulant is frequent in patients withCovid-19 J Thromb Haemost Epub 2020 Apr 23
58 Zhang Y Xiao M Zhang S et al Coagulopathy and antiphospholipid antibodies inpatients with Covid-19 N Engl J Med 2020382e38
59 Filatov A Sharma P Hindi F Espinosa PS Neurological complications of corona-virus disease (COVID-19) encephalopathy Cureus 202012e7352
60 Lu L XiongW Liu D et al New-onset acute symptomatic seizure and risk factors incorona virus disease 2019 a retrospective multicenter study Epilepsia 202061e49ndashe53
61 Vollono C Rollo E Romozzi M et al Focal status epilepticus as unique clinicalfeature of COVID-19 a case report Seizure 202078109ndash112
62 Scheidl E Canseco DD Hadji-Naumov A Bereznai B Guillain-Barre syndromeduring SARS-CoV-2 pandemic a case report and review of recent literatureJ Peripher Nerv Syst 202025204ndash207
63 Camdessanche JP Morel J Pozzetto B Paul S Tholance Y Botelho-Nevers ECOVID-19 may induce Guillain-Barre syndrome Rev Neurol (Paris) 2020176516ndash518
64 Zhang W Zhao Y Zhang F et al The use of anti-inflammatory drugs in thetreatment of people with severe coronavirus disease 2019 (COVID-19) the per-spectives of clinical immunologists from China Clin Immunol 2020214108393
65 Luo P Liu Y Qiu L Liu X Liu D Li J Tocilizumab treatment in COVID-19 a singlecenter experience J Med Virol 202092814ndash818
66 McKee S Positive early data from siltuximab COVID-19 trial [online] Available atpharmatimescomnewspositive_early_data_from_siltuximab_covid-19_trial_1334145 Accessed April 20 2020
67 Brownlee W Bourdette D Broadley S Killestein J Ciccarelli O Treating multiplesclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pan-demic Neurology 202094949ndash952
68 Algahtani H Subahi A Shirah B Neurological complications of Middle East re-spiratory syndrome coronavirus a report of two cases and review of the literatureCase Rep Neurol Med 201620163502683
69 Arabi YM Harthi A Hussein J et al Severe neurologic syndrome associated withMiddle East respiratory syndrome corona virus (MERS-CoV) Infection 201543495ndash501
70 Ding Y He L Zhang Q et al Organ distribution of severe acute respiratory syn-drome (SARS) associated coronavirus (SARS-CoV) in SARS patients implicationsfor pathogenesis and virus transmission pathways J Pathol 2004203622ndash630
71 Ding Y Wang H Shen H et al The clinical pathology of severe acute respiratorysyndrome (SARS) a report from China J Pathol 2003200282ndash289
72 Gu J Gong E Zhang B et al Multiple organ infection and the pathogenesis of SARSJ Exp Med 2005202415ndash424
73 Kim JE Heo JH Kim HO et al Neurological complications during treatment ofMiddle East respiratory syndrome J Clin Neurol 201713227ndash233
74 Lau KK Yu WC Chu CM Lau ST Sheng B Yuen KY Possible central nervoussystem infection by SARS coronavirus Emerg Infect Dis 200410342ndash344
75 Morfopoulou S Brown JR Davies EG et al Human coronavirus OC43 associatedwith fatal encephalitis N Engl J Med 2016375497ndash498
76 Saad M Omrani AS Baig K et al Clinical aspects and outcomes of 70 patients withMiddle East respiratory syndrome coronavirus infection a single-center experiencein Saudi Arabia Int J Infect Dis 201429301ndash306
77 Turgay C Emine T Ozlem K Muhammet SP Haydar AT A rare cause of acuteflaccid paralysis human coronaviruses J Pediatr Neurosci 201510280ndash281
78 Yeh EA Collins A Cohen ME Duffner PK Faden H Detection of coronavirus inthe central nervous system of a child with acute disseminated encephalomyelitisPediatrics 2004113e73ndashe76
79 Hung EC Chim SS Chan PK et al Detection of SARS coronavirus RNA in thecerebrospinal fluid of a patient with severe acute respiratory syndrome Clin Chem2003492108ndash2109
80 Xu J Zhong S Liu J et al Detection of severe acute respiratory syndrome coro-navirus in the brain potential role of the chemokine mig in pathogenesis Clin InfectDis 2005411089ndash1096
81 Hamming I Timens W Bulthuis MLC Lely AT Navis GJ van Goor H Tissuedistribution of ACE2 protein the functional receptor for SARS coronavirus A firststep in understanding SARS pathogenesis J Pathol 2004203631ndash637
82 Rhoades RE Tabor-Godwin JM Tsueng G Feuer R Enterovirus infections of thecentral nervous system Virology 2011411288ndash305
83 Gross PM Chapter 31 circumventricular organ capillaries In Ermisch A Landgraf RRuhle HJ eds Progress in Brain Research New York NY Elsevier 1992219ndash233
84 Fry M Ferguson AV The sensory circumventricular organs brain targets for cir-culating signals controlling ingestive behavior Physiol Behav 200791413ndash423
85 Doobay MF Talman LS Obr TD Tian X Davisson RL Lazartigues E Differentialexpression of neuronal ACE2 in transgenic mice with overexpression of the brainrenin-angiotensin system Am J Physiol Regul Integr Comp Physiol 2007292R373ndashR381
86 Kaur C Rathnasamy G Ling EA The choroid plexus in healthy and diseased brainJ Neuropathol Exp Neurol 201675198ndash213
87 Shigemura N Takai S Hirose F Yoshida R Sanematsu K Ninomiya Y Expressionof renin-angiotensin system components in the taste organ of mice Nutrients 2019112251
88 Allen AM Chai SY Clevers J McKinley MJ Paxinos G Mendelsohn FAO Locali-zation and characterization of angiotensin II receptor binding and angiotensin con-verting enzyme in the human medulla oblongata J Comp Neurol 1988269249ndash264
89 Fodoulian L Tuberosa J Rossier D Landis BN Carleton A Rodriguez I SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the humanolfactory neuroepithelium Neuroscience 2020 Preprint 2020-04-02
90 Gupta K Mohanty SK Kalra S et al The molecular basis of loss of smell in 2019-nCoV infected individuals Open Sci Framework 2020 Preprint 2020-03-28
91 Baig AM Khaleeq A Ali U Syeda H Evidence of the COVID-19 virus targeting theCNS tissue distribution hostndashvirus interaction and proposed neurotropic mech-anisms ACS Chem Neurosci 202011995ndash998
92 Uhlen M Fagerberg L Hallstrom BM et al Proteomics Tissue-based map of thehuman proteome Science 20153471260419
93 Arbour N Cote G Lachance C Tardieu M Cashman NR Talbot PJ Acute andpersistent infection of human neural cell lines by human coronavirus OC43 J Virol1999733338ndash3350
94 Arbour N Ekande S Cote G et al Persistent infection of human oligodendrocyticand neuroglial cell lines by human coronavirus 229E J Virol 1999733326ndash3337
95 Talbot PJ Paquette JS Ciurli C Antel JP Ouellet F Myelin basic protein andhuman coronavirus 229E cross-reactive T cells in multiple sclerosis Ann Neurol199639233ndash240
96 Jacomy H Fragoso G Almazan G Mushynski WE Talbot PJ Human coronavirusOC43 infection induces chronic encephalitis leading to disabilities in BALBCmiceVirology 2006349335ndash346
97 Garg RK Mahadevan A Malhotra HS Rizvi I Kumar N Uniyal R Subacutesclerosing panencephalitis Rev Med Virol 201929e2058
98 Beatman EL Massey A Shives KD et al Alpha-synuclein expression restricts RNAviral infections in the brain J Virol 2015902767ndash2782
99 Bubak AN Como CN Coughlan CM et al Varicella-zoster virus infection ofprimary human spinal astrocytes produces intracellular amylin amyloid-beta and anamyloidogenic extracellular environment J Infect Dis 20202211088ndash1097
100 Hoffman LA Vilensky JA Encephalitis lethargica 100 years after the epidemic Brain20171402246ndash2251
101 McCall S Vilensky JA Gilman S Taubenberger JK The relationship between en-cephalitis lethargica and influenza a critical analysis J Neurovirol 200814177ndash185
102 Klopfenstein T Kadiane-Oussou NJ Toko L et al Features of anosmia in COVID-19 Med Mal Infect Epub 2020 Apr 17
103 Gilani S Roditi R Naraghi M COVID-19 and anosmia in Tehran Iran MedicalHypotheses 2020141109757
104 Ollarves-Carrero MF Rodriguez-Morales AG Bonilla-Aldana DK Rodriguez-Mo-rales AJ Anosmia in a healthcare worker with COVID-19 in Madrid Spain TravelMed Infect Dis 202035101666
105 DeBiasi RL Song X DelaneyM et al Severe COVID-19 in children and young adultsin the Washington DC Metropolitan Region J Pediatr Epub 2020 May 13
NeurologyorgCP Neurology Clinical Practice | Volume 11 Number 2 | April 2021 e63
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract

DOI 101212CPJ0000000000000908202111e48-e63 Published Online before print July 13 2020Neurol Clin Pract
Brigit High Alison M Hixon Kenneth L Tyler et al Neurology and the COVID-19 Pandemic Gathering Data for an Informed Response
This information is current as of July 13 2020
ServicesUpdated Information amp
httpcpneurologyorgcontent112e48fullhtmlincluding high resolution figures can be found at
References httpcpneurologyorgcontent112e48fullhtmlref-list-1
This article cites 88 articles 9 of which you can access for free at
Subspecialty Collections
httpcpneurologyorgcgicollectionviral_infectionsViral infections
httpcpneurologyorgcgicollectionencephalitisEncephalitis
httpcpneurologyorgcgicollectioncovid_19COVID-19
httpcpneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology
okehttpcpneurologyorgcgicollectionall_cerebrovascular_disease_strAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpcpneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpcpneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Neurology All rights reserved Print ISSN 2163-0402 Online ISSN 2163-0933since 2011 it is now a bimonthly with 6 issues per year Copyright copy 2020 American Academy of
is an official journal of the American Academy of Neurology Published continuouslyNeurol Clin Pract


















