
NCCN Lung Cancer - Journal of the National Comprehensive Cancer

National Comprehensive Cancer Network®
Robert W. Carlson, MD Chief Executive Officer
November 27, 2019
Tamara Syrek Jensen, JD Director Coverage and Analysis Group Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244
RE: National Coverage Analysis (NCA) Tracking Sheet for Next Generation Sequencing (NGS) for Medicare Beneficiaiies with Advanced Cancer (CAG-00450R)
Dear Ms. Syrek Jensen:
NCCN Member Institutions
Abramson Cancer Center at the University of Pennsylvania
Fred & Pamela Buffett Cancer Center
Case Comprehensive Cancer Genier/University Hospitals Seidman Cancer Center and Cleveland Clinic Taussig Cancer Institute
City of Hope National Medical Center
Dana-Farber/Brigham and Women's Cancer Center Massachusetts General Hospital Cancer Center
Duke Cancer Institute
Fox Chase Cancer Center
Huntsman Cancer Ins! itute al the University ol Utah
Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance
The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
Robert H. Lurie Comprehensive Cancer Center of Northwestern University
Mayo Clinic Cancer Center
The National Comprehensive Cancer Network® (NCCN®) is pleased to comment on the M . 1 si K
. omorm oun ettering
Proposed Decision Memo for Next Generation Sequencing (NGS) for Medicare cancer center
Beneficiaries with Advanced Cancer (CAG-00450R) as it relates to evidence Mollitt cancer Center
supporting the use of NGS for identification of gennline mutations. The Ohio state University Comprehensive Cancer Center James Cancer Hospital and
As an alliance of 28 leading academic cancer centers in the United States that treat soiove Research 1nstitute
hundreds of thousands of patients with cancer annually, NCCN is a developer of O'Neal comprehensive Cancer Center at UAB
authoritative infonnation regarding cancer prevention, screening, diagnosis, treatment, Roswell Park Comprehensive
and supportive care that is widely used by clinical professionals and payers alike. cancor cantor
NCCN's mission is to improve and facilitate quality, effective, efficient, and accessible Siternan cancer Center at Burnes-Jewish Hospital
cancer care so patients can live better lives. The NCCN Clinical Practice Guidelines in and Washington university
Oncology (NCCN Guidelines®) are a comprehensive set of guidelines detailing the School of Medicine
· 1 d · · d · · h 1 1 97 f St. Jude Children's
sequentla management ec1s10ns an mtervent10ns t at current y app y to percent o Research Hospital/
cancers affecting patients in the United States. NCCN Guidelines® and Library of The Univernity of Tennessee Health Science Center
Compendia products help ensure access to appropriate care, clinical decision-making, Stanford Cancer Institute
and assessment of quality improvement initiatives.
The NCCN Drugs & Biologics Compendium (NCCN Compendium®) has been
recognized by the Centers for Medicare and Medicaid Services (CMS) and clinical professionals in the commercial payer setting since 2008 as an evidence-based reference for establishment of coverage policy and coverage decisions regarding offlabel use of anticancer and cancer-related medications. Further, NCCN Guidelines and Library of Compendia products are utilized by cmmnercial payers that represent more
than 85 percent of covered lives in the United States.
The NCCN Biomarkers Compendium® is a tool developed to identify the appropriate use of biomarkers to screen, diagnose, monitor, and provide predictive and prognostic
3025 Chemical Road, Suite 100 I Plymouth Meeting, PA 19462 215.690.0300 I Fax: 215.690.0280
For Clinicians: NCCN.org I For Patients: NCCN.org/patients
UC Son Diego Moores Cancer Center
UCSF Helen Diller Family Comprehensive Cancer Center
University of Colorado Cancer Center
University of Michigan Rogel Cancer Genier
The University of Texas MD Anderson Cancer Center
University of Wisconsin Carbone Cancer Center
Vanderbilt-Ingram Cancer Center
Yale Cancer Center/ Smilow Cancer Hospital







APPENDIX 1

NCCN.org
Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®)
Version 3.2019 — January 18, 2019
Continue

BR/OV-2
jFor Cowden syndrome dermatologic manifestations, see COWD-1 and for PJS dermatologic manifestations, see NCCN Guidelines for Genetic/Familial High-Risk Assessment: Colorectal.
kIn some cases, multi-gene testing may be a preferable way to begin testing over the single-gene testing process.
ASSESSMENT GENE TESTINGk
See Targeted Testing Criteria forBRCA-Related Breast/Ovarian Cancer
Patient needs and concerns:•
and limitations• Goals for cancer family risk assessment
Detailed family history:• Expanded pedigree, particularly around individuals with a diagnosis of
cancer, to include a three-generational pedigree See BR/OV-B)
• Types of cancer, bilaterality, age at diagnosis• History of chemoprevention and/or risk-reducing surgery• Medical record documentation as needed, particularly prior genetic
testing results for patients and their family members and pathologyreports of primary cancers
Detailed medical and surgical history:• • • Reproductive history• Hormone or oral contraceptive use• Previous breast biopsies and pathology results• History of salpingo-oophorectomy
:•
Dermatologic, including oral mucosaHead circumference
NCCN Guidelines Version 3.2019Breast and/or Ovarian Cancer Genetic Assessment
Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines IndexTable of Contents
Discussion

BRCA-1
aFor further details regarding the nuances of genetic counseling and testing, see BR/OV-A.
bIrrespective of degree of relatedness.cFor the purposes of these guidelines, invasive and ductal carcinoma in situ breast
cancers should be included.dTwo breast cancer primaries includes bilateral (contralateral) disease or two or
more clearly separate ipsilateral primary tumors diagnosed either synchronously or asynchronously.
eClose blood relatives include first-, second-, and third-degree relatives on same side offamily. (See BR/OV-B)
fIncludes fallopian tube and primary peritoneal cancers. BRCA-related ovarian cancersare associated with epithelial, non-mucinous histology. Lynch syndrome can be associated with both non-mucinous and mucinous epithelial tumors. Be attentive for clinical evidence of Lynch syndrome (see NCCN Guidelines for Genetic/Familial High-Risk Assessment: Colorectal). Specific types of non-epithelial ovarian cancers and tumors can also be associated with other rare syndromes. Examples include an association between sex-cord tumors with annular tubules and Peutz-Jeghers syndrome or Sertoli-Leydig tumors and DICER1-related disorders.
gMetastatic prostate cancer is biopsy-proven and/or with radiographic evidence and includes distant metastasis andregional bed or nodes. It is not a biochemical recurrence.
hTesting for Ashkenazi Jewish founder-specific pathogenic/likely pathogenic variant(s), should be performed first.Comprehensive genetic testing may be considered if ancestry also includes non-Ashkenazi Jewish relatives or if other BRCA-related criteria are met. Founder pathogenic/likely pathogenic variants exist in other populations.
iApproximately 2%–5% of unselected cases of pancreatic adenocarcinoma will have a BRCA1/2 pathogenic/likelypathogenic variant. However, the disease is highly lethal and the option to test the affected relative may not be available in the future. Thus, there may be significant benefit to family members in testing these patients near the time of diagnosis. In addition, increasing evidence suggests that identification of a BRCA1/2 pathogenic/likely pathogenic variant may direct use of targeted therapies for patients with pancreatic cancer (See NCCN Guidelines for Pancreatic Adenocarcinoma). (Holter S, Borgida A, Dodd A, et al. J Clin Oncol 2015;33:3124-3129. Shindo K, Yu J, Suenaga M, et al. J Clin Oncol 2017;35:3382-3390.)
jEg, PARP inhibitors for ovarian cancer and metastatic HER2-negative breast cancer; platinum therapy for prostate cancer.See the relevant NCCN treatment guidelines (eg, NCCN Guidelines for Breast Cancer; NCCN Guidelines for Prostate Cancer) for further details.
kThis may be extended to an affected third-degree relative if related through two male relatives (eg, paternal grandfather’smother or sister).
BRCA1/2 TESTING CRITERIAa,b
genetic counseling, and often genetic testing and management.
BRCA testing criteria met
See Follow-up
If BRCA testing criteria not met, consider testing for other hereditary syndromes
If criteria for other hereditary syndromes not met, then cancer screening as per NCCN Screening Guidelines
• Individual from a family with a known BRCA1/2pathogenic/likely pathogenic variant, including suchvariants found on research testingb
• Personal history of breast cancerc + one or more of thefollowing:
Diagnosed 46-50 y with: An additional breast cancer primary at any aged
e with breast cancer at any agee
An unknown or limited family historya
Triple-negative breast cancerDiagnosed at any age with:
e with: – – ovarian carcinoma;f or
– male breast cancer; or– metastatic prostate cancer;g or– pancreatic cancer
d of breast cancer at any age in patient and/or in close blood relatives
h
• Personal history of ovarian carcinomaf
• Personal history of male breast cancer• Personal history of pancreatic canceri
• Personal history of metastatic prostate cancerg
• Personal history of high-grade prostate cancer
e with ovarian carcinoma, pancreatic cancer, or metastatic prostate cancerg at any age or breast cancer <50 y; or
e with breast, or prostate
h
• BRCA1/2 pathogenic/likely pathogenic variant
absence of germline pathogenic/likely pathogenicvariant analysis
• Regardless of family history, some individualswith an BRCAgenetic testing to determine eligibility for targetedtreatment
• An individual who does not meet the other criteriak
limitations of interpreting test results for an
NCCN Guidelines Version 3.2019BRCA-Related Breast and/or Ovarian Cancer Syndrome
Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines IndexTable of Contents
Discussion

BRCA-2
aFor further details regarding the nuances of genetic counseling and testing, see BR/OV-A.lIf of Ashkenazi Jewish descent, in addition to the specific familial pathogenic/likely
pathogenic variant, test for all three founder pathogenic/likely pathogenic variants. Additional testing may be indicated if there is also a significant family history of cancer on the side of the family without the known pathogenic/likely pathogenic variant.
mFor both affected and unaffected individuals of Ashkenazi Jewish descent with no known familial pathogenic/likely pathogenic variant, first test for the three common pathogenic variants. Then, if negative for the three pathogenic/likely pathogenic variants and ancestry also includes non-Ashkenazi Jewish relatives or other BRCA-related criteria are met, consider comprehensive genetic testing. For both affected and unaffected individuals who are non-Ashkenazi Jewish and who have no known familial pathogenic/likely pathogenic variants, comprehensive genetic testing is the approach, if done.
BRCA testing criteria met
BRCA-RELATED FOLLOW-UP
FAMILY STATUS
GENETIC TESTINGa TEST OUTCOMEa SCREENING RECOMMENDATION
Risk assessment and counseling:a
• Psychosocialassessmentand support
• Risk counseling• Education• Discussion of
genetic testing• Informed
consent
Familial BRCA1/2 pathogenic/likely pathogenic variant known
No known familial BRCA1/2 pathogenic/likely pathogenic variant
Recommend BRCA1/2 testing for
pathogenic/likely pathogenic variantl
Consider comprehensive BRCA1/2 testing of patient
member with highest likelihood of a pathogenic/likely pathogenic variantm
or
Consider multi-gene testing, if appropriate
Positive for familial BRCA1/2 pathogenic/likely pathogenic variant
BRCA1/2 testing not performed
Negative for familial BRCA1/2 pathogenic/likely pathogenic variant
Pathogenic/likely pathogenic variant foundNot testedNo pathogenic/likely pathogenic variant foundn
Variant of unknown
n
See Multi-Gene
See BRCA-Related Pathogenic Variant-Positive Management
Cancer screening as per NCCN Screening Guidelines
See BRCA-Related Pathogenic Variant-Positive Management
recommendations according to personal and family history
nIf no pathogenic/likely pathogenic variant is found, consider testing another family member with next highest likelihood of having a pathogenic/likely pathogenic variant and/or other hereditary breast/ovarian cancer syndromes such as Li-Fraumeni (LIFR-1) and/or Cowden syndrome (COWD-1) or multi-gene testing (GENE-1). For additional information on other genetic pathogenic/likely pathogenic variants associated with breast/ovarian cancer risk for which genetic testing is clinically available, see GENE-2.
NCCN Guidelines Version 3.2019BRCA-Related Breast and/or Ovarian Cancer Syndrome
Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines IndexTable of Contents
Discussion

GENE-1
MULTI-GENE TESTING
Overview of multi-gene testing• The recent introduction of multi-gene testing for hereditary forms of cancer has rapidly altered the clinical approach to testing at-risk
• Patients who have a personal or family history suggestive of a single inherited cancer syndrome are most appropriately managed by genetic
• or family history remains suggestive of an inherited susceptibility.
•
• a For many of these genes, there are limited data on the degree of cancer risk and there are no clear guidelines on risk management for carriers of pathogenic/likely pathogenic variants. Not all genes included on available multi-gene tests are necessarily clinically actionable.
• As is the case with high-risk genes, it is possible that the risks associated with moderate-risk genes may not be entirely due to that gene
known pathogenic/likely pathogenic variant alone to assign risk for relatives.• In many cases the information from testing for moderate penetrance genes does not change risk management compared to that based on
family history alone.• Pathogenic/likely pathogenic variants in many breast cancer susceptibility genes involved in DNA repair may be associated with rare
autosomal recessive conditions.•
multiple genes.•
test counseling.
ReferencesaResearch is evolving, and gene carriers should be encouraged to participate in clinical trials or genetic registries.
Continued
Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2019Genetic/Familial High-Risk Assessment: Breast and Ovarian
NCCN Guidelines IndexTable of Contents
Discussion

Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 3.2019Genetic/Familial High-Risk Assessment: Breast and Ovarian
MS-10
and management. The counselor should recommend genetic counselingand testing for at-risk relatives. Since some pathogenic or likely pathogenic variants are associated with rare autosomal recessive conditions (eg, Fanconi anemia is associated with ATM, BRCA2, BRIP1, and PALB2 variants), testing of a partner of a carrier of a pathogenic or likely pathogenic variant may be considered to inform reproductive decision-making.61 See Table 3 for a list of pathogenic/likely pathogenic variants associated with autosomal recessive conditions.
Multi-Gene Testing
Next-generation sequencing allows for the sequencing of multiple genes simultaneously. This is referred to as multi-gene testing. Multi-gene testing for hereditary forms of cancer has rapidly altered the clinical approach to testing at-risk patients and their families. Multi-gene testing simultaneously analyzes a set of genes that are associated with a specific family cancer phenotype or multiple phenotypes. Multiple studies have shown that this approach may detect pathogenic or likely pathogenic variants not found in single-gene testing.62-64 A study of 198 women referred for BRCA1/2testing who underwent multi-gene testing showed 16 deleterious mutations out of 141 women who tested negative for BRCA1/2 (11.4%; 95% CI, 7.0–17.7).63 The discovery of these mutations led to recommendations for further screening. Therefore, findings from multi-gene testing have the potential to alter clinical management.65
Multi-gene testing could include only high-penetrance genes associated with a specific cancer, or both high- and moderate-penetrance genes. Comprehensive cancer risk panels, which include a large number of genes associated with a variety of cancer types, are also available.66 The decision to use multi-gene testing for patient care should be no different than the rationale for testing a single gene known to be associated with the development of a specific type of cancer. Testing is focused on identifying a pathogenic or likely pathogenic variant known to be clinically
actionable; that is, whether the management of an individual patient is altered based on the presence or absence of the variant. Multi-gene testing may be most useful when more than one gene can explain an inherited cancer syndrome. For example, though ovarian cancer is mainly associated with BRCA1/2 pathogenic or likely pathogenic variants, it may also be associated with variants in the following genes: BARD1, BRIP1, MRE11A, MSH2, MSH6, NBN, PALB2, RAD51C, RAD51D, and TP53.67-70
Genes associated with hereditary breast cancer include the following that could potentially be included in a multi-gene test: BRCA1/ 2, ATM,BARD1, CHEK2, PALB2, TP53, PTEN, STK11, and CDH1.10,63,69-75 In these cases where more than one pathogenic or likely pathogenic variant could potentially influence a condition, multi-gene testing may be more efficient and/or cost-effective.66,76,77 Multi-gene testing may also be considered for those who tested negative (indeterminate) for one particular syndrome, but whose personal and family history is suggestive of an inherited susceptibility.66,78
There are several issues to consider regarding multi-gene testing. First, commercially available tests may differ significantly on a number of factors, such as number of genes analyzed, turnaround time, insurance coverage, and variant reclassification protocol, among others. Tests requiring a longer turnaround time may not be suitable for patients who need rapid results. The specific laboratory and multi-gene test should be chosen carefully.66 Second, in some cases, next-generation sequencing may miss some pathogenic or likely pathogenic variants that would have been detected with traditional single-gene analysis.66 Third, pathogenic or likely pathogenic variants identified for more than one gene add complexity that may lead to difficulty in making risk management recommendations.78 A management plan should only be developed for identified pathogenic or likely pathogenic variants that are clinically actionable.

Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 3.2019Genetic/Familial High-Risk Assessment: Breast and Ovarian
MS-11
A major dilemma regarding multi-gene testing is that there are limited data and a lack of clear guidelines regarding degree of cancer risk associated with some of the genes assessed in multi-gene testing, and how to communicate and manage risk for carriers of these genes.73,79-82 This issue is compounded by the low incidence rates of hereditary disease, leading to a difficulty in conducting adequately powered studies.79 Some multi-gene tests may include moderate-penetrance genes, for which there are little available data regarding degree of cancer risk and guidelines for risk management.66,73,83-85 Further, it is possible that the risks associated with these genes may not entirely be due to that gene only, but may be influenced by gene/gene or gene/environment interactions. Also, certain variants in a gene may be associated with a different degree of risk than other variants in that gene. For example, the presence of certain ATMgenetic variants is associated with an increased risk for early-onset breast cancer and frequent bilateral occurrence, but the association between other ATM variants and breast cancer susceptibility is less clear.86-89
As a result of these dilemmas, risk management following detection of a pathogenic or likely pathogenic variant for a moderate-risk gene, and how best to communicate risk to relatives, is currently unknown.85,90 Further, the information gained from testing for moderate-penetrance genes may not change risk management recommendations significantly compared to that based on family history only. Multi-gene tests also increase the likelihood of detecting a VUS.63,64,66,73,74,85,91 Multi-gene analyses of DNA samples from individuals with breast cancer showed that a VUS was found in 33% to 40% of individuals.74 An analysis of 1191 individuals who underwent testing and were enrolled in PROMPT showed that 37% of variants found were classified as a VUS.54 The considerable possibility of detecting a VUS adds to the complexity of counseling following multi-gene testing. However, as multi-gene testing is increasingly used, the frequency of a VUS being detected is expected to decrease.
Multi-gene testing is a new and rapidly growing field, but there is currently a lack of evidence regarding proper procedures and risk management strategies that should follow testing, especially when pathogenic or likely pathogenic variants are found for moderate-penetrance genes and when a VUS is found.92 For this reason, the NCCN Panel recommends that, whenmulti-gene testing is offered, it is done in the context of professional genetic expertise, with pre- and post-test counseling being offered. Panel recommendations are in agreement with recommendations by ASCO, which issued an updated statement regarding genetic testing in 2015.93
Given the limited data available in this field, carriers of a pathogenic or likely pathogenic variant should be encouraged to participate in clinical trials or genetic registries.
Hereditary Breast or Breast/Ovarian Cancer Syndromes
Breast cancer is the most frequently diagnosed cancer globally and is theleading cause of cancer death in women.94 The ACS estimates that 255,180 Americans will be diagnosed with invasive breast cancer and 41,070 will die of the disease in the United States in 2017.95 Up to 10% of breast cancers are due to specific mutations in single genes that are passed down in a family.6,8,69,75 Specific patterns of hereditary breast/ovarian cancers are linked to pathogenic or likely pathogenic variants in the BRCA1/2 genes.96,97 In addition, two very rare hereditary cancer syndromes exhibiting an increased risk for breast cancer are Li-Fraumeni syndrome (LFS) and Cowden syndrome, which are related to germline pathogenic or likely pathogenic variants in the TP53 and PTENgenes, respectively.98,99 Similar to the BRCA1/2 genes, the TP53 andPTEN genes encode for proteins involved in processes related to tumor suppression, such as DNA repair and cell cycle regulation.
These hereditary syndromes share several features beyond elevation of breast cancer risk. These syndromes arise from germline pathogenic or likely pathogenic variants that are not within sex-linked genes; hence, the

Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 3.2019Genetic/Familial High-Risk Assessment: Breast and Ovarian
MS-54
48. Hong YC, Liu HM, Chen PS, et al. Hair follicle: a reliable source ofrecipient origin after allogeneic hematopoietic stem cell transplantation.Bone Marrow Transplant 2007;40:871-874. Available at:http://www.ncbi.nlm.nih.gov/pubmed/17704789.
49. Tran SD, Pillemer SR, Dutra A, et al. Differentiation of human bonemarrow-derived cells into buccal epithelial cells in vivo: a molecularanalytical study. Lancet 2003;361:1084-1088. Available at:http://www.ncbi.nlm.nih.gov/pubmed/12672312.
50. Bougeard G, Baert-Desurmont S, Tournier I, et al. Impact of the MDM2SNP309 and p53 Arg72Pro polymorphism on age of tumour onset in Li-Fraumeni syndrome. J Med Genet 2006;43:531-533. Available at:http://www.ncbi.nlm.nih.gov/pubmed/16258005.
51. Chibon F, Primois C, Bressieux JM, et al. Contribution of PTEN largerearrangements in Cowden disease: a multiplex amplifiable probehybridisation (MAPH) screening approach. J Med Genet 2008;45:657-665.Available at: http://www.ncbi.nlm.nih.gov/pubmed/18456716.
52. Palma MD, Domchek SM, Stopfer J, et al. The relative contribution ofpoint mutations and genomic rearrangements in BRCA1 and BRCA2 inhigh-risk breast cancer families. Cancer Res 2008;68:7006-7014.Available at: http://www.ncbi.nlm.nih.gov/pubmed/18703817.
53. Weitzel JN, Lagos VI, Herzog JS, et al. Evidence for commonancestral origin of a recurring BRCA1 genomic rearrangement identified inhigh-risk Hispanic families. Cancer Epidemiol Biomarkers Prev2007;16:1615-1620. Available at:http://www.ncbi.nlm.nih.gov/pubmed/17646271.
54. Balmana J, Digiovanni L, Gaddam P, et al. Conflicting interpretation ofgenetic variants and cancer risk by commercial laboratories as assessedby the prospective registry of multiplex testing. J Clin Oncol 2016;34:4071-4078. Available at: https://www.ncbi.nlm.nih.gov/pubmed/27621404.
55. Vail PJ, Morris B, van Kan A, et al. Comparison of locus-specificdatabases for BRCA1 and BRCA2 variants reveals disparity in variantclassification within and among databases. J Community Genet
2015;6:351-359. Available at: https://www.ncbi.nlm.nih.gov/pubmed/25782689.
56. Lincoln SE, Yang S, Cline MS, et al. Consistency of BRCA1 andBRCA2 variant classifications among clinical diagnostic laboratories. JCOPrecis Oncol 2017;1. Available at:https://www.ncbi.nlm.nih.gov/pubmed/28782058.
57. Eccles DM, Mitchell G, Monteiro AN, et al. BRCA1 and BRCA2 genetictesting-pitfalls and recommendations for managing variants of uncertainclinical significance. Ann Oncol 2015;26:2057-2065. Available at:http://www.ncbi.nlm.nih.gov/pubmed/26153499.
58. Badalato L, Kalokairinou L, Borry P. Third party interpretation of rawgenetic data: an ethical exploration. Eur J Hum Genet 2017;25:1189-1194.Available at: https://www.ncbi.nlm.nih.gov/pubmed/28832567.
59. Tandy-Connor S, Guiltinan J, Krempely K, et al. False-positive resultsreleased by direct-to-consumer genetic tests highlight the importance ofclinical confirmation testing for appropriate patient care. Genet Med2018;20:1515-1521. Available at:https://www.ncbi.nlm.nih.gov/pubmed/29565420.
60. Green RC, Berg JS, Grody WW, et al. ACMG recommendations forreporting of incidental findings in clinical exome and genome sequencing.Genet Med 2013;15:565-574. Available at:https://www.ncbi.nlm.nih.gov/pubmed/23788249.
61. Offit K, Levran O, Mullaney B, et al. Shared genetic susceptibility tobreast cancer, brain tumors, and Fanconi anemia. J Natl Cancer Inst2003;95:1548-1551. Available at:http://www.ncbi.nlm.nih.gov/pubmed/14559878.
62. Walsh T, Casadei S, Coats KH, et al. Spectrum of mutations inBRCA1, BRCA2, CHEK2, and TP53 in families at high risk of breastcancer. JAMA 2006;295:1379-1388. Available at:http://www.ncbi.nlm.nih.gov/pubmed/16551709.

Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 3.2019Genetic/Familial High-Risk Assessment: Breast and Ovarian
MS-55
63. Kurian AW, Hare EE, Mills MA, et al. Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J ClinOncol 2014;32:2001-2009. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24733792.
64. Kurian AW, Ward KC, Hamilton AS, et al. Uptake, results, andoutcomes of germline multiple-gene sequencing after diagnosis of breastcancer. JAMA Oncol 2018;4:1066-1072. Available at:https://www.ncbi.nlm.nih.gov/pubmed/29801090.
65. Desmond A, Kurian AW, Gabree M, et al. Clinical actionability ofmultigene panel testing for hereditary breast and ovarian cancer riskassessment. JAMA Oncol 2015;1:943-951. Available at:http://www.ncbi.nlm.nih.gov/pubmed/26270727.
66. Hall MJ, Forman AD, Pilarski R, et al. Gene panel testing for inheritedcancer risk. J Natl Compr Canc Netw 2014;12:1339-1346. Available at:http://www.ncbi.nlm.nih.gov/pubmed/25190699.
67. Walsh T, Casadei S, Lee MK, et al. Mutations in 12 genes for inheritedovarian, fallopian tube, and peritoneal carcinoma identified by massivelyparallel sequencing. Proc Natl Acad Sci U S A 2011;108:18032-18037.Available at: http://www.ncbi.nlm.nih.gov/pubmed/22006311.
68. Lilyquist J, LaDuca H, Polley E, et al. Frequency of mutations in alarge series of clinically ascertained ovarian cancer cases tested on multi-gene panels compared to reference controls. Gynecol Oncol2017;147:375-380. Available at:https://www.ncbi.nlm.nih.gov/pubmed/28888541.
69. Couch FJ, Shimelis H, Hu C, et al. Associations between cancerpredisposition testing panel genes and breast cancer. JAMA Oncol2017;3:1190-1196. Available at:https://www.ncbi.nlm.nih.gov/pubmed/28418444.
70. Kurian AW, Hughes E, Handorf EA, et al. Breast and ovarian cancerpenetrance estimates derived from germline multiple-gene sequencingresults in women. JCO Precision Oncology 2017;1:1-12. Available at:http://ascopubs.org/doi/abs/10.1200/PO.16.00066.
71. Decker B, Allen J, Luccarini C, et al. Rare, protein-truncating variantsin ATM, CHEK2 and PALB2, but not XRCC2, are associated withincreased breast cancer risks. J Med Genet 2017;54:732-741. Availableat: https://www.ncbi.nlm.nih.gov/pubmed/28779002.
72. Castera L, Krieger S, Rousselin A, et al. Next-generation sequencingfor the diagnosis of hereditary breast and ovarian cancer using genomiccapture targeting multiple candidate genes. Eur J Hum Genet2014;22:1305-1313. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24549055.
73. Rainville IR, Rana HQ. Next-generation sequencing for inheritedbreast cancer risk: counseling through the complexity. Curr Oncol Rep2014;16:371. Available at: http://www.ncbi.nlm.nih.gov/pubmed/24488544.
74. Tung N, Battelli C, Allen B, et al. Frequency of mutations in individualswith breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer 2015;121:25-33.Available at: http://www.ncbi.nlm.nih.gov/pubmed/25186627.
75. Buys SS, Sandbach JF, Gammon A, et al. A study of over 35,000women with breast cancer tested with a 25-gene panel of hereditarycancer genes. Cancer 2017;123:1721-1730. Available at:https://www.ncbi.nlm.nih.gov/pubmed/28085182.
76. Hall MJ, Obeid E, Daly MB. Multigene panels to evaluate hereditarycancer risk: reckless or relevant? J Clin Oncol 2016;34:4186-4187.Available at: https://www.ncbi.nlm.nih.gov/pubmed/27551136.
77. Manchanda R, Patel S, Gordeev VS, et al. Cost-effectiveness ofpopulation-based BRCA1, BRCA2, RAD51C, RAD51D, BRIP1, PALB2mutation testing in unselected general population women. J Natl CancerInst 2018;110:714-725. Available at:https://www.ncbi.nlm.nih.gov/pubmed/29361001.
78. Walsh T, Lee MK, Casadei S, et al. Detection of inherited mutations forbreast and ovarian cancer using genomic capture and massively parallelsequencing. Proc Natl Acad Sci U S A 2010;107:12629-12633. Availableat: http://www.ncbi.nlm.nih.gov/pubmed/20616022.

Version 3.2019, 01/18/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 3.2019Genetic/Familial High-Risk Assessment: Breast and Ovarian
MS-56
79. Bombard Y, Bach PB, Offit K. Translating genomics in cancer care. JNatl Compr Canc Netw 2013;11:1343-1353. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24225968.
80. Blazer KR, Slavin T, Weitzel JN. Increased reach of genetic cancerrisk assessment as a tool for precision management of hereditary breastcancer. JAMA Oncol 2016;2:723-724. Available at:https://www.ncbi.nlm.nih.gov/pubmed/26869327.
81. Tung N, Domchek SM, Stadler Z, et al. Counselling framework formoderate-penetrance cancer-susceptibility mutations. Nat Rev Clin Oncol2016;13:581-588. Available at:http://www.ncbi.nlm.nih.gov/pubmed/27296296.
82. van Marcke C, De Leener A, Berliere M, et al. Routine use of genepanel testing in hereditary breast cancer should be performed withcaution. Crit Rev Oncol Hematol 2016;108:33-39. Available at:https://www.ncbi.nlm.nih.gov/pubmed/27931838.
83. Cragun D, Radford C, Dolinsky JS, et al. Panel-based testing forinherited colorectal cancer: a descriptive study of clinical testing performedby a US laboratory. Clin Genet 2014;86:510-520. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24506336.
84. LaDuca H, Stuenkel AJ, Dolinsky JS, et al. Utilization of multigenepanels in hereditary cancer predisposition testing: analysis of more than2,000 patients. Genet Med 2014;16:830-837. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24763289.
85. Mauer CB, Pirzadeh-Miller SM, Robinson LD, Euhus DM. Theintegration of next-generation sequencing panels in the clinical cancergenetics practice: an institutional experience. Genet Med 2014;16:407-412. Available at: http://www.ncbi.nlm.nih.gov/pubmed/24113346.
86. Brunet J, Gutierrez-Enriquez S, Torres A, et al. ATM germlinemutations in Spanish early-onset breast cancer patients negative forBRCA1/BRCA2 mutations. Clin Genet 2008;73:465-473. Available at:http://www.ncbi.nlm.nih.gov/pubmed/18384426.
87. Heikkinen K, Rapakko K, Karppinen SM, et al. Association of commonATM polymorphism with bilateral breast cancer. Int J Cancer 2005;116:69-72. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15756685.
88. Thompson D, Antoniou AC, Jenkins M, et al. Two ATM variants andbreast cancer risk. Hum Mutat 2005;25:594-595. Available at:http://www.ncbi.nlm.nih.gov/pubmed/15880680.
89. Tommiska J, Jansen L, Kilpivaara O, et al. ATM variants and cancerrisk in breast cancer patients from Southern Finland. BMC Cancer2006;6:209. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16914028.
90. Obeid EI, Hall MJ, Daly MB. Multigene panel testing and breast cancerrisk: is it time to scale down? JAMA Oncol 2017;3:1176-1177. Available at:https://www.ncbi.nlm.nih.gov/pubmed/28418452.
91. Kapoor NS, Curcio LD, Blakemore CA, et al. Multigene panel testingdetects equal rates of pathogenic BRCA1/2 mutations and has a higherdiagnostic yield compared to limited BRCA1/2 analysis alone in patients atrisk for hereditary breast cancer. Ann Surg Oncol 2015;22:3282-3288.Available at: http://www.ncbi.nlm.nih.gov/pubmed/26219241.
92. Axilbund JE. Panel testing is not a panacea. J Clin Oncol2016;34:1433-1435. Available at:https://www.ncbi.nlm.nih.gov/pubmed/26976416.
93. Robson ME, Bradbury AR, Arun B, et al. American Society of ClinicalOncology Policy statement update: genetic and genomic testing for cancersusceptibility. J Clin Oncol 2015;33:3660-3667. Available at:https://www.ncbi.nlm.nih.gov/pubmed/26324357.
94. Forouzanfar MH, Foreman KJ, Delossantos AM, et al. Breast andcervical cancer in 187 countries between 1980 and 2010: a systematicanalysis. Lancet 2011;378:1461-1484. Available at:https://www.ncbi.nlm.nih.gov/pubmed/21924486.
95. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer JClin 2017;67:7-30. Available at:https://www.ncbi.nlm.nih.gov/pubmed/28055103.

APPENDIX 2

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®)
Genetic/Familial High-Risk Assessment: Colorectal
Version 2.2019 — August 8, 2019
Continue
NCCN.org

NCCN Guidelines Version 2.2019Lynch Syndrome
Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 2.2019Lynch Syndrome
NCCN Guidelines IndexTable of Contents
Discussion
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
LS-1
a An individual with expertise in genetics should be involved in the testing process. Minimum pretest counseling (in person or through written or video) materials with pros and cons of testing should be provided. See Principles of Cancer Risk
.b Irrespective of degree of relatedness.c
diagnosis, multiple primaries, and colorectal or endometrial cancers. Limitations of interpreting test results should be discussed if testing tumors other than colorectal or endometrial cancers. If IHC/MSI previously done, .d The panel recommends tumor testing with IHC and/or MSI be used as the primary approach for pathology lab-based universal screening.e Tumor NGS panels should include at a minimum the MMR genes (MLH1, MSH2, MSH6, PMS2, and EPCAM), other known familial cancer genes, MSI, and BRAF.
f This approach may be preferred in patients with a strong family history or if
g
discussed.h The recommendation to manage patients in whom genetic testing was not done using LS-management recommendations is category 2B.
i For individuals found to have an LS pathogenic variant, see LS management recommendations. j
.
RISK STATUS
No known LS pathogenic variant in proband or family
LS pathogenic variant knownb in family
TESTING STRATEGYa
Genetic testing for familial pathogenic variant
Colorectal or endometrial tumor available for proband or familyc
tumor not availablec
relative unavailable
Tumor testing (See LS-A) with immunohistochemistry (IHC), MSI,d and/or a comprehensive tumor NGS paneleorGermline multi-gene testing (See GENE-1)f,g
Germline multi-gene testing (See GENE-1)f,g
Positive for familial LS pathogenic variant Genetic testing not done (category 2Bh)
Negative for familial LS pathogenic variant
See Tumor Testing Results and Additional Testing Strategies (LS-A 4 of 5)i
Positive pathogenic variant found
Not tested or no pathogenic variant or variant of uncertain
See Lynch Syndrome Management (LS-2, LS-3, and LS-4) and Genetic testing for at-risk family membersa,j
See NCCN Guidelines for Colorectal Cancer Screening - Additional testing may be indicated based on personal and family medical history
See appropriate gene in Table 5 on and Genetic testing for at-risk family membersa,j
Tailored surveillance based on individual and family risk assessment
or
STRATEGIES FOR EVALUATING FOR LS IN INDIVIDUALS MEETING CRITERIA FOR THE EVALUATION OF LSaLSaSTRATEGIES FOR EVALUATING FOR LS IN INDIVIDUALS MEETING CRITERIA FOR THE EVALUATION OF
Noknown LSpathogenicp gvariant in proband or pfamily Germline multi-gene
(S GENE 1testing
orGermline multi-gene testing (S GENE 1)f g
g

NCCN Guidelines Version 2.2019Adenomatous Polyposis Testing Criteria
Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
POLYP-1
a Irrespective of degree of relatedness.b Age of onset, family history, personal history of colorectal cancer, and/or presence of other
c There are clinically relevant yet rarer genes that can cause a polyposis that may be phenotypically indistinguishable from APC/MUTYH polyposis. d Multi-gene panel should include all polyposis and colorectal cancer genes (Stanich P, et al. Clin Gastroenterol Hepatol 2018).e When colonic polyposis is present in a single person with a negative family history,
MUTYH (targeted testing for the two common northern European founder pathogenic
if biallelic pathogenic variants are not found). When colonic polyposis is present only in
and MUTYH is at the discretion of the clinician. MUTYH genetic testing is not indicated based on a personal history of a hepatoblastoma, cribriform-morular variant of papillary thyroid cancer, or multifocal/bilateral CHRPE.
RISK STATUS
TESTING STRATEGY
RESULTS TREATMENT/SURVEILLANCE
• Personal history of 20 cumulative adenomas
• Known pathogenic variant in adenomatous polyposis gene in familya
• Consider testing if a personal history of a desmoid tumor, hepatoblastoma, cribriform-morular variant of papillary thyroid cancer, or multifocal/bilateral CHRPE, if individual meets criteria 1 or 3 for SPS (see SPS-1) with at least some adenomas or personal
cumulative adenomasb
Pathogenic variant(s) known
Genetic testing for familial pathogenic variant
No known pathogenic variants in any polyposis genec
Germline multi-gene testing (preferred)d (See GENE-1)orPolyposis syndrome-
(APC and/or MUTYH)e
ADENOMATOUS POLYPOSIS TESTING CRITERIA
Positive for familial APC pathogenic variant
Genetic testing not done
Negative for familial pathogenic variant
Positive for biallelic MUTYH pathogenic variant
No pathogenic variant found in any polyposis genef
To determine classical FAP vs. AFAP, see FAP/AFAP-1
See NCCN Guidelines for Colorectal Cancer Screening- Additional testing may be indicated based on personal and family medical history
To determine classical FAP vs. AFAP, see FAP/AFAP-1
See MAP-1
Tailored surveillance based on individual and family risk assessment (See CPUE-1 or See NCCN Guidelines for Colorectal Cancer Screening- Average risk)
Positive for pathogenic variant in another polyposis gene
One MUTYH pathogenic variant foundf
Positive for biallelic MUTYH pathogenic variant See MAP-1
Positive for familial APC pathogenic variant
Manage as if positive for the known familial pathogenic variant
Positive for known familial pathogenic variant in another polyposis gene
Genetic testing not done See CPUE-1
One familal MUTYH pathogenic variant foundf
f
variant, testing the children for the familial MUTYH pathogenic variants is indicated. If the
future children could be at-risk for MAP).
Adenomatous Polyposis Testing Criteria
No knownpathogenicp gvariants in anyn any
genecpolyposis
Germline multi-gene testing ng
dggg
(preferred)d
TREATMENT/SURVEILLANCE

NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines IndexTable of Contents
Discussion
Table 3: Examples of Clinical Scenarios for Which Multi-Gene Testing Should and Should Not Be UsedExamples of clinical scenarios for which multi-gene testing should be considered: • Personal medical and/or family cancer history meets criteria for more than one hereditary cancer syndrome (ie, family meets both
BRCA-related breast and/or ovarian cancer and LS clinical criteria or family history of young-onset CRC and oligopolyposis)• Colonic polyposis with uncertain histology• Family cancer history does not meet established testing guidelines, but consideration of inherited cancer risk persists and an
appropriate panel is available• Individuals concerned about cancer predisposition for whom family cancer history is limited or unknown• • Adenomatous polyposisExamples of clinical scenarios for which multi-gene testing SHOULD NOT be considered:f• An individual from a family with a known pathogenic variant and no other reason for multi-gene testing•
f
GENE-3
Continued
MULTI-GENE TESTING

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-26
Colonic Adenomatous Polyposis of Unknown Etiology (CPUE-1)
When genetic testing in an individual with polyposis reveals no APC and one or no MUTYH mutations, surveillance should be tailored based on individual and family risk assessment, as outlined in the guidelines. If the patient has a history of 100 adenomas, the panel recommends that the patient be managed as described above for patients with a personal history of classical FAP.
If the patient has a history of >20 but <100 adenomas, and the adenoma burden is small and considered to be manageable by colonoscopy and polypectomy, the panel recommends colonoscopy and polypectomy every 1 to 2 years. Clearing of all polyps is recommended and can be repeated at short intervals if residual polyps are present.
If the patient has a history of >20 but <100 adenomas, but the adenoma burden is dense and considered unmanageable by polypectomy, the panel recommends a subtotal colectomy. A proctocolectomy may be considered if there is a dense rectal polyposis that cannot be managed by polypectomy.
In patients with a family history of 100 adenomas diagnosed at age <40 years in a first-degree relative, there are limited data to suggest definitive recommendations for when to initiate screening or the interval of screening. The panel suggests consideration for colonoscopy screenings to begin at age 10 to 15 years with the following intervals post initial screen: every 1 year until age 24 years, every 2 years from 24 to 34 years, every 3 years from 34 to 44 years, and then every 3 to 5 years thereafter. If polyposis is detected, the panel recommends that patients be managed as described above for patients with a personal history of classical FAP. In addition, family members affected with polyposis should consider genetic testing as previously described for FAP and MAP.
In patients with a family history of >20 to <100 adenomas in a first-degree relative, there are limited data to suggest definitive recommendations for when to initiate screening or the interval of screening. The panel suggests considering colonoscopy screenings and polypectomy every 3 to 5 years starting at the same age as the youngest diagnosis of polyposis in the family if uncomplicated by cancer or by age 40 years, whichever is earliest. If multiple polyps are found during screenings, the interval for colonoscopies should occur every 1 to 3 years, depending on the type, number, and size of polyps. As described above, family members affected with polyposis should consider genetic testing as previously described for FAP and MAP.
In patients with a family history of >100 adenomas diagnosed at age 40 years in a first-degree relative, there are limited data to suggest definitive recommendations for when to initiate screening or the interval of screening. The panel suggests considering colonoscopy screenings and polypectomy every 2 to 3 years starting at age 40 years if uncomplicated by cancer. If multiple polyps are found during screenings, the interval for colonoscopies should occur every 1 to 3 years, depending on the type, number, and size of polyps. As described above, family members affected with polyposis should consider genetic testing as previously described for FAP and MAP.
Multi-gene Testing (GENE-1)
Next-generation sequencing allows for the sequencing of multiple genes simultaneously. This is referred to as multi-gene testing. The NCCN panel added information regarding multi-gene testing for the 2016 update. The recent introduction of multi-gene testing for hereditary forms of cancer has rapidly altered the clinical approach to testing at-risk patients and their families. Multi-gene testing simultaneously analyzes a set of genes that are associated with a specific family cancer phenotype or multiple phenotypes. Multi-gene testing may include syndrome-specific tests (ie,

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-27
panels that test for only one syndrome like Lynch syndrome), cancer-specific tests (ie, panels that test for more than one gene associated with a specific type of cancer like CRC), and comprehensive cancer panels (ie, panels that test for more than one gene associated with multiple cancers or cancer syndromes).
Multi-gene testing could include only high-penetrance genes associated with a specific cancer, or both high- and moderate-penetrance genes. Comprehensive cancer risk panels, which include a large number of genes associated with a variety of cancer types, are also available.209 The decision to use multi-gene testing for patient care should be no different than the rationale for testing a single gene known to be associated with the development of a specific type of cancer. Testing is focused on identifying a mutation known to be clinically actionable; that is, whether the management of an individual patient is altered based on the presence or absence of a mutation. Multi-gene testing may be most useful when more than one gene can explain a patient’s clinical and family history. In these cases where more than one gene mutation could potentially influence a condition, multi-gene testing may be more efficient and/or cost-effective.209
Multigene testing with panels that include genes associated with Lynch syndrome, as well as other highly penetrant genes associated with CRC, may be cost effective,210 and this approach may detect mutations not found in single-gene testing.211 Multi-gene testing may also be considered for those who tested negative (indeterminate) for one particular syndrome, but whose personal and family history is strongly suggestive of an inherited susceptibility.209,212
A major dilemma regarding multi-gene testing is that there are limited data and a lack of clear guidelines regarding degree of cancer risk associated with some of the genes assessed in multi-gene testing, and how to communicate and manage risk for carriers of these genes.212-214 This issue is compounded by the low incidence rates of hereditary disease, leading to
a difficulty in conducting adequately powered studies.213 Some multi-gene tests may include low or moderate-penetrance genes, for which there are little available data regarding degree of cancer risk and guidelines for risk management.209,214-217 Further, it is possible that the risks associated with these genes may not be due entirely to that gene only, but may be influenced by gene/gene or gene/environment interactions. Multi-gene tests also increase the likelihood of detecting VUS,209,212,214,217-220 with likelihood rates ranging from 17% to 38%.215,217,218,221 The considerable possibility of detecting a VUS adds to the complexity of counseling following multi-gene testing. However, as multi-gene testing is increasingly used, the frequency of a VUS being detected is expected to decrease.
There are other issues to consider regarding multi-gene testing. First, commercially available tests may differ significantly on a number of factors, such as number of genes analyzed, turnaround time, and insurance coverage, among others. Tests requiring a longer turnaround time may not be suitable for patients who need rapid results. The specific laboratory and multi-gene test should be chosen carefully.209 Second, in some cases, next-generation sequencing may miss some mutations that would have been detected with traditional single-gene analysis.209 Third, mutations identified for more than one gene add complexity that may lead to difficulty in making risk management recommendations.212 Amanagement plan should only be developed for identified gene mutations that are clinically actionable; care should be taken to ensure that overtreatment or overscreening does not occur due to findings for which clinical management is uncertain, or findings that are incorrectly interpreted due to lack of evidence.
Multi-gene testing is a new and rapidly growing field, but there is currently a lack of evidence regarding proper procedures and risk management strategies that should follow testing, especially when mutations are found for moderate-penetrance genes and when a VUS is

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-28
found. For this reason, the NCCN panel recommends that multi-gene testing be offered in the context of professional genetic expertise, with pre- and post-test counseling being offered. Panel recommendations are in agreement with recommendations by ASCO, which issued an updated statement regarding genetic testing in 2015.222 Carriers of a genetic mutation should be encouraged to participate in clinical trials or genetic registries.
Multi-gene testing is not recommended when: 1) there is an individual from a family with a known mutation and there is no other reason for multi-gene testing; 2) the patient’s family history is strongly suggestive of a known hereditary syndrome; and, 3) the patient is diagnosed with CRC with MSI or loss of one or more DNA MMR proteins. In these three scenarios, syndrome-specific panels may be considered.
Multi-gene testing may be considered (but may not be limited to based on clinical judgement) the following scenarios:
A patient has a personal or family history that meets criteria for more than one hereditary cancer syndrome (eg, Lynch syndrome and BRCA-related breast and/or ovarian cancer)
Colonic polyposis with uncertain histology
Adenomatous polyposis (specific to APC, MUTYH, POLE, and POLD1)
Family history does not meet criteria for established testing guidelines, but there is suspicion of hereditary cancer, and an appropriate panel is available
Family history is limited or unknown, but patient has concerns about hereditary cancer
As second-line testing when first-line testing is inconclusive
Emerging evidence has identified additional genes that may be associated with increased risk for CRC, and the panel has evaluated the
strength of the evidence based on published reports. For example, there is well-established evidence that the I1307K polymorphism in the APCgene, found in people of Ashkenazi Jewish decent, predisposes carriersto CRC.223-226 Data are emerging for other genes associated with increased risk for CRC, though the data may not be as robust. For instance, one GREM1 single nucleotide polymorphism (SNP) (rs16969681) has been shown to be associated with increased risk for CRC.227,228 Additionally, mutations in the POLE and POLD1 genes may be associated with increased risk for CRC.229-232 In an analysis of 266 unrelated probands with polyposis or who met the Amsterdam criteria, a POLE mutation was found in 1.5% of patients.233 In an analysis of 858 Spanish patients with early-onset and/or familial CRC and/or colonic polyposis, only one patient was found to have a POLE mutation.231
Mutations in the CHEK2 and MSH3 genes may also be associated with increased risk for CRC.234-239 For CHEK2, the 1100delC and I157T variants were found in meta-analytic reviews to be associated with both unselected and familial CRC.237,239 Mutations in the protein-coding gene GALNT12 is also believed to be associated with increased risk for CRC.240-242 Heterozygous mutations in the ATM gene,243 and heterozygous mutations in the DNA RECQL-helicase gene BLM244-246
may also increase risk for CRC. Mutations in the AXIN2 and NTHL1genes are associated with polyposis and oligodontia.247-254 There are emerging data that RPS20 mutations ,ay be associated with increased risk for CRC, but more data are required to strengthen this association.255
Although research has demonstrated a potential risk for CRC associated with these mutations, the value of including these genes for clinical testing (eg, as part of a multi-gene panel) remains uncertain. Nonetheless, the panel recognizes that many testing companies offer panels that include these genes, and that patients are being tested and may need guidance regarding subsequent screening and surveillance.

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-29
Accordingly, while the panel recommends caution in recommending multi-gene testing, guidance on management of results is discussed below.
Evidence to support screening and surveillance is limited, but the panel has conditionally developed a framework of recommendations for genes commonly included in multi-gene panels (GENE-7). Screening recommendations for carriers of GREM1, POLD1, POLE, AXIN2, NTHL1 and/or MSH3 mutations are as follows (GENE-7): begin colonoscopy at age 25 to 30 years, and receive follow-up colonoscopies every 2 to 3 years if negative. If polyps are found, screen with colonoscopy every 1 to 2 years with consideration of surgery if the polyp burden becomes unmanageable by colonoscopy. Surgical evaluation should be provided if appropriate. The panel recognizes that data to support the surveillance recommendations for GREM, POLD, POLE, AXIN2, NTHL1, and/orMSH3 mutations are currently evolving. Therefore, caution should be used when implementing final colonoscopy surveillance regimens in the context of patient preferences and new knowledge that may emerge.
As with the surveillance recommendations for GREM, POLD, POLE, AXIN2, NTHL1, and MSH3 mutations, data to support the surveillance recommendations for APC I1307K and CHEK2 mutations are also currently evolving. Therefore, the panel recommends caution when implementing final colonoscopy surveillance regimens in the context of patient preferences and new knowledge that may emerge. For carriers of APC I1307K and CHEK2 mutations with CRC, the panel recommendscolonoscopy surveillance based on the NCCN Guidelines for Colon Cancer and the NCCN Guidelines for Rectal Cancer. For carriers of APCI1307K and CHEK2 mutations unaffected by CRC with a first-degree relative with CRC, the panel recommends colonoscopy screening every 5 years beginning at age 40 or 10 years prior to the first-degree relative’s age at CRC diagnosis (GENE-7). For carriers unaffected by CRC without
a first-degree relative with CRC, the panel recommends colonoscopy screening every 5 years beginning at age 40 years (GENE-7).
Overall, as data regarding the clinical significance of genes associated with CRC risk emerge, the panel expects that these surveillance recommendations will evolve.

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-43
206. Boparai KS, Reitsma JB, Lemmens V, et al. Increased colorectalcancer risk in first-degree relatives of patients with hyperplastic polyposissyndrome. Gut 2010;59:1222-1225. Available at:http://www.ncbi.nlm.nih.gov/pubmed/20584785.
207. Win AK, Walters RJ, Buchanan DD, et al. Cancer risks for relatives ofpatients with serrated polyposis. Am J Gastroenterol 2012;107:770-778.Available at: http://www.ncbi.nlm.nih.gov/pubmed/22525305.
208. Oquinena S, Guerra A, Pueyo A, et al. Serrated polyposis:prospective study of first-degree relatives. Eur J Gastroenterol Hepatol2013;25:28-32. Available at:http://www.ncbi.nlm.nih.gov/pubmed/23011040.
209. Hall MJ, Forman AD, Pilarski R, et al. Gene panel testing for inheritedcancer risk. J Natl Compr Canc Netw 2014;12:1339-1346. Available at:http://www.ncbi.nlm.nih.gov/pubmed/25190699.
210. Gallego CJ, Shirts BH, Bennette CS, et al. Next-GenerationSequencing Panels for the Diagnosis of Colorectal Cancer and PolyposisSyndromes: A Cost-Effectiveness Analysis. J Clin Oncol 2015;33:2084-2091. Available at: http://www.ncbi.nlm.nih.gov/pubmed/25940718.
211. Walsh T, Casadei S, Coats KH, et al. Spectrum of mutations inBRCA1, BRCA2, CHEK2, and TP53 in families at high risk of breastcancer. JAMA 2006;295:1379-1388. Available at:http://www.ncbi.nlm.nih.gov/pubmed/16551709.
212. Walsh T, Lee MK, Casadei S, et al. Detection of inherited mutationsfor breast and ovarian cancer using genomic capture and massivelyparallel sequencing. Proc Natl Acad Sci U S A 2010;107:12629-12633.Available at: http://www.ncbi.nlm.nih.gov/pubmed/20616022.
213. Bombard Y, Bach PB, Offit K. Translating genomics in cancer care. JNatl Compr Canc Netw 2013;11:1343-1353. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24225968.
214. Rainville IR, Rana HQ. Next-generation sequencing for inheritedbreast cancer risk: counseling through the complexity. Curr Oncol Rep2014;16:371. Available at: http://www.ncbi.nlm.nih.gov/pubmed/24488544.
215. Cragun D, Radford C, Dolinsky JS, et al. Panel-based testing forinherited colorectal cancer: a descriptive study of clinical testing performedby a US laboratory. Clin Genet 2014;86:510-520. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24506336.
216. LaDuca H, Stuenkel AJ, Dolinsky JS, et al. Utilization of multigenepanels in hereditary cancer predisposition testing: analysis of more than2,000 patients. Genet Med 2014;16:830-837. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24763289.
217. Mauer CB, Pirzadeh-Miller SM, Robinson LD, Euhus DM. Theintegration of next-generation sequencing panels in the clinical cancergenetics practice: an institutional experience. Genet Med 2014;16:407-412. Available at: http://www.ncbi.nlm.nih.gov/pubmed/24113346.
218. Kapoor NS, Curcio LD, Blakemore CA, et al. Multigene panel testingdetects equal rates of pathogenic BRCA1/2 mutations and has a higherdiagnostic yield compared to limited BRCA1/2 analysis alone in patients atrisk for hereditary breast cancer. Ann Surg Oncol 2015;22:3282-3288.Available at: http://www.ncbi.nlm.nih.gov/pubmed/26219241.
219. Kurian AW, Hare EE, Mills MA, et al. Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J ClinOncol 2014;32:2001-2009. Available at:https://www.ncbi.nlm.nih.gov/pubmed/24733792.
220. Tung N, Battelli C, Allen B, et al. Frequency of mutations inindividuals with breast cancer referred for BRCA1 and BRCA2 testingusing next-generation sequencing with a 25-gene panel. Cancer2015;121:25-33. Available at:http://www.ncbi.nlm.nih.gov/pubmed/25186627.
221. Yurgelun MB, Allen B, Kaldate RR, et al. Identification of a Variety ofMutations in Cancer Predisposition Genes in Patients With Suspected

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-44
Lynch Syndrome. Gastroenterology 2015;149:604-613.e620. Available at: http://www.ncbi.nlm.nih.gov/pubmed/25980754.
222. Robson ME, Bradbury AR, Arun B, et al. American Society of ClinicalOncology Policy statement update: genetic and genomic testing for cancersusceptibility. J Clin Oncol 2015;33:3660-3667. Available at:https://www.ncbi.nlm.nih.gov/pubmed/26324357.
223. Boursi B, Sella T, Liberman E, et al. The APC p.I1307Kpolymorphism is a significant risk factor for CRC in average risk AshkenaziJews. Eur J Cancer 2013;49:3680-3685. Available at:http://www.ncbi.nlm.nih.gov/pubmed/23896379.
224. Gryfe R, Di Nicola N, Lal G, et al. Inherited colorectal polyposis andcancer risk of the APC I1307K polymorphism. Am J Hum Genet1999;64:378-384. Available at:http://www.ncbi.nlm.nih.gov/pubmed/9973276.
225. Locker GY, Kaul K, Weinberg DS, et al. The I1307K APCpolymorphism in Ashkenazi Jews with colorectal cancer: clinical andpathologic features. Cancer Genet Cytogenet 2006;169:33-38. Availableat: http://www.ncbi.nlm.nih.gov/pubmed/16875934.
226. Liang J, Lin C, Hu F, et al. APC polymorphisms and the risk ofcolorectal neoplasia: a HuGE review and meta-analysis. Am J Epidemiol2013;177:1169-1179. Available at:https://www.ncbi.nlm.nih.gov/pubmed/23576677.
227. Jaeger E, Leedham S, Lewis A, et al. Hereditary mixed polyposissyndrome is caused by a 40-kb upstream duplication that leads toincreased and ectopic expression of the BMP antagonist GREM1. NatGenet 2012;44:699-703. Available at:https://www.ncbi.nlm.nih.gov/pubmed/22561515.
228. Lewis A, Freeman-Mills L, de la Calle-Mustienes E, et al. Apolymorphic enhancer near GREM1 influences bowel cancer risk throughdifferential CDX2 and TCF7L2 binding. Cell Rep 2014;8:983-990.Available at: http://www.ncbi.nlm.nih.gov/pubmed/25131200.
229. Bellido F, Pineda M, Aiza G, et al. POLE and POLD1 mutations in529 kindred with familial colorectal cancer and/or polyposis: review ofreported cases and recommendations for genetic testing and surveillance.Genet Med 2016;18:325-332. Available at:https://www.ncbi.nlm.nih.gov/pubmed/26133394.
230. Palles C, Cazier JB, Howarth KM, et al. Germline mutations affectingthe proofreading domains of POLE and POLD1 predispose to colorectaladenomas and carcinomas. Nat Genet 2013;45:136-144. Available at:https://www.ncbi.nlm.nih.gov/pubmed/23263490.
231. Valle L, Hernandez-Illan E, Bellido F, et al. New insights into POLEand POLD1 germline mutations in familial colorectal cancer and polyposis.Hum Mol Genet 2014;23:3506-3512. Available at:https://www.ncbi.nlm.nih.gov/pubmed/24501277.
232. Elsayed FA, Kets CM, Ruano D, et al. Germline variants in POLE areassociated with early onset mismatch repair deficient colorectal cancer.Eur J Hum Genet 2015;23:1080-1084. Available at:https://www.ncbi.nlm.nih.gov/pubmed/25370038.
233. Spier I, Holzapfel S, Altmuller J, et al. Frequency and phenotypicspectrum of germline mutations in POLE and seven other polymerasegenes in 266 patients with colorectal adenomas and carcinomas. Int JCancer 2015;137:320-331. Available at:https://www.ncbi.nlm.nih.gov/pubmed/25529843.
234. Adam R, Spier I, Zhao B, et al. Exome Sequencing Identifies BiallelicMSH3 Germline Mutations as a Recessive Subtype of ColorectalAdenomatous Polyposis. Am J Hum Genet 2016;99:337-351. Available at:https://www.ncbi.nlm.nih.gov/pubmed/27476653.
235. Berndt SI, Platz EA, Fallin MD, et al. Mismatch repair polymorphismsand the risk of colorectal cancer. Int J Cancer 2007;120:1548-1554.Available at: https://www.ncbi.nlm.nih.gov/pubmed/17205513.
236. Gronwald J, Cybulski C, Piesiak W, et al. Cancer risks in first-degreerelatives of CHEK2 mutation carriers: effects of mutation type and cancer

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-45
site in proband. Br J Cancer 2009;100:1508-1512. Available at: https://www.ncbi.nlm.nih.gov/pubmed/19401704.
237. Liu C, Wang QS, Wang YJ. The CHEK2 I157T variant and colorectalcancer susceptibility: a systematic review and meta-analysis. Asian Pac JCancer Prev 2012;13:2051-2055. Available at:https://www.ncbi.nlm.nih.gov/pubmed/22901170.
238. Orimo H, Nakajima E, Yamamoto M, et al. Association betweensingle nucleotide polymorphisms in the hMSH3 gene and sporadic coloncancer with microsatellite instability. J Hum Genet 2000;45:228-230.Available at: http://dx.doi.org/10.1007/s100380070031.
239. Xiang HP, Geng XP, Ge WW, Li H. Meta-analysis of CHEK21100delC variant and colorectal cancer susceptibility. Eur J Cancer2011;47:2546-2551. Available at:https://www.ncbi.nlm.nih.gov/pubmed/21807500.
240. Guda K, Moinova H, He J, et al. Inactivating germ-line and somaticmutations in polypeptide N-acetylgalactosaminyltransferase 12 in humancolon cancers. Proc Natl Acad Sci U S A 2009;106:12921-12925.Available at: https://www.ncbi.nlm.nih.gov/pubmed/19617566.
241. Clarke E, Green RC, Green JS, et al. Inherited deleterious variants inGALNT12 are associated with CRC susceptibility. Hum Mutat2012;33:1056-1058. Available at:https://www.ncbi.nlm.nih.gov/pubmed/22461326.
242. Segui N, Pineda M, Navarro M, et al. GALNT12 is not a majorcontributor of familial colorectal cancer type X. Hum Mutat 2014;35:50-52.Available at: https://www.ncbi.nlm.nih.gov/pubmed/24115450.
243. Thompson D, Duedal S, Kirner J, et al. Cancer risks and mortality inheterozygous ATM mutation carriers. J Natl Cancer Inst 2005;97:813-822.Available at: https://www.ncbi.nlm.nih.gov/pubmed/15928302.
244. Baris HN, Kedar I, Halpern GJ, et al. Prevalence of breast andcolorectal cancer in Ashkenazi Jewish carriers of Fanconi anemia and
Bloom syndrome. Isr Med Assoc J 2007;9:847-850. Available at: https://www.ncbi.nlm.nih.gov/pubmed/18210922.
245. Cleary SP, Zhang W, Di Nicola N, et al. Heterozygosity for theBLM(Ash) mutation and cancer risk. Cancer Res 2003;63:1769-1771.Available at: https://www.ncbi.nlm.nih.gov/pubmed/12702560.
246. Laitman Y, Boker-Keinan L, Berkenstadt M, et al. The risk fordeveloping cancer in Israeli ATM, BLM, and FANCC heterozygousmutation carriers. Cancer Genet 2016;209:70-74. Available at:https://www.ncbi.nlm.nih.gov/pubmed/26778106.
247. Broderick P, Bagratuni T, Vijayakrishnan J, et al. Evaluation ofNTHL1, NEIL1, NEIL2, MPG, TDG, UNG and SMUG1 genes in familialcolorectal cancer predisposition. BMC Cancer 2006;6:243. Available at:https://www.ncbi.nlm.nih.gov/pubmed/17029639.
248. Lammi L, Arte S, Somer M, et al. Mutations in AXIN2 cause familialtooth agenesis and predispose to colorectal cancer. Am J Hum Genet2004;74:1043-1050. Available at:http://www.ncbi.nlm.nih.gov/pubmed/15042511.
249. Lejeune S, Guillemot F, Triboulet JP, et al. Low frequency of AXIN2mutations and high frequency of MUTYH mutations in patients withmultiple polyposis. Hum Mutat 2006;27:1064. Available at:https://www.ncbi.nlm.nih.gov/pubmed/16941501.
250. Marvin ML, Mazzoni SM, Herron CM, et al. AXIN2-associatedautosomal dominant ectodermal dysplasia and neoplastic syndrome. Am JMed Genet A 2011;155a:898-902. Available at:http://www.ncbi.nlm.nih.gov/pubmed/21416598.
251. Rivera B, Castellsague E, Bah I, et al. Biallelic NTHL1 Mutations in aWoman with Multiple Primary Tumors. N Engl J Med 2015;373:1985-1986.Available at: https://www.ncbi.nlm.nih.gov/pubmed/26559593.
252. Rivera B, Perea J, Sanchez E, et al. A novel AXIN2 germline variantassociated with attenuated FAP without signs of oligondontia or

Version 2.2019, 08/08/19 © 2019 National Comprehensive Cancer Network© (NCCN©), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines IndexTable of Contents
Discussion
NCCN Guidelines Version 2.2019Genetic/Familial High-Risk Assessment: Colorectal
MS-46
ectodermal dysplasia. Eur J Hum Genet 2014;22:423-426. Available at: https://www.ncbi.nlm.nih.gov/pubmed/23838596.
253. Weren RD, Ligtenberg MJ, Kets CM, et al. A germline homozygousmutation in the base-excision repair gene NTHL1 causes adenomatouspolyposis and colorectal cancer. Nat Genet 2015;47:668-671. Available at:http://www.ncbi.nlm.nih.gov/pubmed/25938944.
254. Wong S, Liu H, Bai B, et al. Novel missense mutations in the AXIN2gene associated with non-syndromic oligodontia. Arch Oral Biol2014;59:349-353. Available at:https://www.ncbi.nlm.nih.gov/pubmed/24581859.
255. Nieminen TT, O'Donohue MF, Wu Y, et al. Germline mutation ofRPS20, encoding a ribosomal protein, causes predisposition to hereditarynonpolyposis colorectal carcinoma without DNA mismatch repairdeficiency. Gastroenterology 2014;147:595-598.e595. Available at:http://www.ncbi.nlm.nih.gov/pubmed/24941021.

APPENDIX 3

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
1465NCCN
Guidelines® Insights
Genetic/Familial High-Risk Assessment: Colorectal
CE
© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
From 1UC San Diego Moores Cancer Center; 2Duke Cancer In-stitute; 3University of Michigan Comprehensive Cancer Center; 4The Ohio State University Comprehensive Cancer Center – James Cancer Hospital and Solove Research Institute; 5City of Hope Comprehensive Cancer Center; 6Fox Chase Cancer Center; 7Yale Cancer Center/Smilow Cancer Hospital; 8Massachusetts General Hospital Cancer Center; 9University of Colorado Can-cer Center; 10Hereditary Colon Cancer Foundation; 11Case Com-prehensive Cancer Center/University Hospitals Seidman Cancer Center and Cleveland Clinic Taussig Cancer Institute; 12Siteman Cancer Center at Barnes-Jewish Hospital and Washington Uni-versity School of Medicine; 13Stanford Cancer Institute; 14The Sidney Kimmel Comprehensive Cancer Center at Johns Hop-kins; 15Fred Hutchinson Cancer Research Center/Seattle Cancer Care Alliance; 16Robert H. Lurie Comprehensive Cancer Center of Northwestern University; 17The University of Texas MD An-derson Cancer Center; 18Moffitt Cancer Center; 19Mayo Clinic Cancer Center; 20Fred & Pamela Buffett Cancer Center; 21Me-morial Sloan Kettering Cancer Center; 22Dana-Farber/Brigham and Women’s Cancer Center; 23Vanderbilt-Ingram Cancer Cen-ter; 24Huntsman Cancer Institute at the University of Utah; 25University of Alabama at Birmingham Comprehensive Cancer Center; 26University of Wisconsin Carbone Cancer Center; and 27National Comprehensive Cancer Network.
*Provided content development and/or authorship assistance.
Please NoteThe NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) are a statement of consensus of the authors regarding their views of currently accepted ap-proaches to treatment. The NCCN Guidelines® Insights highlight important changes to the NCCN Guidelines® recommendations from previous versions. Colored markings in the algorithm show changes and the discus-sion aims to further the understanding of these changes by summarizing salient portions of the NCCN Guide-line Panel discussion, including the literature reviewed.
These NCCN Guidelines Insights do not represent the full NCCN Guidelines; further, the National Com-prehensive Cancer Network® (NCCN®) makes no repre-sentation or warranties of any kind regarding the content, use, or application of the NCCN Guidelines and NCCN Guidelines Insights and disclaims any responsibility for their applications or use in any way.
The full and most current version of these NCCN Guidelines are available at NCCN.org.
© National Comprehensive Cancer Network, Inc. 2017, All rights reserved. The NCCN Guidelines and the illustrations herein may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines® Insights Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017Featured Updates to the NCCN Guidelines
Samir Gupta, MD1*; Dawn Provenzale, MD, MS2*; Scott E. Regenbogen, MD3*; Heather Hampel, MS, CGC4*; Thomas P. Slavin Jr, MD5*; Michael J. Hall, MD, MS6*; Xavier Llor, MD, PhD7*; Daniel C. Chung, MD8*; Dennis J. Ahnen, MD9; Travis Bray, PhD10; Gregory Cooper, MD11; Dayna S. Early, MD12; James M. Ford, MD13; Francis M. Giardiello, MD, MBA14; William Grady, MD15; Amy L. Halverson, MD16; Stanley R. Hamilton, MD17; Jason B. Klapman, MD18; David W. Larson, MD, MBA19; Audrey J. Lazenby, MD20; Patrick M. Lynch, MD, JD17; Arnold J. Markowitz, MD21; Robert J. Mayer, MD22; Reid M. Ness, MD, MPH23; Niloy Jewel Samadder, MD24; Moshe Shike, MD21; Shajanpeter Sugandha, MD25; Jennifer M. Weiss, MD, MS26; Mary A. Dwyer, MS27,*; and Ndiya Ogba, PhD27,*
AbstractThe NCCN Guidelines for Genetic/Familial High-Risk Assessment: Colorectal provide recommendations for the management of patients with high-risk syndromes associated with an increased risk of colorectal cancer (CRC). The NCCN Panel for Genetic/Familial High-Risk Assessment: Colorectal meets at least annually to assess comments from reviewers within their institutions, examine relevant data, and reevaluate and update their recommendations. These NCCN Guidelines Insights focus on genes newly associated with CRC risk on multigene panels, the associated evidence, and currently recommended management strategies.
J Natl Compr Canc Netw 2017;15(12):1465–1475 doi: 10.6004/jnccn.2017.0176

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
1466
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
NCCN Guidelines InsightsCE
© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Disclosure of Relevant Financial RelationshipsEditor:Kerrin M. Green, MA, Assistant Managing Editor, JNCCN—Journal of the National Comprehensive Cancer Network, has disclosed that she has no rel-evant financial relationships.
JNCCN:Kimberly Callan, MS, Senior Director, Professional and Patient Publications, NCCN, has disclosed that she has no relevant financial relationships.Genevieve Emberger Hartzman, MA, Journal Production Specialist, NCCN, has disclosed that she has no relevant financial relationships.
CE Authors:Deborah J. Moonan, RN, BSN, Director, Continuing Education, NCCN, has disclosed that she has no relevant financial relationships. (Employed by NCCN until 2/17/17.)Karen Kanefield, Manager, Continuing Education Accreditation and Program Operations, NCCN, has disclosed that she has no relevant financial relationships.Kathy Smith, Manager, CE Grant Writing & Project Management, NCCN, has disclosed that she has no relevant financial relationships.Kristina M. Gregory, RN, MSN, OCN, Vice President, Clinical Information Operations, NCCN, has disclosed that she has no relevant financial relationships.Rashmi Kumar, PhD, Director, Clinical Information Operations, NCCN, has disclosed that she has no relevant financial relationships.
Individuals Who Provided Content Development and/or Authorship Assistance:Samir Gupta, MD, Panel Vice Chair, has disclosed that he has received grant/research support from Epigenomics AG.Dawn Provenzale, MD, MS, Panel Chair, has disclosed that she has no relevant financial relationships.Scott E. Regenbogen, MD, Panel Member, has disclosed that he has no relevant financial relationships.Heather Hampel, MS, CGC, Panel Member, has disclosed that she has received grant/research support from Myriad Genetic Laboratories, Inc.Thomas P. Slavin Jr, MD, Panel Member, has disclosed that he has no relevant financial relationships.Michael J. Hall, MD, MS, Panel Member, has disclosed that he has no relevant financial relationships.Xavier Llor, MD, PhD, Panel Member, has disclosed that he has no relevant financial relationships.Daniel C. Chung, MD, Panel Member, has disclosed that he has no relevant financial relationships.Mary Dwyer, MS, CGC, Senior Manager, Guidelines, NCCN, has disclosed that she has no relevant financial relationships.Ndiya Ogba, PhD, Oncology Scientist/Medical Writer, Guidelines Coordinator, NCCN, has disclosed that she has no relevant financial relationships.
NCCN: Continuing EducationTarget Audience: This activity is designed to meet the educa-tional needs of physicians, nurses, and pharmacists involved in the management of patients with cancer.
Accreditation StatementPhysicians: National Comprehensive Cancer Network is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
NCCN designates this journal-based CE activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their partici-pation in the activity.
Nurses: National Comprehensive Cancer Network is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center`s Commission on Accreditation.
NCCN designates this educational activity for a maximum of 1.0 contact hour.
Pharmacists: National Comprehensive Cancer Network is accredited by the Accreditation Council for Pharmacy Edu-cation as a provider of continuing pharmacy education.
NCCN designates this knowledge-based continuing education activity for 1.0 contact hour (0.1 CEUs) of continuing education credit. UAN: 0836-0000-17-012-H01-P
All clinicians completing this activity will be issued a certificate of participation. To participate in this journal CE activity: 1) re-view the educational content; 2) take the posttest with a 66% minimum passing score and complete the evaluation at http://education.nccn.org/node/81998; and 3) view/print certificate.
Release date: December 10, 2017; Expiration date: December 10, 2018
Learning Objectives: Upon completion of this activity, participants will be able to:
• Integrate into professional practice the updates to the NCCN Guidelines for Genetic/Familial High-Risk Assess-ment: Colorectal
• Describe the rationale behind the decision-making process for developing the NCCN Guidelines for Genetic/Familial High-Risk Assessment: Colorectal
This activity is supported by educational grants from Astellas, AstraZeneca, Celldex Therapeutics, Clovis Oncology, Genomic Health, Inc., Kyowa Hakko Kirin, Jazz Pharmaceuticals, Novartis Pharmaceuticals Corporation, and NOVOCURE. This activity is supported by an independent educational grant from Merck Co., Inc.

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1467NCCN Guidelines Insights
CE
NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate.
Category 2A: Based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate.
Category 2B: Based upon lower-level evidence, there is NCCN consensus that the intervention is appro-priate.
Category 3: Based upon any level of evidence, there is major NCCN disagreement that the intervention is appropriate.
All recommendations are category 2A unless otherwise noted.
Clinical trials: NCCN believes that the best management for any patient with cancer is in a clinical trial. Participa-tion in clinical trials is especially encouraged.
Version 3.2017 © National Comprehensive Cancer Network, Inc. 2017, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. GENE-4
TABLE 4: EVALUATION OF CRC GENES COMMONLY INCLUDED ON MULTI-GENE PANELScMULTI-GENE TESTING
cRPS20 is an emerging gene that is potentially linked to CRC, and there are not enough data at present to include RPS20 on this list. Continued on next page
GENE STRENGTH OFEVIDENCE
RISK LEVEL ASSOCIATION REFERENCE
APC Well-established High Familial adenomatous polyposis (FAP) & Attenuated FAP
See APC and MUTYH Genetic Testing Criteria (APC/MUTYH-1)
APC I1307K mutation
Well-established Moderate Increased frequency in Ashkenazi Jewish individuals; increased risk for colorectal cancer
Boursi B, et al. Eur J Cancer 2013;49:3680-3685.Liang J, et al. Am J Epidemiol 2013;177:1169-1179.
ATM Not well-established
Unclear – moderate at most
Increased risk for breast cancer and colorectal cancer
Thompson D, et al. J Natl Cancer Inst 2005;97:813-822.Olsen JH, et al. Br J Cancer 2005;93:260-265.
AXIN2 Not well-established
Uncertain – presumed high risk from limited case reports
Polyposis and oligodontia
Lammi L, et al. Am J Hum Genet 2004;74:1043-50.Marvin ML, et al. Am J Med Genet A 2011;155A:898-902.Rivera B, et al. Eur J Hum Genet 2014;22:423-6.Lejuene S, et al. Hum Mutat 2006;27:1064.Wong S, et al. Arch Oral Biol 2014;59:349-53.
BLM heterozygotes
Not well-established
Uncertain – none to low
Possible increased risk for colorectal cancer
Cleary et al. Cancer Res 2003;3:1769-71. Baris et al. Isr Med Assoc J 2007;9:847-50.Laitman Y, et al. Cancer Genet. 2016;209:70-4.
BMPR1A Well-established High Juvenile polyposis syndrome
See Juvenile Polyposis Syndrome Guidelines (JPS-1)
CHEK2 Not well-established
Moderate Increased risk for breast, colon, and other cancers
Xiang HP, et al. Eur J Cancer 2011;47:2546-2551.Liu C, et al. Asian Pac J Cancer Prev 2012;13:2051-2055.Gronwald J, et al. Br J Cancer 2009;100:1508-1512.
EPCAM Well-established High Lynch syndrome See Lynch Syndrome Guidelines (LS-1)
OverviewDue to increased lifetime risks of multiple cancers as-sociated with hereditary cancer syndromes, it is im-portant to identify genes that may affect risk assess-ment and potential management strategies.1 In addi-tion, early intervention has the potential to decrease cancer incidence and mortality in affected individu-als.2,3 The recent introduction of multigene testing for hereditary forms of cancer has rapidly altered the clinical approach to testing at-risk patients and their families. Based on next-generation sequencing, mul-tigene testing simultaneously analyzes a set of genes associated with a specific family cancer phenotype or multiple phenotypes, and may include syndrome-specific tests (ie, panels that test for only one syn-drome, such as Lynch syndrome), cancer-specific tests (ie, panels that test for >1 gene associated with a specific type of cancer, such as colorectal cancer [CRC]), and comprehensive cancer panels (ie, pan-els that test for >1 gene associated with multiple can-cers or cancer syndromes). The NCCN Guidelines

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1468NCCN Guidelines InsightsC
E
Version 3.2017 © National Comprehensive Cancer Network, Inc. 2017, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. GENE-5
TABLE 4: EVALUATION OF GENES COMMONLY INCLUDED ON MULTI-GENE PANELSc (CONTINUED)MULTI-GENE TESTING
Continued on next page
GENE STRENGTH OFEVIDENCE
RISK STATUS ASSOCIATION REFERENCE
GALNT12 Not well-established
Uncertain – moderate at most
Increased risk for colorectal cancer
Guda K, et al. Proc Natl Acad Sci U.S.A. 2009;106:12921-12925.Clarke E, et al. Hum Mutat 2012;33:1056-1058.Segui N, et al. Hum Mutat 2014;35:50-52.
GREM1 Not well-established
Uncertain – presumed high risk from limited case reports
Hereditary mixed polyposis syndrome due to a 40kb duplication upstream of GREM1 in Ashkenazi Jewish ancestry only
Jaeger E, et al. Nat Genet 2012; 44:699-703.
MLH1 Well-established High Lynch syndrome
See Lynch Syndrome Guidelines (LS-1)
MSH2 Well-established High Lynch syndromeMSH6 Well-established High Lynch syndrome
MSH3 Not well-established
Uncertain – presumed high risk from limited case reports
Polyposis Adam R, et al. Am J Hum Genet. 2016;99:337-51.
MUTYH biallelic mutations
Well-established High MUTYH-associated polyposis
See APC and MUTYH Genetic Testing Criteria (APC/MUTYH-1)
MUTYH heterozygotes
Not well-established
Uncertain – moderate at most
Possible increased risk for colorectal cancer
Win AK, et al. Gastroenterology 2014;146:1208-1211.
Panel for Genetic/Familial High-Risk Assessment: Colorectal added information regarding multigene testing during the 2016 update.
Multigene testing could include high-risk genes associated with a specific cancer or both high- and moderate-risk genes. Comprehensive cancer risk panels, which include a large number of genes associated with a variety of cancer types, are also available.4 The basis for using multigene testing for patient care should be no different from the rationale for testing a single gene known to be associated with the development of a specific type of cancer. Testing is ideally focused on identifying a mutation known to be clinically actionable. Specifically, a clinically actionable mutation alters patient management when present. Multigene testing may be most useful when more than one gene can explain a patient’s clinical and family history. In these cases, multigene testing may be more efficient and/or cost-effective.4 Multigene testing may also be considered for those who tested negative for a particular syndrome
but whose personal and family history is strongly suggestive of an inherited susceptibility.4,5
Multigene testing is associated with several chal-lenges. Most multigene panels include genes with limited data regarding degree of cancer risk among carriers and that support guidelines for risk manage-ment.4,6–9 In addition, the cancer risk of many of these genes is not clear when ascertained in individuals who do not have the typical phenotype historically associated with the cancer gene.4 Further, it is pos-sible that the risks associated with these genes may not be due entirely to that gene only, but may also be influenced by gene/gene or gene/environment in-teractions. Multigene tests also increase the likeli-hood of detecting variants of unknown/uncertain significance (VUS),4,5,8–12 with likelihood rates rang-ing from 17% to 38%.6,8,10,13 The considerable pos-sibility of detecting a VUS adds to the complexity of counseling following multigene testing. Address-ing these challenges will require large studies with adequate power to assess outcomes, yet such studies

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1469NCCN Guidelines Insights
CE
Version 3.2017 © National Comprehensive Cancer Network, Inc. 2017, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. GENE-6
TABLE 4: EVALUATION OF GENES COMMONLY INCLUDED ON MULTI-GENE PANELSc (CONTINUED)MULTI-GENE TESTING
cRPS20 is an emerging gene that is potentially linked to CRC, and there are not enough data at present to include RPS20 on this list.
Continued on next page
GENE STRENGTH OFEVIDENCE
RISK STATUS ASSOCIATION REFERENCE
NTHL1 Not well-established Uncertain – presumed high from limited case reports
Polyposis Weren RD, et al. Nat Genet 2015;47:668-671.Rivera B, et al. N Engl J Med 2015;373:1985–1986.Broderick P, et al. BMC Cancer 2006:6:243.
POLD1 Not well-established Uncertain – presumed high risk from limited case reports
Polymerase proofreading-associated polyposis
Palles C, et al. Nat Genet 2015; 45:136-144.Spier I, et al. Int J Cancer 2015;137:320-331.Bellido F, et al. Genet Med 2017;18:325-332.
POLE Not well-established Uncertain – presumed high risk from limited case reports
Polymerase proofreading-associated polyposis
Bellido F, et al. Genet Med 2017;18:325-332.
PMS2 Well-established High Lynch syndrome See Lynch Syndrome Guidelines (LS-1)PTEN Well-established Moderate-High Cowden syndrome/ PTEN
Hamartoma syndromeSee NCCN Guideline Genetic Familial High-Risk Assessment: Breast and Ovarian
SMAD4 Well-established High Juvenile polyposis syndrome See Juvenile Polyposis Syndrome Guidelines (JPS-1)
STK11 Well-established High Peutz-Jeghers syndrome See Peutz-Jegher syndrome Syndrome Guidelines (PJS-1)
TP53 Well-established High Li Fraumeni syndrome See NCCN Guideline Genetic Familial High-Risk Assessment: Breast and Ovarian
will be difficult to conduct given the low incidence of hereditary disease.
There are other issues to consider regarding multigene testing. First, commercially available tests may differ significantly on a number of factors, such as number of genes analyzed, turnaround time, and insurance coverage. Tests requiring a longer turn-around time may not be suitable for patients who need rapid results to inform surgical decision-mak-ing or other treatment choices. In addition, there is variation across commercial laboratory providers in the interpretation of genetic variants or mutations; therefore, the specific laboratory and multigene test should be chosen carefully.4 Second, in some cases, next-generation sequencing may miss some muta-tions that would have been detected with tradition-al single-gene analysis.4 Third, mutations identified for more than one gene add complexity that may lead to difficulty in making risk management rec-ommendations.5 A management plan should only be developed for identified gene mutations that are
clinically actionable; care should be taken to ensure that overtreatment or overscreening does not occur due to findings for which clinical management is uncertain, or findings that are incorrectly interpret-ed due to lack of evidence. This issue is particularly salient when the clinical management under con-sideration may include prophylactic surgery, such as colectomy.
Multigene testing is a new and rapidly growing field, but there is currently a lack of evidence regard-ing proper procedures and risk management strate-gies that should follow testing, especially when mu-tations are found for moderate-risk genes or when a VUS is found. For this reason, the NCCN panel rec-ommends multigene testing be offered in the context of professional genetic expertise, with pretest and posttest counseling. Panel recommendations are in agreement with those by ASCO, which issued an up-dated statement regarding genetic testing in 2015.14 Carriers of a genetic mutation should be encouraged to participate in clinical trials or genetic registries.

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1470NCCN Guidelines InsightsC
E
Version 3.2017 © National Comprehensive Cancer Network, Inc. 2017, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
TABLE 5: RECOMMENDED MANAGEMENT FOR GENES THAT MAY CONFER A RISK FOR COLORECTAL CANCERGENE RECOMMENDATIONAPC See NCCN Guidelines for Familial Adenomatous Polyposis (FAP-1)BMPR1A See NCCN Guidelines for Juvenile Polyposis Syndrome (JPS-1)LS syndrome genes (MLH1, MSH2, MSH6, PMS2, EPCAM)
See NCCN Guidelines for Lynch Syndrome (LS-2)
MUTYH biallelic mutations See NCCN Guidelines for MUTYH-Associated Polyposis (MAP-1)PTEN See NCCN Guidelines for Genetic/Familial High-Risk Assessment: Breast and OvarianSTK11 See NCCN Guidelines for Peutz-Jeghers Syndrome (PJS-1)SMAD4 See NCCN Guidelines for Juvenile Polyposis Syndrome (JPS-1)TP53 See NCCN Guidelines for Genetic/Familial High-Risk Assessment: Breast and OvarianGREM1d
• Begin colonoscopy at age 25–30 and every 2–3 y if negative. If polyps are found, colonoscopy every 1–2 y with consideration of surgery if the polyp burden becomes unmanageable by colonoscopy.
• Surgical evaluation if appropriate.
POLD1d
POLEd
AXIN2NTHL1MSH3
APC I1307K mutationd
CHEK2d
• For probands with colorectal cancer and one of these mutations: �See surveillance recommendations for post-colorectal cancer resection
◊ NCCN Guidelines for Colon Cancer ◊ NCCN Guidelines for Rectal Cancer
• For probands unaffected by colorectal cancer with a first-degree relative with colorectal cancer:�Colonoscopy screening every 5 years, beginning at age 40 or 10 years prior to age of first-degree relative’s age at CRC
diagnosis.• For probands unaffected by colorectal cancer and no first-degree relative with colorectal cancer:�Colonoscopy screening every 5 years, beginning at age 40.
MUTYH heterozygotesd
• For probands unaffected by colorectal cancer with a first-degree relative with colorectal cancer:�Colonoscopy screening every 5 years, beginning at age 40 y or 10 years prior to age of first-degree relative’s age at CRC
diagnosis.• For probands unaffected by colorectal cancer with NO family history of colorectal cancer:�Data are uncertain if specialized screening is warranted.
GENE-7
dThe panel recognizes that data to support the surveillance recommendations for these particular genes are evolving at this time. Caution should be used when implementing fi nal colonoscopy surveillance regimens in context of patient preferences and new knowledge that may emerge.
MULTI-GENE TESTING
Multigene testing is not recommended when:
• There is an individual from a family with a known mutation and there is no other reason for multigene testing;
• The patient’s family history is strongly sugges-tive of a specific known hereditary syndrome for which single-gene analysis may provide defini-tive diagnosis; or,
• The patient is diagnosed with CRC with mic-rosatellite instability (MSI) or loss of ≥1 DNA mismatch repair (MMR) proteins.
In these 3 scenarios, syndrome-specific panels may be considered.
Multigene testing may be considered in the following scenarios:
• A patient with a personal or family history that meets criteria for >1 hereditary cancer syndrome (eg, Lynch syndrome and BRCA-related breast and/or ovarian cancer)
• Colonic polyposis with uncertain histology• Adenomatous or mixed polyposis (specific to
APC, MUTYH, POLE, and POLD1)• Family history does not meet criteria for estab-
lished testing guidelines but there is suspicion of hereditary cancer, and an appropriate panel is available
• Family history is limited or unknown but patient has concerns about hereditary cancer
• As second-line testing when first-line testing (eg, syndrome-specific or single-gene) is inconclusive
However, additional indications for multigene testing may exist based on clinical judgment.
Risk for CRC and management of genes with well-established risk for CRC, including Lynch syn-drome, familial adenomatous polyposis (FAP), and MUTYH-associated polyposis (MAP), have been reviewed in detail in prior NCCN Guidelines, and have been updated annually (to view the most re-cent and complete version of these guidelines, visit

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1471NCCN Guidelines Insights
CE
NCCN.org). In the case of many genes newly associ-ated with CRC, the evidence is still emerging. To es-tablish the clinical utility of these genes, it is impor-tant to review the strength of the evidence.15 Previ-ously, the panel conditionally developed a framework of recommendations for genes commonly included in multigene panels (see GENE-7; page 1470). Dur-ing the 2017 guidelines update meeting, the panel evaluated the strength of the evidence based on pub-lished reports supporting these genes. These NCCN Guidelines Insights summarize data focused on genes newly associated with CRC risk and current recom-mended management strategies, although the panel notes that the link between mutations/alterations in some of these genes and increased CRC risk is in-completely defined due to limited evidence. These include mutations/alterations in the following genes: APC (I1307K polymorphism), AXIN2, CHEK2, GREM1, MSH3, MUTYH (monoallelic), NTHL1, POLD1, and POLE.
Genes Newly Associated With CRC Frequently Seen on Multigene Panels: Evidence and Management ApproachesAPC I1307K MutationThe adenomatous polyposis coli (APC) gene is a tu-mor-suppressor gene associated with CRC.16 There is well-established evidence that the I1307K polymor-phism in the APC gene, which occurs in approxi-mately 6% to 8% of individuals of Ashkenazi Jewish decent, predisposes carriers to CRC.17–21 In an analy-sis of 3,305 individuals from Israel who underwent colonoscopic examinations, 8% were identified as carriers of the I1307K polymorphism, and the over-all adjusted odds ratio (OR) for colorectal neoplasia among carriers was 1.51 (95% CI, 1.16–1.98).17 A subgroup analysis found that the prevalence of the I1307K polymorphism in individuals of Ashkenazi Jewish descent was 10.1% and the adjusted OR was 1.75 (95% CI, 1.26–2.45).17 A meta-analysis includ-ing 40 studies showed that compared with carriers of wild-type I1307K, individuals of Ashkenazi Jewish descent who carried the I1307K polymorphism had a significantly increased risk of colorectal neoplasia, with a pooled OR of 2.17 (95% CI, 1.64–2.86).20 Some studies have identified the I1307K polymor-phism in the APC gene in individuals of non–Ash-kenazi Jewish and Arabic descent, although the
prevalence is higher in individuals of Ashkenazi Jew-ish descent.22–24 An analysis of 900 cases from a pop-ulation-based case-control study in northern Israel found the I1307K polymorphism in the APC gene in 78 CRC cases, with a prevalence of 11.2%, 2.7%, and 3.1% among individuals of Ashkenazi Jewish, non-Ashkenazi Jewish, and Arabic descent, respec-tively.23 Overall, however, evidence is insufficient to determine whether risk for CRC associated with the APC I1307K polymorphism differs among individu-als with Ashkenazi descent versus without, and the panel recognizes that some individuals may not be aware of their Ashkenazi heritage.
For carriers of the APC I1307K mutation with CRC, the panel recommends colonoscopy surveil-lance based on NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) for Colon Cancer and for Rectal Cancer (to view the most recent ver-sion of these guidelines, visit NCCN.org). For carri-ers of the APC I1307K mutation unaffected by CRC with a first-degree relative with CRC, the panel rec-ommends colonoscopy surveillance every 5 years be-ginning at age 40 years or at 10 years younger than the first-degree relative’s age at CRC diagnosis (see GENE-7; page 1470). For carriers unaffected by CRC without a first-degree relative with CRC, the panel recommends colonoscopy screening every 5 years be-ginning at age 40 years (see GENE-7; page 1470).
AXIN2 MutationsMutations in the Axin-related protein (AXIN2) gene are associated with polyposis and oligodontia.25–29 In a study of a 4-generation family from Finland, 11 family members had oligodontia, 8 of whom had either CRC or precancerous lesions, attributed to a nonsense mu-tation in the AXIN2 gene.25 Other studies also sup-port the association of AXIN2 mutations and oligo-dontia.27,29 A report described a family with a history of oligodontia and other findings, including colonic polyposis, gastric polyps, a mild ectodermal dysplasia phenotype, and early-onset CRC and breast cancer, in which an inherited AXIN2 mutation (c.1989G>A) segregated in an autosomal dominant pattern.27 An-other study of 23 families with FAP resulted in the identification of a novel AXIN2 variant (c.1387C>T) in one family with attenuated FAP (AFAP).28 Car-riers of the variant had a variable number of polyps but no oligodontia or ectodermal dysplasia.28 During the 2017 update, AXIN2 was added to a list of genes

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1472NCCN Guidelines InsightsC
E
commonly included on multigene panels (see GENE-4; page 1467). For carriers of AXIN2 mutations, the panel recommends initiation of colonoscopic surveil-lance at age 25 to 30 years, and if no polyps are locat-ed, a repeat colonoscopy every 2 to 3 years. If polyps are found, colonoscopic surveillance every 1 to 2 years is recommended, with consideration of surgical inter-ventions if the polyp burden becomes unmanageable by colonoscopy (see GENE-7; page 1470).
CHEK2 MutationsGermline mutations in the cell cycle checkpoint ki-nase 2 (CHEK2) gene are associated with increased risk of breast cancer and CRC.30–32 In a population-based study of 5,953 patients with breast, prostate, or colon cancers (1,934 patients with colon cancer), 533 were CHEK2-positive and 431 were affected relatives.30 After adjusting for mutation type, the risk of colon cancer was higher among relatives of probands with colon cancer than among relatives of patients with prostate or breast cancer (hazard ratio [HR], 4.2; 95% CI, 2.4–7.8; P=.0001).30 Significant associations between CHEK2 mutations and CRC risk have been identified in meta-analyses.31,32 One meta-analysis of 7 studies that included 4,029 cases and 13,844 controls based on search criteria found a significant association between the CHEK2 I157T variant and CRC risk.31 For carriers of CHEK2 mu-tations, the NCCN Panel recommends similar man-agement strategies as described for carriers of the APC I1307K mutation.
GREM1 AlterationsHereditary mixed polyposis syndrome (HMPS) is a rare autosomal dominant condition that occurs pri-marily in individuals of Ashkenazi Jewish descent and is characterized by multiple types of colorectal polyps, extracolonic tumors, onset of polyps in ado-lescence, and progression of some polyps to advanced adenomas.33,34 HMPS is due to a 40-kb duplication upstream of the gremlin 1 gene (GREM1), which increases ectopic GREM1 expression in normal epi-thelium.33 Exome sequencing combined with linkage analyses and detection of copy-number variations identified a 16-kb duplication upstream of GREM1 in a family of non–Ashkenazi Jewish descent with AFAP.35 For carriers of GREM1 alterations, the pan-el recommends similar management strategies as de-
scribed for carriers of AXIN2 mutations (see GENE-7; page 1470).
MSH3 MutationsMutS homolog 3 (MSH3) is a DNA MMR gene implicated in tumorigenesis of colon cancer with MSI.36 Recent data have suggested that biallelic MSH3 germline mutations are a recessive subtype of colorectal adenomatous polyposis.37 During the 2017 NCCN Guidelines update, MSH3 was added to a list of genes commonly included on multigene panels (see GENE-5; page 1468). However, given available data, the panel agreed that the strength of evidence linking MSH3 to increased CRC risk is not currently well established. For carriers of 2 MSH3 mutations, the panel recommends similar management strate-gies as described for carriers of AXIN2 mutations (see GENE-7; page 1470).
MUTYH (Monoallelic) MutationsMUTYH is a base excision repair gene involved in repairing oxidative DNA damage. Individuals with a germline mutation in one allele of the MUTYH gene are thought to have a modest or slightly increased risk of CRC.38–40 A recent study suggests that the risks may be higher than previously estimated.41 This study analyzed 2,332 individuals with monoallelic MUTYH mutations among 9,504 relatives of 264 CRC cases with a MUTYH mutation. The estimated CRC risks, up to 70 years of age, were 7.2% for male carriers of monoallelic MUTYH mutations (95% CI, 4.6%–11.3%) and 5.6% for female carriers (95% CI, 3.6%–8.8%), irrespective of family history.41 The risks for CRC were higher for carriers of monoal-lelic MUTYH mutations with a first-degree relative with CRC.41 Another study evaluated the frequency of monoallelic MUTYH mutations and colorectal adenomas, and found that 13 of 72 individuals with CRC were monoallelic MUTYH mutation carriers, and 11 of the 13 had a family history of cancer in first- or second-degree relatives.42
During the 2017 update, the NCCN Panel re-vised management recommendations for monoal-lelic MUTYH mutation carriers based on the data and expert consensus (see GENE-7; page 1470). For probands unaffected by CRC with a first-degree rela-tive with CRC, the panel recommends colonoscopy surveillance every 5 years, beginning at age 40 years or at 10 years younger than the age of the first-degree

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1473NCCN Guidelines Insights
CE
relative’s age at CRC diagnosis. For probands unaf-fected by CRC without a first-degree relative with CRC, the panel notes that the data are not well established and it is uncertain whether specialized screening is warranted.
NTHL1 MutationsThe endonuclease III–like 1 (NTHL1) gene is in-volved in base excision repair and acts on oxidized pyrimidine residues.43 A recent study suggests a role for NTHL1 mutations in colorectal polyposis.44 Whole-exome sequencing on 51 individuals from 48 families diagnosed with polyposis identified a homo-zygous germline nonsense mutation in NTHL1 in 7 affected individuals from 3 unrelated families.44 Dur-ing the 2017 update, NTHL1 was added to a list of genes commonly included on multigene panels (see GENE-6; page 1469). For carriers of 2 NTHL1 mu-tations, the panel recommends similar management strategies as described for carriers of AXIN2 muta-tions (see GENE-7; page 1470).
POLD1 and POLE MutationsDNA polymerases delta [δ]1 (POLD1) and epsilon [ε] (POLE) are involved in DNA proofreading and replication.45 Mutations in the POLD1 and POLE genes may be associated with polyposis and an in-creased risk for CRC.46–49 Using whole-genome se-quencing in combination with linkage and associa-tion analysis, heterozygous POLD1 and POLE germ-line variants were identified in multiple adenoma and/or CRC cases.47 In an analysis of 858 Spanish patients with early-onset and/or familial CRC and/or colonic polyposis, only 1 patient was found to have a POLE mutation.48 In an analysis of 266 unrelated probands with polyposis or who met the Amster-dam criteria, a POLE mutation was found in 1.5% of patients.50 Novel variants for both POLD1 and POLE have been identified in individuals with CRC,
broadening the phenotypic spectrum of POLD1- and POLE-associated polyposis.46,51 Presently, for carriers of POLD1 and POLE mutations, the panel recom-mends similar management strategies as described for carriers of AXIN2 mutations (see GENE-7; page 1470).
Summary and ConclusionsDuring the panel meeting for the 2017 update, panel members discussed a number of important updates to the NCCN Guidelines for Genetic/Familial High-Risk Assessment: Colorectal, including the strength of evidence linking mutations in genes newly associ-ated with CRC risk and management recommenda-tions for these genes. These include mutations/al-terations in APC (I1307K polymorphism), AXIN2, CHEK2, GREM1 (upstream duplications), MSH3, MUTYH (monoallelic), NTHL1, POLD1, and POLE. Although research has demonstrated a poten-tial risk for CRC associated with mutations in these genes, the value of including these genes for clini-cal testing (eg, as part of a multigene panel) remains uncertain. The panel urges caution in implement-ing routine clinical testing for genes for which the cancer risk and management strategies are currently uncertain, and some panel members have concerns about the observed practice of genetic testing com-panies regularly expanding the list of tested genes despite availability of only weak evidence to support cancer risk. Nonetheless, the panel recognizes that many testing companies offer panels that include these genes, and that patients are being tested and may need guidance regarding subsequent screening and surveillance. As additional data regarding the clinical significance of genes associated with CRC risk emerge, the NCCN Panel expects that these sur-veillance recommendations will continue to evolve.
References1. Yurgelun MB. Next-generation strategies for hereditary colorectal cancer
risk assessment. J Clin Oncol 2015;33:388–393.
2. Jarvinen HJ, Aarnio M, Mustonen H, et al. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology 2000;118:829–834.
3. Jarvinen HJ, Renkonen-Sinisalo L, Aktan-Collan K, et al. Ten years after mutation testing for Lynch syndrome: cancer incidence and outcome in mutation-positive and mutation-negative family members. J Clin Oncol 2009;27:4793–4797.
4. Hall MJ, Forman AD, Pilarski R, et al. Gene panel testing for inherited cancer risk. J Natl Compr Canc Netw 2014;12:1339–1346.
5. Walsh T, Lee MK, Casadei S, et al. Detection of inherited mutations for breast and ovarian cancer using genomic capture and massively parallel sequencing. Proc Natl Acad Sci U S A 2010;107:12629–12633.
6. Cragun D, Radford C, Dolinsky JS, et al. Panel-based testing for inherited colorectal cancer: a descriptive study of clinical testing performed by a US laboratory. Clin Genet 2014;86:510–520.
7. LaDuca H, Stuenkel AJ, Dolinsky JS, et al. Utilization of multigene panels in hereditary cancer predisposition testing: analysis of more than 2,000 patients. Genet Med 2014;16:830–837.

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1474NCCN Guidelines InsightsC
E
8. Mauer CB, Pirzadeh-Miller SM, Robinson LD, Euhus DM. The integration of next-generation sequencing panels in the clinical cancer genetics practice: an institutional experience. Genet Med 2014;16:407–412.
9. Rainville IR, Rana HQ. Next-generation sequencing for inherited breast cancer risk: counseling through the complexity. Curr Oncol Rep 2014;16:371.
10. Kapoor NS, Curcio LD, Blakemore CA, et al. Multigene panel testing detects equal rates of pathogenic BRCA1/2 mutations and has a higher diagnostic yield compared to limited BRCA1/2 analysis alone in patients at risk for hereditary breast cancer. Ann Surg Oncol 2015;22:3282–3288.
11. Kurian AW, Hare EE, Mills MA, et al. Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J Clin Oncol 2014;32:2001–2009.
12. Tung N, Battelli C, Allen B, et al. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer 2015;121:25–33.
13. Yurgelun MB, Allen B, Kaldate RR, et al. Identification of a variety of mutations in cancer predisposition genes in patients with suspected Lynch syndrome. Gastroenterology 2015;149:604–613.e620.
14. Robson ME, Bradbury AR, Arun B, et al. American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol 2015;33:3660–3667.
15. Easton DF, Pharoah PD, Antoniou AC, et al. Gene-panel sequencing and the prediction of breast-cancer risk. N Engl J Med 2015;372:2243–2257.
16. Markowitz SD, Bertagnolli MM. Molecular origins of cancer: molecular basis of colorectal cancer. N Engl J Med 2009;361:2449–2460.
17. Boursi B, Sella T, Liberman E, et al. The APC p.I1307K polymorphism is a significant risk factor for CRC in average risk Ashkenazi Jews. Eur J Cancer 2013;49:3680–3685.
18. Gryfe R, Di Nicola N, Lal G, et al. Inherited colorectal polyposis and cancer risk of the APC I1307K polymorphism. Am J Hum Genet 1999;64:378–384.
19. Laken SJ, Petersen GM, Gruber SB, et al. Familial colorectal cancer in Ashkenazim due to a hypermutable tract in APC. Nat Genet 1997;17:79–83.
20. Liang J, Lin C, Hu F, et al. APC polymorphisms and the risk of colorectal neoplasia: a HuGE review and meta-analysis. Am J Epidemiol 2013;177:1169–1179.
21. Locker GY, Kaul K, Weinberg DS, et al. The I1307K APC polymorphism in Ashkenazi Jews with colorectal cancer: clinical and pathologic features. Cancer Genet Cytogenet 2006;169:33–38.
22. Patael Y, Figer A, Gershoni-Baruch R, et al. Common origin of the I1307K APC polymorphism in Ashkenazi and non-Ashkenazi Jews. Eur J Hum Genet 1999;7:555–559.
23. Rennert G, Almog R, Tomsho LP, et al. Colorectal polyps in carriers of the APC I1307K polymorphism. Dis Colon Rectum 2005;48:2317–2321.
24. Shtoyerman-Chen R, Friedman E, Figer A, et al. The I1307K APC polymorphism: prevalence in non-Ashkenazi Jews and evidence for a founder effect. Genet Test 2001;5:141–146.
25. Lammi L, Arte S, Somer M, et al. Mutations in AXIN2 cause familial tooth agenesis and predispose to colorectal cancer. Am J Hum Genet 2004;74:1043–1050.
26. Lejeune S, Guillemot F, Triboulet JP, et al. Low frequency of AXIN2 mutations and high frequency of MUTYH mutations in patients with multiple polyposis. Hum Mutat 2006;27:1064.
27. Marvin ML, Mazzoni SM, Herron CM, et al. AXIN2-associated autosomal dominant ectodermal dysplasia and neoplastic syndrome. Am J Med Genet A 2011;155A:898–902.
28. Rivera B, Perea J, Sanchez E, et al. A novel AXIN2 germline variant associated with attenuated FAP without signs of oligondontia or ectodermal dysplasia. Eur J Hum Genet 2014;22:423–426.
29. Wong S, Liu H, Bai B, et al. Novel missense mutations in the AXIN2 gene associated with non-syndromic oligodontia. Arch Oral Biol 2014;59:349–353.
30. Gronwald J, Cybulski C, Piesiak W, et al. Cancer risks in first-degree relatives of CHEK2 mutation carriers: effects of mutation type and cancer site in proband. Br J Cancer 2009;100:1508–1512.
31. Liu C, Wang QS, Wang YJ. The CHEK2 I157T variant and colorectal cancer susceptibility: a systematic review and meta-analysis. Asian Pac J Cancer Prev 2012;13:2051–2055.
32. Xiang HP, Geng XP, Ge WW, Li H. Meta-analysis of CHEK2 1100delC variant and colorectal cancer susceptibility. Eur J Cancer 2011;47:2546–2551.
33. Jaeger E, Leedham S, Lewis A, et al. Hereditary mixed polyposis syndrome is caused by a 40-kb upstream duplication that leads to increased and ectopic expression of the BMP antagonist GREM1. Nat Genet 2012;44:699–703.
34. Lieberman S, Walsh T, Schechter M, et al. Features of patients with hereditary mixed polyposis syndrome caused by duplication of GREM1 and implications for screening and surveillance. Gastroenterology 2017;152:1876–1880.e1.
35. Rohlin A, Eiengard F, Lundstam U, et al. GREM1 and POLE variants in hereditary colorectal cancer syndromes. Genes Chromosomes Cancer 2016;55:95–106.
36. Ikeda M, Orimo H, Moriyama H, et al. Close correlation between mutations of E2F4 and hMSH3 genes in colorectal cancers with microsatellite instability. Cancer Res 1998;58:594–598.
37. Adam R, Spier I, Zhao B, et al. Exome sequencing identifies biallelic MSH3 germline mutations as a recessive subtype of colorectal adenomatous polyposis. Am J Hum Genet 2016;99:337–351.
38. Theodoratou E, Campbell H, Tenesa A, et al. A large-scale meta-analysis to refine colorectal cancer risk estimates associated with MUTYH variants. Br J Cancer 2010;103:1875–1884.
39. Win AK, Cleary SP, Dowty JG, et al. Cancer risks for monoallelic MUTYH mutation carriers with a family history of colorectal cancer. Int J Cancer 2011;129:2256–2262.
40. Win AK, Hopper JL, Jenkins MA. Association between monoallelic MUTYH mutation and colorectal cancer risk: a meta-regression analysis. Fam Cancer 2011;10:1–9.
41. Win AK, Dowty JG, Cleary SP, et al. Risk of colorectal cancer for carriers of mutations in MUTYH, with and without a family history of cancer. Gastroenterology 2014;146:1208–1211.e1–5.
42. Rosner G, Bercovich D, Daniel YE, et al. Increased risk for colorectal adenomas and cancer in mono-allelic MUTYH mutation carriers: results from a cohort of North-African Jews. Fam Cancer 2015;14:427–436.
43. Krokan HE, Bjoras M. Base excision repair. Cold Spring Harb Perspect Biol 2013;5:a012583.
44. Weren RD, Ligtenberg MJ, Kets CM, et al. A germline homozygous mutation in the base-excision repair gene NTHL1 causes adenomatous polyposis and colorectal cancer. Nat Genet 2015;47:668–671.
45. Garg P, Burgers PM. DNA polymerases that propagate the eukaryotic DNA replication fork. Crit Rev Biochem Mol Biol 2005;40:115–128.
46. Bellido F, Pineda M, Aiza G, et al. POLE and POLD1 mutations in 529 kindred with familial colorectal cancer and/or polyposis: review of reported cases and recommendations for genetic testing and surveillance. Genet Med 2016;18:325–332.
47. Palles C, Cazier JB, Howarth KM, et al. Germline mutations affecting the proofreading domains of POLE and POLD1 predispose to colorectal adenomas and carcinomas. Nat Genet 2013;45:136–144.
48. Valle L, Hernandez-Illan E, Bellido F, et al. New insights into POLE and POLD1 germline mutations in familial colorectal cancer and polyposis. Hum Mol Genet 2014;23:3506–3512.
49. Elsayed FA, Kets CM, Ruano D, et al. Germline variants in POLE are associated with early onset mismatch repair deficient colorectal cancer. Eur J Hum Genet 2015;23:1080–1084.
50. Spier I, Holzapfel S, Altmuller J, et al. Frequency and phenotypic spectrum of germline mutations in POLE and seven other polymerase genes in 266 patients with colorectal adenomas and carcinomas. Int J Cancer 2015;137:320–331.
51. Esteban-Jurado C, Gimenez-Zaragoza D, Munoz J, et al. POLE and POLD1 screening in 155 patients with multiple polyps and early-onset colorectal cancer. Oncotarget 2017;8:26732–26743.

© JNCCN—Journal of the National Comprehensive Cancer Network | Volume 15 Number 12 | December 2017
Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017
1475NCCN Guidelines Insights
CE
High-Risk Assessment: Colorectal, when should an individual with monoallelic MUTYH mutations unaffected by CRC and with a first-degree relative with CRC consider colonoscopy surveillance?
a. 50 years of age or at 10 years younger than the age of first-degree relative’s age at CRC diagnosis
b. 40 years of age or at 10 years younger than the age of first-degree relative’s age at CRC diagnosis
c. 40 years of age or at 5 years younger than the age of first-degree relative’s age at CRC diagnosis
d. 50 years of age or at 5 years younger than the age of first-degree relative’s age at CRC diagnosis
e. Data are unclear whether specialized screening is needed
choice questions. Credit cannot be obtained for tests complet-ed on paper. You must be a registered user on NCCN.org. If you are not registered on NCCN.org, click on “New Member? Sign up here” link on the left hand side of the Web site to register. Only one answer is correct for each question. Once you suc-cessfully answer all posttest questions you will be able to view and/or print your certificate. Software requirements: Internet
Instructions for CompletionTo participate in this journal CE activity: 1) review the learning objectives and author disclosures; 2) study the education con-tent; 3) take the posttest with a 66% minimum passing score and complete the evaluation at http://education.nccn.org/node/81998; and 4) view/print certificate. After reading the article, you should be able to answer the following multiple-
Posttest Questions
1. According to the 2017 NCCN Guidelines for Genetic/Familial High-Risk Assessment: Colorectal, the following genes newly associated with CRC frequently seen on multigene panels may be associated with an increased risk of CRC:
a. MSH3b. MSH2c. CHEK2d. a and be. a, b, and cf. a and c
2. True or False: An individual from a family with a known mutation and no other reason for multigene testing is an appropriate rationale for considering multigene testing.
3. According to the 2017 NCCN Guidelines for Genetic/Familial



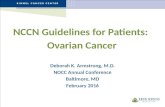


![[Ghiduri][Cancer]NCCN Pain Guidelines - Update](https://static.fdocuments.us/doc/165x107/55cf9686550346d0338c0f31/ghiduricancernccn-pain-guidelines-update.jpg)










