NCCN Breast Cancer Treatment Guidelines Version VIII
92
Breast Cancer Treatment Guidelines for Patients Version VIII/ September 2006
Transcript of NCCN Breast Cancer Treatment Guidelines Version VIII

Breast CancerTreatment Guidelines for Patients
Version VIII/ September 2006

Current ACS/NCCN Treatment Guidelines for Patients
Advanced Cancer and Palliative Care Treatment Guidelines for Patients(English and Spanish)
Bladder Cancer Treatment Guidelines for Patients (English and Spanish)
Breast Cancer Treatment Guidelines for Patients (English and Spanish)
Cancer Pain Treatment Guidelines for Patients (English and Spanish)
Cancer-Related Fatigue and Anemia Treatment Guidelines for Patients(English and Spanish)
Colon and Rectal Cancer Treatment Guidelines for Patients (English and Spanish)
Distress Treatment Guidelines for Patients (English and Spanish)
Fever and Neutropenia Treatment Guidelines for Patients With Cancer(English and Spanish)
Lung Cancer Treatment Guidelines for Patients (English and Spanish)
Melanoma Cancer Treatment Guidelines for Patients (English and Spanish)
Nausea and Vomiting Treatment Guidelines for Patients With Cancer(English and Spanish)
Non-Hodgkin’s Lymphoma Treatment Guidelines for Patients (English and Spanish)
Ovarian Cancer Treatment Guidelines for Patients (English and Spanish)
Prostate Cancer Treatment Guidelines for Patients (English and Spanish)

The mutual goal of the National Comprehensive Cancer Network (NCCN) andthe American Cancer Society (ACS) partnership is to provide patients with state-of-the-art cancer treatment information in an easy to understand language. Thisinformation, based on the NCCN’s Clinical Practice Guidelines, is intended toassist you in a discussion with your doctor. These guidelines do not replace theexpertise and clinical judgment of your doctor.
Breast CancerTreatment Guidelines for Patients
Version VIII/ September 2006

NCCN Clinical Practice Guidelines were developed by a diverse panel of experts.The guidelines are a statement of consensus of its authors regarding the scientificevidence and their views of currently accepted approaches to treatment. The NCCNguidelines are updated as new significant data become available. The PatientInformation version is updated accordingly and available on-line through theAmerican Cancer Society and NCCN Web sites. To ensure you have the mostrecent version, you may contact the American Cancer Society at 1-800-ACS-2345or the NCCN at 1-888-909-NCCN.
©2006 by the American Cancer Society (ACS) and the National ComprehensiveCancer Network. All rights reserved. The information herein may not be reprintedin any form for commercial purposes without the expressed written permissionof the ACS. Single copies of each page may be reproduced for personal and non-commercial uses by the reader.

Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Making Decisions About Breast Cancer Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Inside Breast Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Types of Breast Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Breast Cancer Work Up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Breast Cancer Stages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Breast Cancer Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Treatment of Breast Cancer During Pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Treatment of Pain and Other Symptoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Complementary and Alternative Therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Other Things to Consider During and After Treatment . . . . . . . . . . . . . . . . . . . . . . 29Clinical Trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Work-Up (Evaluation) and Treatment Guidelines . . . . . . . . . . . . . . . 33
Decision TreesStage 0 Lobular Carcinoma in Situ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Stage 0 Ductal Carcinoma in Situ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Stage I, II, and Some Stage III Breast Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Axillary Lymph Node Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46Additional Treatment (Adjuvant Therapy) After Surgery . . . . . . . . . . . . . . . . . 48
Invasive Ductal, Lobular, Mixed, or Metaplastic Cancers with Small Tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .50Invasive Ductal, Lobular, Mixed, or Metaplastic Cancers with Larger Tumors or Lymph Node Spread . . . . . . . . . . . . . . . . . . . . . . . . . . .52Tubular or Colloid Breast Cancers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .54
Adjuvant Hormone Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56Treatment of Large Stage II or Stage IIIA Breast Cancers . . . . . . . . . . . . . . . . . 60Stage III Locally Advanced Breast Cancers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66Follow-up and Treatment of Stage IV Disease or Recurrence of Disease . . . 70Breast Cancer in Pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82

Arthur G. James Cancer Hospital and Richard J. Solove Research Institute at The Ohio State University
City of Hope Cancer Center
Dana-Farber/Partners CancerCare
Duke Comprehensive Cancer Center
Fox Chase Cancer Center
Fred Hutchinson Cancer Research Center/Seattle Cancer Care Alliance
H. Lee Moffitt Cancer Center & Research Instituteat the University of South Florida
Huntsman Cancer Institute at the University of Utah
Memorial Sloan-Kettering Cancer Center
Robert H. Lurie Comprehensive Cancer Center of Northwestern University
Roswell Park Cancer Institute
The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
Siteman Cancer Center at Barnes-Jewish Hospital andWashington University School of Medicine
St. Jude Children’s Research Hospital/University of Tennessee Cancer Institute
Stanford Comprehensive Cancer Center
UCSF Comprehensive Cancer Center
University of Alabama at Birmingham Comprehensive Cancer Center
University of Michigan Comprehensive Cancer Center
The University of Texas M.D. Anderson Cancer Center
UNMC/Eppley Cancer Center at The Nebraska Medical Center
Member Institutions

Introduction
With this booklet, women with breast cancerhave access to information on the way breastcancer is treated at the nation’s leadingcancer centers. Originally developed for cancerspecialists by the National ComprehensiveCancer Network (NCCN), these treatmentguidelines have now been translated for thepublic by the American Cancer Society.
Since 1995, doctors have looked to theNCCN for guidance on the highest quality,most effective advice on treating cancer. Formore than 90 years, the public has relied onthe American Cancer Society for informationabout cancer. The Society’s books andbrochures provide comprehensive, current,and understandable information to hundredsof thousands of patients, their families andfriends. This collaboration between theNCCN and ACS provides an authoritative andunderstandable source of cancer treatmentinformation for the public. These patientguidelines will help you better understandyour cancer treatment and your doctor’scounsel. We urge you to discuss them withyour doctor. To make the best possible use ofthis information, you might begin by askingyour doctor the following questions:
• How large is my cancer? Do I havemore than one tumor in the breast?
• What is my cancer’s grade (how abnormal the cells appear) and histology(type and arrangement of tumor cells)as seen under a microscope?
• Do I have any lymph nodes with cancer(positive lymph nodes, i.e. nodal status)?If yes, how many?
• What is the stage of my cancer?
• Does my cancer contain hormonereceptors? What does this mean for me?
• Is my cancer positive for HER-2? What does this mean for me?
• Is breast-conserving treatment anoption for me?
• In addition to surgery, what other treat-ment do you recommend? Radiation?Chemotherapy? Hormone therapy?
• What are the side effects?• Are there any clinical trials that I
should consider?
Making Decisions AboutBreast Cancer Treatment
On the pages after the general informationabout breast cancer, you’ll find flow chartsthat doctors call decision trees. The chartsrepresent different stages of breast cancer.Each one shows you step-by-step how youand your doctor can arrive at the choices youneed to make about your treatment.
Here you will find background informationon breast cancer with explanations of cancerstage, work-up, and treatment—all categoriesused in the flow charts. We’ve also provided aglossary at the end of the booklet. Words inthe glossary will appear in italics when firstmentioned in this booklet.
Although breast cancer is a very seriousdisease, it can be treated, and it should betreated by a team of health care professionalswith experience in treating women with breastcancer. This team may include a surgeon,radiation oncologist, medical oncologist,radiologist, pathologist, oncology nurse,social worker, and others. But not all women
5

with breast cancer receive the same treat-ment. Doctors must consider a woman’sspecific medical situation and the patient’spreferences. This booklet can help you andyour doctor decide which choices best meetyour medical and personal needs.
Breast cancer can occur in men. Since theincidence is very low, this booklet is forwomen with breast cancer. To learn moreabout breast cancer in men, speak with yourdoctor and contact the American CancerSociety at 1-800-ACS-2345 or visit our Website at www.cancer.org.
Inside Breast Tissue
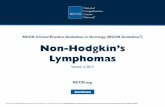
The main parts of the female breast are lobules(milk producing glands), ducts (milk passagesthat connect the lobules and the nipple), andstroma ( fatty tissue and ligaments surround-ing the ducts and lobules, blood vessels, andlymphatic vessels). Lymphatic vessels aresimilar to veins but carry lymph instead ofblood. Most breast cancer begins in the ducts(ductal), some in the lobules (lobular), andthe rest in other breast tissues.
Lymph is a clear fluid that has tissue wasteproducts and immune system cells. Mostlymphatic vessels of the breast lead to under-arm (axillary) lymph nodes. Some lead tolymph nodes above the collarbone (calledsupraclavicular) and others to internal mam-mary nodes which are next to the breastbone(or sternum). Cancer cells may enter lymphvessels and spread along these vessels toreach lymph nodes. Cancer cells may alsoenter blood vessels and spread through thebloodstream to other parts of the body.
Lymph nodes are small, bean shaped col-lections of immune system cells important infighting infections. When breast cancer cellsreach the axillary lymph nodes, they cancontinue to grow, often causing swelling ofthe lymph nodes in the armpit or elsewhere.
If breast cancer cells have spread to theaxillary lymph nodes, it makes it more likelythat they have spread to other organs of thebody as well.
Types of Breast Cancer
Breast cancer is an abnormal growth of cellsthat normally line the ducts and the lobules.Breast cancer is classified by whether thecancer started in the ducts or lobules,whether the cells have “invaded” (grown orspread) through the duct or lobule, and theway the cancer cells look under a microscope.
6
Lobular cells
Lobules
Lobule
Ductcells
Duct
Ducts
NippleAreola
Fatty connective tissue
Diagram of Breast
Source: American Cancer Society, 2006

Breast cancers are broadly grouped into thosethat are still in the breast lobules or ducts(referred to as “noninvasive” or “carcinoma insitu”) and those that have spread beyond thewalls of the ducts or lobules (referred to as“infiltrating” or “invasive”). It is not unusual fora single breast tumor to have combinations ofthese types, and to have a mixture of invasiveand non-invasive cancer.
Carcinoma In Situ Carcinoma is another word for cancer andcarcinoma in situ (CIS) means that the canceris a very early cancer and it is still confined tothe ducts or lobules where it started. It hasnot spread into surrounding fatty tissues inthe breast or to other organs in the body.There are 2 types of breast carcinoma in situ:
• Lobular carcinoma in situ (LCIS): Alsocalled lobular neoplasia. It begins in thelobules, but has not grown through the
lobule walls. Breast cancer specialists donot think that LCIS itself becomes aninvasive cancer, but women with thiscondition do run a higher risk of devel-oping an invasive cancer in either breast.
• Ductal carcinoma in situ (DCIS): Thisis the most common type of noninvasivebreast cancer. In DCIS, cancer cellsinside the ducts do not spread throughthe walls of the ducts into the fatty tissue of the breast. DCIS is treatedwith surgery and sometimes radiation,which are usually curative. If nottreated, DCIS may grow and becomean invasive cancer.
Invasive Breast CancersInvasive cancer describe those cancers thathave started to grow and have spread beyondthe ducts or lobules. These cancers aredivided into different types of invasive breastcancer depending on how the cancer cellslook under the microscope. They are alsogrouped according to how closely they looklike normal cells. This is called the gradewhich helps predict whether the woman hasa good or less favorable outlook. Outlook isreferred to as prognosis.
Invasive (also called Infiltrating) Ductal Carcinoma (IDC)
The cancer starts in a milk passage, orduct, of the breast, but then the cancer cellsbreak through the wall of the duct and spreadinto the fatty tissue. Cancer cells can thenspread into lymphatic channels or blood ves-sels of the breast and to other parts of thebody. About 80% of all breast cancers areinvasive ductal carcinoma.
7
Normal Lymph Drainage
Source: American Cancer Society, 2006
Lymphnodes
Lymphvessels
Internalmammarylymph node
Axillarylymph nodes

Invasive (also called Infiltrating) Lobular Carcinoma (ILC)
This type of cancer starts in the milk-producing glands. Like IDC, this cancer canspread beyond the breast to other parts of thebody. About 10% to 15% of invasive breastcancers are invasive lobular carcinomas.
Mixed TumorsMixed tumors describe those that contain
a variety of cell types, such as invasive ductalcombined with invasive lobular breastcancer. With this type, the tumor is usuallytreated as if it were an invasive ductal cancer.
Medullary CancerThis special type of infiltrating ductal
cancer has a fairly well-defined boundarybetween tumor tissue and normal breast tis-sue. It also has a number of special features,including the presence of immune systemcells at the edges of the tumor. It accounts forabout 5% of all breast cancer. It can be diffi-cult to distinguish medullary breast cancerfrom the more common invasive ductal breastcancer. Most cancer specialists think thatmedullary cancer is very rare, and that cancersthat are called medullary cancer should betreated as invasive ductal breast cancer.
Metaplastic TumorsMetaplastic tumors are a very rare type of
invasive ductal cancer. These tumors includecells that are normally not found in thebreast, such as cells that look like skin cells(squamous cells) or cells that make bone.These tumors are treated similarly to invasiveductal cancer.
Inflammatory Breast Cancer (IBC)Inflammatory breast cancer is a special
type of breast cancer in which the cancer cellshave spread to the lymph channels in the skinof the breast. Inflammatory breast canceraccounts for about 1% to 3% of all breastcancers. The skin of the affected breast is red,swollen, may feel warm, and has the appear-ance of an orange peel. The affected breast maybecome larger or firmer, tender, or itchy. IBCis often mistaken for infection in its early stages.
Inflammatory breast cancer has a higherchance of spreading and a worse outlookthan typical invasive ductal or lobular cancer.Inflammatory breast cancer is always stagedas stage IIIB unless it has already spread toother organs at the time of diagnosis whichwould then make it a stage IV. (See discussionof stage on page 14).
Colloid CarcinomaThis rare type of invasive ductal breast
cancer, also called mucinous carcinoma, isformed by mucus-producing cancer cells.Colloid carcinoma has a better outlook and alower chance of metastasis than invasive lob-ular or invasive ductal cancers of the same size.
Tubular Carcinoma Tubular carcinoma is a special type of
invasive ductal breast carcinoma. About 2%of all breast cancers are tubular carcinomas.Women with this type of breast cancer have abetter outlook because the cancer is less likelyto spread outside the breast than invasivelobular or invasive ductal cancers of the samesize. The majority of tubular cancers are hor-mone receptor positive and HER-2 negative.(See discussion of tumor tests, on page 12.)
8

Breast Cancer Work Up
Evaluating a Breast Lump orAbnormal Mammogram FindingAn evaluation of a breast lump or an abnormalmammogram finding includes a thoroughmedical history, a physical examination, andbreast imaging (such as x-rays). A biopsy isneeded for a suspicious finding, though oftenthese suspicious areas prove to be benign (notcancer). If cancer is found, other x-rays andblood tests are needed. Exactly which testsare helpful depends on the type of cancer, andif and where it has spread. These sectionsprovide a summary of the steps, tests, andtypes of biopsy that may be suggested.
Doctor Visit and ExaminationA women’s first step in having a new breast
lump, symptom, or mammogram changeevaluated is to meet with her doctor. Thedoctor will take a medical history, includingasking a series of questions about symptomsand factors that may be related to breastcancer risk (such as family history of cancer).The physical examination should include ageneral examination of the woman’s body aswell as careful examination of her breasts(called palpation). The doctor will examine:
• the breasts, including texture, size,relationship to skin and chest muscles,and the presence of lumps or masses
• the nipples and skin of the breasts• lymph nodes under the armpit and
above the collarbone• other organs to check for obvious
spread of breast cancer and to helpevaluate the general condition of thewoman’s health
Breast ImagingAfter completing the physical examination
and medical history, the doctor will recommendtests to look at the breast. A mammogram willlikely be done first, unless this has alreadybeen done or if the woman is very young.
Women with a lump in the breast, othersuspicious symptoms, or with a change foundon a screening mammogram, will often havea procedure called a diagnostic mammogram.A diagnostic mammogram includes moremammogram images of the area of concernto give more information about the size andcharacter of the area. A breast ultrasound orsonogram also may be done. Ultrasoundexamination uses high frequency sound wavesto further evaluate a lump or mammogramfinding. Most importantly, ultrasound helpsdetermine if the area of concern is a fluid-filled simple cyst, which is usually not cancer,or is solid tissue that may be cancer.
Some women may have a breast magneticresonance imaging (MRI) procedure in additionto a diagnostic mammogram and ultrasound.In some cases, breast MRI may help definethe size and extent of cancer within the breasttissue. It can also spot other tumors. It may beespecially useful in women who have densebreast tissue that makes it more difficult tofind tumors with a mammogram.
Breast BiopsyIf a woman or her doctor finds a suspicious
breast lump, or if imaging studies show asuspicious area, the woman must have abiopsy. This procedure takes a tissue sampleto be examined under the microscope to seeif cancer is present.
9

There are several different types of breastbiopsies. Biopsy may be done by a needle,where the doctor removes a piece of breasttissue by placing a needle through the skininto the breast. With a surgical biopsy a sur-geon uses a scalpel to cut through the skinand remove a larger piece of breast tissue.Each type of biopsy has advantages and dis-advantages. The type of biopsy procedureused is tailored to each woman’s situationand the experience of her health care team.
In most cases, a needle biopsy is preferredover a surgical biopsy as the first step inmaking a cancer diagnosis. A needle biopsyprovides a diagnosis quickly and with littlediscomfort. In addition, it gives the woman achance to discuss treatment options with herdoctor before any surgery is done. In somepatients, a surgical biopsy may still be neededto remove all or part of a lump for microscopicexamination after a needle biopsy has beendone, or it may be necessary to do a surgicalbiopsy instead of needle biopsy.
Several types of needle biopsies are usedto diagnosis breast cancer. The most commonis a core needle biopsy that removes a smallcylinder of tissue. A suction device attachedto the needle can also be used to removebreast tissue. Another type of biopsy is fineneedle aspiration biopsy (FNA). FNA uses asmaller needle than a core biopsy andremoves a small amount of cells for evaluationunder the microscope. FNA also is used toremove fluid from a suspicious cyst.
A doctor can do a core needle or FNAbiopsy in the office, without the aid of breastx-rays to guide the needle, if the lump can befelt. If a lump cannot be felt easily, ultrasoundor mammograms can be used to guide the
needle during the biopsy. The mammogram-directed technique is called stereotactic nee-dle biopsy. In this procedure, a computerizedview of the mammogram helps the doctorguide the tip of the needle to the right spot.Ultrasound can be used in the same way toguide the needle. The choice between amammogram directed stereotactic needlebiopsy and ultrasound guided biopsy dependson the type and location of the suspiciousarea, as well as the experience and preferenceof the doctor.
Some patients need a surgical (excisional)biopsy. The surgeon generally removes theentire lump or suspicious area and includes azone of surrounding normal appearing breasttissue called a margin. If the tumor cannot befelt, then the mammogram or ultrasound isused to guide the surgeon through a techniquecalled wire localization. After numbing the areawith a local anesthetic, x-ray or ultrasoundpictures are used to guide a small hollowneedle to the abnormal spot in the breast. Athin wire is inserted through the center of theneedle, the needle is removed, and the wire isused to guide the surgeon to the right spot.
Most breast biopsies cause little discomfort.Only local anesthesia (numbing of the skin)is necessary for needle biopsies. For surgicalbiopsies, most surgeons use a local anestheticplus some intravenous medicines to make thepatient drowsy. A general anesthetic is notneeded for most breast biopsies.
Tissue examination and pathology reportAfter a breast biopsy, the biopsy tissue is
sent to a pathology lab where a doctor trainedto diagnose cancer (pathologist) examines itunder the microscope. This process may take
10

11
several days. This examination of the breasttissue determines if cancer is present.
The pathology report is a key part of yourcancer care. This report tells your doctor whattype of cancer you have, and includes manyfacts that will determine the best treatmentfor you.
Your doctor should give you your pathologyresults. You can ask for a copy of your pathologyreport and to have it explained carefully to you.If you want, you can obtain a second opinionof the pathology of your tissue by having themicroscope slides from your tissue sent to aconsulting breast pathologist at an NCCNcancer center or other laboratory suggestedby your doctor.
Other Tests after Cancer Has Been DiagnosedIf the breast biopsy results show that canceris present, the doctor may order other teststo find out if the cancer has spread and tohelp determine treatment. For most womenwith breast cancer, extensive testing providesno benefit and is not necessary. There is notest that can completely reassure you that thecancer has not spread. The NCCN Guidelinesdescribe which tests are needed based on theextent (spread) of the cancer and the resultsof the history and physical examination. Teststhat may be done include:
Chest x-ray: All women with invasivebreast cancer should have a chest x-ray beforesurgery and to see if there is evidence that thebreast cancer has spread to the lungs.
Bone scan: This may provide informationabout spread of breast cancer to the bone.However, many changes that show up on abone scan are not cancer. Unless there are
symptoms of spread to the bone, includingnew pains or changes on blood tests, a bonescan is not recommended except in patientswith advanced cancer. To do a bone scan, asmall dose of a radioactive substance isinjected into your vein. The radioactive sub-stance collects in areas of new bone formation.These areas can be seen on the bone scanimage. Other than the needle stick for theinjection, a bone scan is painless.
Computerized tomography (CT) scans:CT scans are done when symptoms or otherfindings suggest that cancer has spread toother organs. For most women with an earlystage breast cancer, a CT scan is not needed.But if the cancer appears more advanced, aCT of the abdomen and/or chest may be doneto see if the cancer has spread. CT scans takemultiple x-rays of the same part of the bodyfrom different angles to provide detailedpictures of internal organs. Except for theinjection of intravenous dye, necessary formost patients, this is a painless procedure.
Magnetic resonance imaging (MRI):MRI scans use radio waves and magnets toproduce detailed images of internal organswithout any x-rays. MRI is useful in looking atthe brain and spinal cord, and in examiningany specific area in the bone. A special MRIprocedure called a breast MRI with dedicatedbreast coils can also be used to look for tumorsin the breast. Routine MRIs for all patients withbreast cancer are not helpful and not needed.
Positron emission tomography (PET):PET scans use a form of sugar (glucose) thatcontains a radioactive atom. A small amountof the radioactive material is injected into avein. Then you are put into the PET machinewhere a special camera can detect the

radioactivity. Because of the high amount ofenergy that breast cancer cells use, areas ofcancer in the body absorb large amounts ofthe radioactive sugar. Newer devices combinePET scans and CT scans.
Blood Tests: Some blood tests are neededto plan surgery, to screen for evidence ofcancer spread, and to plan treatment aftersurgery. These blood tests include:
• Complete blood count (CBC). Thisdetermines whether your blood has thecorrect type and number of blood cells.Abnormal test results could reveal otherhealth problems including anemia, andcould suggest the cancer has spread tothe bone marrow. Also, if you receivechemotherapy, doctors repeat this testbecause chemotherapy often affects theblood forming cells of the bone marrow.
• Blood chemicals and enzyme tests.These tests are done in patients withinvasive breast cancer (not needed within situ cancer). They can sometimes tellif the cancer has spread to the bone orliver. If these test results are abnormal,your doctor will order imaging tests,such as bone scans or CT scans.
Tumor tests (estrogen receptor, proges-terone receptors, and HER-2/neu): Testingthe tumor itself for certain features is animportant step in deciding what treatmentoptions are best for your particular cancer.The pathology lab tests the cancer tissue thatis removed, either from a biopsy or the finalsurgery.
• Estrogen and Progesterone Receptors:Two hormones in women—estrogen andprogesterone—stimulate the growth ofnormal breast cells and play a role in
many breast cancers. Cancer cellsrespond to these hormones throughthe estrogen receptors (ER) and prog-esterone receptors (PR). ER and PR arecells’ “welcome mat” for these hormonescirculating in the blood. The tumor istested for these receptors in a testcalled a hormone receptor assay. If acancer does not have these receptors,it is referred to as hormone receptornegative (estrogen-receptor negativeand progesterone-receptor negative). If the cancer has these receptors, it isreferred to as hormone receptor positive(estrogen- receptor positive and/orprogesterone-receptor positive) or justER-positive or PR-positive.
The hormone receptors are impor-tant because cancer cells that are ERor PR-positive often stop growing if thewoman takes drugs that either blockthe effect of estrogen and progesteroneor decrease the body’s levels of estrogen.These drugs lower the chance that thecancer will come back (recur) andimprove the changes of living longer.Most women whose breast cancer isER-positive or PR-positive will takethese drugs as part of their treatment.However, these hormone-active drugsare not effective if the cancer does notcontain these receptors.
All breast cancers, with the exceptionof lobular carcinoma in situ, should betested for hormone receptors. Eachwoman should ask her doctor for thesetest results, and if hormone-like drugsor blocking her own hormones shouldbe part of the treatment.
12

• HER-2/neu: About 15-25% of breastcancers have too much of a growth-promoting protein called HER-2/neuand too many copies (more than 2) ofthe gene that instructs the cells to produce that protein. Tumors withincreased levels of HER-2/neu arereferred to as “HER-2 positive.”
HER-2 positive tumors tend to growand spread more rapidly than otherbreast cancers. They can be treated witha drug called trastuzumab that preventsthe HER-2/neu protein from stimulatingbreast cancer cell growth. Recent studieshave shown that trastuzumab givenafter breast cancer surgery for HER-2positive tumors reduces the risk ofrecurrence when the tumor measureslarger than 1 cm in diameter or whenthe cancer has spread to the lymphnodes. Studies also suggest that chemo-therapy containing certain drugs (suchas doxorubicin or epirubicin) may beespecially effective against breastcancers that are HER-2 positive.
Genetic Analysis of Tumor: Treatmentdecisions today are primarily based on hor-mone receptor status, HER-2/neu status,appearance of the cancer under the micro-scope, size of the breast cancer, and extent ofspread of the breast cancer. Recently, therehas been interest in studying the genes inbreast cancers to see if the tumors can bedivided into good prognosis and poor prog-nosis tumors. This information has thepotential to identify those patients whosebreast cancers have not spread to the lymphnodes and who may not need additional
chemotherapy. At the present time morestudies are needed on this new strategy beforespecific recommendations can be made.
Breast Cancer Grade: Pathologists lookat breast cancers under a microscope anddetermine how much they look like normalbreast tissue. This is called the grade of thetumor. Cancers that closely resemble normalbreast tissue get a lower number grade andtend to grow and spread more slowly. In gen-eral, a lower grade number indicates a cancerthat is slightly less likely to spread, and a highernumber indicates a cancer that is slightlymore likely to spread.
Grade is based on the arrangement of thecells in relation to each other; whether theyform tubules, how closely they resemblenormal breast cells (nuclear grade), and howmany of the cancer cells are in the process ofdividing (mitotic count). A low grade (Grade 1)cancer may also be called “well-differentiated”because it more closely resembles normal breastcells. Similarly a high grade tumor (Grade 3)may also be called “poorly differentiated,”since the cells have lost their resemblanceto normal breast cells. A moderate grade(Grade 2) cancer is in between low grade andhigh grade.
The tumor grade is most important inpatients with small tumors without lymph nodeinvolvement. Patients with well-differentiatedtumors may require no further treatment,while patients with moderately or poorly dif-ferentiated tumors usually receive additionalhormonal therapy or chemotherapy.
Ductal carcinoma in situ (DCIS) is gradedin a different way. DCIS is given a nucleargrade, which describes how abnormal the
13

part of the cancer cells that contain the geneticmaterial appears. Sometimes other featuresof DCIS are also used by the pathologist todetermine the grade.
Breast Cancer Stages
Cancers are divided into different groups,called stages, based on whether the cancer isinvasive or non-invasive, the size of thetumor, how many lymph nodes are involved,and whether there is spread to other parts ofthe body.
Staging a cancer is the process of findingout how far the cancer has progressed whenit is diagnosed. Doctors determine the stageof a cancer by gathering information fromphysical examinations and tests on the tumor,lymph nodes, and distant organs.
A breast cancer’s stage is one of the mostimportant factors that may predict prognosis(outlook for cure versus the chance of cancercoming back or spreading to other organs).A cancer’s stage, therefore, is an importantfactor in choosing the best treatment.
Each woman’s outlook with breast cancerdiffers, depending on the cancer’s stage andother factors such as hormone receptors, hergeneral state of health, and her treatment.
You should talk frankly with your doctorsabout your cancer stage and prognosis, andhow they affect treatment options.
System to Define Cancer StageThe system most often used to describe theextent of breast cancer is the TNM stagingsystem. In TNM staging, information aboutthe tumor (T-Stage), nearby lymph nodes (N-Stage), and distant metastases (M-Stage) iscombined and a stage is assigned to specificTNM groupings. The TNM stage groupingsare described using Roman numerals from 0to IV.
The clinical stage is determined by what thedoctor learns from the physical examinationand tests. The pathologic stage includes thefindings of the pathologist after surgery. Mostof the time, pathologic stage is the mostimportant stage since involvement of the lymphnodes can only be accurately determined byexamining them under a microscope.
14
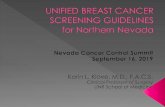
5 cm
2.5 centimeters (cm) = 1 inch1 cm = 10 mm
Tumor Sizes
1 cm 2 cm 3 cm
Source: American Cancer Society, 2006

T stands for the size of the cancer (meas-ured in centimeters: 2.5 centimeters = 1 inch)and whether it is growing directly intonearby tissues. N stands for spread to nearbylymph nodes and M is for metastasis (spreadto other parts of the body).
Categories of T, N, and M
T CategoriesT categories are based on the size of the
breast cancer and whether it has spread tonearby tissue.
Tis: Tis is used only for carcinoma in situor noninvasive breast cancer such as ductalcarcinoma in situ (DCIS) or lobular carcinomain situ (LCIS).
T1: The cancer is 2 cm in diameter (about3⁄4 inch) or smaller.
T2: The cancer is more than 2 cm but notmore than 5 cm in diameter.
T3: The cancer is more than 5 cm in diameter.
T4: The cancer is any size and has spreadto the chest wall or the skin.
N CategoriesThe N category is based on which of the
lymph nodes near the breast, if any, are affectedby the cancer. There are 2 classifications used todescribe N. One is clinical—before surgery—i.e. what the doctor can feel or see on imagingstudies. The other is pathological—what thepathologist can see in lymph nodes removedat surgery.
N0 Clinical: The cancer has not spread tolymph nodes, based on clinical exam.
N0 Pathological: The cancer has notspread to lymph nodes, based on examiningthem under the microscope.
N1 Clinical: The cancer has spread tolymph nodes under the arm on the same sideas the breast cancer. Lymph nodes are notattached to one another or to the surroundingtissue.
N1 Pathological: The cancer is found in 1to 3 lymph nodes under the arm.
N2 Clinical: The cancer has spread tolymph nodes under the arm on the same sideas the breast cancer and are attached to oneanother or to the surrounding tissue. Or thecancer can be seen to have spread to theinternal mammary lymph nodes (next to thesternum), but not to the lymph nodes underthe arm.
N2 Pathological: The cancer has spread to4 to 9 lymph nodes under the arm.
N3 Clinical: The cancer has spread tolymph nodes above or just below the collar-bone on the same side as the cancer, and mayor may not have spread to lymph nodes underthe arm. Or the cancer has spread to internalmammary lymph nodes and lymph nodesunder the arm, both on the same side as thecancer.
N3 Pathological: The cancer has spread to10 or more lymph nodes under the arm or alsoinvolves lymph nodes in other areas aroundthe breast.
M CategoriesThe M category depends on whether the
cancer has spread to any distant tissues andorgans.
M0: No distant cancer spread.M1: Cancer has spread to distant organs.
15

Stage Grouping for Breast CancerOnce the T, N, and M categories have beenassigned, this information is combined toassign an overall stage of 0, I, II, III or IV asseen in the table. The stages identify tumortypes that have a similar outlook and thus aretreated in a similar way.
Breast Cancer Treatment
Breast cancer treatment includes treatmentof the breast and treatment for cancer cellsthat may have spread to other parts of thebody. The breast itself is treated by surgery,often in combination with radiation. Thelymph nodes in the armpit are also studied to
see if the breast cancer has spread. The treat-ment for cancer cells that may have spreadbeyond the breast and lymph nodes in thearmpit is a combination of either hormonetherapy and/or chemotherapy.
Treatment of the BreastMost women with breast cancer will havesurgery. The 2 common types of surgery arebreast-conserving surgery and mastectomy.
Breast-Conserving SurgeryLumpectomy removes only the breast lump
and a rim of normal surrounding breast tissue.Partial or segmental mastectomy or quadran-tectomy removes more breast tissue than alumpectomy (up to one-quarter of the breast).
16
Breast Cancer Stages
Overall Stage T category N category M category
Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage IIA T0 N1 M0T1 N1 M0T2 N0 M0
Stage IIB T2 N1 M0T3 N0 M0
Stage IIIA T0 N2 M0T1 N2 M0T2 N2 M0T3 N1 M0T3 N2 M0
Stage IIIB T4 Any N M0
Stage IIIC Any T N3 M0
Stage IV Any T Any N M1

If cancer cells are present at the outside edgeof the removed breast tissue (the margin),more surgery is usually needed to remove anyremaining cancer. Most often this additionalsurgery is a repeat lumpectomy, but some-times it requires removal of the entire breast(mastectomy).
Radiation therapy is usually given afterthese types of surgery. Side effects of theseoperations include temporary swelling andtenderness and hardness due to scar tissuethat forms in the surgical site.
For most women with stage I or II breastcancer, breast conservation therapy (lumpec-tomy and radiation therapy) is as effective asmastectomy. Survival rates of women treatedwith these 2 approaches are the same. However,breast conservation therapy is not an optionfor all women with breast cancer (see section,“Choosing Between Breast-Conserving Surgeryand Mastectomy” on page 18.) Those who maynot have breast-conserving therapy include:
• prior radiation therapy of the affectedbreast or chest
• suspicious or malignant appearingabnormalities that are widespreadthroughout the breast
• women whose lumpectomy, includingany possible repeat lumpectomy whenneeded, cannot completely removetheir cancer with a satisfactory cosmetic result
• women with active connective tissuedisease involving the skin (especiallyscleroderma or lupus) that makes bodytissues especially sensitive to the sideeffects of radiation
• pregnant women who would requireradiation while still pregnant
• women whose tumors are larger than 5 centimeters (2 inches) and can’t beshrunk by treatment before surgery
Radiation therapy as a part of breast-conserving therapy for invasive cancer cansometimes be omitted. Women who mayconsider lumpectomy without radiationtherapy have all of the following:
• age 70 years or older; and• a tumor 2 cm or less that has been
completely removed; and• a tumor that contains hormone
receptors; and• no lymph node involvement; and• who receive treatment with hormone
therapy
MastectomyMastectomy is removal of the entire breast,
including the nipple. Mastectomy is neededfor some cases, and some women choosemastectomy rather than lumpectomy. (Seediscussion on next page, Choosing BetweenBreast-Conserving Surgery and Mastectomy.)
Different words are used to describemastectomy depending on the extent of thesurgery in the armpit and the muscles underthe breast. In a simple or total mastectomy theentire breast is removed, but no lymph nodesfrom under the arm or muscle tissue frombeneath the breast is removed. In a modifiedradical mastectomy, the entire breast and someaxillary (underarm) lymph nodes are removed.In a radical mastectomy, all the muscle underthe breast is also removed. Radical mastec-tomy is rarely used today, and for mostwomen, this surgery is not more effectivethan more limited forms of mastectomy.
17

Choosing Between Breast-ConservingSurgery and MastectomyThe advantage of breast-conserving surgery(lumpectomy) is that it preserves the appear-ance of the breast. A disadvantage is the needfor several weeks of radiation therapy aftersurgery. Some women who have a mastectomywill still need radiation therapy. Women whochoose lumpectomy and radiation can expectthe same chance of survival as those whochoose mastectomy.
Although most women and their doctorsprefer lumpectomy and radiation therapy, yourchoice will depend on a number of factors,such as:
• how you feel about losing your breast• whether you want to devote the addi-
tional time and travel for radiationtherapy
• whether you would want to have moresurgery to reconstruct your breast afterhaving a mastectomy
• your preference for mastectomy as a wayto “take it all out as quickly as possible”
In determining the preference for lumpec-tomy or mastectomy, be sure to get all thefacts. Though you may have a gut feeling formastectomy to “take it all out as quickly aspossible,” the fact is that in most cases doingso does not provide any better chance of longterm control or a better outcome of treatment.Large research studies with thousands ofwomen participating, and over 20 years ofinformation show that when lumpectomy canbe done, mastectomy does not provide anybetter chance of survival from breast cancerthan lumpectomy plus radiation. It is becauseof these facts that most women do not havetheir breast removed.
Reconstructive SurgeryIf a woman has a mastectomy, she may wantto consider having the breast rebuilt; this iscalled breast reconstruction. This requiresadditional surgery to create the appearanceof a breast after mastectomy. The breast canbe reconstructed at the same time the mas-tectomy is done (immediate reconstruction)or at a later date (delayed reconstruction).Surgeons my use saline-filled implants or tissuefrom other parts of your body.
How do a woman and her doctor decideon the type of reconstruction and when sheshould have the procedure? The answerdepends on the woman’s personal preferences,the size and shape of her breasts, the size andshape of her body, her level of physical exer-cise, details of her medical situation (such ashow much skin is removed), and if she needschemotherapy or radiation.
If you are thinking about breast recon-struction, please discuss this with your doctorwhen you are planning your treatment.
Lymph Node SurgeryIn the treatment of invasive cancer, whethera woman has a mastectomy or lumpectomy,she and her doctor usually need to know ifthe cancer has spread to the lymph nodes.When the lymph nodes are affected, there isan increased likelihood that cancer cells havespread through the bloodstream to otherparts of the body.
Doctors once believed that removing asmany lymph nodes as possible would reducethe risk of developing spread of breast cancerand improve a woman’s chances for long-termsurvival. We now know that removing thelymph nodes probably does not improve the
18

chance for long-term survival. But knowingwhether lymph nodes are involved is impor-tant in selecting the best treatment to preventcancer recurrence.
The only way to accurately determine iflymph nodes are involved is to remove andexamine them under the microscope. Thismeans removing some or all of the lymphnodes in the armpit. In the standard operation,called an axillary lymph node dissection, allthe lymph nodes are removed. This is oftennecessary. In many cases, lymph node testingmay be done with a more limited surgery thatonly removes a few lymph nodes with fewerside effects. This is called sentinel lymph nodebiopsy, and is discussed further below.
For some women with invasive cancer,removing the underarm lymph nodes can beconsidered optional. This includes:
• women with tumors so small and withsuch a favorable outlook that lymphnode spread is unlikely
• instances where it would not affectwhether adjuvant treatment is given
• elderly women• women with serious medical conditions
Lymph node surgery is not necessary withpure ductal carcinoma in situ or pure lobularcarcinoma in situ. A sentinel node biopsy (seebelow) may be done if the woman is havingsurgery (such as mastectomy) that would makeit impossible to do the sentinel node biopsyprocedure if invasive cancer were found inthe tissue removed during the surgery.
The surgical technique used to removelymph nodes from under the armpit dependson the personal circumstances of the patient.
If there are enlarged lymph nodes withapparent spread of the cancer, or the lymphnodes are otherwise found to be involvedwith cancer, then complete axillary lymphdissection is necessary. However, in manycases, the lymph nodes are not enlarged andare not likely to contain cancer. In such cases,the more limited sentinel lymph node biopsyprocedure can be performed.
In the sentinel lymph node biopsy proce-dure the surgeon finds and removes the“sentinel nodes,” the first few lymph nodes intowhich a tumor drains. These are the lymphnodes most likely to contain cancer cells. Tofind these so-called “sentinel lymph nodes,” thesurgeon injects a radioactive substance and/or a blue dye under the nipple or into the areaaround the tumor. Lymphatic vessels carrythese substances into the sentinel lymphnodes and provide the doctor with a “lymphnode map.” The doctor can either see the bluedye or detect the radioactivity with a Geigercounter. The surgeon then removes the markednodes for examination by the pathologist.
If the sentinel node contains cancer, thesurgeon removes more lymph nodes in thearmpit (axillary dissection). This may be doneat the same time or several days after theoriginal sentinel node biopsy. If the sentinelnode is cancer-free, the patient will not needmore lymph node surgery and can avoid theside effects of full lymph node surgery. Thislimited sampling of lymph nodes is notappropriate for some women. A sentinellymph node biopsy should be consideredonly if there is a team experienced with thistechnique.
19

Side Effects of Lymph Node SurgerySide effects of lymph node surgery can be
bothersome to many women. The side effectscan occur with either the full axillary lymphnode dissection or sentinel lymph node biopsy.Side effects are much less common and lesssevere with the sentinel lymph node procedure.
Side effects of lymph node surgery include:• temporary or permanent numbness in
the skin on the inside of the upper arm• temporary limitation of arm and
shoulder movements• swelling of the breast and arm called
lymphedema
Lymphedema is the most significant of theseside effects. If it develops it may be permanent.Most women who develop lymphedema findit bothersome but not disabling. No one canpredict which patients will develop this con-dition or when it will develop. Lymphedemacan develop just after surgery, or even monthsor years later. Significant lymphedema occursin about 10% of women who have axillarylymph node dissection and in up to 5% ofwomen who have sentinel lymph node biopsy.
With care, patients can take steps to helpavoid lymphedema or at least keep it undercontrol. Talk to your doctor for more details.
Some of the steps to take to help avoidlymphedema include:
• Avoid having blood drawn from or IVsinserted into the arm on the side of thelymph node surgery.
• Do not allow a blood pressure cuff tobe placed on that arm. If you are in thehospital, tell all health care workersabout your arm.
• If your arm or hand feels tight orswollen, don’t ignore it. Tell your doctor immediately.
• If needed, wear a well-fitted compression sleeve.
• Wear gloves when gardening or doing other things that are likely tolead to cuts.
For more information on lymphedema, callthe American Cancer Society at 1-800-ACS-2345and ask for Lymphedema: What Every WomenWith Breast Cancer Should Know.
Radiation TherapyRadiation therapy uses a beam of high-energyrays (or particles) to destroy cancer cells leftbehind in the breast, chest wall, or lymphnodes after surgery. Radiation may also beneeded after mastectomy in cases with eithera larger breast tumor, or when cancer is foundin the lymph nodes.
This type of treatment can be given inseveral ways.
• External beam radiation delivers radia-tion from a machine outside the body.This is the typical radiation therapygiven after lumpectomy and is given tothe entire breast with an extra dose(“boost”) to the site of the tumor. It isusually given 5 days a week for acourse of 6 to 7 weeks.
• Brachytherapy, also called internalradiation or interstitial radiation,describes the placement of radioactivematerials in or near where the tumorwas removed. They may be placed inthe lumpectomy site to “boost’ theradiation dose in addition to externalbeam radiation therapy.
20

Recently there has been interest in limitingradiation therapy only to the site of thelumpectomy, referred to as partial breastirradiation. This is based on the observationthat when breast cancer recurs in the breast,the most common place is in the site of theoriginal tumor. Brachytherapy is one techniqueof partial breast irradiation. External beamradiation therapy also can be used to deliverpartial breast irradiation.
The extent of radiation depends onwhether or not a lumpectomy or mastectomywas done and whether or not lymph nodesare involved. If a lumpectomy was done, theentire breast receives radiation with an extraboost of radiation to the area in the breastwhere the cancer was removed to prevent itfrom coming back in that area.
If the surgery was mastectomy, radiation isgiven to the entire area of the skin and musclewhere the mastectomy was done if the tumorwas over 5 cm in size, or if the tumor is closeto the edge of the removed mastectomy tissue.
In patients who have had lumpectomy ormastectomy, further radiation may be rec-ommended if the cancer has spread to thelymph nodes. Radiation may be given to thearea just above the collarbone and along thebreastbone, depending on the number andlocation of involved lymph nodes.
Side effects most likely to occur from radi-ation include swelling and heaviness in thebreast, sunburn-like skin changes in the treatedarea, and fatigue. Changes to the breast tissueand skin usually go away in 6 to 12 months. Insome women, the breast becomes smallerand firmer after radiation therapy. There mayalso be some aching in the breast, and rarely
a rib fracture or second cancer may becaused by the radiation.
Systemic Treatment To reach cancer cells that may have spreadbeyond the breast and nearby tissues, doctorsuse drugs that can be given by pills or byinjection. This type of treatment is called sys-temic therapy. Examples of systemic treatmentinclude chemotherapy, hormone therapy,and monoclonal antibody therapy. Hormonetherapy is only helpful if the tumor is hormonereceptor positive, and trastuzumab (the mono-clonal antibody therapy) is only effective ifthe tumor is HER-2 positive.
Even in the early stages of the disease,cancer cells can break away from the breastand spread through the bloodstream. Thesecells usually don’t cause symptoms, they don’tshow up on an x-ray, and they can’t be feltduring a physical examination. But if they areallowed to grow, they can establish newtumors in other places in the body. Systemictreatment given to patients who have no evi-dence of spread of cancer, but who are at riskof developing spread of the cancer is calledadjuvant therapy. The goal of adjuvant therapyis to kill undetected cancer cells that havetraveled from the breast.
Women who have invasive breast cancershould receive adjuvant therapy, except thosewith very small or well-differentiated tumors.For example, women with hormone receptorpositive disease will receive hormone therapy,and women with HER-2 positive tumors greaterthan 1 cm in diameter or with involvement oflymph nodes will receive monoclonal antibodytherapy with trastuzumab. Chemotherapy mayalso be recommended based on the size of
21

the tumor, grade of the tumor, and presenceor absence of lymph node involvement. Forwomen with breast cancers with hormonereceptor negative tumors, hormone therapyis not effective and in women with HER-2negative tumors, trastuzumab is not effective.In women with tumors that are hormone andHER-2 negative, the only decision is whetheror not to receive chemotherapy.
In most cases, systemic treatment is givensoon after surgery using the results of thesurgery and pathology evaluation to deter-mine the best choice treatment. In somecases, the systemic therapy is given topatients after a needle biopsy but beforelumpectomy or mastectomy. This is calledneoadjuvant treatment. Oncologists givepatients neoadjuvant treatment to try toshrink the tumor enough to make surgicalremoval easier. This may allow women whowould otherwise need mastectomy to havebreast-conserving surgery.
For women whose breast cancer has spreadto other organs in the body (metastases), sys-temic treatment is the main treatment. Thistreatment may be chemotherapy, hormonetherapy, trastuzumab, or combined therapy.
ChemotherapyChemotherapy uses medicines that are toxicto cancer cells and that often kill the cancercells. Usually these cancer-fighting drugs aregiven intravenously (injected into a vein) or asa pill by mouth. Either way, the drugs travelthrough the bloodstream to the entire body.Doctors who prescribe these drugs (medicaloncologists) sometimes use only a single drugand other times use a combination of drugs.
When chemotherapy is given after surgeryfor early stage breast cancer, it is calledadjuvant chemotherapy. Sometimes chemo-therapy is given before surgery. This is calledneoadjuvant chemotherapy. In most cases,adjuvant or neoadjuvant chemotherapy ismost effective when combinations of drugsare used together. Chemotherapy may also begiven to treat breast cancer that has spread toplaces other than the breast or lymph nodes.Both single drugs and combinations of drugsare often used in the treatment of breast cancerthat has spread. Clinical research studiesover the last 30 years have determined whichchemotherapy drugs are most effective. Withcontinued research, better combinations maybe discovered.
Below are listed common combinations ofadjuvant chemotherapy drugs, divided intocombinations for women with HER-2 positivetumors and HER-2 negative tumors. There arealso lists of common chemotherapy optionsfor women who have recurrent or metastaticbreast cancer.
Chemotherapy Drugs Commonly Usedto Treat Breast Cancer
Brand Name Generic Name
Adriamycin Doxorubicin
Cytoxan Cyclophosphamide
Ellence Epirubicin
Navelbine Vinorelbine
Taxol Paclitaxel
Taxotere Docetaxel
Xeloda Capecitabine
Gemzar Gemcitabine
22

Doctors give chemotherapy in cycles, witheach period of treatment followed by a restperiod. The chemotherapy is given on the firstday of each cycle, and then the body is giventime to recover from the effects of chemo-therapy. The chemotherapy drugs are thenrepeated to start the next cycle. The timebetween giving the chemotherapy drugs variesaccording to the specific chemotherapy drug
or combination of drugs. Adjuvant chemo-therapy usually lasts for a total time of 3 to 6months depending on the drugs used.
The side effects of chemotherapy depend onthe type of drugs used, the amount taken, andthe length of treatment. Some women havemany side effects while other women have fewside effects.
23
Adjuvant Chemotherapy Options
ADJUVANT CHEMOTHERAPY OPTIONS FOR HER-2 NEGATIVE TUMORS
FAC/CAF fluorouracil/doxorubicin/cyclophosphamide orFEC/CEF cyclophosphamide/epirubicin/fluorouracil
AC doxorubicin/cyclophosphamide with or without paclitaxel
EC epirubicin/cyclophosphamide
TAC docetaxel/doxorubicin/cyclophosphamide with filgrastim support
A→CMF doxorubicin followed by cyclophosphamide/methotrexate/fluorouracil
E→CMF epirubicin followed by cyclophosphamide/methotrexate/fluorouracil
CMF cyclophosphamide/methotrexate/fluorouracil
AC x 4 doxorubicin/cyclophosphamide followed by sequential paclitaxel x 4,every 2 week regimen with filgrastim support
A→T→C doxorubicin followed by paclitaxel followed by cyclophosphamide,every 2 week regimen with filgrastim support
FEC→T flourouracil/epirubicin/cyclophosphamide followed by docetaxel
ADJUVANT CHEMOTHERAPY OPTIONS FOR HER-2 POSITIVE TUMORS
Adjuvant:AC→T + Trastuzumab doxorubicin/cyclophosphamide followed by paclitaxel
with trastuzumab
Neoadjuvant:T + Trastuzumab→ paclitaxel plus trastuzumab followed byCEF + Trastuzumab cyclophosphamide/epirubicin/fluorouracil plus trastuzumab

• Doxorubicin and epirubicin may causeheart damage but this is uncommon inpeople who do not have a history ofheart disease. If you know you haveheart disease or there is concern youmight have heart disease, your doctormay suggest special heart tests beforeyou use these drugs and may suggestother chemotherapy drugs if yourheart function is weakened.
• Temporary side effects often includeloss of appetite, nausea and vomiting,fatigue, mouth sores, and hair loss.
• Chemotherapy may cause menstrualcycles to stop either temporarily orpermanently.
• Lowering of the blood counts fromchemotherapy is the most commonserious side effect of chemotherapy.Chemotherapy does this by damagingthe blood producing cells of the bonemarrow. A drop in white blood cellscan raise a patient’s risk of infection; ashortage of blood platelets can causebleeding or bruising after minor cutsor injuries; and a decline in red bloodcells can lead to fatigue.
There are treatments for these side effects.There are excellent drugs that prevent or atleast reduce nausea and vomiting. A group ofdrugs called growth factors that stimulatethe production of white blood cells or red
24
Chemotherapy Regimens for Recurrent or Metastatic Breast Cancer
PREFERRED SINGLE AGENTS
• Doxorubicin • Paclitaxel • Vinorelbine• Epirubicin • Docetaxel • Gemcitabine• Pegylated liposomal doxorubicin • Capecitabine • Albumin-bound paclitaxel
PREFERRED COMBINATIONS
• CAF/FAC (cyclophosphamide/doxorubicin/fluorouracil) • CMF (cyclophosphamide/methotrexate/• FEC (fluorouracil/epirubicin/cyclophosphamide) fluorouracil• AC (doxorubicin/cyclophosphamide) • Docetaxel/capecitabine• EC (epirubicin/cyclophosphamide) • GT (gemcitabine/paclitaxel• AT (doxorubicin/docetaxel; doxorubicin/paclitaxel)
PREFERRED AGENTS WITH BEVACIZUMAB
Paclitaxel
OTHER ACTIVE AGENTS
• Cisplatin • Vinblastine• Carboplatin • Fluorouracil continuous IV infusion• Etoposide (in pill form)

blood cells can help bone marrow recoverafter chemotherapy and prevent problemsresulting from low blood counts. Althoughthese drugs are often not necessary, doctorshave been using them to allow them to givethe chemotherapy more often. Talk with yourdoctor about which treatment will be rightfor you.
Premenopausal women will often developearly menopause and infertility from chemo-therapy drugs. The older a woman is whenshe receives chemotherapy, the more likely itis she will stop menstruating or lose her abilityto become pregnant. Some chemotherapies aremore likely to do this than others. However,you cannot depend on chemotherapy toprevent pregnancy, and getting pregnantwhile receiving chemotherapy could lead tobirth defects and interfere with treatment.Therefore, premenopausal women shouldconsider using birth control while receivingchemotherapy. It is safe to have children afterchemotherapy, but it’s not safe to get pregnantwhile on treatment.
Ask you doctor or call the AmericanCancer Society and ask for a copy of specificguidelines for treating many of the sideeffects caused by chemotherapy, such asNausea and Vomiting Treatment Guidelines forPatients With Cancer and Fever and NeutropeniaTreatment Guidelines for Patients With Cancer.
Monoclonal Antibody TherapyTrastuzumab (Herceptin) is an antibodydirected against the HER-2/neu receptor thatis on the surface of the breast cancer cells ofsome patients. Trastuzumab is an importanttreatment option for some patients withHER-2 positive tumors. It may be used asadjuvant therapy with chemotherapy toreduce the risk of recurrence, as neoadjuvanttherapy combined with chemotherapy toshrink the size of the tumor before surgery,and as treatment for metastatic breast cancer.Trastuzumab can cause heart damage andshould be used cautiously when combinedwith other heart damaging drugs such asdoxorubicin and epirubicin.
Bevacizumab (Avastin) is another mono-clonal antibody that may be used in patientswith metastatic breast cancer. It is used incombination with the chemotherapy drugpaclitaxel. Bevacizumab works by preventingthe growth of new blood vessels that supplytumor cells with the blood, oxygen, and othernutrients they need to grow.
Hormone TherapyEstrogen, a hormone produced mostly by theovaries, but also from hormones produced bythe adrenal glands and fat tissue in a woman’sbody, causes some breast cancers to grow.
25
Preferred Chemotherapy Regimens in Combination with Trastuzumab (for HER-2 positive metastatic disease)
• Paclitaxel with or without carboplatin• Docetaxel with or without carboplatin• Vinorelbine

Several approaches can be used to block theeffect of estrogen or to lower estrogen levels.These approaches can be divided into twomain groups:
• Drugs that block the effect of estrogenon cancer cells, called anti-estrogens.These medicines do not decreaseestrogen levels; instead, they preventestrogen from causing the breast cancercells to grow.
• Drugs or treatments that lower theproduction of estrogen in the body.
These treatments are used in two situations:• Women who have hormone receptor
positive breast cancers that appear tohave been completely removed by surgery. This adjuvant therapy reducesthe risk of recurrence or spread.Adjuvant therapy may also includechemotherapy or trastuzumab.
• Women with hormone receptor posi-tive breast cancer that has spread toother parts of the body or in whom thecancer comes back.
Hormone drugs are only effective inwomen whose cancer contains increasedlevels of estrogen or progesterone receptor.Every breast cancer should be tested for thesereceptors, and you should ask your doctorthe results of this test on your cancer. If thecancer is negative for both these receptors,then the hormone drugs are of no benefit.
Often a combination of hormone therapyand chemotherapy are used in the treatmentof breast cancer.
Anti-Estrogen DrugsTamoxifen is the antiestrogen drug used
most often. Taking tamoxifen as adjuvanttherapy after surgery, usually for 5 years,reduces the chance of hormone receptorpositive breast cancer coming back. Tamoxifenis also used to treat metastatic breast cancer.
In many women, tamoxifen causes thesymptoms of menopause, including hotflashes, vaginal discharge, and mood swings.Tamoxifen has two rare, but more serious sideeffects. These are a slightly increased risk ofdeveloping cancer of the lining of the uterus(endometrial cancer) and uterine sarcoma,and a slightly increased risk of developingblood clots. For most women with breastcancer, the benefits of taking the drug faroutweigh the risks.
Toremifene is another antiestrogen closelyrelated to tamoxifen. It may be an option forpostmenopausal women with metastaticbreast cancer.
Fulvestrant is a newer drug that reducesthe number of estrogen receptors. It is ofteneffective in postmenopausal women, even ifthe breast cancer is no longer responding totamoxifen. Hot flashes, mild nausea andfatigue are the major side effects of fulvestrant.
Drugs that Lower Estrogen Levels –Aromatase Inhibitors
Aromatase inhibitors stop estrogen pro-duction in postmenopausal women. Threedrugs in this category have been approvedfor treatment of breast cancer, anastrozole,letrozole, and exemestane. They work byblocking an enzyme that makes estrogen inpostmenopausal women. They cannot stopthe ovaries of premenopausal women from
26

making estrogen. For this reason they areonly effective in postmenopausal women. Forpremenopausal women, tamoxifen remainsthe best drug to use.
The aromatase inhibitors have been com-pared with tamoxifen as adjuvant hormonetherapy. They have fewer side effects thantamoxifen because they don’t cause cancer ofthe uterus and very rarely cause blood clots.They can, however, cause osteoporosis andbone fractures because they remove allestrogen from a postmenopausal woman.They also cause side effects of hot flashes andsometimes joint pain.
The aromatase inhibitors are more effectivethan tamoxifen alone in preventing breastcancer from coming back in postmenopausalwomen. Based on recent studies, many doctorsrecommend including an aromatase inhibitorin the adjuvant hormone therapy in post-menopausal women with hormone receptorpositive breast cancer.
Hormone Therapy and MenopauseAs discussed above, the aromatase
inhibitors are not recommended for pre-menopausal women. Therefore, determiningwhether the patient is menopausal is impor-tant in making treatment decisions. This is notas simple as it may sound, because menstrualperiods can stop as a side effect of treatmentwhile the ovaries continue to make estrogen.Also, sometimes chemotherapy stops theovaries from making estrogen for a short periodof time, but when the ovaries recover fromthe chemotherapy they start making estrogenagain. Therefore, if the use of an aromataseinhibitor is considered in young women,monitoring of hormone levels such as estradiol
and FSH may be required to make sure that awoman is truly postmenopausal.
Ovarian AblationThe ovaries are the source of most estro-
gen in premenopausal women. Destroyingthe ability of the ovaries to produce estrogen(ablation) may be an effective hormone ther-apy to treat premenopausal women withcancers that are positive for the estrogen orprogesterone receptors. Destruction of theovary production of estrogen can be done ina number of ways:
• The ovaries can be removed by surgery(oophorectomy).
• Radiation therapy can be given to theovaries.
• Drugs called luteinizing hormone-releasing hormone (LHRH) agonists orantagonists block estrogen productionby the ovaries.
BisphosphonatesBisphosphonates are used in breast cancer
treatment to strengthen bones that have beenweakened by invading breast cancer cells.The most commonly used bisphosphonatesin breast cancer treatment are pamidronateand zoledronate. These drugs are not usedunless cancer has spread to the bone.
Hormonal treatment with the aromataseinhibitors may also weaken the bones bycausing loss of calcium from the bone (calledosteoporosis) and thus increase the risk of afracture. Therefore, patients treated with anaromatase inhibitor should have their bonestrength tested (called a bone density test) todetermine if medication to strengthen theirbones would be appropriate. Some patients
27

may go into early menopause due to the sideeffects of chemotherapy. Menopause is asso-ciated with bone loss, too. These patients mayalso undergo a bone density test to evaluate thepresence of osteoporosis. There are a numberof medications, including some oral forms ofbisphosphonates, to treat the loss of calciumfrom bone that is not caused by direct breastcancer in the bone. Talk with your doctorabout whether one of these medications isright for you.
Treatment of Breast CancerDuring Pregnancy
Breast cancer is diagnosed in about 1 pregnantwoman out of 3,000. Radiation therapy duringpregnancy is known to increase the risk ofbirth defects, so it is not recommended forpregnant women with breast cancer.
For this reason, breast conservation ther-apy (lumpectomy and radiation therapy) isnot considered an option if radiation cannotbe delayed until it is safe to deliver the baby.However, breast biopsy procedures and evenmodified radical mastectomy are safe for themother and fetus.
Treatment of Pain andOther Symptoms
Most of this booklet discusses ways to removeor destroy breast cancer cells or to slow theirgrowth. But helping you feel as well as youcan and continuing to do the things you enjoydoing are important goals. Don’t hesitate todiscuss your symptoms or how you feel with
your cancer care team. There are effective andsafe ways to treat pain, other symptoms ofbreast cancer, and most of the side effectscaused by breast cancer treatment. If youdon’t tell you health care team, they may haveno way of knowing about your problems.
Complementary andAlternative Therapies
Complementary and alternative medicinesare a group of different types of health carepractices, systems, and products that are notpart of your usual medical treatment. Theymay include herbs, special supplements,acupuncture, massage, and a host of othertypes of treatment. You may hear about dif-ferent treatments from your family andfriends. People will offer all sorts of things,such as vitamins, herbs, stress reduction, andmore as a treatment for your cancer or tohelp you feel better
The American Cancer Society definescomplementary medicine or methods as thosethat are used in addition to your regularmedical care. If these treatments are carefullymanaged, they may add to your comfort andwell-being. Alternative medicines are definedas those that are used instead of your regularmedical care. Some of them have been provenharmful, but are still promoted as “cures.” Ifyou choose to use these alternatives, they mayreduce your chance of fighting your cancer bydelaying or replacing regular cancer treatment.
There is a great deal of interest today incomplementary and alternative treatmentsfor cancer. Many are being studied to find outif they are truly helpful to people with cancer.
28

Before changing your treatment or addingany of these methods, it is best to discuss thisopenly with your doctor or nurse. Somemethods can be safely used along with stan-dard medical treatment. Others, however,can interfere with standard treatment orcause serious side effects. That is why it’simportant to talk with your doctor. Moreinformation about complementary and alter-native methods of cancer treatment is avail-able through the American Cancer Society’stoll-free number at 1-800-ACS-2345 or on ourWeb site at www.cancer.org.
Other Things to ConsiderDuring and After Treatment
During and after your treatment for breastcancer you may be able to speed up yourrecovery and improve your quality of life bytaking an active role in your care. Learnabout the benefits and risks of each of yourtreatment options, and ask questions of yourcancer care team if there is anything you donot understand. Learn about and look out forside effects of treatment, and report theseright away to your cancer care team so theycan take steps to ease them.
Remember that your body is as unique asyour personality and your fingerprints.Although understanding your cancer’s stageand learning about your treatment optionscan help predict what health problems youmay face, no one can say for sure how youwill respond to cancer or its treatment.
You may have special strengths such as ahistory of excellent nutrition and physicalactivity, a strong family support system, or a
deep faith, and these strengths may make adifference in how you respond to cancertreatment. There are also experienced pro-fessionals in mental health services, socialwork services, and pastoral services who mayassist you in coping with your illness.
You can also help in your own recoveryfrom cancer by making healthy lifestylechoices. If you use tobacco, stop now. Quittingwill improve your overall health and the fullreturn of the sense of smell may help youenjoy a healthy diet during recovery. If youuse alcohol, limit how much you drink. Haveno more than 1 drink per day. Good nutritioncan help you get better after treatment. Eat anutritious and balanced diet, with plenty offruits, vegetables, and whole grain foods.
If you are being treated for cancer, beaware of the battle that is going on in yourbody. Radiation therapy and chemotherapyadd to the fatigue caused by the disease itself.To help you with the fatigue, plan your dailyactivities around when you feel your best. Getplenty of sleep at night. And ask your cancercare team about a daily exercise program tohelp you feel better.
A woman’s choice of treatment will likelybe influenced by her age, the image she has ofherself and her body, her hopes and fears,and her stage in life. For example, manywomen select breast-conserving surgery withradiation therapy over a mastectomy forbody image reasons. On the other hand,some women who choose mastectomy maywant the affected area removed, regardless ofthe effect on their body image, and othersmay be more concerned about the sideeffects of radiation therapy than body image.
29

Other issues that concern women includeloss of hair from chemotherapy and thechanges of the breast from radiation therapy.Women on chemotherapy tend to gainweight and it is important to continue to eata healthy diet and exercise as much as yourenergy level will permit. In addition to thesebody changes, women may also be concernedabout the outcome of their treatment. Theseare all factors that affect how a woman willmake decisions about her treatment, how sheviews herself, and how she feels about hertreatment.
Concerns about sexuality are often veryworrisome to a woman with breast cancer.Some treatments for breast cancer can changea woman’s hormone levels and may have anegative impact on sexual interest and/orresponse. A diagnosis of breast cancer whena woman is in her 20s or 30s is especiallydifficult because choosing a partner andchildbearing are often very important duringthis period. Relationship issues are alsoimportant because the diagnosis can be verydistressing for the partner, as well as thepatient. Partners are usually concernedabout how to express their love physicallyand emotionally during and after treatment.
Suggestions that may help a womanadjust to changes in her body image includelooking at and touching her body; seeking thesupport of others, preferably before surgery;involving her partner as soon as possible aftersurgery; and openly talking about the feelings,needs, and wants created by her changedimage.
A cancer diagnosis and its treatment is amajor life challenge, with an impact on youand everyone who cares for you. Before you
get to the point where you feel overwhelmed,consider attending a meeting of a local supportgroup. If you need help in other ways, contactyour hospital’s social service department orcall the American Cancer Society who can helpyou find resources in your area. We are avail-able anytime day or night at 1-800-ACS-2345.
Clinical Trials
The Purpose of Clinical TrialsStudies of promising new or experimentaltreatments in patients are known as clinicaltrials. Researchers conduct studies of newtreatments to answer the following questions:
• Is the treatment helpful?• How does this new type of treatment
work?• Does it work better than other treatment
already available?• What side effects does the treatment
cause?• Are the side effects greater or less than
the standard treatment?• Do the benefits outweigh the side effects?• In which patients is the treatment most
likely to be helpful?
Types of Clinical TrialsA new treatment is normally studied in threephase of clinical trials.
Phase I Clinical TrialsThe purpose of a phase I study is to find
the best way to give a new treatment and howmuch of it can be given safely. Doctors watchpatients carefully for any harmful side effects.The treatment has been well-tested in labo-
30

ratory and animal studies, but the side effectsin patients are not completely known.Although doctors are hoping to help patients,the main purpose of a phase I study is to testthe safety of the drug.
Phase II Clinical TrialsThese are designed to see if the drug works.
Patients are usually given the highest dose thatdoesn’t cause severe side effects (determinedfrom the phase I study) and closely observedfor an effect on the cancer. The doctor will alsolook for side effects.
Phase III Clinical TrialsPhase III studies involve large numbers of
patients. Some phase III clinical trials mayenroll thousands of patients and aredesigned to compare the results of the groupgiven the new or experimental treatmentwith the group that is given the standardtreatment. Patients are randomly assigned toone of the two groups, which means that thepatient and the doctor will not know beforethe study starts which treatment will be given.One group (the control group) will receivethe standard (most accepted) treatment. Theother group will receive the new treatment.Phase III studies are done when researchersbelieve that the two treatments are effective,but that the experimental treatment may offersome advantages. This cannot be proven untilthe results of the two groups are comparedwith each other. The study will be stopped ifthe side effects of the new treatment are toosevere or if one group has had much betterresults than the others.
All patients in a clinical trial are closelywatched by a team of experts to monitor
their progress very carefully. The study isespecially designed to pay close attention toparticipating patients. However, there aresome risks. While most side effects will dis-appear in time, some can be permanent oreven life threatening. Keep in mind, though,that even standard treatment have sideeffects. Depending on many factors, you maydecide to enroll in a clinical trial
Deciding to Enter a Clinical TrialEnrollment in a clinical trial is completely upto you. Your doctors and nurses will explainthe risks and possible benefits of the study toyou in detail and will give you a form to readand sign indicating your understanding of thestudy and your desire to take part. You shouldread the consent form very carefully and becertain that all of your questions about theclinical trial are answered before you sign it.Even after signing the form and after theclinical trial begins, you are free to leave thestudy at any time, for any reason. Taking partin the study will not prevent you from gettingother medical care you may need.
To find out more about clinical trials, askyour cancer care team. Among the questionsyou should ask are:
• What is the purpose of the study?• What kinds of tests and treatments
does the study involve?• What does this treatment do?• What is likely to happen in my case
with or without this new researchtreatment?
• What are my choices and their advantages and disadvantages?
• How could the study affect my daily life?
31

• What side effects can I expect from thestudy? Can the side effects be controlled?
• Will I have to be hospitalized? If so,how often and for how long?
• Will the study cost me anything? Will any of the treatment be free?
• If I am harmed as a result of the research,what treatment would I be entitled to?
• What type of long-term follow-up careis part of the study?
• Has the treatment been used to treatother types of cancers?
The American Cancer Society offers aclinical trials matching service that will helpyou find a clinical trial that is right for you.Simply go to our Web site (www.cancer.org)or call us at 1-800-ACS-2345. You also can geta list of current National Cancer Institutesponsored clinical trials by calling the NCICancer Information Service toll free at 1-800-4-CANCER or visiting the NCI clinical trialsWeb site (www.cancer.gov/ clinical_trials/).
32
NOTES

33
Work-Up (Evaluation) andTreatment Guidelines
Decision TreesThe decision trees on the following pages represent different stages of breastcancer. Each one shows you step-by-step how you and your doctor can arrive atthe choices you need to make about your treatment.
Keep in mind, this information is not meant to be used without the expertise ofyour own doctor who is familiar with your situation, medical history, and per-sonal preferences.
Participating in a clinical trial is an option for women at any stage of breastcancer. Taking part in a study does not prevent you from getting other medicalcare you may need.
The NCCN guidelines are updated as new, significant data become available. Toensure you have the most recent version, consult the Web sites of the AmericanCancer Society (www.cancer.org) or NCCN (www.nccn.org). You may also callthe NCCN at 1-888-909-NCCN or the ACS at 1-800-ACS-2345 for the most recentinformation on these guidelines. If you have questions about your cancer orcancer treatment, please call the American Cancer Society anytime day or nightat 1-800-ACS-2345.

Stage 0 Lobular Carcinoma in Situ The work up for lobular carcinoma in situ(LCIS) includes a complete medical historyand physical examination. A diagnosticmammogram of both breasts is done to see ifthere are any other abnormal areas in eitherbreast. Pathology review (another pathologistto look at the biopsy sample) is suggested tobe certain you have LCIS and not an invasivecancer or another condition.
LCIS is usually not treated with surgeryother than the initial biopsy procedure.Observation (careful follow-up without mas-tectomy) is the preferred option for most
women who are diagnosed with LCISbecause LCIS is not an invasive cancer, nordoes it normally become one. But womenwith LCIS have an increased risk of develop-ing invasive breast cancer in either breast.Ways to reduce the risk of breast cancer havebecome an important option.
There is evidence that two drugs—ralox-ifene and tamoxifen—can lower the risk ofdeveloping a future invasive breast cancer inwomen diagnosed with LCIS. This risk islowered when the drug is taken for a full 5 years.
A preventive mastectomy of both breastsmay be an option for women with LCIS who
34
Treatment Guidelines for Patients
Stage
Stage 0Lobular carcinomain situ (LCIS)
Work-Up (Evaluation) Treatment
• Medical history and physical exam
• Diagnostic mammogram (both breasts)
• Pathology review of biopsy sample
Observation

have a very high risk of developing invasivebreast cancer—for example, women whohave many family members with breastcancer. Your doctor can help you decidewhether to consider this treatment. Youshould also consider genetic counseling tosee if you have a gene that increases your riskof developing breast cancer before deciding tohave a preventive (prophylactic) mastectomy.After mastectomy, breast reconstruction is anoption at the same time as the mastectomyor later on.
If you and your doctor decide on observa-tion as the primary treatment for LCIS, thefollow-up includes a medical history andphysical exam every 6 to 12 months. You shouldhave a mammogram every year. Becausetamoxifen increases endometrial cancer riskin postmenopausal women, women takingthis drug should have a pelvic exam each yearand postmenopausal women should reportany bleeding from the vagina right away.These precautions are not needed if theuterus has been removed (hysterectomy).
35
Stage 0 Lobular Carcinoma in Situ
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Consider taking tamoxifenfor 5 years
In special circumstances, double mastectomy, with orwithout breast reconstructionis an option.
• Medical history and physical examevery 6 to 12 months
• Yearly mammogram unless therewas a double mastectomy
• Yearly pelvic exam for womentaking tamoxifen
Risk Reduction Follow-Up

Stage 0 Ductal Carcinoma in Situ The work up for ductal carcinoma in situ(DCIS) begins with a complete medical his-tory and physical examination. Diagnosticmammograms of both breasts should bedone to help estimate how far DCIS hasspread within the ducts of the breast and tocheck whether the opposite breast containsany abnormal areas. The NCCN recommendsa pathology review (another pathologist tolook at the biopsy sample) to be certain you
have DCIS and not an invasive cancer orother condition. The tumor should also betested for hormone receptors. If any evidenceof invasive cancer is seen in the biopsy, thewoman’s treatment should be according tothe decision trees for invasive cancer. (Seepage 40.)
The NCCN recommends that the marginof normal tissue removed around the DCISshould be at least greater than 1 mm. If DCISis present in only one area and no cancer is
36
Treatment Guidelines for Patients
Stage
Stage 0Ductal carcinomain situ (DCIS)
Work-Up (Evaluation)
• Medical history and physical exam
• Diagnostic mammogram (both breasts)
• Pathology review of biopsy sample
• Measure hormone receptor of tumor
Complete surgical excision
Patient preferredmastectomy

found at the edges of the first surgical excision,the surgical options are either a total mastec-tomy or a lumpectomy. Lymph node surgery(lymph node dissection or sentinel nodebiopsy) is generally not done with DCIS. If alumpectomy is chosen, then radiation therapyto the whole breast with a boost to the site ofthe tumor may or may not be done dependingon several factors, such as woman’s age, otherhealth problems, certain characteristics of the
tumor, and the woman’s preference. The NCCNguidelines recommend that patients interestedin partial breast irradiation participate in aclinical trial.
Mastectomy provides the most certainlocal control of DCIS. But studies have shownthat women with DCIS who are treated withlumpectomy and radiation are in no greaterdanger of dying of breast cancer than thosewho have a mastectomy. They do have a risk
37
Stage 0 Ductal Carcinoma in Situ
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Findings
Widespread DCISin two or moreseparate areas ofthe breast
Marginspositive
Reexcision
Marginsnegative
Primary Treatment(see next page)

of the cancer coming back in the breast, whichwould require a mastectomy. Mastectomy isrecommended if the margins of the excisioncontain cancer and even with repeat surgerythe DCIS cannot be completely removed.Radiation is not needed if a mastectomy isdone unless the DCIS is at the margin of themastectomy. If the mammogram, physicalexamination or biopsy results show that two
or more separate areas of the breast containDCIS, mastectomy is recommended. Withmastectomy, sentinel lymph node biopsymay be done to be certain there is no invasivecancer present, but an axillary lymph nodedissection is not needed.
After lumpectomy, a mammogram is sug-gested to ensure that the entire tumor hasbeen removed.
38
Treatment Guidelines for Patients
Findings
Widespread disease
OR
Margins positive after more surgery
OR
Patient prefers mastectomy
Primary Treatment
Total mastectomy withoutlymph node removal with orwithout breast reconstruction
Margins negative
Lumpectomy without lymph noderemoval followed by radiation
OR
Total mastectomy without lymphnode removal and with or withoutbreast reconstruction
Margins negative andtumor is low grade andsmall (less than 1⁄5 inch)
Lumpectomy followed by radiation
OR
Total mastectomy without lymphnode removal and with or withoutbreast reconstruction
OR
Lumpectomy without radiation

Women with DCIS who are treated withmastectomy can choose to have either imme-diate or delayed breast reconstruction.Women with DCIS treated with lumpectomywith or without radiation and who haveestrogen receptor positive tumors shouldconsider taking tamoxifen for 5 years. Inwomen who have had lumpectomy for DCIS,tamoxifen can lower the risk of developing aninvasive breast cancer in the same breast.
Follow-up for women with DCIS includesa medical history and physical exam every 6months for 5 years, then every year there-after. They should have yearly mammograms.Because tamoxifen increases endometrialcancer risk in postmenopausal women,patients taking this drug should have a pelvicexam every year and should promptly reportany abnormal vaginal bleeding. These pre-cautions are not needed if the uterus wasremoved.
39
Stage 0 Ductal Carcinoma in Situ (continued)
Treatment After Surgery Follow-Up
Consider tamoxifen for 5 yearsfor patients with ER-positiveDCIS treated with lumpectomywith or without radiation
• Medical history and physical exam every6 months for 5 years, then every year;
• Mammogram every year
• Yearly pelvic exam for women takingtamoxifen
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.

40
Stage I, II, and Some Stage IIIBreast CancerThe guidelines for women with stage I and IItumors, and those stage IIIA tumors larger than5 centimeters (2 inches) with breast cancer inthe lymph nodes, but not attached to eachother (T3, N1, M0), recommend the following:
• medical history and physical examination
• complete blood count, platelet count,and liver function tests
• chest x-ray• diagnostic mammograms of both breasts• breast ultrasound and MRI if needed• pathology review of biopsy sample• tests for the presence of hormone
receptors• HER-2/neu test
Bone scan may be ordered and is recom-mended if there is bone pain or abnormalblood tests.
Treatment Guidelines for Patients
Clinical Stage Work-Up (Evaluation)
Stages I and IIand Stage IIIAwith tumorlarger than 5cm and limitedlymph nodespread (T3, N1, M0)
• Medical history and physical exam
• Blood counts and chemical tests
• Chest x-ray
• Diagnostic mammogram (bothbreasts), ultrasound as needed
• Breast MRI with dedicated breastcoil may be considered for breast-conserving surgery
• Pathology review of biopsy sample
• Estrogen/progesterone receptorand HER-2/neu test of tissue
• Bone scan (only done if bone painor tests suggest cancer has spreadto bones)
• Abdominal CT, US, or MRI –optional for stage II, recommendedif blood chemistry tests abnormalor Stage IIIA – T3, N1, M0
If tumor is larger than 2 cm(0.8 inches), and breast-conserving therapy is anoption, consider preoperativetherapy (see page 61)
Mastectomy and sentinelnode biopsy or removal ofunderarm nodes with orwithout breast reconstruction(see page 44)
Lumpectomy and sentinelnode biopsy (see page 46)
OR
Removal of underarmlymph nodes

Abdominal CT scan, ultrasound, or MRImay be ordered for stage II and is recom-mended if the blood tests are abnormal orthe stage is IIIA (T3,N1, M0).
For patients with Stage I or II breast cancer,the surgery can either be a lumpectomy(removing only the cancer and a margin ofsurrounding normal tissue) or complete
removal of the breast (mastectomy). Thisdecision tree only addresses lumpectomy,while mastectomy is addressed on page 44.Lumpectomy as the surgical treatment ispossible in most women with stage I or IIbreast cancer. If the tumor is large (i.e. greaterthan 2 cm in diameter), breast-conservingsurgery is sometimes done after chemotherapy
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
41
Stage I, II, and Some Stage III Breast Cancer
Stage I, II, and Some Stage III (T3, N1, M0)
Radiation to the whole breast (withadded boost to tumor site) and supraclavicular (above the collarbone)area; consider radiation therapy tolymph nodes next to the breastbone
Radiation to the whole breast (withadded boost to tumor site). Possibleradiation to supraclavicular (abovethe collarbone) area and to lymphnodes next to the breastbone
Radiation to the whole breast (withadded boost to former tumor site)
AdditionalTreatmentAfter Surgery(see page 48)
See Treatment forLarge Stage IIBreast Cancers orStage IIIA (page 61)
See Mastectomy(page 44)
Cancer spreadto 4 or morelymph nodes
Cancer spreadto 1, 2, or 3lymph nodes
No cancerspread tolymph nodes

(see page 61). Radiation to the whole breastis recommended as part of the treatmentfollowing lumpectomy in most cases. Extraradiation should be given to the area of thebreast where the tumor was removed. Breastirradiation may be omitted in some patientsover 70 years old with small, hormone recep-tor positive tumors that do not have lymphnode involvement and who are treated withhormone therapy. The NCCN guidelines rec-ommend that patients interested in partialbreast irradiation should participate in aclinical trial.
In addition to removing the cancer bylumpectomy or mastectomy, the lymph nodesunder the arm are examined to see if they
contain cancer. There are 2 choices for exam-ining the lymph nodes—complete axillarylymph node dissection or sentinel lymph nodebiopsy (see discussion in the first part of thisbooklet). This is further described on page 46.Not all patients need lymph node evaluation;these include patients with favorable tumors,where selection of additional treatment willnot be based on whether or not the lymphnodes are involved, or in patients with otherserious medical conditions. These specificcircumstances should be discussed with yourdoctor. If the cancer has spread to lymphnodes, radiation to these areas may be given,depending on the number of involved nodes.
42
Treatment Guidelines for Patients
NOTES

In choosing breast-conserving surgeryversus mastectomy, women must understandthat as long as lumpectomy can be done satis-factorily (based on the factors that follow),the chances of successful treatment and sur-vival are the same with lumpectomy andradiation as with mastectomy. The reasonsfor choosing lumpectomy and mastectomyare discussed in the first part of this booklet.Lumpectomy and radiation therapy are notappropriate in the following women:
• prior radiation therapy of the affectedbreast or chest
• suspicious or malignant appearingabnormalities that are widespreadthroughout the breast
• women whose lumpectomy, includingany possible repeat lumpectomy whenneeded, cannot completely removetheir cancer with a satisfactory cosmetic result
• women with active connective tissuedisease involving the skin (especiallyscleroderma or lupus) that makes bodytissues especially sensitive to the sideeffects of radiation
• pregnant women who would requireradiation while still pregnant
• women whose tumor is larger than 5 centimeters (2 inches) and can’t beshrunk by treatment before surgery
43
Stage I, II, and Some Stage III Breast Cancer (continued)
NOTES

If a woman and her doctor choose a mas-tectomy as her breast cancer treatment, theguidelines recommend radiation after surgeryin the following situations:
• If the cancer has spread to 4 or morelymph nodes, radiation should be givento the area that the breast was removedfrom (the chest wall), the area abovethe collarbone and perhaps the part ofthe chest near the breast bone
• If the cancer has spread to 1 to 3 lymphnodes, there should be considerationgiven to using radiation for the areathat the breast was removed from (thechest wall), the area above the collar-bone, and perhaps the part of chestnear the breastbone.
• Even if there is no spread to lymphnodes, if the tumor is larger than 5 cmor the margins are positive, radiation
44
Treatment Guidelines for Patients
Mastectomy and sentinelnode biopsy or removal ofunderarm nodes with orwithout breast reconstruction
Cancer spread to 4 ormore lymph nodes
Cancer spread to 1,2, or 3 lymph nodes
No cancer in lymphnodes, but tumorlarger than 5 cm orpositive margins
Tumor smaller than5 cm and no cancerspread to nodes

should be given to the area that thebreast was removed from (the chestwall) and possibly the area above thecollarbone and near the breastbone.
• If the tumor is less than 5 cm and themargins are very close, radiation shouldbe given to the area that the breast wasremoved from (the chest wall).
No radiation is needed if the tumor issmaller than 5 centimeters, with good margins,and no spread to lymph nodes.
In all cases where both radiation andchemotherapy are used, the radiation is givenafter chemotherapy unless the chemotherapyregimen is CMF. CMF and radiation can begiven together.
45
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Stage I, II, and Some Stage III Breast Cancer (continued)
After chemotherapy, radiation to the chestwall and supraclavicular (above the collar-bone) area; possible radiation therapy tolymph nodes next to the breastbone
After chemotherapy, possible radiationto the chest wall and supraclavicularlymph nodes and perhaps lymph nodesnext to the breastbone
After chemotherapy, radiation to thechest wall and supraclavicular (abovethe collarbone) area and perhapslymph nodes next to the breastbone
No radiation therapy unlessmargins are very close – thenradiation to the chest wall
AdjuvantTreatment(see page 48)
Stage I, II, and Some Stage III (T3, N1, M0)

Axillary Lymph Node SurgeryIn addition to the surgery for the cancer inthe breast, the lymph nodes under the armare examined in most cases. This providesinformation to guide further treatment and isusually done at the same time as the breastsurgery.
The types of surgery for lymph nodes underthe arm are fully discussed in the first section
of this booklet. The choices are completeremoval of the lymph nodes (axillary lymphnode dissection) or removal of a few lymphnodes in the sentinel lymph node biopsyprocedure. In a mastectomy, the lymph nodesare removed through the same incision (cutin the skin). In a lumpectomy, it is usuallydone through an incision separate from thelumpectomy incision.
46
Treatment Guidelines for Patients
Stage Procedure
ClinicalStage I/II
Sentinel node procedure can be done if:
• There has been no previouschemotherapy or hormonal therapy
AND
• There is a team of doctors experiencedin the sentinel node procedure
No
Yes

Sentinel lymph node biopsy is not appro-priate for all women. It should only be used ifthe woman has not yet had any chemotherapyor hormone therapy, and when the nodes arenot enlarged and are not thought to containcancer based on physical examination at thetime of diagnosis. If a suspicious node is found
on physical exam, it can be first assessed witha needle biopsy and examined under themicroscope. If this biopsy shows no evidenceof cancer, a sentinel node biopsy is still con-sidered appropriate. A sentinel node biopsyshould only be done if the team of doctorshas proven experience with this procedure.
47
Axillary Lymph Node Surgery
Lymph nodes likelycontain cancer asdetermined by physical examination
Lymph nodesare not thoughtto be involvedwith cancer
Sentinel nodemapping andexcision
Usual axillarylymph nodesurgery
OR
Sentinel nodecontains nocancer
Sentinel nodecontains cancer
Sentinel nodenot identified
No furthersurgery
Usual axillarylymph nodesurgery
Usual axillarylymph nodesurgery
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.

Additional Treatment (AdjuvantTherapy) After SurgeryDecisions about adjuvant chemotherapy orhormonal treatment for the most commontypes of cancer (with the exception of tumorswith good prognosis cell types, such astubular or colloid) are based on the status ofthe hormone receptors and whether or notthe tumor is HER-2 positive. This creates 4different groups of tumors based upon thehormone receptor and HER-2 status:
• hormone receptor positive and HER-2positive tumors
• hormone receptor negative and HER-2positive tumors
• hormone receptor positive and HER-2negative tumors
• hormone receptor negative and HER-2negative tumors.
Hormone therapy is used only in tumorsthat are hormone receptor positive, andtrastuzumab is used only for tumors that areHER-2 positive. Chemotherapy is used whenthere is a higher risk of tumor spread basedon tumor stage and grade, or if the tumor ishormone receptor negative. Patients are
48
Treatment Guidelines for Patients
NOTES

49
Additional Treatment (Adjuvant Therapy) After Surgery
often treated with combinations of thesetherapies—hormone therapy, trastuzumaband chemotherapy, depending on the statusof the hormone receptors, HER-2 status, andthe risk for recurrence.
Specific recommendations regardingtype of hormone therapy are discussed onpage 56. Not enough data exists to makestrong recommendations regarding adjuvantchemotherapy for those over the age of 70.Decisions regarding chemotherapy in thisgroup should take into consideration otherhealth conditions.
The decision trees on the following pagesdivide patients into three broad groups:
• those with small invasive ductal or lobular cancers (and its variants) withminimal or no lymph node involvement
• those with larger invasive ductal orlobular cancers, or cancers involvinglymph nodes
• those with cancers with a more favorableoutlook, i.e. tubular or colloid subtypes.
NOTES

Invasive Ductal, Lobular, Mixed, orMetaplastic Cancers with Small Tumors
This decision tree describes patients withinvasive ductal, lobular, mixed or metaplasticcancer that measures up to 1 cm in diameter.The tumor has not spread to the chest wall orskin and the lymph nodes are either notinvolved, or only one lymph node shows avery small deposit of cancer:
• If the tumor is smaller than 0.5 cm, oris a well-differentiated tumor and is no larger than 1 cm, or the tumor isconsidered microinvasive, then noadjuvant treatment is needed. If there islymph node spread smaller than 2 mm,hormone therapy may be given if thetumor is hormone receptor positiveand chemotherapy may be given if thetumor is hormone receptor negative.
50
Treatment Guidelines for Patients
• Tumor less than orequal to 0.5 cm; or
• Microinvasive; or
• Tumor 0.6–1.0 cm,well-differentiated
Tumor 0.6–1.0 cm,moderate/poorly differentiated orunfavorable features
Cancer type is:
• Ductal
• Lobular
• Mixed
• Metaplastic
Breast Cancer Type Size of Tumor
• Tumor doesn’t invadechest wall or skin; and
• No or minimal spreadto lymph nodes

• When the tumor measures 0.6 to 1 cm,is moderately or poorly differentiatedor has unfavorable features (such aslooking aggressive under the micro-scope), hormone therapy with or without chemotherapy is given if thetumor is hormone receptor positive.Chemotherapy alone is given if thetumor is hormone receptor negative.
Whenever chemotherapy is given, itshould be given before hormone therapy.
• Ovarian ablation using surgery, radiationtherapy, or drugs (LHRH agonists orantagonists) may be recommended inpremenopausal women, although thebenefit is uncertain in those who havereceived adjuvant chemotherapy.
51
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Additional Treatment for Invasive Ductal, Lobular, Mixed, or Metaplastic Cancers with Small Tumors
No adjuvant therapy
Consider adjuvanthormone therapy
Consider adjuvantchemotherapy
Adjuvant hormone withor without chemotherapyor ovarian suppression orablation if premenopausal
Consider chemotherapy
Systemic AdjuvantTreatment
Hormone receptor positive
Hormone receptor negative
Hormone receptor positive
Hormone receptor negative
Hormone Responsiveness
No lymph node spreadwhen examined by apathologist
Lymph node spreadsmaller than 2mmwhen examined bya pathologist

Invasive Ductal, Lobular, Mixed, or Metaplastic Cancers with Larger Tumorsor Lymph Node Spread
This decision tree focuses on tumors thatare greater than 1 cm in diameter and/or withpositive lymph nodes. The HER-2 and hormonereceptor status of the tumor are also importantin choosing therapy.
• Chemotherapy is recommended for allpatients in this category. Hormonetherapy and/or trastuzumab are alsoused depending upon the features ofthe tumor. Hormone therapy is recom-mended if the tumor is hormonereceptor positive, and trastuzumab isrecommended if the tumor is HER-2
52
Treatment Guidelines for Patients
Tumor greaterthan 1 cm
Cancer has spreadto lymph nodes,measuring greaterthan 2 mm
Cancer type is:
• Ductal
• Lobular
• Mixed
• Metaplastic
Breast Cancer Type Size of Tumor

positive. Whenever chemotherapy isgiven, it should be given before hormonetherapy.
• The decision to take chemotherapy,hormone therapy, and/or trastuzumab isan important decision in the treatmentof breast cancer. Your doctor should
be able to estimate the likelihood thatthey will improve your outcome. Alongwith your doctors, you should balancethe benefits and the side effects of thetreatment to decide if the treatmentsare right for you.
53
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Adjuvant chemotherapyplus hormone therapyplus trastuzumab
Adjuvant chemotherapyplus hormone therapy
Adjuvant chemotherapyplus trastuzumab
Adjuvant chemotherapy
Systemic AdjuvantTreatment
Hormone receptor positive,HER-2/neu positive
Hormone receptor positive,HER-2/neu negative
Hormone receptor negative,HER-2/neu positive
Hormone receptor negative,HER-2/neu negative
HER-2/neu and Hormone Responsiveness
Additional Treatment for Invasive Ductal, Lobular, Mixed, or Metaplastic Cancers with Larger Tumors or
Lymph Node Spread

Tubular or Colloid Breast CancersThis decision tree addresses tubular or
colloid breast cancers, which have a morefavorable outlook than other types of breastcancer. The hormone receptor status is animportant factor in deciding treatment inthese tumors, but HER-2 status is not, sincethese tumors are usually HER-2 negative. Infact, the diagnosis of tubular cancer shouldbe questioned if the tumor is either hormonereceptor negative or HER-2 positive. Thetreatment options for tubular and colloidtumors are based on the size of tumor and
lymph node status, as well as the status ofhormone receptors. NCCN recommends thefollowing:
• For tumors smaller than 1 cm with noor a very small amount of spread in onelymph node, no treatment is neededafter surgery, although hormone therapymay be considered if the tumor is hormone receptor positive.
• If the tumor is between 1 and 2.9 cm insize, with no or a very small amount ofspread in one lymph node, adjuvantchemotherapy may be considered,
54
Treatment Guidelines for Patients
Less than 1 cm
1–2.9 cm
Greater than orequal to 3 cm
Cancer type is:
• Tubular
• Colloid
Breast Cancer Type Size of Tumor
Tumor does not invadechest wall or skin, andno spread to lymphnodes or spread issmaller than 2 mm toa single node
Cancer spread tolymph node and islarger than 2 mm

with the addition of hormone therapyfor those whose tumor has positivehormone receptors.
• Adjuvant chemotherapy is morestrongly recommended for tumors 3cm in diameter or larger, or those withpositive lymph nodes. Hormone therapyis added if the tumor is hormonereceptor positive.
The benefits of chemotherapy and hormonetherapy are additive. However, the benefit ofchemotherapy may be minimal in patientsover 60 years-old with good prognosistumors who are already receiving hormonetherapy. In these patients, the decision to addchemotherapy to hormone therapy should beindividualized.
55
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Additional Treatment for Tubular or Colloid Breast Cancers
No adjuvant therapy. May consider hor-mone therapy if hormone receptor positive
Consider adjuvant hormonetherapy plus chemotherapy
Consider adjuvant chemotherapy
Adjuvant chemotherapy
Adjuvant hormone therapyplus chemotherapy
Adjuvant hormone therapyplus chemotherapy
Adjuvant chemotherapy
Systemic Adjuvant Treatment
Hormone receptor positive
Hormone receptor negative
Hormone receptor positive
Hormone receptor negative
Hormone receptor positive
Hormone receptor negative
Hormone Responsiveness

Adjuvant Hormone TreatmentThis describes the options for adjuvant hor-monal treatment after breast surgery in womenwhose cancers contained hormone receptors.In the past, tamoxifen has been the standardtherapy. Results of recent clinical trials havepointed to new treatments, particularly theuse of aromatase inhibitors (anastrozole,
letrozole or exemestane) in postmenopausalwomen. Although all aromatase inhibitors areprobably equally effective, they are specificallynamed in this decision tree, based on theresults of clinical trials.
Tamoxifen is the recommended hormonetreatment for premenopausal patients.Treatment with tamoxifen followed by an
56
Treatment Guidelines for Patients
Premenopausal
Postmenopausal
Tamoxifen for 2 to 3 yearswith or without ovariansuppression (LHRH) or ablation (radiation, surgery)
Anastrozole or letrozole for 5 years
Tamoxifen for 2 to 3 years
Tamoxifen for 4.5 to 6 years
Tamoxifen for 5 years if womancan’t take aromatase inhibitor
Premenopausal
Postmenopausal
MenopausalStatus
Adjuvant Treatment

aromatase inhibitor, or an aromatase inhibitoralone is recommended for postmenopausalwomen. Treatment with tamoxifen followedby an aromatase inhibitor is an option forpremenopausal women who become post-menopausal during tamoxifen treatment.
If use of an aromatase inhibitor is con-sidered in a woman who was premenopausal
at the time of her diagnosis of breast cancer,she should monitored for hormone levelssuch as estradiol and FSH to make sure thatshe is truly postmenopausal.
For premenopausal women, tamoxifen for2 to 3 years is recommended. While tamoxifenalone is often recommended, another optionis to combine tamoxifen with efforts to
57
Tamoxifen for full 5 years
Tamoxifen for full 5 years
Letrozole for 5 years
Letrozole for 5 years
Letrozole for 5 years
No further hormone therapy
Exemestane or anastrozoleto complete 5 year adjuvanttherapy
Exemestane or anastrozoleto complete 5 year adjuvanttherapy
Still premenopausal
Now postmenopausal
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Additional (Adjuvant) Hormone Treatment

decrease ovarian production of estrogenusing surgery, radiation, or a medicine calledan LHRH (leutinizing hormone releasinghormone) agonist or antagonist. If thewoman becomes postmenopausal duringtreatment, the tamoxifen should be continuedfor a total of 5 years and followed by 5 years ofletrozole. Another option would be stoppingthe tamoxifen after 2 to 3 years and taking
exemestane or anastrozole for the remaining2 to 3 years. If the woman remains pre-menopausal during the 2 to 3 years of treat-ment with tamoxifen, the tamoxifen shouldbe continued for a total of 5 years. If she thenbecomes postmenopausal, the tamoxifenshould be stopped and letrozole for 5 yearsshould be added.
58
Treatment Guidelines for Patients
NOTES

For women who are postmenopausal atthe beginning of therapy, one choice is anaromatase inhibitor, either anastrozole orletrozole, for 5 years. A second option is to taketamoxifen for 2 to 3 years and then complete5 years of treatment with either anastrozoleor exemestane. A third choice is to taketamoxifen for 4.5 to 6 years and then take
letrozole for 5 years. If a woman can’t take anaromatase inhibitor, then tamoxifen for 5 yearsis an acceptable option. Aromatase inhibitorsmay weaken bones. Therefore, women takingthese drugs may have periodic checks of theirbone strength to determine if they wouldbenefit from bone strengthening drugs.
59
Additional (Adjuvant) Hormone Treatment (continued)
NOTES

Treatment of Large Stage II orStage IIIA Breast Cancers Breast-conserving treatment is usually notrecommended for women with large tumors.However, chemotherapy may shrink thetumor enough to permit a lumpectomy thatcompletely removes the main tumor and stillkeeps the size and shape of the breast accept-able. Preoperative chemotherapy is an option
that allows some women with large tumors(larger than 2 cm) that have not spread to theskin or chest wall to have breast-conservingtreatment if they want it.
The work-up recommended before startingpreoperative chemotherapy includes:
• medical history and physical examination
• blood counts and chemical tests
60
Treatment Guidelines for Patients
Clinical Stage Work-Up
The cancer is larger than 2 cm and doesn’t invadechest wall or skin. Lymphnodes can be enlarged butare movable. Diagnosed byneedle biopsy not excision.Breast-conserving surgerynot possible because toolarge a tumor in the breast.
Wants to preservebreast (Considerneedle biopsy ofenlarged lymphnodes or sentinelnode procedure.Tumor should bemarked so it canbe located afterchemotherapy.)
Doesn’t want topreserve breast
• Medical history and physical examination
• Blood counts and chemistry tests
• Chest imaging
• Diagnostic mammograms (bothbreasts)
• Breast MRI with dedicatedbreast coil may be considered
• Pathology review of biopsy sample
• Hormone receptor tests
• HER-2/neu test
• Bone scan and CT, MRI, or ultra-sound of abdomen if symptomsor abnormal blood tests ortumor over 5 cm with lymphnode spread

• CT scan of the chest or chest x-ray • diagnostic mammography of both
breasts• breast ultrasound and MRI if needed• pathology review of biopsy sample• hormone receptor test of the tumor• HER-2/neu test of the tumor
• bone scan and CT, MRI or ultrasoundof the abdomen if the tumor is largerthan 5 cm (2 inches) with lymph nodespread, or if there are symptoms ofbone spread, such as pain or abnormalblood tests.
61
Treatment of Large Stage II or Stage IIIA Breast Cancers
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Primary Treatment
Tumor eitherdoesn’t shrink, orgrows even aftertrying differentchemotherapy
Tumor shrinksbut still too largefor lumpectomy,even after tryingdifferentchemotherapy
Tumor shrinksenough forlumpectomy
Lumpectomy and removalof underarm lymph nodes(If lymph nodes notinvolved pre-chemotherapyby biopsy, no further lymphnode surgery is necessary.)(Continued on next page)
Mastectomy with removalof underarm nodes, withor without reconstruction(Continued on next page)
Presurgical therapy:
• Chemotherapy
• Hormone ther-apy, if hormone receptor positive
• Trastuzumab if HER-2/neu positive
Treat with mastectomy andsentinel node biopsy orremoval of underarm nodes,with or without reconstruction(see next page)

If there are enlarged lymph nodes, a needlebiopsy can be done before chemotherapy. If thelymph nodes are not enlarged, a sentinel nodeprocedure may be done before chemotherapy.It is recommended that the tumor be markedbefore chemotherapy so that the area can belocated in the event that the tumor completelydisappears on physical examination andmammogram.
The same drugs used as adjuvant treatmentin Stage I or II breast cancer are also usedbefore surgery to shrink the tumors to permita mastectomy or lumpectomy. If the tumor isHER-2 positive, trastuzumab should be addedto the chemotherapy. If the tumor is hormonereceptor positive, then hormone therapy issometimes used instead of chemotherapy. Ifhormone therapy is used instead of chemo-
62
Treatment Guidelines for Patients
NOTES

therapy, the preferred hormone therapy isan aromatase inhibitor in postmenopausalwomen.
If the tumor shrinks from the chemother-apy or hormone therapy, the next step islumpectomy and removal of underarm lymphnodes unless a sentinel lymph node biopsydone before the chemotherapy finds nocancer in the sentinel lymph nodes.
If the tumor doesn’t shrink enough topermit a lumpectomy, another type of chemo-therapy may be given, but a mastectomy willbe needed if there isn’t enough shrinkage in thetumor to allow a lumpectomy. Mastectomymay be followed by breast reconstruction. Theunderarm lymph nodes should be removedunless a sentinel lymph node biopsy donebefore the chemotherapy found no cancer inthe sentinel lymph nodes.
63
Treatment of Large Stage II or Stage IIIA Breast Cancers(continued)
NOTES

After mastectomy or lumpectomy, morechemotherapy may be recommended, depend-ing on the tumor size and number of positivelymph nodes. If the tumor was hormonereceptor-positive, hormone therapy shouldbe given. If a lumpectomy was done, it should
be followed by radiation therapy to the wholebreast and sometimes to the surroundinglymph nodes. The decision to treat the lymphnodes with radiation, or the decision to treatthe skin after mastectomy is based on the sameprinciples as in Stage I and II on page 44.
64
Treatment Guidelines for Patients
Primary Treatment (Local) Adjuvant (Additional)Treatment
Lumpectomy with underarmlymph node removal, with or without reconstruction.Removal of underarm nodesmay be omitted if sentinel nodebiopsy done pre-chemotherapyfinds no cancer.
Mastectomy with underarmlymph node removal, with or without reconstruction.Removal of underarm nodesmay be omitted if sentinel nodebiopsy done pre-chemotherapyfinds no cancer.
Possible additionalchemotherapy(before radiation)
Possible additionalchemotherapy(before radiation)

65
Treatment of Large Stage II or Stage IIIA Breast Cancers(continued)
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Radiation therapy (after surgery)depending on tumor size andlymph node status (see page 44)
AND
Hormonal therapy if hormonereceptor-positive.
Radiation therapy (after surgery)depending on tumor size andlymph node status (see page 44)
AND
Hormonal therapy if hormonereceptor-positive.
See follow-upcare on page 70
Radiation Therapy
NOTES

Stage III Locally Advanced BreastCancers These are advanced cancers that are growinginto the skin or chest wall or have enlargedlymph nodes that are matted together. Thereis no evidence of spread anywhere else in thebody. The recommended work-up for thesestage III breast cancers includes:
• medical history and physical examination
• blood counts and blood tests to measureliver function
• chest CT scan and perhaps chest x-ray • diagnostic mammograms of both
breasts• breast ultrasound test and/or breast
MRI (if needed)• pathology review (second opinion on
the biopsy samples)• hormone receptor test of the biopsy
sample• HER-2/neu test of the biopsy sample• bone scan• CT, MRI, or ultrasound of the abdomen
66
Treatment Guidelines for Patients
Stage III (Tumor growinginto chest wall orskin, or enlargedlymph nodes canbe felt)
• Medical history and physical examination
• Blood count and chemistry tests
• Chest CT scan with or without x-ray
• Diagnostic mammograms (bothbreasts), ultrasound, as needed
• Breast MRI with dedicated breastcoil if needed for breast-conservingsurgery
• Pathology review of biopsy sample
• Pre-chemotherapy hormone receptortests, HER-2/neu test
• Bone scan
• CT, MRI, or ultrasound of abdomen
Clinical Stage Work-Up PreoperativeChemotherapy
• Doxorubicin- orepirubicin- basedor docetaxel-basedpreoperativechemotherapypreferred
• Patients withtumors over-expressing HER-2/neu should beconsidered forneoadjuvantchemotherapyincorporatingtrastuzumab

The treatment for locally advanced breastcancer starts with chemotherapy given beforesurgery. The chemotherapy regimen shouldcontain an anthracycline (doxorubicin or epi-rubicin) or a taxane (paclitaxel or docetaxel)
and should include trastuzumab if the tumoris HER-2 positive. Patients whose tumorsshrink enough to be surgically removed have3 options:
67
Stage III Locally Advanced Breast Cancers
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Primary Treatment
Tumorshrinks
Tumordoes notshrink
Tumor
Tumor doesnot shrink
Individualizedtreatment tobe discussedwith doctor
More chemotherapyand hormone therapyif hormone receptorpresent or unknown,and trastuzumab iftumor is HER-2/neupositive (see follow-up on page 70)
Mastectomy and removal of underarmlymph nodes, radiation to the chest walland lymph nodes above the collarboneand perhaps internal nodes next tobreastbone, with or without delayedbreast reconstruction
OR
Possible lumpectomy or removal ofunderarm lymph nodes, radiation tothe breast and lymph nodes above thecollarbone and perhaps internal nodesnext to breastbone
Consider additionalchemotherapyand/or preoperativeradiation

• Mastectomy and removal of underarmlymph nodes. This is followed by radiation therapy to the chest wall, the lymph nodes above the collarbone,and, if they are enlarged, internal nodesnext to the sternum or breastbone.Breast reconstruction can be donelater if desired.
• Lumpectomy with removal of lymphnodes, if the cancer has shrunk enough,followed by radiation therapy to thebreast and the lymph nodes above thecollarbone, and, if they are enlarged,internal nodes next to the sternum orbreastbone.
• High dose radiation alone to the breastand usual dose radiation to the lymph
68
Treatment Guidelines for Patients
NOTES

NOTES
nodes. Among breast cancer specialists,this option is controversial.
For these patients the guidelines recom-mend adding more chemotherapy after surgery.If the cancer is hormone receptor positive orthe status is unknown, hormone therapy isrecommended. If the tumor is HER-2 positive,trastuzumab is also recommended.
Women with stage IIIA or IIIB breastcancer that doesn’t shrink with their firsttreatment can be treated with anotherchemotherapy regimen and/or radiation. Ifthe tumor shrinks, the patient can be treatedas outlined above. If the tumor does notshrink, the patient should discuss treatmentfor her specific situation with her doctor.
69
Stage III Locally Advanced Breast Cancers (continued)

Follow-up and Treatment of StageIV Disease or Recurrence of Disease Routine follow-up for all patients who have hadinvasive breast cancer includes the following:a medical history and physical exam every 4to 6 months for 5 years, then once a year.
Women who have had a lumpectomyshould have a mammogram of the treatedbreast 6 months after radiation therapy, andthen mammograms of both breasts every year.
Women who have had a mastectomyshould have a yearly mammogram of theremaining breast after the surgery. Becausetamoxifen increases a woman’s risk of devel-oping cancer of the uterus, women takingthis drug should have a yearly pelvic examand should promptly tell their doctor if thereis any abnormal bleeding from the vagina.Women on an aromatase inhibitor or whowent through early menopause on treatment
70
Treatment Guidelines for Patients
• History and physical exam every 4 to6 months for 5 years, then every year
• Mammograms every year. Forlumpectomy patients, the first oneshould be 6 months after radiation
• Women taking tamoxifen: pelvicexam every year if the uterus is present
• Women on aromatase inhibitor orwho have gone through earlymenopause with chemotherapyshould have bone density monitored.
• Medical history and physicalexamination
• Blood count, chemistry tests,and liver function tests
• Chest imaging
• Bone scan
• X-rays of bones that hurt andweight-bearing bones thatare abnormal on bone scan
• CT or MRI of chest andabdomen and/or PET scanmay be recommended
• Biopsy of suspected recurrence if possible
• ER/PR and HER-2/neu testingif not known, hormonereceptor previously negative,or HER-2/neu negative
Routine Follow-Up Work-Up for Stage IV orSuspected Recurrence

should have their bones tested for strengthusing a test called a bone mineral density test.
If there is a suspected recurrence or if thecancer had spread away from the breastwhen it was diagnosed, the work-up includes:
• complete medical history and physicalexamination
• blood counts and chemistry tests• liver function tests• chest imaging• bone scan
71
Follow-up and Treatment of Stage IV Disease or Recurrence of Disease
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
If possible, removecancer, followed byradiation therapy ifnone given before
Treatment of Recurrence
For patient initially treatedwith mastectomy
For patient initiallytreated withlumpectomy andradiation therapy
Mastectomy
Continuedon page 74
Local recurrence(cancer came backin breast, underarmlymph nodes, ornearby tissues)
Systemic recurrence or presenting with advancedcancer (Stage IV cancerspread to distant organs)

Weight-bearing bones that are painful orshowed abnormalities on the bone scanshould also be x-rayed, and CT or MRI scansof the abdomen, chest, or head should be
done if there are symptoms or blood testssuggesting a recurrence in these areas.Another option is a PET scan. A biopsy shouldbe done to confirm the first recurrence
72
Treatment Guidelines for Patients
NOTES

whenever possible. If HER-2/neu testingwas not done on the original cancer or wasnegative, it should be done on a new biopsy
specimen if possible. Likewise, if hormonereceptor tests were not done or were negative,testing for these should be done.
73
Follow-up and Treatment of Stage IV Disease or Recurrence of Disease (continued)
NOTES

A recurrence may be local, meaning thatcancer has returned to the area of the breast,underarm lymph nodes, or nearby tissue. Orit may be systemic, which means that cancerhas spread to distant organs. If the recurrenceis local and the woman has had a mastectomy,the recurrent cancer should be removed by
surgery (if possible). The area of the recur-rence and surrounding tissues should receiveradiation therapy, if it has not been givenbefore. If the cancer cannot be removed withsurgery, the woman should have radiationtherapy if it was not given before. In eithercase, the NCCN recommends considering
74
Treatment Guidelines for Patients
Postmenopausal
Premenopausal
Cancer containshormone receptorswith none or limited spread toorgans such asliver and lungs
Prior mastectomy
Prior lumpectomyor radiation
Cancer doesn’tcontain hormonereceptors, or doesnot respond tohormone therapy,or has spreadextensively tointernal organscausing symptoms
No antiestrogentherapy takenwithin last year
HER-2/neu positive
HER-2/neu negative
Recurrenceis local
Recurrence Site
Antiestrogentherapy takenwithin last year
Recurrence is systemic (distant)
OR
Stage IV (distantmetastasis) whenfirst diagnosed

chemotherapy, hormone therapy, ortrastuzumab. If the woman was first treatedwith lumpectomy and radiation and therecurrence is in the breast, a mastectomyshould be done, and then chemotherapy,hormone therapy, or trastuzumab therapyshould be considered.
If the recurrence is in areas outside thebreast or lymph nodes around the breast, orthe cancer is first diagnosed as stage IV, thetreatment options are based on whether or notthe tumor is hormone receptor positive andwhether the tumor has limited or extensivespread. Hormone therapy with or without
75
Follow-up and Treatment of Stage IV Disease or Recurrence of Disease (continued)
If no response to 3 differentchemotherapy regimens in a row
OR
Very weak and spending most oftime in bed
Treatment of Recurrence or Stage IV
Surgery to remove recurrence if possible,radiation if not given before
Mastectomy
Hormone treatment ortrastuzumab orchemotherapy may berecommended aftersurgery and radiation
Try different hormone therapy
Aromatase inhibitor or an antiestrogen
Ovarian ablation or suppression andeither aromatase inhibitor or antiestrogen
OR
Antiestrogen alone
Trastuzumab with orwithout chemotherapy Supportive
care focusedon relievingsymptoms
Chemotherapy
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.

ovarian ablation is appropriate for the fol-lowing patients:
• The tumor is hormone receptor positive; or
• There is spread only to the bones orsoft tissues; or
• The cancer has spread to other organssuch as the liver or lungs, but theorgans are still working well.
The specific treatment is based on what typeof treatment the patient has received before
and whether or not she is premenopausal orpostmenopausal. For example, if an anti-estrogen such as tamoxifen has been givenwithin the past year, then a different hormonetherapy should be offered. If the patient hasnot received an antiestrogen within the pastyear, the treatment options are based onwhether the patient is pre or postmenopausal.For postmenopausal women, an aromataseinhibitor or antiestrogen would be the firstchoice. Premenopausal women may betreated with an antiestrogen alone. Another
76
Treatment Guidelines for Patients
NOTES

treatment option for premenopausal womenis to block the ovaries from making estrogenand then use hormone therapy similar topostmenopausal patients. The ovaries maybe blocked with a medicine that decreasesestrogen production in the ovary, with radia-tion therapy to the ovary, or by surgicallyremoving the ovaries. If there is spread tobone, either pamidronate or zoledronic acid,along with calcium citrate and vitamin D,should be given to strengthen the bones.
In patients whose tumor is hormone-receptor negative, treatment options dependon whether or not the tumor is HER-2 posi-tive. If the tumor is HER-2 positive, thentrastuzumab may be given, either alone orcombined with chemotherapy. If the tumor isHER-2 negative, chemotherapy alone is rec-ommended. If the tumor does not shrink after3 different chemotherapy regimens, stoppingchemotherapy and providing supportive careto relieve symptoms should be considered.
77
Follow-up and Treatment of Stage IV Disease or Recurrence of Disease (continued)
NOTES

If the hormone therapy causes the cancerto shrink or at least not grow for a while, itwould be continued until the cancer beginsto grow. At that time another hormone treat-ment may be tried. The NCCN recommends
trying at least 3 different hormone treatmentsuntil there is no longer any benefit or thecancer has spread extensively to internalorgans with associated symptoms. At thatpoint chemotherapy is recommended.
78
Treatment Guidelines for Patients
Cancer shrinks oris stable for 6months or longer
If cancer growsor cancer invadesother organs, orside effects nottolerated
Cancer doesn’tshrink
Hormonetreatment
PrimaryTreatment
Response Treatment
Try different hormone therapy
Chemotherapy

Hormone therapy is not recommended in3 situations:
• When the tumor is hormone receptornegative; or
• When the tumor has not responded tothree prior hormone therapies; or
• When the tumor has spread extensivelyto organs such as the lungs or liver, andis causing the organs to not work well.
79
Response Treatment
If no benefit after 3 differenthormone regimens or extensive spread to internalorgans causing symptoms
Supportive care focusedon relieving symptoms
If no benefit after 3 differentchemotherapy regimens
OR
Very weak and spendingmost of time in bed
Chemotherapy
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Follow-up and Treatment of Stage IV Disease or Recurrence of Disease (continued)

Breast Cancer in Pregnancy Breast cancer sometimes occurs duringpregnancy. In this special situation, it is oftennecessary to try and find a treatment programthat helps the mother, but doesn’t hurt thefetus. This is not always possible.
The treatment recommendations dependupon how long the woman has been pregnant.Doctors divide pregnancy into the first 3
months ( first trimester), second 3 months(second trimester), and third 3 months (thirdtrimester). Women who are diagnosed withbreast cancer during the first trimestershould consider the option of having thepregnancy terminated. This is because theuse of drug treatments during the early partof pregnancy may cause damage to the fetus.In general, the treatment options for women
80
Treatment Guidelines for Patients
1st trimester
2nd trimesteror early 3rdtrimester
Discusspregnancytermination
OR
Late 3rdtrimester
Pregnantpatient withbreast cancerand no distantspread
ClinicalPresentation
Primary Treatment
Mastectomy and axillarylymph node dissection
Mastectomy or lumpectomy andaxillary lymph node dissection
Preoperative chemotherapy followedby mastectomy or lumpectomy withaxillary node dissection
Mastectomy or lumpectomy andaxillary lymph node dissection

who are pregnant are similar to those recom-mended in non-pregnant woman except thatchemotherapy should not be given during thefirst trimester of pregnancy, some chemother-apies (such as methotrexate) need to beavoided, and radiation therapy should not beadministered at any point during pregnancy.For this reason, the radiation therapy that is
part of breast-conserving therapy must bepostponed until after the patient has givenbirth. Hormone therapy should not bestarted until after the patient has given birth.
It is important that the cancer doctors ofa woman who have breast cancer while preg-nant communicate and work closely with thewoman’s obstetrician.
81
Adjuvant Treatment
Begin with adjuvant chemotherapy in 2nd trimester,with or without adjuvant radiation after birth, withor without adjuvant hormone therapy after birth
Adjuvant chemotherapy, with or withoutadjuvant radiation after birth, with or withoutadjuvant hormone therapy after birth
Adjuvant chemotherapy, with or withoutadjuvant radiation after birth, with or withoutadjuvant hormone therapy after birth
Possible adjuvant radiation after birth, with orwithout adjuvant hormone therapy after birth
©2006 by the National Comprehensive Cancer Network (NCCN) and theAmerican Cancer Society (ACS). All rights reserved. The information hereinmay not be reproduced in any form for commercial purposes without theexpressed written permission of the NCCN and the ACS. Single copies of eachpage may be reproduced for personal and non-commercial uses by the reader.
Breast Cancer in Pregnancy

82
Adjuvant therapyTreatment that is added to increase the effec-tiveness of a primary therapy. It usually refersto hormonal therapy, chemotherapy, or radi-ation therapy added after surgery to kill anyremaining cancer cells and increase thechances of curing the disease or keeping it incheck.
AntiestrogenA substance that blocks the effects of estrogenon tumors ( for example, the drug tamoxifen).Antiestrogens are used to treat breast cancersthat depend on estrogen for growth.
Aromatase inhibitorsDrugs that block production of estrogensfrom hormones made by the adrenal gland.They are used to treat hormone-sensitivebreast cancer in postmenopausal women.Examples are anastrozole, letrozole, andexemestane.
Axillary lymph node dissectionA surgical procedure in which the lymphnodes in the armpit (axillary nodes) areremoved and examined to find out if breastcancer has spread to those nodes. This is alsodone to remove any cancerous lymph nodes.
BiopsyThe removal of a sample of tissue to seewhether cancer cells are present.
BisphosphonatesDrugs that help strengthen bones weakenedby cancer by encouraging the deposition of
calcium. These include pamidronate andzoledronate.
Breast-conserving treatment or therapySurgery to remove a breast cancer and a smallamount of benign tissue around the cancer,without removing any other part of the breast.This procedure is also called lumpectomy,segmental excision, or limited breast surgery.The method may require an axillary dissectionand usually requires radiation therapy afterthe surgery.
Breast reconstructionSurgery that rebuilds the breast contour aftermastectomy. A breast implant or the woman’sown tissue provides the contour. If desired,the nipple and areola may also be re-created.Reconstruction can be done at same time asthe mastectomy or any time later.
Carcinoma in situAn early stage of cancer, in which the tumoris still only in the structures of the organwhere it first developed—the disease doesnot invade other parts of the organ or spreadto distant sites. Most in situ carcinomas arehighly curable.
ChemotherapyTreatment with drugs to destroy cancer cells.Chemotherapy is often used in addition tosurgery or radiation to treat cancer whenspread (metastasis) is proven or suspected,when the cancer has come back (recurred),or when there is a strong likelihood that thecancer could recur.
Glossary

Clinical stageStage includes evaluation of the size andextent of the cancer, the presence or absenceof spread to lymph nodes, and the presenceor absence of spread to other body organs.Clinical stage is the stage determined only byphysical examination and x-ray or otherimaging studies. This includes determinationof the size of the cancer and evaluation oflymph nodes by the doctor’s examination ofthe armpit. The final stage is the pathologicalstage which is determined from microscopicexamination of the tumor and lymph nodes.Clinical stage is used for initial treatmentplanning.
Clinical trialResearch studies test new drugs or treatmentsand compare them to current, standardtreatments. Before a new treatment is used onpeople, it is studied in the lab. If lab studiessuggest the treatment works, it is tested forpatients. These human studies are calledclinical trials.
CystA fluid-filled mass that is usually not cancer(benign). The fluid can be removed for testing.
Diagnostic mammogramScreening mammograms are performed onwomen with no evidence of lumps or othersymptoms. This includes 2 x-ray views of eachbreast (top to bottom; side-to-side). Diagnosticmammograms include additional x-ray viewsof areas of concern ( found on physical exam-ination or on the screening mammogram) toprovide more information about the size andcharacter of the abnormality.
DuctA hollow passage for gland secretions. In thebreast, a passage through which milk passesfrom the lobule (which makes the milk) to thenipple. These ducts are the starting point formost breast cancers.
Ductal carcinoma in situThe most common type of non-invasivebreast cancer. Cancer cells have not spreadbeyond the ducts.
EstrogenA female sex hormone produced primarily bythe ovaries, and in smaller amounts fromhormones produced by the adrenal glandand fat cells. In breast cancer, estrogen mayhelp the growth of breast cancer cells.
FibroadenomaA type of benign breast tumor made offibrous tissue and glandular tissue. On clinicalexamination or breast self-examination, itusually feels like a firm, round, smooth lump.These usually occur in young women.
Fibrocystic changesA term that describes certain benign changesin the breast; also called fibrocystic disease.Symptoms of this condition are breastswelling or pain. The breasts often feel lumpy ornodular. Because these signs sometimes mimicbreast cancer, a diagnostic mammogram,ultrasound, or even a biopsy may be neededto show that there is no cancer.
FibrosisFormation of fibrous (scar-like) tissue. Thiscan occur anywhere in the body.
83

FulvestrantA drug that reduces the number of estrogenreceptors.
GradeCancer cells are graded by how much theylook like normal cells. Grade 1 (also calledwell-differentiated) means the cancer cellslook like the normal cells. Grade 3 (poorlydifferentiated) cancer cells do not look likenormal cells at all. Grade 1 cancers aren’tconsidered aggressive. In other words, theytend to grow more slowly and metastasizeslower. Grade 3 cancers are more likely togrow fast and metastasize. A cancer’s grade,along with its stage, is used to determinetreatment.
HER-2/neuA gene that produces a type of receptor thathelps cells grow. Breast cancer cells with toomany HER-2/neu receptors tend to be fast-growing and may respond to treatment witha monoclonal antibody called trastuzumab.
HistologyThe way the cancer cells look under themicroscope (described as type and arrange-ment of tumor cells).
HormoneA chemical substance released into the bodyby glands, such as the thyroid, pituitary, orovaries. The substance travels through thebloodstream and sets in motion various bodyfunctions. For example, prolactin, which isproduced in the pituitary gland, begins andsustains the production of milk in the breastafter childbirth.
Hormone receptorThese are the cells’ “welcome mat” for hor-mones circulating in the blood. The receptor isa protein located on a cell’s surface (or withinthe cell cytoplasm) that binds to a hormone.Tumors can be tested for hormone receptorsto see if they can be treated with hormonesor anti-hormones. See also, hormone receptorassay.
Hormone receptor assayA test to see whether a breast tumor has hor-mone receptors and is affected by hormonesor can be treated with hormones.
Hormone therapyCan be treatment with hormones, treatmentwith drugs that interfere with hormone pro-duction or hormone action, or surgical removalof hormone-producing glands to kill cancercells or slow their growth. The most commonhormone therapy for breast cancer is the drugtamoxifen. Other hormonal therapies includearomatase inhibitors, androgens and surgicalremoval of the ovaries (oophorectomy).
In situCancer in situ is localized in its original placeand confined to one area. This describes avery early stage of cancer.
Internal mammary lymph nodesLymph nodes located inside the chest, nextto where the sternum (breastbone) and theribs come together.
Intraductal papillomasSmall, finger-like, polyp-like, non-cancerousgrowths in the breast ducts that may cause abloody nipple discharge. These are most oftenfound in women 45 to 50 years of age. When
84

many papillomas exist, breast cancer risk isslightly increased.
LHRH (luteinizing hormone-releasinghormone) agonists or antagonistsDrugs that block the ovaries from producingestrogen.
Lobular carcinoma in situAlso called lobular neoplasia. Non-invasivecancer that has not spread beyond the lobules.The lobules are the milk-producing parts ofthe breast at the distant end of the ducts.
LumpectomySurgery to remove the breast tumor and asmall amount of surrounding normal tissue.
Lymph nodesSmall, bean-shaped collections of immunesystem tissue located along lymphatic vessels.They remove waste and fluids from lymph andhelp fight infections. Also called lymph glands.
LymphedemaA possible complication after breast cancertreatment. Swelling in the arm is caused byexcess fluid that collects after lymph nodesand vessels are removed by surgery or treatedwith radiation.
Magnetic resonance imaging (MRI)A method of taking pictures of the inside ofthe body. Instead of using x-rays, MRI uses apowerful magnet and transmits radio wavesthrough the body; the images appear on acomputer screen and on film.
MarginThe edge of the tissue removed during surgery.A negative margin is a sign that no cancerwas left behind. A positive margin indicatesthat cancer cells are found at the outer edge
of tissue removed and is usually a sign thatsome cancer remains in the body.
MastectomyRemoval of the entire breast. In a simple ortotal mastectomy surgeons do not cut awayany lymph nodes or muscle tissue; in a modi-fied radical mastectomy, surgeons remove thebreast and some armpit lymph nodes; in aradical mastectomy (now rarely performed)surgeons remove the breast, armpit lymphnodes, and chest wall muscles under thebreast.
MenopauseThe time in a woman’s life when monthlycycles of menstruation stop forever and thelevel of hormones produced by the ovariesdecreases. Menopause usually naturally occursin a woman’s late 40s or early 50s, but it canalso be caused by surgical removal of bothovaries (oophorectomy), or by chemotherapy,which often destroys ovarian function.
MetastasisThe spread of cancer cells to distant areas ofthe body by way of the lymph system orbloodstream.
Monoclonal antibody therapyMonoclonal antibodies (MABs) are made inthe lab and designed to target specific sub-stances called antigens. MABs which havebeen attached to chemotherapy drugs orradioactive substances are being studied tosee if they can seek out antigens unique tocancer cells and deliver these treatmentsdirectly to the cancer, thus killing the cancercells without harming healthy tissue.Trastuzumab is the MAB used to treat HER-2positive breast cancers.
85

Neoadjuvant treatmentUsed to describe systemic therapy, such aschemotherapy or hormone therapy, givenbefore surgery. This type of therapy can shrinksome tumors, so that they are easier to remove.
Nodal statusIndicates whether a breast cancer has spread(node-positive) or has not spread (node-nega-tive) to lymph nodes in the armpit (axillarynodes). The number and site of positive lymphnodes can help predict the risk of cancerrecurrence.
OophorectomySurgery to remove the ovaries.
OvaryReproductive organ in the female pelvis.Normally a woman has two ovaries. Theycontain the eggs (ova) that, when joined withsperm, result in pregnancy. Ovaries producemost of a premenopausal woman’s estrogen.
PalpationUsing the hands to examine. A palpable massin the breast is one that can be felt.
Partial mastectomyA type of breast-conserving surgery thatremoves more breast tissue than a lumpec-tomy (up to one-quarter of the breast). It isalso called a segmental mastectomy or aquadrantectomy.
Pathologic stageIncludes the findings of the pathologist aftersurgery. Most of the time, pathologic stage isthe most important stage since involvementof the lymph nodes can only be accuratelyevaluated by examining them under a micro-scope.
PET (positron emission tomography) scanA total body scan that uses a radioactive formof glucose to detect cancer.
Preoperative chemotherapyChemotherapy given before surgery to shrinksome breast tumors, so they can be removedwith less extensive surgery than would other-wise be needed. Also called neoadjuvantchemotherapy.
ProgesteroneA female sex hormone released by the ovariesduring every menstrual cycle to prepare theuterus for pregnancy and the breasts for milkproduction (lactation).
PrognosisA prediction of the course of disease—or theoutlook for the cure of the patient. For exam-ple, women with breast cancer that is small,does not involve the lymph nodes, and ispromptly treated have a good prognosis.
QuadrantectomyA type of breast-conserving surgery thatremoves more breast tissue than a lumpec-tomy (up to one-quarter of the breast). It isalso called a partial or segmental mastectomy.
RadiationTreatment with high-energy rays (or particles)to kill or shrink cancer cells. The radiationmay come from outside of the body (externalradiation) or from radioactive materialsplaced directly in the tumor (internal orimplant radiation called brachytherapy).Radiation therapy may be used to reduce thesize of a cancer before surgery, to destroy anycancer cells left behind after surgery, or, insome cases, as the main treatment.
86

Segmental mastectomyA type of breast-conserving surgery thatremoves more breast tissue than a lumpectomy(up to one-quarter of the breast). It is also calleda partial mastectomy or a quadrantectomy.
Sentinel node mapping and biopsyIn a sentinel lymph node mapping and biopsy,the surgeon injects a radioactive substanceand/or a blue dye into the area around thetumor. Lymphatic vessels carry these materialsto the sentinel lymph node (also called thesentinel node). The doctor can see the bluedye or detect the radioactivity (with a Geigercounter) in the sentinel node, which is cut outand examined. If the sentinel node containscancer, more axillary lymph nodes areremoved. But if it is free of cancer, the patientcan avoid additional axillary surgery and itspotential side effects.
Side effectsUnwanted effects of treatment, such as hairloss caused by chemotherapy or fatiguecaused by radiation therapy.
SonogramDuring an ultrasound the computer trans-forms the echoes into a picture called asonogram. See ultrasound.
StageA method of describing the size and locationof cancer based upon characteristics of thetumor, the lymph nodes, and whether there isinvolvement of other organs.
Stereotactic needle biopsyA method of needle biopsy that is useful insome cases in which calcifications or a masscan be seen on mammogram, but cannot be
located by touch. Computerized equipmentmaps the location of the mass and this isused as a guide to place the needle.
Supportive careMeasures taken to relieve symptoms andimprove quality of life, but that are notexpected to destroy the cancer. Pain medica-tion is an example of supportive care.
Supraclavicular lymph nodesLymph nodes located in the area just abovethe collarbone.
Systemic therapyTreatment that reaches and affects cellsthroughout the body; for example, chemo-therapy.
TamoxifenThis antiestrogen drug blocks the effects ofestrogen on many organs, such as the breast.Blocking estrogen is desirable in some casesof breast cancer because estrogen promotestheir growth. Recent research suggests thattamoxifen may lower the risk of developingbreast cancer in women with certain riskfactors.
ToremifeneAnother antiestrogen drug, similar to tamoxifen.
UltrasoundHigh frequency sound waves used to produceimages of the breast. See sonogram.
For a more comprehensive glossary, you mayvisit the American Cancer Society Web site atwww.cancer.org
87

88
NOTES

The Breast Cancer Treatment Guidelines for Patients were developed by a diverse group ofexperts and were based on the NCCN clinical practice guidelines. These patient guidelines weretranslated, reviewed, and published with help from the following individuals:
Terri Ades, MS, APRN-BC, AOCNAmerican Cancer Society
Elizabeth Brown, MDNational ComprehensiveCancer Network
Dorothy Shead, MSNational Comprehensive Cancer Network
Kimberly Stump-Sutliff, MS, RNAmerican Cancer Society
Joan McClure, MSNational Comprehensive Cancer Network
The original NCCN Breast Cancer Clinical Practice Guidelines were developed by the following NCCN Panel Members:
Robert W. Carlson, MD/Chair Stanford Hospital and Clinics
Benjamin O. Anderson, MD Fred Hutchinson Cancer Research Center/Seattle Cancer Care Alliance
Harold J. Burstein, MD, PhD Dana-Farber/Partners CancerCare
W. Bradford Carter, MD H. Lee Moffitt Cancer Center &Research Institute at the Universityof South Florida
Stephen B. Edge, MD Roswell Park Cancer Institute
William B. Farrar, MD Arthur G. James Cancer Hospital &RichardJ. Solove Research Instituteat The Ohio State University
Lori J. Goldstein, MD Fox Chase Cancer Center
William J. Gradishar, MD Robert H. Lurie ComprehensiveCancer Center of NorthwesternUniversity
Elizabeth C. Reed, MD UNMC Eppley Cancer Center at The Nebraska Medical Center
Samuel M. Silver, MD, PhD University of MichiganComprehensive Cancer Center
Mary Lou Smith, JD, MBA Consultant
George Somlo, MD City of Hope Cancer Center
Richard Theriault, DO, MBA The University of Texas M. D. Anderson Cancer Center
John H. Ward, MD Huntsman Cancer Institute at the University of Utah
Eric P. Winer, MD Dana-Farber/Partners CancerCare
Antonio C. Wolff, MD The Sidney Kimmel ComprehensiveCancer Center at Johns HopkinsUniversity
Daniel F. Hayes, MD University of MichiganComprehensive Cancer Center
Clifford Hudis, MD Memorial Sloan-Kettering Cancer Center
Mohammad Jahanzeb, MD St. Jude Children’s ResearchHospital/University of TennesseeCancer Institute
Britt-Marie Ljung, MD UCSF Comprehensive Cancer Center
Lawrence B. Marks, MD Duke Comprehensive Cancer Center
Beryl McCormick, MD Memorial Sloan-Kettering Cancer Center
Lisle M. Nabell, MD University of Alabama at BirminghamComprehensive Cancer Center
Lori J. Pierce, MD University of MichiganComprehensive Cancer Center

©2006, American Cancer Society, Inc.No.940508
Reading Grade Level: 10th
1.800.ACS.2345www.cancer.org
1.888.909.NCCNwww.nccn.org