Myra Lalas Pitt Cardiomyopathy. Hypertrophic Cardiomyopathy Cardiomyopathy with hypertrophy of the...
20
Myra Lalas Pitt Cardiomyopathy
-
Upload
lynne-stokes -
Category
Documents
-
view
215 -
download
0
Transcript of Myra Lalas Pitt Cardiomyopathy. Hypertrophic Cardiomyopathy Cardiomyopathy with hypertrophy of the...

Myra Lalas Pitt
Cardiomyopathy

Hypertrophic CardiomyopathyCardiomyopathy with hypertrophy of the LV
(± RV) with histological features of myocyte hypertrophy, myofibrillar disarray, and interstitial fibrosis.
The prevalence in young adults is approximately one in 500.
Frequent cause of sudden death, particularly in young individuals and competitive athletes.
Usually AD- the genes affected code for proteins in the sarcomere
Associated with Pompe Disease

Signs and SymptomsSystolic function is preserved; may have
increased contractility; symptoms are typically caused by diastolic dysfunction (impaired ventricular relaxation) and sometimes LVOT obstruction.
May be asymptomatic Palpitationss, dizziness, syncope, sudden
death.Age of symptom onset: from birth to middle
age

TreatmentBeta-blockers : mainstays of therapy. Combination therapy (Beta-blocker and
CCB) may be considered in patients with severe hypertrophy and severe outflow obstruction.
LVOTO myectomy: Children with severe LVOTO.

Dilated CardiomyopathyCardiomyopathy with increased ventricular size
and reduced contractility in the absence of coronary, valvar, or pericardial disease.
Highest rate of disease in newborns and infants.
M> F1-yr mortality is about 50% without cardiac
transplantation.Genetics: 1/3 have familial form, AD (most
common is cytoskeletal protein involvement), X-linked (typically occurs in boys with rapid progression; elevated CK-MM)
Signs and SymptomsShortness of breath, fatigue, orthopnea,
diaphoresis, chest pain, palpitations, exercise intolerance, syncope.
Tachypnea, tachycardia, diaphoresis, S3 or S4 gallop, holosystolic murmur (MR), hepatomegaly, ± ascites or peripheral edema.


TreatmentOutpatient ManagementACE inhibitors and beta-
blockers (metoprolol/carvedilol): Mainstays of therapy
Diuretics: May be useful for symptomatic edema; no proven long-term benefit
Digoxin: Now used less often, but may improve symptoms in some patients
Inpatient ManagementInotropic medications avoided
whenever possible; reserved for compromised hemodynamic states (milrinone ± low-dose dopamine)
Diuretics: Decrease pulmonary edema acutely; may improve preload in volume overload states
Mechanical circulatory support: Ventricular assist devices and ECMO for those who fail medical management as a bridge to recovery or transplantation
Cardiac transplantation

Restrictive CardiomyopathyDefinition: Cardiomyopathy with abnormal
stiffness of the ventricular wall leading to impaired ventricular filling.
Rare type of cardiomyopathyHas the worst outcome of all forms of
cardiomyopathy (especially in children)Sudden death occurs within 2 to 5 years of
diagnosis in more than 50% of patients.Genetics: inherited in <10% of patients,
usually AD

Signs and Symptoms
CHF (dyspnea, orthopnea, and abdominal pain), syncope, or sudden death.
S4; holosystolic murmur of AV valve insufficiency if the patient has pulmonary hypertension, hepatomegaly.


TreatmentHeart transplantation is the only definitive
therapy and is often recommended as primary therapy.
May use antiarhythmics.In general, meds may cause acute
hemodynamic changes and are usually not effective.

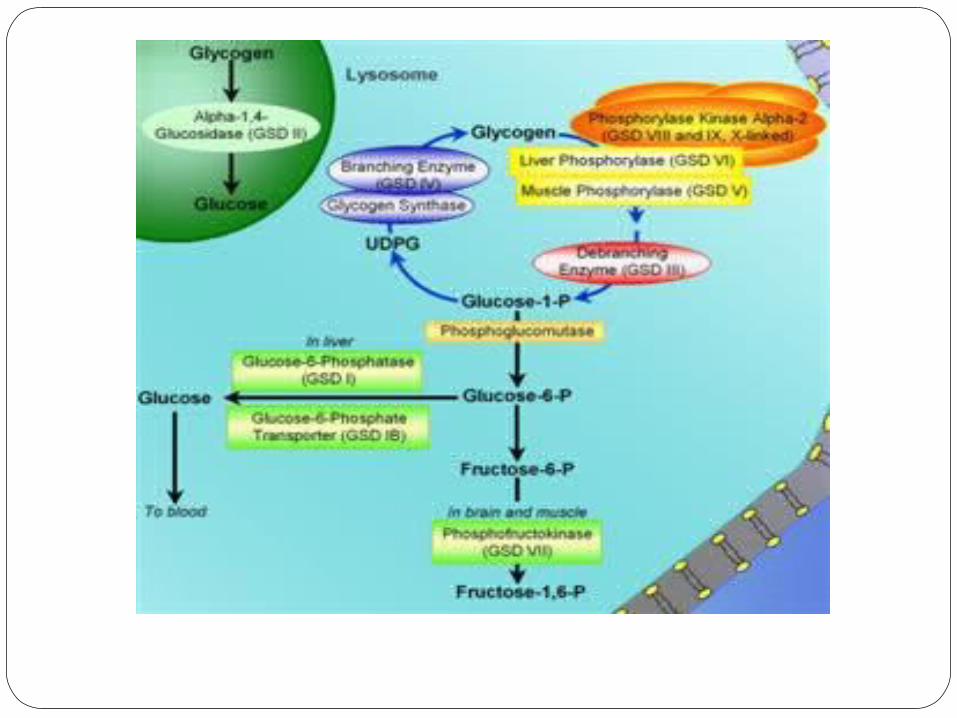
Glycogen Storage DiseaseInheritance: AR (except some forms of
type VI and IX X-linked).Clinical presentation: Pathologic
glycogen storage (eg, hepatomegaly) or organ dysfunction (eg, muscle weakness, muscular atrophy, cardiomyopathy, renal tubulopathy) or hypoglycemia.
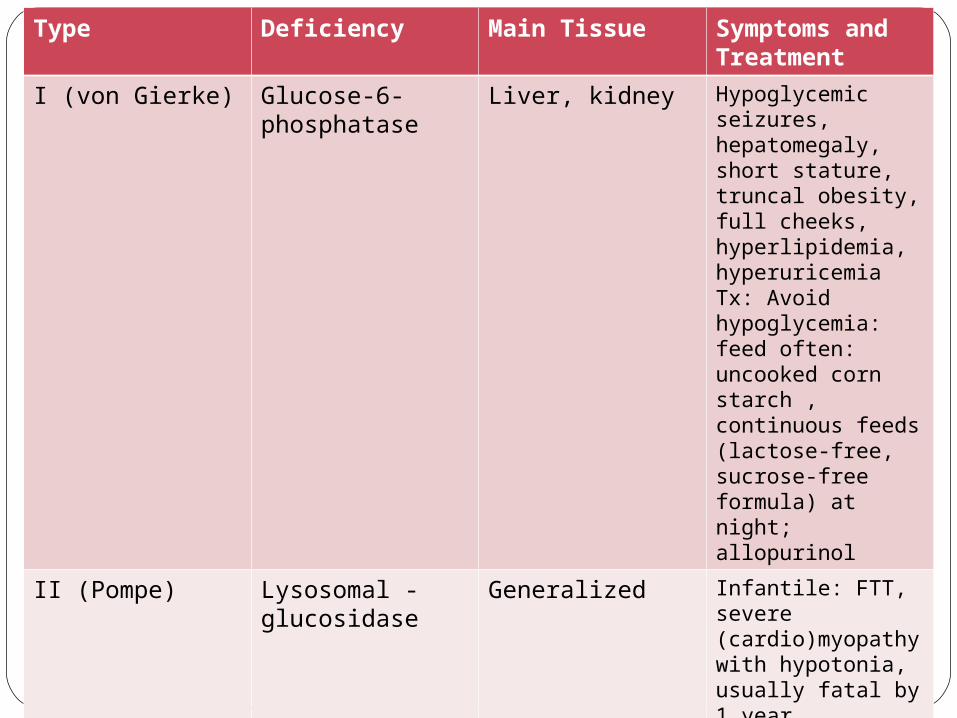
Type Deficiency Main Tissue Symptoms and Treatment
I (von Gierke) Glucose-6-phosphatase
Liver, kidney Hypoglycemic seizures, hepatomegaly, short stature, truncal obesity, full cheeks, hyperlipidemia, hyperuricemiaTx: Avoid hypoglycemia: feed often: uncooked corn starch , continuous feeds (lactose-free, sucrose-free formula) at night; allopurinol
II (Pompe) Lysosomal -glucosidase
Generalized Infantile: FTT, severe (cardio)myopathy with hypotonia, usually fatal by 1 yearJuvenile or adult: Progressive muscular weakness with minimal or absent cardiac involvementTx: IV enzyme replacement Q2wk

Type Deficiency Main Tissue Symptoms and Treatment
III (Cori/ Forbes) Debranching enzyme
Liver, muscle Hepatomegaly, (cardio)myopathy, short stature, hypoglycemiaTx: Frequent PO feeding to maintain normoglycemia
V (McArdle*) Myophosphorylase
Muscle Myalgia, muscle cramps, exercise intolerance, muscular weakness.Tx: Encourage moderate aerobic exercise, oral sucrose before exercise, ± creatinine, vitamin B6 supplementation

PREP QuestionYou are evaluating a 12-year-old boy who has been
fatigued for 2 weeks. His mother reports that he had an upper respiratory tract infection 2 weeks ago, and his appetite has been decreased since then. On physical examination, he is afebrile and has a heart rate at rest of 110 beats/min. His respiratory rate is 22 breaths/min. His lungs are clear, and he has a gallop rhythm without murmurs on cardiac auscultation. You discern hepatomegaly and mild jugular venous distention.
Of the following, the MOST likely diagnosis isa. anemiab. dilated cardiomyopathyc. Kawasaki diseased. primary pulmonary hypertensione. pulmonary embolism

Answer: BThe gallop rhythm, hepatomegaly, and jugular venous
distention described for the boy in the vignette support the diagnosis of congestive heart failure (CHF), most likely due to myocardial dysfunction associated with dilated cardiomyopathy.
Laboratory support for the myocardial failure seen in patients who have CHF can be demonstrated by an elevation in the brain natriuretic peptide value. Results of this test almost always are abnormal in patients who have significant CHF.
Among the many causes of CHF are large-volume left-to-right shunts with pulmonary overcirculation, pressure load on the myocardium, inadequate blood flow to the myocardium, infection or infiltration of the myocardium, or genetic or idiopathic diseases of the myocardium.
ReferencesLowry AW, Bhakta KY, Nag PK, "Chapter 8. Cardiology" (Chapter). Lowry AW, Bhakta
KY, Nag PK: Texas Children's Hospital Handbook of Pediatrics and Neonatology:http://www.accesspediatrics.com/content/7434509.
Lowry AW, Bhakta KY, Nag PK, "Chapter 17. Genetics" (Chapter). Lowry AW, Bhakta KY, Nag PK: Texas Children's Hospital Handbook of Pediatrics and Neonatology:http://www.accesspediatrics.com/content/7439230.
www.uptodate.com