Myocardial Ischemia Redefined: Optimal Care in CAD
12
Myocardial Ischemia Redefined: Optimal Care in CAD
description
Myocardial Ischemia Redefined: Optimal Care in CAD. Learning objectives. To improve patient management through a better understanding of:. Pathophysiology of myocardial ischemia Efficacy and safety of behavioral and pharmacologic approaches to minimize recurring ischemic episodes - PowerPoint PPT Presentation
Transcript of Myocardial Ischemia Redefined: Optimal Care in CAD

Myocardial Ischemia Redefined:Optimal Care in CAD

Learning objectives
To improve patient management through a better understanding of:
• Pathophysiology of myocardial ischemia
• Efficacy and safety of behavioral and pharmacologic approaches to minimize recurring ischemic episodes
• Clinical trials investigating multiple treatment targets
• Current clinical guidelines

Curriculum overview
• Epidemiology and prevalence of myocardial ischemia– Magnitude of the problem– Challenges in selected populations
• Issues in contemporary clinical practice
• Scientific review
• Clinical trial update
• New guidelines in myocardial ischemia management
• Risk stratification

Chronic ischemic heart disease: Overview
• Highly prevalent– 6.5-16.5 million in the US
• Multifactorial etiology– CAD, hypertension, hypertrophic cardiomyopathy, valvular heart
disease
• High socioeconomic burden– Depression– ↓Quality of life– High costs of care
Gibbons RJ et al. www.acc.org.

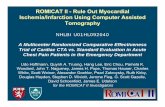
Repeat revascularization is common post-PCI/CABG
Kempf J et al. Presented at ESC. 2007.
N = 18,240 who underwent elective PCI or CABG
46
30
0
10
20
Patients(%)
Recurrentangina
2nd revascularization
30
40
50

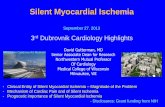
Angina increases cost of care
0
10
20
30
40
50
Patients (%)
Asymptomatic CAD Angina
Prior to diagnosis Following diagnosis
ED visits HospitalizationsED visits
Kempf J et al. Presented at Scientific Forum on Quality of Care and Outcomes Res in CV Disease. 2006.
US managed care enrollees, n = 140,001 with asymptomatic CAD, n = 23,535 with angina Dx*
Average yearly cost/patient
$11,530 (asymptomatic CAD)
vs $22,004 (angina)
*And Rx nitrates and/or β-blockers and/or CCBs

Challenges in selected populations: Pathophysiology and implications of ischemic heart disease in women
Women
Elderly Diabetes
Ischemic heart
disease

WISE: Landmark study in women
Goals:
• Improve diagnostic testing for ischemic heart disease in women
• Study pathophysiologic mechanisms for ischemia in the absence of epicardial coronary artery stenoses
• Evaluate the influence of menopausal status and reproductive hormone levels on diagnostic testing results
Bairey Merz CN et al. J Am Coll Cardiol. 1999;33:1453-61.Women’s Ischemia Syndrome Evaluation
Prospective cohort study conducted at 4 US sites

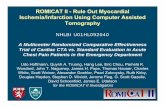
WISE: Persistent chest pain in women predicts future CV events
Johnson BD et al. Eur Heart J. 2006;27:1408-15.
With CADHR 1.17 (0.76–1.80)P = 0.49
Without CADHR 1.89 (1.06–3.39)P = 0.03
Event-freesurvival
(%)
Years from PChP diagnosis (at one year)
0.7
0.6
1
0.9
0.8
0 1 2 3 4 5 6
Neither PChPNo CAD
No PChPCAD
Both
n = 673 WISE participants with chest pain at baseline
PChP = persistent chest pain

WISE: Persistent chest pain associated with diminished QOL
No obstructive CAD Obstructive CAD
No PChP PChPNo
PChP PChP
Angina symptoms
Typical presentation (%) 30 33 32 40
Intensity (range 1-5) 2.3 2.6* 2.6 2.6
Daily frequency (%) 30 49* 34 39*
Psychological symptoms
Perceived QOL† 7.3 6.6* 7.1 6.6
Depression‡ 8.8 12.2* 9.3 12.9*
Anxiety‡ 18.0 20.1* 17.7 20.1
*Adjusted P ≤ 0.04†Range: 1 - 10 (best); ‡score = trait
Johnson BD et al. Eur Heart J. 2006;27:1408-15. Bairey Merz CN et al. J Am Coll Cardiol. 1999;33:1453-61.

*
** * *
WISE: CAD imposes an economic burden
Shaw LJ et al. Circulation. 2006;114:894-904.
N = 883 women with angiographic CAD
80
70
60
50
40
30
20
10
0
Cumulative observed
direct costs ($, thousands)
Nonobstructive CAD
2 3 4 5
1 vessel CAD 2 vessel CAD 3 vessel CAD
Follow-up (years)
1
*P < 0.0001 nonobstructive vs 1-3 vessel CAD

Contemporary clinical practice of ischemic heart disease
Adapted from Timmis AD et al. Heart. 2007;93:786-91.
Angiogram
Cardiologist referral
Treatment(Angina, risk factors)
Risk stratification(Stress test, CT angio)
Presentation to PCP
Incident angina
Visible
Submerged
Revas
Healthy population
Opportunity for early detection, risk stratification, and medical therapy
Revas = revascularization