Myasthenia Gravis Erin O’Ferrall Colin Chalk March 11, 2009.
42
Myasthenia Gravis Erin O’Ferrall Colin Chalk March 11, 2009
-
Upload
amberlynn-price -
Category
Documents
-
view
216 -
download
1
Transcript of Myasthenia Gravis Erin O’Ferrall Colin Chalk March 11, 2009.

Myasthenia Gravis
Erin O’Ferrall
Colin Chalk
March 11, 2009

Objectives
To identify key features of the history & physical exam of a patient with Myasthenia Gravis (MG)
To learn how to elicit a history of fatigable weakness
Learn what investigations to order if you suspect a diagnosis of MG
Describe what are MUSK antibodies and their significance
Discuss the potential therapies and evidence for each
To describe the approach and management to refractory MG
To describe the role of thymectomy

Outline
Case
History & Physical exam
Investigations
Treatment
Case

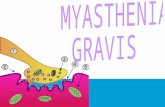
Neuromuscular Junction (NMJ)

Case 1
57yr old female with 3 month history of fatigue, ptosis, dysphagia

Clinical Course of MG
Current estimates of prevalence? ~20 in 100 000

Bimodal Distribution

History
What are the presenting symptoms of MG?
Ocular (ptosis, diplopia) 45-50%
Bulbar (dysarthria, dysphagia) 20%
Extremity weakness (usually proximal) 30-35%
Distal extremity -rare
Respiratory -rare

History: General
Key:
Elicit a history of fatigable weaknessDifferentiate from generalized weakness or fatigue: affects the specific muscle group being used
Ask about repetitive activities: talking on the phone, chewing
Recovery with rest...How to you feel first thing in the morning?
Does your weakness ever get better after a nap or a rest?

Diplopia:Worse with prolonged reading, watching TV, driving
Ptosis: Droopy eyelidsDo you ever have to hold (or tape) your eye open?Compensatory frontalis contraction can give you a headacheWorse with bright lightsMay wear sunglasses (also to hide droopy eyes)
Dysarthria:Nasal quality; breathy, hoarseWith long conversations or presentations or singingDo you avoid talking on the phone? Or only make calls in the morning?
Facial weakness: sleepy or sad appearanceDysphagia:
“food gets stuck”
SOB:Worse supine

History: for follow-ups...
ExacerbationsTriggers
medicationsInfectionsHeat/ fever, stress, menstrual cycle/ pregnancy, Hyperthyroidism
For known MG patientsMedication effects & side effectsPyridostigmine: onset, offset or missed dose effects
Can have fixed weakness with atrophy (late or MUSK)

Physical Exam: fatigability
Rowin, Julie CONTINUUM: Lifelong Learning in Neurology Volume 15(1) Myasthenic Disorders and ALS February 2009 pp 13-34
Can also use to assess SOB

Physical Exam
PtosisDescribe (%complete, mm below upper pupil margin)
Compensation: head tilt, frontalis contraction
Worse with upgaze; better with rest/ cooling
Curtain sign aka enhanced ptosis or paradoxical ptosis
Lid twitch sign

Physical Exam: what do you see here?
(the patient was asked to smile)

Questions
Can the weakness be focal?One-sided ptosis
Foot drop
Even single digit weakness for finger extn
Isolated head drop
Can the weakness be limited to dysphagia or respiratory muscles only?
How many remain restricted to EOM?When will you know?

Investigations
What tests would you order?AntibodiesTensilon & Ice Pack testEMG/ NCS: what should you ask for?
Repetitive stimulationSingle fiber EMG (SFEMG)
CT chest

AchR Abs in MG?
Anti-AChR antibody is positive in what percentage of generalized & ocular MG?
85-90% of generalized adult MG patients
50% of childhood MG
50-70% of Ocular MG
MUSKIn >40% of patients with no Ach Abs
“Seronegative”

Are Ach Abs pathogenic?
Give three mechanisms:Block AchR
Complement mediated lysis of endplate
Accelerated degradation of cross-linked AchRs

MuSKreceptor tyrosine kinase in muscle; IgGIn general MG: 30-70% of AChR negative MG patients (Pestronk); 40-50% (Bradley 5th Ed) Compared to AChR Ab patients, Patients with Musk antibodies are:
Slightly younger on average but can occur at any ageMore femalesSimilar clinical presentation to MG with AChR OR have atypical presentations
atrophy (ex: tongue)Respiratory weakness
May be more difficult to treat and have permanent weaknessLess response to AchEI
Very rare to have thymoma; effect of thymectomy =uncertainUsually NOT seen with pure ocular MG (1 case report)Usually NOT seen in patients with AChR positivity (1 case report)


Agrin, released by motor neurons, induces clustering of AChR’s, by interacting with MuSK on myotube membranes.

Seronegative MG
Is there such thing as seronegative MG?
In one study, 66% of “seronegative” MG patients were found to have antibodies to AChR
Leite MI et al Brain (2008); 131:1940

Tensilon TestEdrophonium chloride
Inhibits acetylcholinesterase
Onset 30 seconds; duration 5-10 minNEED A CLEAR OBJECTIVE ENDPOINT
Works best with complete ptosis
Compare to placebo (saline)Prepare atropineGive test dose 1-2 mg then up to 10 mg totalSFX:
salivation, sweating, nausea, abdo cramping, fasciculations; hypotension & bradycardia are rare (may be as low as 0.16%)
Sensitivity 71.5- 95%Specificity: not clear but can be positive in many other conditions (even ALS or normal controls)Not availible

Ice pack test
Apply ice pack to ptotic lid
Sensitivity89%
Specificity100% (!?)

EMG: repetitive stimulation
Decremental response of CMAP amplitude or area with 2-5 Hz stimulation
Sensitivity 53-100% for generalize; 10-17% for ocular If safe: stop mestinon 12 hr before EMG!

Single Fiber EMG

Treatment

Treatment: the basics
What should you tell your MG patients?Always tell physicians (especially surgeons/ anesthetists). Why?What to do if you can’t swallow or get short of breath. Why?Don’t take medications / OTC / vitamins/ herbals without consulting an MD or pharmacist
Check B12, TSH. Why?“Should I get the flu shot?”Prednisone: bone protections & monitor for side effects (BP, glucose, cataracts, etc)

Drugs that unmask or exacerbate MG

Medications that can cause autoimmune MGD-Penicillamine, chloroquine, alpha-interferon, IL-2, wasp stings or coral snake bite, trimethadione
Implicated in isolated instances or MG exacerbation:
Cimetidine, citrate, chloroquine, diazepam, lithium carbonate, quinine, beta blockers, trihexylphenidyl hydrochloride, radiocontrast material, gemfibrozil, ?statins

Treatment: what are the options?
Mestinon: symptomatic therapyImmune Modulators:
PrednisoneAzathioprineMycophenylate mofetilCyclosporineIVIGPLEX

IVIG -Class I -First line therapy for short term use in worsening of moderate to severe MG. See Zinman et al Neurology 2007; 68: 837
Treatment

Thymectomy
How many MG patients have a thymic tumour?10% of MG patients have a thymic tumour 20% of patients with MG whose symptoms began between 30 and 60 yrs had thymoma lower incidence of thymoma if symptoms began after age 60
And the rest?70% of MG patients have hyperplastic changes (germinal centers) …indicate as active immune response
thymic tumours are usually benign, well-differentiated, encapsulated and can be completely removed

Thymectomy
Mandatory if you have a thymoma but if not...AAN practice parameter (2000)
For patients with nonthymomatous autoimmune MG, thymectomy is recommended as an option to increase the probability of remission or improvement (Class II).
Often done in generalized MG patients <50 yrs within 1-2 yr of disease onset (expert opinion)Trial underway: Dr Chalk...
Multicenter, single blind RCT (thymectomy or not)Ab positive, < 60 yr

Refractory MG
Is this really refractory MG or is this under treated MG?Adequate doses & duration of medicationsDid you try all the options we already discussed?ComplianceIs the thymoma gone or did you miss one?
Is this really MG? Comorbidities? Check thyroid
Could this be a congenital form of MG?Is the risk worth the potential benefit if you want to resort to experimental therapies:
Rituximab (Ab to Cd20): case seriesTacrolimus (suppresses T cell activation)Stem cell transplant???

Case 1: HPI
57 yr F with 3 month history of fatigue, ptosis, dysphagia3 months: Fatigue & “weak all over”Ptosis:
right side, better in am (for first 5-10 minutes); needed to tape her eye open; did not note recovery with rest; progressively worse
Blurred vision1 mo: progressive dysphagia

Case1: PMHx
Graves diseaseCoincidence?
Headaches
All: sulfa
Med: synthroid, prn ibuprofen, sudafed

Case 1
On exam...
Ptosis
Proximal weakness of the limbs
What to do?

Case 1: Investigations
Tensilon test
EMGsfEMG
CT chest: thymic mass
What now?

Case 1: Mngmt
Thymectomy: thymoma
IVIG
Prednisone
Mestinon
D/c home 10 postop

Conclusion
Signs & symptoms of MG can be elicited by the history and physical exam--> clinical diagnosisThe diagnosis of MG can be confirmed by electrophysiological & serological testsAnti-Musk patients are probably differentTreatment consists of symptomatic & immune modulatory therapiesThymectomy is mandatory for thymoma and should be considered for non-thymomatous patients (consider enrolling in a trial)

ReferencesContinuum Feb 2009; 15(1): 13-82
See Ethics chapter by K Brownell & Phil!
Bradley 4th & 5th Edwww.utdol.com: comprehensive list of drugs to avoid in MGGood reviews:
Muscle & Nerve Apr 2004Lancet June 30, 2001
AAN guideline on thymectomy 2000Evidence for treatments & good review of pathophysiology:
Nat Clin Prac Neurol Jun 2008
Important papers:L Zinman Neurol Mar 13, 2007 (IVIG RCT)‘Seroneg MG’ Brain May 31, 2008