Myasthenia gravis rehabilitation
32
Myasthenia Gravis
-
Upload
mohamed-fazly -
Category
Health & Medicine
-
view
604 -
download
2
Transcript of Myasthenia gravis rehabilitation

Myasthenia Gravis

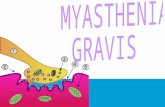
Introduction• Myasthenia gravis (MG) is a neuromuscular disease that leads to fluctuating muscle weakness and fatigue
• Caused by a breakdown in the normal communication between nerves and muscles
• There is no cure for myasthenia gravis, but treatment can help relieve signs and symptoms

Signs and symptoms• Initial complaint is a specific muscle weakness• Extraocular muscle weakness or ptosis• Bulbar muscle weakness is also common, along with weakness of head extension and flexion
• Limb weakness may be more severe proximally than distally
• Weakness is typically least severe in the morning and worsens as the day progresses

• Weakness is increased by exertion and alleviated by rest
• Weakness progresses from mild to more severe over weeks or months, with exacerbations and remissions
• About 87% of patients have generalized disease within 13 months after onset
• Difficulty breathing, chewing, swallowing


• Factors that worsen MG symptoms :– Fatigue– Illness– Stress– Extreme heat– Some medications (chloroquine, procaine, lithium, phenytoin, beta-blockers, procainamide, statins)

Diagnosis• Neurological examination• Edrophonium test• Ice pack test• Blood analysis• Repetitive nerve stimulation• Single-fiber electromyography (EMG)• Pulmonary function tests

Treatment• Cholinesterase inhibitors• Corticosteroids• Immunosuppressant• Plasmapheresis• Intravenous immunoglobulin (IVIG)• Surgery

Physical Rehabilitation

Introduction• MG symptoms tend to progress over time, usually reaching their worst within a few years after the onset of the disease
• Muscle weakness caused by MG worsens as the affected muscles are used repeatedly, therefore symptoms usually improve with rest

Factors limiting daily physical function in stable MG
• Neuromuscular fatigue• Low CV fitness levels (20% below normal)• Diminished physiological fitness reserve (high energy cost of walking at peak fitness level)
• Percent body fat 2-X normal (45%) and poor fitness contribute to mobility disability


Reduced daily physical activity =Formula for physical deconditioning
And poor cardiovascular health
Free living daily ambulatory activity levels of 3500 steps/day in MG are comparable to
disabled frail elderly and about 1/3 the level needed to sustain fitness and health
Low energy expenditure of free living daily activity and normal diet = OBESITY

Potential benefits of physical therapy in MG
• Weight reduction• Decrease in risk of hypertension, diabetes, cholesterol
• Decrease in risk of cardiac diseases• Decrease in risk of osteoporosis• Mood elevation ; improve cognitive function• Enhance baseline functional capacity, improved mechanical efficiency

Management Strategy• There is a lot of variance between patients with MG• No one exercise program is same and treatment strategies may vary
• Evaluation-– Strength– Flexibility– Mobility– Balance– Gait


Exercise Goals• Enhance ability to function daily• Decrease risk of falling• Completion of functional tasks and maintenance of independence
• Smoothness and coordination of activities• Once MG is stable, consistent exercise will elevate baseline functional capacity which will diminish the effect of MG exarcebation

Exercise Considerations• The dollar per day rule• Exercise at the best time of day• Exercise at peak dose of medication (pyridostigmine)
• Exercise large, proximal muscle groups for short periods of time building up only to moderate intensity
• Do not exceed moderate intensity exercise level

Moderate Exercise Intensity
• HR should not elevate greater than 30 bpm from resting baseline
• Patient should not become short of breath at peak of exercising
• MG symptoms should not become worse during exercise (drooping of eyes)
• Patient should not be tires after 2 hours of exercise• Patient should not have severe residual muscle soreness the day post exercise

Types of Exercise used in MG• Aerobic Exercises• Strength exercises• Swimming• Postural exercise• Breathing exercise


• Strength Exercise – – Should be done progressively– Range of motion (flexibility) to light resistance to full resistance
– Start with lower prescription : 3 sets of 5 reps– If significant weakness is present, active assist exercises may be necessary (therapist help)
• The primary goal of therapy is to build the individual's strength to facilitate return to work and activities of daily living
• Do not overdo resistive training to the point of fatigue



• Swimming– Patients should swim in water where they can touch the bottom
– Deep water is dangerous and may cause patient to over exert

• Postural Exercises-– Important in assisting with breathing, speaking and swallowing
– Keeps bones and joints in the correct alignment so that muscles are being used properly
– Prevents fatigue because muscles are being used more efficiently, allowing the body to use less energy


• Breathing exercises -– Help improve lung function– Include inspiratory muscle training• Pursed lip breathing• Diaphragmatic breathing
– These exercises can improve respiratory endurance as many people with MG have affected respiratory muscles


In myasthenia gravis, good days alternate with bad, and the physical
therapist should modify the rehabilitation program
accordingly

Reference
• http://www.myastheniagravis.org/• Myasthenia Gravis foundation of America http://www.myasthenia.org/
• http://www.mdguidelines.com/• http://www.pivotalphysio.com/• http://www.livestrong.com/