Myasthenia gravis
27
1 CHAPTER 1 INTRODUCTION 1.1. Background Myasthenia gravis is a chronic autoimmune neuromuscular disease characterized by varying degrees of weakness of the skeletal (voluntary) muscles of the body. The name myasthenia gravis, which is Latin and Greek in origin, literally means "grave muscle weakness." With current therapies, however, most cases of myasthenia gravis are not as "grave" as the name implies. In fact, for the majority of individuals with myasthenia gravis, life expectancy is not lessened by the disorder. The hallmark of myasthenia gravis is muscle weakness that increases during periods of activity and improves after periods of rest. Certain muscles such as those that control eye and eyelid movement, facial expression, chewing, talking, and swallowing are often, but not always, involved in the disorder. The muscles that control breathing and neck and limb movements may also be affected.
description
Transcript of Myasthenia gravis

1
CHAPTER 1
INTRODUCTION
1.1. Background
Myasthenia gravis is a chronic autoimmune neuromuscular disease characterized by
varying degrees of weakness of the skeletal (voluntary) muscles of the body. The name
myasthenia gravis, which is Latin and Greek in origin, literally means "grave muscle weakness."
With current therapies, however, most cases of myasthenia gravis are not as "grave" as the name
implies. In fact, for the majority of individuals with myasthenia gravis, life expectancy is not
lessened by the disorder.
The hallmark of myasthenia gravis is muscle weakness that increases during periods of
activity and improves after periods of rest. Certain muscles such as those that control eye and
eyelid movement, facial expression, chewing, talking, and swallowing are often, but not always,
involved in the disorder. The muscles that control breathing and neck and limb movements may
also be affected.

2
CHAPTER 2
MYASTHENIA GRAVIS
2.1. Definition
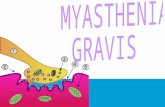
Myasthenia gravis is a relatively rare autoimmune disorder of peripheral nerves in which antibodies form against acetylcholine (ACh) nicotinic postsynaptic receptors at the myoneural junction. A reduction in the number of ACh receptors results in a characteristic pattern of progressively reduced muscle strength with repeated use of the muscle and recovery of muscle strength following a period of rest.
2.2. Epidemiology
The prevalence of myasthenia gravis in the United States ranges from 0.5-14.2 cases per 100,000 people. The prevalence has increased over the past 2 decades, primarily because of the increased life span of patients with the disease but also because of earlier diagnosis.
In the past (pre-1960), untreated myasthenia gravis carried a mortality rate of 30-70%. In the modern era, patients with myasthenia gravis have a near-normal life expectancy.Morbidity results from intermittent impairment of muscle strength, which may cause aspiration, increased incidence of pneumonia, falls, and even respiratory failure if not treated. In addition, the medications used to control the disease mayproduce adverse effects.With prompt diagnosis and treatment, the mortality rate of myasthenic crisis is less than 5%.
Onset of myasthenia gravis at a young age is slightly more common in Asians than in other races.The male-to-female ratio of myasthenia gravis in children and adults is 2:3.A female predominance exists in the young adult peak (ie, patients aged 20-30 y), and a slight male predominance exists in the older adult peak (ie, patients older than 50 y).The male-to-female ratio in children with myasthenia gravis and another autoimmune condition is 1:5.

3
Onset of myasthenia gravis peaks in neonates because of transfer of maternal autoantibodies, in those aged 20-30 years, and in those older than 50 years.
2.3. Etiology
The cause of myasthenia gravis is unknown, but it is clearly an autoimmune disease in which the specific antibody completely has been characterized. In up to 90% of generalized cases, IgG to the nicotinic Ach receptor is present. Females and people with certain human leukocyte antigen (HLA) types have a genetic predisposition to autoimmune diseases.
As with other autoimmune diseases, a derangement of immune regulation occurs. Sensitization to a foreign antigen that has cross-reactivity with the nicotinic ACh receptor has been proposed as a cause of myasthenia gravis, but the triggering antigen has not yet been identified.
2.4. Pathogenesis
The polyclonal IgG antibodies to AChR are produced by plasma cells in peripheral lymphoid organs, bone marrow, and thymus. These cells are derived from B cells that have been activated by antigen-specific T-helper (CD4+) cells. The T cells have also been activated, in this case, by binding to AChR antigenic peptide sequences (epitopes) that rest on the histocompatibility antigens on the surface of antigen-presenting cells.
The AChR antibodies react with multiple determinants, and enough antibodies circulate to saturate up to 80% of all AChR sites on muscle. A small percentage of the anti-AChR molecules interfere directly with the binding of ACh, but the major damage to end plates seems to result from actual loss of receptors owing to complement-mediated lysis of the membrane and to acceleration of normal degradative processes (internalization, endocytosis, lysosomal hydrolysis) with inadequate replacement by new synthesis.

4
As a consequence of the loss of AChR and the erosion and simplification of the end plates, the amplitude of miniature end plate potentials is about 20% of normal, and patients are abnormally sensitive to the competitive antagonist curare. The characteristic decremental response to repetitive stimulation of the motor nerve reflects failure of end plate potentials to each threshold so that progressively fewer fibers respond to arrival of a nerve impulse. How the autoimmune disorder starts is not known. In human disease, in contrast to experimental MG in animals, the thymus gland is almost always abnormal often with multiple lymphoid follicles showing germinal centers (“hyperplasia of the thymus”), and in about 15% of patients, there is an encapsulated benign tumor, a thymoma. These abnormalities are impressive because the normal thymus is responsible for the maturation of T cells that mediate immune protection without promoting autoimmune responses. AChR antibodies are synthesized by B cells in cultures of hyperplastic thymus gland. The hyperplastic glands contain all the elements needed for antibody production: class II HLA-positive antigen-presenting cells, T-helper cells, B cells,

5
and AChR antigen; that is, mRNA for subunits of AChR has been detected in thymus, and “myoid cells” are found in both normal and hyperplastic thymus. The myoid cells bear surface AChR and contain other muscle proteins. When human myasthenic thymus was transplanted into severely congenitally immunodeficient mice, the animals produced antibodies to AChR that bound to their own motor end plates, even though weakness was not evident.
Excessive and inappropriately prolonged synthesis of thymic hormones that normally promote differentiation of T-helper cells may contribute to the autoimmune response. Still another possible initiating factor is immunogenic alteration of the antigen, AChR, at end plates, because penicillamine therapy in patients with rheumatoid arthritis may initiate a syndrome that is indistinguishable from MG except that it subsides when administration of the drug is stopped.
There are few familial cases of the acquired autoimmune disease, but disproportionate frequency of some HLA haplotypes (B8, DR3, DQB1) in MG patients suggests that genetic predisposition may be important. Other autoimmune diseases also seem to occur with disproportionate frequency in patients with MG, especially hyperthyroidism and other thyroid disorders, SLE, rheumatoid arthritis, pernicious anemia, and pemphigus.
Most AChR antibodies are directed against antigenic determinants on the extracellular portion of the protein farthest out from the membrane rather than the ACh-binding site. The summed effects of the polyclonal anti-AChR antibodies, especially those that fix complement, result in destruction of the receptors. Physiologic studies indicate impaired postsynaptic responsiveness to ACh, which accounts for the physiologic abnormalities, clinical symptoms, and beneficial effects of drugs that inhibit acetylcholinesterase (AChE). If binding or blocking antibodies are absent, tests can be done for “modulating” antibodies that enhance degradation of the receptors in cultured cells, bringing the number of positive tests to 90.
2.5. Pathology
The overt pathology of MG is found primarily in the thymus gland. About 70% of thymus glands from adult patients with MG are not involuted and weigh more than normal. The glands show lymphoid hyperplasia: In normal individuals, germinal centers are numerous in lymph nodes and spleen but are sparse in the thymus. Immunocytochemical methods indicate that these thymic germinal centers contain B cells, plasma cells, HLA class II DR-positive T cells, and dendritic cells.
Another 10% of myasthenic thymus glands contain thymomas of the lymphoepithelial type. The lymphoid cells in these tumors are T cells; the neoplastic elements are epithelial cells. Benign thymomas may nearly replace the gland, with only residual glandular material at the

6
edges, or they may rest within a large hyperplastic gland. Thymomas tend to occur in older patients, but in Castleman's series, 15% were found in patients between ages 20 and 29 years. They may invade contiguous pleura, pericardium, or blood vessels, or seed onto more distant thoracic structures, including the diaphragm; however, they almost never spread to other organs. In older patients without thymoma, the thymus gland appears involuted, often showing hyperplastic foci within fatty tissue on microscopic examination of multiple samples.
In about 50% of cases, muscles contain lymphorrhages, which are focal clusters of lymphocytes near small necrotic foci without perivascular predilection. In a few cases, especially in patients with thymoma, there is diffuse muscle fiber necrosis with infiltration of inflammatory cells; similar lesions are only rarely encountered in the myocardium. Lymphorrhages are not seen near damaged neuromuscular junctions (although inflammatory cells may be seen in necrotic end plates in rat experimental autoimmune MG), but morphometric studies have shown loss of synaptic folds and widened clefts.
Some nerve terminals are smaller than normal, and multiple small terminals are applied to the elongated, simplified postsynaptic membrane; others are absent. Other end plates appear normal. On residual synaptic folds, immunocytochemical methods show Y-shaped antibody-like structures, IgG, complement components 2 and 9, and complement membrane attack complex.
2.6. Special Forms of Myasthenia Gravis
2.6.1. Juvenile and Adult Forms
Typical MG may begin at any age, but it is most common in the second to fourth decades. It is less frequent before age 10 or after age 65 years. Circulating AChR antibodies are demonstrated in 85% to 90% of patients with generalized MG and 50% to 60% of those with restricted ocular myasthenia. Patients without antibodies do not differ clinically or in response to immunotherapy; this seronegative MG may be more common in patients who are symptomatic before puberty. These are the typical forms of MG; other forms are rare.
2.6.2. MuSK Myasthenia
Among those with no detectable anti-AChR (10% to 15%), up to 70% have antibodies to MuSK. MuSK serves in postsynaptic differentiation and mediates agrin-induced AChR clustering. MuSK myasthenia particularly involves ocular, facial, and bulbar muscles and has high risk of respiratory insufficiency. Repetitive nerve stimulation shows decrement and there is jitter on single-fiber EMG, as in AchR myasthenia. Patients are more often girls or women and younger than those with AChR-MG. Plasmapheresis is of benefit while anticholinesterases are

7
not, nor is thymectomy. There have been no reports of lymphoid hyperplasia with germinal centers in thymectomy samples. The anti-MuSK syndrome usually responds to prednisone but sometimes with higher doses than the AChR antibody disorder.
2.6.3. Neonatal Myasthenia
About 12% of infants born to myasthenic mothers have a syndrome characterized by impaired sucking, weak cry, limp limbs, and, exceptionally, respiratory insufficiency. Symptoms begin in the first 48 hours and may last several days or weeks, after which the children are normal. The mothers are usually symptomatic but may be in complete remission; in either case, AChR antibodies are demonstrable in both mother and child. Symptoms disappear as the antibody titer in the infant declines. Severe respiratory insufficiency may be treated by exchange transfusion, but the natural history of the disorder is progressive improvement and total disappearance of all symptoms within days or weeks. Respiratory support and nutrition are the key elements of treatment. Rare instances of arthrogryposis multiplex congenita have been attributed to transplacental transfer of antibodies that inhibit fetal AChR.
2.6.4. Congenital Myasthenia
Children with congenital MG, although rarely encountered, show several characteristics. The mothers are asymptomatic and do not have circulating anti-AChR in the blood. Usually, no problem occurs in the neonatal period; instead, ophthalmoplegia is the dominant sign later in infancy. Limb weakness may be evident. The condition is often familial. Antibodies to AChR are not found, but there are decremental responses to repetitive stimulation. Ultrastructural and biochemical examination of motor end plates, microelectrode analysis, and identification of mutations have delineated a series of disorders that include both presynaptic, synaptic, and postsynaptic proteins including not only AChR but the ColQ part of AChE, choline acetylase, rapsyn, MuSK, the Nav1.4 sodium channel, plectin, and Dok-7. Disorders of the ion channel formed by the AChR molecule include the slow-channel syndrome, in which the response to ACh is enhanced because the opening episodes of the channel are abnormally prolonged. Forearm extensors tend to be selectively weak. More than 11 different mutations have been identified in different AChR subunits. Quinidine shortens the prolonged openings and gives therapeutic benefit. A fast-channel syndrome, with impaired response to ACh, has been reported in rare patients with mutations of the ε-subunit. Another mutation in the same subunit leads to abnormal kinetics of AChR activation so that the channel opens more slowly and closes more rapidly than normal. The 38 known mutations in the ε-subunit are inherited recessively and result in severe lack of AChR in the end plates. One syndrome results from mutations in the collagen tail subunit of AChE, creating a deficiency of the enzyme.
The British team led by Angela Vincent and the late John Newsom-Davis found clinical differences between those with mutations in the AChR ε-subunit and those with mutations in

8
rapsyn, the end plate AChR clustering protein. The receptor mutations caused congenital ophthalmoplegia, bulbar symptoms, and limb weakness. The rapsyn mutations caused an early-onset syndrome with arthrogryposis and life-threatening crises in childhood or a late-onset syndrome beginning in adolescence or later and resembling seronegative myasthenia. Dok-7 binding impairs MuSK signaling and this myasthenic syndrome is relatively common. It is associated with a proximal (limb-girdle) weakness. Slow-channel syndrome benefits from quinidine; fast-channel syndromes, from 3,4-diaminopyridines. Anticholinesterase drugs may help in some of these disorders, but parents should be warned that sudden apneic spells may be induced by mild infections.
2.6.5. Drug-Induced Myasthenia
The best example of this condition occurs in patients treated with penicillamine for rheumatoid arthritis, scleroderma, or hepatolenticular degeneration (Wilson disease). The clinical manifestations and AChR antibody titers are similar to those of typical adult MG, but both disappear when drug administration is discontinued. Cases attributed to the anticonvulsant, trimethadione (Tridione), have been less thoroughly studied.
2.7. Diagnosis
The diagnosis of MG can be made without difficulty in most patients from the characteristic history and findings on examination. The dramatic improvement that follows the injection of neostigmine bromide (Prostigmin) or edrophonium (Tensilon) makes the administration of these drugs pertinent. Return of strength in weak muscles occurs uniformly after the injection of neostigmine or edrophonium , if no such response occurs, the diagnosis of MG is uncertain. Demonstration of the pharmacologic response is sometimes difficult. However, if the clinical features are suggestive, the test should be repeated, perhaps with a different dosage or rate of administration. Withholding anticholinesterase medication overnight may be helpful. False-positive responses to edrophonium are exceptional but have been recorded with structural lesions, such as a brain stem tumor. (MG can also coexist with other diseases, such as Graves ophthalmopathy or the Lambert-Eaton syndrome.)
The diagnosis of MG is buttressed by the finding of high titers of antibodies to AChR, but a normal titer does not exclude the diagnosis. Somnier found that the test had a specificity of more than 99.9%; sensitivity was 88% because of negative tests.
Responses to repetitive stimulation and single-fiber EMG also help. If a thymoma is present, the diagnosis of MG (rather than some other neuromuscular disease) is likely. In the past, clinicians used the increased sensitivity to curare as a test to prove that a syndrome

9
simulating MG was actually psychasthenia or something else; however, the test was inconvenient and, if done without proper precautions, was hazardous. Since the advent of the antibody test, the curare test has disappeared.
In the neostigmine test, 1.5 to 2 mg of the drug and atropine sulfate, 0.4 mg, are given intramuscularly. Objective improvement in strength is recorded at 20-minute intervals up to 2 hours. Edrophonium is given intravenously in a dose of 1 to 10 mg. The initial dose is 2 mg followed in 30 seconds, if necessary, by an additional 2 mg and in another 15 to 30 seconds by 5 mg to a maximum of 10 mg. Improvement is observed within 30 seconds and lasts a few minutes. Most responses are seen with doses less than 5.0 mg. Because of the immediate and dramatic nature of the response, edrophonium is preferred for evaluation of ocular and other cranial muscle weakness, and neostigmine may be reserved for evaluation of limb or respiratory weakness, which may require more time. Placebo injections are sometimes useful in evaluating limb weakness, but placebo is not necessary in evaluating cranial muscle weakness because that abnormality cannot be simulated. For all practical purposes, a positive response is diagnostic of MG.
2.7.1. Symptoms
The symptoms of MG have three general characteristics that together provide a diagnostic combination. Formal diagnosis depends on demonstration of the response to cholinergic drugs, electrophysiologic evidence of abnormal neuromuscular transmission, and demonstration of circulating antibodies to AChR or MuSK.
The fluctuating nature of myasthenic weakness is unlike any other disease. The weakness varies in the course of a single day, sometimes within minutes, and it varies from day to day or over longer periods. Major prolonged variations are termed remissions or exacerbations; when an exacerbation involves respiratory muscles to a need for intubation for assisted mechanical ventilation, it is called a crisis. An “exacerbation” may be ameliorated by noninvasive ventilation or may be a transient worsening without respiratory distress. Variations sometimes seem related to exercise; this and the nature of the physiologic abnormality have long been termed “excessive fatigability,” but there are practical reasons to de-emphasize fatigability as a central characteristic of MG. Patients with the disease almost never complain of fatigue or symptoms that might be construed as fatigue except when there is incipient respiratory muscle weakness. Myasthenic symptoms are always owing to weakness and not to rapid tiring. In contrast, patients who complain of fatigue, if they are not anemic or harboring a malignant tumor, almost always have emotional problems, usually depression.
The second characteristic of MG is the distribution of weakness. Ocular muscles are affected first in about 40% of patients and are ultimately involved in about 85%. Ptosis and diplopia are the symptoms that result. Other common symptoms affect facial or oropharyngeal

10
muscles, resulting in dysarthria, dysphagia, and limitation of facial movements. Together, oropharyngeal and ocular weakness cause symptoms in virtually all patients with acquired MG. Limb and neck weakness is also common, but in conjunction with cranial weakness. Almost never are the limbs affected alone.
Crisis is most likely to occur in patients with oropharyngeal or respiratory muscle weakness. It seems to be provoked by respiratory infection in many patients or by surgical procedures, including thymectomy, although it may occur with no apparent provocation. Both emotional stress and systemic illness may aggravate myasthenic weakness for reasons that are not clear; in patients with oropharyngeal weakness, aspiration of secretions may occlude lung passages to cause rather abrupt onset of respiratory difficulty. Major surgery may be followed by respiratory weakness without aspiration, however, so this cannot be the entire explanation. Spontaneous crisis seems to be less common now than it once was.
The third characteristic of myasthenic weakness is the clinical response to cholinergic drugs. This occurs so uniformly that it has become part of the definition, but it may be difficult to demonstrate in some patients, especially those with purely ocular myasthenia.
Aside from the fluctuating nature of the weakness, MG is not a steadily progressive disease. The general nature of the disease, however, is usually established within weeks or months after the first symptoms. If myasthenia is restricted to ocular muscles for 2 years, certainly if it is restricted after 3 years, it is likely to remain restricted, and only in rare cases does it then become generalized. Distinguishing solely ocular myasthenia from generalized myasthenia soon after onset is challenging. Solely ocular myasthenia differs serologically from generalized myasthenia because AChR antibodies are found in lower frequency—50%—and in low titer. Additionally, single-fiber EMG is more likely to be normal. Current debate centers on ability to predict generalized spread after ocular onset. Some suggest that early immunosuppression will suppress/retard generalization. However, there have been no reports of successful weaning from these medications followed by complete remission. Spontaneous remissions occur in about 25% of all patients and are also more likely to occur in the first 2 years.
Before the advent of ICUs and the introduction of positive pressure respirators in the 1960s, crisis was a life-threatening event, and the mortality of the disease was about 33%. With improved respiratory care, however, patients rarely die of MG, except when cardiac, renal, or some other disease complicates the picture.

11
2.7.2. Signs
Vital signs and findings on general physical examination are usually normal, unless the patient is in crisis. Weakness of the facial and levator palpebrae muscles produces a characteristic expressionless appearance with drooping eyelids. Weakness of ocular muscles may cause paralysis or weakness of isolated ocular muscles, limitation of conjugate gaze, complete ophthalmoplegia in one or both eyes, or a pattern resembling internuclear ophthalmoplegia. Weakness of oropharyngeal or limb muscles, when present, can be shown by appropriate tests.
Respiratory muscle weakness can be detected by pulmonary function tests, which should not be limited to measurement of vital capacity but should also include inspiratory and expiratory pressures, the measurement of which may be abnormal even before overt symptoms are evident. Muscular wasting of variable degree is found in about 10% of patients, but is not focal and is usually encountered only in patients with malnutrition caused by severe dysphagia. Fasciculations do not occur, unless the patient has received excessive amounts of cholinergic drugs. Sensation is normal and the reflexes are preserved, even in muscles that are weak.
The Medical Scientific Advisory Board (MSAB) of the Myasthenia Gravis Foundation of America (MGFA) formed a Task Force in May 1997 to address the need for universally accepted classifications, grading systems, and methods of analysis for patients undergoing therapy and for use in therapeutic research trials. Thus, MGFA Clinical Classification was created.
Class Io Any ocular muscle weaknesso May have weakness of eye closureo All other muscle strength is normal
Class IIo Mild weakness affecting other than ocular muscleso May also have ocular muscle weakness of any severity
Class IIao Predominantly affecting limb, axial muscles, or botho May also have lesser involvement of oropharyngeal muscles
Class IIbo Predominantly affecting oropharyngeal, respiratory muscles, or botho May also have lesser or equal involvement of limb, axial muscles, or both
Class IIIo Moderate weakness affecting other than ocular muscleso May also have ocular muscle weakness of any severity
Class IIIao Predominantly affecting limb, axial muscles, or botho May also have lesser involvement of oropharyngeal muscles

12
Class IIIbo Predominantly affecting oropharyngeal, respiratory muscles, or botho May also have lesser or equal involvement of limb, axial muscles, or both
Class IVo Severe weakness affecting other than ocular muscleso May also have ocular muscle weakness of any severity
Class IVao Predominantly affecting limb and/or axial muscleso May also have lesser involvement of oropharyngeal muscles
Class IVbo Predominantly affecting oropharyngeal, respiratory muscles, or botho May also have lesser or equal involvement of limb, axial muscles, or both
Class Vo Defined by intubation, with or without mechanical ventilation, except when used
during routine postoperative management.o The use of a feeding tube without intubation places the patient in class IVb.
2.7.3. Laboratory Data
Routine examinations of blood, urine, and CSF are normal. The characteristic electrodiagnostic abnormality is progressive decrement in the amplitude of muscle action potentials evoked by repetitive nerve stimulation at 3 or 5 Hz. In generalized MG, the decremental response can be demonstrated in about 90% of patients, if at least three neuromuscular systems are used (medianthenar, ulnar-hypothenar, accessory-trapezius). In microelectrode study of intercostal muscle, the amplitude of miniature end plate potentials is reduced to about 20% of normal. This is caused by a decrease in the number of AChR available to agonists applied by microiontophoresis. In single-fiber EMG, a small electrode measures the interval between evoked potentials of the muscle fibers in the same motor unit. This interval normally varies, a phenomenon called jitter, and the normal temporal limits of jitter have been defined. In MG, the jitter is increased, and an impulse may not appear at the expected time; this is called blocking, and the number of blockings is increased in myasthenic muscle. All these electrophysiologic abnormalities are characteristic of MG, but blocking and jitter are also seen in disorders of ACh release. The standard EMG is usually normal, occasionally shows a myopathic pattern, and almost never shows signs of denervation unless some other condition supervenes. Similarly, nerve conduction velocities are normal.
Antibodies to AChR are found in 85% to 90% of patients of all ages with generalized MG if human muscle is used as the test antigen. There have been no false-positive results except for rare patients with Lambert-Eaton syndrome or thymoma without clinical MG, or in

13
remission; these may be considered unusual forms of MG. Antibodies may not be detected in patients with strictly ocular disease, in some patients in remission (or after thymectomy), or even in some patients with severe symptoms. The titer does not match the severity of symptoms; patients in complete clinical remission may have high titers. Antibodies to myofibrillar proteins (titin, myosin, actin, actomyosin) are found in 85% of patients with thymoma and may be the first evidence of thymoma in some cases. In the first report of seronegative myasthenia. Found no clinical differences between patients who had or lacked AChR antibodies. Subsequently, more than half of these seronegative patients were found to have antibodies to MuSK. Subsequently, some investigators found that the clinical picture is almost always one of generalized MG with predominantly bulbar signs, poor and inconsistent responses to pyridostigmine, immunosuppressants, or thymectomy but excellent response to plasmapheresis. It is detected antibodies to rapsyn-clustered AChR on human embryonic kidney cells by fluorescence-activated cell sorting in 66% (25/38) of sera that had previously tested negative for binding to AChR in solution.
The different forms of congenital MG can be identified only in a few special centers that are prepared to perform microelectrode and ultrastructural analyses of intercostal muscle biopsies for miniature end plate potentials, AChR numbers, and determination of bound antibodies. It seems likely that DNA analysis may ultimately suffice for diagnosis.
Other serologic abnormalities are encountered with varying frequency, but in several studies, antinuclear factor, rheumatoid factor, and thyroid antibodies were encountered more often than in control populations. Laboratory (and clinical) evidence of hyperthyroidism occurs at some time in about 5% of patients with MG. Radiographs of the chest (including 10-degree oblique films) provide evidence of thymoma in about 15% of patients, especially in those older than 40 years. CT of the mediastinum demonstrates all but microscopic thymomas. MRI is not more sensitive than CT.
2.8. Differential Diagnosis
The differential diagnosis includes all diseases that are accompanied by weakness of oropharyngeal or limb muscles, such as the muscular dystrophies, amyotrophic lateral sclerosis (ALS), progressive bulbar palsy, ophthalmoplegia of other causes, and the asthenia of psychoneurosis or hyperthyroidism. There is usually no difficulty in differentiating these conditions from MG by the findings on examination and by the failure of symptoms in these conditions to improve after parenteral injection of neostigmine or edrophonium. Occasionally, blepharospasm is thought to mimic ocular myasthenia, but the forceful eye closure in that condition involves both the upper and the lower lids; the narrowed palpebral fissure and signs of active muscle activity are distinctive.

14
The only other conditions in which clinical improvement has been documented after use of edrophonium are other disorders of neuromuscular transmission: botulinum intoxication, snake bite, organophosphate intoxication, or unusual disorders that include features of both MG and the Lambert-Eaton syndrome. Denervating disorders, such as motor neuron disease or peripheral neuropathy, do not show a reproducible or unequivocal clinical response to edrophonium or neostigmine. The response should be unequivocal and reproducible. If a structural lesion of the third cranial nerve seems to respond, the result should be photographed (and published).
2.9. Prognosis
Given the current treatment that combines cholinesterase inhibitors, immunosuppressive drugs, plasmapheresis, immunotherapy, and supportive care in an ICU setting (when appropriate), most patients with myasthenia gravis have a near-normal life span. Thymectomy results in complete remission of the disease in a number of patients. However, the prognosis is highly variable, ranging from remission to death.The mortality rate is probably less than 4.
2.10. Treatment
Clinicians must choose the sequence and combination of five kinds of therapy: Anticholinesterase drug therapy and plasmapheresis are symptomatic treatments, whereas thymectomy, steroids, and other immunosuppressive drugs may alter the course of the disease.
2.10.1. Anticholinesterase Therapy
It is generally agreed that anticholinesterase drug therapy should be given as soon as the diagnosis is made. Of the three available drugs—neostigmine, pyridostigmine bromide, and ambenonium (Mytelase)—pyridostigmine is the most popular but has not been formally assessed in controlled comparison with the other drugs. The muscarinic side effects of abdominal cramps and diarrhea are the same for all three drugs but are least severe with pyridostigmine; none has more beneficial or adverse effects than another and all can be regarded as safe. The usual starting dose of pyridostigmine is 60 mg given orally every 4 hours while the patient is awake. Depending on clinical response, the dosage may be increased, but incremental benefit is not to be expected in amounts greater than 120 mg every 2 hours.

15
If patients have difficulty eating, doses can be taken about 30 minutes before a meal. If patients have special difficulty on waking in the morning, a prolongedrelease 180-mg tablet of pyridostigmine (Mestinon Timespan) can be taken at bedtime. Muscarinic symptoms can be ameliorated by preparations containing atropine (0.4 mg) with each dose of pyridostigmine. Excessive doses of atropine can cause psychosis, but the amounts taken in this regimen have not had that effect. Other drugs may be taken if diarrhea is prominent. Combinations of two drugs are no better than any one drug alone.
Although cholinergic drug therapy sometimes gives impressive results, there are serious limitations. In ocular myasthenia, ptosis may be helped, but some diplopia almost always persists. In generalized MG, patients may improve remarkably, but some symptoms usually remain. Cholinergic drugs do not return function to normal, and the risk of crisis persists because the disease is not cured. Therefore, one of the other treatments is used promptly to treat generalized MG.
2.10.2. Thymectomy
Thymectomy was originally reserved for patients with serious disability because the operation had a high mortality. With advances in surgery and anesthesia, however, the operative mortality is now negligible in major centers. About 80% of patients without thymoma become asymptomatic or go into complete remission after thymectomy; although there has been no controlled trial of thymectomy, these results seem to diverge from the natural history of the untreated disease.
Thus, thymectomy is now recommended for most patients with generalized MG. Decisions made for children or patients older than 65 must be individualized. Although it is safe, thymectomy is a major operation and is not usually recommended for patients with ocular myasthenia unless there is a thymoma. The thymoma should be resected but so should the remaining thymus that may show hyperplasia. The beneficial effects of thymectomy are usually delayed for months or years. It is never an emergency measure, and other forms of therapy are used in the interim. Mantegazza et al. found a remission rate of about 50% at 6 years after surgery with either the standard transsternal operation or a minimally invasive thorascopic operation.
2.10.3. Steroids
Prednisone therapy is used by some authorities to prepare patients for thymectomy, but that function is also served by plasmapheresis or by IVIG therapy. Exchanges of about 5% of calculated blood volume may be given several times before the day of surgery to be certain that the patient is functioning as well as possible and to ameliorate or avoid a postoperative respiratory crisis. Plasmapheresis is also used for other exacerbations; the resulting

16
improvement, seen in most patients, may be slight or dramatic and may last only a few days or several months. Plasmapheresis is safe but expensive and is not convenient for many patients. Indwelling catheters may lead to misplacement, bleeding, or infection. IVIG is easier to administer but is even more expensive. It is preferred over plasmapheresis in those with poor venous access, including children.
2.10.4. Plasmapheresis
Plasma exchange is used as a short-term intervention for patients with sudden worsening of myasthenic symptoms for any reason, to rapidly improve strength before surgery, and as a chronic intermittent treatment for patients who are refractory to all other treatments. The need for plasma exchange, and its frequency of use is determined by the clinical response in the individual patient. Almost all patients with acquired myasthenia gravis improve temporarily following plasma exchange. Maximum improvement may be reached as early as after the first exchange or as late as the fourteenth. Improvement lasts for weeks or months and then the effect is lost unless the exchange is followed by thymectomy or immunosuppressive therapy. Most patients who respond to the first plasma exchange will respond again to subsequent courses. Repeated exchanges do not have a cumulative benefit.
2.10.5. Intravenous Immune Globulin (IVIG)
Several groups have reported a favorable response to high-dose (2 grams/kg infused over 2 to 5 days) IVIG. Possible mechanisms of action include down-regulation of antibodies directed against AChR and the introduction of anti-idiotypic antibodies. Improvement occurs in 50 to 100% of patients, usually beginning within 1 week and lasting for several weeks or months. The common adverse effects of IVIG are related to the rate of infusion. The mechanism of action is not known but is probably non-specific down regulation of antibody production.
2.10.6. Immunosupressive Drug
If a patient is still seriously disabled after thymectomy, most clinicians use prednisone, 60 to 100 mg daily, to achieve a response within a few days or weeks. An equally satisfactory response can be seen with a lower dosage, but it takes longer; for instance, if the dose is 25 to 40 mg, benefit may be seen in 2 to 3 months. Once improvement is achieved, the dosage should be gradually tapered to 20 to 35 mg every other day. This has become a popular treatment for disabled patients, but there has been no controlled trial. If the patient does not improve in about 6 months or if there are unacceptable side effects from the steroids, treatment with azathioprine (Imuran), cyclosporine or cyclophosphamide would be considered, in doses up to 2.5 mg/kg daily for an adult. All of these may have major life-threatening side effects. The dosage should be increased gradually.

17
Another popular immunosuppressive drug that is being investigated as a steroid-sparing agent is mycophenolate mofetil (CellCept). In one report, 73% of 85 patients improved; adverse effects led to discontinuation of treatment in 6%. In another multicenter study, the drug was no better than placebo, but 70% of those taking placebo improved, and many clinicians still find value in mycophenolate. Whether steroids and immunosuppressive drugs have additive effects is also uncertain, and the relative risks are difficult to assess. The numerous side effects of prednisone must be weighed against the possibilities of marrow suppression, susceptibility to infection, or delayed malignancy in patients who are given immunosuppressive drugs.
Prednisone, 15 to 35 mg on alternate days, is also recommended by some clinicians for ocular myasthenia, weighing risks against potential benefit. For some patients in sensitive occupations, the risks of prednisone therapy may be necessary (e.g., actors, police officers, roofers or others who work on heights or those who require stereoscopic vision). Ocular myasthenia is not a threat to life, and pyridostigmine may alleviate ptosis. An eye patch can end diplopia, and prisms help some patients with stable horizontal diplopia. Thymectomy has become so safe that it might be considered for ocular myasthenia that is truly disabling.
Patients with thymoma are likely to have more severe MG and are less likely to improve after thymectomy; nevertheless, many of these patients also improve if the surrounding thymus gland is excised in addition to the tumor.
Myasthenic crisis arises in about 10% of myasthenic patients. It is more likely to occur in patients with dysarthria, dysphagia, and documented respiratory muscle weakness, presumably because they are liable to aspirate oral secretions, but crisis may also occur in other patients after respiratory infection or major surgery (including thymectomy). The principles of treatment are those of respiratory failure in general. Cholinergic drug therapy is usually discontinued once an endotracheal tube has been placed and positive pressure respiration started; this practice avoids questions about the proper dosage or cholinergic stimulation of pulmonary secretions. Crisis is viewed as a temporary exacerbation that subsides in a few days or weeks. The therapeutic goal is to maintain vital functions and to avoid or treat infection until the patient spontaneously recovers from the crisis. Cholinergic drug therapy need not be restarted unless fever and other signs of infection have subsided, there are no pulmonary complications, and the patient is breathing without assistance.
To determine whether plasma exchange or IVIG actually shortens the duration of crisis would require a controlled trial, but that has not been done. Even so, pulmonary intensive care is now so effective that crisis is almost never fatal and many patients go into a remission after recovery from crisis. Because of advances in therapy, MG is still serious, but not so grave.

18
REFERENCES
Aminoff M.J., Greenberg D.A, Simon R.P., 2005, Myasthenia Gravis, Clinical Neurology 6 th
Edition, United States of America, McGarw-Hill Companies; 183-184
Howard J.A., (2007, December 3), Myasthenia Gravis a Summary, accessed on 6 th April 2010,
from http://www.myasthenia.org/hp_clinicaloverview.cfm
Kumar P., Clark M., 2009, Neuromuscular Junction Conditions, Kumar & Clark’s Clinical
Medicine 7th edition, Spain, Saunders Elsevier; 1180-1181
Rowland L.P., Pedley T.A, 2010, Myasthenia Gravis, Merritt’s Neurology 12th Edition, New
York, Lippincott William and Wilkin; 845-850
Shah K.A., (2009, January 15), Myasthenia Gravis (Neurology), accessed on 6th April 2010, from
http://emedicine.medscape.com/article/1171206-overview