Myasthenia gravis
13
Presented by: Jessica Faye Manansala Myasthenia Gravis
Transcript of Myasthenia gravis

Presented by: Jessica Faye Manansala
Myasthenia Gravis

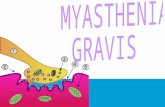
Myasthenia gravis, an autoimmune disorder affecting the myoneural junction, is characterized by varying degrees of weakness of the voluntary muscles.
Women tend to develop the disease at an early age (20-40 yrs of age)
In men (60-70 yrs of age)
What is myasthenia gravis?

Pathophysiology


Ocular muscle – diplopia (double vision)Ptosis (drooping of the eyelid)
Major signs and symptomsBulbar symptom- weakness of the muscle of face and
throatGeneralized weakness- resulting decrease vital
capacity and respiratory failureDysphonia (voice impairment)- this may result
increase risk for choking and aspiration
Myasthenia gravis is purely a motor disorder with noeffect on sensation or coordination.
Clinical manifestations

Myasthenic crisis
Cholinergic crisis
Complications

is an exacerbation of the diseaes process.Crisis may result from disease exacerbation
or a specific precipitation event.Most common precipitator is infection;
medicattion change, surgery, pregnancy and high environmental temp.
SymptomsSevere generalized muscle weakness and
respiratoryAnd bulbar weakness that may result
respiratory failure
Myasthenic Crisis

Symptoms of anticholinergic overmedication may mimic the symptoms of exacerbation
Differentation can be achieved with the edrophonium chloride (tensilon) test.
Difference between myasthenic & cholinergicMyasthenic- improves immediately following
adminstration of edrophoniumCholinergic- crisis may experience no
improvement or deteriorate
Cholinergic Crisis

Myasthenic crisis – neostigmine methylsulfate, prostigmine is admin IM or IV until the pt. is able to swallow oral anticholinestrase meds.
-plasma pheresis and IVIG- reduce antibody load
Cholinergic crisis – all anticholinestrase meds should be stop
- Atrophine sulfate should be given- an antidote for anticholinestrase medication.
Treatment for myasthenic & cholinergic crisis

Anti cholinestrase testEdrophonium chloride (tensilon) injected
through IV- 2mg at a time to a total of 10mg (30sec after
injection, facial muscle weakness & ptosis should resolve for about 5min=+). Atrophine (o.4mg)should availabale for side effects.
Repetitive nerve stimulation test- it records the electrical activity in target muscle after nerve stimulation.
MRI- for enlarged thymus gland
Diagnostic findings for MG

Administration of anticholinestrase agent Pyridostigmine bromide (mestinon) &
neostigmine bromide (prostigmine)Effect: provide symptomatic refief by increasing
the relative concentration of available acetylcholine at the neuro muscular junction. Improve strength and less fatigue
Immunosuppresive therapy CorticosteroidsEffect: to reduce production of the antibodyPrednisone taken on alternate days to lower the
incidence of side effects.
Medical Management

Plasmapheresis- blood cells & antibody containing plasma are separated, then cells and plasma substitutes are reinfused.
Effect: plasma exchange used to treat exacerbations. The improvement may last only a few weeks
IV immune globulin – nearly effective as plasmapheresis in controlling symptoms exacerbation.
Thymectomy - it can decrease or eliminate the need for medication

The end