Mvss part v weaning & liberation from mechanical ventilation
41
Mechanical Ventilatory Support Series Part V: Weaning & Liberation from Mechanical Ventilation Santi Silairatana, MD Division of Pulmonary Medicine, Department of Medicine, Faculty of Medicine Vajira Hospital Navamindradhiraj University
-
Upload
santi-silairatana -
Category
Health & Medicine
-
view
3.265 -
download
2
Transcript of Mvss part v weaning & liberation from mechanical ventilation
Mechanical Ventilatory Support Series
Part V:
Weaning & Liberation from Mechanical Ventilation
S a n t i S i l a i r a t a n a , M D
D i v i s i o n o f Pu l m o n a r y M e d i c i n e , D e p a r t m e n t o f M e d i c i n e , Fa c u l t y o f M e d i c i n e Va j i r a H o s p i t a l
N a v a m i n d r a d h i r a j U n i v e r s i t y
Outlines
Rationale of weaning
Weaning failure
Methods of weaning
Predictors of weaning success/failure
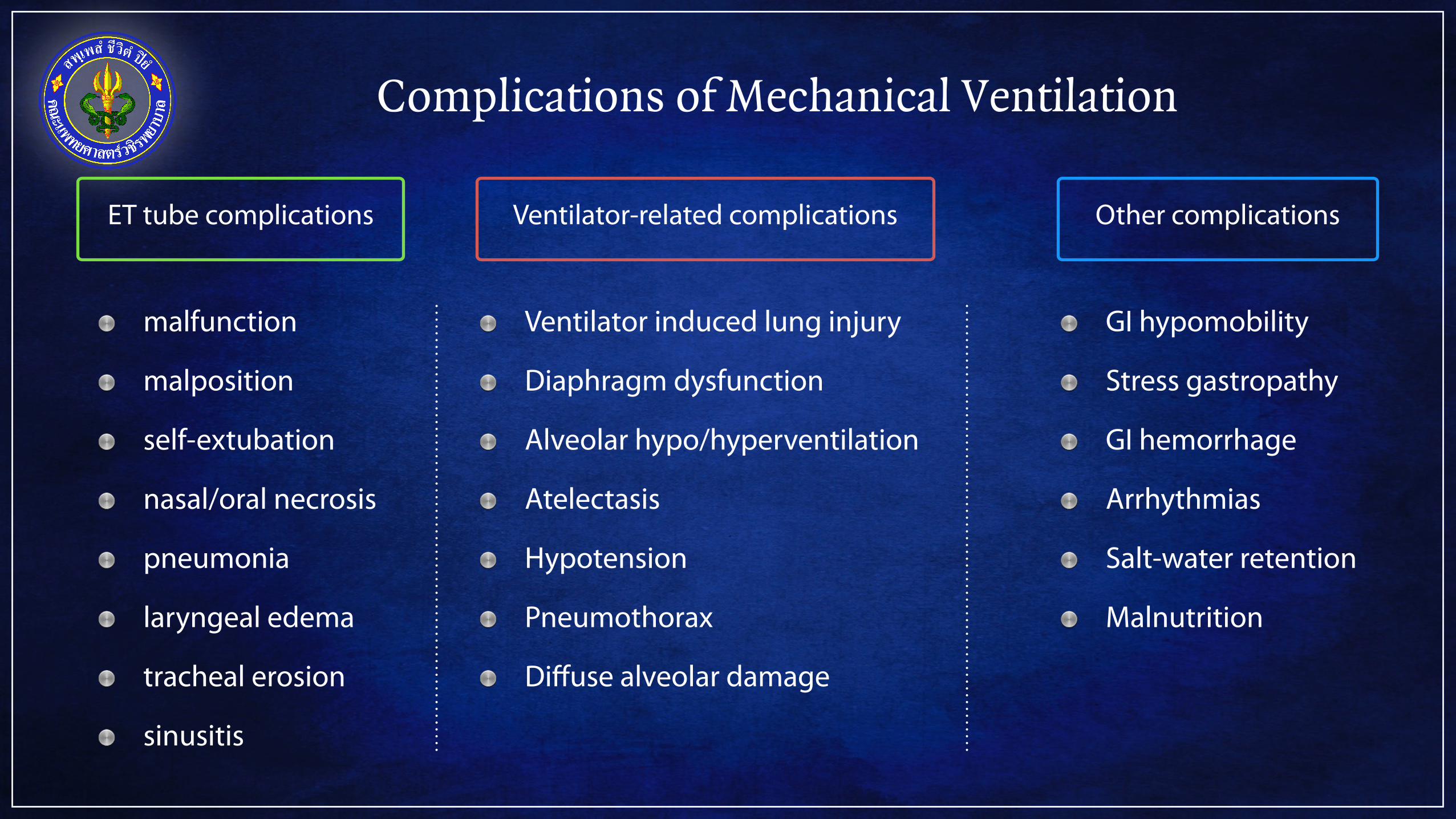
Complications of Mechanical Ventilation
Other complicationsET tube complications
malfunction
malposition
self-extubation
nasal/oral necrosis
pneumonia
laryngeal edema
tracheal erosion
sinusitis
Ventilator-related complications
Ventilator induced lung injury
Diaphragm dysfunction
Alveolar hypo/hyperventilation
Atelectasis
Hypotension
Pneumothorax
Diffuse alveolar damage
GI hypomobility
Stress gastropathy
GI hemorrhage
Arrhythmias
Salt-water retention
Malnutrition
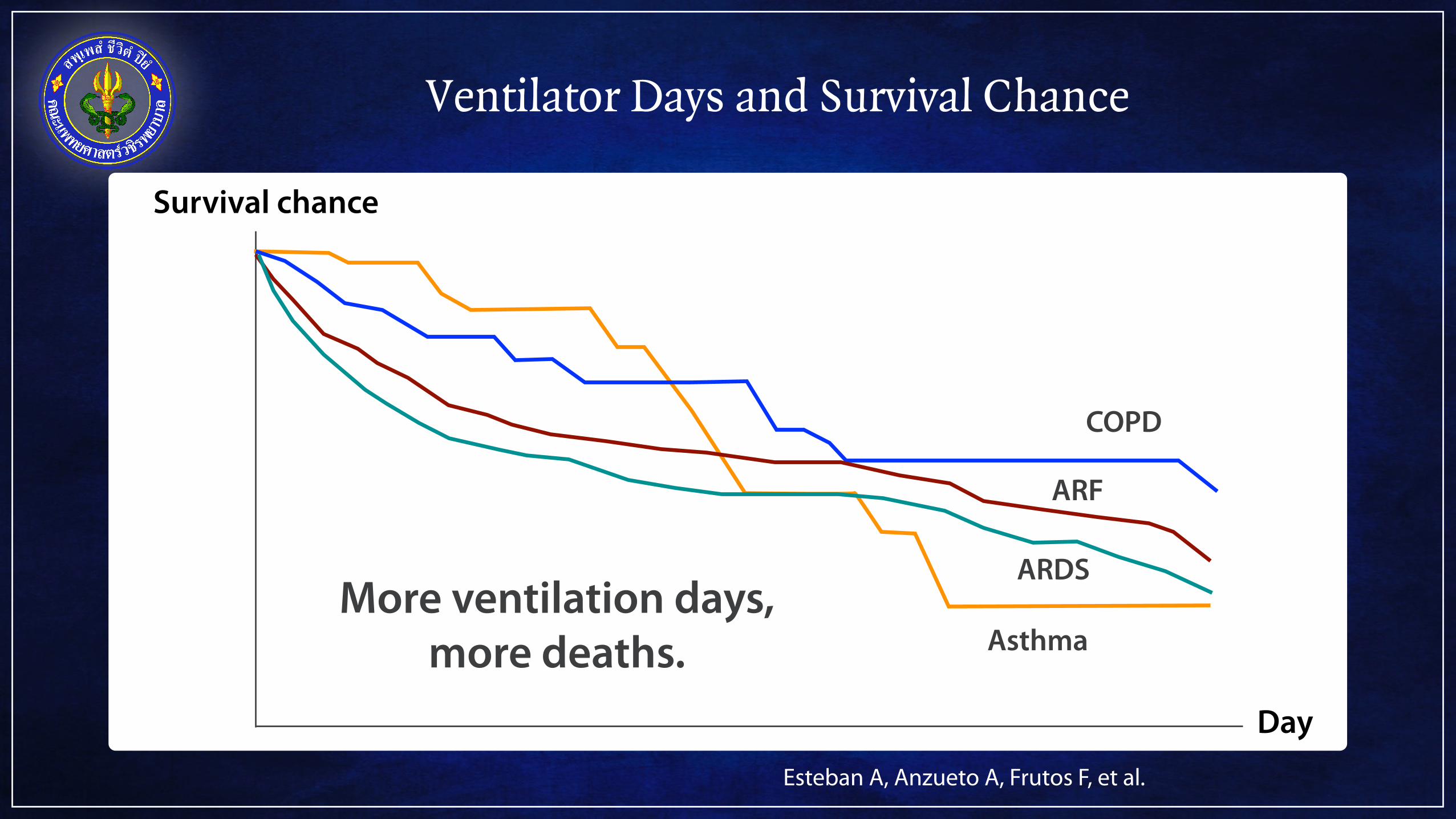
Ventilator Days and Survival Chance
Esteban A, Anzueto A, Frutos F, et al.
More ventilation days, more deaths.
Day
Survival chance
Asthma
COPD
ARF
ARDS
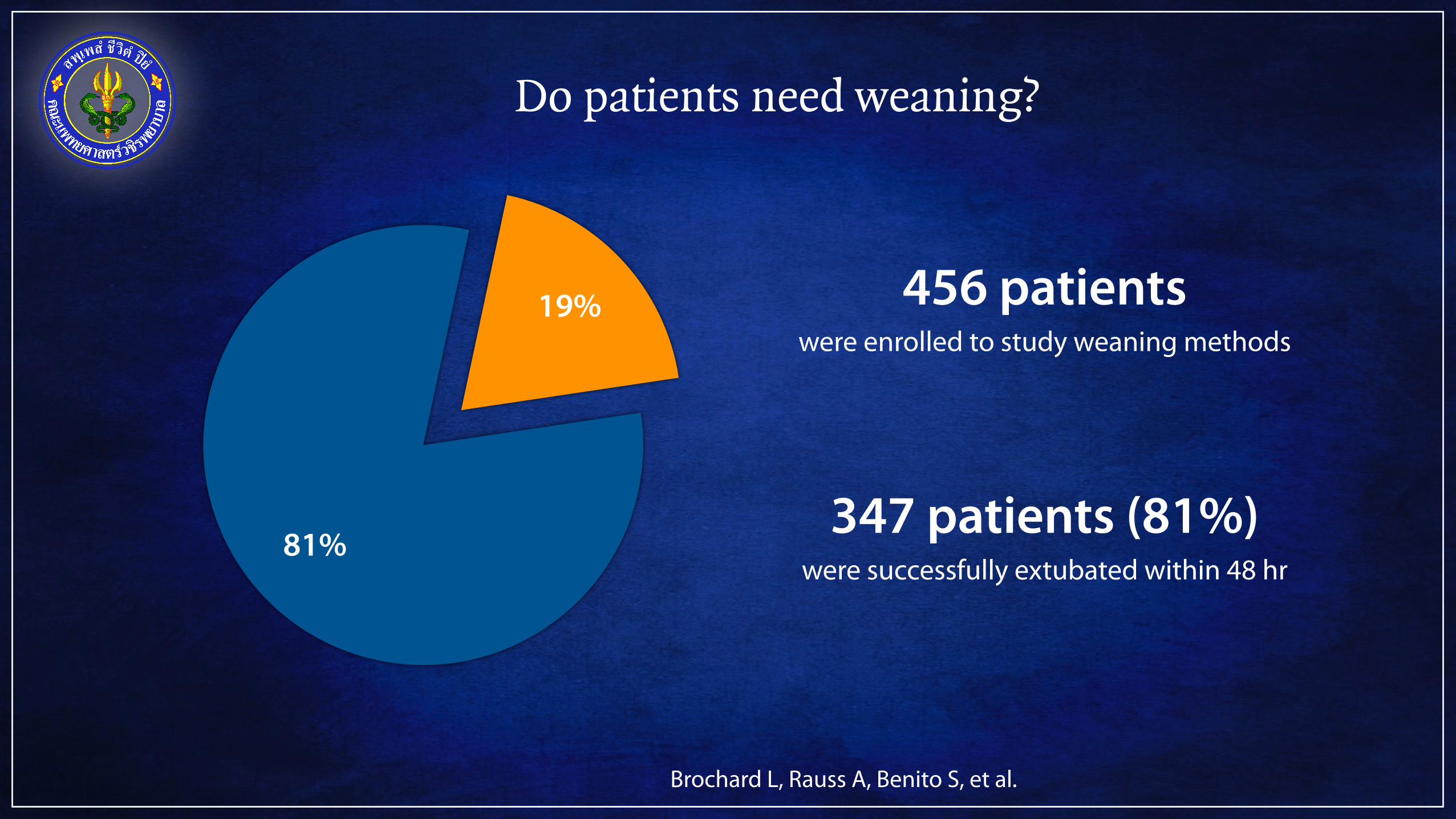
Do patients need weaning?
19%
81%
Brochard L, Rauss A, Benito S, et al.
456 patients were enrolled to study weaning methods
347 patients (81%) were successfully extubated within 48 hr
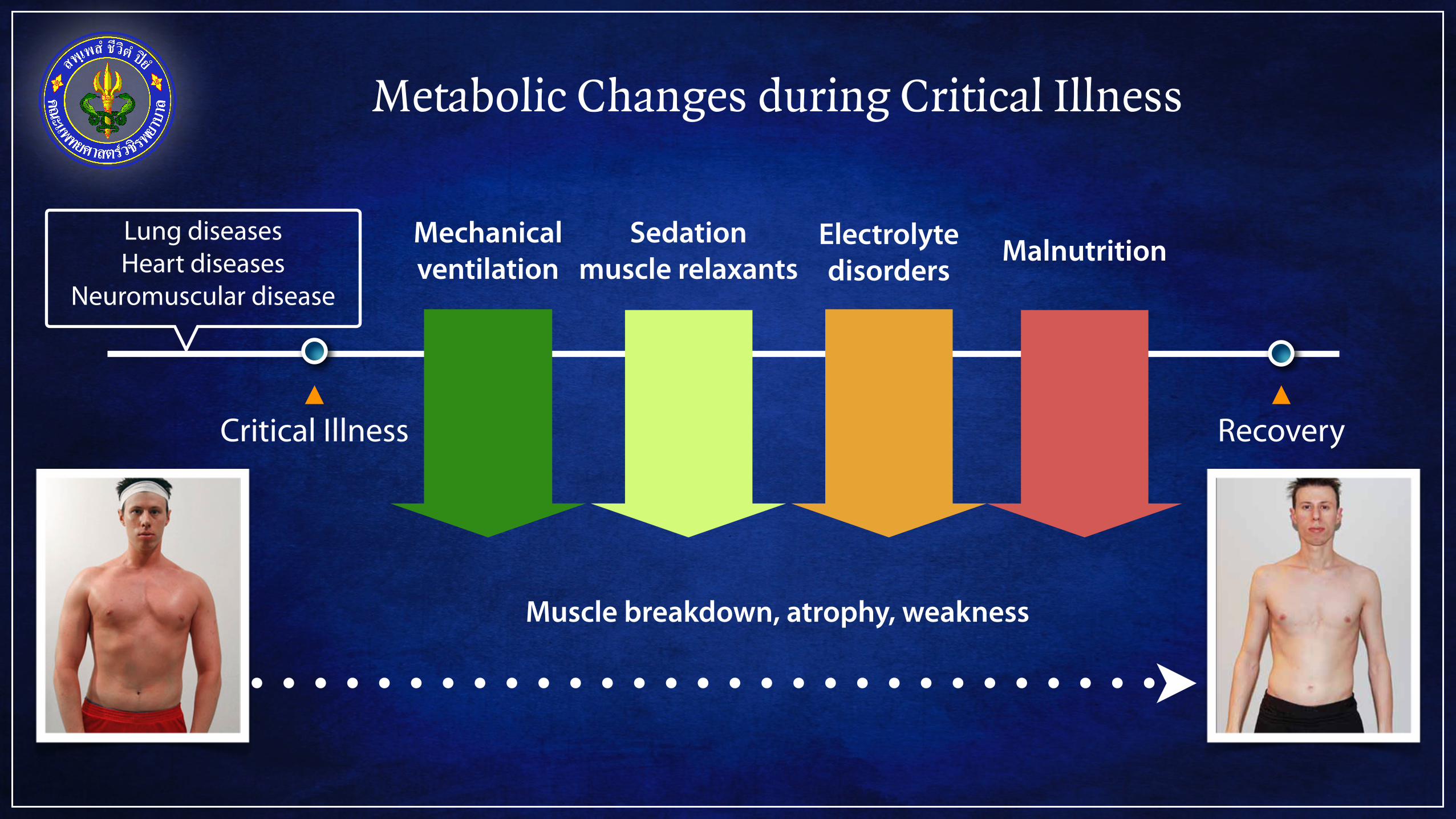
Metabolic Changes during Critical Illness
Critical Illness Recovery
Lung diseases Heart diseases
Neuromuscular disease
Mechanical ventilation MalnutritionElectrolyte
disordersSedation
muscle relaxants
Muscle breakdown, atrophy, weakness

Outlines
Rationale of weaning
Weaning failure
Methods of weaning
Predictors of weaning success/failure
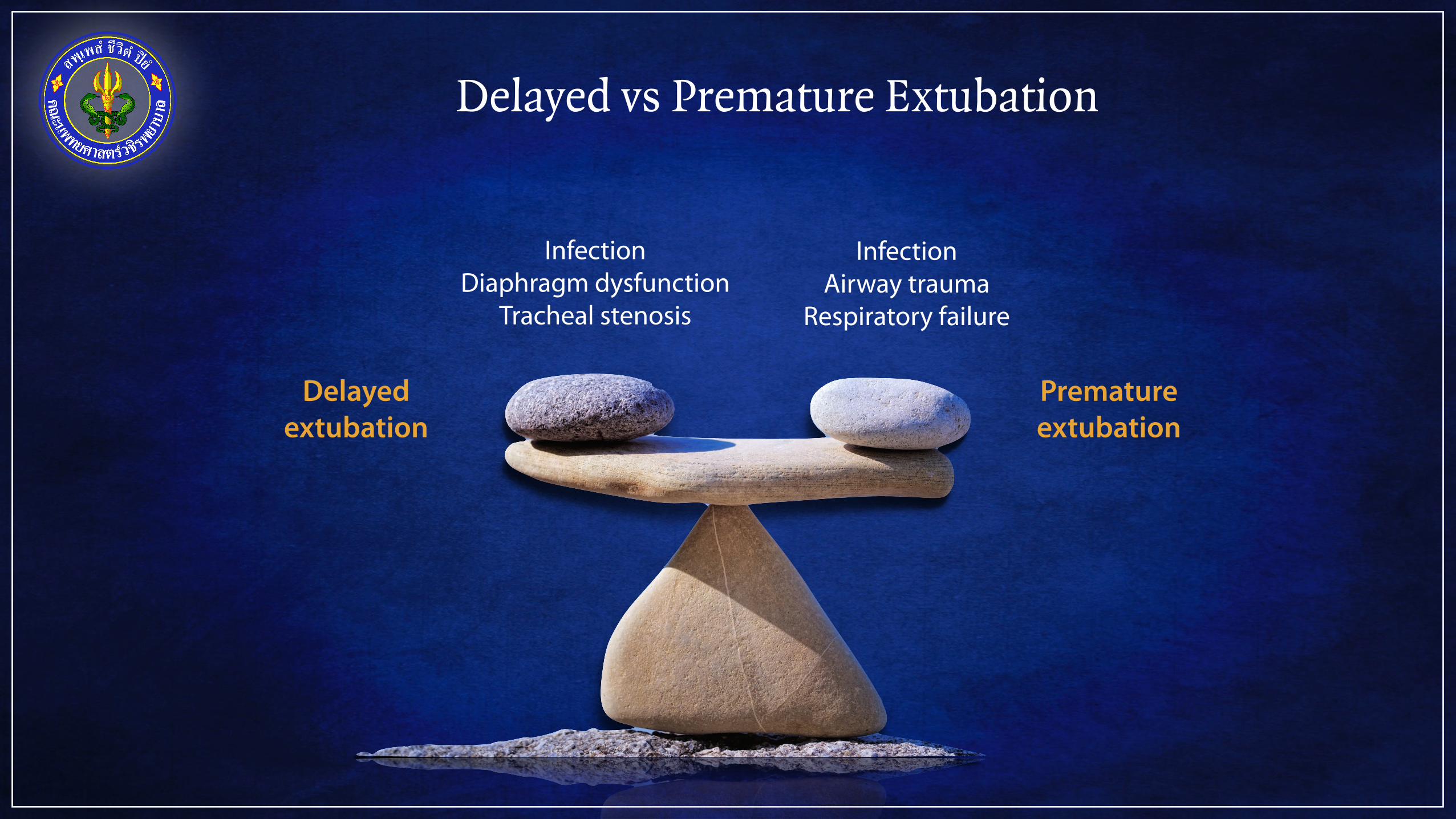
Delayed vs Premature Extubation
Delayed extubation
Premature extubation
Infection Diaphragm dysfunction
Tracheal stenosis
Infection Airway trauma
Respiratory failure
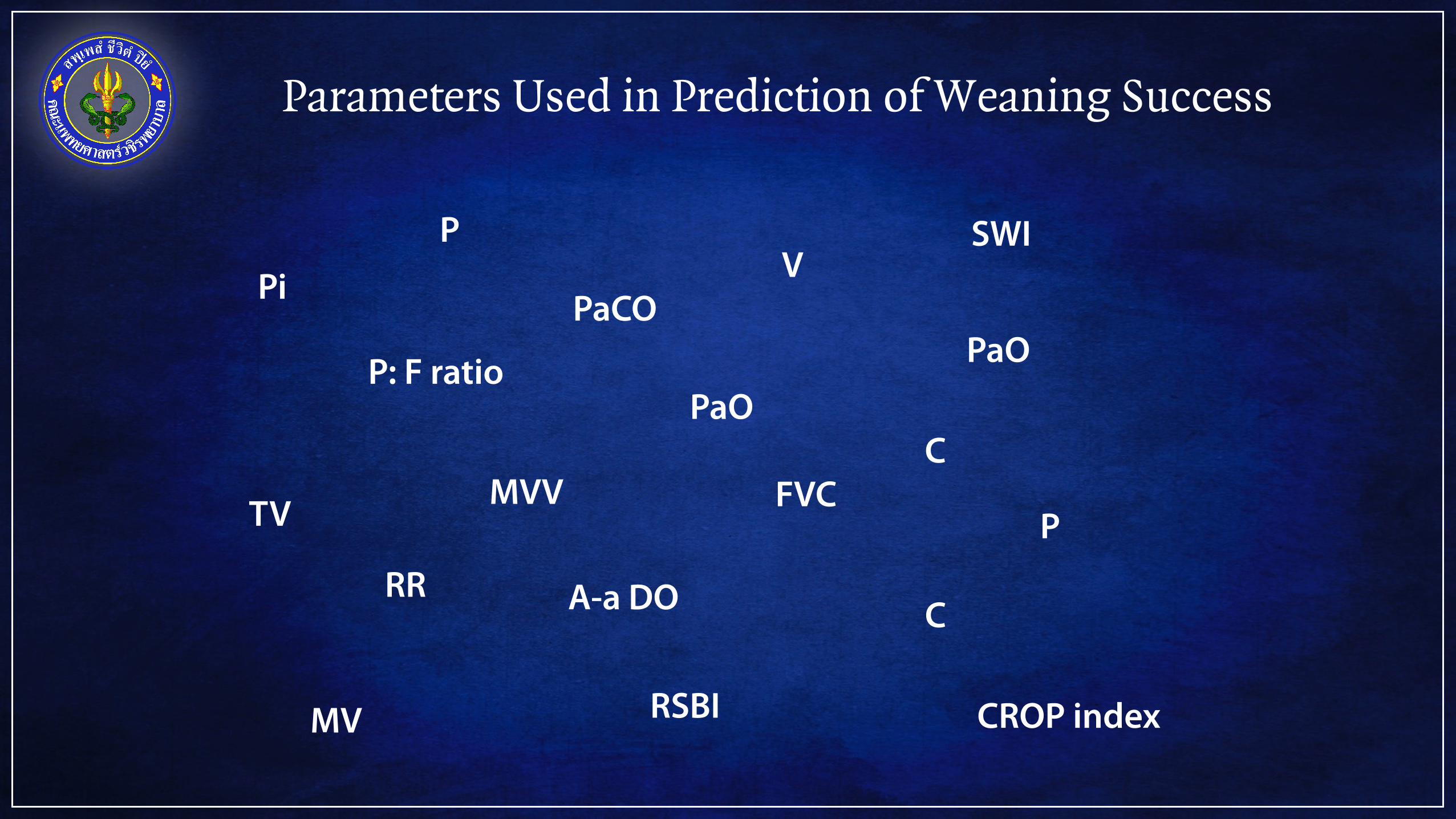
Parameters Used in Prediction of Weaning Success
PaOP: F ratio PaO
A-a DO
Pi
FVC
PaCO
MV
TV MVV
RR
PV
C
C
RSBI CROP index
P
SWI
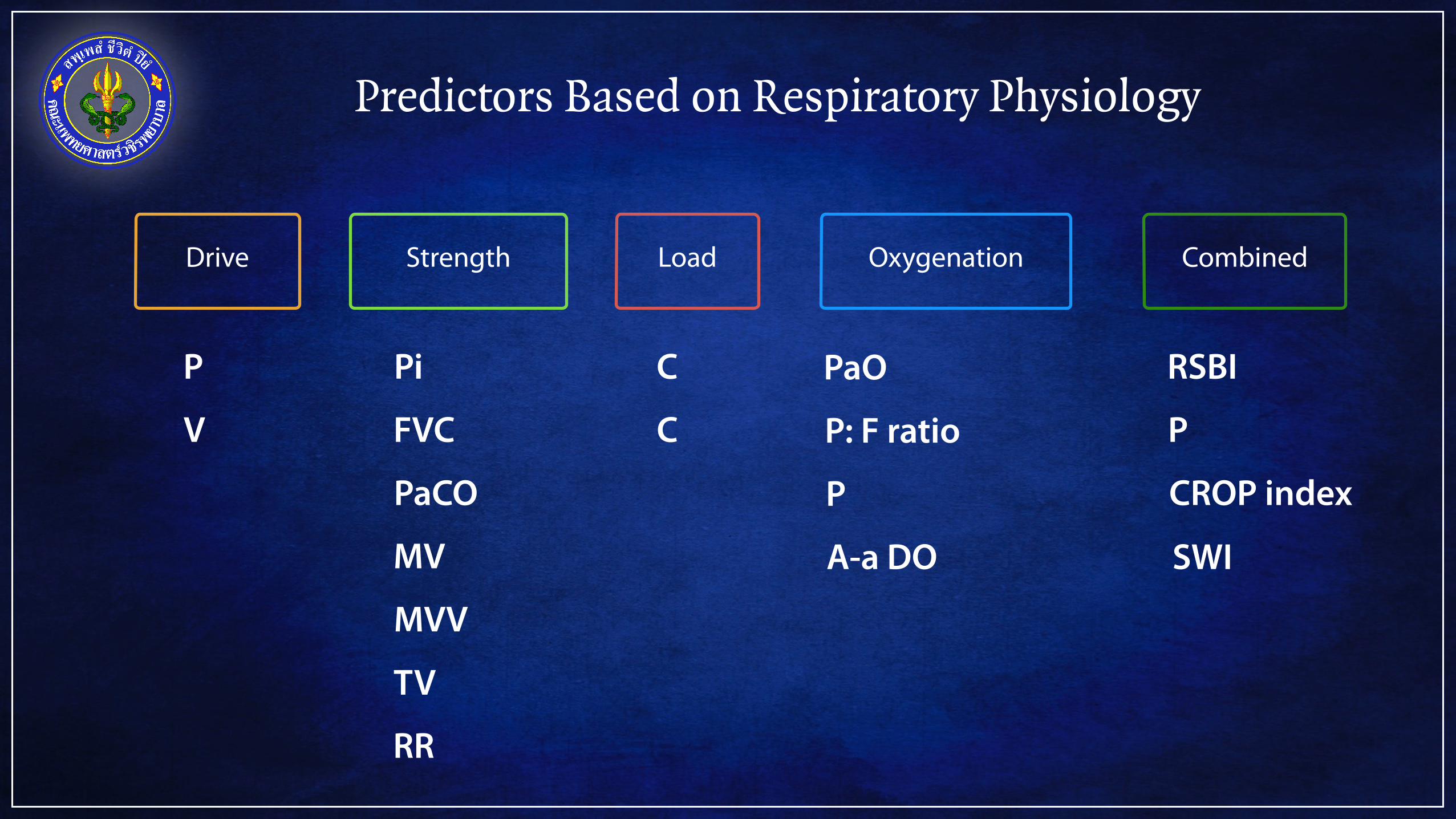
Predictors Based on Respiratory Physiology
PaO
P: F ratio
P
A-a DO
Pi
FVC
PaCO
MV
TV
MVV
RR
P
V C
C RSBI
CROP index
P
SWI
Oxygenation CombinedLoadStrengthDrive
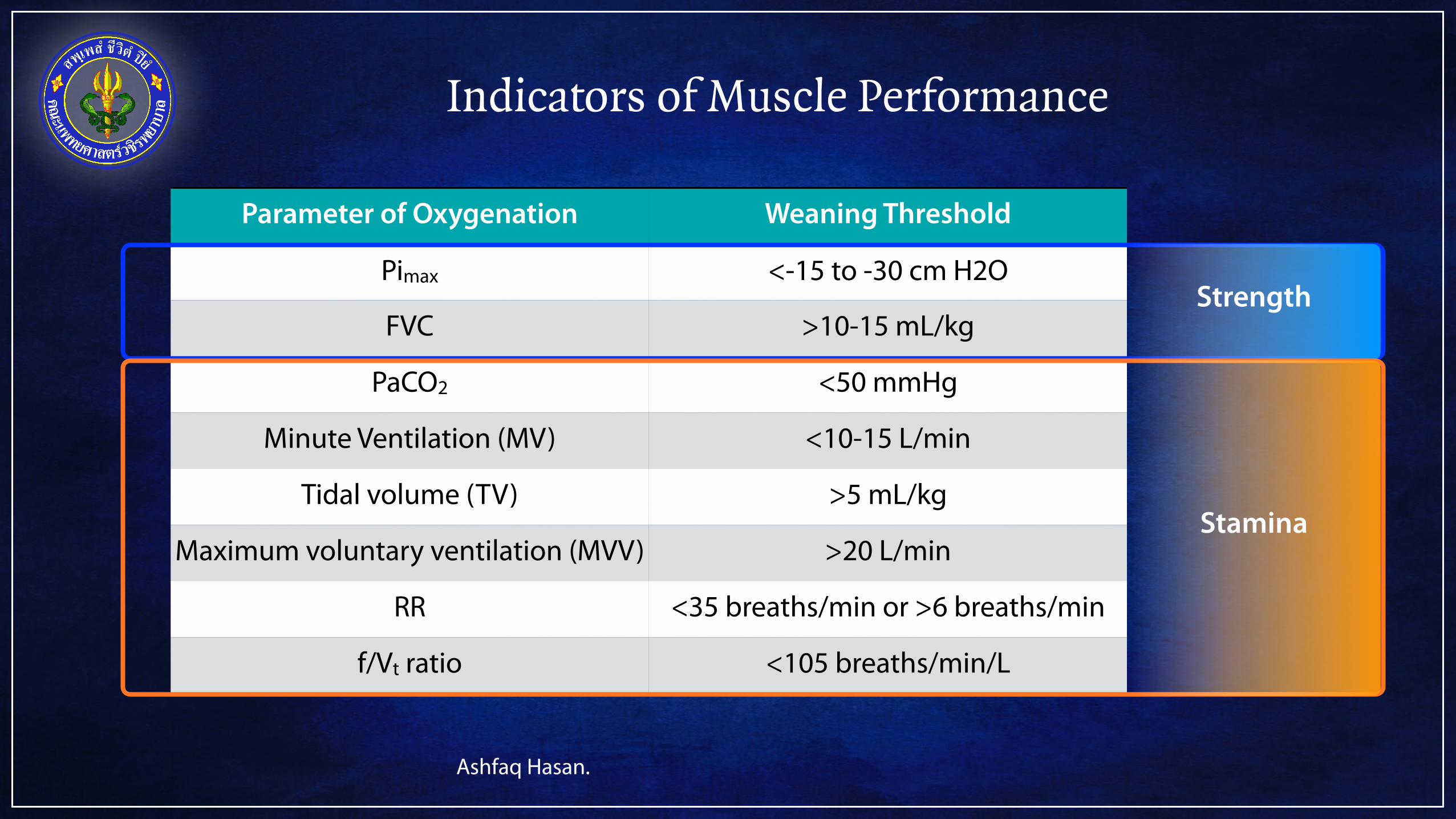
Indicators of Muscle Performance
Parameter of Oxygenation Weaning Threshold
Pimax <-15 to -30 cm H2O
FVC >10-15 mL/kg
PaCO2 <50 mmHg
Minute Ventilation (MV) <10-15 L/min
Tidal volume (TV) >5 mL/kg
Maximum voluntary ventilation (MVV) >20 L/min
RR <35 breaths/min or >6 breaths/min
f/Vt ratio <105 breaths/min/L
Strength
Stamina
Ashfaq Hasan.
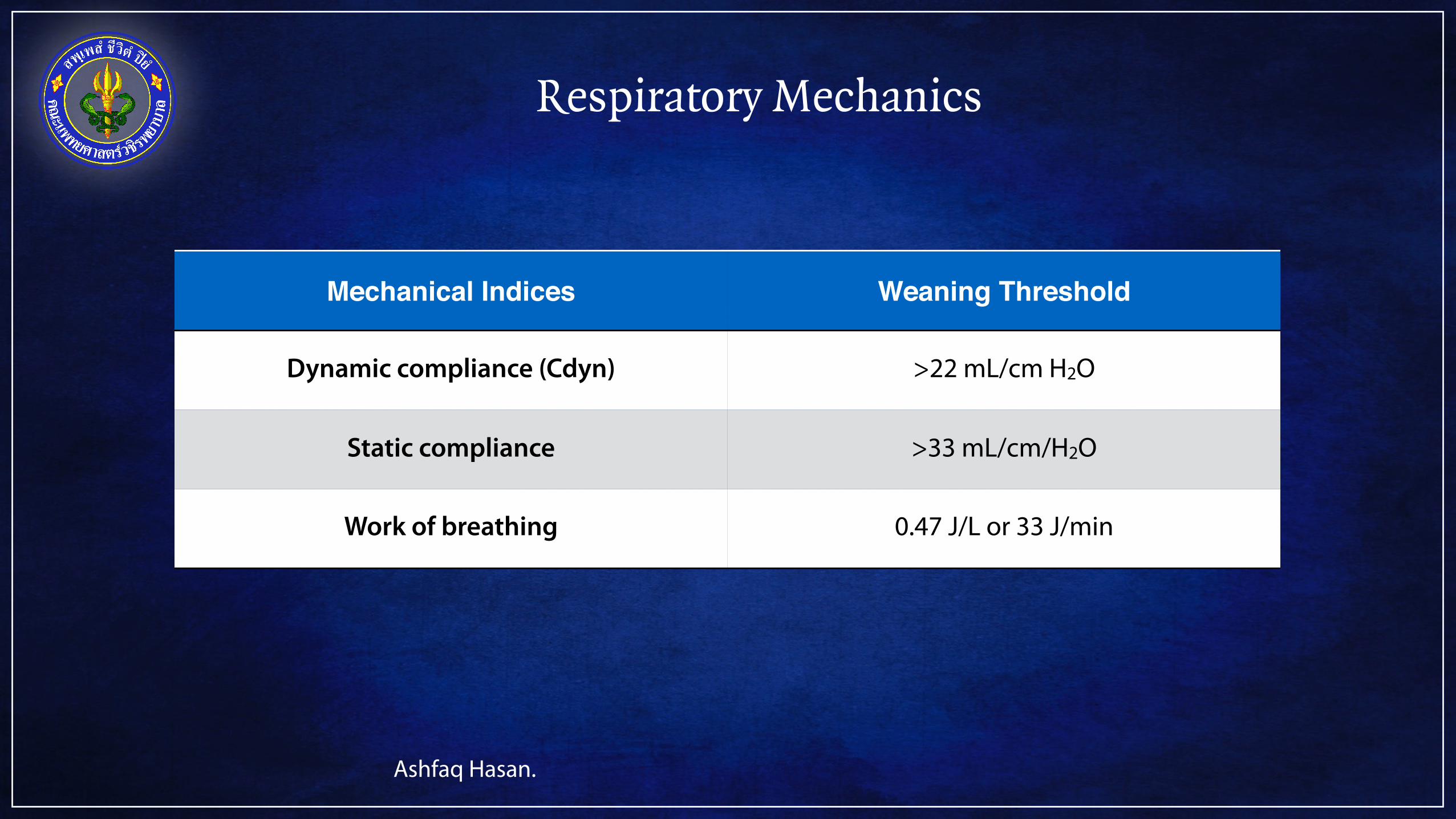
Respiratory Mechanics
Mechanical Indices Weaning Threshold
Dynamic compliance (Cdyn) >22 mL/cm H2O
Static compliance >33 mL/cm/H2O
Work of breathing 0.47 J/L or 33 J/min
Ashfaq Hasan.
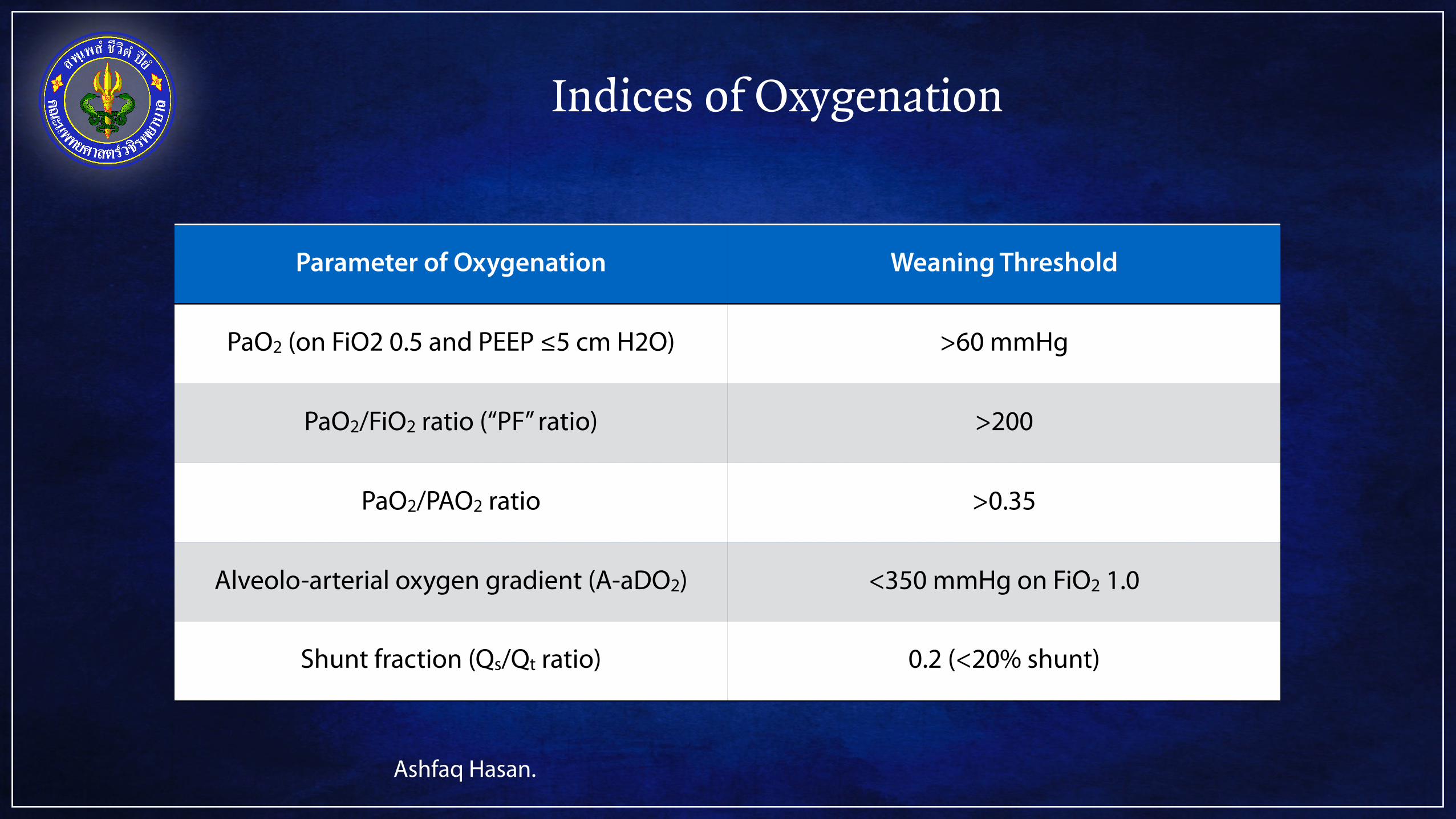
Indices of Oxygenation
Parameter of Oxygenation Weaning Threshold
PaO2 (on FiO2 0.5 and PEEP ≤5 cm H2O) >60 mmHg
PaO2/FiO2 ratio (“PF” ratio) >200
PaO2/PAO2 ratio >0.35
Alveolo-arterial oxygen gradient (A-aDO2) <350 mmHg on FiO2 1.0
Shunt fraction (Qs/Qt ratio) 0.2 (<20% shunt)
Ashfaq Hasan.

Composite Indices
Composite Indices Weaning Threshold Failure Threshold
RSBI (f/Vt) ratio <105 breaths/min/mL >105 breaths/min/mL
CROP index >13 mL/breaths/min N/A
P0.1/Pmax ≤0.9 N/A
SWI <9/min >11/min
RSBICROPSWI
Ashfaq Hasan.
Outlines
Rationale of weaning
Weaning failure
Methods of weaning
Predictors of weaning success/failure
Readiness to Wean
The cause of respiratory failure has improved
The patient is oxygenating adequately
The arterial pH is >7.25
The patient is ale to initiate an inspiratory effort
The patient is hemodynamically stable
No myocardial ischemia
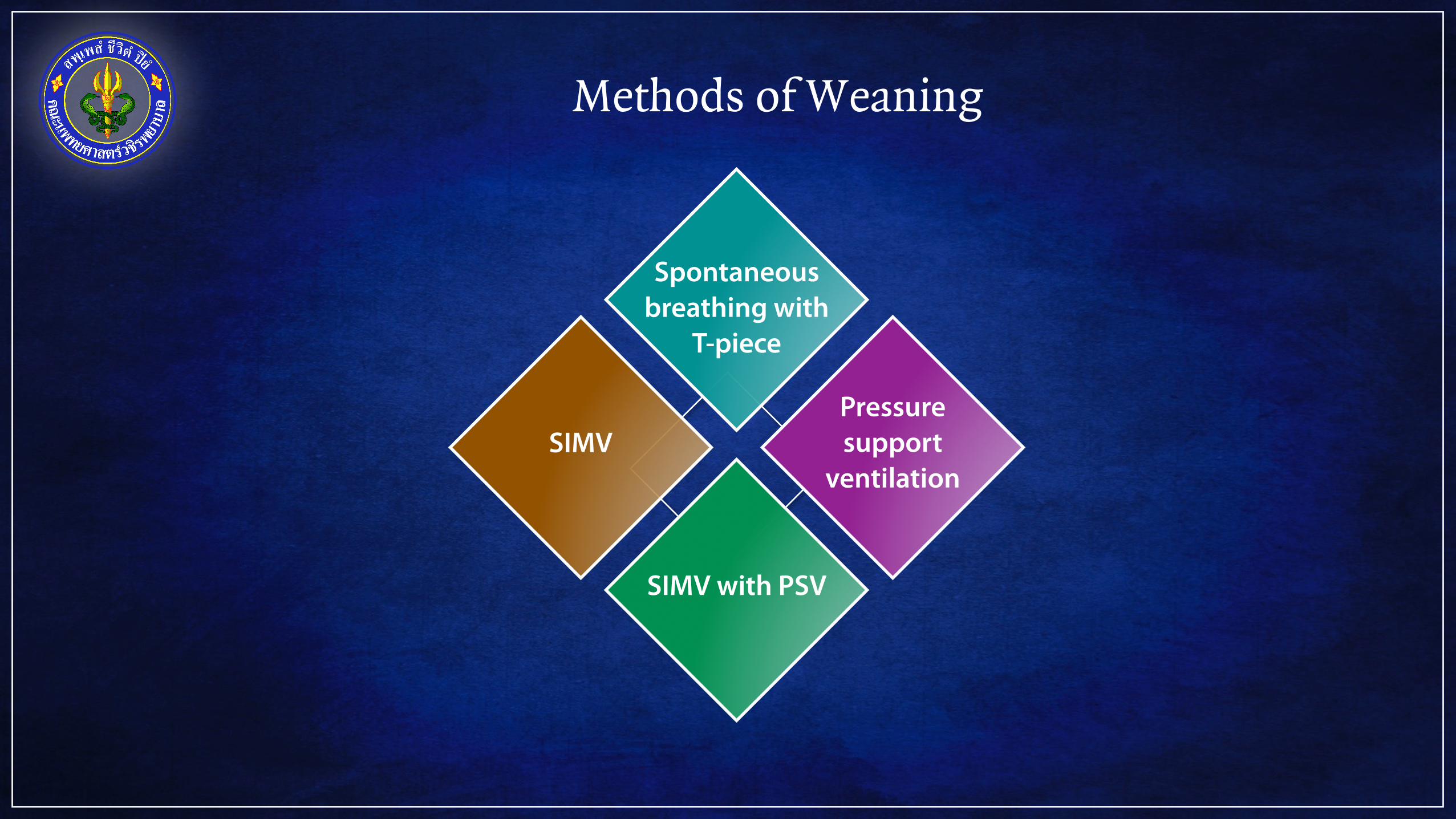
Methods of Weaning
Spontaneous breathing with
T-piece
Pressure support
ventilation
SIMV with PSV
SIMV
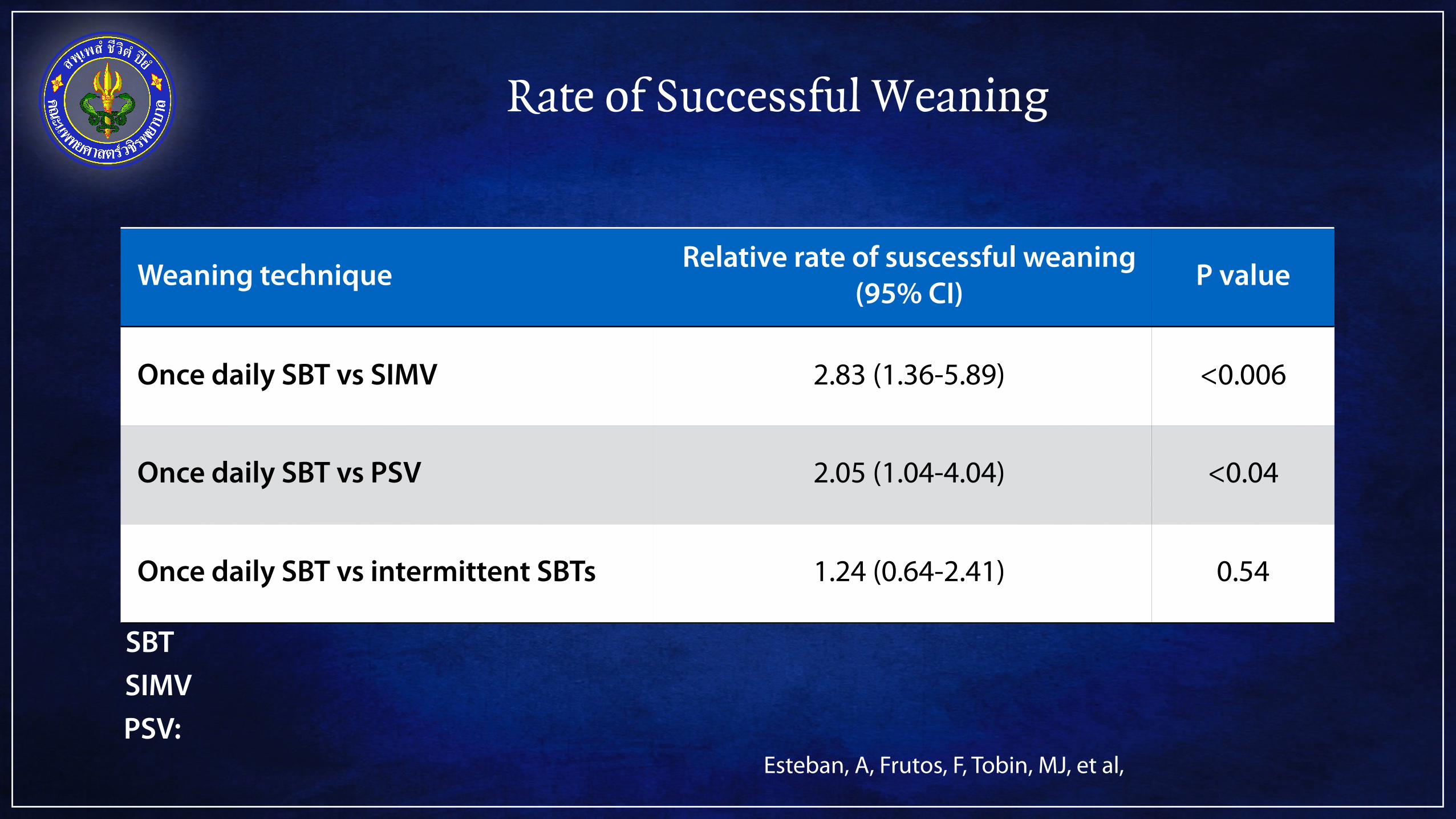
Rate of Successful Weaning
Weaning technique Relative rate of suscessful weaning (95% CI) P value
Once daily SBT vs SIMV 2.83 (1.36-5.89) <0.006
Once daily SBT vs PSV 2.05 (1.04-4.04) <0.04
Once daily SBT vs intermittent SBTs 1.24 (0.64-2.41) 0.54
SBT
Esteban, A, Frutos, F, Tobin, MJ, et al,
SIMVPSV:
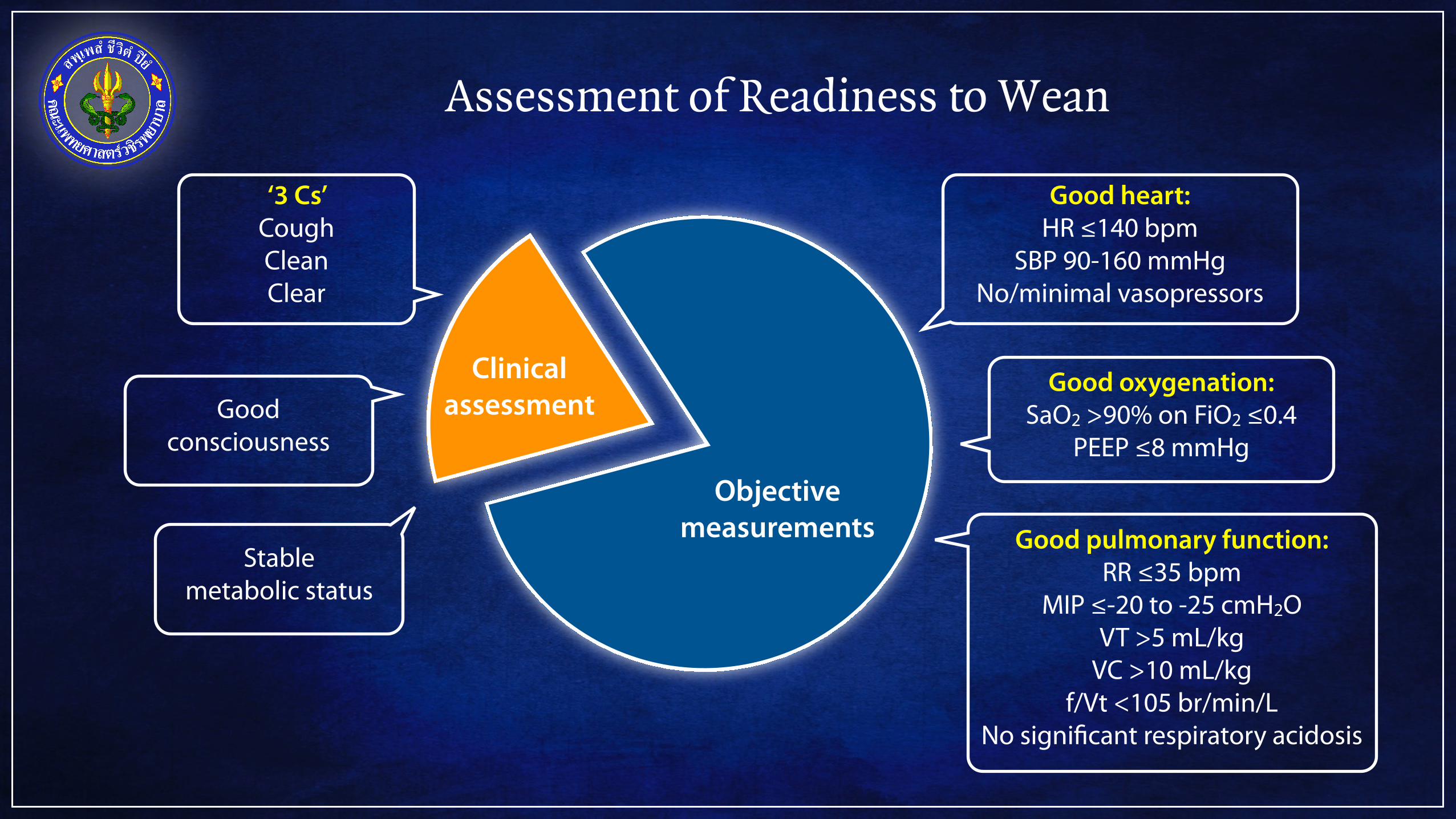
Assessment of Readiness to Wean
Clinical assessment
Objective measurements
Good heart: HR ≤140 bpm
SBP 90-160 mmHg No/minimal vasopressors
Good oxygenation: SaO2 >90% on FiO2 ≤0.4
PEEP ≤8 mmHg
‘3 Cs’ Cough Clean Clear
Good consciousness
Good pulmonary function: RR ≤35 bpm
MIP ≤-20 to -25 cmH2O VT >5 mL/kg
VC >10 mL/kg f/Vt <105 br/min/L
No significant respiratory acidosis
Stable metabolic status
Spontaneous Breathing with T-piece Trial

Weaning with PSV
1 2 3 4 5 6
Record Tidal volume
P peak
Set Level of PS 80-85% of
P peak
Monitor clinical signs periodically
Gradual decrease
PS 2 cmH2O twice per day
PS 6-8 cmH2O PEEP ≤5 cmH2O
T-piece trial or
Extubation
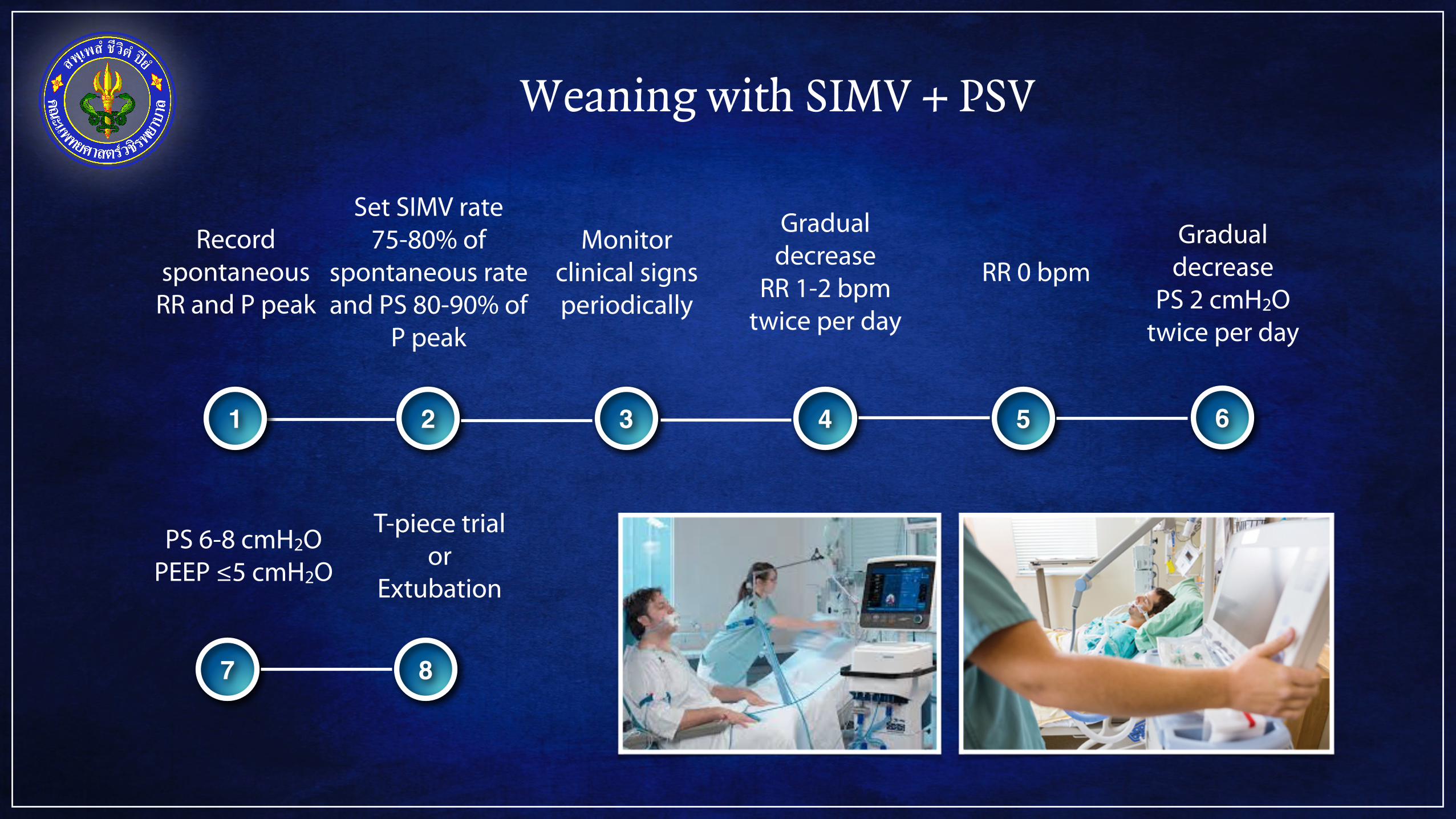
Weaning with SIMV + PSV
1 2 3 4 5 6
Record spontaneous
RR and P peak
Set SIMV rate 75-80% of
spontaneous rate and PS 80-90% of
P peak
Monitor clinical signs periodically
Gradual decrease
RR 1-2 bpm twice per day
RR 0 bpmGradual
decrease PS 2 cmH2O
twice per day
7 8
PS 6-8 cmH2O PEEP ≤5 cmH2O
T-piece trial or
Extubation
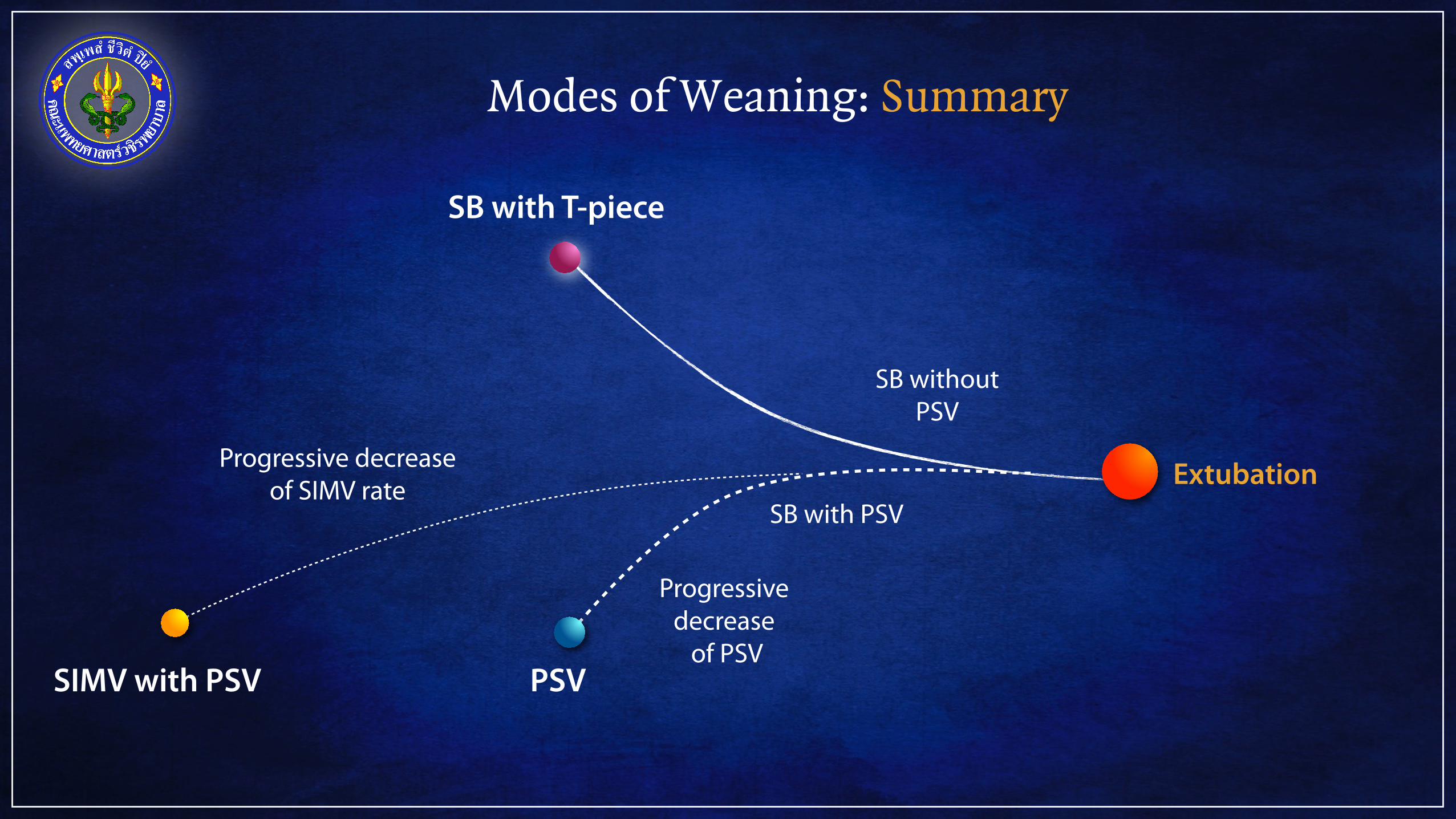
Modes of Weaning: Summary
SIMV with PSV
Progressive decrease of SIMV rate
Progressive decrease
of PSVPSV
SB with PSV
SB with T-piece
SB without PSV
Extubation
Outlines
Rationale of weaning
Weaning failure
Methods of weaning
Predictors of weaning success/failure
Weaning Failure
Either
the failure of Spontaneous breathing trial
or
the need for reintubation within 48 h
following extubation
J-M. Boles et al.
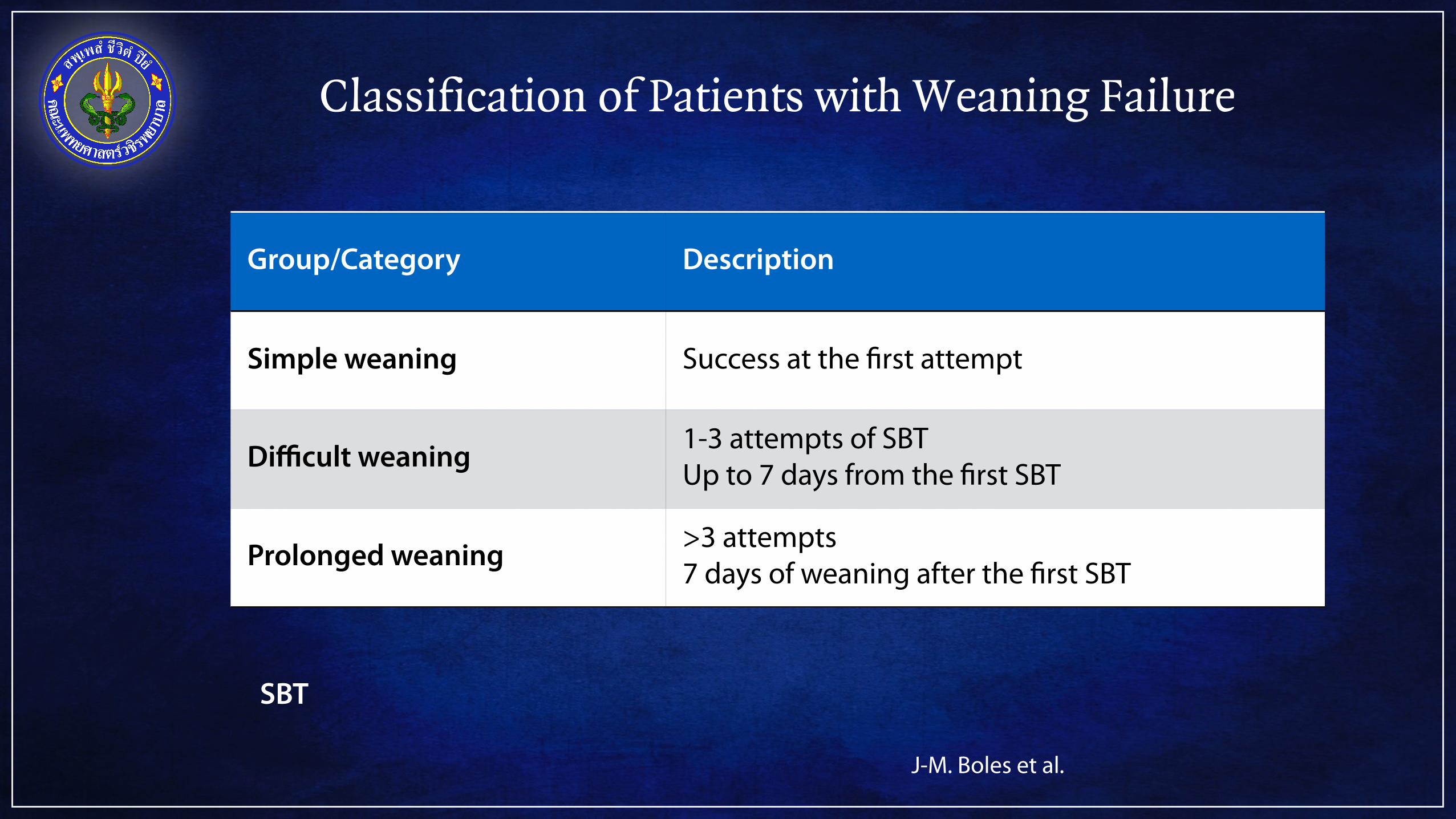
Classification of Patients with Weaning Failure
Group/Category Description
Simple weaning Success at the first attempt
Difficult weaning 1-3 attempts of SBT Up to 7 days from the first SBT
Prolonged weaning >3 attempts 7 days of weaning after the first SBT
SBT
J-M. Boles et al.
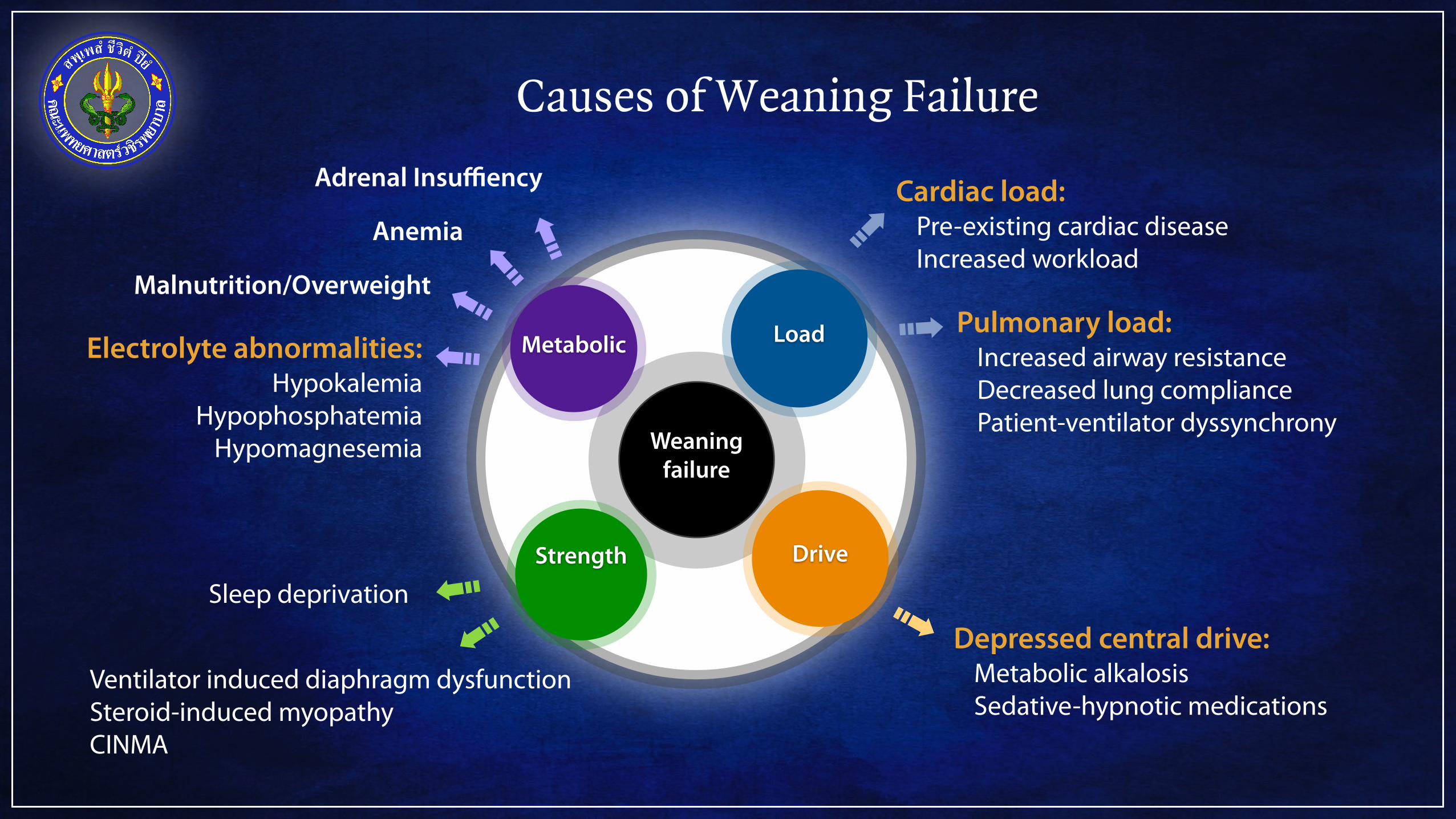
Causes of Weaning Failure
Weaningfailure
LoadMetabolic
Strength Drive
Cardiac load: Pre-existing cardiac disease Increased workload
Pulmonary load: Increased airway resistance Decreased lung compliance Patient-ventilator dyssynchrony
Depressed central drive: Metabolic alkalosis Sedative-hypnotic medications
Electrolyte abnormalities: Hypokalemia
Hypophosphatemia Hypomagnesemia
Ventilator induced diaphragm dysfunction Steroid-induced myopathy CINMA
Malnutrition/Overweight
Anemia
Sleep deprivation
Adrenal Insuffiency
Inadequate Central Drive
Excess sedation
Metabolic alkalosis: Nasogastric suctioning
CNS diseases: Stroke
Encephalitis Encephalopathy
Sleep disordered breathing: central sleep apnea
Obesity hypoventilation syndrome
Cardiogenic Weaning Failure
Oxygen consumption by muscle
Oxygen delivery by the heart=
Oxygen delivery
Stroke volume x HR (O+ (0.0031 x PaO
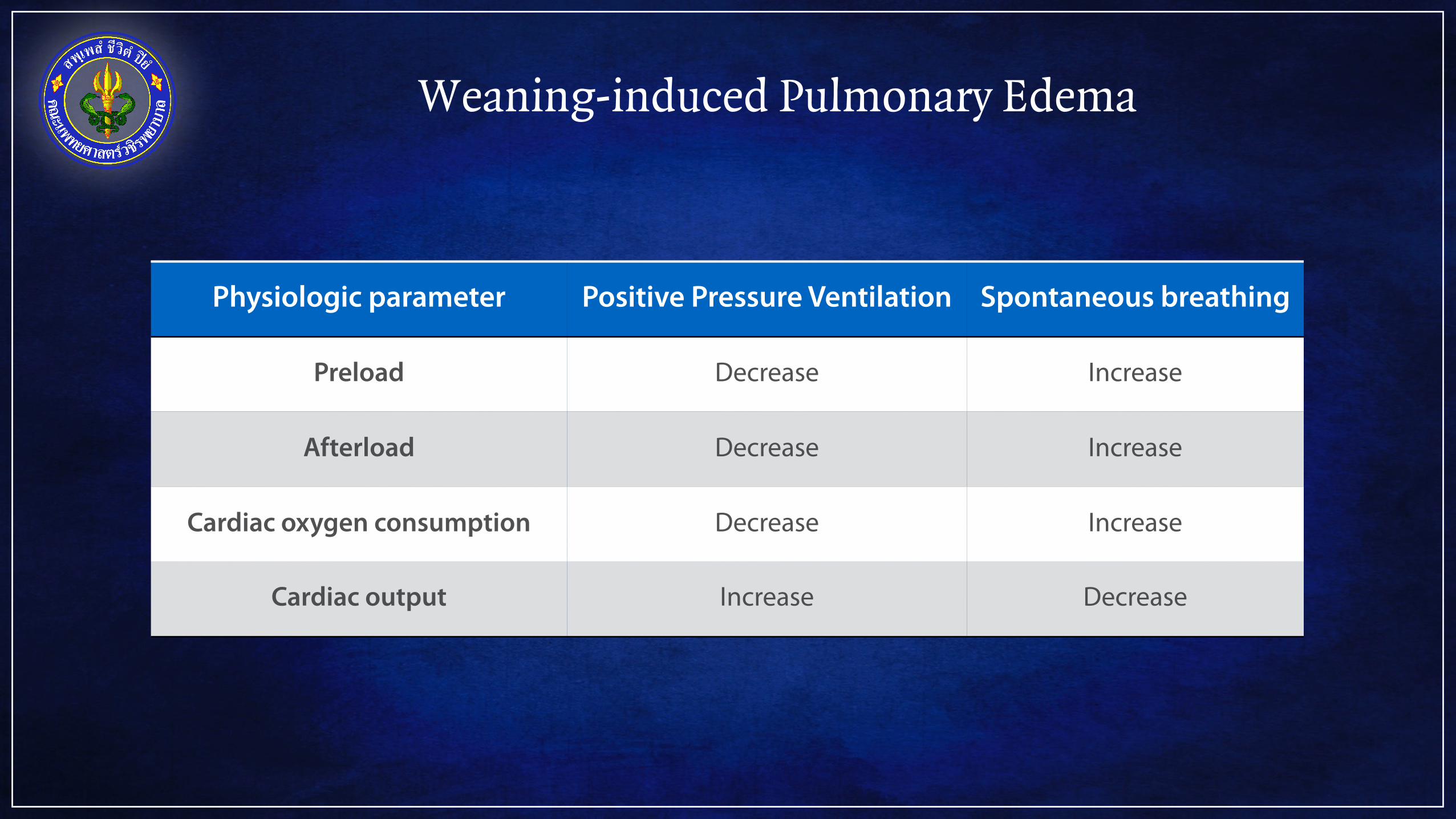
Weaning-induced Pulmonary Edema
Physiologic parameter Positive Pressure Ventilation Spontaneous breathing
Preload Decrease Increase
Afterload Decrease Increase
Cardiac oxygen consumption Decrease Increase
Cardiac output Increase Decrease
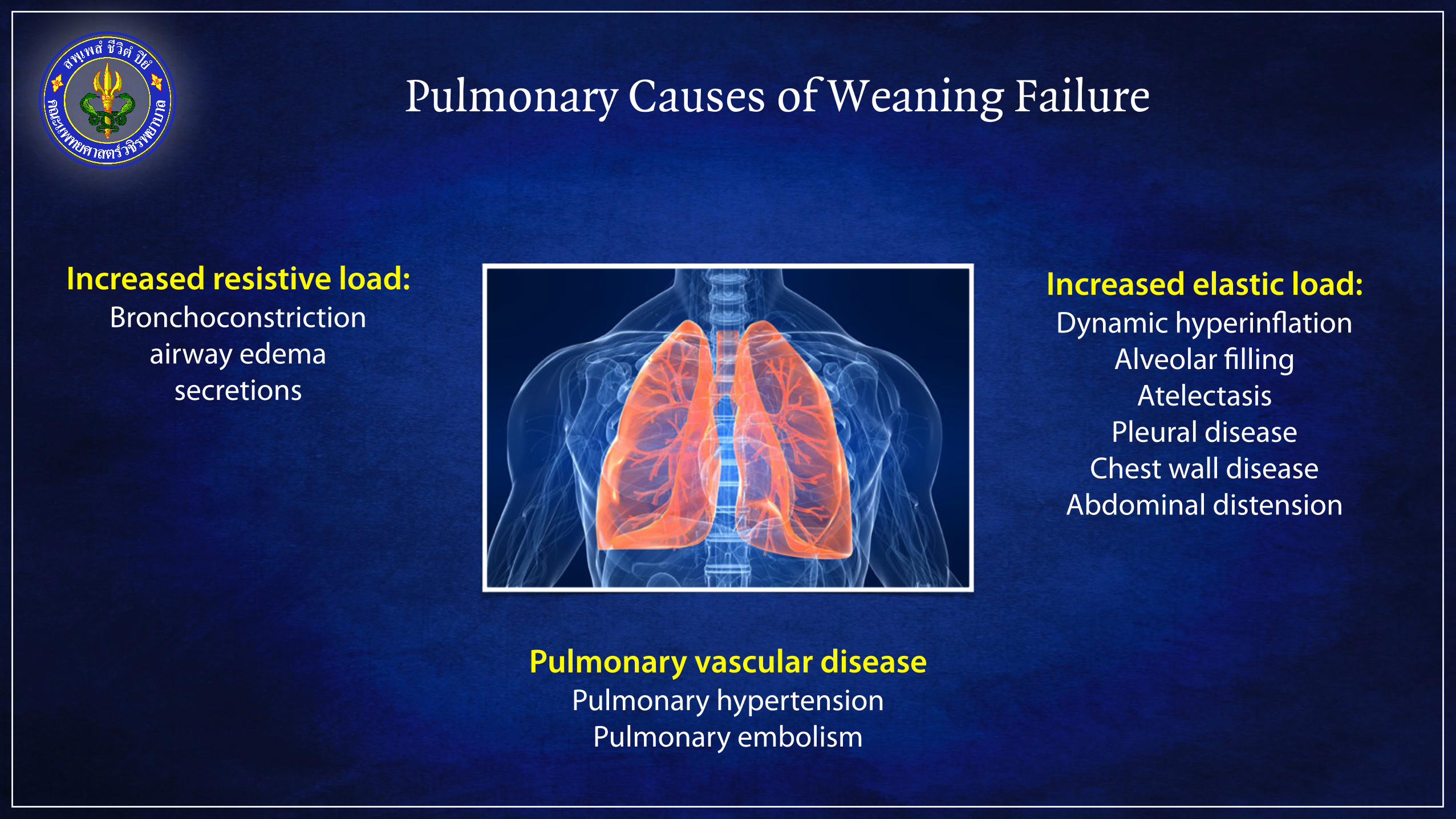
Pulmonary Causes of Weaning Failure
Increased resistive load: Bronchoconstriction
airway edema secretions
Increased elastic load: Dynamic hyperinflation
Alveolar filling Atelectasis
Pleural disease Chest wall disease
Abdominal distension
Pulmonary vascular disease Pulmonary hypertension
Pulmonary embolism
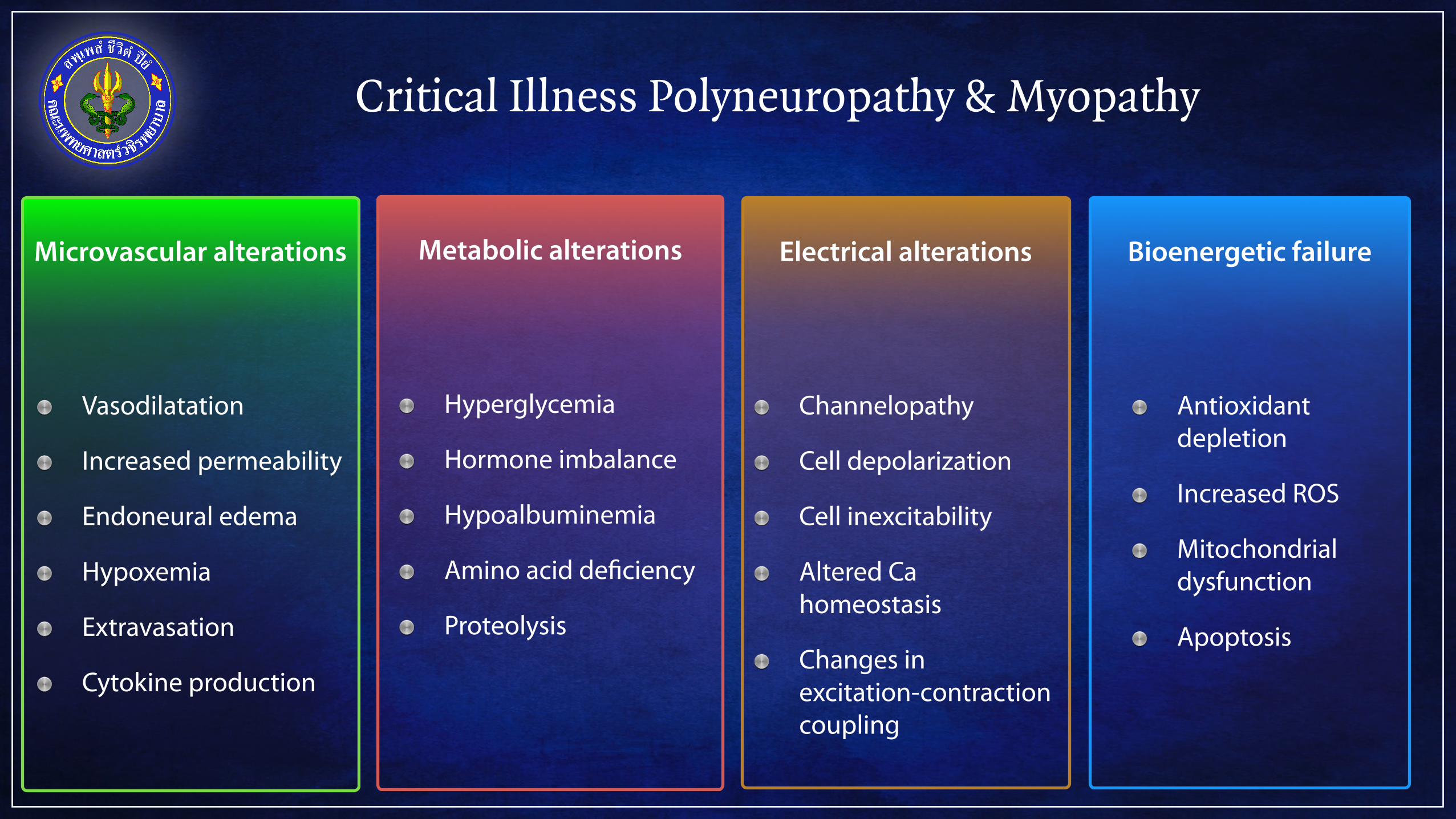
Critical Illness Polyneuropathy & Myopathy
Microvascular alterations
Vasodilatation
Increased permeability
Endoneural edema
Hypoxemia
Extravasation
Cytokine production
Metabolic alterations
Hyperglycemia
Hormone imbalance
Hypoalbuminemia
Amino acid deficiency
Proteolysis
Bioenergetic failure
Antioxidant depletion
Increased ROS
Mitochondrial dysfunction
Apoptosis
Electrical alterations
Channelopathy
Cell depolarization
Cell inexcitability
Altered Cahomeostasis
Changes in excitation-contraction coupling

Sleep Deprivation
Ventilatory response to hypercapnia
Ventilatory response to hypoxia
Increased collapsibility of upper airway
Negative nitrogen balance
Decreased respiratory muscle endurance
Increased oxygen consumption
Increased carbon dioxide production
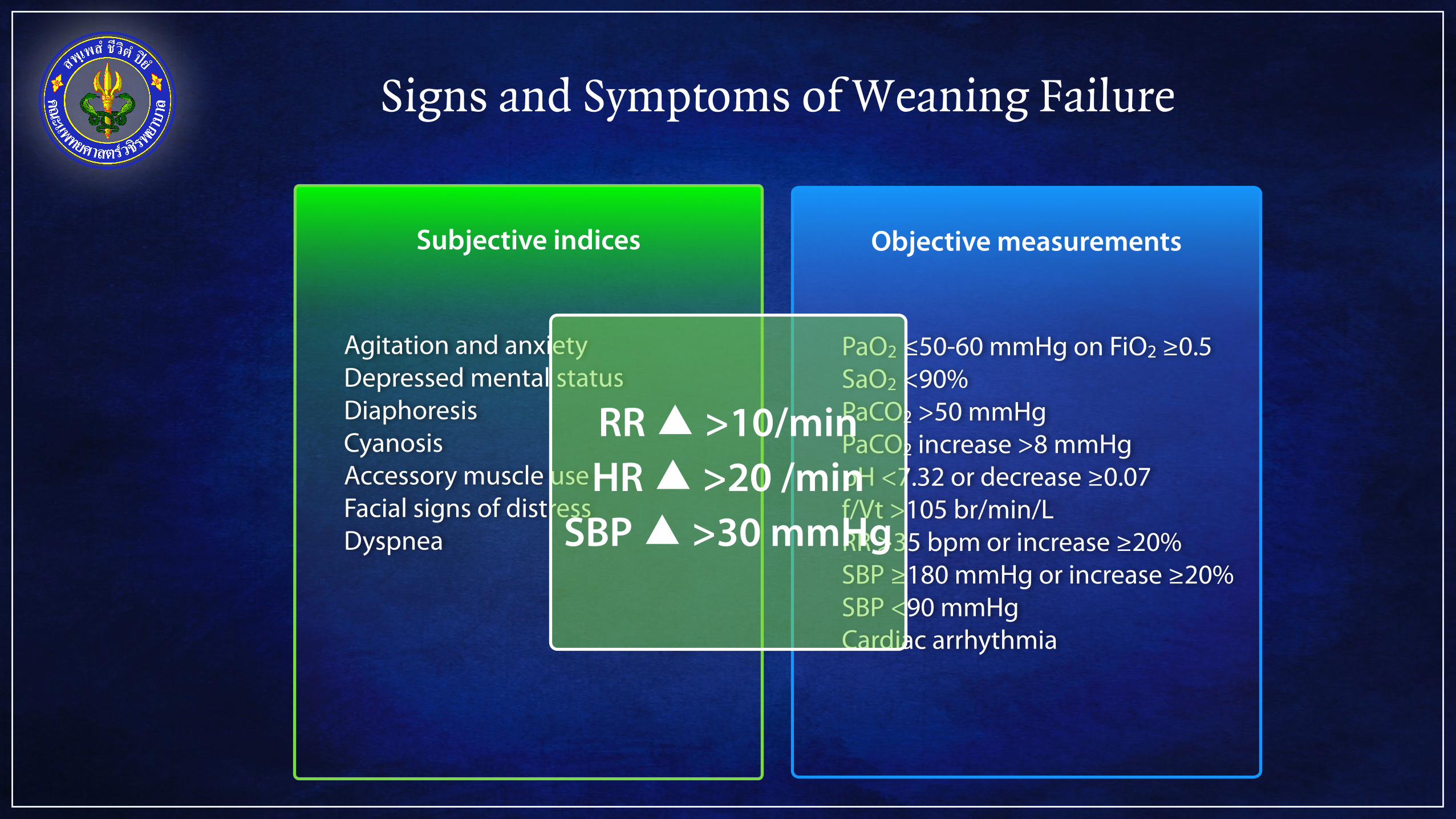
Signs and Symptoms of Weaning Failure
Subjective indices
Agitation and anxiety Depressed mental status Diaphoresis Cyanosis Accessory muscle use Facial signs of distress Dyspnea
Objective measurements
PaO2 ≤50-60 mmHg on FiO2 ≥0.5 SaO2 <90% PaCO2 >50 mmHg PaCO2 increase >8 mmHg pH <7.32 or decrease ≥0.07 f/Vt >105 br/min/L RR >35 bpm or increase ≥20% SBP ≥180 mmHg or increase ≥20% SBP <90 mmHg Cardiac arrhythmia
RR ▲ >10/min HR ▲ >20 /min
SBP ▲ >30 mmHg
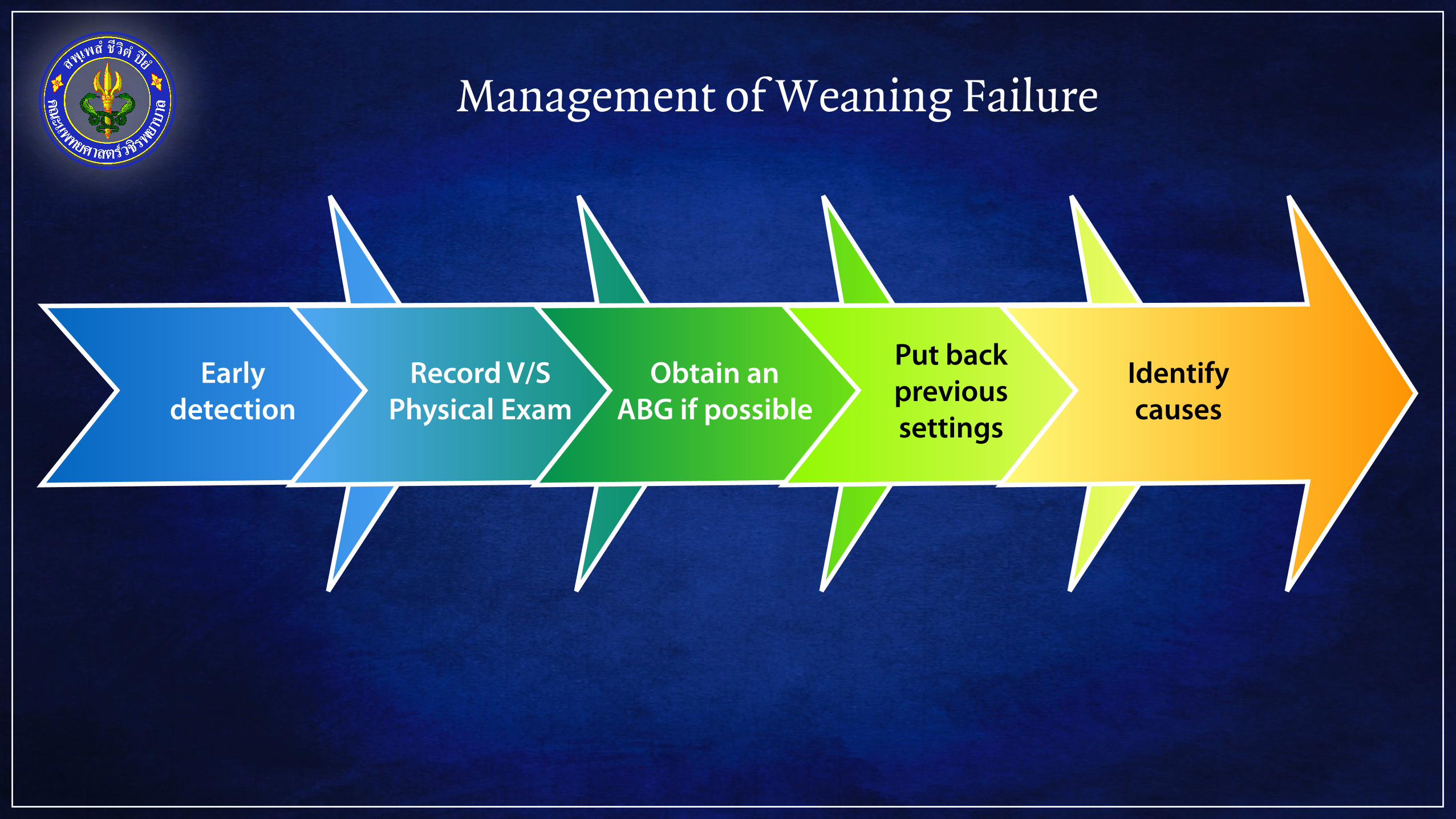
Management of Weaning Failure
Early detection
Record V/S Physical Exam
Obtain an ABG if possible
Put back previous settings
Identify causes
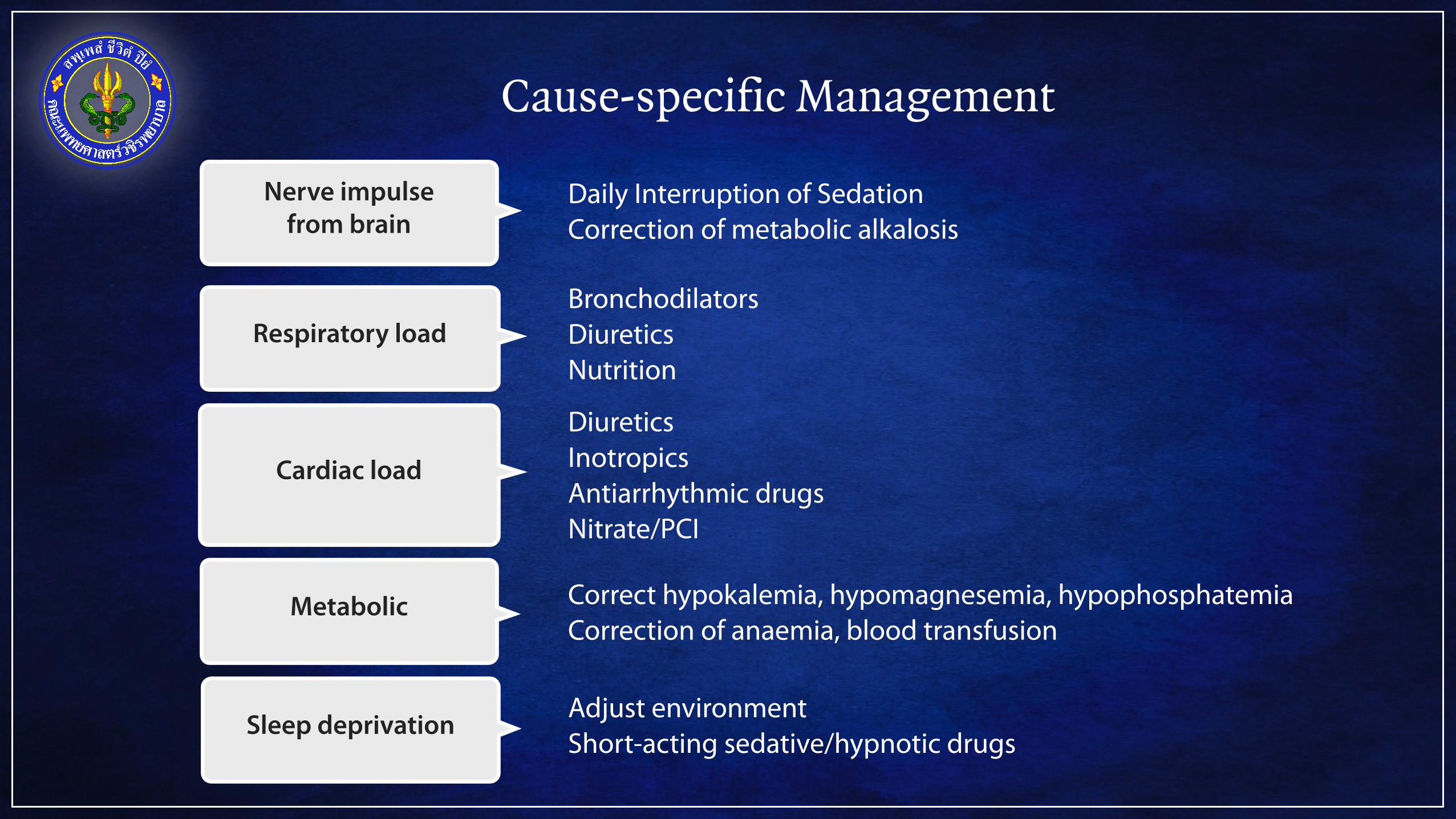
Cause-specific Management
Respiratory load
Nerve impulse from brain
Cardiac load
Metabolic
Daily Interruption of Sedation Correction of metabolic alkalosis
Bronchodilators Diuretics Nutrition
Diuretics Inotropics Antiarrhythmic drugs Nitrate/PCI
Correct hypokalemia, hypomagnesemia, hypophosphatemia Correction of anaemia, blood transfusion
Sleep deprivation Adjust environment Short-acting sedative/hypnotic drugs
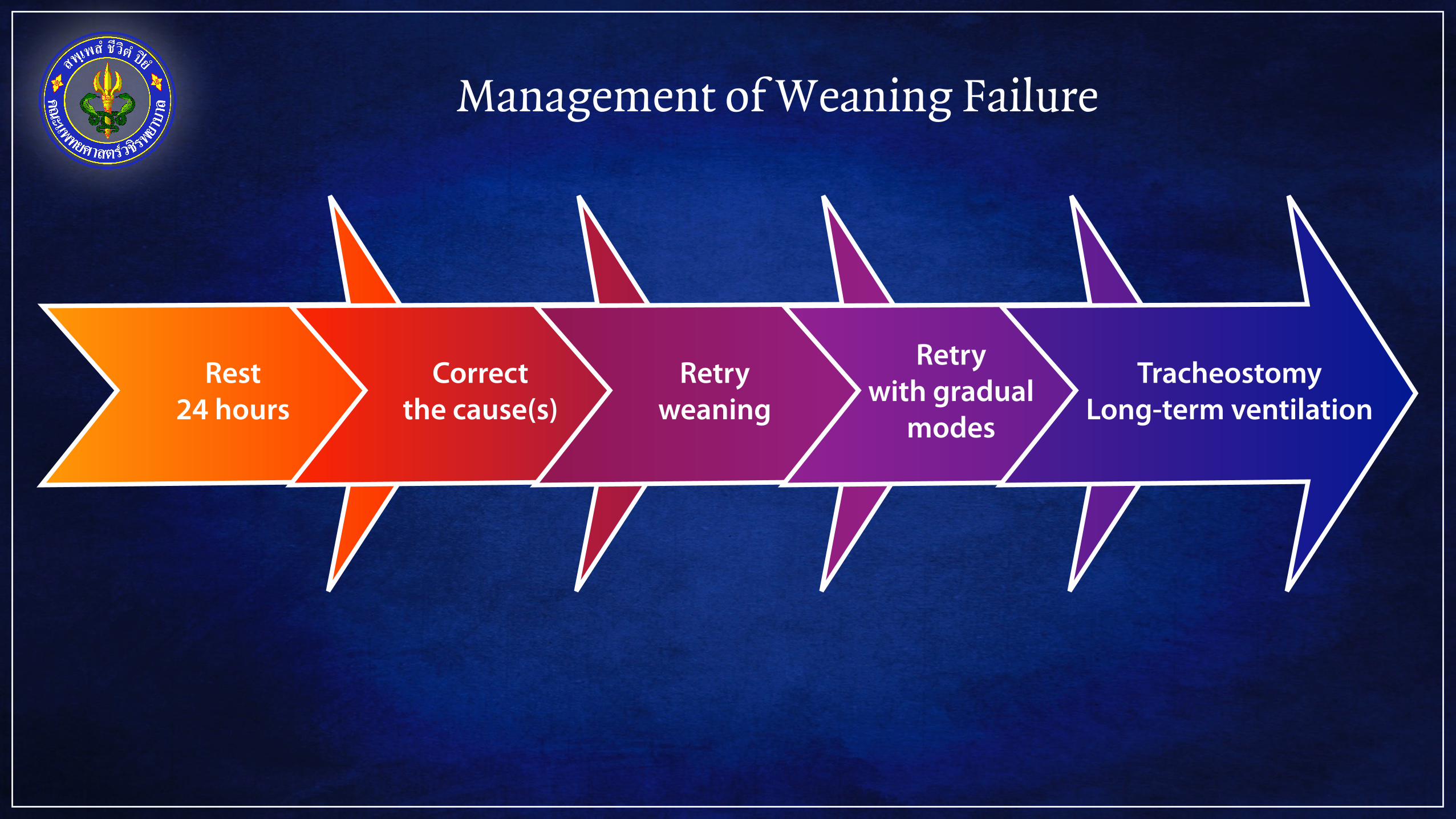
Management of Weaning Failure
Rest24 hours
Correct the cause(s)
Retry weaning
Retry with gradual
modes
Tracheostomy Long-term ventilation
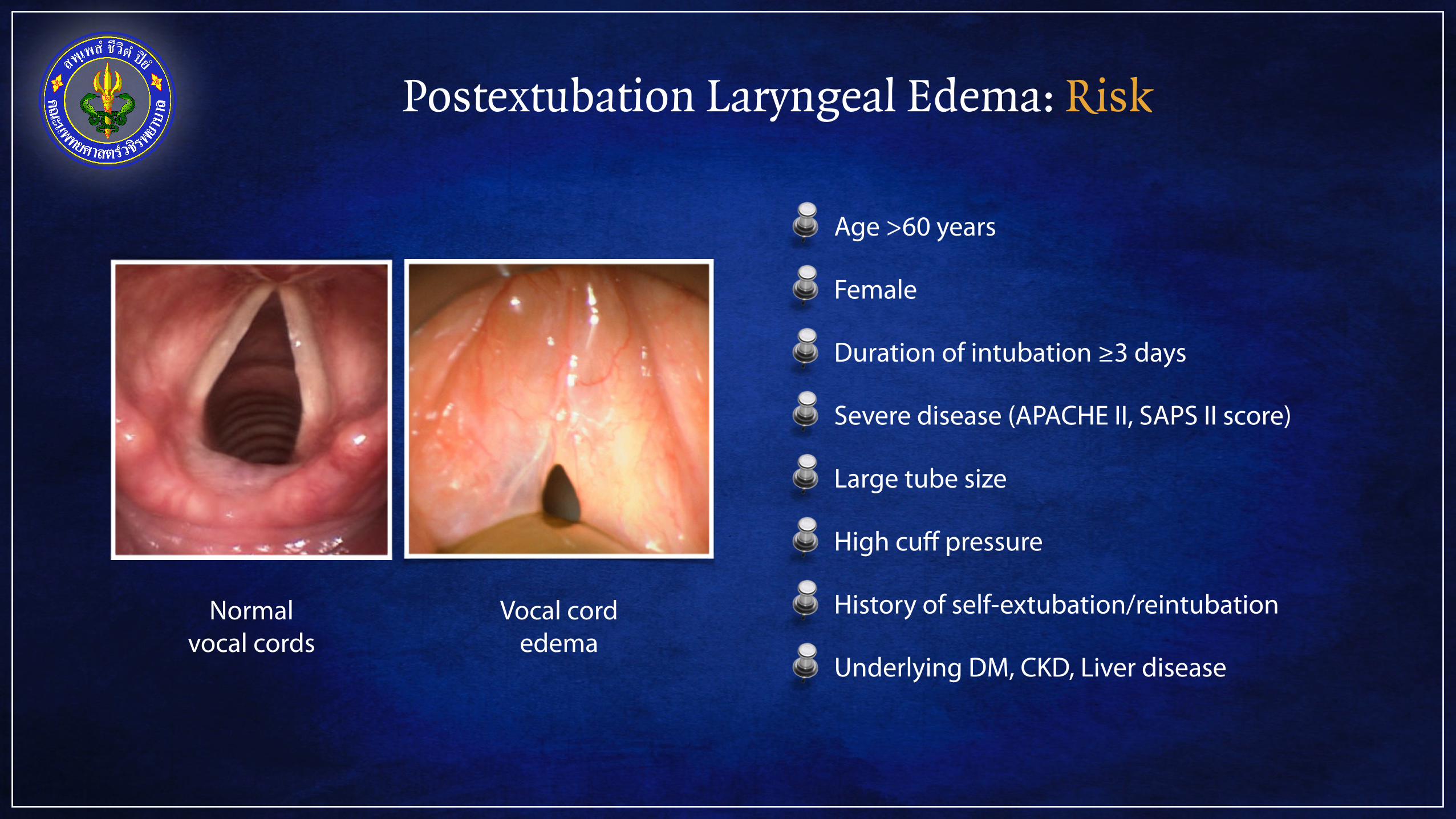
Postextubation Laryngeal Edema: Risk
Normal vocal cords
Vocal cord edema
Age >60 years
Female
Duration of intubation ≥3 days
Severe disease (APACHE II, SAPS II score)
Large tube size
High cuff pressure
History of self-extubation/reintubation
Underlying DM, CKD, Liver disease
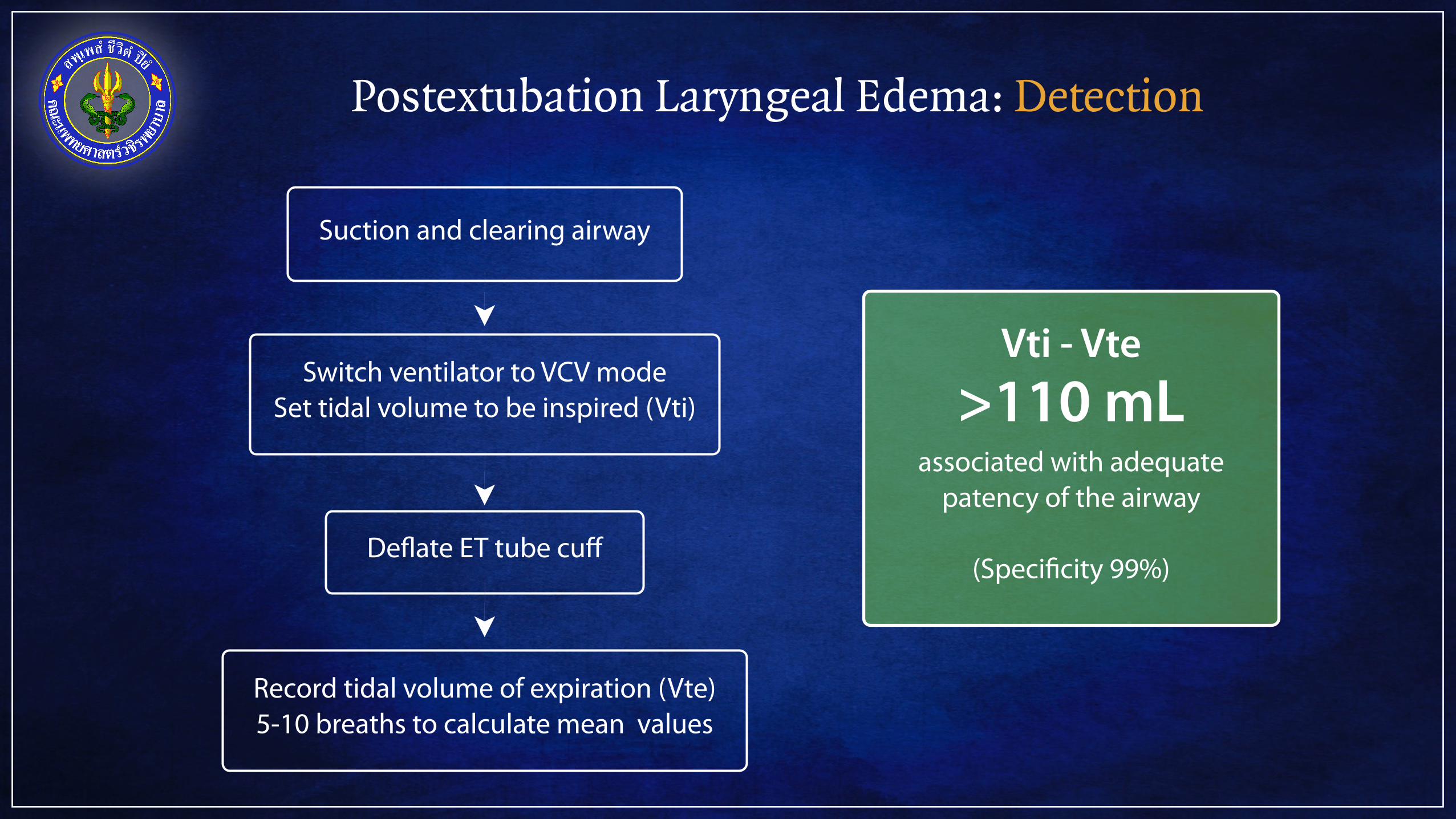
Postextubation Laryngeal Edema: Detection
Suction and clearing airway
Switch ventilator to VCV mode Set tidal volume to be inspired (Vti)
Deflate ET tube cuff
Record tidal volume of expiration (Vte) 5-10 breaths to calculate mean values
Vti - Vte >110 mL
associated with adequate patency of the airway
(Specificity 99%)
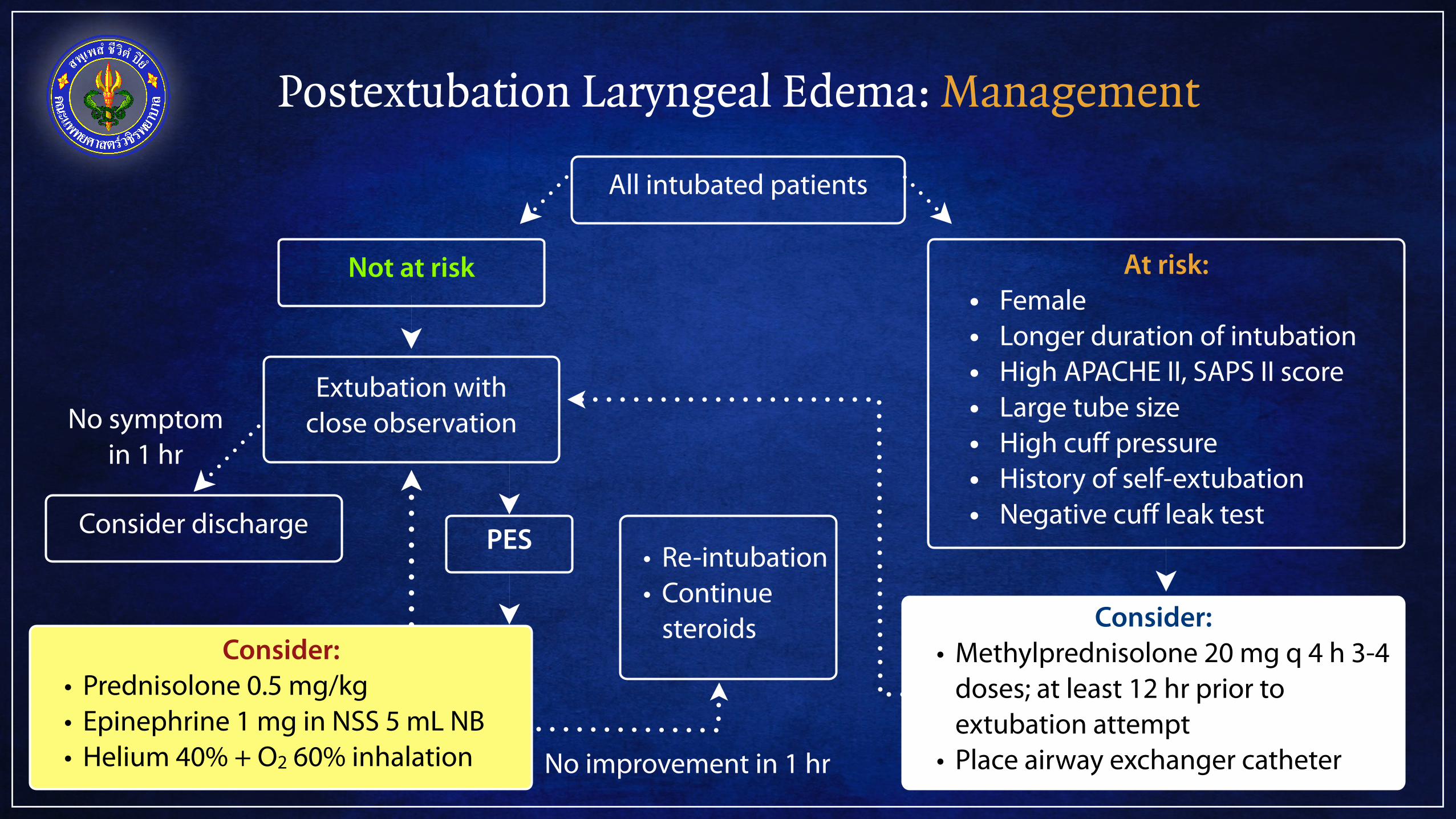
Postextubation Laryngeal Edema: Management
All intubated patients
At risk: • Female • Longer duration of intubation • High APACHE II, SAPS II score • Large tube size • High cuff pressure • History of self-extubation • Negative cuff leak test
Not at risk
Consider: • Methylprednisolone 20 mg q 4 h 3-4
doses; at least 12 hr prior to extubation attempt
• Place airway exchanger catheter
Extubation with close observation
Consider discharge
Consider: • Prednisolone 0.5 mg/kg • Epinephrine 1 mg in NSS 5 mL NB • Helium 40% + O2 60% inhalation
PES • Re-intubation • Continue
steroids
No improvement in 1 hr
No symptom in 1 hr
Thank You