Moving’from’m/eHealth’proof’of ... · 1 PROPHYLAXIS & PREVENTION Client Knowledge 2...
77
‹#› ‹#› Moving from m/eHealth proof of concept studies to national scale: a multistakeholder approach Dr. Garrett Mehl, Scientist, Department of Reproductive Health WHO ERS Consultation The role of e/mHealth in tuberculosis and tobacco control 26 February, 2015
Transcript of Moving’from’m/eHealth’proof’of ... · 1 PROPHYLAXIS & PREVENTION Client Knowledge 2...

‹#›‹#›
Moving from m/eHealth proof of concept studies to national scale: a multi-‐stakeholder approach
Dr. Garrett Mehl, Scientist, Department of Reproductive Health
WHO ERS ConsultationThe role of e/mHealth in tuberculosis and tobacco
control
26 February, 2015

Overview
• Risk adversity to innova(ons
• mHealth as catalyst for health systems
• Pilots as necessary proof of concept for mHealth strategies along con(nuum of scale
• Cri(cal consideraHons in scaling mHealth
• Value drivers in mul(-‐stakeholder partnerships
• What next? Moving toward na(onally-‐scaled integrated m/eHealth systems

Government Choices
Garre@ Mehl: [email protected]
• Government spending on health in low-‐income countries is constrained (>50% African countries = <$14/capita)
• Government decisions on investments in new areas must be evidence-‐based to maximize health impact of limited resources and minimize risk

TB / Tobacco interven>ons of known efficacy exist and are
well described
Package of Essential
Noncommunicable (PEN) Disease
Interventions for
Primary Health Care
in Low-Resource Settings
CANCER
HEART
DISEASE
& STROKE
DIABETES
CHRONIC
RESPIRATORY
DISEASE

LegendmHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons

INTERVENTIONOF)KNOWNEFFICACY
QUALITY)&COVERAGEOF)HEALTH
INTERVENTION
LegendmHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons

INTERVENTIONOF)KNOWNEFFICACY
QUALITY)&COVERAGEOF)HEALTH
INTERVENTION
poor$
demand
for$services
LegendmHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons

INTERVENTIONOF)KNOWNEFFICACY
QUALITY)&COVERAGEOF)HEALTH
INTERVENTION
poor$
demand
for$services
failure(to(
follow(guidelines(Legend
mHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons

INTERVENTIONOF)KNOWNEFFICACY
QUALITY)&COVERAGEOF)HEALTH
INTERVENTION
commodi&es)stockout)
insufficient)workforce)
inaccessibility)of)facili&es
poor$
demand
for$services
failure(to(
follow(guidelines(Legend
mHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons

INTERVENTIONOF)KNOWNEFFICACY
QUALITY)&COVERAGEOF)HEALTH
INTERVENTION
commodi&es)stockout)
insufficient)workforce)
inaccessibility)of)facili&es
poor$
demand
for$services
failure(to(
follow(guidelines(Legend
mHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons

INTERVENTIONOF)KNOWNEFFICACY
QUALITY)&COVERAGEOF)HEALTH
INTERVENTION
commodi&es)stockout)
insufficient)workforce)
inaccessibility)of)facili&es
poor$
demand
for$services
failure(to(
follow(guidelines(Legend
mHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons

INTERVENTIONOF)KNOWNEFFICACY
QUALITY)&COVERAGEOF)HEALTH
INTERVENTION
commodi&es)stockout)
insufficient)workforce)
inaccessibility)of)facili&es
poor$
demand
for$services
failure(to(
follow(guidelines(Legend
mHealth functioningas bridge to overcomespecific constraints to effective coverage
Examples of constraints that reduce potential for achieving coverage and quality of intervention within target populations
mHealth strategies as catalysts for valid health interven>ons
Constraints
mHealth Strategies

1PROPHYLAXIS
& PREVENTION
Client Knowledge
2
DETECTION & DIAGNOSIS
Reach at-risk Populations
Feasible and Accurate
Diagnostic Methods
3
LINKAGE TO CARE
Transport Barriers
Referrals
Financial Barriers
Risk Perception among Clients
4 FOLLOW UP & RETENTION TO
CARE
Referrals
Sustained Motivation
Among Clients
Adherence to Medication Regimen
Regular Check Ups
Financial Barriers
Transport Barriers
6
QUALITY OF CARE
Provider Performance
Access to Key Commodities
Continuity of Care
7
COORDINATION OF CARE
Integrated Data at Different
Levels of Care
Provider-ProviderCommunication
Provider-Client Communication
Disease Surveillance
Health System Performance Monitoring
Challenge Domains Related to TB/NCDs
Adapted: G.S Bloomfield et al. (2014) doi:10.1186/1744-‐8603-‐10-‐49 [email protected]

m/eHealth is not Monolithic: 12 domains of mHealth Usage
1Client(educa-on(&(behaviour(change(communica-on((BCC)
2 Sensors(&(point-of-care(diagnos3cs
3Registries)/)vital)events)tracking
4 Data%collec*on%and%repor*ng%%
Electronic*health*records5
Electronic*decision*support*(informa3on,*protocols,*algorithms,*checklists)
6
Provider(to(providercommunica0on((user(groups,(consulta0on)
7
Provider(workplanning(&(scheduling(
8
9 Provider)training)&)educa1on
Human&resource&management10
Supply&chain&management11
Financial'transac+ons'&'incen+ves12
TECHNICAL CONCEPT
mHealth innovations as health system strengthening tools:12 common applications and a visual frameworkAlain B Labrique,a Lavanya Vasudevan,a Erica Kochi,b Robert Fabricant,c Garrett Mehld
This new framework lays out 12 common mHealth applications used as health systems strengtheninginnovations across the reproductive health continuum.
T he rapid proliferation of mHealth projects—albeitmainly pilot efforts—has generated considerable
enthusiasm among governments, donors, and imple-menters of health programs.1 In many instances, thesepilot projects have demonstrated conceptually howmHealth can alleviate specific health system con-straints that hinder effective coverage of healthinterventions.
Large-scale implementation or integration of thesemHealth innovations into health programs has beenlimited, however, by a shortage of empirical evidencesupporting their value in terms of cost, performance, andhealth outcomes.1–4 Governments in low- and middle-income countries face numerous challenges and com-peting priorities, impeding their ability to adopt innova-tions.2 Thus, they need robust, credible evidence aboutmHealth projects in order to consider mHealth alongsideessential health interventions, and guidance aboutwhich mHealth solutions they should consider toachieve broader health system goals.2 Their tolerancefor system instability or failure can be low, even whenthe status quo may be equally, or more, unreliable.
Current larger-scale effectiveness and implementa-tion research initiatives are working to address theevidence gaps and to demonstrate the impact of mHealthinvestments on health system targets.1 Other efforts areunderway to synthesize such findings.5
MHEALTH AS A HEALTH SYSTEMSSTRENGTHENING TOOL
Recent mHealth reviews have proposed that innovatorsfocus on the public health principles underlying
mHealth initiatives, rather than on specific mHealthtechnologies.6 International agencies and researchorganizations have also endeavored to frame mHealthinterventions within the broader context of healthsystem goals or health outcomes.2 The term ‘‘healthsystem’’ includes all activities in which the primarypurpose is to promote, restore, or maintain health.7
Some elements of a framework for evaluating healthsystems performance by relating the goals of the healthsystem to its essential functions have been proposedpreviously, which we believe can serve as a model forarticulating and justifying mHealth initiatives andinvestments.7
Applying a health systems lens to the evaluation ofmHealth initiatives requires different indicators andmethodologies, shifting the assessment from whetherthe mHealth initiative ‘‘works’’ to process evaluation orproxy indicators of the health outcome(s) of interest.This new way of thinking would facilitate selection ofmHealth tools that are appropriate for identifiedchallenges. In other words, it would drive people tofirst identify the key obstacles, or constraints, todelivering proven health interventions effectively, andto then apply appropriate mHealth strategies thatcould overcome these health system constraints.8
Presenting mHealth as a range of tools for over-coming known health system constraints, as a healthsystems ‘‘catalyst,’’ may also improve communicationbetween mHealth innovators and health programimplementers. Communicating mHealth technologiesas tools that can enhance delivery of life-savinginterventions through improvements in health systemsperformance, such as coverage, quality, equity, orefficiency, will resonate with health decision-makers.7
Hence, rather than being perceived as siloed, stand-alone solutions, mHealth strategies should be viewedas integrable systems that should fit into existinghealth system functions and complement the health
a Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USAb United Nations Children’s Fund (UNICEF), New York City, NY, USAc frog Design, New York City, NY, USAd World Health Organization, Geneva, SwitzerlandCorrespondence to Garrett Mehl ([email protected]).
Global Health: Science and Practice 1
10.9
745/
GH
SP-D
-13-
0003
1 A
dvan
ce A
cces
s Arti
cle
publ
ished
on
Aug
ust 6
, 201
3 as
doi
: G
lob
Hea
lth S
ci P
ract
Ref: Labrique AB, Vasudevan L, Kochi E, Fabricant R, Mehl G. mHealth innovaXons as health system strengthening tools: 12 common applicaXons and a visual framework. Global Health: Science and PracXce. 2013 Aug 15;1(2):160–71.

Source: James Bon-‐Tempo -‐ linearityofexpecta8on.blogspot.ch
The Purpose of ICT for development is to Increase effec>veness or efficiency (or both)

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology Ananya (BBC)
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
WHO mTERG mHealth ClassificaHons
RapidPro

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology Ananya (BBC)
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
WHO mTERG mHealth ClassificaHons
RapidPro

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology Ananya (BBC)
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
WHO mTERG mHealth ClassificaHons
RapidPro

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology Ananya (BBC)
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
WHO mTERG mHealth ClassificaHons
RapidPro

Text-‐it
What is the effect of strategy on interven>on quality and coverage?
WHO mTERG Priority for Evidence

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology MAMA
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
Text-‐it
What is the effect of strategy on interven>on quality and coverage?
WHO mTERG Priority for Evidence

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology MAMA
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
Text-‐it
What is the effect of strategy on interven>on quality and coverage?
WHO mTERG Priority for Evidence

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology MAMA
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
Text-‐it
What is the effect of strategy on interven>on quality and coverage?
WHO mTERG Priority for Evidence

mHealth Technology
technology(ies) (opera(ng system + code + func(ons)
mHealth Strategy
func(on, use, purpose (to address constraints)
Text messages to improve informa8on and demand for ANC
visits
mHealth Project strategy + geo + technology MAMA
Health IntervenHon
Specific Health interven(on targeted for enhanced effect 4 ANC visits
Text-‐it
What is the effect of strategy on interven>on quality and coverage?
WHO mTERG Priority for Evidence

Considera>ons for Evalua>ng mHealth Solu>ons
•At what stage of development is the technology?
•What corresponding stage of evalua>on is appropriate?

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
InnovationsCATALYSTInnovate Evaluate Scale up Improve health

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Generate Ideas
Foster Development
TechnicalSupport
Facilitate strategiclinkages
X
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Generate Ideas
Foster Development
TechnicalSupport
Facilitate strategiclinkages
Research to validate
X
X
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Generate Ideas
Foster Development
TechnicalSupport
Facilitate strategiclinkages
Research to validate
Research Synthesis
Research to op>mize interven>on
X
X
X
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Generate Ideas
Foster Development
TechnicalSupport
Facilitate strategiclinkages
Research to validate
Research Synthesis
Research to op>mize interven>on
Facilitate Scale-‐up
Implementa>on Research
Facilitate Adop>on
X
X
X
X
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Generate Ideas
Foster Development
TechnicalSupport
Facilitate strategiclinkages
Research to validate
Research Synthesis
Research to op>mize interven>on
Facilitate Scale-‐up
Implementa>on Research
Facilitate Adop>on
X
X
X
X
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Mechanisms thatFacilitate widespread adop>on
X
Facilitate ins>tu>onaliza>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Generate Ideas
Foster Development
TechnicalSupport
Facilitate strategiclinkages
Research to validate
Research Synthesis
Research to op>mize interven>on
Facilitate Scale-‐up
Implementa>on Research
Facilitate Adop>on Mechanisms thatFacilitate widespread adop>on
X
X
X
X
X
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Facilitate ins>tu>onaliza>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health
Proof of concept -‐ valida>on

maturity
expecta,ons
1: Trigger2: Peak
of InflatedExpectations
3: Trough ofDisillusionment 4: Slope of Enlightenment 5: Plateau of
Productivity
Generate Ideas
Foster Development
TechnicalSupport
Facilitate strategiclinkages
Research to validate
Research Synthesis
Research to op>mize interven>on
Facilitate Scale-‐up
Implementa>on Research
Facilitate Adop>on Mechanisms thatFacilitate widespread adop>on
X
X
X
X
X
Innova>ons “Lifecycle”, and strategic ques>ons related to
maturity of solu>on
Facilitate ins>tu>onaliza>on
Solu>ons?
Efficacious?
Effec>ve?
Regulatory Approval?
GuidelinesNeeded?
Barriers to Adop>on?
Cost effec>ve?
MOH Adop>on?Sustainable?
Value compared with alterna>ves?
Ins>tu>onalized?
Replica>on occurring?
InnovationsCATALYSTInnovate Evaluate Scale up Improve health
Post-‐efficacy:Adop>on, Scale,
Ins>tu>onaliza>on,Replica>on, Sustainability

“Maturity” of the mHealth Project
Amou
nt of InformaX
on (R
ED)
Threshold of “Informa:on”
Stability FuncXonality Useability Efficacy EffecXveness
“Evidence” threshold at each stage across The mHealth maturity lifecycle
OF WHAT ?

“Maturity” of the mHealth Project
Amou
nt of InformaX
on (R
ED)
Threshold of “Informa:on”
Stability FuncXonality Useability Efficacy EffecXveness
Methodology
Systems Engineering QualitaXve QuanXtaXve Mixed Q/Q / M&E
“Evidence” threshold at each stage across The mHealth maturity lifecycle
OF WHAT ?
MEASURED HOW ?

WHO mTERG for RMNCH Monitoring and Evalua>on Ques>ons by Maturity Phase

FuncXonality: does the
m/eHealth tool funcXon as intended?
QuesHons: Can they use the m/eHealth tool?
Can they demonstrate ability to use the tool?
•Technical factors•OrganizaXonal factors
WHO mTERG for RMNCH Monitoring and Evalua>on Ques>ons by Maturity Phase

FuncXonality: does the
m/eHealth tool funcXon as intended?
QuesHons: Can they use the m/eHealth tool?
Can they demonstrate ability to use the tool?
•Technical factors•OrganizaXonal factors
Usability: How do users interact with m/eHealth
tool?
QuesHons: Do Health Workers actually use it?
Do they perceive benefits using the app?
•User Coverage•User Response•User AdopXon
WHO mTERG for RMNCH Monitoring and Evalua>on Ques>ons by Maturity Phase

FuncXonality: does the
m/eHealth tool funcXon as intended?
QuesHons: Can they use the m/eHealth tool?
Can they demonstrate ability to use the tool?
•Technical factors•OrganizaXonal factors
Usability: How do users interact with m/eHealth
tool?
QuesHons: Do Health Workers actually use it?
Do they perceive benefits using the app?
•User Coverage•User Response•User AdopXon
WHO mTERG for RMNCH Monitoring and Evalua>on Ques>ons by Maturity Phase
Effect: How does the mHealth tool improve health service delivery?
QuesHons:Are there system improvements resulXng from health workers’ use of mHealth tool?
•Availability•Cost•Efficiency•Quality•UXlizaXon

FuncXonality: does the
m/eHealth tool funcXon as intended?
QuesHons: Can they use the m/eHealth tool?
Can they demonstrate ability to use the tool?
•Technical factors•OrganizaXonal factors
Usability: How do users interact with m/eHealth
tool?
QuesHons: Do Health Workers actually use it?
Do they perceive benefits using the app?
•User Coverage•User Response•User AdopXon
Outcomes: Does m/eHealth tool improvements in service delivery affect health?
QuesHons: Are there improved health outcomes resulXng from use across mulXple workers?
•Improved health outcomes
WHO mTERG for RMNCH Monitoring and Evalua>on Ques>ons by Maturity Phase
Effect: How does the mHealth tool improve health service delivery?
QuesHons:Are there system improvements resulXng from health workers’ use of mHealth tool?
•Availability•Cost•Efficiency•Quality•UXlizaXon

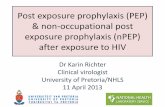
TB/HIV Treatment Care Cascade
Adapta:on from: C.P. Hudson. Bulle:n of the World Health Organiza:on, 2001, 79 (1)
100%
50%
35%
30%
6%
4%
3%
1%
Acquire TB
Access TesXng facility
Diagnosed with TB
Prescribed adequate TB Treatment
Begin Treatment within 2 weeksComplete Treatment
Treatment effecXve
TransiXon to long term HIV care
Popula8on

mHealth innova>ons to overcome Health Service and Knowledge Gaps
Adapta:on from: C.P. Hudson. Bulle:n of the World Health Organiza:on, 2001, 79 (1)
Poten>al mHealth solu>ons
Reminders, incen>ves to complete treatment
Educa>on, incen>ve
Quality of Care: Point of Care Diagnos>c tool
Incen>ve to seek treatment
Iden>fy closest ado-‐friendly Facility
Informa>on, Self Screen via mobile
Register All Clients
100%
50%
35%
30%
6%
4%
3%
1%
Acquire TB
Access TesXng facility
Diagnosed with TB
Prescribed adequate TB Treatment
Begin Treatment within 2 weeksComplete Treatment
Treatment effecXve
TransiXon to long term HIV care
Popula8on

Poten>al interven>on improvement resul>ng from mHealth strategies
Poten>al mHealth solu>ons
Reminders, incen>ves to complete treatment
Educa>on, incen>ve
Quality of Care: Point of Care Diagnos>c tool
Incen>ve to seek treatment
Iden>fy closest ado-‐friendly Facility
Informa>on, Self Screen via mobile
7%
3%
18%
40%
50%
65%
Popula8on
100%
50%
35%
30%
6%
4%
3%
1%
Acquire TB
Access TesXng facility
Diagnosed with TB
Prescribed adequate TB Treatment
Begin Treatment within 2 weeksComplete Treatment
Treatment effecXve
TransiXon to long term HIV care

ConsideraHons for m/eHealth on journey
to naHonal scale

Scaling up what?
•mHealth Technology
• mHealth Strategy
• mHealth Project
Innovate Evaluate Scale up Improve health

mHealth Evidence Needs

mHealth Category Evidence needs/value
mHealth Technology Stability, scale, diversity of usage....
mHealth Strategy Evidence of impact?
mHealth Project Specific use case, usability assessment, implementa(on details, efficacy
mHealth Evidence Needs

mHealth Category Evidence needs/value
mHealth Technology Stability, scale, diversity of usage....
mHealth Strategy Evidence of impact?
mHealth Project Specific use case, usability assessment, implementa(on details, efficacy
mHealth Evidence Needs

mHealth Category Evidence needs/value
mHealth Technology Stability, scale, diversity of usage....
mHealth Strategy Evidence of impact?
mHealth Project Specific use case, usability assessment, implementa(on details, efficacy
mHealth Evidence Needs

mHealth Category Evidence needs/value
mHealth Technology Stability, scale, diversity of usage....
mHealth Strategy Evidence of impact?
mHealth Project Specific use case, usability assessment, implementa(on details, efficacy
mHealth Evidence Needs

“C O R R E C T” ExpandNET AQributes of “Scaleability”• Credible in that they are based on sound evidence and/or advocated
by respected persons or ins4tu4ons
• Observable to ensure that poten4al users can see the results in prac4ce
• Relevant for addressing persistent or sharply felt problems
• RelaHve advantage over exis4ng prac4ces so that poten4al users are convinced the costs of implementa4on are warranted by the benefits
• Easy to install and understand rather than complex and complicated
• CompaHble with the poten4al users’ established values, norms and facili4es; fit well into the prac4ces of the na4onal programme
• Testable so that poten4al users can see the interven4on on a small scale prior to large-‐scale adop4on

The WHO M.A.P.S. Tool:mHEALTH Assessment and
Planning for Scale
Tools for:•Standard Tools for describing mHealth scale-‐up•Qualita(ve self assessment and planning; •Quan(ta(ve measurement and planning
Development and Valida8on:Informed by WHO RHR research support to 26 mHealth projects under UN IWG cataly(c grant mechanism

MAPS Integrated Framework of Scale for mHealth: Axes
1 2 3 4 5 6

Axis I. Groundwork1. Does the m/eHealth tool have a clear
theory of change and a roadmap for scale, with a clearly arNculated endgame ?
1

Axis II. PartnershipsIs the ENVIRONMENT supporNve of the m/eHealth tool expansion by:
• government, target user, and private sector engagement ?
2

Stakeholder Value DriversStakeholder IllustraHve examples Evidence required Key decision
DonorsDFID, Rockefeller FoundaHon,
Bill and Melinda Gates FoundaHon, etc.
PotenHal for health outcome or populaHon benefit; sustainability
Investment, promoHon
Private sectorMobile network operators, PharmaceuHcal companies,
medical device manufacturers
PotenHal return on investment Investment
Regulator FDA Risk, safety versus benefit Market authorizaHon
Health Technical Agency WHO EffecHveness, clinical
outcome
CreaHon of clinical guidelines; best pracHces
established
MOH and Payers Ministries of health, insurance companies
Value for money; system benefits; relevance to government goals
Reimbursement; eligibility for treatment;
budget line
Health-‐care Professionals
Health workers, NGOs, Professional bodies
Clinical outcome; cost-‐effecHveness AdopHon of innovaHons
Pa<ents/end-‐users Clients, Family members Usability; perceived
benefit; preferenceUHlizaHon of innovaHon; personal investment
adapted from GSMA, 2011

Axis V. Opera8onsIs the PROJECT able to expand and sustain growth given: current human resource and implementa>on requirements?
5

Poten>al interven>on improvement resul>ng from mHealth strategies
Adapta:on from: C.P. Hudson. Bulle:n of the World Health Organiza:on, 2001, 79 (1)
Poten>al mHealth solu>ons
Reminders, incen>ves to complete treatment
Educa>on, incen>ve
Quality of Care: Point of Care Diagnos>c tool
Incen>ve to seek treatment
Iden>fy closest ado-‐friendly Facility
Informa>on, Self Screen via mobile
7%
3%
18%
40%
50%
65%
Popula8on
100%
50%
35%
30%
6%
4%
3%
1%
Acquire TB
Access TesXng facility
Diagnosed with TB
Prescribed adequate TB Treatment
Begin Treatment within 2 weeksComplete Treatment
Treatment effecXve
TransiXon to long term HIV care

Degraded impact due to implementa>on weaknesses
Adapta:on from: C.P. Hudson. Bulle:n of the World Health Organiza:on, 2001, 79 (1)
Poten>al mHealth solu>ons
Reminders, incen>ves to complete treatment
Educa>on, incen>ve
Quality of Care: Point of Care Diagnos>c tool
Incen>ve to seek treatment
Iden>fy closest ado-‐friendly Facility
Informa>on, Self Screen via mobile
Register All Clients
5%
2%
12%
35%
40%
55%
Popula8on
100%
50%
35%
30%
6%
4%
3%
1%
Acquire TB
Access TesXng facility
Diagnosed with TB
Prescribed adequate TB Treatment
Begin Treatment within 2 weeksComplete Treatment
Treatment effecXve
TransiXon to long term HIV care

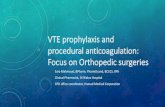
A cascading model for prioriHzing and operaHonalizing the role of integrated
mHealth strategies for UHC
Availability of Medicines and Equipment
Availability of Human Resources
Accessibility of Health Facilities
Contact Coverage
Continuous Coverage
Effective Coverage
Total Population
Supp
lyDe
man
dAc
coun
tabi
lity
Quali
ty
Financial CoverageCost
Target Population
mHEALTH STRATEGIES
Accountability Coverage
B
C
D
E
F
G
H
A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
•Supply Management •Counterfeit Prevention
•Human Resource Management •Provider Training •Telemedicine
•Hotlines •Client Mobile Apps •Client information content subscriptions
•Behavior Change Communication(BCC) •Incentives
•Persistent Electronic Health Records•Provider-to-Provider Communication•Workplanning •Reminders
•Decision Support •POC diagnostics •Telemedicine •Reminders •Incentives
•Mobile financial transactions
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cove
rage
of H
ealth
In
terv
entio
ns of
Kno
wn Ef
ficac
y
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C
Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
PERSPECTIVE
Prioritizing integrated mHealthstrategies for universalhealth coverageGarrett Mehl1* and Alain Labrique2
As countries strive toward universal health coverage, mobile wireless technologies—mHealthtools—in support of enumeration, registration, unique identification, and maintenance ofhealth records will facilitate improved health system performance. Electronic forms andregistry systems will enable routine monitoring of the coverage of essential interventionsfor individuals within relevant target populations. A cascading model is presented forprioritizing and operationalizing the role of integrated mHealth strategies.
The goals of universal health coverage (UHC)are shaping the global health agenda (1, 2),emphasizing that all people, irrespective ofsocioeconomic status, should have accessto health services they need, without in-
curring financial hardship. These ideas, echoingthe 1948 Universal Declaration of Human Rights,were reinforced as a central strategy for globalhealth in the World Health Organization (WHO)2010 World Health Report and a 2012 UnitedNations General Assembly Resolution (3, 4).Achieving UHC, while addressing proximal anddistal contributors to poor coverage and qualityof care, often requires rectifying decades-old dys-function in supply-and-demand aspects of healthsystems. Creative financing and private-sectorengagementmay offset some basic health servicecosts but are unlikely to do so at the scale re-quired to cover the millions who need care. In-novations are required that improve unrestrictedaccess to, and full use of, affordable qualityservices.Meanwhile, for two decades, plummeting costs
have led to nearly ubiquitous access to telecom-munications technologies (5); this has occurredindependently of the global health or develop-ment communities, driven by market forces andconsumer demand. The ability of even simplephones to connect to complex digital systems isproving transformative for low- and middle-income country (LMIC) populations (Fig. 1). Ashealth program implementers struggle to scaleup and integrate public health interventions ofknown efficacy (such as vaccines, micronutrients,and skilled birth attendance), strategies leverag-ing mobile wireless technologies—mHealth—areincreasingly part of a systems-thinking approachto resolving these challenges (6).Global health agencies are beginning to advo-
cate the prudent use ofmHealth solutions, guidedby evidence demonstrating their usability, func-
tionality, reliability, and impact under real-worldconditions (7). Country-level health informationsystems that enable national aggregate record-keeping and facility-level medical records havebeen facilitated by low-cost, open-source robustsystems such as District Health Information Sys-tems (DHIS2) and Open Medical Record Systems(OpenMRS). Enterprise-grade mHealth systemsare also gradually emerging. The past 5 years haveseen substantial maturation of the field, with atleast threeWHO-led initiatives [mHealth Technicaland Evidence Review Group (mTERG), eHealthTechnical Advisory Group (eTAG), and the Interna-tional TelecommunicationsUnion–WHOMobileHealth for Non-Communicable Diseases Initiative],accompanied by numerous other mHealth com-munities of practice. Several hundred randomized
trials are under way worldwide, measuring theefficacy ofmHealth strategies (8).However,most ofthese innovations remainvertical in their approach;that is, addressing single problems faced by healthsystems. A framework to help prioritize investmentsand opportunities for collaboration has been ab-sent, especially given the complexity of health sys-tems, where the receipt of quality care by clients isoften contingent on several preceding layers ofenabling conditions. Knowing who is in need ofservices, having the necessary human resourcesand commodities in adequate supply, and con-necting these together at the right time and placeare elements critical to success. Government agen-cies have been slow to consider innovations thathelp with each of these challenges, such as thosebeing developed in the mHealth space, perhapsbecause the harmonization of innovations across
these health system layers is adaunting task. Drawing fromseminal work in health systemsanalysis, we provide a novelframework for visualizing andplanning how mHealth inno-vations can be applied to helpsurmount common and persist-ent constraints along the path-ways toward the achievement ofUHC goals.People-centered integrated care
requires numerous coordinatedinputs. In 1978, Tanahashi (9)proposed a cascading model toillustrate how health systemslose performance because ofbottlenecks at successive levels,each dependent on the previouslayer. Gaps in information, train-ing, quality, and equitable distri-bution contribute to accumulatedlosses of potential, leading to di-minished health system perfor-mance. Tanahashi’s model helpsidentify opportunities for im-provements in particular strataof the system, with cascadingbenefits to each layer above it (10).As mHealth moves from an eraof experimentation—dominatedby targeted vertical solutions—
toward cross-sectoral health systems that integratenumerous mHealth strategies, we have adaptedTanahashi’s model to illustrate where digital in-vestments can have the greatest impact towardthe achievement of UHC. Previously, we pro-posed that mHealth innovations be viewed notas a direct way to achieve a health outcome butas a strategy to overcome obstinate barriers tothe delivery of known efficacious interventions(7). This reframing allowed researchers to focusonmeasuring the catalytic role of mHealth tools:how a mobile intervention was able to improveefficiency or the coverage of an intervention,such as childhood vaccinations, that has previ-ously been shown to save lives. Although thishelped bridge the dialogue between mHealthinnovators and health systems policy-makers,
1284 12 SEPTEMBER 2014 • VOL 345 ISSUE 6202 sciencemag.org SCIENCE
1Department of Reproductive Health and Research, WorldHealth Organization, Geneva, Switzerland. 2Department ofInternational Health, Johns Hopkins Bloomberg School ofPublic Health, Baltimore, MD, USA.*Corresponding author. E-mail: [email protected]
Fig. 1. D-tree International nutrition program to identify and treatearly childhoodmalnutrition, UrbanDistrict, Zanzibar. [Credit: MarkLeong/World Health Organization]
Cita>on: Mehl G, Labrique A. Priori(zing integrated mHealth strategies for universal health coverage. Science. 2014. DOI: 10.1126/[email protected]

Universal Health Coverage Core Principles
Quality
Coverage
Affordability

Universal Health Coverage
“All people, irrespec4ve of socioeconomic status, should have access to quality health services they need, without incurring financial hardship.”

Universal Health Coverage
Quality
Coverage
Affordability
Accountability

How do we operaHonalize these UHC concepts for
planning integrated naHonalTB and tobacco control m/
eHealth programmes?

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
Availability of Medicines and Equipment
Sup
ply
B•Supply Management •Counterfeit Prevention
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
Availability of Medicines and Equipment
Sup
ply
B•Supply Management •Counterfeit Prevention
Availability of Human Resources C•Human Resource Management •Provider Training •Telemedicine
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
Availability of Medicines and Equipment
Sup
ply
B•Supply Management •Counterfeit Prevention
Availability of Human Resources C•Human Resource Management •Provider Training •Telemedicine
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C
Accessibility of Health Facilities D•Hotlines •Client Mobile Apps •Client information content subscriptions

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
Availability of Medicines and Equipment
Sup
ply
B•Supply Management •Counterfeit Prevention
Availability of Human Resources C•Human Resource Management •Provider Training •Telemedicine
Contact CoverageDem
and
E•Behavior Change Communication(BCC) •Incentives
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C
Accessibility of Health Facilities D•Hotlines •Client Mobile Apps •Client information content subscriptions

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
Availability of Medicines and Equipment
Sup
ply
B•Supply Management •Counterfeit Prevention
Availability of Human Resources C•Human Resource Management •Provider Training •Telemedicine
Contact CoverageDem
and
E•Behavior Change Communication(BCC) •Incentives
Continuous Coverage F•Persistent Electronic Health Records•Provider-to-Provider Communication•Workplanning •Reminders
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C
Accessibility of Health Facilities D•Hotlines •Client Mobile Apps •Client information content subscriptions

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
Availability of Medicines and Equipment
Sup
ply
B•Supply Management •Counterfeit Prevention
Availability of Human Resources C•Human Resource Management •Provider Training •Telemedicine
Contact CoverageDem
and
E•Behavior Change Communication(BCC) •Incentives
Continuous Coverage F•Persistent Electronic Health Records•Provider-to-Provider Communication•Workplanning •Reminders
Effective Coverage
Qual
ity G•Decision Support •POC diagnostics •Telemedicine •Reminders •Incentives
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C
Accessibility of Health Facilities D•Hotlines •Client Mobile Apps •Client information content subscriptions

Total Population
Target Population
mHEALTH STRATEGIES
A
B
C
D
E
F
G
H
TARG
ET: U
nive
rsal
Cov
erag
e of
Hea
lth
Inte
rven
tions
of K
now
n Ef
ficac
y Supply category performance is limited by the weakest of the three components
mHealth strategies appropriate to improve performance gaps in each layer
Gap in performance at each layer needed for UHC
Illustra>ve mHealth Strategies for UHC
Acc
ount
abili
ty
Accountability Coverage A •Client Registration •Electronic Medical Records •Unique Identifiers •Data Collection and Reporting •Screening Tools •Civil Registration and Vital Events
Availability of Medicines and Equipment
Sup
ply
B•Supply Management •Counterfeit Prevention
Availability of Human Resources C•Human Resource Management •Provider Training •Telemedicine
Contact CoverageDem
and
E•Behavior Change Communication(BCC) •Incentives
Continuous Coverage F•Persistent Electronic Health Records•Provider-to-Provider Communication•Workplanning •Reminders
Effective Coverage
Qual
ity G•Decision Support •POC diagnostics •Telemedicine •Reminders •Incentives
Financial CoverageCost H •Mobile financial transactions
DE
TE
RM
INA
NT
S
LA
YE
RS
O
F
UH
C
Accessibility of Health Facilities D•Hotlines •Client Mobile Apps •Client information content subscriptions

Summary: Cri8cal Elements• Value Drivers for each stakeholder, par4cularly government
and other par4es who can ensure sustainability and ins4tu4onaliza4on -‐ including business models
• Demonstrated effecHveness at each maturity stage
• Integra4on of already validated ICT innovaHons, effect at each cascading level
• Grounded in end-‐user reality of current workflows and informa4on flows, but contributes disrupHon where warranted
• Standards-‐based, interoperable with other solu4ons, allowing for re-‐purposing and customiza4on
• Costs for adapta4on, support, and ins4tu4onaliza4on clearly described

Thank you.Dr. Garref [email protected]
Pilo>>s is a natural and necessary part of any new innova>on space:
It is cri>cal to validate mHealth strategies through pilots for later -‐ possible -‐ na>onal
integra>on and ins>tu>onaliza>on