
Models of the Impact of Triage Nurse Standing Orders on ...
37
Models of the Impact of Triage Nurse Standing Orders on Emergency Department Length of Stay Saied Samiedaluie Alberta School of Business, University of Alberta [email protected] Vera Tilson Simon Business School, University of Rochester [email protected] Armann Ingolfsson Alberta School of Business, University of Alberta [email protected] Standing orders allow triage nurses in emergency departments (EDs) to order tests for certain medical conditions before the patient sees a physician, which could reduce the patient’s length of stay (LOS). Several medical studies have documented a decrease in average ED LOS for a target patient population, resulting from the use of standing orders. We formulate models of the operational impact of standing orders and test several policies for whether to order tests at triage for individual target patients, as a function of ED congestion. We find that a threshold policy, with a threshold whose value can be estimated easily from model primitives, performs well across a wide range of parameter values. We demonstrate potential unintended consequences of the use of standing orders, including over testing and spillover effects on non-target patients. 1. Introduction Mathematical models of queueing networks and their applications in manufacturing sys- tems, communication networks, and other settings have been investigated extensively. Routing of customers to optimize system performance is an important topic within this literature. Two understudied aspects of routing are (1) the impact of policy decisions regarding admissible routing decisions and (2) the way in which human servers make rout- ing decisions. We study an important policy decision for routing in health care systems, namely, whether to enact standing orders. Standing orders permit one type of server (a triage nurse) to make a decision (order medical tests) that is typically restricted to another type of server (an emergency physi- cian). Standing orders specify conditions under which a triage nurse is permitted to order tests but they typically do not specify operational conditions under which ordering tests is desirable, from a system or patient point of view. Empirical findings from the medical liter- ature have demonstrated that the use of standing orders in emergency departments (EDs) 1
Transcript of Models of the Impact of Triage Nurse Standing Orders on ...

Models of the Impact of Triage Nurse StandingOrders on Emergency Department Length of Stay
Saied SamiedaluieAlberta School of Business, University of Alberta
Vera TilsonSimon Business School, University of Rochester
Armann IngolfssonAlberta School of Business, University of Alberta
Standing orders allow triage nurses in emergency departments (EDs) to order tests for certain medical
conditions before the patient sees a physician, which could reduce the patient’s length of stay (LOS). Several
medical studies have documented a decrease in average ED LOS for a target patient population, resulting
from the use of standing orders. We formulate models of the operational impact of standing orders and
test several policies for whether to order tests at triage for individual target patients, as a function of ED
congestion. We find that a threshold policy, with a threshold whose value can be estimated easily from model
primitives, performs well across a wide range of parameter values. We demonstrate potential unintended
consequences of the use of standing orders, including over testing and spillover effects on non-target patients.
1. Introduction
Mathematical models of queueing networks and their applications in manufacturing sys-
tems, communication networks, and other settings have been investigated extensively.
Routing of customers to optimize system performance is an important topic within this
literature. Two understudied aspects of routing are (1) the impact of policy decisions
regarding admissible routing decisions and (2) the way in which human servers make rout-
ing decisions. We study an important policy decision for routing in health care systems,
namely, whether to enact standing orders.
Standing orders permit one type of server (a triage nurse) to make a decision (order
medical tests) that is typically restricted to another type of server (an emergency physi-
cian). Standing orders specify conditions under which a triage nurse is permitted to order
tests but they typically do not specify operational conditions under which ordering tests is
desirable, from a system or patient point of view. Empirical findings from the medical liter-
ature have demonstrated that the use of standing orders in emergency departments (EDs)
1

2
typically leads to reduced average length of stay (LOS) for the target group of patients.
Empirical work in operations management (OM) has identified early task initiation (ETI)
(Batt and Terwiesch 2017) as a mechanism through which human servers pre-order tests
more frequently when the system is congested. Our analysis complements these studies
by mathematically comparing an array of routing policies (ranging from always to never
using standing orders) in terms of their performance for the system as a whole as well as
for individual patient categories.
Standing orders (also termed complaint specific protocol, and advanced triage protocol)
allow health care providers who are not explicitly licensed to place orders for medical
tests and treatments to do so, for patients presenting with specific symptoms (the target
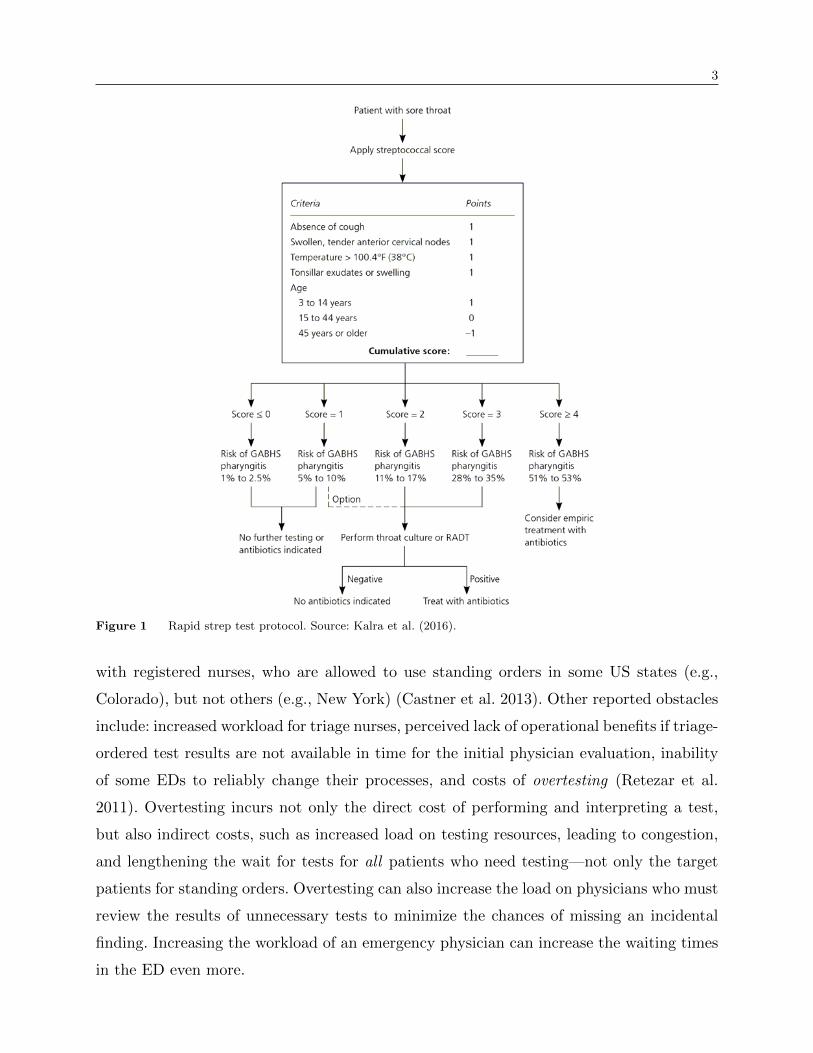
patients), by following a codified protocol. One common example is standing orders for a
bacterial culture test for throat pain patients (Figure 1), which can reduce ED LOS because
the test is time-consuming, whereas the low acuity of the condition can mean low priority
for the patient, and a long wait for initial evaluation by a physician (Settelmeyer 2018).
Another common example is the Ottawa Ankle Rules protocol (Figure 2) to determine
whether a patient presenting with an ankle injury requires an X-ray (Shell et al. 1993).
Having the X-ray available in time for the patient’s first evaluation by the physician reduces
the patient’s ED LOS.
A typical ED process flow (Figure 3) involves triage by a nurse, initial evaluation by
a physician, diagnostic tests or treatment ordered by the physician, and the physician’s
decision on disposition, i.e., discharge or admission to the hospital. This series of steps,
with potential waiting periods in between, constitutes the critical path, whose duration
determines a patient’s ED LOS, which is a key performance measure (Wiler et al. 2015).
Standing orders can reduce ED LOS for target patients for two reasons: (1) Having test
results available in time for the patient’s initial evaluation by a physician can eliminate
the need for the physician to revisit the case, and (2) Completing the tests during the time
the patient waits for the initial physician evaluation moves the testing off the critical path.
Physician-staffed triage is another modification to standard ED flow that also permits
early ordering of tests (Russ et al. 2010) and is therefore operationally similar to standing
orders.
Published empirical studies in the medical literature generally confirm that the use
of standing orders reduces ED LOS for the orders’ target population. Yet, the use of
standing orders is not universal. One obstacle is regulations: ED triage is generally staffed
3
Figure 1 Rapid strep test protocol. Source: Kalra et al. (2016).
with registered nurses, who are allowed to use standing orders in some US states (e.g.,
Colorado), but not others (e.g., New York) (Castner et al. 2013). Other reported obstacles
include: increased workload for triage nurses, perceived lack of operational benefits if triage-
ordered test results are not available in time for the initial physician evaluation, inability
of some EDs to reliably change their processes, and costs of overtesting (Retezar et al.
2011). Overtesting incurs not only the direct cost of performing and interpreting a test,
but also indirect costs, such as increased load on testing resources, leading to congestion,
and lengthening the wait for tests for all patients who need testing—not only the target
patients for standing orders. Overtesting can also increase the load on physicians who must
review the results of unnecessary tests to minimize the chances of missing an incidental
finding. Increasing the workload of an emergency physician can increase the waiting times
in the ED even more.

4
Figure 2 Ottawa Ankle Rules protocol. Source: Bachmann et al. (2003).
Viewing an ED as a network of queues holds the potential for leveraging analysis methods
that have been developed for other settings, such as manufacturing. To realize that poten-
tial, however, it is crucial to recognize and understand how human behavior (of servers and
patients) impacts system behavior. For example, while standard queueing models predict
less delay if ED patients wait in a pooled physician’s queue rather than being assigned to a
particular physician queue on arrival, empirical work (Song et al. 2015) shows the opposite
effect, possibly caused by strategic behavior of physicians.
Similarly, the behavior of triage nurses and physicians could greatly impact the effective-
ness of standing order protocols. Such protocols typically only specify the patient-related
conditions that need to be met in order for tests to be ordered, but leave it to the dis-
cretion of triage nurses to decide whether to order tests. It is reasonable to expect that
triage nurses will consider current levels of congestion and possibly other operational fac-
tors. Indeed, the only two medical protocols that we know of that incorporate operational
factors (Hwang et al. 2016, Li et al. 2018) specify that standing orders should be initiated
when the time until initial evaluation by a physician is expected to be longer than some
threshold. Triage nurses that follow such a policy can be viewed as an example of the ETI
mechanism. ETI has been identified as an important mechanism through which system
load can influence service time in a queueing network (Batt and Terwiesch 2017, Delasay

5
et al. 2016). Observational studies have found that the use of ETI increases with conges-
tion (Batt and Terwiesch 2017). In addition to studying how activation of ETI by human
servers depends on congestion and other factors, it is also important to study optimal or
near-optimal policies for using ETI to reduce ED LOS (Batt and Terwiesch 2017) and that
is the area to which we contribute.
We formulate a queueing network model to investigate the use of standing orders in an
ED. We analyze the utilization of testing and physician resources under the two extreme
policies of never using standing orders and always using standing orders. Through the
utilization analysis, we identify a parameter β, which is easily computed from the model
primitives, that we expect to be indicative of whether the use of standing orders will be
effective. We develop a Markov Decision Process (MDP) formulation for a finite-capacity
ED and analyze this formulation to characterize a congestion-sensitive standing orders
policies that minimize ED LOS averaged over all patients. We show that an easy-to-use
threshold policy, with a single threshold that is obtained through complete enumeration,
performs nearly as well as the optimal policy across a wide range of parameters. We further
show that an approximate threshold policy, obtained as a linear function of lnβ, performs
almost as well. We use discrete event simulation (DES) to investigate the impact of relaxing
the capacity constraint and a simplifying assumption of a single physician. We demonstrate
potential unintended consequences of the use of standing orders, including spillover effects
on ED patients who are not subject to the standing order protocol.
The rest of the paper is organized as follows: Section 2 reviews related literature; Section
3 describes a typical ED process flow and how the use of standing orders changes the
flow; Section 4 presents the mathematical model, analyzes resource utilization, presents
the MDP formulation, and the threshold policy; and Section 5 reports results of numerical
experiments. Section 6 concludes.
2. Literature Review
We review four streams of literature relevant to our study: (1) medical studies on the impact
of standing orders on ED LOS, (2) DES studies of standing orders, (3) studies of staffing
triage with providers licensed to place medical orders (an alternative to standing orders),
and (4) OM papers examining costs and benefits of various alternatives for post-triage
prioritization of ED patients.
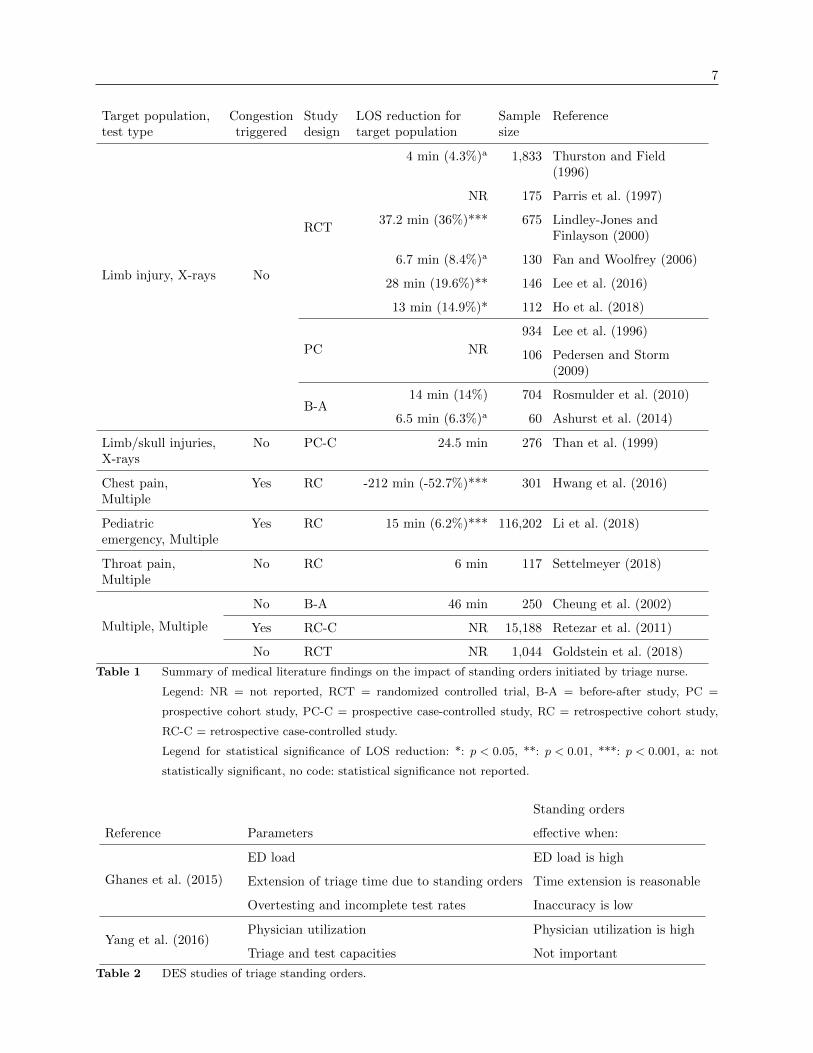
Stream 1: Table 1 summarizes findings from 17 medical studies of standing orders. Nine
studies were included in a 2011 systematic review (Rowe et al. 2011), and eight were

6
published after 2011. The primary outcome measure for most studies is ED LOS for the
target population and most studies report reductions in this measure, ranging in magnitude
from 4 to 46 minutes (4.3 to 36%), as shown in the fourth column of Table 1. (See Table 9
for a summary of results from studies whose outcome measures were defined differently, in
terms of start point, end point, or patient inclusion criteria). A single study (Hwang et al.
2016) found an increase in ED LOS for the target population but this study failed to control
for ED congestion levels—standing orders were used only when the ED was congested,
when patients were experiencing longer waiting times. Eleven studies investigated standing
orders for ordering X-rays for limb injuries. The remaining studies examined standing
orders for patient complaints such as throat pain, pediatric emergency, and chest pain.
Most studies mention no operational or congestion-related criteria for whether to initiate
standing orders. The three exceptions mention criteria based on anticipated time until
placement in a treatment area being above a threshold (Hwang et al. 2016, Retezar et al.
2011) or anticipated time until test results are available being below a threshold (Li et al.
2018). Reliable estimates of processing times or delays are not easy to obtain by the triage
nurse. Information about the number of patients waiting in different parts of the ED are
likely easier to obtain, and this is the type of information that we assume is available for
the policies we propose.
Several other factors are identified as important to the operational effectiveness of stand-
ing orders. If triage nurses order more tests than physicians, the potential benefits of
standing orders can be lost (Thurston and Field 1996). Having the test results ready before
the physician sees the patient is another critical factor. In Parris et al. (1997), where no
significant LOS reduction was found, only 77% of patients had their X-rays ready before
being evaluated by the physician. Hwang et al. (2016) report that having the tests com-
pleted reduced the time from physician evaluation to disposition by 16.9%. Therefore,
service capacity and variations in the workload of servers performing standing orders can
influence the orders’ impact.
Stream 2: Two studies (Ghanes et al. 2015, Yang et al. 2016) have investigated the
use of standing orders, under the assumption that standing orders are used for all target
patients—as opposed to using standing orders only when congestion-related criteria are
met. Table 2 compares the factors that these studies found to be important indicators of
when the use of standing orders is effective.
Stream 3: Staffing triage with a physician or a similarly licensed provider is an alternative
to standing orders. This practice introduces a trade-off between placing such providers at
7
Target population,test type
Congestiontriggered
Studydesign
LOS reduction fortarget population
Samplesize
Reference
Limb injury, X-rays No
RCT
4 min (4.3%)a 1,833 Thurston and Field(1996)
NR 175 Parris et al. (1997)
37.2 min (36%)*** 675 Lindley-Jones andFinlayson (2000)
6.7 min (8.4%)a 130 Fan and Woolfrey (2006)
28 min (19.6%)** 146 Lee et al. (2016)
13 min (14.9%)* 112 Ho et al. (2018)
PC NR
934 Lee et al. (1996)
106 Pedersen and Storm(2009)
B-A14 min (14%) 704 Rosmulder et al. (2010)
6.5 min (6.3%)a 60 Ashurst et al. (2014)
Limb/skull injuries,X-rays
No PC-C 24.5 min 276 Than et al. (1999)
Chest pain,Multiple
Yes RC -212 min (-52.7%)*** 301 Hwang et al. (2016)
Pediatricemergency, Multiple
Yes RC 15 min (6.2%)*** 116,202 Li et al. (2018)
Throat pain,Multiple
No RC 6 min 117 Settelmeyer (2018)
Multiple, Multiple
No B-A 46 min 250 Cheung et al. (2002)
Yes RC-C NR 15,188 Retezar et al. (2011)
No RCT NR 1,044 Goldstein et al. (2018)
Table 1 Summary of medical literature findings on the impact of standing orders initiated by triage nurse.
Legend: NR = not reported, RCT = randomized controlled trial, B-A = before-after study, PC =
prospective cohort study, PC-C = prospective case-controlled study, RC = retrospective cohort study,
RC-C = retrospective case-controlled study.
Legend for statistical significance of LOS reduction: *: p < 0.05, **: p < 0.01, ***: p < 0.001, a: not
statistically significant, no code: statistical significance not reported.
Standing orders
Reference Parameters effective when:
Ghanes et al. (2015)
ED load ED load is high
Extension of triage time due to standing orders Time extension is reasonable
Overtesting and incomplete test rates Inaccuracy is low
Yang et al. (2016)Physician utilization Physician utilization is high
Triage and test capacities Not important
Table 2 DES studies of triage standing orders.

8
triage or at later stages in the ED process flow. At least one medical study has found that
staffing triage with physician assistants reduced both rates of leaving without being seen
(LWBS) and the time patients spend occupying an ED bed (Nestler et al. 2012). This
practice has been criticized as prioritizing hospital profits over patient care and leading
to over-testing (Corl 2019). OM scholars have investigated policies for the allocation of
physicians to triage vs. post-triage stages, so as to optimize time to first treatment and
timely discharges (Zayas-Caban et al. 2019) or to optimize the tradeoff between staffing
cost and revenue loss from patients who leave without being seen (Kamali et al. 2018).
Stream 4: OM researchers have modeled other triage routing possibilities besides early
ordering of tests via either standing orders and physician-staffed triage. In particular,
they have investigated streaming of patients based on acuity level (Cochran and Roche
2009), predicted disposition (discharged or admitted to hospital) (Saghafian et al. 2012),
or predicted complexity (number of patient interactions in the ED) (Saghafian et al. 2014).
ED physician’s prioritization of newly arrived patients vs. in-process patients has also been
examined by OM researchers. The contexts included in-process patients creating additional
work for the physician though interruptions (Dobson et al. 2013), considerations of trade-
offs between the time-to-first treatment and LOS (Huang et al. 2015, Hu et al. 2018), and
lack of information about the state of ED queues (Ansari et al. 2019). Other OM papers
related to management of EDs are reviewed by Hu et al. (2018).
3. ED Process Flow, with and without Standing Orders
In this section, we describe a typical process flow in an emergency department and discuss
how the implementation of standing orders changes the flow.
3.1 ED Process Flow without Standing Orders
Figure 3 illustrates a typical process flow for an ED that does not use standing orders.
Patients register upon arrival and then wait for triage. The triage is performed by a nurse
who learns of patient’s primary reason for visiting the ED, and determines based on the
patient’s condition, how urgently the patient needs to be evaluated by an ED physician. In
the order of priority determined by the triage nurse, the patient is allocated a bed in the
ED, and then an initial evaluation is performed by an ED physician. In some cases, the
physician treats and discharges the patient during this initial exam (e.g., a patient needs
stitches for a cut). In other cases, the physician requires additional information to arrive

9
Figure 3 The default care pathway of a patient in an ED.
at a diagnosis and reach a decision on patient disposition. The additional information may
come from diagnostic tests, or from responses to treatment.
A diagnostic test may be performed at the bedside in the ED (e.g., a pregnancy ultra-
sound), in a hospital lab using a sample collected in the ED (e.g., a complete blood count),
or at another unit of the hospital (e.g., an MRI scan). Depending on available testing
capacity, a patient may need to wait to be tested or wait to have a treatment started.
There can be a significant delay between the last step in the test or treatment process
which involves the patient (e.g., drawing a blood sample) and the instant when the test
results or treatment response become available. After this information becomes available,
the ED physician decides whether to discharge the patient or to admit the patient to a
hospital ward. Patients then depart from the ED, although patients directed to a hospital
ward may need to wait in an ED bed until a ward bed becomes available.
Patients might abandon, either prior to initial evaluation (“left without/before being
seen”) or after initial evaluation but prior to disposition (“left against medical advice”).
We omit abandonment from Figure 3, in order to focus on process flow features that are
most relevant to our study.
3.2 ED Process Flow with Standing Orders
Figure 4 depicts an ED process flow that incorporates standing orders. At triage, the
triage nurse decides whether or not the patient’s condition is covered by a standing orders

10
protocol. If the condition is not covered by a protocol, the process continues as before. If
the triage nurse determines that the condition is subject to a protocol, there is a second
decision to be made: whether or not to invoke the test ordering protocol. Placing test
and treatment orders increases the nurse’s workload. For some medical conditions in some
hospitals, standing orders are the default process, but for other conditions test orders at
triage are triggered by operational factors (e.g., expected wait time for initial assessment
by a physician is longer than 15 minutes as in Hwang et al. (2016)).
Figure 4 The standing order model in an ED.
4. Analysis of Standing Order Routing Policies
In this section we describe a mathematical model of ED flow with standing orders. We use
this model to generate policies for post-triage routing of patients who are identified at triage
imperfectly as presenting with a medical condition that is subject to a standing order. The
routing policies specify the operational conditions under which patients should be routed
from triage directly to testing. In Section 5, we numerically compare the performance of
these policies.
4.1 Mathematical Model
We divide patients into two classes based on whether an ED physician would determine
that the patient belongs to the standing orders target population and therefore needs
testing (target patients; proportion ψ) or not (other patients; proportion 1−ψ). The triage

11
nurse correctly identifies all target patients and correctly identifies a proportion ν of other
patients. Thus, ν(1−ψ) is the proportion of all patients triaged as other by the nurse. The
proportion of patients triaged as belonging to the target population (“triaged as target”
for short) is 1− ν(1−ψ). The probability that a patient is in the target population, given
that the patient was triaged as target is:
η=ψ
1− ν(1−ψ). (1)
We consider only the time period that begins with a patient’s placement in a treatment
space and finishes when a disposition decision is made. There is a single ED physician,
and a single-server testing resource; patients do not abandon, they have at most one test
encounter, and only one post-test evaluation with the ED physician. Test results are avail-
able as soon as the testing service completes. Figure 5 illustrates the patient flow, assuming
that standing orders are used.
Initial
evaluation (physician)
Discharge
Testing
Post-test
evaluation (physician)
Discharge Q2: Post-test
Testing Q1: Testing
Arrival Triage (nurse)
Triaged as other
Triaged as target
Routing (nurse)
Sent to physician
Testing
Q3: Triaged as target
Q4: Triaged as other
Figure 5 Patient flow in the mathematical model for an ED with standing orders.
The model has four queues: Q1: patients waiting for testing; Q2: patients waiting for
post-test physician evaluation; Q3: patients triaged as target but routed to physician first,
waiting for physician evaluation; and Q4: patients triaged as other, waiting for physician
evaluation.
Full state information is available at the time of the routing decision: the number of
patients in each queue, and which queue (if any) the physician is currently serving. The
number of patients waiting or being served in Queue i at time t is denoted by Qi(t). To
simplify certain expressions we introduce echelon variables: Ei(t) =Qi(t) + · · ·+Q4(t), for
i= 1, . . . ,4, which implies E4(t)≤E3(t)≤E2(t)≤E1(t).
New patient arrivals are Poisson with arrival rate λ. Service times are independent and
exponentially distributed, with rate µi, for patients in Queue i, i∈ 1,2,3,4. We assume
that the service rate for an initial physician evaluation does not depend on whether the
patient was triaged as target or other (µ3 = µ4).

12
The model is Markovian. The state vector is X(t) =(E(t),R(t)
), where E(t) =
(E1(t),E2(t),E3(t),E4(t)) and R(t) indicates whether the physician is idle (R(t) = 0) or
providing service for a patient from Queue i (R(t) = i), i∈ 2,3,4. We define
q1 = (1,0,0,0), q2 = (1,1,0,0), q3 = (1,1,1,0), q4 = (1,1,1,1). (2)
The operation E+qi corresponds to “add one patient to Queue i”.
The physician is idle (R(t) = 0) if and only if all of the physician queues are empty
(E2(t) = 0). The physician can serve a patient whose test has been completed (R(t) = 2)
only if Q2(t)> 0. The physician can conduct an initial evaluation for a patient triaged as
target (R(t) = 3) only when Q3(t)> 0. The physician can conduct an initial evaluation for
a patient triaged as other (R(t) = 4) only when Q4(t)> 0. We denote the set of possible
values for R given the state of the queues by Ω(E(t)
).
To model a system without standing orders, we eliminate the differentiation between
target and other patients, remove the routing decision, and combine Q3 and Q4 into a
single queue for initial evaluation.
4.2 Stability Analysis
In this section we analyze the stability of the system. Our goal is to generate high-level
insight into when using standing orders is likely to be useful. We focus on two extreme
routing policies: “never standing orders” (NSO), and “always standing orders” (ASO).
The physician uses a work-conserving policy to select the next patient to serve. Denote
the utilization of Resource s under Policy γ as uγs , where s ∈ testing,physician and
γ ∈ NSO,ASO. The system is stable under policy γ if uγs < 100% for both resources.
Under NSO, only the fraction ψ of arrivals that are in the target population are tested,
and therefore:
uNSOtesting =
ψλ
µ1
. (3)
Recalling that µ3 = µ4, the physician’s utilization under NSO is
uNSOphysician = λ
(1
µ3
+ψ
µ2
), (4)
because the physician performs an initial evaluation for every arriving patient, and a post-
test evaluation for every patient in the target population.

13
Under ASO, all patients triaged as target are directed to testing prior to being seen by
the physician. Hence, the testing resource is utilized more heavily under ASO than under
NSO:
uASOtesting =
(1− ν(1−ψ))λ
µ1
= uNSOtesting +
(1− ν)(1−ψ)λ
µ1
. (5)
The physician’s workload also changes: under ASO there is a single encounter with each
patient. The average duration of this encounter is 1/µ3 for patients triaged as other (frac-
tion ν(1−ψ)) and 1/µ2 for patients triaged as target. Therefore,
uASOphysician = λ
(ν(1−ψ)
µ3
+1− ν(1−ψ)
µ2
)= uNSO
physician +λ
((1− ν)(1−ψ)
µ2
− 1− ν(1−ψ)
µ3
).
(6)
In contrast to the testing resource, which is certain to be more highly utilized under ASO,
the physician might be more or less utilized under ASO, that is, the final term in (6) could
be positive or negative.
The ASO policy is unlikely to reduce overall ED LOS if the average total service time (in
testing and with the physician) is longer under ASO than under NSO, i.e., the increase in
service time due to unnecessary tests and post-test evaluations on other patients is larger
than the savings from avoiding the initial physician evaluation of target patients:
ψ
µ3
< (1− ν) (1−ψ)
(1
µ1
+1
µ2
− 1
µ3
). (7)
The inequality (7) can be re-written as
β =
(1 +
ψ
(1− ν)(1−ψ)
)1/µ3
1/µ1 + 1/µ2
< 1. (8)
Thus, all else being equal, average system service time tends to be longer under ASO
than NSO in situations in which testing and post-test evaluation are lengthy (1/µ1 + 1/µ2
is large), initial evaluation is short (1/µ3 is small), triage is inaccurate (ν is small), and
the target population is small (ψ is small). This analysis, however, does not take into
consideration the effects of congestion or the benefit of dynamic policies, which we discuss
in the following sections. In Section 5, we demonstrate that the parameter β is predictive
of how well the ASO and NSO policies perform, and that β can be used to develop a
near-optimal threshold policy.

14
4.3 MDP Formulation
With standing orders in use, the queue control policy concerns only patients that are
triaged as target. Such a patient is routed upon arrival either to the testing queue (Q1) or
the initial physician evaluation queue (Q3). In addition, the physician must decide which
queue to serve next, upon completion of a service. A policy γ should specify both decisions
for every state of the system.
We formulate the problem as an infinite-horizon average-cost MDP. The state vector
under policy γ is Xγ(t) = (Eγ(t),Rγ(t)). We assume for tractability that the ED has a
finite capacity B, which implies E1(t)≤B. The state space is
X =
X(t) =
(E(t),R(t)
) ∣∣∣∣Ei(t)∈Z+,∀i,E4(t)≤E3(t)≤E2(t)≤E1(t)≤B,R(t)∈Ω(E(t)
).
Here, Z+ denotes the non-negative integers.
Consider a policy that randomly routes patients triaged as target upon arrival and
randomly selects the next queue to serve by the physician. Under such policy, every state
of the system can be reached from every state, which implies that weak accessibility holds
for the underlying Markov chain. Therefore, the optimal average cost is constant and
independent of the initial state.
We seek a routing policy that minimizes the expected average number of patients in the
system:
gγ =L= lim supT→∞
1
TE[∫ T
0
Eγ1 (t)dt
]. (9)
The state and action spaces are finite, hence for the average reward criterion there exists
an optimal stationary deterministic policy (Puterman 2014, Theorem 9.1.8). Therefore,
we consider only policies from the set ΠMD of Markovian stationary deterministic poli-
cies. Under our assumptions Xγ(t) is a continuous time Markov chain. Transition rates
between states are finite, and therefore Xγ(t) is uniformizable for all γ ∈ΠMD. We define
the uniformization constant
Λ = λ+µ1 +µ2 +µ3 +µ4, (10)
so that the time between transitions is exponentially distributed with rate Λ. We redefine
Xγ(k), k= 1,2, . . . to be the corresponding discrete time Markov chain. Finding γ ∈ ΠMD
that minimizes (9) is equivalent to finding a policy γ minimizing
gγ =gγ
Λ= lim sup
K→∞
1
KE[ K∑k=1
Eγ1 (k)
]. (11)

15
The average cost of the optimal policy, γ∗, is
g∗ = minγ∈ΠMD
gγ (12)
The optimal average cost and the bias function w(E,R) satisfy the equation:
w(E,R) =1
Λ(E1− g∗) + pc(E) ·hc(E,R) + ps(E) ·hs(E,R)
+ pt(E) ·ht(E,R) + pr(R) ·∑
(ξ,pξ)∈Ξ(R)
pξ ·hr(E+ ξ)
+(
1− pc(E)− ps(E)− pt(E)− pr(R))·w(E,R), ∀ (E,R)∈X . (13)
The first term on the right of (13) is the difference between the total number of patients in
the system in state (E,R) and the optimal average cost. The four middle terms correspond
to system transitions, representing the product of the probability of a particular transition
and the bias function after that transition. The final term corresponds to self-transition,
and is included because of the uniformization.
We now elaborate on each of the four main terms in (13). When the system is full, no
new patients can arrive. The probability of a new arrival that is triaged as target is
pc(E) =(
1− ν(1−ψ))λ
Λ·1(E1 <B), (14)
and hc(E,R) corresponds to the routing decision:
hc(E,R) = min
w(E+q1,R)
w(E+q3,3) ·1(E2 = 0) +w(E+q3,R) ·1(E2 > 0)
. (15)
The term w(E+ q1,R) represents routing the patient to the testing queue Q1, while the
other term represents routing the patient to the physician queue Q3. If the physician is
idling when such a patient arrives to Q3, the physician immediately begins the patient’s
initial evaluation. Otherwise, the physician continues with the current service.
The probability of a new patient arrival that is triaged as other is
ps(E) = ν(1−ψ)λ
Λ·1(E1 <B). (16)
The function hs(E,R) corresponds to the change in state upon arrival of a patient known
not to require testing, who therefore joins Q4:
hs(E,R) =w(E+q4,4) ·1(E2 = 0) +w(E+q4,R) ·1(E2 > 0) (17)

16
Testing is conducted whenever the test queue is not empty. The probability of test
completion prior to any other transition is
pt(E) =µ1
Λ·1(Q1 > 0). (18)
Once the testing is completed, the patient moves to the queue of patients awaiting a post-
test physician evaluation (Q2). If the physician is idling when a test is completed, the
physician immediately initiates the post-test evaluation. Thus, we define ht(E,R) as
ht(E,R) =w(E−q1 +q2,2) ·1(E2 = 0) +w(E−q1 +q2,R) ·1(E2 > 0) (19)
Modeling of the completion of the physician’s evaluation is more involved because the
physician services multiple queues. The probability of the physician completing a service
prior to another system transition is given by
pr(R) =
µ4Λ, R= 4
µ3Λ, R= 3
µ2Λ, R= 2
0, R= 0
(20)
Ξ(R) is the set of tuples denoting transitions and their probabilities upon completion of
physician service R:
Ξ(R) = (ξ, pξ)=
(−q4,1), R= 4
(−q3 +q1, η), (−q3,1− η), R= 3
(−q2,1), R= 2
(0,1), R= 0.
(21)
If the physician completes a post-test evaluation (R = 2), a patient is removed from Q2
with probability 1. The R= 4 case is similar. If the physician is idle (R= 0), then nothing
happens to the queue lengths, with probability 1. The complicated case involves the physi-
cian evaluating a patient who may or may not need testing (R = 3). In that case, with
probability η (defined in (1)), the patient requires testing and is therefore removed from
Q3 and added to Q1. Otherwise, with probability 1− η, the patient does not need testing
and is simply removed from Q3.
Finally, hr(E) models the physician choosing optimally which queue to serve:
hr(E+ ξ) = minR′∈Ω(E+ξ)
w(E+ ξ,R′). (22)

17
4.4 Structure of the Optimal Control Policy
It is natural to conjecture that if it is optimal to route a patient from triage to the physician
first in a particular state, then that routing will remain optimal if more patients are waiting
for testing, and all else remains the same. Similarly, we expect that if physician-first routing
is optimal in a particular state, that routing will remain optimal if fewer patients are
waiting for the physician, and all else remains the same. Conversely, if test-first routing
is optimal in a particular state, then we expect that routing to remain optimal if fewer
people are waiting for testing, or if more people are waiting for the physician. In other
words, we expect the optimal routing decision to be monotonic with respect to each of the
four queue lengths.
We prove monotonicity of the optimal routing with respect to the length of the testing
queue, Q1, in Proposition 1. The proof is in Appendix B.
Proposition 1. Consider a state (E,R) for which the system is not full (E1 < B) and
both the testing server and the physician are busy (Q1 > 0,E2 > 0). If physician-first routing
is optimal for a patient triaged as target, then this action remains optimal if there is one
additional patient in the testing queue, i.e., in state (E+q1,R). Similarly, if testing-first
routing is optimal for a patient triaged as target, then this action remains optimal if there
is one less patient in the testing queue, i.e., in state (E−q1,R).
We provide numerical evidence for monotonicity of the optimal policy with respect to
the physician queue lengths, Qi, i= 2,3,4, using a problem instance with B = 15, ψ= 30%,
ν = 85%, 1λ
= 17 min, 1µ1
= 18 min, 1µ2
= 10 min, and 1µ3
= 1µ4
= 7.5 min. Figure 6 illustrates
the optimal routing policy for a patient triaged as target, for states in which E1 < B
and two of the four queues are empty. Panels (a)-(c) of Figure 6 illustrate the optimal
policy when the number of patients in the testing queue and one of the physician queues
is varied, while the length of the other two physician queues is zero. All panels display the
monotonicity of the optimal policy with respect to the length of queues for this problem
instance. We also investigated monotonicity of the optimal policy for states that are not
illustrated in Figure 6. For every state for which E1 <B, Q1 > 0, and E2 > 0, we checked
the number of times the optimal policy changes the routing decision as we increase the
length of each queue by one patient. Out of 16,380 cases, only in 23 cases the optimal
policy switches twice, where the second switch happens near the E1 = B boundary. In
other cases, the optimal policy changes at most once as we increase the queue lengths.

18
Q2
Q1
(a) Q3 =Q4 = 0
Q3
Q1
(b) Q2 =Q4 = 0
Q4
Q1
(c) Q2 =Q3 = 0
Figure 6 An example of the optimal routing policy for a patient triaged as target.
Circle: Send the patient to testing. Square: send the patient to physician first.
4.5 A Threshold Routing Policy
The monotonicity of the optimal policy implies that optimal decisions involve state-
dependent threshold, which could be complicated to use in practice. This motivates us to
investigate the performance of a policy based on a single threshold, θ:
If E2−Q1 ≥ θ, then route to testing,
Otherwise, route to the physician.(23)
(Recall that E2 − Q1 is the difference between the number of patients waiting for the
physician and the number of patients waiting for testing.) This policy includes ASO (θ=
−B) and NSO (θ = +B) as special cases. The optimal value of θ can be determined by
evaluating L for all 2B + 1 possible values of θ. Alternatively, the optimal threshold can
be estimated as a function of the parameter β from (8), as we will see in Section 5.
To complete the policy, we need to specify how the physician selects the next patient
to examine. In Section 5, we use both Markov chain calculations and a DES model to
evaluate the performance of threshold policies. In our Markov chain calculations, we use a
randomized policy with probabilities that are proportional to queue lengths (see Appendix
C) as an approximation to FCFS. In the DES model, we use FCFS (see Appendix D).
5. Numerical Experiments
In this section, we use numerical experiments to compare NSO, ASO, and the two thresh-
old policies, in terms of their optimality gap, defined as the percent increase in L, the
average number of patients in the system, relative to the optimal policy. We show that the
parameter β, which is defined in (8), is predictive of the performance of threshold policies.
In particular, we find that NSO and ASO, the two policies most frequently used in prac-
tice, perform poorly when | lnβ|< 1. In contrast, we find that an approximate threshold
(θ) policy, in which θ is estimated as a linear function of lnβ, is nearly optimal.

19
We close this section with a series of DES experiments, to study the impact of standing
order policies on target and non-target patients as well as the impact of removing the
finite-capacity and single-server assumptions. We show that the performance difference
between NSO and ASO grows with the system capacity, and that using standing orders to
minimize LOS for all patients could have the unintended consequence of increasing LOS
for target patients.
5.1 Problem Instances
We generate a full factorial experiment by varying six factors: the average time the physi-
cian spends with a patient (τ), the target population proportion (ψ), the initial examination
duration as a proportion of the total time the physician spends with a target patient (κ),
the overtesting rate under ASO (σ), and the utilization of resources under NSO (uNSOphysician
and uNSOtesting). Table 3 lists the factor values. With the exception of τ , these factors are
dimensionless. We fix the value of τ , which is without loss of generality, as this corresponds
to setting the time unit for the analysis. The factors τ , ψ, κ, and σ correspond directly to
quantities that are typically reported in studies of standing orders in the medical literature,
which helps us to choose realistic values for those factors. We directly control the utiliza-
tions of the two resources under NSO, and we use the results from our stability analysis
in Section 4.2 to determine factor combinations for which the system is stable under NSO
but not under ASO.
In what follows, we show how to determine the model primitives, ν, λ, µ1, µ2, and µ3,
from the experimental factors. In addition to (3)-(4) that define utilization of resources
under NSO, we have the following relationships between the experimental factors and the
model primitives:
τ =1
µ3
+ψ
µ2
, κ=
1µ3
1µ3
+ 1µ2
, σ= (1− ν)(1−ψ).
The model primitives can be computed from the experimental factors as follows:
λ=uNSO
physician
τ, ν = 1− σ
1−ψ,
µ1 =uNSO
physician
uNSOtesting
ψ
τ, µ2 =
κ+ (1−κ)ψ
(1−κ)τ, µ3 =
κ+ (1−κ)ψ
κτ.
The values selected for the experimental factors in Table 3 result in 35 = 243 problem
instances, which constitutes our training set. Table 4 shows minimum and maximum values

20
Parameter Minimum Baseline Maximum Reference(s)
Average time physician spends witha patient (τ)
— 22 min — Chonde et al. (2013)
Target population proportion (ψ) 10% 25% 70% Valtchinov et al. (2019),Compeau et al. (2016), Ghaneset al. (2015), Liu et al. (2014)
Initial examination duration asproportion of total service time fortarget patients (κ)
20% 35% 50% Yang et al. (2016), Ellis et al.(2006), Graff et al. (1993)
Overtesting rate (σ) 1% 5% 10% Yang et al. (2016), Thurstonand Field (1996), Lee et al.(1996), Davies (1994), Macleodand Freeland (1992)
Physician utilization under NSO(uNSO
physician)50% 80% 95% Yang et al. (2016), Ellis et al.
(2006), Graff et al. (1993)
Testing utilization under NSO(uNSO
testing)50% 80% 95% Steindel and Howanitz (2001),
Edelstein et al. (2010)
Table 3 Experimental factors and their values.
for the model primitives and the resource utilizations under ASO across all the problem
instances in the training set. In Section 5.2, we use these problem instances to evaluate the
performance of the optimal threshold policy and in Section 5.3 we use them for estimating
the best threshold based on the model primitives.
Parameter Minimum Maximum
Arrival rate (λ) 1.36 2.59
Testing service rate (µ1) 0.14 3.63
Post-test examination service rate (µ2) 0.95 4.64
Initial examination service rate (µ3) 3 10.36
True negative rate (ν) 66.7% 98.9%
Physician utilization under ASO (uASOphysician) 29.4% 108.6%
Testing utilization under ASO (uASOtesting) 50.7% 190.0%
Table 4 Minimum and maximum values for the model primitives and resource utilizations under ASO, derived
from experimental factor values. All rates are per hour.
We create an additional set of problem instances by randomly selecting values for the
experimental factors from a uniform distribution given by the minimum and maximum
values reported in Table 3. These new problem instances constitute our test set. We use
the test set in Sections 5.3 and 5.4 to compare the performance of different policies.
For all the experiments in Sections 5.2-5.4, we set ED capacity as B = 15 and find L
by computing stationary probabilities from the transition matrices for a given problem
21
instance and a routing policy (see Appendix C). All problem instances are stable under
the finite-capacity assumption, even instances for which uASOtesting > 1 or uASO
physician > 1. We
compute and report the proportion of patients that are blocked, to assess the impact of
the finite-capacity assumption.
In Section 5.5, we study the performance of the system using DES. We focus on variants
of the base case, which is the instance corresponding to the baseline values in Table 3.
Details for the simulation model are provided in Appendix D.
5.2 Performance of the Optimal Threshold Policy
In this section, we study the performance of the threshold policy described in Section 4.5.
We find the optimal threshold (θ∗) by evaluating L(θ) for θ from −B to +B. We refer to
this policy as the optimal threshold policy.
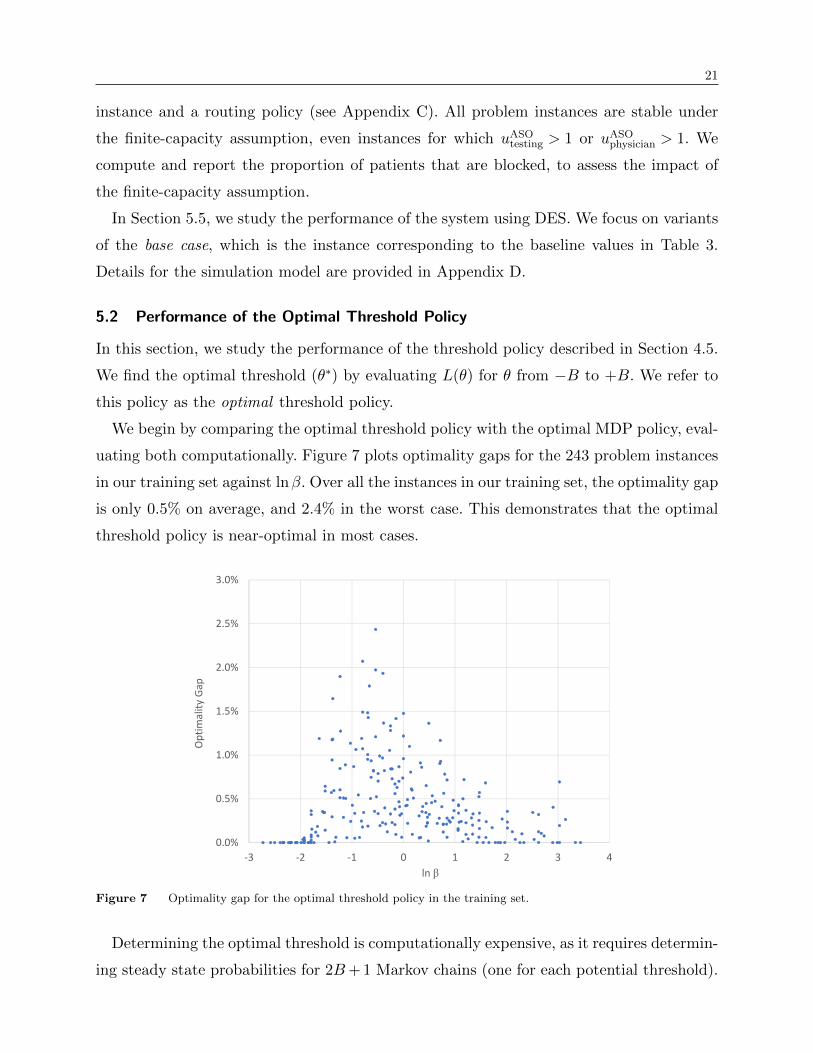
We begin by comparing the optimal threshold policy with the optimal MDP policy, eval-
uating both computationally. Figure 7 plots optimality gaps for the 243 problem instances
in our training set against lnβ. Over all the instances in our training set, the optimality gap
is only 0.5% on average, and 2.4% in the worst case. This demonstrates that the optimal
threshold policy is near-optimal in most cases.
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
-3 -2 -1 0 1 2 3 4
Opt
imal
ity G
ap
ln β
Figure 7 Optimality gap for the optimal threshold policy in the training set.
Determining the optimal threshold is computationally expensive, as it requires determin-
ing steady state probabilities for 2B+ 1 Markov chains (one for each potential threshold).

22
Figure 8 shows that the optimal threshold θ∗ and lnβ are highly correlated. In the next
section, we investigate the performance of an approximate threshold policy, in which θ∗ is
estimated as a linear function of lnβ.
-18
-15
-12
-9
-6
-3
0
3
6
9
12
15
18
-3 -2 -1 0 1 2 3 4
Opt
imal
Thr
esho
ld
ln β
Figure 8 Optimal thresholds (θ∗) for the instances in the training set.
5.3 Approximate Threshold Policy
We use the values of lnβ and θ∗ in the training set to estimate four regressions models,
shown in Table 5. For Models A and B, we utilize the entire training set (243 instances).
Model A is linear and Model B is piecewise linear, obtained by estimating separate regres-
sion models for two subsets of the training set: one for instances with β ≤ 1 (133 instances)
and another one for instances with β ≥ 1 (113 instances). For Models C and D, we discard
33 instances for which θ∗ =−B or +B. Similar to Model B, the coefficients in Model D
are estimated separately for 106 instances with β ≤ 1 and for 107 instances with β ≥ 1.
We evaluate the performance of the four models by computing the estimated threshold
(θ), evaluating L(θ), and comparing it to L for the optimal MDP policy, for every instance
in the test set. The results are at the bottom of Table 5. Model D performs best, with an
average optimality gap of 1.0% (compared to 0.7% for the optimal threshold policy) and
therefore we use Model D for the remainder of our analysis.
5.4 Extreme Routing Policies: NSO and ASO
In this section, we study the performance of the two extreme routing policies: NSO, which
sends all patients triaged as target to physician first, and ASO, which always routes those

23
Approximate threshold (θ) Optimal
Model A Model B Model C Model D threshold (θ∗)
β ≤ 1Intercept 2.70 (0.19) 0.10 (0.33) 2.39 (0.19) -0.15 (0.36)
Slope -4.75 (0.13) -7.01 (0.26) -4.10 (0.16) -7.22 (0.37)
N/Aβ ≥ 1
Interceptas above
1.51 (0.48)as above
0.90 (0.43)
Slope -3.62 (0.32) -2.79 (0.31)
β ≤ 1/β ≥ 1 R2 0.84 0.85/0.54 0.76 0.78/0.44
Out-of-sampleoptimality gap
Minimum 0.0% 0.0% 0.0% 0.0% 0.0%
Average 1.8% 1.2% 1.6% 1.0% 0.7%
Median 1.3% 1.0% 1.3% 0.8% 0.6%
Standard deviation 1.5% 0.8% 1.4% 0.7% 0.5%
Maximum 8.5% 3.9% 8.5% 3.9% 2.2%
Winning policy∗ 28.8% 63.4% 45.3% 74.1% N/A
Table 5 Four models for estimation of θ∗. Standard errors are shown in parentheses.∗ The percentages do not add up to 100% because of ties.
patients to testing. According to the medical literature we reviewed, these two extreme
policies are most frequently used in the clinical settings.
Figure 9 shows the test set optimality gaps for NSO, ASO, and the approximate threshold
policy. ASO performs well for lnβ > 1 and NSO performs well for lnβ <−1. Outside these
ranges, the performance of ASO and NSO is abysmal, with optimality gaps exceeding 100%
for some instances. The approximate threshold policy, in contrast, has optimality gaps
below 3.9% if based on Model D (and below 8.5% for Models A, B, and C). This indicates
that hospitals can improve their performance if they use standing orders selectively, based
on testing congestion and physician congestion.
5.5 DES Experiments: Relaxing the Finite-Capacity and Single-Server Assumptions
In this section, we use DES to further explore our model of standing orders. First, we
validate our Markov chain calculations by confirming, for a set of problem instances, the
agreement between the average number of patients in the system obtained via simulation
and that computed from the Markov chain probabilities. Table 6 shows that the Markov
chain results are within the DES confidence intervals.
5.5.1 Relaxing ED Capacity Constraint. We imposed a capacity constraint in
our MDP and Markov chain calculations, for tractability. In reality, EDs do have capacity
constraints, although the exact capacity value could be difficult to determine. We use the

24
0%
20%
40%
60%
80%
100%
120%
140%
160%
-3 -2 -1 0 1 2 3
Opt
imal
ity G
ap
ln β
Threshold Policy (Model D) NSO ASO
Figure 9 Optimality gap for NSO, ASO, and the approximate threshold policy in the test set.
Average number in system Blocking probability
Policy Markov chain Simulation Markov chain Simulation
ASO 7.70 7.61 ± 0.25 5.7% 5.5% ± 0.6%
Threshold policy 6.01 6.06 ± 0.18 2.3% 2.5% ± 0.4%
NSO 6.36 6.39 ± 0.15 2.8% 2.7% ± 0.3%
Table 6 Comparison of Markov chain and simulation performance estimates for the base case with B = 15.
DES model to explore the impact of increasing capacity or removing the capacity constraint
entirely, for the base case.
The base case optimal and approximate thresholds are identical: θ∗ = θ = 2. The base
case has lnβ =−0.25, which suggests (recall Figure 9) that ASO will perform poorly.
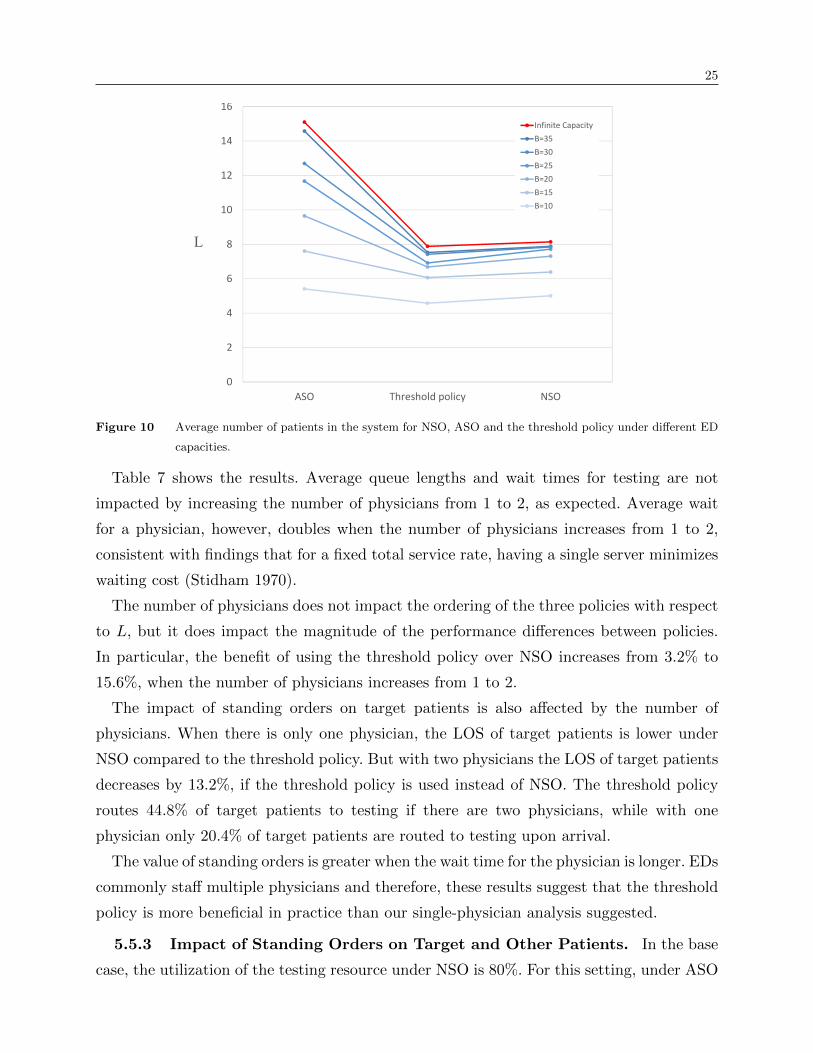
Figure 10 shows that as the capacity B increases, the average number in system increases,
for ASO, NSO, and the threshold policies, as one would expect. The cost (in terms of
percent increase in L) of using ASO rather than NSO increases from 19.1% to 85.4%
when B changes from 15 to ∞. The benefit of using the threshold policy rather than NSO
decreases from 5.1% to 3.2% over the same range of B values.
5.5.2 Increasing the Number of Physicians. We assumed a single physician for
tractability in our analysis of Section 4. Here, we investigate the robustness of our findings
to this assumption. We keep the capacity infinite, increase the number of physicians from
1 to 2, and halve the physician service rates (µi, i= 2,3,4) in order to keep the physician
utilization constant.
25
0
2
4
6
8
10
12
14
16
ASO Threshold policy NSO
L
Infinite CapacityB=35B=30B=25B=20B=15B=10
Figure 10 Average number of patients in the system for NSO, ASO and the threshold policy under different ED
capacities.
Table 7 shows the results. Average queue lengths and wait times for testing are not
impacted by increasing the number of physicians from 1 to 2, as expected. Average wait
for a physician, however, doubles when the number of physicians increases from 1 to 2,
consistent with findings that for a fixed total service rate, having a single server minimizes
waiting cost (Stidham 1970).
The number of physicians does not impact the ordering of the three policies with respect
to L, but it does impact the magnitude of the performance differences between policies.
In particular, the benefit of using the threshold policy over NSO increases from 3.2% to
15.6%, when the number of physicians increases from 1 to 2.
The impact of standing orders on target patients is also affected by the number of
physicians. When there is only one physician, the LOS of target patients is lower under
NSO compared to the threshold policy. But with two physicians the LOS of target patients
decreases by 13.2%, if the threshold policy is used instead of NSO. The threshold policy
routes 44.8% of target patients to testing if there are two physicians, while with one
physician only 20.4% of target patients are routed to testing upon arrival.
The value of standing orders is greater when the wait time for the physician is longer. EDs
commonly staff multiple physicians and therefore, these results suggest that the threshold
policy is more beneficial in practice than our single-physician analysis suggested.
5.5.3 Impact of Standing Orders on Target and Other Patients. In the base
case, the utilization of the testing resource under NSO is 80%. For this setting, under ASO

26
One physician Two physicians
Operational measure ASO Thresholdpolicy
NSO ASO Thresholdpolicy
NSO
Physician utilization* 68.6% 77.1% 80.4% 68.7% 75.0% 80.2%
Testing utilization 94.4% 84.5% 80.1% 94.5% 87.1% 81.3%
Physician queue length* 1.64 2.35 3.45 1.61 2.19 3.51
Testing queue length 11.83 3.92 3.09 11.89 4.19 3.51
Physician wait time (min)* 44.87 53.87 75.23 87.97 104.95 151.91
Testing wait time (min) 1059.13 402.41 333.28 1071.30 417.74 375.82
LOS - Other patients triaged as other (min) 59.97 72.21 90.37 119.07 140.43 183.34
LOS - Other patients triaged as target (min) 1236.56 134.31 91.88 1304.83 290.40 185.73
LOS - Other patients (min) 138.41 76.35 90.47 198.13 150.42 183.50
LOS - Target patients (min) 1214.12 622.96 613.32 1296.26 740.34 852.86
LOS - All patients (min) 405.27 214.53 221.60 465.65 300.05 353.92
L= average number in system 15.10 7.88 8.14 17.42 10.93 12.95
Proportion of target patients routed to test-ing after triage
100% 20.4% 0% 100% 44.8% 0%
Table 7 Comparison of different policies for the base case with infinite ED capacity.
* Averaged over the two physicians for the problem with two physicians
the testing queue is very congested and the average wait times are implausible (see the
‘ASO’ column for ‘One Physician’ in Table 7). We now add to our analysis a variant of the
base case, in which we decrease uNSOtesting from 80% to 50%. This change reduces the average
duration of testing from 88 min to 55 min. All other experimental parameters are held
fixed. The resulting lnβ is 1.08, so for this case we expect the performance of ASO would
be better than NSO. The threshold values are θ= θ∗ = 0, that is, we route patients triaged
as target to the physician if the physician queue is shorter than the testing queue.
Table 8 shows, for the base case and its variant, how the average wait and service times
change for different patient groups when we switch from NSO to the threshold policy or
to ASO. The purpose of this analysis is to investigate what might happen in an ED that
transitions from never using standing orders to using standing orders, either always, or
when recommended by the threshold policy.
As expected, for the instance with uNSOtesting = 50%, both ASO and the threshold policy
outperform NSO. In this instance, target patients are better off under either ASO or the
threshold policy as their waiting and service times decrease. Their service time decreases
as they now have only a single interaction with the physician. Their wait time decreases

27
because the physician’s utilization is lower, so the wait for the physician is shorter. The
decrease in the service time is larger for ASO because all target patients have only a single
encounter with the physician under this policy. Under the threshold policy, 23.1% of target
patients still have two encounters with the physician. Nevertheless, with the threshold
policy all patient categories experience shorter system waits as compared to their waits
under NSO and ASO.
Misclassified patients (‘other patients triaged as target’) are worse off under both ASO
and the threshold policy, and particularly so under ASO. Under ASO, they not only see an
increase in their service time because of unnecessary testing followed by a longer evaluation
by the physician—their waiting times are also longer as they have to wait for testing.
With ASO performing poorly for our base case, we focus our attention on the threshold
policy. The last row of Table 8 shows that for our base case where uNSOtesting = 80%, on average,
patients are better off under the threshold policy. The average LOS is 8.12 minutes less
than under NSO. It is notable that this improvement is due to lower physician utilization
which decreases the wait time for the largest category of patients (‘other triaged as other’).
Target patients are, in fact, worse off. Although their average service time is shorter, as
20.4% of them have only one encounter with the physician, the increased utilization of the
testing service increases their average wait.
The medical studies that we reviewed in Section 2 appear to take the viewpoint that the
aim is to reduce ED LOS and the means to do so is to reduce ED LOS for target patients.
None of the studies report the overall ED LOS, however, or otherwise measure possible
spillover effects on other patients. This simulation experiment demonstrates the importance
of measuring the overall ED LOS. It shows that a negative finding with respect to the
target group could, paradoxically, occur even if overall ED performance has improved.
Patient category Percentage Time in uNSOtesting = 50% uNSO
testing = 80%
process Threshold ASO Threshold ASO
Target 25%Wait -98.04 -83.85 12.71 616.01
Service -11.56 -15.03 -3.07 -15.02
Other triaged as target 5%Wait -12.61 46.00 17.43 1042.57
Service 51.97 68.84 25.00 102.11
Other triaged as other 70% Wait -31.68 -34.57 -18.08 -30.35
All patients 100% ED LOS -47.60 -43.26 -8.12 186.19
Table 8 Changes in the average process times (min) when using ASO and the approximate threshold policy
instead of NSO under different testing utilizations.
28
6. Discussion, Limitations, Conclusion
Standing orders allow an ED triage nurse to initiate certain medical tests for target patients
before they are seen by a physician. In the medical literature, standing orders are consid-
ered as a tool to reduce the ED LOS by reducing LOS for the target patients, without
taking a system-wide viewpoint. Further, only a few studies that we reviewed have reported
information on how triage nurses ascertained operational state of the ED when they made
the decision to invoke the standing orders. Standing orders protocols make the ETI mech-
anism possible, and the empirical OM literature suggests that servers are more likely to
initiate tasks early when the system is congested. In this paper, we developed a series of
mathematical and simulation models to investigate the impact of standing orders on the
ED as a whole and derived a simple but near-optimal threshold policy that indicates when
it is beneficial to enact standing orders.
Our policy is based on a single threshold (θ). It recommends that patients triaged as
target should be routed to testing if the difference between the number of patients waiting
for a physician and the number of patients waiting for testing is greater than or equal to θ.
We demonstrated that the optimal value of θ can be approximated using a linear function
of lnβ, where β is calculated from the model primitives. Our numerical results showed that
the performance of the approximate threshold policy is within 1.0% of the optimal policy.
The use of the approximate threshold policy requires accurate information on the oper-
ational status of the ED. This information can be obtained through direct observation of
the queues in the ED or could be available to the triage nurse through a computerized
information system. The continuing digitization of ED environments has facilitated avail-
ability of such information. For example, the Ministry of Health and Wellbeing of South
Australia informs constituents virtually in real-time of the operational status of the EDs
in the region (Government of South Australia 2020). Their ED dashboard is updated every
30 minutes, providing the expected ED waiting times, the number of patients waiting for
consults, radiology services, inpatient beds, etc.
Through our DES experiments, we investigated in detail the impact of standing orders
for different patient categories. In particular, we found that using standing orders could
improve the performance of an ED, not by decreasing the ED LOS of the target patients,
but rather through impacting other patients who are not subject to this mechanism. This
happens as sending some of target patients to the testing after triage decreases the load
for the physician, which in turn results in shorter wait times for the physician. We also

29
found that when the utilizations of the resources are higher, then using the approximate
threshold policy leads to greater improvements for the whole system compared to the
extreme routing policies—always or never using standing orders.
One of the limitations of our model is that we assumed the test results of those patients
routed to testing are ready before their first encounter with the physician. As this is not
always the case in an ED (Parris et al. 1997), one important extension of our work is
to incorporate the possibility of not having the test results available in time. Another
limitation of our model is that we considered stationary arrival rates for the patients. Our
threshold policy is based on a model that does not consider the fluctuations in the ED load
and staffing throughout the day. It would be interesting to study how taking into account
such variability in the inputs could impact the performance of our proposed policy.
References
Ansari, S, SMR Iravani, Q Shao. 2019. Optimal control policies in service systems with limited information
on the downstream stage. Naval Research Logistics (NRL) 66(5) 367–392.
Ashurst, JV, T Nappe, S Digiambattista, A Kambhampati, S Alam, M Ortiz, P Delpais, BG Porter, A Kurt,
BG Kane, et al. 2014. Effect of triage-based use of the Ottawa foot and ankle rules on the number
of orders for radiographic imaging. The Journal of the American Osteopathic Association 114(12)
890–891.
Bachmann, LM, E Kolb, MT Koller, J Steurer, G ter Riet. 2003. Accuracy of Ottawa ankle rules to exclude
fractures of the ankle and mid-foot: systematic review. British Medical Journal 326(7386) 417.
Batt, RJ, C Terwiesch. 2017. Early task initiation and other load-adaptive mechanisms in the emergency
department. Management Science 63(11) 3531–3551.
Castner, J, S Grinslade, Jr Guay, AZ Hettinger, JY Seo, L Boris. 2013. Registered nurse scope of practice
and ed complaint-specific protocols. Journal of Emergency Nursing 39(5) 467–473.
Cheung, WWH, L Heeney, JL Pound. 2002. An advance triage system. Accident and Emergency Nursing
10(1) 10–16.
Chonde, S, C Parra, CJ Chang. 2013. Minimizing flow-time and time-to-first-treatment in an emergency
department through simulation. 2013 Winter Simulations Conference (WSC). IEEE, 2374–2385.
Cochran, JK, KT Roche. 2009. A multi-class queuing network analysis methodology for improving hospital
emergency department performance. Computers & Operations Research 36(5) 1497–1512.
Compeau, S, M Howlett, S Matchett, J Shea, J Fraser, R McCloskey, P Atkinson. 2016. Does elimina-
tion of a laboratory sample clotting stage requirement reduce overall turnaround times for emergency
department stat biochemical testing? Cureus 8(10).

30
Corl, K. 2019. Hospitals’ new emergency department triage systems boost profits but compromise care.
https://www.statnews.com/2019/09/05/triage-system-boost-profits-compromises-care/.
Accessed 2020-05-25.
Davies, J. 1994. X-ray vision of shorter queues. Nursing Times 90(21) 52.
Delasay, M, A Ingolfsson, B Kolfal. 2016. Modeling load and overwork effects in queueing systems with
adaptive service rates. Operations Research 64(4) 867–885.
Dobson, G, T Tezcan, V Tilson. 2013. Optimal workflow decisions for investigators in systems with inter-
ruptions. Management Science 59(5) 1125–1141.
Edelstein, WA, M Mahesh, JA Carrino. 2010. MRI: time is dose—and money and versatility. Journal of the
American College of Radiology: JACR 7(8) 650.
Ellis, DG, J Mayrose, M Phelan. 2006. Consultation times in emergency telemedicine using realtime video-
conferencing. Journal of Telemedicine and Telecare 12(6) 303–305.
Fan, J, K Woolfrey. 2006. The effect of triage-applied Ottawa ankle rules on the length of stay in a Canadian
urgent care department: A randomized controlled trial. Academic Emergency Medicine 13(2) 153–157.
Ghanes, K, O Jouini, M Wargon, Z Jemai. 2015. Modeling and analysis of triage nurse ordering in emer-
gency departments. 2015 International Conference on Industrial Engineering and Systems Management
(IESM). IEEE, 228–235.
Goldstein, L, M Wells, C Vincent-Lambert. 2018. A randomized controlled trial to assess the impact of
upfront point-of-care testing on emergency department treatment time. American Journal of Clinical
Pathology 150(3) 224–234.
Government of South Australia, Ministry of Health and Wellbeing. 2020. Emergency department dashboard.
https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/
about+us/our+performance/our+hospital+dashboards/about+the+ed+dashboard/emergency+
department+dashboard. Accessed 2020-05-25.
Graff, LG, S Wolf, R Dinwoodie, D Buono, D Mucci. 1993. Emergency physician workload: A time study.
Annals of Emergency Medicine 22(7) 1156–1163.
Ho, JKM, JPC Chau, JTS Chan, CHY Yau. 2018. Nurse-initiated radiographic-test protocol for ankle
injuries: A randomized controlled trial. International Emergency Nursing 41 1–6.
Hu, X, S Barnes, B Golden. 2018. Applying queueing theory to the study of emergency department oper-
ations: a survey and a discussion of comparable simulation studies. International Transactions in
Operational Research 25(1) 7–49.
Huang, J, B Carmeli, A Mandelbaum. 2015. Control of patient flow in emergency departments, or multiclass
queues with deadlines and feedback. Operations Research 63(4) 892–908.
Hwang, CW, T Payton, E Weeks, M Plourde. 2016. Implementing triage standing orders in the emergency
department leads to reduced physician-to-disposition times. Advances in Emergency Medicine 2016.

31
Kalra, MG, KE Higgins, ED Perez. 2016. Common questions about streptococcal pharyngitis. American
Family Physician 94(1) 24–31.
Kamali, MF, T Tezcan, O Yildiz. 2018. When to use provider triage in emergency departments. Management
Science 65(3) 1003–1019.
Lee, KM, TW Wong, R Chan, CC Lau, YK Fu, KH Fung. 1996. Accuracy and efficiency of X-ray requests
initiated by triage nurses in an accident and emergency department. Accident and Emergency Nursing
4(4) 179–181.
Lee, WW, L Filiatrault, RB Abu-Laban, A Rashidi, L Yau, N Liu. 2016. Effect of triage nurse initiated
radiography using the Ottawa ankle rules on emergency department length of stay at a tertiary centre.
Canadian Journal of Emergency Medicine 18(2) 90–97.
Li, Y, Q Lu, H Du, J Zhang, L Zhang. 2018. The impact of triage nurse-ordered diagnostic studies on
pediatric emergency department length of stay. The Indian Journal of Pediatrics 85(10) 849–854.
Lindley-Jones, M, BJ Finlayson. 2000. Triage nurse requested X-rays—are they worthwhile? Emergency
Medicine Journal 17(2) 103–107.
Liu, S, B Liu, HB Xiao. 2014. The utilisation of ECG in the emergency department. The Briish Journal of
Cardiology 21 1–2.
Macleod, AJ, P Freeland. 1992. Should nurses be allowed to request X-rays in an accident & emergency
department? Emergency Medicine Journal 9(1) 19–22.
Nestler, DM, AR Fratzke, CJ Church, L Scanlan-Hanson, AT Sadosty, MP Halasy, JL Finley, A Boggust,
EP Hess. 2012. Effect of a physician assistant as triage liaison provider on patient throughput in an
academic emergency department. Academic Emergency Medicine 19(11) 1235–1241.
Parris, W, S McCarthy, AM Kelly, S Richardson. 1997. Do triage nurse-initiated X-rays for limb injuries
reduce patient transit time? Accident and Emergency Nursing 5(1) 14–15.
Pedersen, GB, JO Storm. 2009. Emergency department X-rays requested by physicians or nurses. Ugeskrift
for Laeger 171(21) 1747–1751.
Puterman, ML. 2014. Markov Decision Processes.: Discrete Stochastic Dynamic Programming . Wiley.
Retezar, R, E Bessman, R Ding, SL Zeger, ML McCarthy. 2011. The effect of triage diagnostic standing
orders on emergency department treatment time. Annals of Emergency Medicine 57(2) 89–99.
Rosmulder, RW, JJ Krabbendam, AH Kerkhoff, ER Schinkel, LF Beenen, JS Luitse. 2010. “Advanced triage”
improves patient flow in the emergency department without affecting the quality of care. Nederlands
Tijdschrift Voor Geneeskunde 154 A1109–A1109.
Rowe, BH, C Villa-Roel, X Guo, MJ Bullard, M Ospina, B Vandermeer, G Innes, MJ Schull, BR Holroyd.
2011. The role of triage nurse ordering on mitigating overcrowding in emergency departments: A
systematic review. Academic Emergency Medicine 18(12) 1349–1357.

32
Russ, S, I Jones, D Aronsky, RS Dittus, CM Slovis. 2010. Placing physician orders at triage: The effect on
length of stay. Annals of Emergency Medicine 56(1) 27–33.
Saghafian, S, WJ Hopp, MP Van Oyen, JS Desmond, SL Kronick. 2012. Patient streaming as a mechanism
for improving responsiveness in emergency departments. Operations Research 60(5) 1080–1097.
Saghafian, S, WJ Hopp, MP Van Oyen, JS Desmond, SL Kronick. 2014. Complexity-augmented triage:
A tool for improving patient safety and operational efficiency. Manufacturing & Service Operations
Management 16(3) 329–345.
Settelmeyer, D. 2018. Evaluation of an evidence-based throat-pain protocol to reduce left-without-being-seen,
length of stay, and antibiotic prescribing. Journal of Emergency Nursing 44(3) 236–241.
Shell, IG, GH Greenberg, RD McKnight, RC Nair, I McDowell, M Reardon, JP Stewart, J Maloney. 1993.
Decision rules for the use of radiography in acute ankle injuries: Refinement and prospective validation.
Journal of American Medical Association 269(9) 1127–1132.
Song, H, AL Tucker, KL Murrell. 2015. The diseconomies of queue pooling: An empirical investigation of
emergency department length of stay. Management Science 61(12) 3032–3053.
Steindel, SJ, PJ Howanitz. 2001. Physician satisfaction and emergency department laboratory test
turnaround time: Observations based on College of American Pathologists Q-Probes studies. Archives
of Pathology & Laboratory Medicine 125(7) 863–871.
Stidham, S. 1970. On the optimality of single-server queuing systems. Operations Research 18(4) 708–732.
Than, KC, YL Leong, BS Ngiam. 1999. Initiation of X-rays by the triage nurse: competency and its effect on
patients’ total time spent in the accident and emergency department. Annals of Emergency Medicine
34(4) S60.
Thurston, J, S Field. 1996. Should accident and emergency nurses request radiographs? Results of a multi-
centre evaluation. Emergency Medicine Journal 13(2) 86–89.
Valtchinov, VI, IK Ip, R Khorasani, JD Schuur, D Zurakowski, J Lee, AS Raja. 2019. Use of imaging in
the emergency department: Do individual physicians contribute to variation? American Journal of
Roentgenology 213(3) 637–643.
Wiler, JL, S Welch, J Pines, J Schuur, N Jouriles, S Stone-Griffith. 2015. Emergency department performance
measures updates: Proceedings of the 2014 emergency department benchmarking alliance consensus
summit. Academic Emergency Medicine 22(5) 542–553.
Yang, KK, SSW Lam, JMW Low, MEH Ong. 2016. Managing emergency department crowding through
improved triaging and resource allocation. Operations Research for Health Care 10 13–22.
Zayas-Caban, G, J Xie, LV Green, ME Lewis. 2019. Policies for physician allocation to triage and treatment
in emergency departments. IISE Transactions on Healthcare Systems Engineering 9(4) 342–356.

33
A. Summary of Empirical Medical Literature
Duration
Reference Location (months) LOS reduction for target population
Thurston and Field(1996)
UK NR Overall: 4 min (4.3%)a, Sent for X-rays: 14min (29.2%)a
Parris et al. (1997) Australia 5.5 With a fracture: 14 mina, Without afracture: 6 mina
Lindley-Jones andFinlayson (2000)
UK 0.5 37.2 min (36%)*** in time from triage totreatment decision
Fan and Woolfrey (2006) Canada 3 6.7 min (8.4%)a
Lee et al. (2016) Canada 12 28 min (19.6%)**
Ho et al. (2018) Hong Kong NR 13 min (14.9%)*
Lee et al. (1996) Hong Kong 3 Sent for X-rays: 18.59 min***
Pedersen and Storm(2009)
Denmark NR For 75% patients: 21 min (60%) in time fromadmittance to X-rays request; 24 min(26.6%) in time from admittance to patientreturned from X-ray
Rosmulder et al. (2010) Netherlands 0.75 Overall: 14 min (14%); Those who requireadditional diagnostic investigation: 27 min(18%)
Ashurst et al. (2014) USA 10 6.5 min (6.3%)a
Than et al. (1999) Singapore 3 24.5 min
Hwang et al. (2016) USA 5 -212 min (-52.7%)***; 26 min (16.9%)* intime from physician evaluation to dispositiontime if all tests were completed before thepatient was seen by the physician
Li et al. (2018) China 5 15 min (6.2%)***
Settelmeyer (2018) USA 3 6 min
Cheung et al. (2002) Canada NR 46 min
Retezar et al. (2011) USA 32 52 min (18%) in time between placement ofthe patient in treatment room anddisposition decision
Goldstein et al. (2018) South Africa 5.5 For a subset of tests: 20%* in time from firstphysician evaluation to disposition decision
Table 9 Additional information from the medical studies on the impact of standing orders initiated by triage
nurse.
Legend: NR = not reported.
Legend for statistical significance of LOS reduction: *: p < 0.05, **: p < 0.01, ***: p < 0.001, a: not
statistically significant, no code: statistical significance not reported.
B. Proof of Proposition 1
Consider state (E,R), where E1 <B. It is optimal to send a new patient triaged as target
to the physician first if
w(E+q3,R)≤w(E+q1,R).

34
To demonstrate the monotonicity of the optimal policy with respect to Q1, we begin by
proving that
∆(E,R) =w(E+q1,R)−w(E+q3,R)
is monotonically nondecreasing in E1 while other state variables are fixed.
Lemma 1. If E1 <B, Q1 > 0, and E2 > 0, then ∆(E,R) is monotonically nondecreasing
in E1.
Proof. Define ∆k(E,R) for k= 0,1,2, . . . as
∆k(E,R) =wk(E+q1,R)−wk(E+q3,R), ∀E;E1 <B,R, (24)
where wk are the value functions generated at stage k of the relative value iteration algo-
rithm. The algorithm starts with an initial value function w0 and recursively calculates
wk(E,R) as wk+1 =Dwk, where D is the DP mapping defined by (13):
(Dwk)(E,R) =E1
Λ+ pc(E) ·hkc (E,R) + ps(E) ·hks(E,R)
+ pt(E) ·hkt (E,R) + pr(R) ·∑
(ξ,pξ)∈Ξ(R)
pξ ·hkr(E+ ξ)
+(
1− pc(E)− ps(E)− pt(E)− pr(R))·wk(E,R). (25)
In the above, hkc , hks , h
kt , and hkr are defined as in Section 4 but using wk instead of w.
We prove by induction that the desired property is maintained through iterations of the
algorithm.
We assume w0(E,R) = 0 for all states. ∆0(E,R) is monotonically nondecreasing in E1.
Assume that this property is true for ∆k(E,R), which constitutes the induction hypothesis.
We show that the monotonicity property holds for ∆k+1(E,R) as well.
From (24) and (25) we have
∆k+1(E,R) =(Dwk)(E+q1,R)− (Dwk)(E+q3,R)
=pc(E+q1) min[wk(E+ 2q1,R),wk(E+q1 +q3,R)
]− pc(E+q3) min
[wk(E+q1 +q3,R),wk(E+ 2q3,R)
]+ ps(E+q1)wk(E+q1 +q4,R)− ps(E+q3)wk(E+q3 +q4,R)
+ pt(E+q1)wk(E+q2,R)− pt(E+q3)wk(E+q3−q1 +q2,R)
+ pr(R)∑
(ξ,pξ)∈Ξ(R)
pξ
(min
R′∈Ω(E+q1+ξ)wk(E+q1 + ξ,R′)− min
R′∈Ω(E+q3+ξ)wk(E+q3 + ξ,R′)
)

35
+(
1− pc(E+q1)− ps(E+q1)− pt(E+q1)− pr(R))wk(E+q1,R)
−(
1− pc(E+q3)− ps(E+q3)− pt(E+q3)− pr(R))wk(E+q3,R). (26)
The transition probabilities in the states (E+q1,R) and (E+q3) are all equal. Therefore,
we simplify (26):
∆k+1(E,R) =pc(E+q1)(
min[wk(E+ 2q1,R),wk(E+q1 +q3,R)
]−min
[wk(E+q1 +q3,R),wk(E+ 2q3,R)
])+ ps(E+q1)
(wk(E+q1 +q4,R)−wk(E+q3 +q4,R)
)+ pt(E+q1)
(wk(E+q2,R)−wk(E+q3−q1 +q2,R)
)+ pr(R)
∑(ξ,pξ)∈Ξ(R)
pξ
(min
R′∈Ω(E+q1+ξ)wk(E+q1 + ξ,R′)− min
R′∈Ω(E+q3+ξ)wk(E+q3 + ξ,R′)
)+(
1− pc(E+q1)− ps(E+q1)− pt(E+q1)− pr(R))(wk(E+q1,R)−wk(E+q3,R)
).
By further simplifications we have
∆k+1(E,R) =pc(E+q1)(
min[0,∆k(E+q1,R)
]+ max
[0,∆k(E+q3,R)
])+ ps(E+q1)∆k(E+q4,R) + pt(E+q1)∆k(E−q1 +q2,R)
+ pr(R)∑
(ξ,pξ)∈Ξ(R)
pξδk(E,R, ξ)
+(
1− pc(E+q1)− ps(E+q1)− pt(E+q1)− pr(R))
∆k(E,R), (27)
where
δk(E,R, ξ) = minR′∈Ω(E+q1+ξ)
wk(E+q1 + ξ,R′)− minR′∈Ω(E+q3+ξ)
wk(E+q3 + ξ,R′).
Note that Ω(E+q1 +ξ)⊆Ω(E+q3 +ξ). Denote the state of the physician after the optimal
decision is taken by R when the state is (E+q1 + ξ) (the first minimization in δk(E,R, ξ))
and by R when the state is (E+q3 + ξ) (the second minimization in δk(E,R, ξ)). If R= R,
then δk(E,R, ξ) is reduced to ∆k(E+ ξ, R). If R 6= R, then in the second minimization we
should have wk(E+q3 + ξ, R)≤wk(E+q3 + ξ, R), which gives
δk(E,R, ξ) =wk(E+q1 + ξ, R)−wk(E+q3 + ξ, R)≥ wk(E+q1 + ξ, R)−wk(E+q3 + ξ, R)
= ∆k(E+ ξ, R).

36
So, in any case we have
∆k+1(E,R)≥pc(E+q1)(
min[0,∆k(E+q1,R)
]+ max
[0,∆k(E+q3,R)
])+ ps(E+q1)∆k(E+q4,R) + pt(E+q1)∆k(E−q1 +q2,R)
+ pr(R)∑
(ξ,pξ)∈Ξ(R)
pξ∆k(E+ ξ, R)
+(
1− pc(E+q1)− ps(E+q1)− pt(E+q1)− pr(R))
∆k(E,R). (28)
Given the induction hypothesis we can verify that every term on the right of (28) is non-
decreasing in E1 and therefore we conclude ∆k+1(E,R) is also nondecreasing in E1.
As k→∞, we have wk→ w, and consequently ∆k→∆. The monotonicity property is
preserved through iterations and therefore ∆(E,R) is non-decreasing in E1. This completes
the proof of Lemma 1.
In state (E,R) for which E1 <B, Q1 > 0, and E2 > 0, if physician-first routing is optimal
for a patient triaged as target, then ∆(E,R) ≥ 0. If there is one additional patient in
the testing queue, i.e., in state (E + q1,R), then we know that ∆(E + q1,R) ≥∆(E,R)
according to Lemma 1, and therefore the physician-first routing remains optimal in state
(E+q1,R).
If testing-first routing is optimal for a patient triaged as target in state (E,R), then
∆(E,R) ≤ 0. If there is one less patient in the testing queue, i.e., in state (E − q1,R),
then ∆(E−q1,R)≤∆(E,R) according to Lemma 1, and therefore the testing-first routing
remains optimal in state (E−q1,R). This completes the proof of Proposition 1.
C. Calculation of Optimal Policy and Optimal Threshold Policy
For the optimal policy results reported in Section 4, we solved the MDP formulated in
Section 4, using the relative value iteration algorithm for unichain models (Puterman 2014,
pp. 373–374), implemented using Python 3.6 with the stopping criteria ε= 10−3.
For the optimal policy results reported in Section 5, we modified the MDP formulated
in Section 4 by replacing (22) with the following rule for routing patients to the physician,
in order to approximate an FCFS policy:
A patient is selected from Qi, i= 2,3,4, with probability Qi/E2, if E2 > 0,
Otherwise, the physician remains idle.(29)
We solved this modified MDP using the relative value iteration algorithm, implemented
using Python 3.6 with the stopping criteria ε= 10−5 and a maximum of 10,000 iterations.

37
For the optimal threshold policy results reported in Section 5, we constructed the transi-
tion probability matrix P (θ) for the Markov chain induced by using (23) for triage routing
and (29) for physician routing. We obtained the stationary probability vector π for this
Markov chain by solving the system Aπ= b, using the SciPy Python library (Release 1.4.1).
The matrix A was set to P (θ)T − I, with the last row replaced by a row of ones, and
b= [0, . . . ,0,1]T . We then used π to compute L(θ) =∑
x∈X π(x)E1(x), where we have used
x to index states in X .
D. DES Models
We developed DES models using Arena software Version 15.10.00001 to simulate patient
flow in an ED with and without standing orders, as described in Figures 3–4. Our simulation
results are based on 100 replications of 30 days, with a warm-up period of 10,000 minutes
(6.94 days).
A physician selects the next patient to see according to an FCFS policy. In the model
with two physicians, new patients are randomly assigned to one of the physicians upon
arrival. A patient is always seen by their assigned physician.


















