
Mobilized CD34+ Cells for Refractory Angina: Design and Rationale for the RENEW Study Thomas J....
31
Mobilized CD34+ Cells for Refractory Angina: Design and Rationale for the RENEW Study Thomas J. Povsic, MD, PhD on behalf of the RENEW Investigators
-
Upload
felicity-dawson -
Category
Documents
-
view
220 -
download
3
Transcript of Mobilized CD34+ Cells for Refractory Angina: Design and Rationale for the RENEW Study Thomas J....

Mobilized CD34+ Cells for Refractory Angina:
Design and Rationale for the RENEW Study
Thomas J. Povsic, MD, PhDon behalf of the RENEW Investigators

All Rights Reserved, Duke Medicine 2007
Disclosure Statement of Financial Interest
• Grant/Research Support• Grant/Research Support
• Baxter Healthcare Corporation• Revalesio Inc.
Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below.
Affiliation/Financial Relationship Company

All Rights Reserved, Duke Medicine 2007
Scope
• Estimated that 600,000 – 1.8 million Americans suffer from refractory angina
• 50,000 – 100,000 new cases per year• Increasing incidence• Poor QOL• Variable outcomes• Poor success of novel therapeutics

All Rights Reserved, Duke Medicine 2007
Treatment effect of bone marrow cells implantation on total exercise time on treadmill test.
Tse H et al. Eur Heart J 2007;28:2998-3005
PROTECT-CAD Trial

All Rights Reserved, Duke Medicine 2007
Treatment effect of bone marrow cells implantation on left ventricular ejection fraction as determined by cardiac magnetic resonance imaging.
Tse H et al. Eur Heart J 2007;28:2998-3005
PROTECT-CAD Trial

All Rights Reserved, Duke Medicine 2007
van Ramshorst, J. et al. JAMA 2009;301:1997-2004
Double Blind Placebo Controlled Trial of Treatment of Refractory Angina with BM MNCs

All Rights Reserved, Duke Medicine 2007
van Ramshorst, J. et al. JAMA 2009;301:1997-2004
Double Blind Placebo Controlled Trial of Treatment of Refractory Angina with BM MNCs

All Rights Reserved, Duke Medicine 2007
Original Description of Endothelial Progenitor Cells (EPC) in Adults•CD34+ cells isolated•Cultured on fibronectin•Grew into colonies resembling embryonic blood islands
Asahara et al. Science 1997;275:964-7
All Rights Reserved, Duke Medicine 2007
Treatment Groups 1) PBS: 100 µl 2) Low 34: 5X103 cells/ rat kg 3) Mid 34: 5X105 cells/ rat kg 4) Mid MNC: 5X105 cells/ rat kg 5) High MNC: tMNCs containing Mid EPC dose n=8~10 in each group
PreClinical Models

All Rights Reserved, Duke Medicine 2007
0
10
20
30
40
50
***
PBSLow34
MidMNC
Mid34
High MNC
Fractional Shortening (%)
16
20
24
28
PBSLow34
MidMNC
Mid34
**
Regional Wall Motion Score
HighMNC
* *
Human CD34 Transplant Improves Left Ventricular Function Post-MI
Kawamoto et al, Circulation (2006) 114:2163Less fibrosis, more endothelial markers with CD34+ cells

All Rights Reserved, Duke Medicine 2007
1 x 105 CD34+ cells/kg
5 x 105 CD34+ cells/kg
Endomyocardial Mapping and Injection with NOGAIsolex selected CD34+ cells / Placebo Rx
Cell Mobilization (GCSF 5mcg/kg/d x 5d)Apheresis on Day 5
Follow-up Safety and Efficacy Assessments:1,2, 4 weeks and 2, 3, 6, 9, and 12 months; ETT at 3, 6, 12 months
MRI at 6 months, SPECT at 6 & 12 months
Screening and Baseline Visits
Placebo
Randomization
Phase 1 Randomized, Double-Blind, Placebo Controlled Dose-Escalation Trial of Autologous CD34+ Cell Therapy for Refractory Myocardial Ischemia
Subject population (n=24)
• CCS class III or IV Angina• Attempted “best” medical
therapy• Non-candidate for
Surgical/Perc. revasc.• Ischemia on SPECT• 1-6 min. Bruce protocol with
angina or anginal equivalent at baseline
• AICD or LifeVest
5 x 104 CD34+ cells/kg

All Rights Reserved, Duke Medicine 2007
Phase I: The Dose Range is Feasible
1.00
10.00
100.00
ControlNo cells
Group 1 5 X 104 cells
Group 21 x 105 cells
Group 3 5 X 105 cells
A
uto
-CD
34+
Cell D
ose/k
g x
10
4
(
log
scale
)
Actual Auto-CD 34+ Cell Dose Delivered / kg (n = 6 / dose group)
Losordo D W et al. Circulation 2007;115:3165-3172

All Rights Reserved, Duke Medicine 2007
3 6 12-20
-15
-10
-5
0
5
10
Control
CD34+ Cell
Angina Episodes per week
(Change from Baseline)
Phase I: Angina FrequencyEpisodes per Week
12 month control data is not represented due to control patient cross-over after 6 months
Months
+6.5
-11.6**
-4.5
-12.6-15.6
**p=0.053 ANOVA between treatment groups Losordo D W et al. Circulation 2007;115:3165-3172

All Rights Reserved, Duke Medicine 2007
1 x 10^5 CD34+ cells/kg (n = 55)
5 x 10^5 CD34+ cells/kg (n = 56)
Endomyocardial Mapping and Injection with NOGAIsolex selected CD34+ cells / Placebo Rx
Cell Mobilization (GCSF 5mcg/kg/d x 5d)Apheresis on Day 5
Follow-up Safety and Efficacy Assessments:1 - 7 days, and 1, 3, 6, and 12 months; ETT at 3, 6, 12 months
MRI at 6 months, SPECT at 6 & 12 months
Screening and Baseline Visits
Placebo (n = 56)
Randomization
Randomized, Double-Blind, Placebo Controlled Trial of Autologous CD34+ Cell Therapy for Refractory Myocardial Ischemia
Subject population (n=167)
• 21-80 yrs• CCS class III or IV Angina• Attempted “best” medical
therapy• Non-candidate for
Surgical/Perc. revasc.• Ischemia on SPECT• 3-10 min. mod. Bruce
protocol with angina or anginal equivalent at baseline

All Rights Reserved, Duke Medicine 2007
Change in Angina Counts

All Rights Reserved, Duke Medicine 2007
Change in Angina – 12 months
All Rights Reserved, Duke Medicine 2007
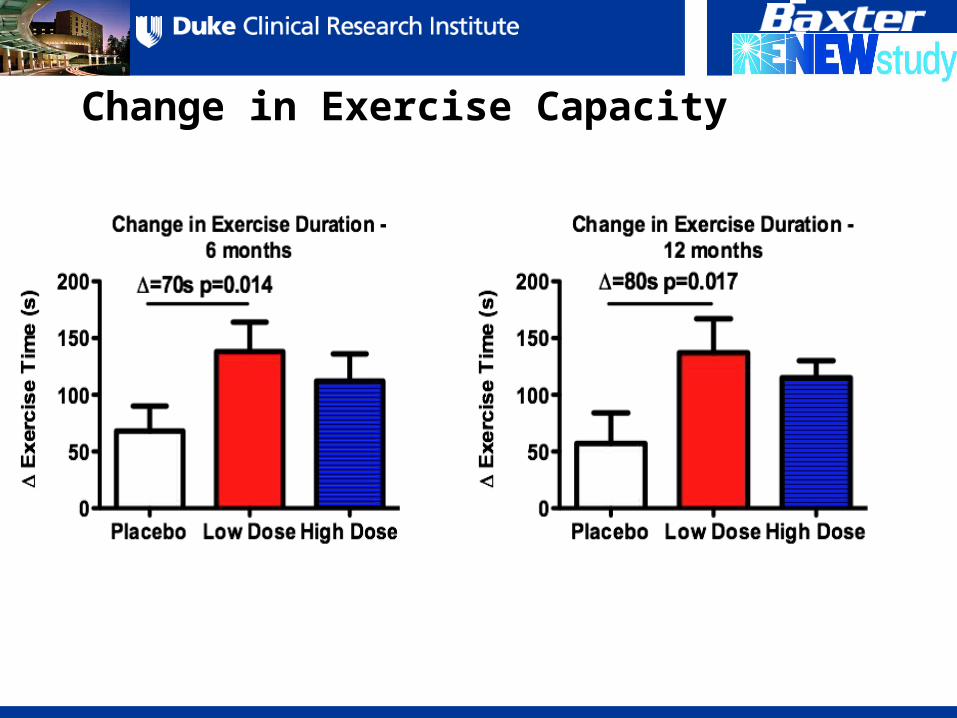
Change in Exercise Capacity

All Rights Reserved, Duke Medicine 2007
Control 1x105
CD34+cells/kg
5x105
CD34+cells/kg
p-value*
Death 3(5.4%) 0(%) 0(%) 0.107
MI 7 (12.5%)
3(5.5%) 3(5.4%) 0.305
Death, MI 10(17.9%)
3(5.5%) 3(5.4%) 0.058
Death, MI, Urgent Revasc
11(19.6%)
5(9.1%) 4(7.1%) 0.106
Death, MI, Urgent Revasc,
Worse CHF, ACS
15(26.8%)
7(12.7%) 7(12.5%) 0.093
Pts with MACE events from start of mobilization thru 12 mo in injected pts; *= Fisher’s Exact Test
Major Adverse Cardiac Events (12 Months)

All Rights Reserved, Duke Medicine 2007
Control 1x105
CD34+cells/kg
5x105
CD34+cells/kg
p-value*
Death 7(12.5%) 1(1.8%) 2(3.6%) 0.081
MI 10 (17.9%)
9(16.4%) 6(10.7%) 0.587
Death, MI 15(26.8%)
10(18.2%) 6(10.7%) 0.096
Death, MI, ACS
Hospitalization
17(30.4%)
10(18.2%) 8(14.3%) 0.101
Death, MI, ACS or Worse
CHF Hospitalizatio
n
19(33.9%)
12(21.8%) 9(16.1%) 0.078
Pts. with MACE events from start of mobilization thru 12 mo in injected pts.; *= Fisher’s Exact Test
Major Adverse Cardiac Events (24 Months)

All Rights Reserved, Duke Medicine 2007
Efficacy Comparison: Change in ETT
0
20
40
60
80 7080
23.8
45.9
2416
35
Δ E
xerc
ise T
ime

All Rights Reserved, Duke Medicine 2007
CD34-6 Month CD34-12 Month
Ranexa CARISA EECP
Angina/week -3 -5.6 -0.43 -0.8 -1.4
-5.5
-4.5
-3.5
-2.5
-1.5
-0.5
Change in Angina Episodes per Week
Ch
ang
e in
Nu
mb
ers
of
An
gin
alE
pis
od
es P
er W
eek

All Rights Reserved, Duke Medicine 2007
RENEW:
A Prospective, Randomized, Double-Blinded, Active-controlled Study to Determine the Efficacy and Safety of Targeted Intramyocardial Delivery of G-CSF Mobilized Autologous CD34+ Cells For the Improvement In Total Exercise Time in Subjects with Refractory Angina and Chronic Myocardial Ischemia
• RENEW is the first trial of cell therapy for CV disease designed to fulfill requirements for US regulatory approval
• Powered to demonstrate efficacy on clinical endpoints• Largest planned US trial in cell therapy• Largest currently enrolling cell therapy trial in CV disease• RENEW represents a landmark study in the field, setting
benchmarks for development of other cell therapies for CV disease.

All Rights Reserved, Duke Medicine 2007
RENEW Efficacy and Safety Endpoints
• Primary Efficacy Endpoint– Change in total exercise duration using a standardized
Modified Bruce Protocol ETT at 12 months
• Secondary Efficacy Endpoints– Change in angina frequency at 12 months– Change in exercise duration and angina frequency at 6
months
• Exploratory Endpoints– Incidence of MACE* and SAEs in all subjects
* MACE: all death, non-fatal MI, CVA, Cardiac rehosp

All Rights Reserved, Duke Medicine 2007
1 x 105 CD34+ cells/kg (n = 200)
Unblinded Standard of Care (n = 100)
Cell Mobilization (G-CSF 5 mg/kg/d x 4d)Apheresis on Day 5
Screening and Baseline Visits
Active Control(n = 100)
Randomization
Safety Assessments during 24 month follow-up: AEs,
SAEs, MACE
RENEW Study Design
Inclusion Criteria:• 21-80 yrs• CCS class III or IV Angina• Attempted “best”
medical therapy• Non-candidate for Surgical/Perc. revasc.• Ischemia w/stress• 3-10 min. mod. Bruce
protocol with angina or anginal equivalent at baseline
• ETT reproducible <20%• 7 angina/wk
Exclusion Criteria:• Recent hospitalization• Other angiogenic trials• Must be willing to forgo other
angiogenic/experimental txt x 2 years
Pre-Qual Committee Central Review

All Rights Reserved, Duke Medicine 2007
Auto-CD34+ Cell Product: Centralized Processing
Mobilization, apheresis, and shipment to centralized manufacturing facility
Apheresis at Clinical
Site
ISOLEX CD34+ cell selection, syringe preparation, release testing, and shipment to clinical sites
Cell Processing
at Centralized
Facility
Receive product, NOGA mapping and injection in catheter lab
Injection at Clinical
Site
Auto CD34+ Cell Product
<48 hrs
<48 hrs

All Rights Reserved, Duke Medicine 2007
1 x 105 CD34+ cells/kg (n = 200)
Unblinded Standard of Care (n = 100)
Intramyocardial Mapping and Injection with NOGA
ISOLEX selected CD34+ cells / Placebo
Cell Mobilization (G-CSF 5 mg/kg/d x 4d)Apheresis on Day 5
Efficacy Assessments during 12 month follow-up: ETT, angina frequency, and QoL
(SF-36)Safety Assessments during 24 month
follow-up: AEs, SAEs, MACE
Screening and Baseline Visits
Active Control(n = 100)
Randomization
Safety Assessments during 24 month follow-up: AEs,
SAEs, MACE
RENEW Study Design
Inclusion Criteria:• 21-80 yrs• CCS class III or IV Angina• Attempted “best”
medical therapy• Non-candidate for Surgical/Perc. revasc.• Ischemia w/stress• 3-10 min. mod. Bruce
protocol with angina or anginal equivalent at baseline
• ETT reproducible <20%• 7 angina/wk
Exclusion Criteria:• Recent hospitalization• Other angiogenic trials• Must be willing to forgo other
angiogenic/experimental txt x 2 years
Pre-Qual Committee Central Review

All Rights Reserved, Duke Medicine 2007
Monitoring Committees• Steering Committee
– Responsible for oversight of study, data interpretation, protocol and amendments, publications
– Oversee country activities
• Data Safety Monitoring Board– Will be un-blinded and will oversee safety and integrity of study– Recommend changes in study arms– Meetings after 10, 25, 50, 100, 200 and 300 patients
• Clinical Events Committee– Blindly adjudicate clinical events
• Pre-Qualification Committee
27

All Rights Reserved, Duke Medicine 2007
Study Population: Main Inclusion Criteria
• Male or female subjects who are 21 to 80 years of age• CCS class III or IV chronic refractory angina• On maximal tolerated doses of anti-anginal drugs
– At least 2 of 4 classes recommended
• Unsuitable for conventional revascularization as determined at site and confirmed by an independent pre-qualification committee
• Objective evidence of inducible ischemia in the potential injection target zone, using clinically accepted assessment of ischemia within 1 year of screening provided the subject has remained clinically stable
• LVEF ≥25% at screening.• Minimum average of 7 angina or angina-equivalent episodes per week• Able to complete a minimum of 3 minutes but no more than 10 minutes on a
treadmill using the Modified Bruce Protocol during 2 ETTs performed during screening period with ≤ 20% variability
• Subject must experience angina or angina-equivalent symptoms at each of the 2 ETTs

All Rights Reserved, Duke Medicine 2007
Comparator ArmsBlinded Active Control Unblinded Standard of Care
Advantages
Only true double-blind design
Blinding minimizes both subject and assessor bias
Impact of placebo effect on safety endpoints allows for more rigorous comparisons
Allows for assessment of efficacy of the cell product
Regulatory Considerations (combo product)
Safety of Auto-CD34+ cell therapy versus SOC may be assessed
Eliminates potential impact of intervention on cardiac outcomes
Subjects will reflect those of general refractory angina population
Regulatory Considerations
Challenges Potential periprocedural safety risks due to minimal apheresis & femoral artery access
Utility of clinical comparison
May negatively impact subject enrollment and retention (issues with differential retention)
No placebo effect: subjects may have a poorer perception of overall health.
Patients may seek out other options
No reasonable efficacy assessment

All Rights Reserved, Duke Medicine 2007
Statistical Plan• Sample Size
– 400 completed subjects
– 90% power to detect 60 second
difference in mean change from
baseline in total exercise time
• Statistical Approach– Closed form testing procedure on
primary and secondary efficacy
endpoints
– Allows for potential inclusion of
secondary efficacy endpoints in
product label

All Rights Reserved, Duke Medicine 2007
Conclusions
• RENEW is the first trial of cell therapy for CV disease designed to fulfill requirements for US regulatory approval
• Powered to demonstrate efficacy on clinically important endpoints
• Largest planned US trial in cell therapy
• Largest currently enrolling cell therapy trial in CV disease
• RENEW represents a landmark study in the field, setting benchmarks for development of other cell therapies for CV disease.


















