MITRAL REGURGITATION IN PATIENT WITH SEVERE...
48
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases “Sotiria” Athens
Transcript of MITRAL REGURGITATION IN PATIENT WITH SEVERE...

MITRAL REGURGITATION IN PATIENT WITH
SEVERE AORTIC VALVE STENOSIS
Ioannis Alexanian, MD, PhD Department of Cardiology
General Hospital of Chest Diseases “Sotiria” Athens
I HAVE NOTHING TO DECLARE

Management of severe aortic stenosisGuidelines on the management of valvular heart Disease ESC 2012
European Heart Journal (2012) 33, 2451–2496

Aortic valve and double-valve replacement in the last 10 years
Nombela-Franco L. et al J Am Coll Cardiol 2014;63:2643–58

THE FUTURE OF TRANSCATHETER AORTIC VALVE IMPLANTATION
European Heart Journal (2016) 37, 803–810
Germany
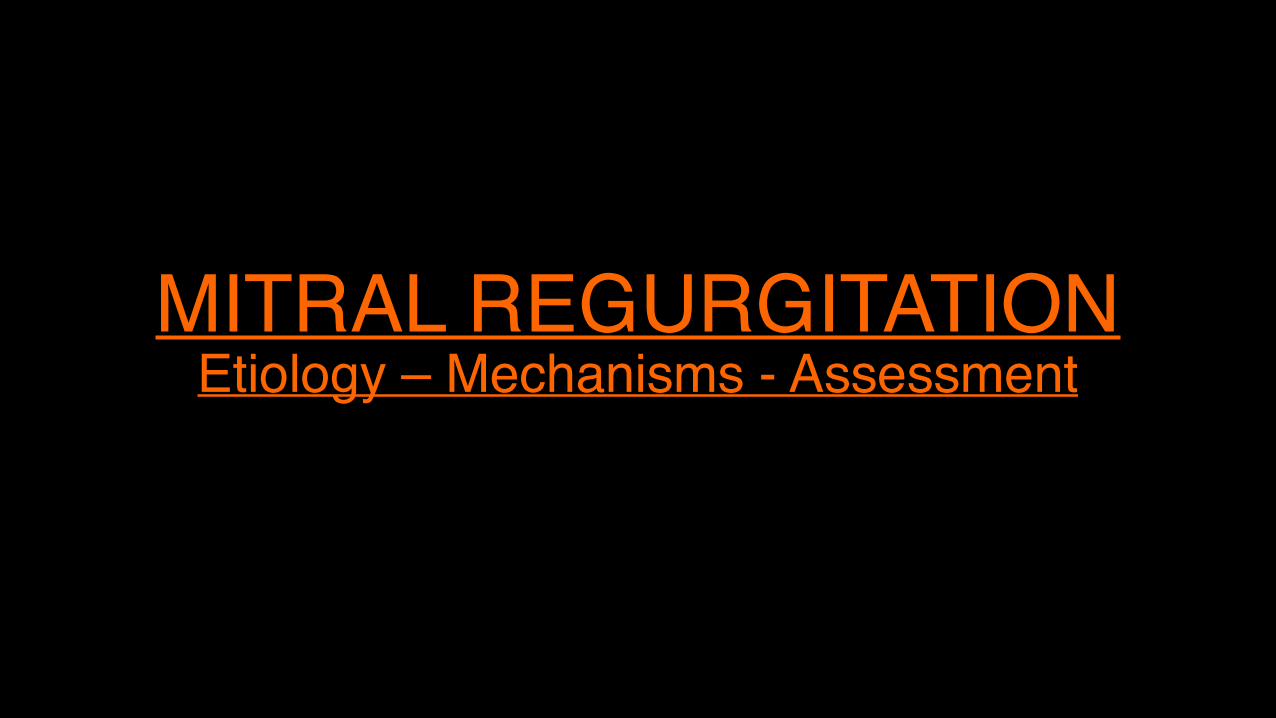
MITRAL REGURGITATION Etiology – Mechanisms - Assessment
Dal-Bianco J. et al. Can J Cardiol. 2014 September ; 30(9): 971–981

Causes and mechanisms of mitral regurgitation
Mechanism
Organic Functional
CauseNon-ischemic
• Degenerative (annular calcification, flail leaflets);
• Rheumatic; • Endocarditis; • Iatrogenic (drugs, radiation); • Inflammatory (lupus, endomyocardial
fibrosis…); • Traumatic (rupture papillary muscle or
chord)
• Cardiomyopathy; • Myocarditis; • Any cause of left
ventricular remodelling
Ischemic Rupture papillary muscle Functional ischemic
J Am Coll Cardiol 2014;63:2643–58
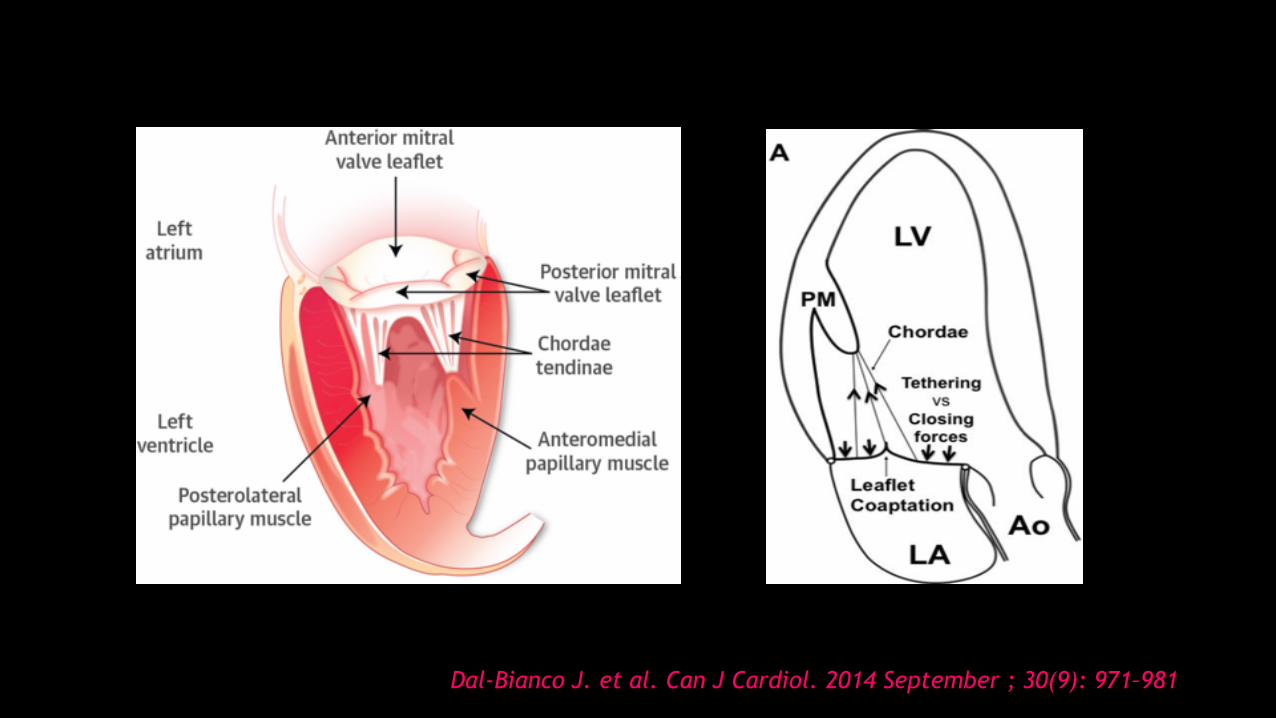
Heterogeneity of FMR

Zamorano ZL et al. Heart. 2015 Jan;101(2):146-54
Echocardiography assessment of MR severity: main approachesMethod Recording technique/equation Strengths Limitations
Colour jet areaApical image, includes LA Nyquist limit 50–60 cm/s Trace maximum regurgitant jet MR jet/LA area
MR screening
Dependent on technical and haemodynamic factors Correlation with severity is poor Not recommended to quantify severity
Vena contracta width
Colour flow through the MV in PLAX or apical 4C view Identify the image with maximal flow through the valve VCW is the narrowest region of the regurgitant jet
Simple method Independent of haemodynamics, pressure and flow rate
Low colour gain, poor acoustic window, failure to assess multiple jets, non-circular EROA: underestimate VCW High colour gain, AF: overestimate VCW Dynamic behaviour of MR
PISA method
Apical 4C view / Mid systole Nyquist limit ≈15–40 cm/s Peak CW MR velocity EROA=2πr2×Va/peak MRV RVol=EROA×VTIMR
Independent of haemodynamics, pressure and flow rate Preferred quantitative approach
Assumption of a hemispheric shape and a circular EROA Dynamic behaviour of MR
Volumetric method
Apical 4C view/apical 5C view PW at the MV/PW at the LVOT Mitral annulus diameter/LVOT diameter Mitral inflow volume=MV d×0.785×VTIMV LVOT volume=LVOT d×0.785×VTILVOT RVol=mitral inflow volume−LV outflow volume RF=RVol ×100/mitral inflow volume EROA=RVol/VTIMR
Integration of the systolic behaviour of MR Alternative method if PISA or VCW are not accurate or applicable
Time consuming Inaccurate if significant AR Less reproducible Not recommended as first line method
3D echocardiography
Full volume colour Doppler or 3D zoom acquisitions of the MR jet: dataset cropping with MPR tools for evaluation of VCA
Diagnosis of location and extent of disease No geometrical assumptions Functional MR, multiple or eccentric jets
Poor acoustic window Poor spatial and temporal resolution of live acquisition of 3D colour Doppler Off line manipulation Dynamic behaviour of MR

Echocardiographic evaluation of mitral regurgitation severity Mild Moderate SevereSpecific signs Central jet Small (<4 cm²) MR more than mild
but no criteria for severe MR
largeLA area <10% of LA >40% of LAVCW <0.3cm ≥0.7 cmFlow convergence No or minimal Large Systolic reversal in pulmonary veins
No Yes
Supportive signs A-wave dominance MR more than mild
but no criteria for severe MR
E wave >1.5m/sDoppler MR signal Low-density High-densityLV and LA size Normal EnlargedQuantitative parameters RVol (ml/beat) <30 30-59 ≥60 RVol (ml/beat) in FMR* ≥30RF (%) <30 30-49 ≥50ERO (cm²) <0.20 0.20-0.39 ≥0.40 ERO (cm²) in FMR* ≥0.20
J Am Coll Cardiol 2014;63:2643–58
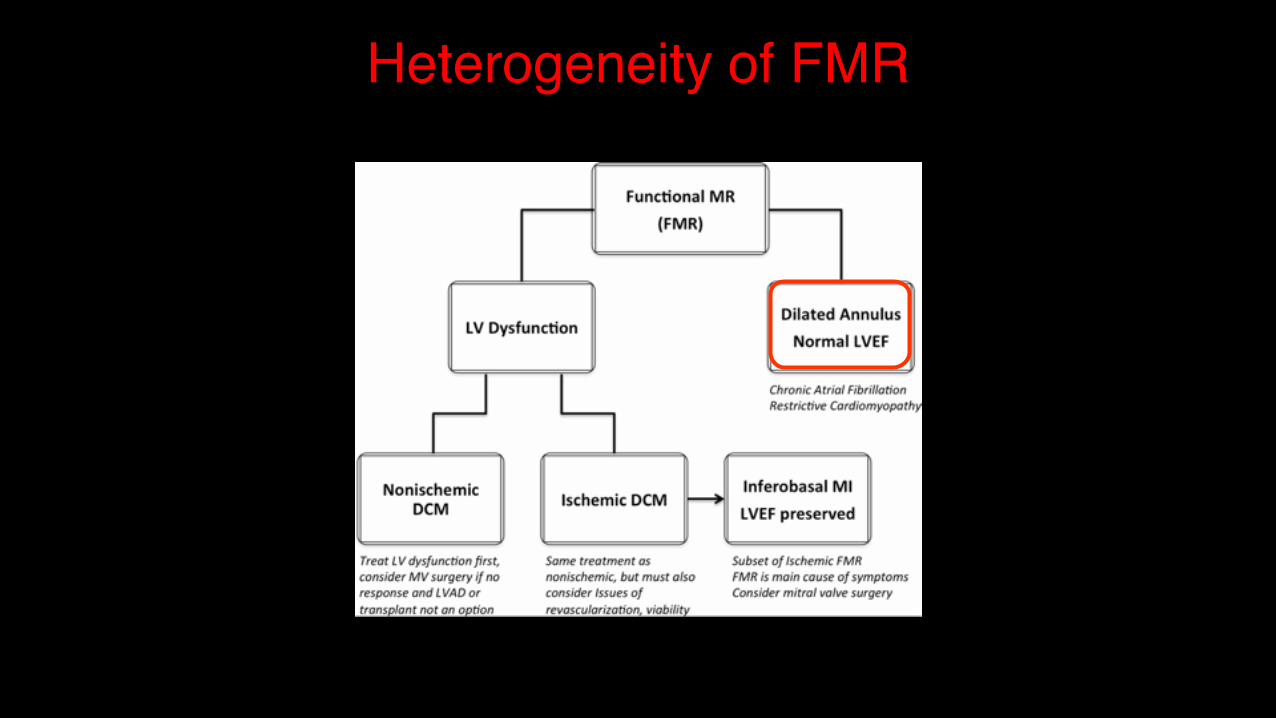
Proposed algorithm for primary MR severity assessment with echocardiography
Zamorano ZL et al. Heart. 2015 Jan;101(2):146-54

Pathophysiology of concomitant mitral regurgitation in aortic stenosis
European Heart Journal (2014) 35, 2627–2638

SURGICAL AORTIC VALVE REPLACEMENT (SAVR) IN THE PRESENCE OF SIGNIFICANT MR

Guidelines on the management of valvular heart Disease ESC 2012
When MR is associated with severe AS, its severity may be overestimated in the presence of the high ventricular pressures and careful quantification is required.
As long as there are no • morphological leaflet abnormalities (flail or prolapse, post-
rheumatic changes, or signs of infective endocarditis), • mitral annulus dilatation or marked abnormalities of LV
geometry, Surgical intervention on the mitral valve is in general not necessary and non-severe secondary MR usually improves after the aortic valve is treated.
European Heart Journal (2012) 33, 2451–2496

Changes in Moderate Mitral Regurgitation (Functional Etiology) After Surgical Aortic Valve Replacement
J Am Coll Cardiol 2014;63:2643–58
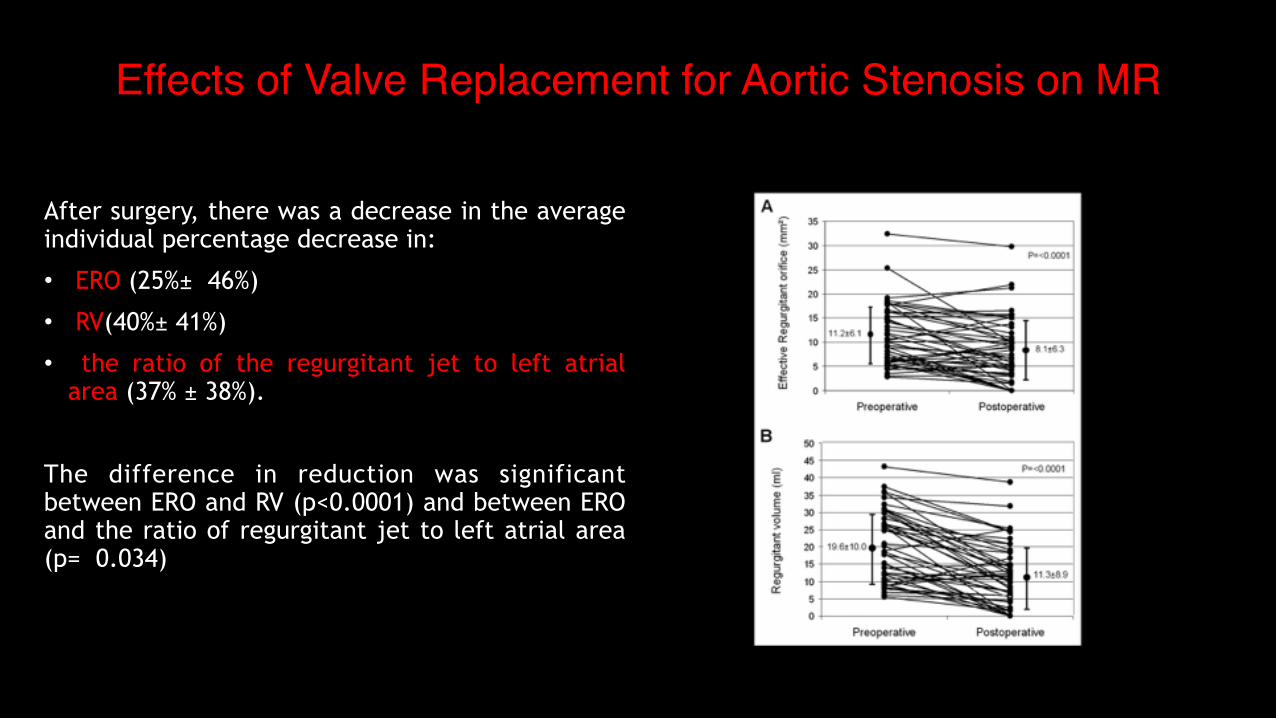
Effects of Valve Replacement for Aortic Stenosis on MR
After surgery, there was a decrease in the average individual percentage decrease in:
• ERO (25%± 46%)
• RV(40%± 41%)
• the ratio of the regurgitant jet to left atrial area (37% ± 38%).
The difference in reduction was significant between ERO and RV (p<0.0001) and between ERO and the ratio of regurgitant jet to left atrial area (p= 0.034)

Aortic Valve Replacement and Concomitant Mitral Valve Regurgitation in the Elderly
• Moderate MR was an independent risk factor impacting long-term survival
• MR persisted or worsened in 65.4% of patients with intrinsic mitral valve disease (myxomatous, calcific, or ischemic MR)
• MR improved in 81.8% of functional MR patients
Barreiro C. et al. Circulation. 2005;112 [suppl I]:I-443–I-447
408 consecutive elderly patients underwent isolated AVR and were stratified into no/mild MR (Group I; n=338) versus moderate MR (Group II; n= 70)

Effect of Aortic Valve Replacement for Aortic Stenosis on Severity of MR
Vanden Eynden F. et al. Ann Thorac Surg 2007;83:1279–84
80 patients Preoperative MR was moderate (2) in 78 patients (97.5%) and moderate-severe (3) in 2 patients (2.5%). MR was classified as rheumatic (32%), ischemic (32%), functional (21%), and myxomatous (15%).
The etiology of mitral regurgitation before AVR was independently correlated with MR improvement

Natural History and Predictors of Outcome in Patients With Concomitant Functional MR at the Time of AVR
Ruel M. et al. Circulation. 2006;114[suppl I]:I-541–I-546
AS patients with FMR ≥2 and 1 additional risk factor • LA >5 cm • preoperative pAVgradient <60 mm Hg, • AF were at increased risk for the composite outcome and of MR>2 at 18 months postoperatively.
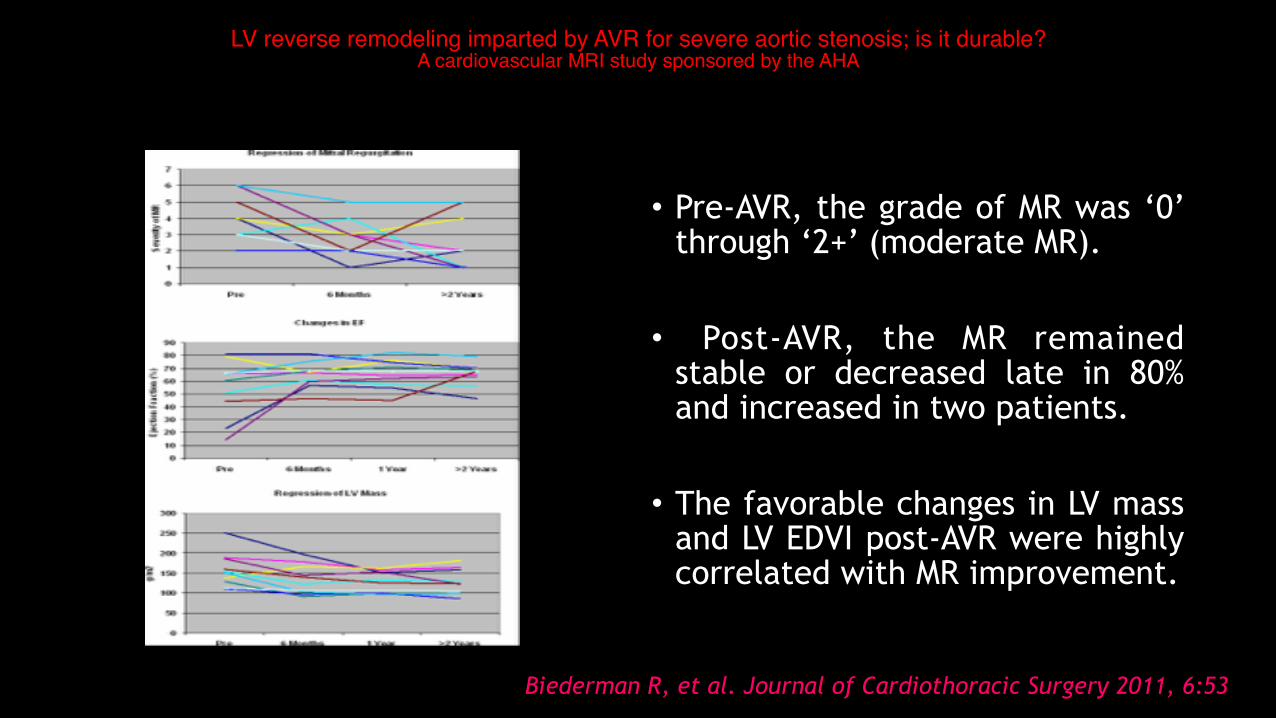
LV reverse remodeling imparted by AVR for severe aortic stenosis; is it durable? A cardiovascular MRI study sponsored by the AHA
• Pre-AVR, the grade of MR was ‘0’ through ‘2+’ (moderate MR).
• Post-AVR, the MR remained stable or decreased late in 80% and increased in two patients.
• The favorable changes in LV mass
and LV EDVI post-AVR were highly correlated with MR improvement.
Biederman R, et al. Journal of Cardiothoracic Surgery 2011, 6:53

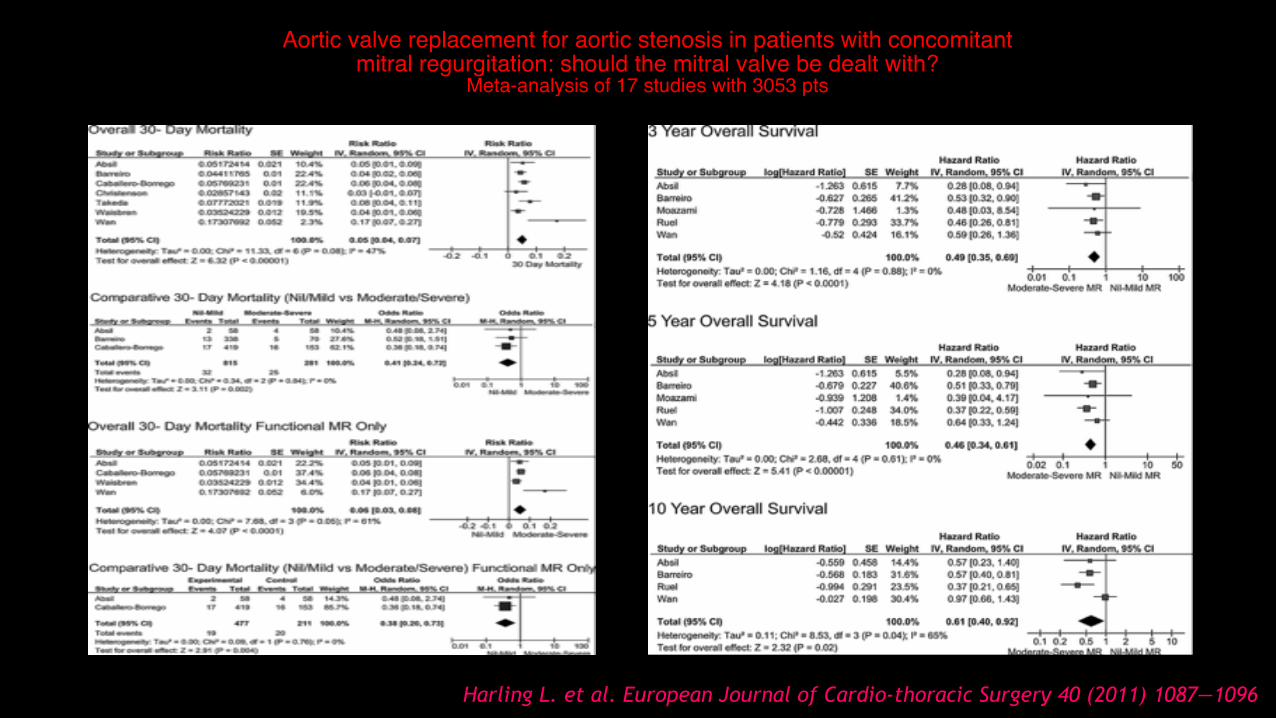
Aortic valve replacement for aortic stenosis in patients with concomitantmitral regurgitation: should the mitral valve be dealt with?
Meta-analysis of 17 studies with 3053 pts
• Reduction in the trans-mitral pressure gradient
• Reverse ventr icular remodel ing as demonstrated by a reduction in LV mass and LVED diameter.
Reverse remodeling may play a further role in patients with evidence of LV dilatation, where mitral valve leaflet tethering occurs secondary to outward displacement of the papillary muscles
Independent predictors of improvement in MR following AVR • Higher preoperative LV mass • Larger LVEDD • Larger LVEDV
Harling L. et al. European Journal of Cardio-thoracic Surgery 40 (2011) 1087—1096
Etiology of preoperative MR did not have a significant effect on the improvement of MR postoperatively
Aortic valve replacement for aortic stenosis in patients with concomitantmitral regurgitation: should the mitral valve be dealt with?
Meta-analysis of 17 studies with 3053 pts
Harling L. et al. European Journal of Cardio-thoracic Surgery 40 (2011) 1087—1096
INDIDENCE AND ETIOLOGY OF MR IN PATIENTS WHO UNDERWENT TAVR

Prevalence of moderate/severe mitral regurgitation in patients undergoing TAVI
European Heart Journal (2014) 35, 2627–2638

Etiology of Mitral Regurgitation in Patients Undergoing TAVR
J Am Coll Cardiol 2014;63:2643–58
MR is usually more frequent than functional MR in the general population, functional MR accounts for approximately 50% of patients with MR in patients who have undergone TAVR. No study to date has reported the incidence of mixed MR etiologies,.
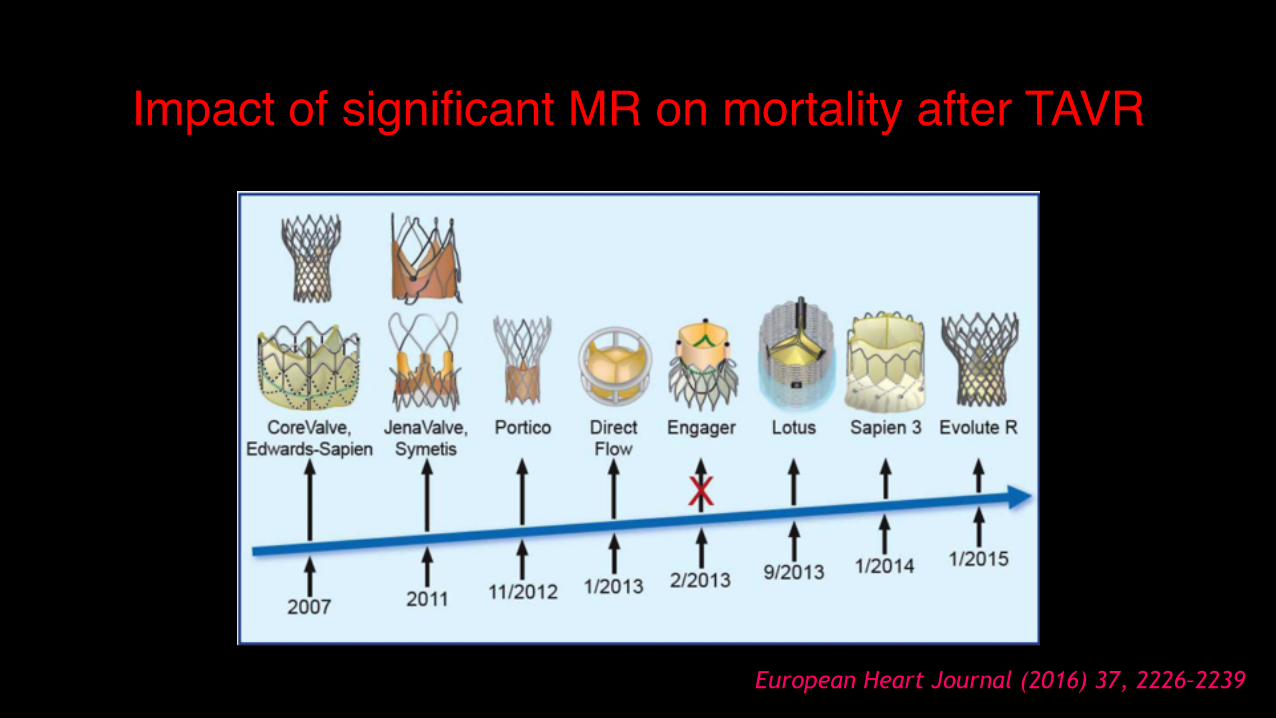
Impact of significant MR on mortality after TAVR
European Heart Journal (2016) 37, 2226–2239

Predictors of One-Year Mortality After TAVI for Severe Symptomatic Aortic Stenosis
Zahn R et al. Am J Cardiol 2013;112:272-279
Previous MR≥ 2 is an independent predictor of 1-year mortality
N=1391
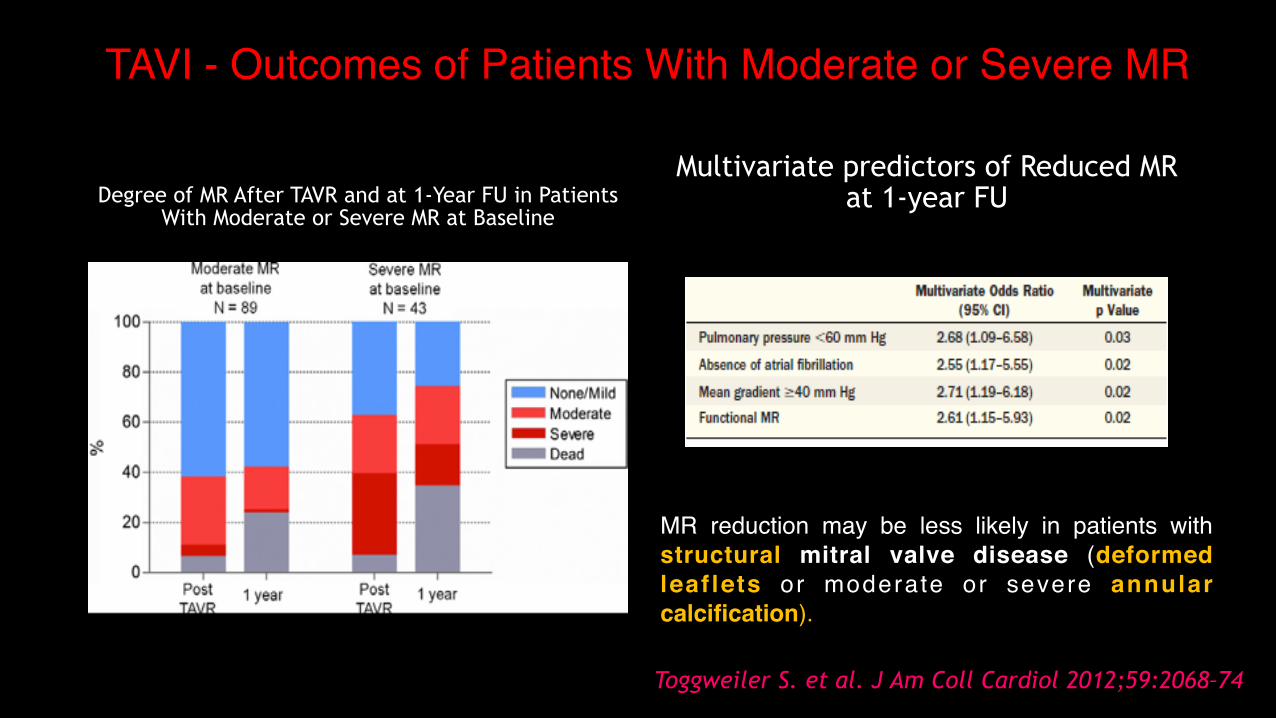
TAVI - Outcomes of Patients With Moderate or Severe MR
Degree of MR After TAVR and at 1-Year FU in Patients With Moderate or Severe MR at Baseline
Multivariate predictors of Reduced MR at 1-year FU
Toggweiler S. et al. J Am Coll Cardiol 2012;59:2068–74
MR reduction may be less likely in patients with structural mitral valve disease (deformed leaf lets or moderate or severe annular calcification).

Coexisting Mitral Regurgitation Impairs Survival After TAVIMeta-analysis n=13672pts
Early all-cause mortality Overall all-cause mortality
Ann Thorac Surg 2015;100:2270–7
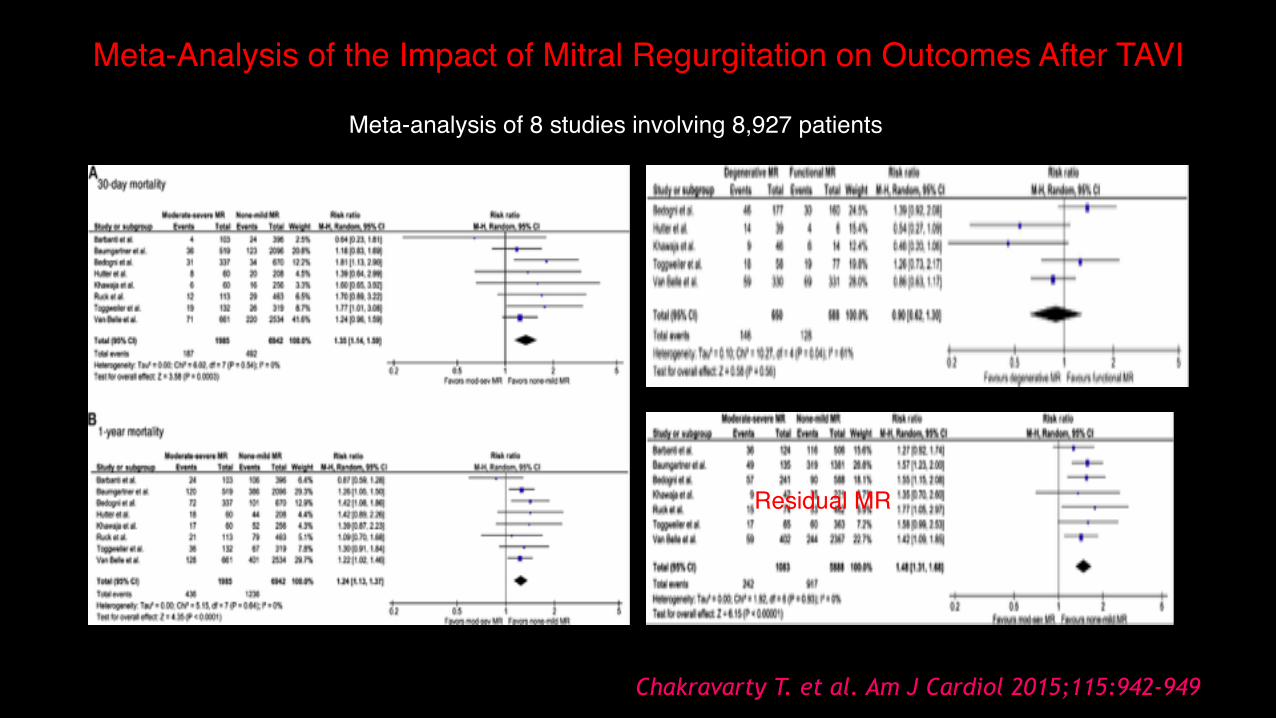
Meta-Analysis of the Impact of Mitral Regurgitation on Outcomes After TAVI
Meta-analysis of 8 studies involving 8,927 patients
Chakravarty T. et al. Am J Cardiol 2015;115:942-949
Residual MR

Clinical impact and evolution of MR after TAVR a meta-analysis
8 studies including 8015 pts SEV: 3474 pts BEV: 4492 pts
Nombela-Franco L, et al. Heart 2015;0:1–11

Changes in Mitral Regurgitation After TAVI
J Am Coll Cardiol 2014;63:2643–58

Changes in Mitral Regurgitation After TAVI
MR in Patients Referred for TAVI Using the Edwards Sapien
Prosthesis Mechanisms and Early Postprocedural Changes
Catheter Cardiovasc Interv 75:43–49 (2010)
J Am Soc Echocardiogr 2012;25:160-5
N=254

5-year outcomes of TAVI or surgical AVR for high surgical risk patients with aortic stenosis - PARTNER 1
Lancet 2015; 385: 2477–84

Evaluation of Flow After TAVR in Patients With Low-Flow Aortic Stenosis
JAMA Cardiol. 2016;1(5):584-592

Mitral and aortic regurgitation following TAVR
Heart 2016;102:701–706

Predictive Factors Associated With Improvement in MR Severity After Aortic Valve Replacement (SAVR and TAVR)
MR etiology (functional vs. organic) SAVR TAVR
Absence of pulmonary hypertension SAVR TAVR
Absence of AF SAVR TAVR
LVEF (low vs. normal) and LV diameters SAVR TAVR
Mean gradient SAVR TAVR
Residual Aortic regurgitation SAVR TAVR
Increased LA size SAVR
Coronary artery disease or previous MI SAVR
Prosthesis patient mismatch SAVR
Absence of mitral annular calcification with restriction
TAVR
Valve type (ES vs. CoreValve) TAVR Greater improvement with ES
Deeper implantation Core valve TAVR
J Am Coll Cardiol 2014;63:2643–58

Mitral Regurgitation After TAVR
J Am Coll Cardiol Intv 2016;9:1603–14
N=1110, MR≥3 16%
The presence of calcific burden in moderate to severe degrees within the mitral annulus and leaflets associates with greater stiffness of mitral structures, suggesting an organic nature of mitral valve disease, thus hindering MR improvement after TAVR.
If this high degree of calcification appears together with a larger annulus diameter, it may preclude from regression of the dilation despite correction of the ventricular pressure overload.
Only 13.1% of patients with persistent MR met criteria for percutaneous mitral repair

Percutaneous treatment of MR after TAVR
European Heart Journal (2016) 37, 2226–2239
MitraClip

Coronary sinus annuloplasty. The cardiac dimensions CARILLON device
Mitralign annular plication
Valtech CardioBand
European Heart Journal (2016) 37, 2226–2239

Improvement of functional capacity after staged percutaneous treatment in 12 patients with aorto-mitral bivalvular heart disease.
• 254 patients underwent TAVI.
• 17 patients (6.7%) had preoperative severe MVR that remained unchanged after TAVI. Due to exacerbation of symptoms 12 patients were subsequently submitted to MV repair with the MitraClipVR device.
Catheterization and Cardiovascular Interventions 82:E552–E563 (2013)
Staging of the two interventions allows the possibility of a spontaneous regression of the MVR after sole treatment of AVS and may prevent unnecessary potentially dangerous treatments. The percutaneous approach is more amenable for a staged strategy. TAVI does not seem to impact on the technical feasibility and complexity of a subsequent MitraClipVR therapy.

Surgical and interventional management of mitral valve regurgitation: a position statement from the ESC Working Groups on Cardiovascular Surgery
and Valvular Heart Disease
Eur Heart J. 2015 Jul 7

MANAGEMENT OF CONCOMITANT MODERATE TO SEVERE MR IN
PATIENTS WITH SEVERE AS

Decisional Algorithm for Management of Patients With Severe Aortic Stenosis and Concomitant Mitral Regurgitation
J Am Coll Cardiol 2014;63:2643–58

TAKE HOME MESSAGES I
• Significant mitral regurgitation (MR) is a common entity (∼15-20%) in patients with severe aortic stenosis undergoing SAVR or TAVI
• Preoperative quantification of MR should be performed with the effective regurgitant orifice (EROA). Vena contracta might be used to corroborate the quantitative results.
• Significant MR seems to have a negative impact on early and late survival in patients undergoing SAVR or TAVI.

TAKE HOME MESSAGES II
• Moderate–severe MR improved in about 50% of the patients following SAVR or TAVI especially in those with LV dysfunction and functional MR
• The decision-making process should be based in the assessment of operative risk, MR severity, etiology and likelihood of MR improvement after isolated AVR.

THANK YOU