Mitral Valve Prolapse, Flailed Mitral Valve Mitral Annular Calcification
J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 9 , N O . 8 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 6 . 0 3 . 0 1 1
IMAGING VIGNETTE
Cardiac Amyloidosis Presenting asSevere Mitral Regurgitation
Khawaja Afzal Ammar, MBBS, MS,a Bijoy K. Khandheria, MD,a Tanvir Bajwa, MD,a Steven C. Port, MD,aSuhail Allaqaband, MD,a Renuka Jain, MD,a Gary Neitzel, MD,b A. Jamil Tajik, MDa
ALTHOUGH MILD TO MODERATE MITRAL REGURGITATION IS COMMON IN CARDIAC AMYLOIDOSIS (CA),
severe mitral regurgitation as the primary presenting finding is rare (1). We present 3 such cases of patientswith severe mitral regurgitation who on further workup were discovered to have CA (2) (Figures 1 to 6). Wefound atypical nodularity along the coaptation margin of the anterior mitral leaflets as a mechanism behindsevere mitral regurgitation, likely from local amyloid infiltration, creating an “amyloidoma.” Because multi-modality imaging provided further evidence in favor of CA, the initial Congo red staining results, negative forCA, were ignored. Advanced histological techniques confirmed the diagnosis of CA. All cases markedlyimproved with unconventional therapeutic approaches (percutaneous mitral valve repair n ¼ 2, and cardiac
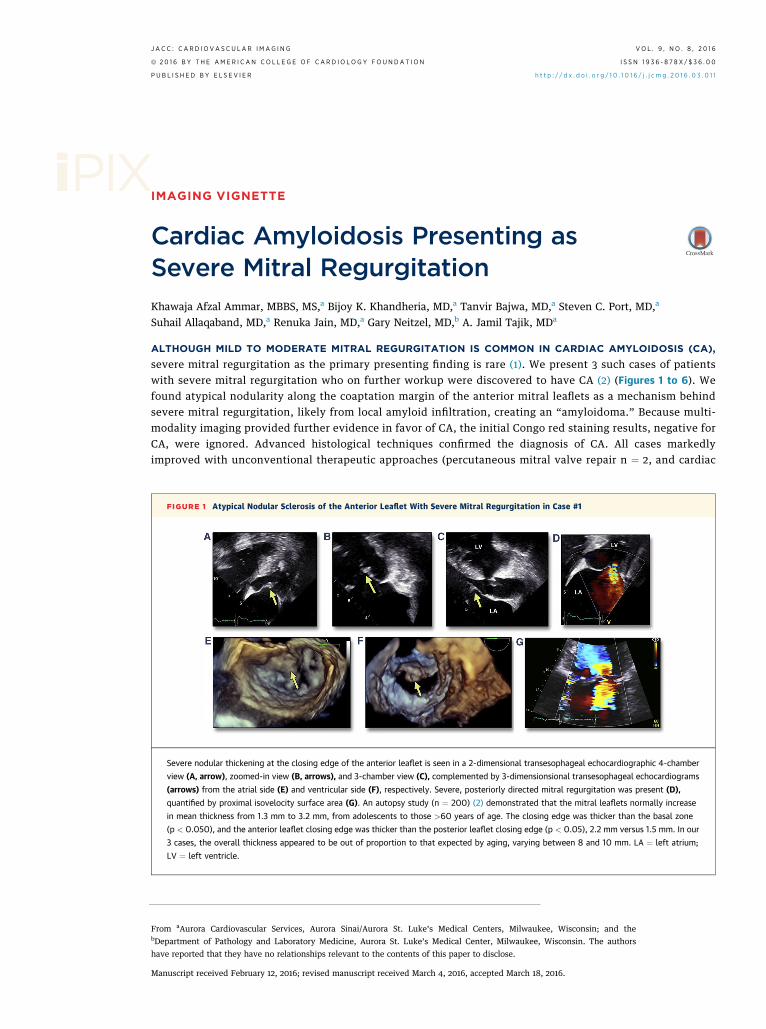
FIGURE 1 Atypical Nodular Sclerosis of the Anterior Leaflet With Severe Mitral Regurgitation in Case #1
Severe nodular thickening at the closing edge of the anterior leaflet is seen in a 2-dimensional transesophageal echocardiographic 4-chamber
view (A, arrow), zoomed-in view (B, arrows), and 3-chamber view (C), complemented by 3-dimensionsional transesophageal echocardiograms
(arrows) from the atrial side (E) and ventricular side (F), respectively. Severe, posteriorly directed mitral regurgitation was present (D),
quantified by proximal isovelocity surface area (G). An autopsy study (n ¼ 200) (2) demonstrated that the mitral leaflets normally increase
in mean thickness from 1.3 mm to 3.2 mm, from adolescents to those >60 years of age. The closing edge was thicker than the basal zone
(p < 0.050), and the anterior leaflet closing edge was thicker than the posterior leaflet closing edge (p < 0.05), 2.2 mm versus 1.5 mm. In our
3 cases, the overall thickness appeared to be out of proportion to that expected by aging, varying between 8 and 10 mm. LA ¼ left atrium;
LV ¼ left ventricle.
From aAurora Cardiovascular Services, Aurora Sinai/Aurora St. Luke’s Medical Centers, Milwaukee, Wisconsin; and thebDepartment of Pathology and Laboratory Medicine, Aurora St. Luke’s Medical Center, Milwaukee, Wisconsin. The authors
have reported that they have no relationships relevant to the contents of this paper to disclose.
Manuscript received February 12, 2016; revised manuscript received March 4, 2016, accepted March 18, 2016.
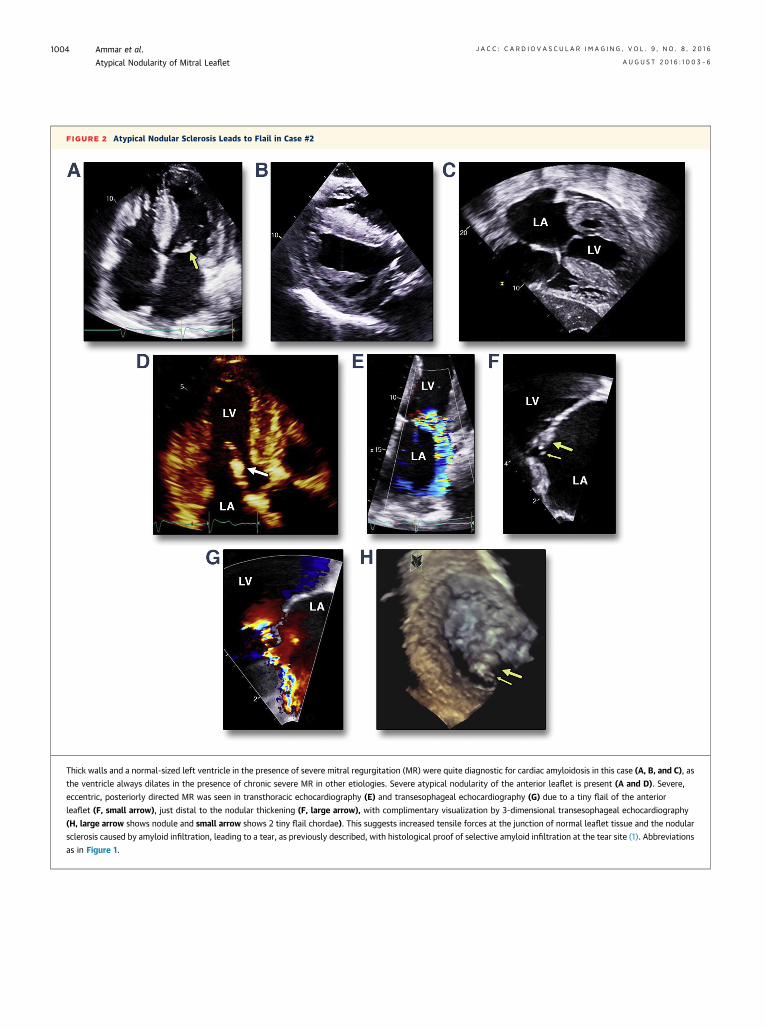
FIGURE 2 Atypical Nodular Sclerosis Leads to Flail in Case #2
Thick walls and a normal-sized left ventricle in the presence of severe mitral regurgitation (MR) were quite diagnostic for cardiac amyloidosis in this case (A, B, and C), as
the ventricle always dilates in the presence of chronic severe MR in other etiologies. Severe atypical nodularity of the anterior leaflet is present (A and D). Severe,
eccentric, posteriorly directed MR was seen in transthoracic echocardiography (E) and transesophageal echocardiography (G) due to a tiny flail of the anterior
leaflet (F, small arrow), just distal to the nodular thickening (F, large arrow), with complimentary visualization by 3-dimensional transesophageal echocardiography
(H, large arrow shows nodule and small arrow shows 2 tiny flail chordae). This suggests increased tensile forces at the junction of normal leaflet tissue and the nodular
sclerosis caused by amyloid infiltration, leading to a tear, as previously described, with histological proof of selective amyloid infiltration at the tear site (1). Abbreviations
as in Figure 1.
Ammar et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 9 , N O . 8 , 2 0 1 6
Atypical Nodularity of Mitral Leaflet A U G U S T 2 0 1 6 : 1 0 0 3 – 6
1004
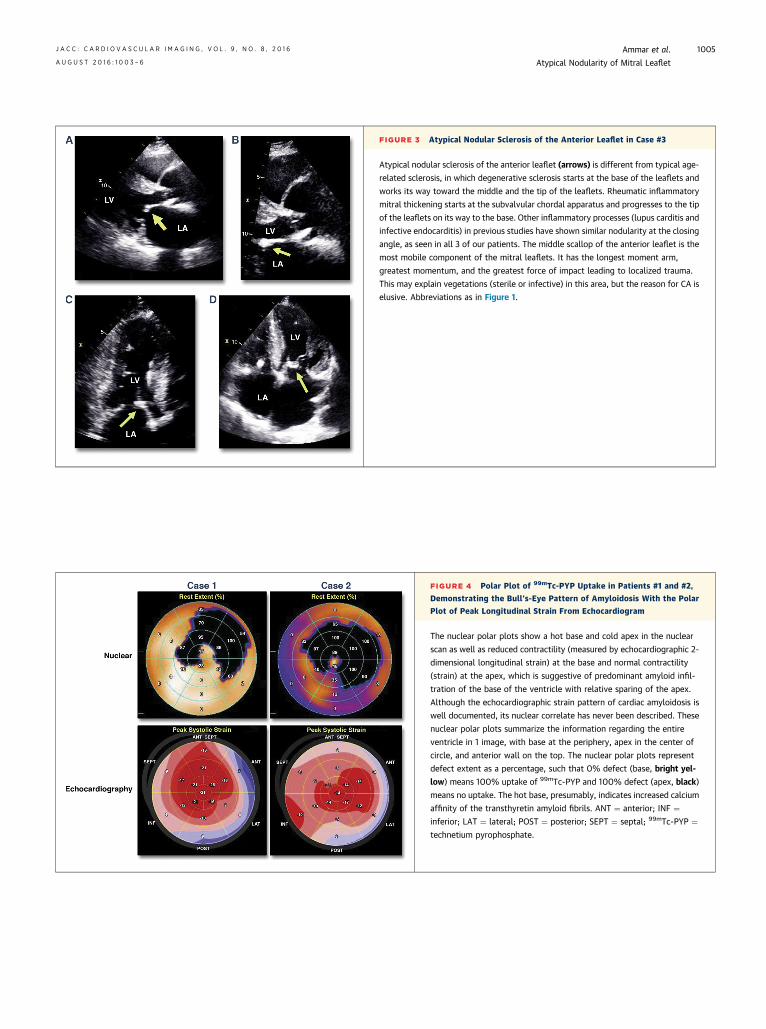
FIGURE 3 Atypical Nodular Sclerosis of the Anterior Leaflet in Case #3
Atypical nodular sclerosis of the anterior leaflet (arrows) is different from typical age-
related sclerosis, in which degenerative sclerosis starts at the base of the leaflets and
works its way toward the middle and the tip of the leaflets. Rheumatic inflammatory
mitral thickening starts at the subvalvular chordal apparatus and progresses to the tip
of the leaflets on its way to the base. Other inflammatory processes (lupus carditis and
infective endocarditis) in previous studies have shown similar nodularity at the closing
angle, as seen in all 3 of our patients. The middle scallop of the anterior leaflet is the
most mobile component of the mitral leaflets. It has the longest moment arm,
greatest momentum, and the greatest force of impact leading to localized trauma.
This may explain vegetations (sterile or infective) in this area, but the reason for CA is
elusive. Abbreviations as in Figure 1.
FIGURE 4 Polar Plot of 99mTc-PYP Uptake in Patients #1 and #2,
Demonstrating the Bull’s-Eye Pattern of Amyloidosis With the Polar
Plot of Peak Longitudinal Strain From Echocardiogram
The nuclear polar plots show a hot base and cold apex in the nuclear
scan as well as reduced contractility (measured by echocardiographic 2-
dimensional longitudinal strain) at the base and normal contractility
(strain) at the apex, which is suggestive of predominant amyloid infil-
tration of the base of the ventricle with relative sparing of the apex.
Although the echocardiographic strain pattern of cardiac amyloidosis is
well documented, its nuclear correlate has never been described. These
nuclear polar plots summarize the information regarding the entire
ventricle in 1 image, with base at the periphery, apex in the center of
circle, and anterior wall on the top. The nuclear polar plots represent
defect extent as a percentage, such that 0% defect (base, bright yel-
low) means 100% uptake of 99mTc-PYP and 100% defect (apex, black)
means no uptake. The hot base, presumably, indicates increased calcium
affinity of the transthyretin amyloid fibrils. ANT ¼ anterior; INF ¼inferior; LAT ¼ lateral; POST ¼ posterior; SEPT ¼ septal; 99mTc-PYP ¼technetium pyrophosphate.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 9 , N O . 8 , 2 0 1 6 Ammar et al.A U G U S T 2 0 1 6 : 1 0 0 3 – 6 Atypical Nodularity of Mitral Leaflet
1005
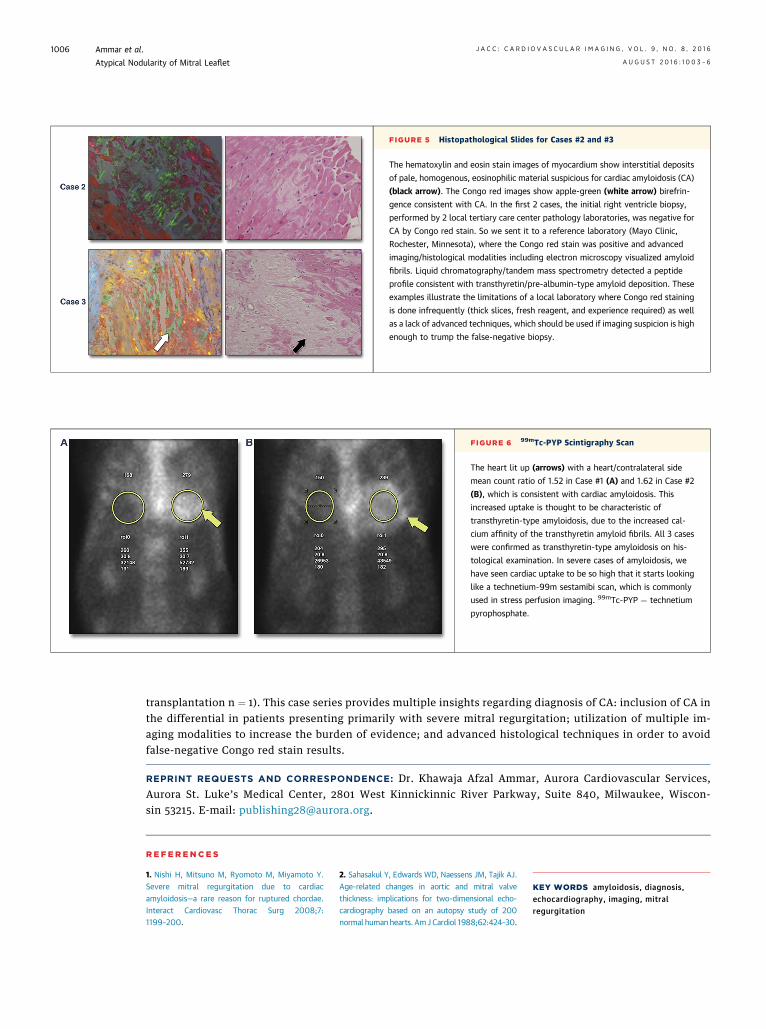
FIGURE 5 Histopathological Slides for Cases #2 and #3
The hematoxylin and eosin stain images of myocardium show interstitial deposits
of pale, homogenous, eosinophilic material suspicious for cardiac amyloidosis (CA)
(black arrow). The Congo red images show apple-green (white arrow) birefrin-
gence consistent with CA. In the first 2 cases, the initial right ventricle biopsy,
performed by 2 local tertiary care center pathology laboratories, was negative for
CA by Congo red stain. So we sent it to a reference laboratory (Mayo Clinic,
Rochester, Minnesota), where the Congo red stain was positive and advanced
imaging/histological modalities including electron microscopy visualized amyloid
fibrils. Liquid chromatography/tandem mass spectrometry detected a peptide
profile consistent with transthyretin/pre-albumin–type amyloid deposition. These
examples illustrate the limitations of a local laboratory where Congo red staining
is done infrequently (thick slices, fresh reagent, and experience required) as well
as a lack of advanced techniques, which should be used if imaging suspicion is high
enough to trump the false-negative biopsy.
FIGURE 6 99mTc-PYP Scintigraphy Scan
The heart lit up (arrows) with a heart/contralateral side
mean count ratio of 1.52 in Case #1 (A) and 1.62 in Case #2
(B), which is consistent with cardiac amyloidosis. This
increased uptake is thought to be characteristic of
transthyretin-type amyloidosis, due to the increased cal-
cium affinity of the transthyretin amyloid fibrils. All 3 cases
were confirmed as transthyretin-type amyloidosis on his-
tological examination. In severe cases of amyloidosis, we
have seen cardiac uptake to be so high that it starts looking
like a technetium-99m sestamibi scan, which is commonly
used in stress perfusion imaging. 99mTc-PYP ¼ technetium
pyrophosphate.
Ammar et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 9 , N O . 8 , 2 0 1 6
Atypical Nodularity of Mitral Leaflet A U G U S T 2 0 1 6 : 1 0 0 3 – 6
1006
transplantation n ¼ 1). This case series provides multiple insights regarding diagnosis of CA: inclusion of CA inthe differential in patients presenting primarily with severe mitral regurgitation; utilization of multiple im-aging modalities to increase the burden of evidence; and advanced histological techniques in order to avoidfalse-negative Congo red stain results.
REPRINT REQUESTS AND CORRESPONDENCE: Dr. Khawaja Afzal Ammar, Aurora Cardiovascular Services,Aurora St. Luke’s Medical Center, 2801 West Kinnickinnic River Parkway, Suite 840, Milwaukee, Wiscon-sin 53215. E-mail: [email protected].
RE F E RENCE S
1. Nishi H, Mitsuno M, Ryomoto M, Miyamoto Y.Severe mitral regurgitation due to cardiacamyloidosis—a rare reason for ruptured chordae.Interact Cardiovasc Thorac Surg 2008;7:1199–200.
2. Sahasakul Y, Edwards WD, Naessens JM, Tajik AJ.Age-related changes in aortic and mitral valvethickness: implications for two-dimensional echo-cardiography based on an autopsy study of 200normal human hearts. AmJ Cardiol 1988;62:424–30.
KEY WORDS amyloidosis, diagnosis,echocardiography, imaging, mitralregurgitation