Message from theAaron Hartstein Kevin Gross Mark Gaddis Kristin Kelley John Tunnell Ryan B. Cyr...
28
May/June 2008 The Official Publication of the American Academy of Orthopaedic Manual Physical Therapists INSIDE THIS ISSUE... Message from the AAOMPT President Tim Flynn, PT, PhD Let the Secret Out! Vol. 14, No. 2 2 Credentialed Fellowship Programs . 4 Committee Reports ..... 5 Reports from the Executive Board.. 8 Paris Award Acceptance Speech................... 10 Clinical Pearl .............. 17 Research Pearl ........... 18 Practice Affairs Corner .....20 Kaltenborn I Must Teach Award Form ........... 24 John McMennell Service Award Form ........... 25 AAOMPT Membership Benefits .................. 26 AAOMPT Membership Application .............. 28 007 was an exciting year for the Academy. We are pushing 2000 members...a long ways from our early “out of a garage” operations in Biloxi, MS (Mike Rogers, you remember those days well!). Fueled by a rich heritage of passionate Founding Fellows with a big vision, the AAOMPT has blossomed into a major player on the professional advo- cacy scene. The Academy is involved in many national and international activities which often go unnoticed. For example, I would call your attention to the language consensus document that was recently published in JOSPT and JMMT. Ad- ditionally, in December of 2007, the AAOMPT published the Manual Therapy Description of Advanced Specialist Prac- tice (DASP), which is one of the core/ foundational documents for development of a Manual Therapy Fellowship as well as for attaining credentialing recognition by the APTA. In addition, the Academy has been working on many levels with the APTA and IFOMT to rapidly facilitate research, practice, and marketing of our unique skill set. These are just a couple of the many examples of what the AAOMPT has been doing to advance the interests of our members. Inevitable to growth and the pas- sage of time is an increase in operational costs. The AAOMPT is no exception. Combined with AAOMPT’s increasing advocacy and support on many fronts to advance the interests of OMPT, the abil- ity for AAOMPT to best serve its members will be hampered without an adjustment in membership dues. AAOMPT dues have maintained a steady $95 for members and $125 for fellow members for the past 5 years. Just to give our members advance notice, we will be planning to propose an increase in dues by $30 to $125 for members and $155 for fellow members beginning in 2009. We think this is a very reasonable increase in light of the many benefits that being a member of AAOMPT affords you. It is also important to remember that $45 of these dues goes to the JMMT and is not part of our ongoing operational expenditures, thus currently the cost of membership is only $50 for members and $80 for fellow members. The increase in cost of membership that goes directly to the AAOMPT’s operational expenditures will be $80 for members and $110 for fellow members. Annual Conference has always been one of the year’s highlights for our members, however we’re about to take it up a notch. One of the biggest initiatives in 2008 is a new “look and feel” to our 2008 Annual Confer- ence in Seattle, Washington on October 30 through November 2, 2008. The Academy has partnered with Let’s Meet (www.letsmeet. net) to help take our conference and exhibit to the next level of growth. This year’s confer- ence will be one of the most action-packed
Transcript of Message from theAaron Hartstein Kevin Gross Mark Gaddis Kristin Kelley John Tunnell Ryan B. Cyr...

May/June 2008
The Official Publication of the American Academy of Orthopaedic Manual Physical Therapists
InsIde ThIs Issue...
Message from the AAOMPT PresidentTim Flynn, PT, PhD
Let the Secret Out!
Vol. 14, No. 2
2
Credentialed
Fellowship Programs . 4
Committee Reports ..... 5
Reports from
the Executive Board.. 8
Paris Award Acceptance
Speech ................... 10
Clinical Pearl .............. 17
Research Pearl ........... 18
Practice Affairs Corner .....20
Kaltenborn I Must Teach
Award Form ........... 24
John McMennell Service
Award Form ........... 25
AAOMPT Membership
Benefits .................. 26
AAOMPT Membership
Application .............. 28
007 was an exciting year for the Academy. We are pushing 2000 members...a long ways from our
early “out of a garage” operations in Biloxi, MS (Mike Rogers, you remember those days well!). Fueled by a rich heritage of passionate Founding Fellows with a big vision, the AAOMPT has blossomed into a major player on the professional advo-cacy scene. The Academy is involved in many national and international activities which often go unnoticed. For example, I would call your attention to the language consensus document that was recently published in JOSPT and JMMT. Ad-ditionally, in December of 2007, the AAOMPT published the Manual Therapy Description of Advanced Specialist Prac-tice (DASP), which is one of the core/foundational documents for development of a Manual Therapy Fellowship as well as for attaining credentialing recognition by the APTA. In addition, the Academy has been working on many levels with the APTA and IFOMT to rapidly facilitate research, practice, and marketing of our unique skill set. These are just a couple of the many examples of what the AAOMPT has been doing to advance the interests of our members.
Inevitable to growth and the pas-sage of time is an increase in operational costs. The AAOMPT is no exception. Combined with AAOMPT’s increasing
advocacy and support on many fronts to advance the interests of OMPT, the abil-ity for AAOMPT to best serve its members will be hampered without an adjustment in membership dues. AAOMPT dues have maintained a steady $95 for members and $125 for fellow members for the past 5 years. Just to give our members advance notice, we will be planning to propose an increase in dues by $30 to $125 for members and $155 for fellow members beginning in 2009. We think this is a very reasonable increase in light of the many benefits that being a member of AAOMPT affords you. It is also important to remember that $45 of these dues goes to the JMMT and is not part of our ongoing operational expenditures, thus currently the cost of membership is only $50 for members and $80 for fellow members. The increase in cost of membership that goes directly to the AAOMPT’s operational expenditures will be $80 for members and $110 for fellow members.
Annual Conference has always been one of the year’s highlights for our members, however we’re about to take it up a notch. One of the biggest initiatives in 2008 is a new “look and feel” to our 2008 Annual Confer-ence in Seattle, Washington on October 30 through November 2, 2008. The Academy has partnered with Let’s Meet (www.letsmeet.net) to help take our conference and exhibit to the next level of growth. This year’s confer-ence will be one of the most action-packed


May/June 2008 - Articulations - 3
N E W F E L L O W S
AAOMPT OFFICERSPresident Timothy W. Flynn, PT, PhD Phone (303) 964-5137 E-mail: [email protected] Vice President Bob Rowe, PT, DMTPhone (904) 858-7317 Fax (904)858-7284E-mail: [email protected] Secretary Jake Magel, PT, DSc Phone (505) 368-7119 Fax (505) 368-7078 E-mail: [email protected] Treasurer John Childs, PT, PhD E-mail: [email protected] Member-at-Large Haideh Plock, PT, ATC E-mail: [email protected]
Immediate Past President Ken Olson, PT, DHSc E-mail: [email protected]
COMMITTEE CHAIRPERSONSStandards (Co-chairs):Catherine Patla, PT, DHScPhone (904) 826-0084 Fax (904) 826-0085E-mail: [email protected] Porter Hoke, PTPhone (503) 775-6449E-mail: [email protected]
Education (Co-chairs):Marcie Swift, PT, PhDPhone (913) 588-6759 Fax (913) 588-4568E-mail: [email protected] & Lisa Furto, PTPhone: (815) 748-5282 E-mail: [email protected]
Examination:Michael Puniello, PT, DPTPhone (781) 749-5833 Fax (781) 740-9141E-mail: [email protected]
Research: H. James Phillips, PT, PhDE-mail: [email protected]
Membership: Cheri Hodges, PT, DPTPhone (480) 502-8128 E-mail: [email protected]
Articulations Editor:David Miers, PTPhone (610) 258-5321E-mail: [email protected]
Nominations/Awards: Liz SlusarzE-mail: [email protected]
Practice Affairs:Bill Boissonnault, PT, DHScE-mail: [email protected]
International Affairs:Chris Showalter, MPTPhone (631) 298-5367 Fax (631) 298-3810E-mail: [email protected]
Public Relations:Britt Smith, PT Phone (970) 263-4079E-mail: [email protected]
in history in light of the practice act issues in Washington State and the opportunity to come alongside the Washington State Chapter to advocate for change. The meeting will include David Butler and Dr. Steven George, internationally recognized clinician-researchers in manual physical therapy, along with Dr. Richard Deyo who will be highlighting the alarming rates of spine surgery in this country. Addi-tionally, a host of grass roots advocacy initiatives will be occurring that will energize the Washington state PT to “take back the streets” when it comes to spinal manipulation. We have a goal to attract 750 attendees in 2008. Help make it happen by planning to attend now. If you’ve never attended a previous AAOMPT Conference, talk to someone who has. You will find out hands down why it’s the best physical therapist meeting in the country year after year. If you’re a regular, bring someone with you! Don’t miss out on the opportunity to showcase the Academy to someone new. And mark your calendars now because we will be advocating directly with the new U.S. Congress and Administration as
AAOMPT goes to Washington, DC from October 14-18, 2009!
Although our membership has always been an active one, it is time for our breakout year and we are asking each of you to aggressively promote the Academy amongst all you know who have an interest in OMPT. In keeping with this goal, the AAOMPT will be running a “Let the Secret Out!” cam-paign in which we’d like to ask every current member to recruit at least 1 new member during 2008. Recruit 2 or more new members, and you will make up for any slackers in our midst! In all seriousness, there is no reason why we shouldn’t have 5K members by the end of 2008! This represents exponential growth which will be immediately felt by our ability to advocate and promote the interests of our members.
Your Executive Committee is excited to serve you, and we can’t say thanks enough for the hundreds of hours that our members put in on behalf of the best professional orga-nization in PT. AAOMPT’s ability to advance the interests of its membership is only limited to the size of our vision. Your Executive has a big one!
President’s Message (continued from page 1)
Katarzyna SachaLaura Von Wullerstorff
Brian J. FinleyAaron Hartstein
Kevin GrossMark GaddisKristin KelleyJohn TunnellRyan B. CyrSandra A. Do
Jeffrey S. AlbertsonJennifer Brien
Dexter WittJames Bjornson
Marisa Rasile, MPTFrank Ko
Steven M. VanKlompenburgValerie Lovejoy
Edward BoudreauAngela Dominica Listug, DPT
Christine L. Kott-Soper, PTBettina Howell, MPT,CFMT
Jennifer KunzaL.N. Shankarkrishnan, PT
4 - Articulations - May/June 2008
T
Daemen College Orthopedic Manual Physical Therapy Fellowship4380 Main Street, Amherst, NY 14226Contact: Ron Schenk, PT, PhD, OCS, FAAOMPT, Cert. MDTPhone: 716/839-8360Fax: 716/839-8345E-mail: [email protected]
Institute of Orthopaedic Manual Therapy c/o Orthopaedics Plus101 Cambridge, Burlington, MA 01803Contact: Martin Langaas, PT, OMTPhone: 781/932-8866Fax: 781/229-8374E-mail: [email protected]
The Institute of Physical Art Certified Functional Manual Therapist Fellowship 43449 Elk Run, Steamboat Springs, CO 80487Contact: Gregory Johnson, PT, FFCFMTPhone: 970/870-9521Fax: 970/870-9531E-mail: [email protected]
Institute of Rehabilitation and Training Orthopedic Manual Therapy FellowshipSelect Medical Corp.211 Sweet Briar Lane, Prattville, AL 36067Contact: C. Andy Gustafson,Phone: 334/221-1870Fax: 334/365-7724E-mail: [email protected]
International Academy of Orthopedic Medicine (IAOM) - US Fellowship in Orthopedic Manual TherapyPO Box 86177, Tucson, AZ 85754(Sites in Alaska and Texas)Contact: Phil Sizer, Jr., PT, PhD, OCS, FAAOMPTPhone: 520/318-4266Fax: 520/318-0849E-mail: [email protected]
Kaiser Hayward Physical Therapy Fellowship in Advanced Orthopedic Manual Therapy 27400 Hesperian Blvd, Hayward, CA 94545Contact: Carol Jo Tichenor, PT, MAPhone: 510/675-4259Fax: 510/675-3241E-mail: [email protected]
Kaiser Permanente Los Angeles Orthopaedic Manual Therapy FellowshipKaiser Permanente Medical Center - Physical Medicine and Rehabilitation6041 Cadillac Ave, West Los Angeles, CA 90034Contact: Joseph Godges, PT, DPT, MA, OCSPhone: 323/857-2422Fax: 310/215-0780E-mail: [email protected]
Recognized Clinical Fellowships in OMPT by AAOMPT
List continued on page 6
he 2008 AAOMPT conference will be arriving before we know it. The con-ference is filled with topics related to the conference theme Pain: From Science to Solution along with legislative issues in Washington and professional issues abroad. The conference will take place in the beautiful Bell Harbor convention center where there will be waterfront views that will allow you to take in the atmosphere in the spectacular city of Seattle. The conference dates are 10/29 through 11/2. Keynote speakers David Butler, PT and Steven George, PT will be addressing different dimensions of the science behind pain management. In addition, keynote speaker, Richard Deyo, MD, will be discussing the evidence behind management of spine conditions and the alarming increase of invasive procedures of in the United States. A 30 minute panel has been added at the end of Friday so the keynote speakers can give their different perspectives on ques-tions related to pain management.
The 2008 conference brings a large selection of pre-conferences to be selected from this year. Among these pre-conferences, Ken Olson, William Bois-sonnault, and Steve McDavitt will present a half-day pre-conference on legisla-tion issues in the west, particularly the state of Washington. The cost of this half day pre-conference will be donated to the Washington PT-PAC.
Among the many great educational experiences you will have at the confer-ence, we are planning on equally exciting social events. Come prepared for the Saturday night Halloween reception as there will be a costume competition. The Student Special Interest Group will be organizing lots of fun events including a dance competition that was a hit last year. The city of Seattle will have plenty of Halloween festivities happening, so bring your families. Let’s Meet will be send-ing out a list of these events.
The conference hotel is at the Seattle Marriott Waterfront hotel and will host some of our events. The hotel is across the street from the Bell Harbor Convention Center. The Executive and Conference Committee hope you will support the conference and future conferences by booking at this year’s confer-ence center. The numbers we produce at each hotel every year help our resume for the following years in being accepted at conference facilities. The great sup-port we got in 2007 has helped us with our current planning and as we continue to grow as an organization we continue to need your support in selecting to stay at our conference hotels. You will be absolutely pleased with your stay at the Marriot as it sits along the waterfront and hosts beautiful views. The special rate for the conference is $189. Call soon to book at the registration number: 1-800-455-8254.
Registration for the conference is in a new format that will make registra-tion easier for you and help us developing future conferences. You will learn more about the conference speakers and events from the registration link on the Academy website at www.aaompt.org. The link will take you to Let’s Meet website who is the professional group hired to coordinate the conference and registration. Registration will be running mid April, so get all your friends and colleagues to register! We will see you there!
2008 AAOMPT Conference Lisa Furto PT, DPT, MTC, FAAOMPT

May/June 2008 - Articulations - 5
Committee Reports
Standards CommitteeRespectfully submitted by
Ann P. Hoke & Catherine Patla
The committee has been working on multiple important tasks and planning for future projects that include:
10 year-fellow renewal process •Provide a FAQs answer list to facilitate •fellow renewalReview of fellowship program annual •reportsCoordination with APTA Fellowship •Credentialing Committee AAOMPT Standards Document Revi-•sion: Task Force formationIFOMT International Monitoring: •advance planning for 2011
Fellow Renewal
A list of answers to your frequently asked questions and concerns will soon be available.
The Fellow renewal application is available on the AAOMPT web site, and the application deadline is July 15. Exten-sions are possible if you need a little extra time with one or more of the requirements. Please contact the Standards Committee if you have concerns.
The Committee will be reviewing the 2008 applications for fellowship renewal and the 2007 applications-with-extensions and plans to complete the process in August. We invite all the 2008 re-creden-tialed fellows to attending the opening reception of the AAOMPT conference in Seattle on October 30th, to receive their recognition.
Fellowship Program ReportsThank you to the fellowship directors
for providing us with the extra details in your 2007 reports. This information will be needed for the IFOMT International
Monitoring process (scheduled for 2011). Through the AAOMPT representa-
tive, Patty McCord, the Standards commit-tee remains in close communication with the APTA’s Committee for Clinical Resi-dency and Fellowship Program Credential-ing (CCRFPC). Representatives of both committees met in February 2008 at CSM to further foster that communication, and also with a goal to minimize the report re-quirements and eventually consolidate the APTA and AAOMPT annual fellowship reports into one.
AAOMPT Standards Document (1999)
Planning has begun on assembling a Task force to revise and update the Stan-dards document.
This will be timely, as a revised IFOMT Standards document is also near-ing completion.
Fellows and fellowship programs will be kept updated on the progress of this project.
Fellowship Graduates Graduates from fellowship programs
are encouraged to apply to AAOMPT soon after completion of their fellowship pro-gram. FAAOMPT status with the Academy is for a term of 10 years, starting from the date of graduation from the fellowship program.
New fellows are encouraged to attend the opening reception of the AAOMPT conference in Seattle on October 30th, to receive recognition from their peers.
Standards CommitteeThe committee chairs would like to
acknowledge and thank the committee members for their past and on-going work: Jim Beazell, Carol Courtney, Tamara Little, Patty McCord
Nominating CommitteeSubmitted by: Liz Slusarz, PT, MS, OCS,
FAAOMPT
The Nominating Committee would like to thank Alycia Markowski (outgo-ing chair) for her service and leadership over the past three years. Alycia stream-lined and organized the operations of this committee. As the incoming chair, I am pleased to report that the committee of Myra Pumphry, and Tobi Baldwin, along with our Member at Large, Haideh Plock, are looking forward to another year of recognizing our outstanding fellow col-leagues and recruiting individuals to serve on AAOMPT committees.
We are presently seeking nominations for both the John Mc.Mennell Service Award and the Kaltenborn “Teach I Must” Award. Specific information regarding the eligibility requirements and nomina-tion process is printed within this issue of Articulations as well as available online. Nominations should be submitted via email to Liz Slusarz at [email protected]. We have received several excellent nomina-tions over the past few years making the decisions very difficult. We encourage you to continue to submit your nominations as we have many talented and accomplished colleagues that deserve recognition. The deadline for nominations is August 1, 2008.
There are three positions for election in 2008: President, Vice President and Nominating Committee Member. All positions are for a three year term begin-ning in January, 2009. Candidates for these positions must be Fellows of the Academy. Nomination forms are available in this issue of Articulations, online or can be obtained by email from Liz Slusarz at the above email address. Deadline for nomina-tions is November 1, 2008.
We encourage you all to participate in the award nominations and consider running for office to stay involved in our profession and the Academy. We look forward to our 2008 AAOMPT conference in Seattle, Washington.

6 - Articulations - May/June 2008
Recognized Clinical Fellowships in OMPT by AAOMPT
Nomination for Nominating Committee Member
Term: 3 years, beginning January 2009
Duties: The nominating committee member shall:
a) Participate in maintaining the Academy’s nomination and election process for officers and awards.
b) Will serve as chairperson during the final or 3rd year of their service.
Nominees must be Fellows of the Academy.
Nominee: ______________________________________________
Phone: (w) ____________________________________________
(h) _____________________________________________
Nominated by: __________________________________________
Phone: (w) ____________________________________________
(h) ____________________________________________
Address of nominee:_____________________________________
City: _________________State: ____________Zip: _________
Deadline for submission: November 1, 2008. Please include: (1) personal statement not to exceed 150 words, (2) biographical information not to exceed 150 words, (3) a passport-sized photo, and (4) a signed statement agreeing to serve if elected.
ALL NOMINATIONS SHOULD BE MAILED TO:AAOMPT Nominations
C/o Liz Slusarz49 Margaret Dr.
Walnut Creek, CA 94596
Or email the above information to:[email protected]
North American Institute of Orthopaedic Manual Therapy (NAIOMT), Inc. Clinical Fellowship1574 Coburg Rd, PMB 129, Eugene, OR 97401-4802Contact: Ann Porter-Hoke, PT, OCS, FCAMT, FAAOMPTPhone: 800/706-5550Fax: 541/485-0016E-mail: [email protected]
Ola Grimsby Institute Orthopaedic Manual Therapy Fellowship4420 Hotel Circle Court, Suite 210San Diego, CA 92108Contact: Julia ChepakPhone: 800/646-6128Fax: 619/298-4225E-mail: [email protected]
Regis University Manual Therapy FellowshipDepartment of Physical Thereapy3333 Regis Blvd, G-4Denver, CO 80221-1099Contact: Timothy Flynn, PT, PhD, OCS, FAAOMPTPhone: 303-458-4344Fax: 303/964-5400E-mail: [email protected]
The Manual Therapy Institute2901 Livorno Cove, Cedar Park, TX 78613Contact: Pieter Kroon, PT, OCS, FAAOMPTPhone: 512/422-4258Fax: 512/467-7203E-mail: [email protected]
University of Illinois at Chicago Fellowship in Orthopedic Manual Physical Therapy1919 West Taylor Street, 4th Floor, Chicago, IL 60612Contact: Carol Courtney, PT, PhD, ATC, FAAOMPTPhone: 312/996-8381Fax: 312/996-4583E-mail: [email protected]
University of St. Augustine For Health Sciences Clinical Fellowship1 University Blvd., St. Augustine, FL 32086 Contact: Catherine Patla, PT, DHSc, OCS, FAAOMPTPhone: 904/826-0084Fax: 904/826-0085 E-mail: [email protected]
U.S. Army - Baylor University Postprofessional Doctoral Program in Orthopaedic Manual Physical Therapy Brooke Army Medical Center3851 Roger Brooke Drive, Fort Sam Houston, TX 78234Contact: MAJ Norman “Skip” Gill, PT, DSc, OCS, FAAOMPT, CertMDTPhone: 210/916-2651Fax: 210/916-4074E-mail: [email protected] For active US Military personnel only

May/June 2008 - Articulations - 7
Committee Reports (continued from page 5)
AAOMPT 2008 Conference in Seattle, Washington 10/29-11/2I. Coordinating events with Let’s Meeta.
Established project plan i. Established marketing planii. Established timeline for conference planning eventsiii. Let’s Meet hired for managing registration process. iv.
Registrationb. Registration online should open in mid April.i. New and efficient registration site managed my Let’s Meet. AAOMPT ii. website will have registration link that will take registrants to Let’s Meet’s website. Demographic information will collected for develop-ment of future conferences.
Marketingc. Target surrounding states and Canadai. Request assistance from committee and members in spreading market-ii. ing through our PT community. Please contact [email protected] if you are able to assist.
Pre-conferencesd. David Butler, Steven George and Julie Whitman/Josh Cleland/Robert i. WainnerKen Olson, Steve McDavitt, William Boissonnault, and guest speakers ii. will be presenting Manipulation legislative battles, advocacy, and physical therapy to assist in educating WA PTs
Thursday half day conference will be $35 to attendees (stu-1. dents- free with accepted donations)Money will be donated to the Washington political action 2. fund. WA is assisting with marketing3.
Keynote speakers – David Butler, Steven George and Richard Deyo iii. will be presenting on Friday with a 30 minute discussion panel before Friday’s Student Meet and Greet/Poster presentation night. Breakoutsiv.
Selected March 11. st
Committee appreciates all the outstanding RFP submissions2. Planning FUN Saturday night reception with costume contests and v. much more!
Student Special Interest Group - Brett Neilson with University of Puget Sound e. will be the student liaison assisting with the student programs at the 2008 con-ference.
AAOMPT 2009 Conference in Washington D.C. 10/14 – 10/18II. Location: Hyatt Regency in Crystal Citya. Keynote speakers: b.
Paul Hodgesi. Deydre Teyhenii. Additional speakers to be announcediii.
Capital Hill day to be planned during pre-conference time period.c.
Education CommitteeConference division
International Affairs Committee
Submitted by Chris Showalter, Chair
REGISTER NOW FOR IFOMT The 2008 IFOMT Congress and
Conference will be held in Rotterdam June 8-13, 2008. The theme is “Connecting Science to Quality of Life” and featured speakers include: Bill Vicenzino, Jillianne Leigh Cook, Deborah Falla, Lorimer Mos-ley, Mark Jones, Karim Kahn, Paul Hodges and many more. More details can be found at www.ifomt2008.nl/.
Administrative sessions will include discussion of changes to the IFOMT Stan-dards, Potential organization name change to include the term “Physical Therapists”, Standardizing manipulation terminology, and a potential logo change.
Delegates will also be voting on the venue for the next Congress to be held in 2012. There are 2 current bidders: Quebec, Canada, and London, England.
EC AMERICASEC Americas members, USA and
Canada, continue in their efforts to reach out to manual therapists interested in join-ing EC Americas. Membership is open to organizations that represent manual thera-pists in countries from Central and South America and the Caribbean. An “Introduc-tion to EC Americas” letter is available in English and Spanish.
If you know a manual therapist from the region, or think you know someone who may know one please email me at [email protected] and I would be happy to send you both letters.
Membership CommitteeRespectfully submitted by Cheri Hodges,
DPT, MAppSc, OCS, FAAOMPT
The membership committee has been busy developing a strategic plan to promote new memberships in all categories. Our top priority as a committee is to regain those past members of our organization that have not renewed their membership. Please confirm your membership status is current on our website. It has come to our attention that some members thought they had renewed their membership for this year, but in fact, their membership status had not actually been renewed. The membership committee will be developing a plan to improve the membership renewal process as our first priority. Please look for the ad coming soon in JOSPT promoting AAOMPT membership and pass the ad on to a colleague facilitating a strong and uni-

8 - Articulations - May/June 2008
fied campaign for “Let the Secret Out”. Matt Beaty is the new chair for the
membership committee of the AAOMPT-sSIG. The “Let the Secret Out” campaign is being extended to the sSIG with a twist. The executive committee has asked its members to recruit 1-2 new members, but the sSIG is planning on topping that by recruiting 3-4 new student members each. They are also trying to get a big group to go to the 2008 Annual Conference in Se-attle. Feel free to contact Matt at [email protected] or [email protected].
Committee Reports (continued from page 7)
Treasurer’s ReportSubmitted by John Childs with assistance
from Craig Crosby and Jamie Bellamy
Budget for 2008Income $ 56,258.77Expenses $113,017.87Difference $ -56,759.10*
Income & Expenses for 2008 (January – March 24, 2008)Income $ 98,089.06Expense $ 64,466.20Difference $ 33,622.86
(PAF) Practice Affairs Fund (January – March 24, 2008)Income $ 26,005Expenses $ 15,000Difference $ 11,005
Assets as of March 24, 2008Operating Account $151,466.98Practice Affairs Fund (PAF) $ 93,603.24Reserve Fund $125,015.40 Total Assets $370,085.62
*Income for conference is budgeted for July-October
Member-at-Large ReportSubmitted by Haideh Plock, PT, ATC
Board Certified in OrthopedicsFellow, American Academy of Orthopedic
Manual Physical Therapists
It’s hard to believe that summer is almost here. Don’t wait too long- get your nominations in for the John Mc. Mennell service award and the Kaltenborn “Teach I Must” award. Information on both of these awards can be found in the Nomi-nating Committee report and also within this issue of Articulations. Please take the time to nominate one of our many skilled and deserving members for these awards. Unfortunately only one recipient can be chosen for each award, so if someone was nominated in the past but did not receive the award, consider nominating them again.
The Membership Committee has been very busy this year. Our Academy membership continues to grow and we want to continue to foster that trend. The Membership Committee along with the Executive is running a “Let the Secret Out” campaign. We are asking each current member to recruit one new member this year. The strength of our organization lies within our members. I guarantee each of us knows at least one other therapist who
would benefit from being a member of this organization. We have an exceptional annual conference and the AAOMPT is also very visible in the fights to keep our professional rights. The Journal of Manual and Manipulative Therapy is also included in your membership dues. I personally feel that the Academy is an excellent value for the benefits we receive. Any manual therapist should jump at the chance to support this organization that defends our ability to practice as we have been trained to practice and provides excellent research and evidence based education.
Thank you to all the new members who joined AAOMPT this past year. And a big thank you to the members who continue to renew their memberships. AAOMPT serves the entire membership as well as defends the practice of manual physical therapy. Without your support we could not defend our profession effectively. I would also like to recognize the work and effort by our members who volunteer their time on different AAOMPT committees. Your work does not go un-noticed. It is amazing that this organization has achieved all it has from work done by hard work-ing volunteers who are passionate about manual physical therapy.
Research CommitteeSubmitted by H. James Phillips, PT,
PhD, OCS, FAAOMPT
The research committee has posted a call for abstracts for poster and platform presentations for this year’s annual conference in Seattle. Due to the overwhelming success of having the poster presentations on Friday evening at last year’s conference, we will again
present posters on Friday, October 31st, with wine and cheese refreshments. All abstracts should be sent to committee chair Jim Phillips at [email protected].
A call has also gone out for propos-als for our two research grants. This year, Cardon has increased their grant to $6,000 and the OPTP grant will be $4,000. Thanks venders! All grant pro-posals should also be sent electronically to Jim at [email protected].

May/June 2008 - Articulations - 9
Our national chapter of IFOMT, the AAOMPT, faces many challenges in the upcoming 2-3
years. Many of you may have heard how the Chiropractic profession continues to challenge our use of manipulation, and has taken this to an all new level by trying to gather 80,000 signatures by 2010 to take the issue to the voters in the state of Or-egon. How can we possibly convince the public that our training and expertise of our value, when we are unable to convince our own PT profession?
At present, we the AAOMPT only have 1865 members. Nationwide we have approximately 125,000 PT’s, which unfortunately means our AAOMPT mem-bership represents less than 1.5% of our profession. Our profession is literally now fighting a battle to defend it’s right to prac-tice Manipulation, but has no army. We need to “beef up” our numbers to defend itself, so ensure victory is ours.
Each of us can change this.We need an “army” of clinicians
of excellence…...we need to encourage AAOMPT membership growth. Although we are fortunate to coordinate our efforts with the APTA, we need to share our enthusiasm with others, our thrill of OMT practice what we all do so well, all in the name of helping our own patients to reach their greatest potentials for recovery. We therefore need to recruit PT’s to JOIN THE AAOMPT!!
Consider the possibilities:AAOMPT BROCHURE: you 1.)
have access to a brand NEW AAOMPT brochure that was revised this year. This is a resource for you to either email and/or distribute to PT’s you know. You can order brochures by a link on the AAOMPT web site.PT SCHOOLS: we need PT’s 2.) who are interested in going to PT Schools and share about the AAOMPT. We are in the process of developing new materials to aide in your presentation. Just think how many new members we could have if we just had 50% of the new graduates? Tim Flynn has done a wonderful job getting his PT Students to attend the last 2 annual conferences!!Study Groups OR “An EVE-3.) NING” w/ OMT” offer a 1 time (or monthly) evening event
Membership profile for 2008
Founding Members: 8 Student Members: 149Full Fellow: 464 Institutional Members: 14Members: 894 North American Members: 7Overseas Members: 2
2008 TOTAL: 1538
MEMBERSHIP:
STAND UP AND BE HEARD!!
to share the value of OMT with PT colleagues in your commu-nity.NATIONAL PT MONTH: 4.) how many of us take advantage of this? October has come and gone. Promote PT and OMT at the same time. Start a campaign for next yearTeach Continuing Education: 5.) spend a few minutes on promot-ing the AAOMPT to your audi-ence. Include brochures in your handouts and course manual.
Our ideas are only limited by our creativity and enthusiasm. If we work together, if even 50% of our current members recruited just ONE PT, we can ensure we build our membership by 600 members by Seattle’s 2008 conference!! Go AAOMPT.
Jeff Giulietti, MPT, ATC, OCS, CSCS, COMT, FAAOMPT, Membership & Practice Affairs

10 - Articulations - May/June 2008
Physical Therapist Advocacy is OUR Principal Course of ActionIt is Not a Spectator Sport!
OSCILLATIONS - Paris Award Acceptance Speech
What can I say? What words could possibly define or il-lustrate the powerful impact
receiving this award has had on me? The best I can say is that I am tremendously honored and humbled to stand before the colleagues I so admire, deeply respect and appreciate, to receive this award of acknowledgement for contributions I have made to the Orthopaedic Section and its 16,500 members. My sincer-est gratitude goes to the Orthopaedic Section Executive Committee, Awards Committee and those of you who surren-dered your time and effort to distinguish me in this regard.
Throughout my career I have had the privilege of collaborating and men-toring with many of the previous Paris awardees including Lola Rosenbaum, Bill Boissonnault, Carol Jo Tichenor, Nancy White, Dorothy Santi, Rick Ritter, Joe Farrell and especially Stanley Paris. Rec-ognizing this gives me even deeper pride in receiving this award.
What is genuinely meaningful to me is being able to publicly acknowledge amongst the kin of my colleagues my deep admiration and love for my wife of 31 years, Martha and our 18 y.o. twin daughters Anna and Kathy who through these many years of my service have accepted and supported my boundless passion and sacrifice for my practice and profession and who have likely forfeited even more themselves. They have been the pulse of meaningful reality that has kept me on track through the storms of professional service that as many of you who have served know, can easily sway one from the real important elements of life. My daughters could not be here tonight but my wife Martha is here and in gratitude I would like her to stand and be recognized.
What about my affiliation with Dr.
Stanley Paris, the Section’s first President in 1974, after whom this award is named? I first met Dr. Stanley Paris and his faculty in 1982 and even though I have had many mentors since then, Dr. Paris especially has continued to provide me with guiding influence to this day. I have always viewed Stanley as a practitioner, teacher and leader ahead of his time who not only raised the bar on practice standards and professional-ism but more importantly has been one of the leaders in taking the responsibility of promoting the need for advocacy in physi-cal therapist practice.
In his teachings, Stanley has always discussed the meaningful collaborative and interdependent role of the Physician and Physical Therapist and directed us to pre-cisely advocate our autonomous identity.
Dr. Paris’s curriculum has always promoted clinical principles of examina-
tion, evaluation, diagnosis of dysfunction, reasoning for choosing interventions, defining a prognosis and developing treat-ment plans from the clinical assessment. In his course notes on The Foundation of Clinical Orthopaedics in the late 80’s Stanley emphasized a chapter describ-ing managing patient care with “Clinical Studies that Influence Clinical Decision Making in PT”. Other topics across his manual therapy courses included concepts in business management of a PT clinic, addressing the patient needs, how to be professional and futuristic controversial discussions on the future of PT including the Doctoring profession, Chiropractic infringement and POPTS (or, referral for profit). This practice framework and information was in Dr. Paris’s educational format and objectives well before the public presentation of The
by Stephen C.F. McDavitt PT, DPT, MS, FAAOMPT
Martha McDavitt, Stephen McDavitt and Tim Flynn.

May/June 2008 - Articulations - 11
Guide to Physical Therapist Practice, Sackett’s presentation of evidence based practice and Vision 2020.
Stanley’s vision and actions toward our autonomy (what he referred to earlier as “professionalism and private practice”), by professing and demonstrating our need to advocate for our rights to prac-tice PT at an autonomous level early on, is what impressed upon me the value and need for professional advocacy. I believe that appreciation combined with my relevant personal challenges experienced in the frontlines of private practice in the 80’s and 90’s, and through contentious legislative regulatory debates that I will bring up later, facilitated me to become deeply engaged in the advocacy/leader-ship process. I became infected with the tenacious desire to remove unnecessary conventional clinical barriers and abate pointless PT practice prohibitions. I found through that realization that physical therapist advocacy is our princi-pal course of action; it is not a spectator sport! Recognizing this historical mentor-ing impact adds further significance to me in receiving this award named in Dr. Paris’ legacy of praiseworthy leadership.
In consideration of all this recogni-tion and decoration however, I remain
feeling somewhat so undeserving of this award because it is all of you; my wife and children, the members of the Sec-tion (including previous Paris awardees), the AAOMPT and the APTA, that have provided me the opportunities to serve, guided me and have over many years, already supported my advocacy leadership contributions to our profession at a capac-ity I believe that has given me so much more in return.
Since advocacy of our practice has been my platform, defining our ongoing need for active individual and group advo-cacy in PT practice is what I will address tonight.
So how did I get here, what have I done, what are my acknowledgements and what do I have to share? That is what I am supposed to address. Let me just say this at the get go here that it is not in my nature to sing my own praises about what I am being recognized for. I am a mission man of focus, first on a strategy and then on achieving the desired outcome. I see myself as pulling the oars like everyone else. Besides, there are too many colleagues that shared in my work and enabled me to have a role in facilitating the outcomes of advocacy I helped orchestrate and deploy over the past 19 or so years. I will there-
fore share my experience in my personal practice development parallel with the evolution of PT practice that I believe led me where I am with involvement in lead-ing multiple PT advocacy initiatives and outcomes. From this personal viewpoint I hope this will enable you all to respect and appreciate why we all must take ownership in actions of practice advocacy for the quality and survival of our prac-tice of physical therapy as individuals, as specialists and as an association.
So again, how did I get here? Reading from my faculty recom-
mendations thirty two years ago when I graduated from PT school in 1976, I was rated as “An average student that works hard.” Of course I worked hard, I was av-erage. PT school was no cakewalk. I did not see myself as a leader in the profes-sion, nor did anyone else; I think.
My mind set after the load of PT school was; I’m done! I was never; “going back to school, teach, or own and operate my own practice”. I certainly had no vision of being involved in advocacy for the profession. Who me? Not my job! I “gotta” get a job and practice.
Sounds a bit selfish and apathetic for a “professional”, don’t you think? Com-pared to the current post-professional development directives, DPT curriculum and clinical graduate today in their quest for Vision 2020, I do not feel I was “a true professional” when I graduated. It took quite some time to be professionally mentored and cultivated.
Frankly, when considering the comparative lack of depth in PT prac-tice competencies and professionalism of that time it is quite understandable. After all, my teachers and their teachers had come from a practice environment of the 60’s that was very different from today. The PT culture of the times from 1950’s through the early 70’s viewed private practice as controversial. “PTs are a service group dedicated to medicine as opposed to making a profit.” The PT’s in the late 60’s and early 70’s practiced based on the 1960 HOD resolution to establish the baccalaureate degree as the
Stephen McDavitt and Bob Rowe.

12 - Articulations - May/June 2008
minimal standard for the PT. It was not until 1973 that the APTA Code of Ethics and Guide to Professional Conduct supported practice by referral as opposed to prescription.
Therefore the practice settings, mind set and parameters of the time for me were as follows:
Treatment by prescription was •greater than by referral where the Physician was directive. Relatively minimal Direct Access.•Masters level of education was a •mere blip on the radar screen.Minimum private practice, since •PTs were mostly employed. PT’s viewed themselves as attaining a “job” not “developing a practice” Salaries? My salary @$10,000.00•Mobilization / manipulation, some-•thing later near and dear to me was at that time considered Chiroprac-tic and pseudoscience! Even though PTs at that time practiced and
appreciated the values and outcomes of mobilization / manipulation, with their close ties to medicine, PTs of that time who practiced it, kept it “in the closet”.
What followed soon after I graduated and started practicing however included the following circumstances that began to reshape my and our practice:
The public benefits of practice with-1. out referral and the need to define and manage advanced educational competency were emphasized by PTs through the mid to late 1970’s.
In 1979 the APTA House of Delegates 2. recognized the knowledge-accumula-tion and expertise of PTs by prescrib-ing post-baccalaureate education for all entry-level PT education programs. MPT.
In 1979-1980, after 3-4 years of hospital based inpatient and outpatient practice, and upon appreciating the dynamic evolution within PT practice of that time, my professional values and vi-sion changed. I wanted to be proactively, clinically prepared and professionally competitive. In 1980, I returned to gradu-ate school and receive an Advance Masters in PT.
In the years 1980-1981 while I was finishing Graduate School and began teaching, the APTA House of Delegates sanctioned practice without referral as ethical where legal. Following that time and during the following decade (1981-1991) while I was teaching and de-veloping and expanding my solo practice, initiatives for practice without referral in PT practice accelerated and thus began the relatively exponential legislative initiatives and challenges for direct access. Medicine was concerned about the act of PTs claiming to make a medical diagnosis and chiropractic about a formal sanction-ing of PTs manipulating.
Over those post-graduate and practice development years, through my culmination of professional growth, I developed a deeper appreciation and passion for the independent practice of PT in clinical orthopaedics and especially manual therapy and its outcomes. With that experience and in identification with those practice privileges and outcomes, I developed a strong desire to abate any unnecessary regulatory limitations on the independent level of physical therapist practice.
In appreciation of this movement toward independent patient management through practice without referral, in 1989 I proposed to the Maine Chapter that passing legislation to allow Direct Access was in our best interest and the timing was as good as it would ever be. I was as-signed the Direct Access Committee and later with my Co-Chair David White PT we prepared our rural state for what we thought would mainly be the challenges from the medical society. Where we were challenged the greatest however was from the Chiropractors.
Stephen McDavitt with fellow award recipient Stanley Paris.

May/June 2008 - Articulations - 13
Discussing the details of those in-valid and contentious debates are beyond our time limit here. In summary, absent of formal descriptions of practice and armed only with limited manual therapy literature and grass roots efforts, we succeeded in defeating the Chiropractic resistance against spinal manipulation and became the 25th State to achieve PT direct access in 1991.
I was sold on local advocacy early on, but that contentious, insulting and demeaning Maine legislative challenge is what I believe to be the catalyst to my passion and drive for working at a national level for practice protection and advocacy. That experience fueled an internal tenacity for PT practice protec-tion I never knew I had. I realized then that all of PT practice required on-going monitoring for protection and advocacy, and we needed to stop reinventing the wheel.
Along those lines, in expectation of similar challenges nation wide and so as to not have others reinvent the wheel, I produced our 400 page manual of strategic information and provided it to all APTA Components at the following Government Affairs Forum to compliment the “Direct Access Packet”.
The late 80’s and 90’s brought further change and demands for PT advocacy. Practice without referral as ethical where legal and direct access initiatives became catalysts for development of the compe-tency based consensus documents The Guide to Physical Therapist Practice and A Normative Model of Physical Therapist Education. Continuous advancement of clinical practice competency during the
1990s through education, specialization, residencies, and fellowships warranted mapping out in greater detail the current and future practice of physical therapy.
Accordingly, in 2000, the APTA House of Delegates further expanded and defined its future view of the pro-fession’s advanced clinical practice by adopting the APTA Vision Statement for Physical Therapy 2020. Those practice changes driven by the membership in the decade 1994-2004 placed significant demands on practice initiatives from the APTA, the Orthopaedic Section and the AAOMPT.
During the span of those years I was privileged to be recruited to three formal professional assignments that
I was sold on local advocacy early on, but that con-tentious, insulting and demeaning Maine legislative challenge is what I believe to be the catalyst to my passion and drive for working at a national level for practice protection and advocacy.

14 - Articulations - May/June 2008
truly propelled my career toward higher levels in PT advocacy through national leadership.
In 1993 Joe Farrell as President 1. of the AAOMPT realized the im-mediate need to protect our manual therapy practice rights and to promote best practice and education policies. In 1994 at the AAOMPT annual conference he approached me based on my Maine experience with defending the practice of spinal manipulation and upon nomination I was appointed as the AAOMPT Practice Affairs Chair which is a position I developed and held from 1994-2003.
Similar 2. needs were appreciated by Bill Bois-sonnault as President of the Orthopaedic Section and I was asked and accepted to Co-Chair the Orthopaedic Section Practice Committee with Helene Fearon in late 1996. I later took over as Chair and I held this appointment in tandem with that of AAOMPT from 1998-2004. I further served as the Orthopaedic Section Delegate from 2001-2004.
In 1998 with the appreciation of 3. the surging challenges on achieving direct access and the related confron-tations on maintaining the practice scope of mobilization / manipula-tion, the AAOMPT, the Orthopaedic Section and the APTA BoD realized a need of A Manipulation Task Force. With my experience and ties to the relevant on-going initiatives of the AAOMPT and the Orthopaedic Section I was appointed the task force Co-Chair in 1999 and remained its Chair 2000-2004.
In the years 1994-2004, with the
collaborative guidance and support of Bill Boissonnault and Mike Cibulka; Presidents of the Orthopaedic Section, Joe Farrell, Mike Rogers and Ken Olson; Presidents of AAOMPT and various APTA BoD Liaisons and Staff Directors at APTA, we facilitated, framed and maintained a “Tri-alliance” or “Synergy” collaboration (AAOMPT-APTA-Orthopaedic Section) as it pertained to practice protection and ad-vocacy. The purpose was to begin not only an advocacy action plan of initiatives for orthopaedics, manual therapy and direct access but to also begin an exemplary tem-plate to be used anywhere in PT practice to enhance advocacy through collaboration in communication, networking, access and monitoring.
I will sequentially mention a few of those outcomes that promoted and en-gaged in successful collaborative advocacy and how these seeded other advocacy initiatives elsewhere.
In 1995 we developed the “Manipu-•lation Forum” whose purpose was to create a face to face networking opportunity for PTs to nationally collaborate, share, empathize and communicate on their experiences and action plans as it pertains to manual therapy and direct access.
In 1997, with an increased awareness •of states trading mobilization/manipu-lation for direct access, new materials were created for the APTA Direct Access Packets to abate this.
In 1998 with an awareness of PTA’s •and ATC’s being inappropriately provided psychomotor education on mobilization/manipulation and other interventions, the AAOMPT Prac-
tice Affairs Committee produced a position statement on inappro-priate teaching and practicing of such interventions which was later with editorials co-sponsored by the Orthopaedic Section, the APTA BoD and 17 Sections passing in the APTA HoD as the Position on Interventions Exclusively Performed by Physical Therapists.
We also lobbied and achieved pass-•ing in the APTA HoD the Position on Continuing Education for Physi-cal therapist Assistants and Other Supportive Personnel. This helps continuing education instructors objectively validate student compe-
tency with inclusive and exclusive crite-ria while preventing discrimination and enhancing patient safety.
In the years •1998-1999 with consensus across AAOMPT, the Orthopaedic Sec-tion and APTA, the definition for Mobilization/Manipulation was revised for the 1999 Guide revision. This operational definition by way of its practice description param-eters as opposed to the ambiguity of tissue barriers provides protection of practice across the variety of state regulation requirements.
Between the end of 1998 through •June of 1999, 18 states experienced 22 pieces of legislation put forth by Chiropractors to prohibit PTs from spinal manipulation. The APTA, the AAOMPT and the Orthopaedic Section compiled materials and pro-vided guidance to all of those states who then successfully defeated those threats. A sample of those materials includes the Manipulation Take Ac-tion Packet and the Compendium on Manual Manipulative Therapy.
I have further realized a love, passion and tenacity for developing and protecting a profession I can not even begin to explain.

May/June 2008 - Articulations - 15
In appreciation from that experi-ence the tri-alliance agreed at the 1999 manipulation forum that a consolidation of resources and proactive nation wide strategies were warranted. A consideration of a manipulation task force was pro-posed by me and Bill Boissonnault. After consulting with APTA, and complet-ing a national component survey, it was determined that a national scope of the manipulation threat issues was significant.
In September 1999, the APTA BoD sanctioned a Manipulation Task Force with me as the Orthopaedic Section/AAOMPT contact, and Jerry Conley as the APTA Staff contact appointed Co-chairs. The group formulated a strategic plan and initiatives directed at proactive and reactive strategies for legislation, regulation, practice and education. This TF yielded outcomes including but not limited to;
Open forums, debates, panel discus-sions and programming at CSM, APTA Annual Conferences and AAOMPT conferences.
Immediate response documents to abate last minute legislative chal-lenges. (McDavitt / Rogers Road Show Doc.)
Collaboration with the Education Section and others to produce educa-tional experiences of greater depth at entry level professional curriculum. (Manipulation Educational manual)
Enhanced evidence through research for CAPTE to sanction a revision for mobilization / manipulation, to include thrust and non-thrust tech-niques in the 2004 Physical Thera-pist Evaluative Criteria.
The list goes on with too much to discuss any further in this arena. What I would like to point out, however, is that many other APTA initiatives beyond the APTA Manipulation Task Force have followed suit by using our “tri-alliance”
template, such as the referral for-profit task force to enhance national and global networking, collaboration, and produce materials to enhance PT advocacy that includes defending or promoting any ele-ment of physical therapist practice in any state or jurisdiction.
For approximately 19 years, I have personally engaged and committed my passionate energy in PT practice affairs ad-vocacy that has included holding multiple state and national APTA and AAOMPT positions. The greatest honor and privilege
in the domain of advocacy has been to be elected for a second term to serve over 70K APTA members on the 15 member APTA Board of Directors. The past 2 Presidents and 4 APTA Boards have been wonderful mentors and colleagues to learn, deliberate and collaborate with. Over this time, I have further realized a love, passion and tenacity for develop-ing and protecting a profession I can not even begin to explain. Hardly the mind set I had in 1976! I have also appreciated two other more important concepts not
Photos Needed for History of the Academy
Stanley Paris, Ron Schenk and
Ken Olson met in San Diego during
CSM in February to outline a strat-
egy to develop a written and photographic history of the
Academy. Once complete, it will be placed on the Acad-
emy website. Dave Miers has offered to help coordinate
the photographic portion of the project. Members who
have photographs of Academy events are asked to send
a digital or hard copy of the photographs to Dave Miers
([email protected]). Other documents that may assist
in writing the history of the Academy can be sent to Ken
Olson.
From this personal viewpoint I hope this will enable you all to respect and appreciate why we all must take ownership in actions of practice advocacy for the quality and survival of our practice of physical therapy as individuals, as specialists and as an association.

16 - Articulations - May/June 2008
apparent to me in 1976 that I believe are extremely important today:
Professional advocacy is not a spec-1. tator sport and there is no better ACTIVE advocate for your practice and profession than you!
If you don’t take care of yourself, 2. you have no quality of life. If you don’t take care of your profession or professional organization you have no quality of your profession or your practice. Just ask the Chiropractic Profession
and its 8 organizations that compete and lack consensus with each other.
Advocacy or, support, encourage-ment, backing, sponsorship and promo-tion of our profession, is every individual PT’s responsibility to be complimented by the networking and reinforcement
The Dash By Linda Ellis (www.lindaslyrics.com/thedashpoem.html)
I read of a man who stood to speak at the funeral of a friend.He referred to the dates on her tombstone from the beginning…to the end.
He noted that first came the date of her birth and spoke of the following dates with tears, but he said what mattered most of all was the dash between those years.
For the dash represents all time that she spent alive on earth…and now only those who loved her know what the little line is worth.
For it matters not, how much we own;The cars….the house…the cash.What matters most is how we live and love and how we spend the dash.
So think about this long and hard…are there things you’d like to change?For you never know how much time is left. (You could be at “dash mid-range”)
If we could just slow down enough to consider what’s true and real,and always try to understand the way other people feel.
And be less quick to anger and show appreciation moreand love the people in our lives like we’ve never loved before
If we treat each other with respect, and more often wear a smile…remembering this special dash might only last a little while.So when your eulogy’s being read with your life’s actions to rehash..would you be proud of the things they say about how you spent your dash?
tools available from their Chapter, Section, Specialty and Association. My colleague John Wallace appropriately professes “our patient is our practice and our practice is our business”. I also believe the necessity for all of us engaging in PT advocacy across the spectrum from our one–on–one direct patient practice to education, reimburse-ment, marketing, legislation and research to appreciate that; our patient is our practice, our practice is our business, our profession is our responsibility and our association is our insurance. I repeat; our patient is our practice, our practice is our business, our profession is our responsibility and our association is our insurance. Autono-mous advocacy has a price in personal and financial commitment whose outcomes are priceless.
Advocacy is an act that can be enacted by anyone. Average or not- in PT practice advocacy, there is room for everyone and a
reason for everyone to participate. Who is “average” today may be a leader tomor-row!
Abraham Lincoln was quoted as stating “Those who chose not to partici-pate in democracy are doomed by those who do”. The same could be said about advocacy.
So now it’s your turn to start. When one mentions creating and
taking opportunities for advocacy, many pessimists view difficulty. Winston Churchill has been quoted as acknowl-edging that “a pessimist sees difficulty in every opportunity, and an optimist sees opportunity in every difficulty”.
What is advocacy to you? Is it an act in pessimism or optimism? What is your mind set, practice set and where is your level of interest and passion for the challenge to take the advocacy baton in the movement for our professions practice vision, growth and opportunity? What will you do to be known as the practitioner of choice?
In closing, I would like to read this poem and make a few final comments relevant to the core values of profession-alism I feel are relevant to PT advocacy.
Beyond my personal beliefs and goals I know the dash in my professional lifespan will be advocating for what I know is an eclectic profession like no other that can make the difference in bringing the highest quality of life to years and whose practitioners are truly practitioners of choice deserving of all Vision 2020 stands for.
Like the “Life is good” slogan from Bert and John Jacobs; “Life is good. Do what you like and like what you do” (www.lifeisgood.com). “PT practice is good. Advocate what you like and like what you advocate.”
See you in the front lines, where many hands make light work and where the practice outcomes we desire to attain will be achieved from our active individ-ual and grouped advocacy for our great profession and practice.
Again, I thank you for this wonder-fully meaningful recognition and the opportunity to share my thoughts.

May/June 2008 - Articulations - 17
CLINICAL PEARL
General Non-thrust Mobilization TechniqueTargeting the Thoracic Spine
Derek S. Dalton, SPT and Christopher A. Covert, SPT
For this technique, the patient begins in the long-sitting position on the treatment plinth with their hands
placed behind their neck and elbows flared out laterally (Figure 1). The physical therapist (PT) then places his anterior tibia on the plinth and assesses the proper posi-tioning of his femur by visually estimating where the patient’s thoracic spine will be positioned once they are lowered back into the supine position. The patient is then instructed to begin slowly lowering into the supine position, while the PT assists with this task as needed and ensures that the patient does not pull their cervical spine into forced flexion. The patient is now lying supine with their thoracic spine on the therapist’s femur (Figure 2). While this treatment technique is very general in nature, the knee can be placed at various regions of the thoracic spine in an attempt to target a specific region of the thoracic spine. In this case, the therapist is target-ing the upper thoracic segments. It should be noted that recent research has indicated that specificity with targeting specific spinal segments is low.1 The PT then threads his hands through the space created by the pa-tient’s upper extremities and cervical spine until the hands are placed on the patient’s lateral trunk at the desired portion of the patient’s ribcage (Figure 3). To target the upper thoracic segments, the hands are placed higher on the ribcage. As lower segments are targeted, the therapist simply moves the hands distally toward the infe-rior portion of the ribcage. At this point, the PT provides a “scooping” or “lifting” motion in order to take up the slack in the region of the thoracic spine over the therapist’s femur and then slightly leans backward to create an extension moment.
The technique is gentle and care should be taken to ensure that the cervical spine is not stressed. This technique, while
it is a non-thrust technique, usually pro-duces cavitation. However, early research findings regarding the success of thrust manipulation targeting the thoracic spine for mechanical neck pain indicate that the number of cavitations in the thoracic spine is not strongly correlated to outcomes.2 It is unclear if this can be generalized to non-thrust techniques; however, Cleland et al3 have found that thrust techniques targeting the thoracic spine provided superior out-comes to non-thrust techniques in patients with mechanical neck pain. Furthermore, there is evidence that choice of treatment technique may not be as important as once thought.4
The authors of this clinical pearl were unable to find the described technique in the peer-reviewed literature, so no claims regarding its effectiveness can be defini-tively made. Anecdotally, it appears to assist in allowing patients who tend to maintain a kyphotic posture and report thoracic discomfort to maintain a more upright posture and improve their pain free range of motion. This technique could potentially be utilized in cases when thrust manipulation techniques, for whatever rea-son, are considered to carry a greater than acceptable risk. This technique, with some variations, has been reported elsewhere.5-7
Ross JK, Bereznick DE, McGill SM. Determining cavitation location during lumbar and thoracic spinal manipulation: 1. Is spinal manipulation accurate and specific? Spine. 2004;29:1452-1457.Cleland JA, Flynn TW, Childs JD, Eberhart S. The audible pop from thoracic spine thrust manipulation and its relation 2. to short-term outcomes in patients with neck pain. J Manual Manipulative Ther 2007;15:143-154.Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C, Childs JD. Short-term effects of thrust versus non-thrust 3. mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial. Phys Ther. 2007;87:431-440.Chiradejnant A, Maher CG, Latimer J, Stepkovitch N. Efficacy of “therapist selected” versus “randomly selected” 4. mobilization techniques for the treatment of low back pain: a randomized controlled trial. Aust J Physiother. 2003;49:233-241.Stoddard A. Manual of Osteopathic Technique. London: Hutchinson Medical Publications, 1959.5. Snider K, Steele KM. West Virginia School of Osteopathic Medicine Mini Manual of Muscle Energy and HVLA 6. Techniques. West Virginia: West Virginia School of Osteopathic Medicine, 1997.Philip Fisher DO, PhD. Personal Communication. 2007.7.
Figure 1
Figure 2
Figure 3

18 - Articulations - May/June 2008
RESEARCh PEARL
ClINICAl BOTTOM lINE(S):Patients with lumbar spinal stenosis (LSS) can benefit •from physical therapy interventions. A greater proportion of lumbar spinal stenosis patients •benefited from a program consisting of manual physical therapy, body weight supported treadmill walking and specific exercises compared with a program of flexion exercises and unsupported treadmill walking.
CITATION(S):Whitman JM, Flynn, TW, Childs JD et al. A Comparison •Between Two Physical Therapy Treatment Programs for Patients With Lumbar Spinal Stenosis: A Randomized Clinical Trial. Spine. 2006; 31(22): 2541-2549.
ThREE/FOuR PART quESTION:In patients with lumbar spinal stenosis does a treatment •program of manual therapy and body weight supported treadmill walking provide a better outcome than treatment with flexion exercises and treadmill walking only?
ThE STuDy:This was a multi-center, randomized controlled trial with •blinded outcome assessment. 58 patients, age • ≥ 50 years, with pain in the lumbopelvic region and lower extremities, MRI evidence of lumbar spinal stenosis, and a patient rating of sitting as a better position for symptom severity than standing.Two groups (n=29 for each group) participated in twelve •45-60 min sessions of physical therapy twice weekly for 6 weeks.The Flexion Exercise and Walking Group (FExWG) •received lumbar flexion exercises, an unsupported tread-mill walking program and 10 minutes of sub-therapeutic ultrasound treatment. Ultrasound was added to mitigate the potential for an attention effect to occur. The exercises consisted of three 30-second bouts of unilateral and bilat-eral knee to chest exercises. Additionally, all participants (in both groups) were asked to perform a home exercise program including daily walks without provoking their symptoms and performing the prescribed exercises. The Manual Physical Therapy, Exercise, and Walking •Group (MPTExWG) received manual therapy to the thoracic and lumbar spine, pelvis, and lower extremities; specific exercises in addition to the flexion exercises in
the FExWG group; and body-weight supported treadmill walking. The primary outcome measure was the Global Rating of •Change (GRC) and improvement was defined as scores of +3 (“somewhat better”) or greater. The GRC ranges from -7 (“a very great deal worse”) to 0 (“about the same”) to + 7 (“a very great deal better”)Data was collected at baseline, 6 weeks, 1 year, and a long •term follow up (average 27-29 months)
ThE EvIDENCE:There was a significant association between treatment •group and perceived recovery (P=0.0015) at the 6 week point. However, at the 1 year and long term follow up there was no longer a significant association between group and perceived recovery. The table shows the percent of perceived recovery for both groups at the three time periods.
COMMENTS:Only about 3 patients need to be treated with the MP-•TExWG program to prevent 1 patient from not achieving perceived recovery at 6 weeks (NNT=2.6)Improvements in disability, satisfaction, and treadmill •walking tests favored the MPTExWG at all follow-up points.
Physical Therapy Treatment for Patients with Lumbar Spinal Stenosis
Appraised by: Arjen Holdinga, PT, FAAOMPTDate Appraised: March 2008
Kill or update by: March 2009
Research Pearl Physical Therapy Treatment for Patients with Lumbar Spinal Stenosis
Appraised by: Arjen Holdinga PT, FAAOMPT
Date Appraised: March 2008 Kill or update by: March 2009
Clinical Bottom Line(s):
Patients with lumbar spinal stenosis (LSS) can benefit from physical therapy interventions. A greater proportion of lumbar spinal stenosis patients benefited from a program consisting of manual physical
therapy, body weight supported treadmill walking and specific exercises compared with a program of flexion exercises and unsupported treadmill walking.
Citation(s):
Whitman JM, Flynn, TW, Childs JD et al. A Comparison Between Two Physical Therapy Treatment Programs for Patients With Lumbar Spinal Stenosis: A Randomized Clinical Trial. Spine. 2006; 31(22): 2541-2549.
Three/four part question.
In patients with lumbar spinal stenosis does a treatment program of manual therapy and body weight supported treadmill walking provide a better outcome than treatment with flexion exercises and treadmill walking only?
The study:
This was a multi-center, randomized controlled trial with blinded outcome assessment. 58 patients, age 50 years, with pain in the lumbopelvic region and lower extremities, MRI evidence of lumbar spinal
stenosis, and a patient rating of sitting as a better position for symptom severity than standing. Two groups (n=29 for each group) participated in twelve 45-60 min sessions of physical therapy twice weekly for 6
weeks. The Flexion Exercise and Walking Group (FExWG) received lumbar flexion exercises, an unsupported treadmill
walking program and 10 minutes of sub-therapeutic ultrasound treatment. Ultrasound was added to mitigate the potential for an attention effect to occur. The exercises consisted of three 30-second bouts of unilateral and bilateral knee to chest exercises. Additionally, all participants (in both groups) were asked to perform a home exercise program including daily walks without provoking their symptoms and performing the prescribed exercises.
The Manual Physical Therapy, Exercise, and Walking Group (MPTExWG) received manual therapy to the thoracic and lumbar spine, pelvis, and lower extremities; specific exercises in addition to the flexion exercises in the FExWG group; and body-weight supported treadmill walking.
The primary outcome measure was the Global Rating of Change (GRC) and improvement was defined as scores of +3 (“somewhat better”) or greater. The GRC ranges from -7 (“a very great deal worse”) to 0 (“about the same”) to + 7 (“a very great deal better”)
Data was collected at baseline, 6 weeks, 1 year, and a long term follow up (average 27-29 months) The Evidence:
There was a significant association between
treatment group and perceived recovery (P=0.0015) at the 6 week point. However, at the 1 year and long term follow up there was no longer a significant association between group and perceived recovery. The table shows the percent of perceived recovery for both groups at the three time periods.
LSS Patients Receiving Physical Therapy
010
2030405060
708090
6 Weeks 1 Year Long- term
Perc
eive
d Re
cove
ry (%
)
FExWGMPTExWG
Comments: Only about 3 patients need to be treated with the MPTExWG program to prevent 1 patient from not achieving
perceived recovery at 6 weeks (NNT=2.6) Improvements in disability, satisfaction, and treadmill walking tests favored the MPTExWG at all follow-up points.

May/June 2008 - Articulations - 19
THE CARDON REHABILITATION PRODUCTS GRANTup to $6,000
THE ORTHOPAEDIC PHYSICAL THERAPY PRODUCTS GRANTup to $4,000
ELIGIBILITY: The principal investigator must be a member in good standing with the AAOMPT.
TOPIC AREA: A study that relates to orthopaedic manual physical therapy (OMPT).
SUBMISSION: Each proposal must include the following:Title page (title, name of investigator(s), address, phone, email of principal investigator) 1. Abstract 2. Significance Section (describing significance of the study to the PT profession in terms of the Guide to Physical Therapist Practice)3. Background Section with literature review relevant to the study4. Subjects, Methods, Data Analysis Sections 5. Statement of protection of rights of human subjects (sample consent form must be included and Institutional Review Board 6. documentation if available)Time Table Section for completion of project stages (each grant will be presented at the annual fall conference in October)7. Detailed Budget Section8. CV for each investigator9. References10. Appendices (as needed to strengthen the proposal)11.
Please note: members of the Research Committee are available to assist you with the submission of your research proposal. Please contact H. James Phillips ([email protected]) with your questions.
DEADLINE: One copy of the proposal must be e-mailed in pdf or MSWord format no later than June 15, 2008.
SEND PROPOSALS to this e-mail address: [email protected] - H. James Phillips, Chair Research Committee
REVIEW PROCESS: The members of the AAOMPT research committee serve as the review committee for awarding these grants. Scoring will be based on significance of the study to OMPT, quality of the research design, potential for successful completion, and appropriateness of the budget. Reviewers are NOT blinded to author(s) identity, but reviewers identity will remain confidential.
RESPONSIBILITIES OF THE REVIEWERS: The reviewers will independently score each proposal. The chairperson of the Research Committee will tally the scores and advise the AAOMPT Board of Directors of the Committee’s selection for the award. Each reviewer will also make recommendations for improvement of each proposal during their reviews. This evaluative information will be provided to all investigators.
RECIPIENT’S OBLIGATION: The recipient of this award will 1) acknowledge the source of their research grant award (CARDON REHABILITATION PRODUCTS or OPTP) on all publications and presentations derived from this study 2) ac-knowledge AAOMPT support on all publications and presentations derived from this study, 3) provide a yearly progress report to the AAOMPT Research Committee by the anniversary date of the grant if the proposed work continues for more than one year, 4) present the findings of this study at the AAOMPT annual conference within two years of receiving the award, and 5) submit the study for publication in a peer review journal.
On behalf of all of the members of the AAOMPT, the following vendors are recognized for their generosity and commitment in support of research in orthopaedic manual physical therapy:
CARDON REHABILITATION PRODUCTSORTHOPEDIC PHYSICAL THERAPY PRODUCTS
CALL FOR RESEARCH PROPOSALS 2008

20 - Articulations - May/June 2008
Practice Affairs Corner
Advocacy and Education
The areas of service that I am most proud of are the contributions the Academy has made regarding advocacy and education. Legislation and education are intimately related, and I have had personal experiences that illustrate this point.
In 2001, the Illinois Prairie State Chiropractic Association filed a complaint with the Illinois department of professional regulations that the Northern Illinois Uni-versity Physical Therapy program was teach-ing “chiropractic techniques” and thereby violating the PT practice act. Since I was the primary orthopaedic physical therapy faculty member at NIU at that time, I was invited to attend a hearing conducted on this matter in which I presented arguments that what I taught was within physical therapists’ scope of practice and was in full compliance with physical therapist academic program accreditation guidelines. The chiropractors argued that since Illinois law prohibited Physical therapists from performing “chiro-practic techniques” that physical Therapists should not be allowed to perform and teach high velocity thrust manipulation. “Chiro-practic technique” is currently not defined in Illinois law, and we argued that physical therapists can not possibly teach or practice “chiropractic technique” because we do not receive the full training in chiropractic phi-losophy that chiropractors receive in their professional education.
We were able to successfully defend our position because of the resources provided by the Academy and APTA manipulation task force and because we used the “profes-sional education” argument. This is a very common strategy in legislative and regula-tory turf wars between professional health care groups. The typical approach is to argue that the public is at risk of harm if legislation is passed to expand the scope of practice beyond the professional education. While I was legislative chairman for the Illinois Physical Therapy association, in a two year span we successfully used this argument with the Athletic trainers, massage thera-pists, and occupational therapists.
In 2003, the Academy established a goal to work to enhance the level of instruc-tion of manipulation in Physical Therapist professional education and worked with the APTA to put together the manipula-tion education committee. The result was development of the Manipulation Educa-tion Manual (MEM) designed to provide resources for physical therapist educators on how to enhance the professional cur-riculum on manipulation including thrust.2 The committee also worked with the APTA committees revising the Commission on accreditation of physical therapist educa-tion (CAPTE) Evaluative Criteria3 and the Normative model for Physical Therapists Education4 to clarify in the 2005 revisions of these consensus documents that both thrust and non-thrust manipulation for the spine and extremities must be taught in physical therapist professional education programs. The committee members also provided educational programming at professional meetings and a 2 day continuing education course to bring the contents of the Manipu-lation Education Manual to the attention of physical therapist academic and clinical educators.
Evidence of the positive impact of the Manipulation Education Manual occurred in Illinois earlier this year when the Illinois Chiropractic Society, with the support of the Illinois Osteopathic Medical Society, proposed legislation to define …”chiro-practic technique” as a “manipulation” that is…”equivalent to GD Maitland’s range of movement scale grade V.”5
Since Physical Therapists in Illinois are prohibited from performing ”chiropractic technique”, this definition would prohibit physical therapists’ ability to practice thrust manipulation in Illinois and also prevent physical therapists from calling a thrust a Grade V mobilization/manipulation.
Illinois Physical Therapy Association President Peter McMenamin and I had an opportunity to meet with the lobbyists and leaders of these two organizations to explain that mobilization/manipulation includ-
The following is an ex-cerpt from Ken Olson’s recent John McMennell Service Award speech. This well-deserved honor was marked by an insightful speech, highlighting a number of personal experiences Ken has endured related to chiropractic legisla-tive challenges. The experience described here is similar to many recent state challenges put forth by the chiro-practors; attacking our educational training. The use of official docu-ments spearheaded by the Academy and APTA were instrumental in the Illinois Chapter success. Please spread the word about the documents de-scribed here Congratula-tions Ken!

May/June 2008 - Articulations - 21
ACADEMY MEMBERS STAY CONNECTEDThe American Academy
of Orthopedic Manual Physical Therapists
2104 Delta Way, #7Tallahassee, FL 32308
850-222-0397
Craig Crosby Executive Director [email protected] www.aaompt.org
Articulations is published three times a year.
Advertisers please contact David Miers
(610) 258-5321 [email protected]
for a rate card.
© AAOMPT 2008 All Rights Reserved.
We need your help in keeping our AAOMPT online database record of your membership up to date.
If you would go to: www.aaompt.org and then to the Member Resources Tab, the expanded menu below the tab shows: update Member Information about two-thirds of the way down on that menu. Click on that selection ( www.aaompt.org/registerupdatemembersform.cfm) and it will take you to a screen that asks you to log-in.
Notice that it says “My Profile” above the log-in.
Your log-in, unless you’ve changed it, is your first and last name, and your password is AAOMPT. If you’ve forgot-ten your password, click on “Forget Your Password” and enter your e-mail address for it to be e-mailed to you. Once you’ve logged into your personal profile page, you may change your username or pass-word, but please make a record of it.
Your assistance in keeping that in-
formation current allows us to mail to you your Articulations newsletter, the JMMT, and any other correspondence that is ap-propriate to be mailed. It also allows us to contact you by e-mail and send you Press Releases that you can readily use in your local practices. This it our only method of contacting you on short notice.
Remember that the AAOMPT dues year begins every year on January 1 and ends on December 31. Membership status on your profile indicates whether or not your membership is Active or Inactive within the database. Active members have access to all password protected areas of the site, whereas Inactive members may only make changes to their profile and/or pay dues.
You may make changes to your Main Contact Information in the fields pro-vided on the profile. Not all fields may be changed by you, but you may change criti-cally important information such as your mailing address; phone information and e-mail address.
ing thrust have been an integral part of physical therapists’ scope of practice since the inception of the profession and are taught in Physical Therapist professional education pro-grams. The osteopathic physician listened to our arguments, but wanted to check our claims for him self. His research included contacting a Physical Therapist professional educa-tion program in Illinois; the director of the program, who is a pediatric specialist, was able to explain to the osteopathic physician that manipulation, including thrust, is taught in their program and gave him the website where he could ac-cess the Manipulation Education Manual. The next day the Osteopathic physician called Peter McMenamin to say that he was impressed with the Manipulation Education Manual and was satisfied that physical therapists were being well educated and trained to perform thrust manipulation. The osteopathic society withdrew their support for the legislation, which combined with physical therapists’ lobbying efforts, killed the legislation.
In this case, the education helped to defeat the legisla-tion.”
Ken Olson, 2007 John McMennell Service Award Acceptance Speech. This speech was published with permission from JMMT and can be found on the JMMT website.

22 - Articulations - May/June 2008

May/June 2008 - Articulations - 23
Featured Speakers: David Butler and Steve George
Pain: From Science to Solutions
The 14th Annual Conference of the American Academy of Orthopaedic Manual Physi-cal Therapists will be held October 30 to November 2, 2008, in Seattle, WA.. Interested individuals are invited to submit abstracts of original research for presentation in platform (oral presentation) or poster format. The AAOMPT research committee chairman, H. James Phillips, must receive the abstract via e-mail by June 1, 2008. Abstracts received after this date will be returned. You will be notified of the acceptance/rejection of your abstract in July. If you have any questions call the research committee chairman at (201) 370 7195 or via e-mail at: [email protected]. For additional organization information, check our website, www.aaompt.org.
Content. The Academy is soliciting all avenues of research inquiry from case-report and case-series up to clinical trials. The Academy is particularly interested in research evaluat-ing intervention strategies using randomized-controlled clinical trials. The abstract should include 1) Purpose; 2) Subjects; 3) Method; 4) Analyses; 5) Results; 6) Conclusions; 7) Clinical Relevance.
PubliCation. The accepted abstracts will be published in The Journal of Manual& Manipula-tive Therapy, which has hardcopy readership in over 40 countries, and on-line publication.
SubmiSSion Format. The format for the submitted abstracts is as follows:The abstract must be submitted by email in MS Word format to the research committee chairman ([email protected]). The abstract should fit on one page with a one-inch margin all around. The text should be typed as one continuous paragraph. Type the title of the research in ALL CAPS at the top of the page followed by the authors’ names. Immediately following the names, type the institution, city, and state where the research was done. Please include a current email address where you can be contacted.
PreSentation. The presentation of the accepted research will be in either a slide or poster session, at the discretion of the Research Committee. The slide session will be limited to 10 minutes followed by a 5-minute discussion; this session will be primarily for research reports and randomized clinical trials. The poster session will include a viewing and question answer period and will be primarily for case report/series. PreSentation awardS. The platform and poster presentations deemed of the highest quality of those presented at the annual conference will be awarded the AAOMPT Richard Erhart Ex-cellence in Research Award (platform), and the AAOMPT Outstanding Case Report (poster). The awards include free tuition for the AAOMPT conference the following year.
H. James Phillips, PT, PhD, OCS, ATC, FAAOMPTSeton Hall UniversityS. Orange, NJ [email protected]
AAOMPT 2008CALL FOR ABSTRACTS

24 - Articulations - May/June 2008
hISTORy: Dr. Kaltenborn has been a consummate teacher and leader in OMPT for decades. His worldwide teaching and books on arthrokinematics and specific manipula-tive techniques have profoundly influenced today’s clinicians, teachers, and researchers. He was instrumental in bringing together leaders of the OMPT residency programs in the U.S. to found the AAOMPT. This paved the way for full membership in the Inter-national Federation of Orthopaedic Manipulative Therapists.
PuRPOSE: To award an outstanding instructor in an APTA credentialed clinical fel-lowship in orthopaedic manual physical therapy.
ElIGIBIlITy: Candidates must be nominated by one of their students or former students with 1. a second by another student or former student.Students must be currently enrolled in, or have completed, an APTA creden-2. tialed OMPT Fellowship program.Nominees must be a member of the AAOMPT.3. Members of the AAOMPT Executive Committee are excluded from eligibility 4. during their term in office.
CRITERIA FOR SElECTION:Nominees should have significantly influenced the process of learning and ap-1. plying orthopaedic manual physical therapy principles and techniques to patient care.The quality of the nomination letters, not the number of letters received will as-2. sist in determining the recipient of this award.
PROCEDuRE FOR NOMINATION:Any current or former student of an APTA credentialed OMPT Fellowship pro-1. gram may nominate candidates for the award.All nominations must have a second by another current or former student of an 2. APTA credentialed OMPT Fellowship program.Nominations should be sent via email to Liz Slusarz, Nominating Committee 3. Chairman sluszl@pacbellDeadline for nominations is August 1, 2008.4. Materials to be completed and submitted for each nomination shall include the 5. following:
A support statement from the nominator highlighting the reason for the a. nomination and how the instructor has influenced his or her process of learning and applying orthopaedic manual physical therapy principles and techniques to patient care.A support statement to second the nomination, which should be simi-b. larly detailed while highlighting the above information.Both submissions should include the following information:c.
The instructor’s namei. The program the instructor teaches inii. Contact information for both the nominee and the nominator.iii.
Kaltenborn “Teach I Must” Award
The Award and its Presentation:
The Academy Executive will present the award at the AAOMPT Annual Meeting.
The Academy will award the recipi-ent a full confer-ence registration.
Deadline for nominations is August 1, 2008
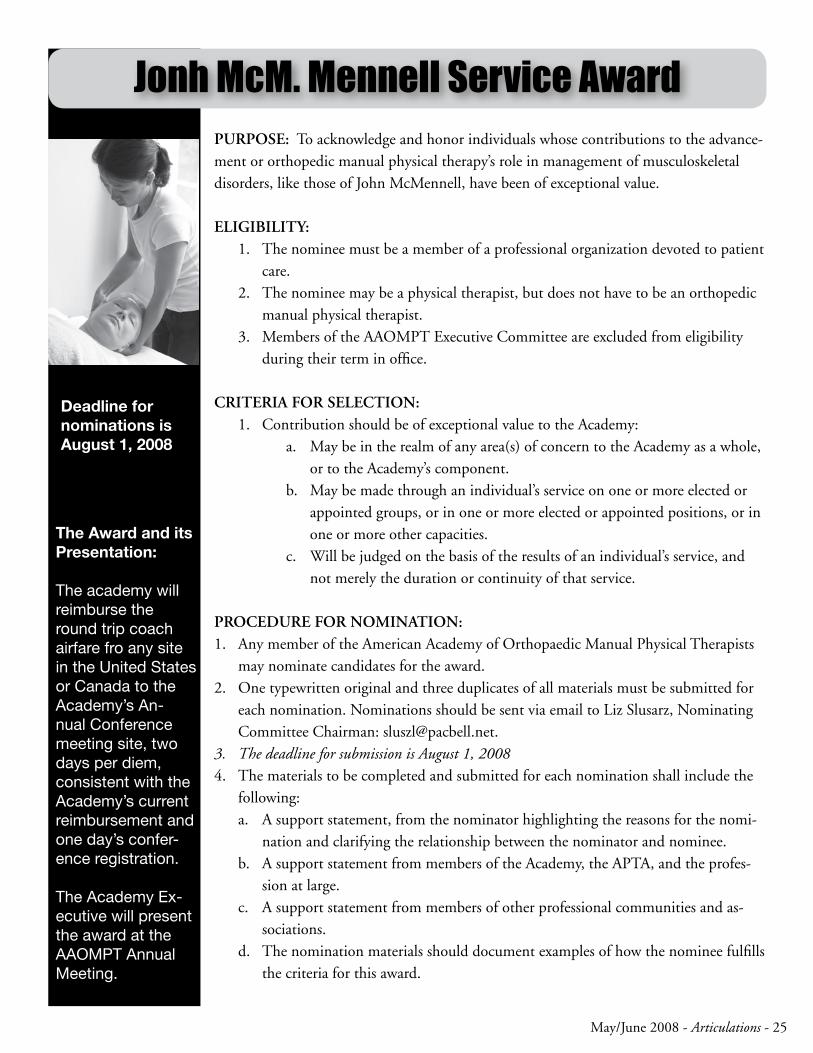
May/June 2008 - Articulations - 25
PurPose: To acknowledge and honor individuals whose contributions to the advance-ment or orthopedic manual physical therapy’s role in management of musculoskeletal disorders, like those of John McMennell, have been of exceptional value.
eligibility:The nominee must be a member of a professional organization devoted to patient 1. care.The nominee may be a physical therapist, but does not have to be an orthopedic 2. manual physical therapist.Members of the AAOMPT Executive Committee are excluded from eligibility 3. during their term in office.
Criteria for seleCtion:Contribution should be of exceptional value to the Academy:1.
May be in the realm of any area(s) of concern to the Academy as a whole, a. or to the Academy’s component.May be made through an individual’s service on one or more elected or b. appointed groups, or in one or more elected or appointed positions, or in one or more other capacities.Will be judged on the basis of the results of an individual’s service, and c. not merely the duration or continuity of that service.
ProCedure for nomination:Any member of the American Academy of Orthopaedic Manual Physical Therapists 1. may nominate candidates for the award.One typewritten original and three duplicates of all materials must be submitted for 2. each nomination. Nominations should be sent via email to Liz Slusarz, Nominating Committee Chairman: [email protected] deadline for submission is August 1, 20083. The materials to be completed and submitted for each nomination shall include the 4. following:
A support statement, from the nominator highlighting the reasons for the nomi-a. nation and clarifying the relationship between the nominator and nominee.A support statement from members of the Academy, the APTA, and the profes-b. sion at large.A support statement from members of other professional communities and as-c. sociations.The nomination materials should document examples of how the nominee fulfills d. the criteria for this award.
Jonh McM. Mennell Service Award
The Award and its Presentation:
The academy will reimburse the round trip coach airfare fro any site in the United States or Canada to the Academy’s An-nual Conference meeting site, two days per diem, consistent with the Academy’s current reimbursement and one day’s confer-ence registration.
The Academy Ex-ecutive will present the award at the AAOMPT Annual Meeting.
Deadline for nominations is August 1, 2008

26 - Articulations - May/June 2008
MEMBER TYPE
AAOMPT MEMBER:Any physical therapist who is a current member or eligible for membership in the American Physical Therapy Asso-ciation.
AAOMPT FELLOW:A fellow is a physical therapist who has been recognized by their peers as having reached the standards of the Academy. There are several ways this can be achieved (ref: AAOMPT Bylaws and Constitution Updated August 2, 1996). A fellow is a full voting member of the Academy.
STUDENT MEMBER:Any full time student enrooled in a graduate or undergraduate physi-cal therapy program who is a current member or eligible for membership in the American Physical Therapy As-sociation. Student members will have a reduced membership fee to be set by the AAOMPT executive.
FOREIGN MEMBER:A physical therapist living and work-ing outside the United States who is interested in supporting the objectives of the Academy.
INSTITUTIONAL MEMBERS:Any educational, research or clinical institution with an interest in orthopae-dic manual physical therapy.
BENEFITS
• Receives the Academy newsletter - Articulations
• A subscription to Journal of Manual and Manipulative Therapy
• Discount for “Standards” document & DACP
• Eligible to apply for fellowship if qualified
• Eligible to chair and serve on com-mittees
• Eligible to serve on Executive as Member-At-Large
• Discounts on Academy sponsored seminars and annual conference
• Receives the Academy newsletter - Articulations
• A subscription to Journal of Manual and Manipulative Therapy
• Discount for “Standards” document & DACP
• Discounts on Academy sponsored seminars and annual conference
• Eligible to serve on Executive Com-mittee
• May use the designation FAAOMPT after their name
• Receives the Academy newsletter - Articulations
• Discounts for Academy sponsored conference
• Receives the Academy newsletter - Articulations
• A subscription to Journal of Manual and Manipulative Therapy
• Receives the Academy newsletter - Articulations
• A subscription to Journal of Manual and Manipulative Therapy
• Free copy of “Standards” document• Discounts for “Standards” docu-
ment & DACP
DUES
$95.00 per year
$125.00 per year plus a one time appli-cation fee ($100.00)
(Associate dues paid in same year are credited towards fellow dues)
$15.00 per year for a basic student membership without journal
$60.00 per year with a subscription to the Journal of Manual & Manipulative Therapy included
North America $105.00 per year
Overseas $115.00 per year
$160.00 per year
AAOMPT MEMBERSHIP BENEFITS
NOTE: Memberships will be on an annual basis and will run from January 1st through December 31st for the year in which the application and full pay-ment of dues are received. Individual memberships and subscriptions will become effective the date on which payment is received and will be retroac-tive. Applications received after September 30th will include membership for the remainder of the calendar year and the following year. However, in order to ensure that new members receive complete volumes, subscriptions will not begin until the fol-lowing calendar year.


2008 AAOMPT NEW MEMBER APPLICATION for licensed U.S. physical therapists
Name:
Address:
Home Phone: Work Phone:
Fax:
E-mail: PT License #
Are you an APTA Member? __Yes __NoAre you an Orthopaedic Section Member? __Yes __NoAre you an OCS? __Yes __No
MEMBERSHIP CATEGORY:AAOMPT Member $95 Institutional Member $160 Recognized Fellowship Programs $160Foreign Members North America $105 Overseas $115 Practice Affairs Fund donation $______ (voluntary contribution) 140 Club $______ ($140 suggested donation) Student Member (w/o journal) $15 (w/journal) $60Student membership good for 1 year post graduation date. Provide graduation date:Name of school:
METHOD OF PAYMENT: (Make checks payable to AAOMPT) Check or money order enclosed Charge my credit card: Visa Mastercard Amount to charge $ Credit Card number Exp. Date
Signature
If you DO NOT wish to have your contact information available for mailing labels or the AAOMPT Directory, please check here ______.
Please return this form with payment to: AAOMPT Headquarters2104 Delta Way, #7 • Tallahassee, FL 32303 • (850) 222-0397 • Fax (850) 222-0342 • [email protected] you are not receiving your Journals, please contact John Medeiros at the Journal of Manual & Manipulative Therapy at (503) 359-2322
2104 Delta Way, #7Tallahassee, FL 32303
PRSRT. STD.U.S. Postage
P A I DTallahassee, FL
Permit #625
JUST A REMINDERPlease notify us when you have a change of address. Journals and newsletters are sent third class and will
not be forwarded by the post office.