Mesangial proliferative GN
31
Mesangial proliferative GN
-
Upload
edwinchowyw -
Category
Health & Medicine
-
view
6.287 -
download
0
description
Renal pathology tutorial for nephrologists
Transcript of Mesangial proliferative GN

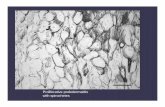
Mesangial proliferative GN

• Mesangioproliferative pattern of glomerular injury is characterized by the expansion of mesangial matrix and the mesangial hypercellularity. These changes can occur in immune complex-mediated diseases, such as IgA nephropathy or class II lupus nephritis or non-immune diseases such as early diabetic glomerulosclerosis, and some forms of minimal change disease and primary focal sclerosis.

Lupus nephritis Class II
• Histopathology: • Mesangioproliferative pattern of glomerular injury;
the mesangium is expanded and hypercellular• The glomerular basement membranes are of
unremarkable thickness and texture• The tubulointerstitium is usually unremarkable
• Immunofluorescence: • There is 'full house' reactivity (reactivity for IgG,
IgM, and IgA), with granular deposits in the mesangium

• Electron microscopy: • Visceral epithelial cells: Unremarkable, and the foot processes
are well preserved. Sometimes a few subepithelial deposits can be found
• Glomerular basement membranes: Usually of normal appearance and texture
• Glomerular endothelial cells: May contain tubuloreticular structures. Rare, small subendothelial electron-dense deposits can be seen scattered in a few places; if large subendothelial deposits are seen, the proliferative forms of lupus nephritis (classes III or IV) should be strongly considered
• Mesangium: Expanded by increase in cellular elements and extracellular matrix with sometimes large and confluent fine granular, electron-dense deposits



IgA• Histopathology: • Light microscopic examination reveals a mesangioproliferative
pattern of glomerular injury (mesangial hypercellularity and expansion of mesangial matrix)
• The glomerular basement membranes are of unremarkable thickness and texture
• The tubulointerstitium is usually unremarkable
• Immunofluorescence: • There is dominant reactivity for IgA in the mesangium; C3 may
be equally or less reactive. There is usually stronger reactivity for lambda then for kappa light chains in the mesangial deposits.

• Electron microscopy: • Visceral epithelial cells: Usually unremarkable, and
the foot processes are well preserved• Glomerular basement membranes: May be thin;
there is a higher incidence of thin glomerular basement membrane disease in IgA nephropathy than in any other glomerular disease {6}
• Glomerular endothelial cells: Usually unremarkable, and tubuloreticular structures are not seen
• Mesangium: Increase in cellularity and extracellular matrix, with fine granular electron-dense deposits that are sometimes large and confluent



Resolving PIGN• Histopathology: • Mesangial hypercellularity and expansion• Neutrophils are not evident, endocapillary
proliferation is not present (or is minimal)• Some of the glomeruli may appear unremarkable• In some cases, inflammatory process does not
resolve and results in glomerular and tubulointerstitial scarring
• Immunofluorescence: • Coarse granular C3 reactivity in the mesangium and
along the capillary loops

• Electron microscopy: • Visceral epithelial cells: There may be focal effacement
of foot processes• Glomerular basement membranes: Subepithelial
deposits may be still present, particularly in areas of mesangial notch, but subendothelial deposits have resolved
• Glomerular endothelial cells: May show non-specific changes; tubuloreticular structures are not seen
• Mesangium: Increase in cellularity and extracellular matrix, with sometimes large and confluent fine granular electron-dense deposits; mesangial deposits are predominant in resolving phase of the disease



Fibrillary GN
• Fibrillary glomerulopathy is characterized by progressive clinical course, variable histologic patterns (most commonly membranoproliferative or mesangioproliferative), with extracellular deposition of Congo red negative material, ultrastructurally consisting of non-branching, randomly arranged microfibrils 12-30 nm in diameter, usually with polyclonal IgG4 immunofluorescence reactivity.

• Etiology: • Unclear etiology; fibrillary GN is only rarely associated with B-
cell neoplasias while the link is stronger in cases of immunotactoid glomerulopathy {1}
• Clinical: • Occurs more commonly in older patients (very rare in children)
and Caucasians• There is usually nephrotic range proteinuria; other presenting
symptoms vary, including nephrotic syndrome, acute renal failure, rapidly progressive nephritis, chronic renal insufficiency
• Outcome may be dependent on histologic pattern of injury {2}

• Histopathology: • Commonly, there is mesangial expansion with increased mononuclear
inflammatory cells and matrix and peripheral capillary loop thickening (MPGN-like pattern of injury); sometimes, the predominant pattern is mesangioproliferative (if the deposition is not involving capillary loops) or even less commonly, membranous, diffuse proliferative, or sclerosing patterns may be seen {2}
• Proliferative changes, such as increased endocapillary proliferation or crescent formation, are uncommon but occur
• Congo red stain is negative• Silver stain may reveal “moth eaten” appearance (non-reactive deposits
admixed with reactive matrix)
• Immunofluorescence: • There is polyclonal deposition of IgG (most often IgG1 or IgG4) and C3 in the
mesangium and along the peripheral capillary loops; in less than 10% of cases, the reactivity will be of monoclonal IgG; in very rare cases there will be no immunoglobulin reactivity.

• Electron microscopy: • Visceral epithelial cells: Focal, sometimes marked
effacement of visceral epithelial cell foot processes• Glomerular basement membranes: Usually marked
thickening of the membranes with extensive fibrillary deposits; the deposition extends to subepithelial, subendothelial, and paramesangial spaces. The fibrils are non-branching, randomly oriented, 12-30 nm in diameter
• Glomerular endothelial cells: Show loss of fenestrations and other non-specific changes; they do not contain tubuloreticular structures
• Mesangium: Usually expanded by matrix and organized fibrillary deposits




Immunotactoid Glomerulopathy• Immunotactoid glomerulopathy is a glomerular
disease characterized by deposition of abnormal proteins (paraproteins) that are Congo red negative by light microscopy and show microtubular or fibrillary substructure by electron microscopy. The microtubules are usually greater than 30 nm in diameter, sometimes with central core, and are arranged parallel to the glomerular basement membranes. There is usually monoclonal immunoglobulin reactivity by immunofluorescence. Clinically, immunotactoid glomerulopathy is strongly associated with B-cell lymphoproliferative disorders.

• Etiology: • Deposition of abnormal monoclonal protein in
patients with paraproteinemia and lymphoproliferative disorder
• Clinical: • Usually occurs in patients over 60 years of age• Usually presents with nephrotic range proteinuria;
other presenting symptoms vary, from nephrotic syndrome, hematuria, acute renal failure, rapidly progressive nephritis, chronic renal insufficiency

• Histopathology: • Commonly, there is mesangial expansion with increased mononuclear
inflammatory cells and matrix and peripheral capillary loop thickening (MPGN-like pattern of injury); rarely, the predominant pattern can be mesangioproliferative (if the deposition is not involving capillary loops) or, even less commonly, predominantly membranous
• Proliferative changes, such as increased endocapillary proliferation or crescent formation, can be seen on rare occasions
• Congo red stain is negative• Silver stain may reveal “moth eaten” appearance (non-reactive
deposits admixed with reactive matrix)
• Immunofluorescence: • Monoclonal (kappa or lambda) reactivity of immunoglobulins (usually
IgG)

• Electron microscopy: • Visceral epithelial cells: Focal, sometimes marked effacement of
visceral epithelial cell foot processes• Glomerular basement membranes: Microtubular deposits,
frequently in parallel arrangements, can be seen in subepithelial and intramembranous locations, extending to the paramesangial and mesangial compartment; the basement membrane can be affected with deposits in various degrees. The fibrils or microtubules are non-branching, usually greater than 30 nm (10-90 nm) in diameter
• Glomerular endothelial cells: Show loss of fenestrations and other non-specific changes; they do not contain tubuloreticular structures
• Mesangium: Usually expanded by matrix and organized microtubular deposits



Early diabetic glomerulosclerosis• Histopathology: • In early diabetic glomerulosclerosis, there is mesangial expansion due to increase in amount
of matrix, with or without mesangial hypercellularity. There are no Kimmelstiel-Wilson nodules at this stage of disease
• Peripheral capillary loops are usually of normal thickness and microaneurysms are not seen in early stages
• Insudative lesions are usually not seen (fibrin cap, capsular drop)• Mild patchy tubular atrophy and interstitial fibrosis and non-specific, predominantly
mononuclear cell inflammatory infiltrate• Various degrees of vascular sclerosis and hyalinosis• In early diabetic change, findings are milder, with mild mesangial sclerosis and mild arteriolar
hyalinosis; glomerular hypertrophy is probably the earliest sign of diabetic renal pathology• Congo red stain is negative
• Immunofluorescence: • Mild linear reactivity for albumin and IgG along the capillary loops; no immune deposits

• Electron microscopy: • Visceral epithelial cells: Focal effacement of visceral
epithelial cell foot processes, in the absence of electron-dense deposits
• Glomerular basement membranes: Usually of normal thickness or slightly thickened
• Glomerular endothelial cells: Various non-specific changes; do not contain tubuloreticular structures
• Mesangium: Normal cell elements and expansion of extracellular matrix in the absence of electron-dense deposits


Minimal Change Disease
• Can have some mesangial hypercellularity

![An epidemiological model for proliferative kidney disease ... · An epidemiological model for proliferative ... [18, 35]. Overt infec-tion ... An epidemiological model for proliferative](https://static.fdocuments.us/doc/165x107/5c00b25409d3f225538b84ad/an-epidemiological-model-for-proliferative-kidney-disease-an-epidemiological.jpg)


![Diabetic Retinopathy (Non Proliferative DR [NPDR] and ......1 of 20 Diabetic Retinopathy (Non Proliferative DR [NPDR] and Proliferative DR [PDR]) TYPE CODE DESCRIPTION Diagnosis: ICD-10-CM](https://static.fdocuments.us/doc/165x107/603395928c16ee65b2116f33/diabetic-retinopathy-non-proliferative-dr-npdr-and-1-of-20-diabetic-retinopathy.jpg)