
MERCY MEDICAL CENTER BUGS N DRUGS MAY 2016
34
MERCY MEDICAL CENTER BUGS-N-DRUGS MAY 2016 Clean your hands often and correctly for you and your patient’s health!!!!!! May 5 is the World Health Organization's World Hand Hygiene Day. Hand hygiene (washing with soap and water or using hand sanitizer) is the most effective way to prevent the spread of infections. Because it is the number one way to stop the spread of germs, it is important to clean your hands often. Remember: CLEAN HANDS COUNT for safe healthcare! When should I wash my hands? Many illnesses can be prevented with regular hand hygiene using soap and water or alcohol-based hand sanitizer. Clean your hands often, and request that others do the same. Before eating Before, during, and after preparing food After using the bathroom After coughing, sneezing, blowing your nose, or caring for someone who is ill After taking out the garbage After petting animals When visiting someone who is sick Whenever your hands look or feel dirty How do I wash my hands correctly? According to the Centers for Disease Control and Prevention: 1. Wet your hands with clean, running water (warm or cold), turn off the tap, and apply soap. 2. Lather your hands by rubbing them together with the soap. Be sure to lather the backs of your hands, between your fingers, and under your nails. 3. Scrub your hands for at least 20 seconds. Need a timer? Hum the “Happy Birthday” song from beginning to end twice. 4. Rinse your hands well under clean, running water. 5. Dry your hands using a clean towel or air dry them, and use a paper towel to turn off the faucet, and then throw it away. HAPPY CINCO DE MAYO AND WORLD HAND HYGIENE DAY
Transcript of MERCY MEDICAL CENTER BUGS N DRUGS MAY 2016

MERCY MEDICAL CENTER BUGS-N-DRUGS MAY 2016
Clean your hands often and correctly for you and your patient’s health!!!!!!
May 5 is the World Health Organization's World Hand Hygiene Day. Hand hygiene (washing with soap and water or using hand sanitizer) is the most effective way to prevent the spread of infections. Because it is the number one way to stop the spread of germs, it is important to clean your hands often. Remember: CLEAN HANDS COUNT for safe healthcare!
When should I wash my hands? Many illnesses can be prevented with regular hand hygiene using soap and water or alcohol-based hand
sanitizer. Clean your hands often, and request that others do the same.
Before eating Before, during, and after preparing food
After using the bathroom After coughing, sneezing, blowing your nose, or caring for someone who is ill After taking out the garbage After petting animals When visiting someone who is sick
Whenever your hands look or feel dirty
How do I wash my hands correctly? According to the Centers for Disease Control and Prevention:
1. Wet your hands with clean, running water (warm or cold), turn off the tap, and apply soap. 2. Lather your hands by rubbing them together with the soap. Be sure to lather the backs of your
hands, between your fingers, and under your nails. 3. Scrub your hands for at least 20 seconds. Need a timer? Hum the “Happy Birthday” song from
beginning to end twice. 4. Rinse your hands well under clean, running water. 5. Dry your hands using a clean towel or air dry them, and use a paper towel to turn off the faucet,
and then throw it away.
HAPPY CINCO DE MAYO AND
WORLD HAND HYGIENE DAY

How do I clean my hands without soap or water? If soap and water are not available, use an alcohol-based hand sanitizer that contains at least 60
percent alcohol. Alcohol-based hand sanitizers can quickly reduce the number of germs on hands in some situations, but sanitizers do not eliminate all types of germs
Apply the product to the palm of one hand. Rub your hands together. Rub the product over all surfaces of your hands and fingers until your hands are dry.
I didn’t see my healthcare provider or visitors wash their hands. Now what? Scary but true: It has been estimated that fewer than half of healthcare workers clean their hands as
often as they are supposed to. Germs on healthcare workers’ hands can transmit dangerous infections to patients. Did you see your healthcare providers or visitors wash their hands? If not, ask politely them to wash again (e.g., “Do you mind cleaning your hands again before the exam?”). Please speak up for
your care. Don’t be shy. After all, we’re talking about your health.

Iowa’s New Candor Law – Improving Physician-Patient Communication
Passed in 2015 by the Iowa Legislature, Candor - Communication and Optimal Resolution – facilitates a confidential conversation between physicians and patients following an unanticipated outcome. OBJECTIVES:
The physician will: 1. Understand the basic components of the Iowa Candor Legislation. 2. Articulate the importance of open and timely communication with patients and
families. 3. Identify barriers and discuss strategy with apology and open communication. 4. Conclude that open and timely communication can preserve a trusting relationship with your patient and enable patients and families to heal. 5. Implement tools, strategies, and best practices for handling apology and communication after an unanticipated
outcome or adverse event.
ACCREDITATION The Cedar Rapids Medical Education Foundation is accredited by the Iowa Medical Society (IMS) to provide continuing medical education for physicians. The Cedar Rapids Medical Education Foundation designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit ™ for each conference attended. Physicians should only claim credit commensurate with their participation in the activity. CONFLICT OF INTEREST DISCLOSURE As a sponsor accredited by the Iowa Medical Society, the Cedar Rapids Medical Education Program must assure balance, independence, objectivity and scientific rigor in all its individually sponsored or jointly sponsored educational activities. All faculty participating in a sponsored activity are expected to disclose to the activity audience any significant financial interest or other relationship (1) with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in an educational presentation and (2) with any commercial supporters of the activity (significant financial interest or other relationship can include such things as grants, or research support, employee, consultant, major stock holder, member of speakers bureau, etc.) The intent of this disclosure is not to prevent a speaker with a significant financial or other relationship from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remains for the audience to determine whether the speaker’s interests or relationship may influence the presentation with regard to exposition or conclusion. Disclosure forms for each presenter are on file in the CME office. DURING PRESENTATIONS THERE ARE OCCASIONALLY DISCUSSIONS OF UNAPPROVED USE OF FDA APPROVED DRUGS, DEVICES OR TREATMENTS. THIS MUST BE DISCLOSED TO THE AUDIENCE DURING THE LECTURE. Attorneys Robert Thompson and Shelly Davis have disclosed that they do not have interest in commercial support.
Candor Training RSVP Form
I Will Attend:
Name Clinic Please Print Please Print
Please fax form to Paramount Health Options at
319-366-5434 or email Sara at [email protected]
Intended Audience: MD’s, DO’s, ARNP’s and PA’s – AMA CME Credit Available
Date: Tuesday May 24, 2016
Time: 5:30—6:30 PM – light appetizers will be served
Where: Hall Perrine Community Rooms A & B
701 10th
St SE, Cedar Rapids, IA 52403
Speakers: Attorneys Robert Thompson and Shelly Davis, both with MMIC
Sponsors: Paramount Health Options and TrueNorth Companies
Announcing the 2016
Michael J. Daly, MD, Humanitarian Award
Dr. Michael J. Daly (1941-2010) was, from the start, destined for adventure. Born in Scotland, Mike was raised in Kenya, completed medical school in Ireland and residency in England. He later practiced in Kenya, England, Dubai and Saudi Arabia. In the mid-1970s, he was a British Red Cross surgeon in Cambodia, where he at once had his heart captured by Elizabeth, the woman who would soon become his wife, and who survives him and mothered their three daughters, and, where he was also captured, with more immediate and more immediately life-threatening consequences, by the Khmer Rouge. Mike’s experiences during this time are depicted in the Oscar-winning film, The Killing Fields, in the guise of Dr. MacEntire. In 1988, Mike made his way to Cedar Rapids, where he practiced as a general surgeon until his retirement in 2007. Along the way, he became a friend to many in greater Cedar Rapids, not just to his fellow physicians and to his own staff, but to nurses, volunteers and, most especially, to patients. During this time, too, Mike was particularly devoted to teaching, with many a Family Medicine resident having had the privilege of working — and learning — at his side, this Program Director among them, me blessed all the more by knowing Mike and his family as friends. To honor Mike, to honor all that he accomplished in his lifetime, to honor all the good that he himself exemplified in the practice of medicine, the Cedar Rapids Family Medicine Residency instituted the Michael J. Daly, MD, Humanitarian Award in 2011, conferring it annually since.

The Award The award, The Thistle, will be presented at the graduation ceremony of the Cedar Rapids Family Medicine Residency in late June.
Purpose To each year recognize a Cedar Rapids community physician who exhibits the kind of courage, compassion and love for life that Dr. Michael Daly himself exemplified. Criteria
• A physician practicing in the Cedar Rapids community, or in the broader community, who also:
o In practice exemplifies the values of Dr. Michael Daly, whether through service to the local population or through volunteerism elsewhere, and, specifically in the areas of professional service and personal sacrifice
o Is committed, overall, to the greater good • Alternatively, a physician who once practiced in the Cedar Rapids community and who
meets the above criteria by prior or current experience
Nominating Process
• Complete and submit the attached nomination form to Dr. Gordon • Feel free to include any other supporting documents, e.g. letters, newspaper articles,
curriculum vitae
Selection Committee Selection will be internal to the residency program, specifically to faculty.
Deadline for Nominations May 15, 2016

Sponsoring Institution: Cedar Rapids Family Medicine Residency Contact: [email protected]

The Michael J. Daly, MD,
Humanitarian Award
Nomination Form Please complete this form and return, with any supporting materials, by Friday, May 20, 2016, to Dr. Gordon’s inbox on his desk or scan and e-mail to [email protected] Nominator: Name ________________________________________________________ Title __________________________________________________________ Nominee: Name ________________________________________________________ Title __________________________________________________________
Supporting Information:
_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Iowa Mission: Lifeline Statewide STEMI Guideline
January 14th, 2016
Over the last year, the Interventional Cardiology Steering Committee of the Iowa Mission: Lifeline Task Force, comprised of interventional cardiologists from each of the PCI Receiving Hospitals and representing statewide coverage for STEMI patients, has been actively involved in an initiative to enhance heart attack care in Iowa. This group has been working together on a statewide ST-Elevation Myocardial Infarction (STEMI) Guideline for use at non-PCI hospitals throughout the state. The intent of creating this guideline is:
1. To develop and promote a standardized, pre-determined course of action for STEMI patients that arrive at non-PCI hospitals, which is already approved by the receiving interventionists, in order to improve STEMI patient outcomes across the state.
2. Ensure all STEMI patients consistently receive the most appropriate care possible, based on time and distance from a PCI capable hospital, and that this care is based on the most recent guidelines set forth by the American College of Cardiology and the American Heart Association.
3. Ensure 12-Lead ECG transmissions from EMS providers in the field are being utilized in the activation of STEMI patient protocols in referring hospitals and PCI Centers, prior to the patient arriving.
During the development process, the guideline was circulated throughout the state to ensure that stakeholders had an opportunity to review the guideline to ask questions and voice concerns. The guideline that is attached is the culmination of this process.
The Mission: Lifeline Emergency Physician Committee was also consulted on the guideline development process and has been very instrumental in the development and collaboration process over the months of effort put forth to develop this guideline.
A statewide guideline is a key step in the development of this statewide STEMI system of care. The Interventional Cardiology Steering Committee of the Iowa Mission: Lifeline Task Force encourages its use by all referring hospitals.
Through data collection at the PCI hospitals, progress toward the outlined goals will be monitored. The Task Force and the Steering Committee will regularly review this data, and nationally recognized standards, for the need to adjust the guideline. With the rollout of this guideline, statewide data will be monitored and evaluated for the following goals:
1. Improved utilization of EMS for signs of a heart attack through public awareness campaigns 2. Reduced First Medical Contact (FMC) to 12-Lead ECG times; 3. Reduced Door to 12-Lead ECG Times in referring and receiving hospitals; 4. Reduction in “door-in to door-out” times of STEMI patients in referring hospitals; 5. Increase in the use of fibrinolytics, when appropriate, for STEMI patients by referring physicians; 6. Reduction in Door to Needle times in referring hospitals administering fibrinolytics for STEMI patients; 7. Reduction of overall First Medical Contact (FMC) to Device times.

The volunteer Task Force of Iowa Mission: Lifeline has worked diligently over the past year to move forward with the implementation of equipment, technology, education and data collection tools throughout the state to improve STEMI patient outcomes.
My signature below signifies that the cardiology group and hospital I am representing, approve of the attached Iowa Statewide STEMI guideline and will support the implementation and adherence to the guideline.
Respectfully Submitted, ______________________________________________ ______________________ Signature Date ______________________________________________ Printed Name ______________________________________________ Cardiology Group ______________________________________________ PCI Center Representation

Iowa Mission: Lifeline
Statewide STEMI Guideline for Non-PCI Hospitals (DRAFT)
STEMI Criteria: • ST elevation at the J point in
o Men: at least 2 contiguous leads of ≥2 mm (0.2 mV) in leads V2–V3 and/or ≥ 1 mm (0.1mV) in other contiguous chest leads or the limb leads.
o Women: ≥1.5 mm (0.15 mV) in leads V2–V3 and/or ≥ 1 mm (0.1mV) in other contiguous chest leads or the limb leads.
• Signs & Symptoms of discomfort suspect for AMI (Acute Myocardial Infarction) or STEMI with a duration >15 minutes <12 hours.
• Although new, or presumably new, LBBB at presentation occurs infrequently and may interfere with ST-elevation analysis, care should be exercised in
not considering this an acute myocardial infarction (MI) in isolation. If in doubt, immediate consult with PCI receiving center is recommended.
• If initial ECG is not diagnostic but suspicion is high for STEMI, obtain serial ECG at 5-10 minute intervals.
Patient Care Priorities Prior to Transport or During Transport
Titrate oxygen (starting at 2L/min) to maintain SpO2 between 90%-94%
Aspirin 324 mg PO chewable
Cardiac Monitor & attach hands-free defibrillator pads
Obtain vital signs and pain scale
NTG 0.4mg SL every 5 min or Nitropaste PRN for chest pain (hold for
SBP < 90)
Analgesia (Morphine sulfate or Fentanyl) IV PRN for pain
Establish Saline Lock #1 large bore needle
Administer one of the following:
Heparin - IV loading dose (70 Units/kg - max 4,000 units)
Optional to Heparin:
Enoxaparin (Lovenox):
Age < 75: 30mg IV plus 1 mg/kg SC (max 100mg)
Age > 75: No bolus. 0.75 mg/kg SC (max 75mg)
Administer one of the following:
Ticagrelor (Brilinta) - 180mg PO or;
Optional to Brillinta:
Clopidogrel (Plavix) 600 mg PO or;
Prasugrel (Effient) 60 mg PO. (Precautions with Prasugrel: Do
not use in patients with active bleeding, history of TIA or stroke,
age > 75 years, body weight less than 60 kg or 132 lbs.)
PRIMARY PCI Pathway – FMC to PCI less than
120 minutes – ACTIVATE CATH LAB
Goal: Door-in to Door-out in < 30 minutes
FIBRINOLYSIS Pathway - FMC to PCI anticipated
to be > 120 min
Goal: Door to Needle < 30 minutes followed by
immediate transfer to PCI hospital
ABSOLUTE CONTRAINDICATIONS FOR FIBRINOLYSIS (TNK) IN STEMI
1. Any prior intracranial hemorrhage
2. Known structural cerebral vascular lesion (e.g., arteriovenous
malformation)
3. Known malignant intracranial neoplasm (primary or metastatic)
4. Ischemic stroke within 3 months EXCEPT acute ischemic stroke
within 3 hours
5. Suspected aortic dissection
6. Active bleeding or bleeding diathesis (excluding menses)
7. Significant closed-head or facial trauma within 3 months
If ECG is transmitted from the field (EMS) and a STEMI is identified, the following should be done prior to patient arrival:
Alert on-call provider if not in-house Notify Receiving PCI Hospital Emergency Dept. Physician
Activate Transferring agency (Air or Ground) If Arrived by EMS, Leave Patient on Ambulance Cot
1st ECG time goal: 10 minutes from patient arrival
RELATIVE CONTRAINDICATIONS FOR FIBRINOLYSIS: (TNK) IN STEMI
1. History of chronic severe, poorly controlled hypertension
2. Severe uncontrolled hypertension on presentation (SBP more
than 180 mm Hg or DBP more than 110 mm Hg)
3. History of prior ischemic stroke more than 3 months, dementia,
or known intracranial pathology not covered in contraindications
4. Traumatic or prolonged CPR (over 10 minutes)
5. Major surgery (within last 3 weeks)
6. Recent internal bleeding (within last 2-4 weeks)
7. Noncompressible vascular punctures
8. For streptokinase/anistreplase: prior exposure (more than 5 days
ago) or prior allergic reaction to these agents
9. Pregnancy
10. Active peptic ulcer
11. Current use of oral anticoagulants (Warfarin, Dabigatran,
Rivaroxaban, Apixaban, etc.)
If Patient is contraindicated for Fibrinolysis,
Follow Transport Guidelines for Primary PCI

Patient Care when time allows — Do Not Delay Transport
� Establish large bore IV with NS @TKO, left arm preferred
� Atorvastatin (Lipitor) 80 mg PO
� Obtain Labs: cardiac markers (CKMB, Trop I), CBC, BMP, PT/INR, PTT,
and pregnancy serum if childbearing age (do not delay transport
waiting for results)
� NTG 0.4mg SL every 5 min or Nitropaste PRN for chest pain (hold for
SBP < 90)
� Analgesia (Morphine sulfate or Fentanyl) IV PRN for pain
� Consider Metoprolol (Lopressor) 50 mg PO if patient hypertensive
(>160/90). May consider additional doses if clinically indicated. Hold if
SBP < 120, Pulse ox < 92%, HR < 60 or active CHF or Asthma
Goal: Door-in to Door-out in < 30 minutes
Immediately Transport to PCI Hospital
Tenecteplase (TNKase) IV over 5 seconds:
Patient age ≤75 – FULL DOSE
Patient age >75 – Contact Cardiologist for Consideration of HALF DOSE
Titrate oxygen (starting at 2L/min) to maintain SpO2 between 90%-94%
Aspirin 324 mg PO chewable times 1 dose (if not already given)
Clopidogrel (Plavix)
age ≤75 300 mg loading dose
age >75 only 75 mg total
Repeat EKG 30 minutes after fibrinolytics administration if possible
Immediately Transport to PCI Hospital
Do not give Fibrinolytics (TNKase, rPA, or TPA) for Primary
PCI Patients
Unfractionated Heparin (UFH):
• Heparin IV Bolus (60 Units/kg, max 4,000 Units)
• Heparin IV Drip (12 Units/kg/hr, max 1,000 Units/hr)
Optional to Heparin:
Enoxaparin (Lovenox):
Age < 75: 30mg IV plus 1 mg/kg SC (max 100mg)
Age > 75: No bolus. 0.75 mg/kg SC (max 75mg)
http://www.heart.org/missionlifelinenia
PRIMARY PCI Pathway – FMC to PCI less than
120 minutes – ACTIVATE CATH LAB (continued)
Goal: Door-in to Door-out in < 30 minutes
FIBRINOLYSIS Pathway - FMC to PCI anticipated
to be > 120 min (continued)
Goal: Door to Needle < 30 minutes
List and contact info for Primary PCI Hospitals:
Methodist Jennie Edmundson – Council Bluffs 1-844-536-6431
CHI Health Mercy Hospital – Council Bluffs
UnityPoint St. Luke’s Hospital – Sioux City 712-635-2022
Mercy Medical Center – Sioux City 712-279-2222
Trinity Regional Medical Center – Ft. Dodge 515-574-6684
Central Iowa Healthcare – Marshalltown 641-754-5040
Mary Greeley Medical Center – Ames 515-239-2251
Mercy Medical Center – Des Moines 877-886-3729
Mercy West Lakes – West Des Moines 877-886-3729
UnityPoint Iowa Methodist – Des Moines 800-806-1787
UnityPoint Iowa Lutheran – Des Moines 800-806-1787
Ottumwa Regional Health Center – Ottumwa
University of Iowa Hospitals & Clinics – Iowa City 319-467-6666
Mercy Hospital – Iowa City 319-688-7874
UnityPoint St. Luke’s Hospital – Cedar Rapids 888-369-7105
Mercy Medical Center – Cedar Rapids
Covenant Medical Center – Waterloo 319-272-4327
UnityPoint Allen Hospital – Waterloo 319-235-3697
Mercy Medical Center North – Mason City 877-422-7162
Great River Medical Center – West Burlington 319-768-4700
Genesis Medical Center – Davenport 563-421-7681
UnityPoint Trinity Regional Health System – Bettendorf
Mercy Medical Center – Clinton 563-244-3641
UnityPoint Finley Hospital – Dubuque 563-589-2560
Mercy Medical Center – Dubuque

Laboratory tests are often affected by the quality of the specimen received. The is-sues that cause testing inter-ference differ by test and in-strument methodology. For chemistry and immunochem-istry tests, hemolysis, icterus, and lipemia are the most com-
mon interferences.
Hemolysis is the destruction of red blood cells. Most often this occurs in vitro as a result of specimen collection or pro-cessing, but it can occur in vivo as the result of a disease process. When samples are hemolyzed, the contents of the RBCs are released in the plasma, causing falsely high levels of analytes like potassi-um and LDH. The red color seen in the plasma of hemo-lyzed specimens can also cause interference with spec-trophotometric tests. Com-mon causes of in vitro hemol-ysis are: using a too small or too large bore needle, pulling back on the syringe with too much force, transferring blood from a syringe to tube with force instead of allowing the vacuum to transfer, and vigor-ous shaking of tubes instead
of gentle inversion.
Icterus in patient samples is caused by high levels of biliru-bin in the patient’s plasma. While nothing can be done to prevent this, it can interfere with some laboratory test re-sults. Affected results will have a comment placed on
the report as applicable.
Lipemia is increased plasma turbidity caused by high levels of lipoproteins, most notably chylomicrons. Lipemia can interfere with some tests. There is typically no way to prevent lipemia during speci-men collection since it is an in vivo phenomenon. The La-boratory has technology to separate the lipoproteins from the plasma to minimize inter-
ference.
Hemolysis is the most com-mon specimen integrity issue, the only one that can be con-trolled, and it interferes with the most tests. It is one of the most common causes of
specimen rejection.
Previously, hemolysis was judged visually, which led to inconsistency between staff
members and variable speci-men rejection. Because he-molysis levels affect each test differently, it was impossible to customize rejection criteria
for every test.
Mercy Lab has recently imple-mented objective measure-ment of hemolysis, icterus, and lipemia (HIL) indices for chemistry and immunochem-istry tests. Each test has been customized to provide our scientific staff warnings about specimen interference and corrective action only at a level that is clinically signifi-
cant.
An example HIL results from the chemis-
try analyzer
For more information about HIL indices, please contact Mike Smith, MBL, MLS(ASCP), Core Lab Manager at 398-6132 or [email protected] For more information about how to prevent specimen integrity is-sues, contact Stacey Mohr, MLT(ASCP), Pre-Analytical Lab Man-ager, at 398-6833 or
Visit our website at:
http://
www.mercycare.org/
services/laboratory/
Main Lab Phone
398-6001
Lab Fax 398-6004
Stacey Mohr, Pre
-Analytical Mgr.
398-6833 (o)
480-4367 (c)
Microbiology 398-6834
Transfusion
Services
398-6840
Pathology 398-6003
Sarah Dricken,
Director
398-6008 (o)
899-1592 (c)
Mercy Medical
Center Lab Contacts:
Sample Quality Measurement for Chemistry Tests
Lab Notes April 2016

Entresto (sacubitril/valsartan), a ther-apeutic heart failure medication, may cause interference with BNP meas-urement. Entresto contains a nepri-lysin inhibitor, which causes BNP to rise. The use of serial monitoring of BNP for risk assessment and thera-peutic monitoring will be affected by this drug.
The recommended alternative is the use of pro-BNP to monitor patients on Entresto therapy.
Pro-BNP can be ordered in Epic as a miscellaneous test (LAB147040) and will be sent to Mayo.
For questions, please contact Mike Smith, MBL, MLS(ASCP) at [email protected] or 398-6132.
A new OB Panel option is available—
the Obstetric Panel with HIV
(LAB153788). This panel includes
CBC with differential, Hepatitis B
Surface Antigen, HIV Ag/Ab, RPR,
Rubella IgG Antibody, and a Type and
Screen.
This panel was created in response to
CPT coding changes effective in 2016.
The previous OB panel is still in use
and includes all of the above except
the HIV Ag/Ab.
Please join us in celebrating Medical Labor-
atory Professionals Week April 24-30, 2016!
Thank you to the phlebotomists, lab assis-
tants, medical laboratory scientists, medical
laboratory technicians, histologists, cytolo-
gists, transcriptionists, pathologist assis-
tants, and pathologists that make quality
laboratory testing possible every day!
Entresto and BNP Interference New OB Panel
Medical Laboratory Professionals Week 2016!
Zoster Virus, and Cryptococcus neofor-mans/gattii. Testing will be available 24/7. A formal announcement will be made when the test is available.
This test joins other rapid molecular of-ferings, including the Respiratory Panel by PCR, Stool Pathogens by PCR, and the Blood Culture Microarray. MMC Lab is committed to offering rapid diagnos-
tics to support faster diagnosis and treat-ment by clinicians at the bedside. For more information on our rapid molecu-lar menu, contact Joe Janutka, MS, MLS(ASCP), Microbiology Supervisor at [email protected] or at 861-7701.
Coming Soon...Meningitis/Encephalitis Rapid Molecular Panel
Page 2 Lab Notes
The MMC Microbiology Lab is in the pro-cess of validating a new rapid molecular panel for meningitis/encephalitis. This assay tests for 14 bacterial, viral, and fungal targets in cerebrospinal fluid. Targets include: E. coli K1, Haemophilus influenzae , Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiae, Streptococcus pneumoniae, CMV, Enterovirus, Herpes Simplex Virus 1, Herpes Simplex Virus 2, Human herpes-virus 6, Human Parechovirus, Varicella

Collection of Quality Specimens for Microbiology Testing
High quality Laboratory test results depend on properly collected specimens.
This is especially true in Microbiology, where the pathogenic organism can-
not be identified if it is not collected and transported optimally and/or con-
taminating organisms obscure the causative organism.
General Guidelines for Specimen Collection
1. Collect the specimen from the actual site of infection, avoiding contamination from adjacent tissues.
2. Swabs are generally the least effective collection method. Collection is often representative of surface or normal
flora rather than the causative agent and can represent colonization rather than infection. The small volume of
specimen provided and the poor release of organisms from the swab make recovery less than optimal.
3. Use appropriate collection devices: sterile, leak-proof specimen containers. Use appropriate transport media
when indicated. Check expiration dates prior to collecting the specimen.
4. If appropriate, decontaminate the skin surface prior to collection. Allow the appropriate contact time (generally,
at least 2 minutes) to maximize the antiseptic effect.
5. For specimens with more than one test order, ensure that the proper transport is utilized and all specimens are
labeled correctly. Please ensure that all orders on the specimen have been placed and collection documented be-
fore sending the specimen to the Lab.
Specific Site Information:
Abscesses
1. Decontaminate the surface.
2. Collect purulent material aseptically from an undrained abscess using a sterile needle and syringe.
3. Transfer 5-10 mL of the aspirated material to an anaerobic transport vial and send to the Lab immediately.
4. Swabs are a poor choice because they dry easily and because of the limited amount of material obtained. Swabs
are not optimal for fungal culture, anaerobic culture, or decubitus ulcers. Procurement of tissue aseptically from
the site of infection is recommended. Swabs are not acceptable for mycobacterial cultures, perirectal abscesses,
or oral abscesses.
Body Fluids
1. Body fluids include: pleural, peritoneal, pericardial, and synovial. CSF is its own entity.
2. Fluid aspiration rather than swab collection will increase the probability of identifying the causative organism.
3. Provide adequate fluid for culture (at least 5-10 mL)
4. Fluid should be transported in a sterile container, not in culturettes.
Cellulitis
Swabs and leading edge aspirates with or without injection of saline fail to yield etiologic agents in the majority of cas-
es. If an unusual organism is suspected, a leading edge (advancing margin) punch biopsy is the recommended speci-
men of choice. Place biopsy in sterile container with small volume of non-bacteriostatic saline.

Tissue
1. Collect tissue aseptically. Include material from both the center and the edge of the lesion.
2. Place the specimen in a sterile container on sterile gauze moistened with non-bacteriostatic saline.
3. Do not submit tissue in formalin.
4. Transport to the Laboratory as soon as possible after collection.
5. Do not jam the tissue into a culturette using the swab; this is not an acceptable transport device.
Wounds
1. For closed wounds, refer to Abscess and Cellulitis.
2. For open wounds:
1. Clean the sinus tract opening of the wound surface mechanically, without using a germicidal agent, to
remove as much of the superficial flora as possible.
2. Attempt to culture the base or edges of the wound to avoid collecting normal flora organisms.
3. The following are preferred specimens for sinus tracts:
A. Aspiration of material obtained by needle or catheterization.
B. Curettings from the lining of the sinus tract.
4. Swabs of the sinus tracts are acceptable only if the above cannot be obtained. Swabs of the sinus tracts
may not accurately reflect the underlying disease process.
5. Do not submit cultures of superficial lesions for anaerobic culture. Biopsy of advancing margin of the
wound is the preferred specimen for anaerobes, mycobacteria, and fungi.
Culture ordering in Epic can be challenging. The Microbiology is happy to assist you in ordering the correct test(s) -
please call them at x. 6834 for assistance.
Adapted from Johns Hopkins Medical Microbiology Specimen Collection Guidelines

P a g e | 1
Medication Management Committee Mercy Medical Center Cedar Rapids, Iowa
Volume 24 March 2016
Formulary Deletion Razadyne (Galantamine)
Policies/Protocols -Potassium Replacement Protocol revision (tentative go-live April 11th) -Hazardous Medication Policy revision -Medication Waste Disposal Policy
Therapeutic Interchanges Medication Ordered
Interchanged To
Aclidinium (Tudorza) 1 inhalation BID
Tiotropium (Spiriva) 1 inhalation daily
Membership Fadi Yacoub, Chair Vincent Reid, MD Susan Schima, MD Chris Walsh, MD Asma Al-Zougbi, MD Usha Renganathan, MD Martin Cearras, MD Mary Brobst Lauren Cumings Sarah Schloss, ARNP Stephanie Hoenig, ARNP
Jamie Sinclair
Becky Prier Ariel Loring Lisa Ridge Jen Goings Linda Klein Megan Standish Kathy Swift Andrea Bennett Nadiya Baumhover
I N S I D E T H I S I S S U E
Formulary Deletions
Formula Interchanges
Policy Approvals
|

Memory Disorders Clinic
Laurence Krain, MD, PCI Neurology and Sleep Medicine is the Medical Director of Mercy’s Memory Disorders Clinic. Dr Krain provides care for patients on their initial visits. Joni Henderson, ARNP, Mercy’s Memory Disorders Clinic provides care for patients on their follow up visits.
The Memory Clinic evaluates and treats patients exhibiting signs of dementia, Alzheimer’s disease, and other degenerative brain disorders.
This clinic's goal is to help patients and their families compensate for cognitive and behavior changes, allowing persons with memory disorders to stay in their homes as long as possible.
Physician referral is needed.
If you have questions please call (319) 398-6435.

701 10th Street SE Cedar Rapids, IA 52403-1292 (319) 398-6011
PHYSICIAN MEMO
DATE: March 28, 2016
FROM: Mercy Pediatric Inpatient Center
SUBJECT: Mercy Expands Advanced Pediatric Outpatient Services Mercy Medical Center’s Pediatric Inpatient Center has expanded its offerings to include advanced outpatient services in its hospital-based setting. The new services are considered part of Mercy’s Pediatric Treatment Center, which is simply the designation for the outpatient services that take place within the current Pediatric Inpatient Center, located on Level 8 of the hospital. Services offered include:
• Blood pressure checks • Blood transfusions • Cardioversion – chemical or electric • Injectable antibiotics • Intravenous infusions per treatment protocols for migraine, rheumatoid arthritis,
ulcerative colitis, etc. • Migraine treatments • Mild sedation for procedures • Port access and lab draws • Rabies series • Urology services • Wound care (dressing changes, packing, etc.)
To make a referral in Epic, select “Ambulatory Referral to Pediatric Treatment Center.” For more information or to make a referral by phone, please contact the Pediatric Inpatient Center at (319) 398-6551.

Page 1 of 3
Potassium Replacement Protocol Edits:
Situation: • Beginning Monday April 11th, a revised Potassium Replacement Protocol will be LIVE.
Background: • Feedback was received from nursing that the current Potassium Replacement Protocol was confusing. • An EPIC report was utilized to identify stakeholders and the main location this protocol is used in is ICC and SIC. The main
providers who utilize this are Hospitalists, Intensivists and General Surgeons.
Assessment: 1. The current protocol is missing information which was included in the old paper version of the protocol. This missing text
was reviewed by pharmacy and determined to still be current. This text was added as purple informational text to the top of the protocol:
o Exclusion criteria added:
o Instructions for how to utilize the protocol added:
o Instructions for pain/irritation at the site of administration added:
March 2016 - Approved by Clinical Readiness, Medical Director Council and Medication Management

Page 2 of 3
2. The current nursing communication order within the protocol is confusing:
o Current order:
o Revised order. This now includes text reminding nursing the protocol expires in 48 hours:
3. An order for telemetry if potassium is less than 3 mEq/L is missing so we added the following order:
4. The medication orders from the protocol do not include verbiage stating they are from the protocol. They also do not have a
reminder for when to repeat the potassium lab: o Current med order example:
March 2016 - Approved by Clinical Readiness, Medical Director Council and Medication Management

Page 3 of 3
o Revised med order example:
5. A lab order is in each section of the protocol, but the provider or RN has to remember to select it:
o Current lab orders:
o Revised lab section. We have pulled the labs out of the med section and created a required lab section:
Recommendations:
• Be aware of the changes beginning April 11th. • Pharmacy, ICC Shift Supervisors and SIC Shift Supervisors have reviewed and approved the edits. • Dr. Yacoub, Dr. Cearras, Dr. Baustian and Dr. Royer have provided feedback and their suggestions are reflected in the above
screen shots.
March 2016 - Approved by Clinical Readiness, Medical Director Council and Medication Management

Revised by: S. Hite, RN Date Revised: 4/8/2016
Potassium Replacement Protocol (Order Set)
Potassium replacement protocol is ordered via a provider and is good for 48 hours from the time the order
is entered. This protocol allows nursing staff to reorder potassium replacement based on lab levels that are
drawn at specific intervals. Once 48 hours has lapsed nursing staff would be required to contact the
provider for further orders.
Follow The Steps Below:
Provider established that Potassium replacement is needed
1. Click on Orders Activity
2. Click Go to Order Sets
3. Enter Potassium Replacement
4. Open Order Set:
a. Purple Text is to guide the proper use of this order set
b. General Nursing Interventions are defaulted
c. Medication is ordered based on the level. NOTE some levels indicate both PO and IV to be
ordered. Review Purple text for details.

Revised by: S. Hite, RN Date Revised: 4/8/2016
d. Repeat Lab is ordered based on the current level as was the medication. NOTE: the defaulted
date and time of the lab will need to be reviewed and modified to the appropriate time lab
should be drawn. To evaluate lab is to be drawn; review the details of the medication you
have selected to see the Frequency and indicated # of doses to be given. ** If the
replacement med is delayed for any reason this order may need to be modified again.
Example This will demonstrate a K+ lab of 2.6 :
1. Select the Medication for the appropriate K+ Level:
2. Select Lab, modify the time in the order composer. To determine the time lab should be drawn
review the following details from the example above:
a. Last PO dose given @ 1200, so 2 hours after would be 1400
b. Last IV dose given @ 1000 w/ 1 hour infusion, so 2 hours after is 1300
Defaulted time needs to be modified based on the med order above!
Revised by: S. Hite, RN Date Revised: 4/8/2016 © 2012 Epic Systems Corporation.
Confidential.
c. Lab should be ordered to be drawn @ 1400 according to the last dose of potassium given.
3. Sign
4. Give meds according to MAR schedule
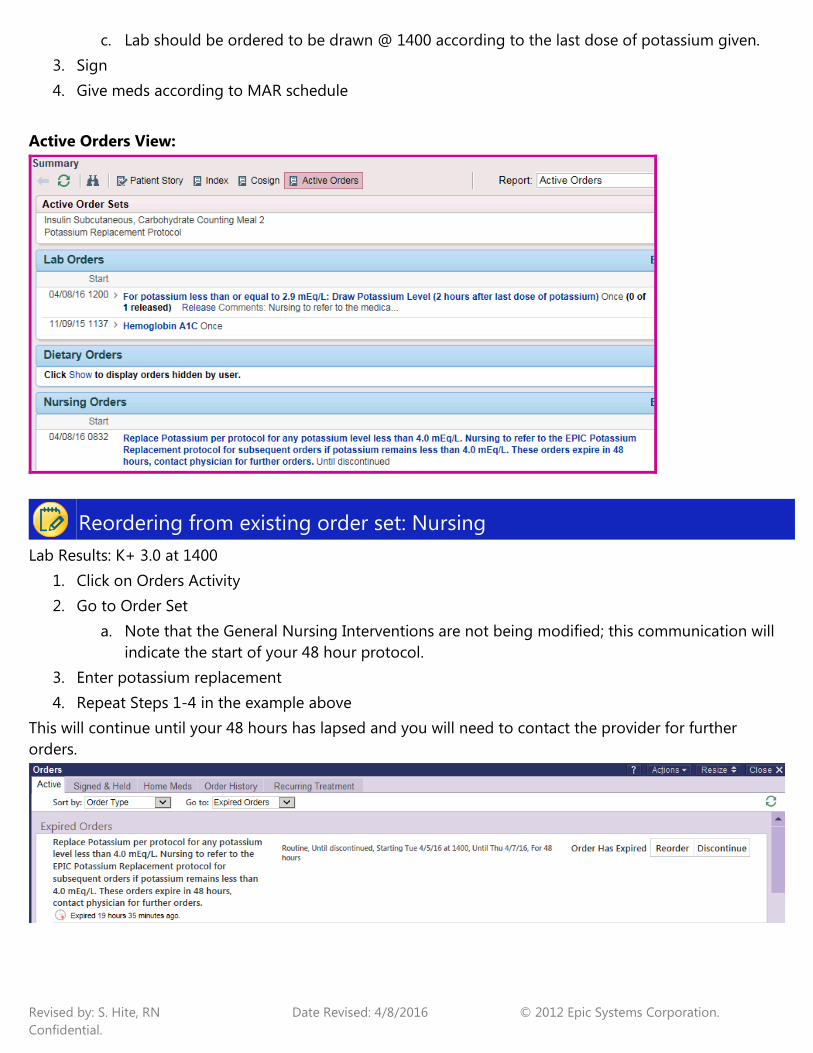
Active Orders View:
Reordering from existing order set: Nursing
Lab Results: K+ 3.0 at 1400
1. Click on Orders Activity
2. Go to Order Set
a. Note that the General Nursing Interventions are not being modified; this communication will
indicate the start of your 48 hour protocol.
3. Enter potassium replacement
4. Repeat Steps 1-4 in the example above
This will continue until your 48 hours has lapsed and you will need to contact the provider for further
orders.

Page 1 of 2
Heparin Nomogram Edits: Situation:
• Questions have arisen regarding the lab nursing communication orders in the Heparin Nomograms and the max dose on the infusion. Background:
• Nursing reported that providers are sometimes changing the therapeutic range in the administration instructions of the Heparin orders. • If the administration instructions are edited, it does not update the nursing communication orders; therefore, the orders are conflicting. • If the adjustment based on the nomogram would result in a dose greater than 2,000 units/hr, the rate is not always capped at the max
dose ordered. Assessment:
• There are two nursing communication orders in the Heparin Nomograms regarding the frequency of the PTT labs based on the therapeutic range. It lists the therapeutic range as 48-65.
• If the provider changes the therapeutic range in the administration instructions, the therapeutic range in the nursing communication
orders do not update. The orders are then conflicting. Recommendation:
• Remove the numbers from the nursing communication orders. The therapeutic range is listed in the administration instructions of the Heparin orders, so it is not necessary to repeat it in the nursing communication orders.
• Screen shot of the Heparin order which lists the therapeutic range in the admin. instructions:
March 2016 – Approved by Pharmacy, Medication Management and Clinical Readiness

Page 2 of 2
• Increase the max infusion rate to 3,000 units/hr and add admin. instructions to the Heparin orders “Maximum infusion rate is 3,000 units/hr. If the suggested action would result in a dose over 3,000 units/hr, contact provider”.
• Contact Pharmacy with questions at 398-6811.
March 2016 – Approved by Pharmacy, Medication Management and Clinical Readiness

Page 1 of 3
VTE Prophylaxis Edits in Order Sets: Situation:
• Beginning April 11th several VTE Prophylaxis edits will be LIVE in order sets.
Background: • The Medication Management Committee and Pharmacy recommended
edits best on current best practice.
Assessment: • Order sets were analyzed and the VTE Prophylaxis sections were edited to
reflect the requests. Recommendations:
• See attached screen shots of the edits. • Contact Pharmacy with any questions at 398-6811.

Page 2 of 3
VTE Prophylaxis edits:
1. If Lovenox or Heparin are selected, the CBC has been updated to a frequency of “every other day” instead of “every third day” to reflect the newest guidelines from the Medication Management Committee:
2. If Coumadin is selected, there is now a “Coumadin Placeholder” order to signify current
Coumadin therapy as a reminder to ensure Coumadin and labs are ordered at DC. There is also now an option to select “Pharmacy to dose warfarin”:

Page 3 of 3
3. A common reason for no Pharmacologic Prophylaxis is “Patient is on therapeutic
anticoagulation”. This is now its own option in this section so it is easier to select if applicable.

Mercy Medical Center CONSENT FOR BLOOD / BLOOD COMPONENT TRANSFUSION
Instructions: For Inpatients − one consent needed per admission.
*Note − Patients do not need to sign this separate Blood Transfusion Consent if they have already signed the Acknowledgement of Information and Special Consent to Operation or Other Procedure. For outpatients − one consent needed per year.
I have authorized Dr. and/or such assistants as may be selected and supervised to transfuse blood / blood components.
The following has been discussed with me:
• The need for transfusion and its potential benefits • The risks of transfusion, including disease transmission, transfusion reaction, and fluid overload • The alternatives to transfusion to include: no treatment, intravenous (IV) fluid, oxygen, iron therapy, etc.
I understand that I have the right to refuse.
I understand the risks, benefits, and alternatives involved in receiving a blood / blood component transfusion. All of my questions have been answered to my satisfaction. Please check one box, then sign and date below.
� I CONSENT to receiving the transfusion services described above. � I REFUSE to consent, and knowingly decline to receive the transfusion services described above.
Signature of Patient / Legal Representative Relationship if not the Patient
Witness to Signature of Patient / Legal Representative
Date and Time
Approval & Date: Medical Executive Committee 01/04/2011 999−50079 03/11
J−2 CONSENT FOR BLOOD / BLOOD COMPONENT
TRANSFUSION
, U#:

Produced by Eastern Iowa Sleep Center A Partnership: UnityPoint-St.Luke’s • Mercy Medical Center • Physicians’ Clinic of Iowa
The Provider’s CornerOSA Treatment has a major impact on comorbidities Per an American Academy of Sleep Medicine survey after one year of OSA treatment: Hypertension – 41% report BP improvement, 17% report decrease in medication. Diabetes – 31% report improved HbA1c. Asthma and breathing conditions – 70% of patients reported symptoms as mild.
Depression, anxiety & mental health – 49% report improvement in mental health. Heart disease – 56% reported their risk of heart disease had declined. Lowering patients’ risk for stroke, heart attack, diabetes, depression, lung disease, hypertension via OSA treatment is making a difference. Overall patients reported good improvement in sleep quality. Great results! For more results see page 3 for the EISC Report 2015.
The EISC Belle Plaine location has been added to the Referral Order form. Providers will be able to check a box indicating EISC Cedar Rapids or EISC Belle Plaine. If neither is marked the Cedar Rapids location will be considered the default location. The Referral Order form is located on our website at eiSleep.com/forms
URGENT need for a patient’s study? Remember, we often have people that need to cancel and reschedule their study for various reasons. Patients waiting for an earlier study date are placed on the Call List and are contacted to fill these spots. Factors that may slow down getting patients in quickly include but are not limited to: insurance pre-authorization, the patient’s personal schedule, the patient’s transportation.
Eastern Iowa Sleep Center in Belle Plaine, Iowa!
In this issueProvider’s Corner: OSA Treatment Impact
Hot Topic: Drowsy Driving
What’s New: EISC Report, Surgery Pre-Op, SDB Impact
What’s Coming: Better Sleep Month & RMC Sleep Lab
EISC Core Values To our patients, their families, and partners, we are committed to uphold the following values:
• Service that is unparalleled
• Listening and creating individualized treatment
• Excellence in quality, professional care
• Efficient and welcoming, with easy access
• Patient-centered, innovative & compassionate care
Eastern Iowa Sleep Center600 7th St. SE, 2nd floorCedar Rapids, IA 52401Phone: 319-362-4433 / 877-361-4433 Fax: 319-362-4466 Office hours: 8am-4:30pm
1010 8th Ave.Belle Plaine, IA 52208Operation hours: 5:30pm-7:00am
eiSleep.com
EISC is excited to be open for service in Benton County and its surrounding areas starting as of March 10, 2016. EISC provides sleep study services at 1010 8th Ave in Belle Plaine, Iowa in addition to its current location in Cedar Rapids. Sleep concerns are increasing
among providers and patients as awareness of the possible health implications increase. EISC – on the move in 2016! Visit eiSleep.com
MAY 2016 VOLUME 5 • ISSUE 1

Oral ApplianceEISC provides oral appliance titration sleep studies for dental professionals who have advanced training in dental sleep medicine. EISC works with a number of dentist in the area that are members of the American Academy of Dental Sleep Medicine. Patients are referred for oral appliance therapy only after a sleep study establishes a diagnosis of OSA by a healthcare provider.
Inspire ImplantsEISC is now trained to provide implant titration sleep studies for the fully implanted Inspire Therapy. Inspire Therapy is a small implanted system that senses breathing patterns and delivers mild stimulation to key airway muscles which keeps the airway open during sleep. This option has a limited patient profile. Questions? Contact the PCI Sleep Medicine line at 319-247-3240.
Home Sleep Test vs In-LabThe American Academy of Sleep Medicine recommends the Home Sleep Test to be used for the diagnosis of Obstructive Sleep Apnea (OSA) ONLY. No other co- morbid conditions may be present.
EISC offers one-to-one patient education when your patient is referred here. This improves the study results and reduces the anxiety of patients. EISC also offers Sleep Technician support during the patients sleep time. Questions? Visit eiSleep.com/contact
Eastern Iowa Sleep Center, represented by Lisa Gleason, Administrative Director, attended the Sleep Health & Safety Conference hosted by the National Sleep Foundation (NSF) in Washington D.C. on November 6th. The event coincided with the NSF’s Drowsy Driving Prevention Week, November 1-8, 2015.
Mark R. Rosekind, Ph.D., Administrator, National Highway Traffic Safety Administration (NHTSA) was the keynote speaker. Other speakers included leaders from Exxon Mobile Corp, National Transportation Safety Board (NTSB), Walter Reed Army Institute of Research, Volvo, Ford Motor, and Vehicle Design Technologies among others. The auto manufacturers are rapidly incorporating technology to reduce drowsy driving accidents. Collaboration between all national, state and local leaders was an emphases.
Top 3 preventable causes of fatal motor vehicle crashes in the U.S. are:
• Drunk Driving at 10,800 deaths annually
• Drowsy Driving at 6,800 deaths annually
• Distracted Driving at 5,500 deaths annually
Statistics included 56 million drivers admit driving drowsy monthly, 1/3 fatal-to-driver truck crashes are fatigue-related, 50,000 drowsy driving debilitating injuries each year and 6,800 drowsy driving fatalities each year.
Risk factors included time of day, number of hours awake, sleep deficiency, sleep quality, age and medication/drug use. Peak drowsy driving danger times include 5am-8am and 3pm-5pm. Truck accidents high peak time is between 3am-7am since truckers mainly drive at night due to lack of roadway space during the day.
Crash Risk is higher for drivers with Obstructive Sleep Apnea (OSA) as opposed to those who are able to obtain better quality sleep by using CPAP treatment. Studies show regarding age, an adverse effect of sleep deprivation on reaction time is much greater in young adults making them at higher risk for crashes.
SleepSmartz
Hot Topic:Drowsy Driving
MARK ROSEKIND (NHTSA)

Thank you to all the healthcare providers that have joined the effort to identify patients with Sleep Disorder Breathing (SDB). See below the EISC Report 2015 stats for your consideration.• Patients sent for a sleep study to
determine OSA – here’s the results:- Mild (AHI 5-14) – 28% - Moderate (AHI 15-30) – 25%- Severe (AHI >31) – 20%- Normal (AHI <5) – 27% of which
patients had other sleep issues such as inadequate sleep hygiene, insomnia or RLS/PLMS
• Ages served – 1.5 year old to age 95• Gender served – 53% men/47% women• Patients were identified by the
following providers: Family Medicine/Internist 59%, Sleep Medicine 20%, Pulmonology 12%, Cardiology 6% and ENT 3%
Pre-Procedure OptimizationThe Face to Face office visit documenta-tion and pre-authorization are the keys to coordinating the patient’s sleep study and treatment. How to ensure the patient gets the best coordinated care for surgery:• Pre-Op Physical Screening: be sure
to screen for SBD to assist with anesthesia concerns. ASK about sleep!- Patient and bed partner complaints- Co-morbidities should raise suspicion- Poor work or school performance- Epworth sleepiness scale: correlates
with perception of sleepiness- Warning Signs & Symptoms: daytime
sleepiness, snoring, gasping/choking when asleep, witnessed stopped breathing, fatigue, impotence, morning headaches
- Two (or more) symptoms need to be documented in the Progress Notes
• STAR and PACE are identifying patients that need a sleep study and treatment prior to surgery. The patient will need to be sent back to their doctor or the patient can be referred to Sleep Medicine at PCI for the Face to Face for documentation and pre-authorization. EISC is prepared and has been providing service for urgent requests such as these.
MAY 2016 VOLUME 5 • ISSUE 1
What’s New:EISC Report & Sleep Disordered Breathing Impact
RecommendationsBe sure to read the Sleep Medicine Physicians’ recommendation section in the sleep study report to determine the next steps for patient care. This information is located near the bottom of the first page of the report. Questions? Call 319-362-4433.
EducationEISC is available to present Sleep education. EISC offers seminars that fit all needs. Seminars can be given in any time frame (15 minutes to 45 minutes for example) and during various shifts. EISC offers this education for free. Presentations can include: staff wellness in regards to Sleep; shift work concerns and understanding how poor Sleep increases health problems, the topics are endless. Questions? Call 319-362-4433.

What’s Coming: RMC New Sleep LabThe RMC River Ridge Pavilion was completed Nov 2015. EISC and Regional Medical Center in Manchester are currently working on the new sleep lab. This is Phase 2 of the new construction RMC series. EISC is excited about the new 2 bed room sleep study suites, tech area and newly renovated area surrounding the lab. Patients will experience high quality care in a comfortable and quiet location l
Did you know?
When we sleep well, we wake up feeling refreshed and alert for our daily activi-ties. Sleep affects how we look, feel and perform on a daily basis, and can have a major impact on our overall quality of life.
To get the most out of our sleep, both quantity and quality are important. If sleep is cut short, the body doesn’t have time to complete all of the phases needed for muscle repair, memory consolidation and release of hormones regulating growth and appetite. Then we wake up less prepared to concentrate, make decisions, or engage fully in activities.
How does sleep contribute to all of these things?
Sleep architecture follows a pattern of alternating REM (rapid eye movement) and NREM (non-rapid eye movement) sleep throughout a typical night in a cycle that repeats itself about every 90 minutes.
What role does each state and stage of sleep play?
NREM (75% of night): As we begin to fall asleep, we enter NREM sleep, which is composed of stages 1-4:
Stage 1• Between being awake and falling
asleep, light sleep.
Stage 2• Onset of sleep, becoming disengaged
from surroundings, breathing and heart rate are regular, body temperature drops (so sleeping in a cool room is helpful).
Stages 3 and 4• Deepest and most restorative sleep,
blood pressure drops, breathing becomes slower, muscles are relaxed,
blood supply to muscles increases, tissue growth and repair occurs, energy is restored.
• Hormones are released, such as: growth hormone, essential for growth and development, including muscle development.
REM (25% of night): First occurs about 90 minutes after falling asleep and recurs about every 90 minutes, getting longer later in the night.
• Consolidates memory and learning, supports daytime performance, brain is active and dreams occur, eyes dart back and forth, body becomes immobile and relaxed as muscles are turned off.
Sleep helps us thrive by contributing to a healthy immune system, and can also balance our appetites by helping to regulate levels of the hormones ghrelin and leptin, which play a role in our feelings
of hunger and fullness. So when we’re sleep deprived, we may feel the need to eat more, which can lead to weight gain.
The one-third of our lives that we spend sleeping, far from being “unproductive,” plays a direct role in how full, energetic and successful the other two-thirds of our lives can be.
SleepSmartz MAY 2016 VOLUME 5 • ISSUE 1
May is Better Sleep Month


















