Mental state decoding abilities in clinical depression
12
Research report Mental state decoding abilities in clinical depression B Lisa Lee T , Kate L. Harkness, Mark A. Sabbagh, Jill A. Jacobson Department of Psychology Queen’s University, Kingston, Ontario, Canada K7L 3N6 Received 10 December 2004; accepted 9 February 2005 Abstract Background: Depression is associated with profound impairments in social functioning. Past research and theory suggests that these impairments may be related to a difficulty in the ability of depressed individuals to identify and decode others’ social cues. However, the nature of this difficulty is equivocal. This investigation is the first to adopt a theory-of-mind framework to examine unipolar depressed individuals’ ability to identify complex mental states from eye expressions. Methods: Women with unipolar clinical depression (N = 52) and nondepressed controls (N = 30) completed the bReading the Mind in the Eyes TaskQ (Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., Plumb, I., 2001. The bReading the Mind in the EyesQ test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry, 42, 241–251.). All participants also completed self-report measures assessing depressive and anxious symptoms. Results: Depressed women were significantly impaired in their ability to identify mental states in the Eyes task compared to nondepressed participants. This difference remained after controlling for anxiety and was stronger for the affective than the somatic symptoms of depression. Limitations: The present study was limited by its sample size, resulting in low power for some comparisons. In addition, the study is limited by its use of a heterogeneous depressed sample, including outpatients and volunteers from the community, as well as its use of only female participants. Conclusions: Our results demonstrate that severely depressed individuals are significantly impaired in their ability to decode others’ mental states. We suggest that strategies based on improving basic theory-of-mind reasoning could be incorporated into current therapeutic interventions for depressed individuals to ameliorate their understanding and interpretation of social information. D 2005 Elsevier B.V. All rights reserved. Keywords: Major depression; Theory of mind; Mental state decoding 1. Introduction A primary clinical feature of depression is a profound impairment in social functioning. Depressed individuals exhibit reduced social competence 0165-0327/$ - see front matter D 2005 Elsevier B.V. All rights reserved. doi:10.1016/j.jad.2005.02.007 B Declaration of interest. None of the authors involved with this research had financial interest in the investigation. T Corresponding author. Tel.: +1 613 533 6003; fax: +1 613 533 2499. E-mail address: [email protected] (L. Lee). Journal of Affective Disorders 86 (2005) 247 – 258 www.elsevier.com/locate/jad
Transcript of Mental state decoding abilities in clinical depression

www.elsevier.com/locate/jad
Journal of Affective Disord
Research report
Mental state decoding abilities in clinical depressionB
Lisa LeeT, Kate L. Harkness, Mark A. Sabbagh, Jill A. Jacobson
Department of Psychology Queen’s University, Kingston, Ontario, Canada K7L 3N6
Received 10 December 2004; accepted 9 February 2005
Abstract
Background: Depression is associated with profound impairments in social functioning. Past research and theory suggests that
these impairments may be related to a difficulty in the ability of depressed individuals to identify and decode others’ social cues.
However, the nature of this difficulty is equivocal. This investigation is the first to adopt a theory-of-mind framework to
examine unipolar depressed individuals’ ability to identify complex mental states from eye expressions.
Methods: Women with unipolar clinical depression (N =52) and nondepressed controls (N =30) completed the bReading the
Mind in the Eyes TaskQ (Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., Plumb, I., 2001. The bReading the Mind in the
EyesQ test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child
Psychol. Psychiatry, 42, 241–251.). All participants also completed self-report measures assessing depressive and anxious
symptoms.
Results: Depressed women were significantly impaired in their ability to identify mental states in the Eyes task compared to
nondepressed participants. This difference remained after controlling for anxiety and was stronger for the affective than the
somatic symptoms of depression.
Limitations: The present study was limited by its sample size, resulting in low power for some comparisons. In addition, the
study is limited by its use of a heterogeneous depressed sample, including outpatients and volunteers from the community, as
well as its use of only female participants.
Conclusions: Our results demonstrate that severely depressed individuals are significantly impaired in their ability to decode
others’ mental states. We suggest that strategies based on improving basic theory-of-mind reasoning could be incorporated into
current therapeutic interventions for depressed individuals to ameliorate their understanding and interpretation of social
information.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Major depression; Theory of mind; Mental state decoding
0165-0327/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.jad.2005.02.007
B Declaration of interest. None of the authors involved with this
research had financial interest in the investigation.
T Corresponding author. Tel.: +1 613 533 6003; fax: +1 613
533 2499.
E-mail address: [email protected] (L. Lee).
1. Introduction
A primary clinical feature of depression is a
profound impairment in social functioning. Depressed
individuals exhibit reduced social competence
ers 86 (2005) 247–258

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258248
(Fisher-Beckfield and McFall, 1982; Levendosky et
al., 1995), have fewer social interactions (Gotlib and
Lee, 1989), and find these encounters less rewarding
and less enjoyable than do nondepressed individuals
(Nezlek et al., 2000). These negative interpersonal
experiences often cause depressed individuals to
isolate themselves, thereby perpetuating their depres-
sion (Rippere, 1980). Because the interpersonal
difficulties of depressed individuals are so pervasive,
it is important to obtain a more detailed understanding
of the cognitive mechanisms that might underlie these
social problems.
One framework that has been used to understand
impaired social functioning in clinical conditions is
btheory of mindQ (e.g., Baron-Cohen, 1989; Langdonet al., 2002; Richell et al., 2003). Broadly construed,
theory of mind refers to the everyday ability to ascribe
mental states (e.g., beliefs, emotions, intentions) to
others to understand and predict their social behavior.
There are two separable aspects of theory of mind: (1)
decoding mental states from perceivable social
information such as tone of voice, body posture, or
facial expression, and (2) reasoning about mental
states by integrating contextual and historical infor-
mation about a person (e.g., idiosyncratic experiences,
knowledge, attitudes) to understand behavior (Sab-
bagh, 2004).
The theory-of-mind framework has proved very
useful in understanding the social deficits associated
with schizophrenia, autism, and psychopathy. For
example, patients with schizophrenia are impaired at
both decoding mental states from pictures of faces
(Craig et al., 2004; Kington et al., 2000; Oguz et al.,
2003) and making judgments about false beliefs or
ambiguous intentions based on contextual information
(Craig et al., 2004; Frith and Corcoran, 1996; Mazza
et al., 2001; Pickup and Frith, 2001; Janssen et al.,
2003; Greig et al., 2004).
However, we know of only two studies that have
applied a theory-of-mind framework to depression. In
one, patients with affective disorders (bipolar- and
unipolar-depressed patients) did not perform differ-
ently from healthy controls on a second-order false
belief task (Doody et al., 1998), thereby suggesting
that individuals with affective disorders may not be
impaired in mental state reasoning. However, a more
recent study has reported poor performance in similar
false belief tasks in a sample of bipolar-depressed and
bipolar-manic patients (Kerr et al., 2003). Given the
conflicting findings of these two studies, it is unclear
whether depressed individuals have difficulty with
theory-of-mind tasks that require reasoning about
mental states.
A wider body of literature may be relevant to
understanding whether patients with unipolar depres-
sion have difficulties with first-order theory-of-mind
tasks that involve decoding mental states. Specifically,
researchers have identified poor facial emotion
recognition as a possible factor underlying depressed
individuals’ social difficulties (e.g., Deldin et al.,
2000). Emotions are a type of mental state and, hence,
emotion recognition may rely in part on mental state
decoding skills. Several studies found that depressed
individuals were impaired at recognizing facial
emotions. These studies required participants to match
a target photograph to one of an array of other
photographs that depicted stereotypical emotions
(Rubinow and Post, 1992) or to determine whether
pairs of faces were the same or different (Feinberg et
al., 1986; Asthana et al., 1998). Intriguingly, however,
Asthana et al. (1998) found that depressed patients
also were impaired at a visuo-spatial pattern-matching
task involving simple non-face patterns. Thus, in these
studies, it is unclear whether depressed individuals are
impaired in their ability to recognize emotional
content, or simply had general deficits in visuo-spatial
pattern matching.
Other studies in this area have found a different
pattern of results. For example, several studies
found that depressed individuals exhibited a bias
to preferentially identify negative emotions (Mandal
and Bhattacharya, 1985; Gur et al., 1992; Bouhuys
et al., 1997; Bouhuys et al., 1999; Hale, 1998).
However, the paradigm employed by the majority of
these studies required participants to recall emotions
from memory or freely label emotion terms,
processes that themselves are associated with
negative biases in depression independent of emo-
tion recognition (Dalgleish and Watts, 1990).
Furthermore, two studies utilizing emotion recog-
nition tasks that did not require either free recall/
labeling or visual–spatial discrimination found no
differences in performance between depressed and
nondepressed participants (Gessler et al., 1989;
Gaebel and Wolwer, 1992). However, in these
studies, both groups performed at near ceiling

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258 249
levels, thus limiting the sensitivity of the measure to
detect subtle differences in performance.
This brief review suggests that significant prob-
lems with the methodologies that have been used to
measure facial emotion recognition abilities among
depressed individuals may account for the conflicting
findings of these studies. It is thus an open question as
to whether patients with unipolar depression have
difficulties decoding others’ mental states.
In the current study we assess mental state
decoding using the bReading the Mind in the EyesQtask (bEyes taskQ; Baron-Cohen et al., 2001). The
Eyes task was developed as a test of adult theory-of-
mind abilities and involves the identification of a
wide range of complex mental states. Across 36
trials, participants are shown a picture of the eye
region of the face (from the nose to the brow)
surrounded by four mental state terms (e.g., reflec-
tive, irritated, confident, ashamed). Participants select
from the four terms the one that best matches the
mental state portrayed in the picture. This task has
been used in a large number of studies investigating
mental state decoding skills in patients with autism
or Asperger’s syndrome (Dorris et al., 2004; Klein-
man et al., 2001; Rutherford et al., 2002), schizo-
phrenia (Craig et al., 2004; Kelemen et al., 2003),
psychopathy (Richell et al., 2003), dementia (Greg-
ory et al., 2002), and dysphoria (Harkness et al., in
press).
The Eyes task has two main strengths that make it
an excellent method for assessing mental state
decoding in depression. First, it is quite difficult.
The information carried by the eyes, while reliable, is
quite subtle and difficult to interpret when information
about other features of the face are not available
(Ekman and Friesen, 1978). Previous studies with the
Eyes task showed that healthy adults perform at about
70% accuracy (Baron-Cohen et al., 2001), thereby
allowing for detection of subtle group differences.
Second, the Eyes task is procedurally simple and
imposes very little demand on peripheral cognitive
systems that may be collaterally affected in depression
(i.e., free recall, visuo-spatial matching).
1.1. Goals and hypotheses
The first goal of the current investigation is to
examine differences in theory-of-mind decoding
between clinically depressed and nondepressed indi-
viduals using the Eyes task. Based on previous studies
with other clinical groups, we predict that individuals
with depression will be impaired in their ability to
decode others’ mental states in relation to nonde-
pressed individuals.
Our second goal is to examine whether individual
differences in the severity and specific symptoms of
depression differentially predict mental state decoding
abilities among depressed individuals. First, we
predict that those who are severely depressed will be
more impaired on the Eyes task than those with a mild
to moderate level of depression. Second, we predict
that certain symptoms will drive the negative associ-
ation between depression severity and theory-of-mind
performance. In particular, we predict that the
affective symptoms of depression, such as anhedonia,
low motivation, and hopelessness will be more
strongly related to performance on this social skill
than somatic symptoms, such as insomnia, loss of
appetite, and low energy.
2. Method
2.1. Participants
Clinically depressed adult women were referred
from the outpatient Mood Disorders Unit of the
Providence Continuing Care Centre-Mental Health
Services (PCCC, MHS) or the Adult Psychiatry
Outpatient Unit of Hotel Dieu Hospital (HDH) or
were recruited from the wider community. Nonde-
pressed adult women were recruited from the
community. Community recruitment was accom-
plished via radio and newspaper advertisements,
posted fliers, and referrals from private practitioners.
All depressed participants recruited from the com-
munity took part in a brief interview by telephone
to determine eligibility for the study. This interview
involved the bmajor depressive disorderQ module of
the Structured Clinical Interview for DSM-IV Axis I
Disorders (SCID-I/P; First et al., 1995), as well as
questions regarding the presence of comorbid exclu-
sionary diagnoses. To be included in the clinically
depressed group, women had to be over 18 years of
age and have a primary diagnosis of current
unipolar major depression. Women who had a

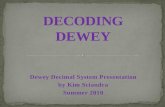
Fig. 1. Sample items from: (a) Eyes task (panicked is the target, or
correct, answer), (b) Animal task (ferocious is the target), and (c)
Gender task (female is the target).
L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258250
current or past diagnosis of a psychotic disorder,
bipolar disorder, substance dependence or a serious
medical condition that could cause depression (e.g.,
hypothyroidism) were excluded. These potential
comorbid conditions were excluded to increase the
internal validity of the study. In particular, our aim
is to investigate the specific relationship of theory-
of-mind skills to unipolar major depression. Hence,
it was necessary to exclude individuals who
suffered from comorbid conditions that may, them-
selves, be causally related to their depression.
To be included in the nondepressed control group,
women had to be over 18 years of age and have no
psychiatric history. Nineteen participants were
excluded based on the phone screen, leaving 67
depressed and 34 nondepressed women. These
women participated in the study at an on-campus
laboratory, or at PCCC, MHS if they were patients at
this facility.
At the appointment, all participants were assessed
with the SCID-I/P. This structured interview derives
diagnoses according to Diagnostic and Statistical
Manual for Mental Disorders criteria (DSM-IV;
American Psychiatric Association, 1994). SCID
interviews were conducted by the second author (a
clinical psychologist with extensive training and
experience with the SCID) or the first author, an
advanced graduate student who was trained to bgoldstandardQ reliability status by the second author (see
Grove et al., 1981 for details on achieving bgoldstandardQ status). Five women in the depressed
group were excluded at this stage because they did
not meet criteria for current major depression, and
10 were excluded because they had a history of
mania, psychosis, or substance dependence. Four
women in the control group were excluded because
they had a history of psychiatric illness. Thus, the
final sample comprised 52 women who met DSM-
IV criteria for major depression and 30 nonde-
pressed women.
2.2. Experimental tasks
2.2.1. Eyes task
The task consists of 36 black-and-white photo-
graphs (15 cm�6 cm) of the eye region of faces from
just above the eyebrows to halfway down the bridge
of the nose (Sample items are presented in Fig. 1).
Participants selected the one of four mental state
adjectives (three distracters and the correct adjective)
that described the person’s mental state. The task was
presented on a laptop computer screen. The photo-
graph was centered on the screen, and the four
descriptive adjectives were placed at the four corners
of the photograph equally spaced from the center of
the screen. Participants responded by pressing one of
four keys on the keyboard (i.e., S, X, K, M) identified
by colored stickers. These keys were chosen because
they are spatially analogous to the location of the
adjectives at the corners of the picture. Participants’
responses and response times were digitally recorded.
For some analyses, the 36 eyes stimuli were classified
into three valence categories: 12 negative (e.g.,
bupsetQ), 8 positive (e.g., bfriendlyQ), and 16 neutral
(e.g., breflectiveQ) based upon pilot research (see
Harkness et al., in press).
We developed two control tasks to help ensure that
any differences found between the groups on the Eyes
task could not be attributed to peripheral differences
in task demands or low-level perceptual processing:
(1) Animals task: 12 black-and-white pictures of

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258 251
different animals were presented in a similar fashion
as the pictures of eyes, and participants selected the
best adjective (out of four) that described the animal;
and (2) Gender task: 12 pictures from the Eyes task
were randomly selected and presented with the words
bmaleQ and bfemaleQ at the bottom corners of the
picture. Again, participants were asked to select the
appropriate adjective.
2.3. Measures
2.3.1. Demographic interview
This information sheet contained questions regard-
ing sex, age, education level attained, occupational
status, number of children, and treatment status.
2.3.2. Depression severity measures
The 21-item Hamilton Rating Scale for Depression
interview (HRSD; Hamilton, 1960) and the 21-item
self-report Beck Depression Inventory (BDI-II; Beck,
1996) were administered to determine the presence
and severity of depression symptoms. Both measures
are widely used in the study of depression, and
considerable evidence supports their strong psycho-
metric properties (Beck et al., 1988; Rehm and
O’Hara, 1985).
2.3.3. Mood and Anxiety Symptom Questionnaire
(MASQ; Watson and Clark, 1991)
This 90-item self-report questionnaire yields
indexes of specific anxious and depressive symp-
toms. The instrument is shown to have good
convergent and discriminant validity (Watson et al.,
1995). Studies have indicated that more than 50% of
individuals with major depression suffer from a
comorbid anxiety disorder (e.g., Dobson and
Cheung, 1990) and an even larger percentage
experience significant anxiety symptoms. Anxiety
has been associated with poor social functioning and
negative interpersonal experiences (Weary and
Edwards, 1994). Furthermore, anxious participants
are more accurate in the identification of negative
facial emotions than are non-anxious participants
(Lundh and Ost, 1996; Veljaca and Rapee, 1998; Foa
et al., 2000). Thus, the MASQ allowed us to control
for the effect of anxiety symptoms in examining the
relation of depression to mental state decoding
abilities.
2.3.4. Procedure
After a complete description of the study, partic-
ipants provided written informed consent. All partic-
ipants were administered the demographic
questionnaire, the SCID-I/P, and the HRSD. Then
participants completed the experimental tasks, which
were combined and presented in a single block (60
trials total), and trials were randomly selected from
among all tasks. Following the experimental tasks,
participants completed the self-report measures of
mood. Participants were then debriefed, and those
recruited from advertisements were paid $10. The
protocol for this study was approved by the IRB at
Queen’s University.
3. Results
3.1. Preliminary item analyses
Accuracy on each of the three experimental tasks
was defined as the percentage of items on which
participants selected a designated target adjective
(see Baron-Cohen et al., 2001). To confirm the
validity of each item, we conducted a series of
Bonferonni-corrected binomial tests comparing the
proportion of participants who selected the target
adjective to the proportion that would be expected
by chance ( p =0.25 for the Eyes and Animal tasks
and p=0.50 for the Gender task). For the 36 eyes
stimuli, more participants selected the target than
would be expected by chance for all but one item
(at least 23/52 depressed participants and 16/30
nondepressed participants, binomial test, p b0.0013).
The same results were obtained for the 12 stimuli
used in the Animal task (at least 22/52 depressed
and 15/30 nondepressed participants, binomial test,
pb0.0041) and the 12 stimuli in the Gender task (at
least 16/52 depressed and 23/30 nondepressed
participants, binomial test, p b0.0041). Thus, after
deleting the invalid items, the Eyes, Animal, and
Gender tasks consisted of 35, 11, and 11 items,
respectively.
3.2. Demographic and clinical differences
We examined three groups based on depression
severity (Beck et al., 1988): (1) mildly/moderately

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258252
depressed: women meeting DSM-IV criteria for major
depression with BDI scores between 10 and 23
(n =15); (2) severely depressed: women meeting
DSM-IV criteria for major depression with BDI scores
above 23 (n =37); and (3) nondepressed: participants
with no history of psychiatric illness (n =30).
The demographic and clinical characteristics by
group are presented in Table 1. Significant differences
were obtained across the groups for age,
F(2,79)=6.14, p =0.003, and education, F(2,79)=
3.18, p =0.04. The nondepressed group was signifi-
cantly older than the mildly/moderately depressed and
severely depressed groups, t(43)=2.63, p =0.01 and
t(65)=2.97, p=0.004, respectively. In addition, the
nondepressed group was significantly more highly
educated than the severely depressed group,
t(65)=2.52, p =0.01. However, neither age nor years
of education emerged as significant covariates in the
primary analyses, p’sN0.38. Therefore, results of the
uncontrolled analyses are reported below. Depressed
participants recruited from the community did not
Table 1
Demographic and clinical characteristics of the sample by group
Mild/moderate depression group (n =15)
VARIABLE N % M S.D.
Age 37.5 12.7
Marital status: married 6 40.0
Divorced, widowed 2 13.4
Never married 7 46.7
Education: grade 8 or less 0 0
Grade 9–12 1 6.7
Part college 7 46.7
Graduated college 2 13/3
Graduate degree 5 33.3
Occupation: unemployed 4 26.7
Homemaker 1 6.7
Professional 3 20.0
Sales, service 5 33.3
Student 2 13.3
Treatment: therapy 1 6.7
Medication 0 0
Both 11 73.3
No treatment 3 20.0
Age of onset 25.3 10.6
Previous episodes 5.1 6.3
Anxiety disorder 10 66.7
BDI score 16.6 5.1
HRSD score 11.7 5.4
AA score 29.1 9.6
differ on the experimental tasks from those referred
from outpatient clinics ( p’sN0.10), thus these groups
were examined together.
3.3. Overall accuracy analyses
Fig. 2 shows percent accuracy on the three tasks
(i.e., Eyes, Animal, and Gender tasks) for depressed
and nondepressed groups. Percent accuracy on the
Gender task was examined separately because it is a
statistically easier task (i.e., it involves choosing
between two answers as opposed to four). An analysis
of covariance (ANCOVA) was conducted with group
as the between-subjects factor (severely depressed vs.
mild/moderately depressed vs. nondepressed) and
percent accuracy on the Gender task as the dependent
measure. Total score on the Anxious Arousal (AA)
index of the MASQ was entered as a covariate. The
analysis revealed no significant effect of depression
group on the Gender task, F(2,74)=2.03, p =0.13. As
well, level of anxiety was not a significant covariate,
Severe depression group (n =37) Control group (n =30)
N % M S.D. N % M S.D.
39.9 12.5 50.6 17.1
17 45.9 14 46.7
7 18.9 9 30.0
13 35.1 7 23.3
1 2.7 0 0
9 24.3 0 0
6 16.2 9 30.0
18 48.6 16 53.3
3 8.1 5 16.7
21 56.8 10 33.3
3 8.1 1 3.3
0 0 7 23.3
11 29.7 5 16.7
2 5.4 7 23.3
7 18.9
4 10.8
23 62.2
3 8.1
20.7 10.4
6.2 9.7
18 48.6
36.5 6.7 3.2 4.5
17.4 6.6 1.0 1.8
37.7 12.6 20.5 4.6

Task
Eyes Animals Gender
Per
cent
Acc
urac
y
60
70
80
90
100 ControlsMild/Moderate DepressionSevere Depression
Fig. 2. Means for percent accuracy on Eyes, Animal, and Gender
task for depressed and nondepressed groups.
L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258 253
F(1,74)=2.39, p =0.13. These null results were
expected given that the Gender task served as a
control for mental state decoding abilities.
Next, a 3�2 (group� task) mixed-design
ANCOVA was conducted, with group (severely
depressed vs. mild/moderately depressed vs. nonde-
pressed) as the between-subjects factor, task (Eyes
task vs. Animal task) as the within-subjects factor, and
percent accuracy on the task as the dependent
measure. Total score on AA was entered as a
covariate. The main effect of task was significant,
F(1,74)=5.01, p =0.03, such that, across groups, the
Animal task was easier than the Eyes task. The main
effect of group was not significant, F(2,74)=1.14,
p =0.33. However, a significant group by task
interaction was found, F(2,74)=3.28, p =0.04. Con-
sistent with hypotheses, the severely depressed group
was significantly less accurate than was the nonde-
pressed group on the Eyes task, t(65)=2.24, p=0.03,
but these two groups did not significantly differ on the
Animal task, t(65)=1.36, p =0.18. Similarly, the mild/
moderately depressed group was less accurate than the
nondepressed group at a trend level on the Eyes task,
t(43)=1.66, p=0.10, but did not differ significantly
from the nondepressed group on the Animal task,
t(43)=0.41, p=0.69. The two depressed groups did
not differ significantly on either the Eyes or the
Animals tasks, t(50)=0.02, p =0.98 and t(50)=0.72,
p =0.48, respectively.
The anxiety covariate was significant, F(1,74)=
6.79, p =0.01, such that increasing anxiety predicted
poorer performance on both the Eyes and Animal
tasks. However, the interaction between the anxiety
covariate and task was not significant, F(1,74)=0.36,
p =0.55. Thus, the effect of severe depression
remained a significant predictor of poor performance
on the Eyes task over and above the effect of
anxiety.
3.4. Response time (RT) analyses
To ensure that the difference in accuracy on the
Eyes task between severely depressed and nonde-
pressed groups was not solely attributable to differ-
ences in RT, a 3�2 (group� task) mixed-design
ANCOVA was conducted with group as the between-
subjects factor, task (Eyes task vs. Animal task) as the
within-subjects factor, and the mean RT on the task as
the dependent measure. Total score on AA was
entered as a covariate. Only the main effect of task
was significant, F(1,74)=8.40, p =0.005. That is,
collapsed across groups, participants spent more time
on the Eyes task (M =8390.82, S.D.=3732.05) than
on the Animal task (M =6195.88, S.D.=2792.73).
There were no other main or interaction effects,
p’sN0.70. Thus, the severely depressed group’s
decreased performance on the Eyes task relative to
the nondepressed group was not due to differences
between groups in RT.
3.5. Mental state valence analyses
We next examined whether the valence of the
mental state expressed in the eyes influenced perform-
ance across the groups (see Fig. 3). A mixed model
ANCOVA was conducted with valence (negative vs.
positive vs. neutral) as the within-subjects factor,
group (severely depressed vs. mild/moderately
depressed vs. nondepressed) as the between-subjects
factor, and percent accuracy on the Eyes task as the
dependent measure. Neither the main effect of valence
nor the valence by group interaction was significant,
F(2,73)=0.74, p =0.48, and F(4,148)=1.03, p =0.39,
respectively. Thus, collapsed across group, accuracy
did not differ across negative, positive, and neutral
mental states, nor did accuracy differ among groups
across negative, positive, and neutral mental states. In

Emotional Valence
Negative Positive Neutral
Per
cent
Acc
urac
y
60
70
80
90
100 Controls Mild/Moderate Depression Severe Depression
Fig. 3. Means for percent accuracy on negative, positive, and neutral
eyes items of the Eyes task for depressed and nondepressed groups.
L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258254
addition, anxiety was not a significant covariate,
F(2,73)=0.84, p =0.43.
3.6. Depression symptom analyses
Contrary to the first part of our second hypothesis,
no relation was found between depression severity
and performance on the Eyes task within the
depressed groups. That is, among those who were
depressed, those with a severe depression were not
more impaired on the task than those with a milder
level of depression. However, while quantitative
differences in the overall level of depression severity
did not predict differences in theory-of-mind reason-
ing, it may still be the case that qualitative differences
in specific symptom profiles may have differential
relations to theory-of-mind performance. To test this
hypothesis we derived two summary scores, based on
previous factor analytic study of the HRSD (Steer et
al., 1987): (1) affective depression: This factor
comprised the summed scores for the HRSD symp-
toms of depressed mood, guilt, suicide, work and
activities, and retardation; and (2) somatic depression:
This factor comprised the summed scores for the
HRSD symptoms of early, middle, and late insomnia,
anxiety-somatic, somatic-gastrointestinal, somatic-
general, genital symptoms, hypochondriasis, and
weight loss.
We performed a hierarchical linear regression with
accuracy on the Eyes task as the criterion. Scores on
affective depression and somatic depression were
entered together as a block. (Entering reaction time
on the Eyes task to the model as a covariate did not
change the pattern of results and, thus, the non-covaried
findings are presented.) The overall model was
significant, R2=0.14, F(2,46)=3.43, p =0.04. Consis-
tent with hypotheses, affective depression was signifi-
cantly negatively related to Eyes task performance
among the depressed women (b =�0.38, p =0.01),
while somatic depression was not (b =0.24, p =0.12).
4. Discussion
The main goal of the present study was to
investigate mental state decoding abilities in women
with unipolar major depression. Consistent with our
predictions, we found that severely depressed women
were significantly less accurate in identifying complex
mental states from pictures of eyes than were nonde-
pressed women across the range of positively,
negatively, and neutrally valenced mental states. Our
findings are the first to show a deficit in mental state
decoding in patients with unipolar depression. In
addition, they are in line with several studies reporting
an impairment in more general facial emotion
recognition (Feinberg et al., 1986; Zuroff and Colussy,
1986; Persad and Polivy, 1993; Rubinow and Post,
1992; Asthana et al., 1998). More importantly, our
findings suggest that depressed individuals’ impair-
ment in this area may be independent of more general
cognitive and perceptual deficits because these
women did not differ from nondepressed individuals
on the control tasks, which were matched with respect
to surface cognitive and perceptual demands.
A compelling interpretation of the present findings
is that patients with clinical depression have a specific
impairment in the theory-of-mind ability to recognize
and decode others’ mental states. Yet, one alternative
explanation that we cannot entirely rule out is that
depressed individuals have a more general cognitive or
perceptual deficit in the ability to process facial
stimuli. We attempted to control for this explanation
by including the two control tasks and, indeed, no
evidence was found for significant differences among
the groups on these tasks. For example, in the Gender

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258 255
task depressed individuals were not significantly
impaired in their ability to process the physical
features of the eyes stimuli and organize them into
male and female categories. However, all groups
performed at near ceiling levels, thus limiting the
ability of the task to discriminate performance among
groups and raising the possibility that depressed
participants showed impaired performance on the Eyes
task because it was cognitively the most difficult of the
three experimental tasks. Perhaps with a gender-
discrimination task that was more difficult, depressed
individuals would have shown impairment on this task
as well. In support of this possibility, a recent study has
shown that the characteristic brain electrophysiolog-
ical response to face stimuli appears to be abnormal in
patients with depression (Deldin et al., 2000).
The question of why patients with depression have
difficulties decoding mental states is one of clear
importance and requires more research. In particular,
future research that includes other theory-of-mind
tests (such as the false belief task) will be helpful in
validating the present findings and confirming their
specificity to theory-of-mind reasoning. Nonetheless,
these issues do not cast doubt on our main claim. That
is, irrespective of its root cause, patients with clinical
depression clearly do have difficulties decoding
mental states of others based on subtle visual
information.
Our second goal was to investigate whether
individual differences in depression severity and the
specific affective vs. somatic symptom factors of
depression predict differences in mental state decoding
among depressed individuals. In terms of our first
hypothesis, contrary to predictions, performance on
the Eyes task did not vary as a function of depression
severity. Indeed, mean accuracy on the Eyes task was
identical for both the mild/moderate and severe
depression groups (i.e., 70% accuracy for both
groups). However, the difference between the mild/
moderate depression group and the nondepressed
control group failed to reach statistical significance
due to increased variability in the scores of these
depressed participants on the Eyes task (i.e.,
S.E.=0.03 for the mild/moderate depression group
and S.E.=0.01 for the severe depression group).
Interestingly, the results of the present study run
counter to those obtained in a recent study from our
lab in which mental state decoding was examined in
dysphoric individuals (i.e., individuals with elevated
levels of depression symptoms, but who did not meet
DSM-IV criteria for a major depressive episode;
Harkness et al., in press). In this study, dysphoric
individuals (mean BDI=17.7) performed significantly
better on the Eyes task than a non-dysphoric control
group. This effect persisted in two independent
replications and was robust after controlling for
demographic variables, anxiety symptoms, and reac-
tion time. By contrast, the exact opposite pattern of
performance was obtained in the present study even
among those with mild/moderate depression who
exhibited roughly the same level of depression
severity (mean BDI=16.6) as those in our previous
study, but who did meet DSM-IV criteria for major
depression.
While there may be several reasons for this
dissociation, one intriguing possibility is that there is
a fundamental qualitative difference between the
ddysphoriaT of our non-clinical sample and the
diagnosis of major depression in the clinical sample,
despite similar quantitative levels of depression
severity. That is, the presence of depressive symptoms
is qualitatively quite different from having the
syndrome of depression. This qualitative difference
may underlie a difference in the way social informa-
tion is processed by clinically depressed vs. dysphoric
individuals.
This suggestion is consistent with the results
bearing on the second part of our second hypothesis,
in which we found that performance on the Eyes task
was particularly impaired among those who scored
high on the affective symptoms of depression. These
symptoms include depressed mood, guilt, anhedonia,
retardation, and suicidality, and are very similar to the
symptoms that comprise the subtype of hopelessness
depression (HD; Abramson et al., 1989). HD is
associated with an overwhelming sense that negative
life events are likely to occur, that they will have a
devastating impact, and that they are entirely uncon-
trollable (Abramson et al., 1989). HD has been
associated with a lack of interest in others and poor
social problem-solving (Bonner and Rich, 1988;
Reinecke et al., 2001). In effect, individuals experi-
encing HD may have essentially bgiven upQ in trying
to rectify negative circumstances and thus are unlikely
to allocate cognitive resources to attending to and
processing social information.

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258256
These latter results are intriguing, as they
suggest that not all forms of depression are
associated with poor theory-of-mind reasoning
skills. In particular, regardless of the level of global
depression severity, the presence of specific affec-
tive symptoms may indicate a clinical subtype of
depression particularly likely to be associated with
compromised mental state decoding. Future research
examining the specific symptoms and symptom
clusters associated with theory-of-mind ability
across the full spectrum of non-clinical and clinical
depression severity is required to fully address this
issue.
4.1. Limitations and future directions of research
The present study was limited by its sample size,
resulting in low power for some comparisons. In
particular, low power may have limited our ability
to find an effect of depression on accuracy in the
Eyes task across mental states of a negative,
positive, and neutral emotional valence. In addition,
the study is limited by its use of a heterogeneous
depressed sample, including outpatients and volun-
teers from the community. However, the use of
such a sample may also be seen as a strength as it
increases the generalizability of the findings in
comparison to more homogenous samples. Impor-
tantly, preliminary analyses revealed no differences
in accuracy on the Eyes task between the two types
of referrals. Nevertheless, our sample may differ in
important ways from a non-referred epidemiological
sample. Furthermore, the present study was limited
by its use of only women participants; thus future
study with a mixed sample is required to ensure
generalizability to men with depression.
Future research also is required to determine
whether impaired theory-of-mind decoding in
depressed individuals is a stable trait-like phenom-
enon, or whether this deficit is state-dependent.
Preliminary results using second-order theory-of-
mind reasoning tasks suggest that deficits on a false
belief task are observed even during remission,
suggesting that impaired theory of mind may
represent a trait-like vulnerability for psychopathol-
ogy (Inoue et al., 2004). Similar studies are now
required to generalize this finding to the founda-
tional skill of theory-of-mind decoding.
5. Conclusions
Severe depression, and specifically the affective
symptoms of depression, was associated with signifi-
cant impairment in the ability to decode others’
mental states. Intact mental state decoding supports
everyday social interactions. A breakdown in the
ability to pick up on others’ subtle nonverbal cues
may be a critical factor in understanding the profound
social difficulties experienced by depressed individu-
als. This compromised ability may lead depressed
individuals to respond inappropriately, eliciting neg-
ative reactions from others and potential rejection.
Given the important role of nonverbal cues in human
communication, the findings of this investigation have
potentially important clinical implications. For exam-
ple, research into the theory-of-mind deficits of
individuals with autism have led to major clinical
advances such as the development of techniques for
early diagnosis (Baird et al., 2000) and interventions
that aim to improve their understanding and inter-
pretation of social information (Swettenham et al.,
1996). Strategies could also be incorporated into
current therapeutic interventions for depressed indi-
viduals to improve their day-to-day social functioning.
Acknowledgements
This research was supported by a grant from the
Canada Foundation for Innovation to Kate Harkness
and Mark Sabbagh, and was part of Lisa Lee’s
Master’s thesis. We are grateful to Roumen Milev,
Michela David, Amarendra Singh, and Eva Barnett-
Cowan for supplying patient referrals. We also wish to
thank Tina Chen, Erin Cordingley, James Lackie,
Lynne Lamarche, and Veronica Legnini for their help
with data coding and data management. Finally, we
thank Simon Baron-Cohen for graciously providing
us with stimulus materials.
References
Abramson, L.Y., Metalsky, G.I., Alloy, L.B., 1989. Hopelessness
depression: a theory-based subtype of depression. Psychol. Rev.
96, 358–372.
American Psychiatric Association, 1994. Diagnostic and Statistical
Manual of Mental Disorders, 4th ed. APA, Washington.

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258 257
Asthana, H.S., Mandal, M.K., Khurana, H., Haque-Nizamie, S.,
1998. Visuospatial and affect recognition deficit in depression.
J. Affect. Disord. 48, 57–62.
Baird, G., Charman, T., Baron-Cohen, S., Cox, A., Swettenham, J.,
Wheelwright, S., Drew, A., 2000. A screening instrument for
autism at 18 months of age: a 6-year follow-up study. J. Am.
Acad. Child Adolesc. Psych. 39, 694–702.
Baron-Cohen, S., 1989. The autistic child’s theory of mind: a case
of specific developmental delay. J. Child Psychol. Psychiatry
30, 285–297.
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., Plumb, I.,
2001. The bReading the Mind in the EyesQ test revised version:
a study with normal adults, and adults with Asperger syndrome
or high-functioning autism. J. Child Psychol. Psychiatry 42,
241–251.
Beck, A.T., 1996. Beck Depression Inventory-II. Psychological
Corporation, San Antonio, TX.
Beck, A.T., Steer, R.A., Garbin, M.G., 1988. Psychometric proper-
ties of the Beck depression inventory: twenty-five years of
evaluation. Clin. Psychol. Rev. 8, 77–100.
Bonner, R.L., Rich, A.R., 1988. A prospective investigation of
suicidal ideation in college students: a test of a model. Suicide
Life-Threat. Behav. 18, 245–258.
Bouhuys, A.L., Geerts, E., Mersch, P.P.A., 1997. Relationship
between perception of facial emotions and anxiety in clinical
depression: does anxiety-related perception predict persistence
of depression? J. Affect. Disord. 43, 213–223.
Bouhuys, A.L., Geerts, E., Gordijn, M.C.M., 1999. Gender-specific
mechanisms associated with outcome of depression: perception
of emotions, coping and interpersonal functioning. Psychiatry
Res. 85, 247–261.
Craig, J.S., Hatton, C., Craig, F.B., Bentall, R.P., 2004. Persecutory
beliefs, attributions and theory of mind: comparison of patients
with paranoid delusions, Asperger’s syndrome and healthy
controls. Schizophr. Res. 69, 29–33.
Dalgleish, T., Watts, F.N., 1990. Biases of attention and memory in
disorders of anxiety and depression. Clin. Psychol. Rev. 10,
589–604.
Deldin, P.J., Keller, J., Gergen, J.A., Miller, G.A., 2000. Right-
posterior face processing anomaly in depression. J. Abnorm.
Psychology 109, 116–121.
Dobson, K.S., Cheung, E., 1990. Relationship between anxiety and
depression: conceptual and methodological issues. In: Maser,
J.D., Cloninger, C.R. (Eds.), Comorbidity of Mood and Anxiety
Disorders. APA, Washington, DC, pp. 611–632.
Doody, G.A., Gotz, M., Johnstone, E.C., Frith, C.D., Cunningham
Owens, D.G., 1998. Theory of mind and psychoses. Psychol.
Med. 28, 397–405.
Dorris, L., Espie, C.A.E., Knott, F., Salt, J., 2004. Mind-reading
difficulties in the siblings of people with Asperger’s syndrome:
evidence for a genetic influence in the abnormal development of
a specific cognitive domain. J. Child Psychol. Psychiatry 45,
412–418.
Ekman, P., Friesen, W.V., 1978. Facial Action Coding System.
Consulting Psychologists Press, Palo Alto, CA.
Feinberg, T.E., Rifkin, A., Schaffer, C., Walker, E., 1986.
Facial discrimination and emotional recognition in schizo-
phrenia and affective disorders. Arch. Gen. Psychiatry 43,
276–279.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1995.
Structured Clinical Interview for DSM-IV Axis I Disorders.
Biometrics Research Department, New York State Psychiatric
Institute, New York.
Fisher-Beckfield, D., McFall, R.M., 1982. Development of a
competence inventory for college men and evaluation of
relationships between competence and depression. J. Consult.
Clin. Psychol. 50, 697–705.
Foa, E.B., Gilboa-Schechtman, E., Amir, N., Freshman, M.,
2000. Memory bias in generalized social phobia: remember-
ing negative emotional expressions. J. Anxiety Disord. 14,
501–519.
Frith, C.D., Corcoran, R., 1996. Exploring dtheory of mindT in
people with schizophrenia. Psychol. Med. 26, 521–530.
Gaebel, W., Wolwer, W., 1992. Facial expression and emotional
face recognition in schizophrenia and depression. Eur. Arch.
Psychiatry Clin. Neurosci. 242, 46–52.
Gessler, S., Cutting, J., Frith, C.D., Weinman, J., 1989. Schizo-
phrenic inability to judge facial emotion: a controlled study. Br.
J. Clin. Psychol. 28, 19–29.
Gotlib, I.H., Lee, C.M., 1989. The social functioning of depressed
patients: a longitudinal assessment. J. Soc. Clin. Psychol. 8,
223–237.
Gregory, C., Lough, S., Stone, V., Erzinclioglu, S., Martin, L.,
Baron-Cohen, S., Hodges, J.R., 2002. Theory of mind in
patients with frontal variant frontotemporal dementia and
Alzheimer’s disease: theoretical and practical implications.
Brain 125, 752–764.
Greig, T.C., Bryson, G.J., Bell, M.D., 2004. Theory of mind
performance in schizophrenia: diagnostic, symptom, and neuro-
psychological correlates. J. Nerv. Ment. Dis. 192, 12–18.
Grove, W., Andreasen, N., McDonald-Scott, P., Keller, M., Shapiro,
R., 1981. Reliability studies of psychiatric diagnosis. Arch. Gen.
Psychiatry 38, 408–413.
Gur, R.C., Erwin, R.J., Gur, R.E., Zwil, A.S., 1992. Facial emotion
discrimination: II. Behavioral findings in depression. Psychiatry
Res. 42, 241–251.
Hale, W.W., 1998. Judgment of facial expressions and depression
persistence. Psychiatry Res. 80, 265–274.
Hamilton, M., 1960. A rating scale for depression. J. Neurol.
Neurosurg. Psychiatry 23, 56–62.
Harkness, K.L., Sabbagh, M.A., Jacobson, J.A., Chowdrey, N.K.,
Chen, T., in press. Enhanced accuracy of mental state decoding
in dysphoric college students. Cognition Emotion.
Inoue, Y., Tonooka, Y., Yamada, K., Kanba, S., 2004. Deficiency
of theory of mind in patients with remitted mood disorder.
J. Affect. Disord. 82, 403–409.
Janssen, I., Krabbendam, L., Jolles, J., van Os, J., 2003. Alterations
in theory of mind in patients with schizophrenia and non-
psychotic relatives. Acta Psychiatr. Scand. 108, 110–117.
Kelemen, O., Rita, E., Miklosne, P., Szaboles, K., Zoltan, J., 2003.
The relationship between btheory of mindQ and IQ in patients
with schizophrenia. Psychiatr. Hung. 18, 95–98.
Kerr, N., Dunbar, R.I., Bentall, R.P., 2003. Theory of mind deficits
in bipolar affective disorder. J. Affect. Disord. 73, 253–259.

L. Lee et al. / Journal of Affective Disorders 86 (2005) 247–258258
Kington, J.M., Jones, L.A., Watt, A.A., Hopkin, E.J., Williams, J.,
2000. Impaired eye expression recognition in schizophrenia.
J. Psychiatr. Res. 34, 341–347.
Kleinman, J., Marciano, P.L., Ault, R.L., 2001. Advanced theory of
mind in high-functioning adults with autism. J. Autism Dev.
Disord. 31, 29–36.
Langdon, R., Coltheart, M., Ward, P.B., Catts, S.V., 2002. Disturbed
communication in schizophrenia: the role of poor pragmatics
and poor mind-reading. Psychol. Med. 32, 1273–1284.
Levendosky, A.A., Okun, A., Parker, J.G., 1995. Depression and
maltreatment as predictors of social competence and social
problem-solving skills in school-age children. Child Abuse
Neglect 19, 1183–1195.
Lundh, L.G., Ost, L.G., 1996. Recognition bias for critical faces in
social phobics. Behav. Res. Ther. 34, 787–794.
Mandal, M.K., Bhattacharya, B.B., 1985. Recognition of facial
affect in depression. Percept. Mot. Skills 61, 13–14.
Mazza, M., De Risio, A., Surian, L., Roncone, R., Casacchia, M.,
2001. Selective impairments of theory of mind in people with
schizophrenia. Schizophr. Res. 47, 299–308.
Nezlek, J.B., Hampton, C.P., Shean, G.D., 2000. Clinical depres-
sion and day-to-day social interaction in a community sample.
J. Abnorm. Psychol. 109, 11–19.
Oguz, K., Rita, E., Miklosne, P., Szabolcs, K., Zoltan, J., 2003. The
relationship between btheory of mindQ and IQ in patients with
schizophrenia. Psychiatr. Hung. 18, 95–98.
Persad, S.M., Polivy, J., 1993. Differences between depressed
and nondepressed individuals in the recognition of and
response to facial emotional cues. J. Abnorm. Psychol. 102,
358–368.
Pickup, G.J., Frith, C.D., 2001. Theory of mind impairments in
schizophrenia: symptomatology, severity and specificity. Psy-
chol. Med. 31, 207–220.
Rehm, L.P., O’Hara, M.W., 1985. Item characteristics of the
Hamilton rating scale for depression. J. Psychiatr. Res. 19,
31–41.
Reinecke, M.A., DuBois, D.L., Schultz, T.M., 2001. Social problem
solving, mood, and suicidality among inpatient adolescents.
Cogn. Ther. Res. 25, 743–756.
Richell, R.A., Mitchell, D.G., Newman, C., Leonard, A., Baron-
Cohen, S., Blair, R.J., 2003. Theory of mind and psychopathy:
can psychopathic individuals read the dlanguage of the eyesT?Neuropsychologia 41, 523–526.
Rippere, V., 1980. What makes depressed people feel worse? Behav.
Res. Ther. 18, 87–97.
Rubinow, D.R., Post, R.M., 1992. Impaired recognition of affect in
facial expression in depressed patients. Biol. Psychiatry 31,
947–953.
Rutherford, M.D., Baron-Cohen, S., Wheelwright, S., 2002. Read-
ing the mind in the voice: a study with normal adults and adults
with Asperger syndrome and high functioning autism. J. Autism
Dev. Disord. 32, 189–194.
Sabbagh, M.A., 2004. Understanding orbitofrontal contributions to
theory-of-mind reasoning: implications for autism. Brain Cogn.
55, 209–219.
Steer, R.A., Beck, A.T., Riskind, J.H., Brown, G., 1987. Relation-
ships between the Beck depression inventory and the Hamilton
psychiatric rating scale for depression in depressed outpatients.
J. Psychopathol. Behav. 9, 327–339.
Swettenham, J.G., Baron-Cohen, S., Gomez, J.C., Walsh, S., 1996.
What’s inside someone’s head? Conceiving of the mind as a
camera helps children with autism acquire an alternative to a
theory of mind. Cogn. Neuropsychiatry 1, 73–88.
Veljaca, K.A., Rapee, R.M., 1998. Detection of negative and
positive audience behaviours by socially anxious subjects.
Behav. Res. Ther. 36, 311–321.
Watson, D., Clark, L.A., 1991. The mood and anxiety symptom
questionnaire. Unpublished manuscript, University of Iowa.
Department of Psychology, Iowa City.
Watson, D., Weber, K., Assenheimer, J.S., Clark, L.A., Strauss,
M.E., McCormick, R.A., 1995. Testing a tripartite model: I.
Evaluating the convergent and discriminant validity of an-
xiety and depression symptom scales. J. Abnorm. Psychol.
104, 3–14.
Weary, G., Edwards, J.A., 1994. Social cognition and clinical
psychology: anxiety, depression, and the processing of social
information. In: Wyer, R.S.J, Srull, T.K. (Eds.), Handbook of
Social Cognition, Basic Processes vol. 1. Lawrence Erlbaum
Associates, Hillsdale, NJ, pp. 289–338.
Zuroff, D.C., Colussy, S.A., 1986. Emotion recognition in
schizophrenic and depressed patients. J. Clin. Psychol. 42,
411–416.