Meningitis and Encephalitis: Diagnostic and … broad differential diagnosis (>100 causes) ......
32
1 Meningitis and Encephalitis: Diagnostic and Management Challenges October 28 th , 2017 Infectious Diseases update 2017 Rodrigo Hasbun, MD MPH FIDSA UT Health Medical School Professor of Medicine Section of Infectious Diseases Objectives & Disclosures Objectives 1) Discuss the management dilemmas in community- acquired meningitis syndromes. 2) Describe the current utilization of cranial imaging and adjunctive dexamethasone in the US. 3) Explore novel technologies and clinical models that could aid physicians in their management of CNS infections. Disclosures: Biomeriaux, Biofire Diagnostics.
-
Upload
truongphuc -
Category
Documents
-
view
231 -
download
3
Transcript of Meningitis and Encephalitis: Diagnostic and … broad differential diagnosis (>100 causes) ......

1
Meningitis and Encephalitis: Diagnostic
and Management Challenges
October 28th, 2017
Infectious Diseases update 2017
Rodrigo Hasbun, MD MPH FIDSA
UT Health Medical School
Professor of Medicine
Section of Infectious Diseases
Objectives & Disclosures
� Objectives
� 1) Discuss the management dilemmas in community-
acquired meningitis syndromes.
� 2) Describe the current utilization of cranial imaging and
adjunctive dexamethasone in the US.
� 3) Explore novel technologies and clinical models that
could aid physicians in their management of CNS
infections.
� Disclosures: Biomeriaux, Biofire Diagnostics.
2
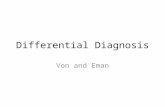
� 37 Hospitals in 20 countries from 2012-2014
� 1504 out of 2583 (58%) of all CNS infections had
unknown etiologies
Aseptic Meningitis
(Wallgren 1925)
� Acute community-acquired syndrome
� with cerebrospinal fluid (CSF) pleocytosis
� in the absence of a positive Gram stain and
culture, without a parameningeal focus or a
systemic illness,
� and with a good clinical outcome
3
4
5
Meningitis with a negative Gram stain is
seen in 94% of patients with CAM.
➤➤➤➤Physician Uncertainty
�A broad differential diagnosis (>100 causes)
�An increasing immunosuppressedpopulation
�Relative lack of experience of physicians with bacterial meningitis
�Lack of recent prospective clinical studies documenting the actual proportion of treatable etiologies
�The majority have unidentified etiologies
.
Hasbun R. Curr Inf Dis Rep 2000, 2:345-351
Solutions
1. To derive and validate a clinical models that identifies a subgroup of patients with meningitis and a negative Gram stain who are at low risk of having an adverse clinical outcome and for an urgent treatable cause.
2. Explore novel molecular diagnostic techniques3. Standardize diagnostic algorithms

6
7
8
Risk Scores in adults with meningitis with
negative Gram stain
� Low risk (<1%) for an adverse clinical outcome in 567
adults if age <60, normal neuro exam and CSF glucose
>45. (Khoury et al. Mayo Clin Proc. 2012 Dec;87(12):1181-8)
� Zero risk (0%) for an urgent treatable etiology in 960
adults if immunocompetent, normal neuro exam and
CSF glucose>45, CSF protein <100 and Serum WBC
<12K. (Hasbun R, et al. Journal of Infection 2013; 67, 102-110)
9

10
Pros and Cons of Film Array
Pros
• Rapid, easy to do, excellent diagnostic accuracy, small sample size (0.2ul), checks for urgent etiologies and etiologies that can help discharge the patient.
• Only multiplex Meningitis Encephalitis panel
Cons
• Does not check for West Nile virus, TB, travel related pathogens (Zika, Toscana, Chickengunyan)
• False positive with S. pneumoniae
� Advantages
� Unbiased
� Rapid
� CSF or brain tissue
� Disadvantages
� Cost
� Contamination and
latent organisms
� Availability
Next-generation
Sequencing
Samia N. Naccache et al. Clin Infect Dis. 2015;60:919-923

11
Clinical CourseNext-generation
sequencing
Wilson MR et al. NEJM 2014;370:2408-2417
12
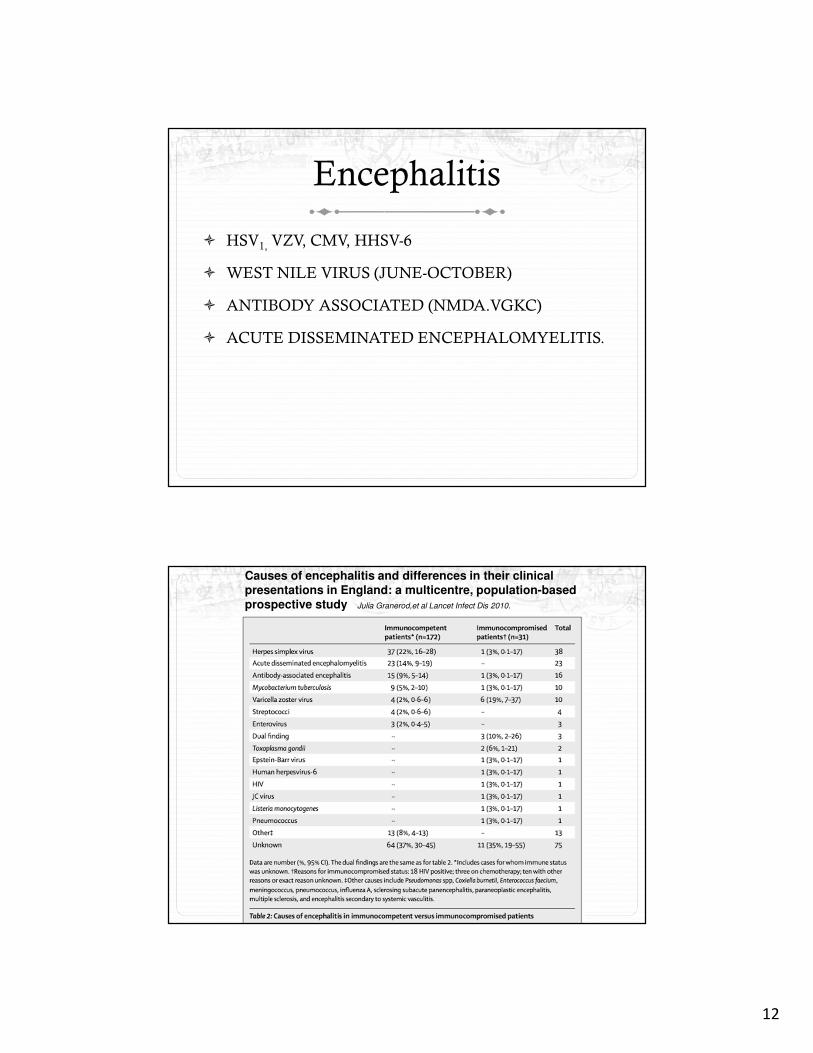
Encephalitis
� HSV1, VZV, CMV, HHSV-6
� WEST NILE VIRUS (JUNE-OCTOBER)
� ANTIBODY ASSOCIATED (NMDA.VGKC)
� ACUTE DISSEMINATED ENCEPHALOMYELITIS.
Causes of encephalitis and differences in their clinicalpresentations in England: a multicentre, population-basedprospective study Julia Granerod,et al Lancet Infect Dis 2010.
13
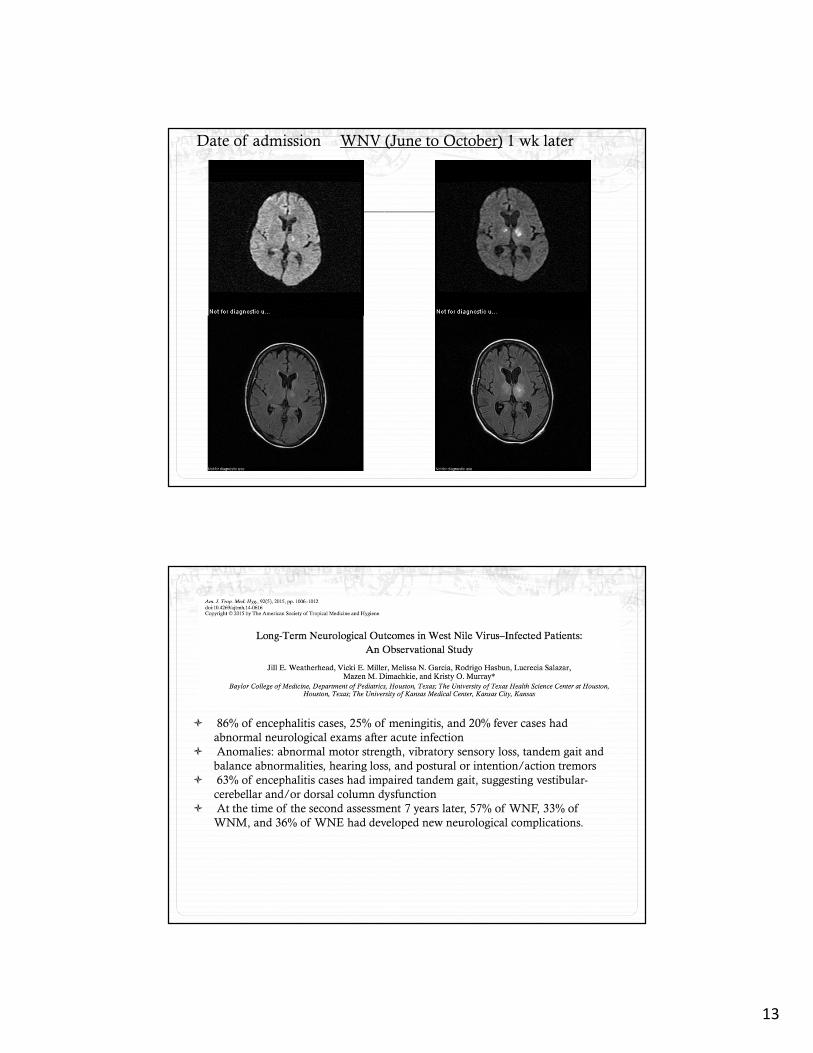
Date of admission WNV (June to October) 1 wk later
� 86% of encephalitis cases, 25% of meningitis, and 20% fever cases had
abnormal neurological exams after acute infection
� Anomalies: abnormal motor strength, vibratory sensory loss, tandem gait and
balance abnormalities, hearing loss, and postural or intention/action tremors
� 63% of encephalitis cases had impaired tandem gait, suggesting vestibular-
cerebellar and/or dorsal column dysfunction
� At the time of the second assessment 7 years later, 57% of WNF, 33% of
WNM, and 36% of WNE had developed new neurological complications.
14
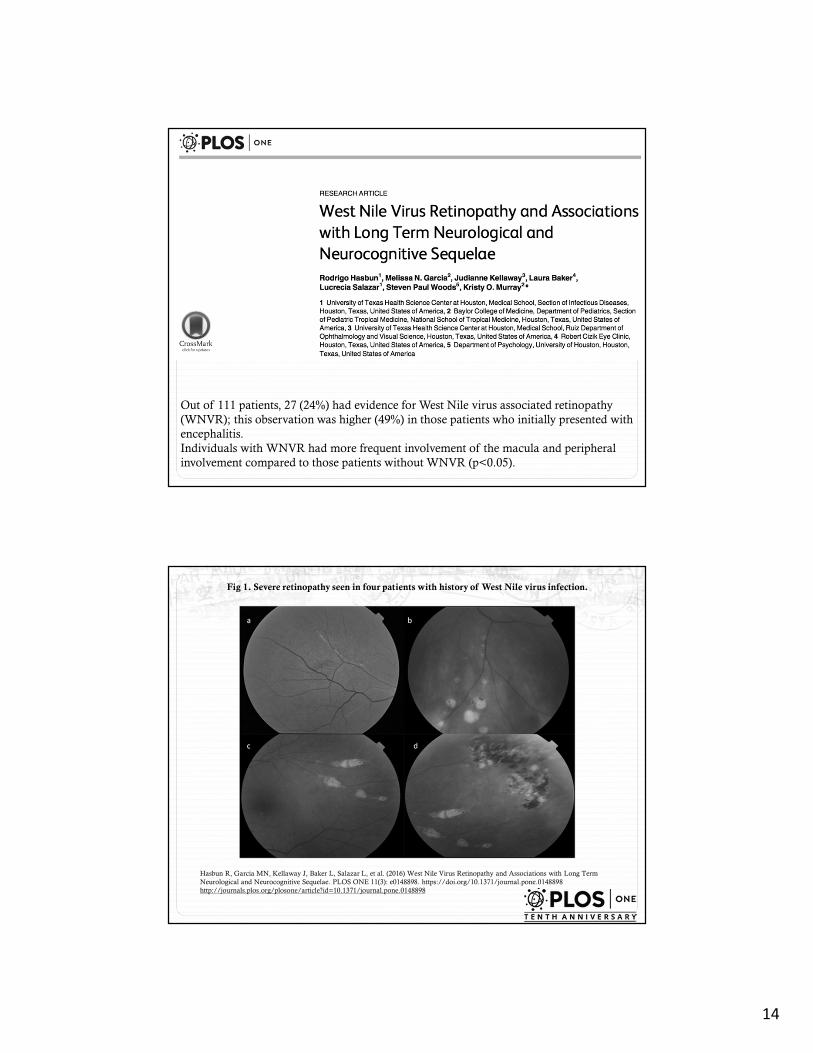
Out of 111 patients, 27 (24%) had evidence for West Nile virus associated retinopathy
(WNVR); this observation was higher (49%) in those patients who initially presented with
encephalitis.
Individuals with WNVR had more frequent involvement of the macula and peripheral
involvement compared to those patients without WNVR (p<0.05).
Fig 1. Severe retinopathy seen in four patients with history of West Nile virus infection.
Hasbun R, Garcia MN, Kellaway J, Baker L, Salazar L, et al. (2016) West Nile Virus Retinopathy and Associations with Long Term
Neurological and Neurocognitive Sequelae. PLOS ONE 11(3): e0148898. https://doi.org/10.1371/journal.pone.0148898
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0148898

15
Table 3. Neurocognition, fatigue, depression and activities of daily living in WNV retinopathy.
Hasbun R, Garcia MN, Kellaway J, Baker L, Salazar L, et al. (2016) West Nile Virus Retinopathy and Associations with Long Term
Neurological and Neurocognitive Sequelae. PLOS ONE 11(3): e0148898. https://doi.org/10.1371/journal.pone.0148898
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0148898
Table 4. Bivariate analyses and Logistic Regression Analysis of Factors Associated with WNV
Retinopathy.
Hasbun R, Garcia MN, Kellaway J, Baker L, Salazar L, et al. (2016) West Nile Virus Retinopathy and Associations with Long Term
Neurological and Neurocognitive Sequelae. PLOS ONE 11(3): e0148898. https://doi.org/10.1371/journal.pone.0148898
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0148898
16
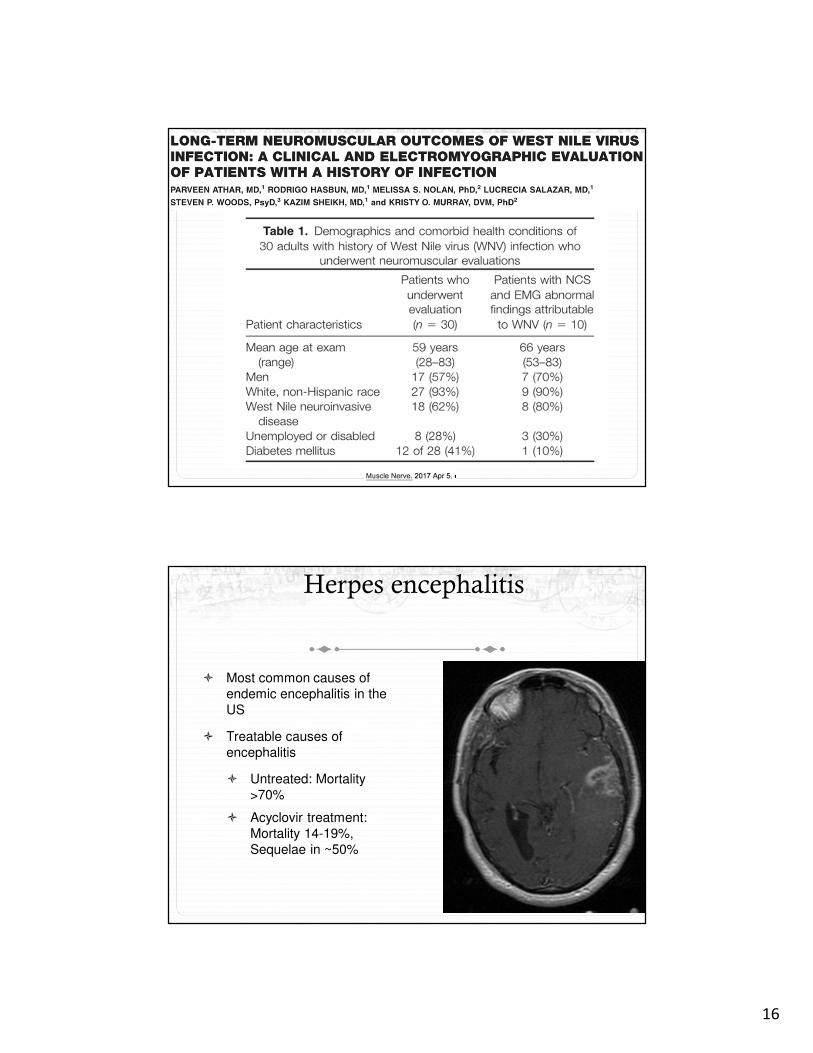
Herpes encephalitis
� Most common causes of
endemic encephalitis in the
US
� Treatable causes of
encephalitis
� Untreated: Mortality
>70%
� Acyclovir treatment:
Mortality 14-19%,
Sequelae in ~50%

17
Adjunctive Valacyclovir for HSE
� Outcome:
� Primary: Mattis Dementia rating
scale (MDRS) at 12 months
� No difference in primary or 2ndary
outcomes
Gnann JW et al. Clin Infect Dis 2015;61:683-691.
18
The frequency of autoimmune N-methyl-D-aspartate receptor encephalitis
surpasses that of individual viral etiologies in young individuals enrolled in
the California Encephalitis Project.
Gable MS, Sheriff H, Dalmau J, Tilley DH, Glaser CA.Clin Infect Dis. 2012 Apr;54(7):899-904.
� 65% of anti-NMDAR encephalitis occurred in patients
aged <18 years.
� This disorder demonstrated a predilection for females,
seizures, language dysfunction, psychosis, and EEG
abnormalities more frequent in patients with anti-
NMDAR encephalitis and autonomic instability
(P<0.05) c/w viral etiologies.
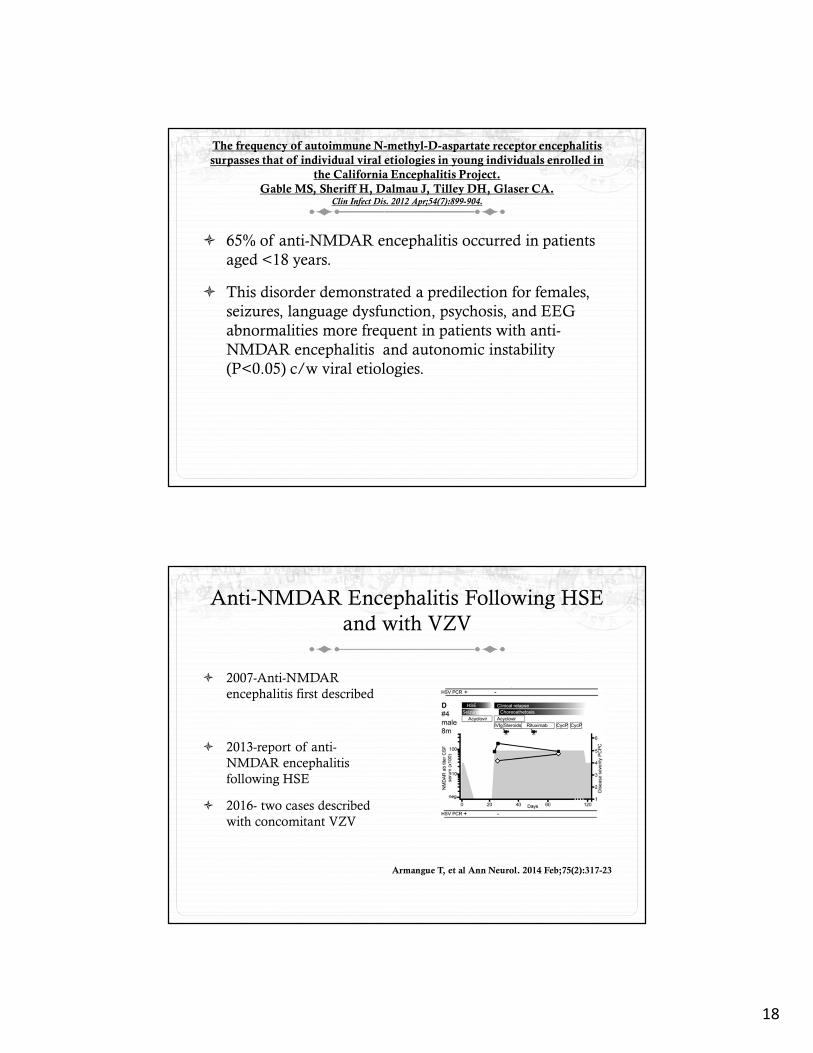
Anti-NMDAR Encephalitis Following HSE
and with VZV
� 2007-Anti-NMDAR
encephalitis first described
� 2013-report of anti-
NMDAR encephalitis
following HSE
� 2016- two cases described
with concomitant VZV
Armangue T, et al Ann Neurol. 2014 Feb;75(2):317-23
19
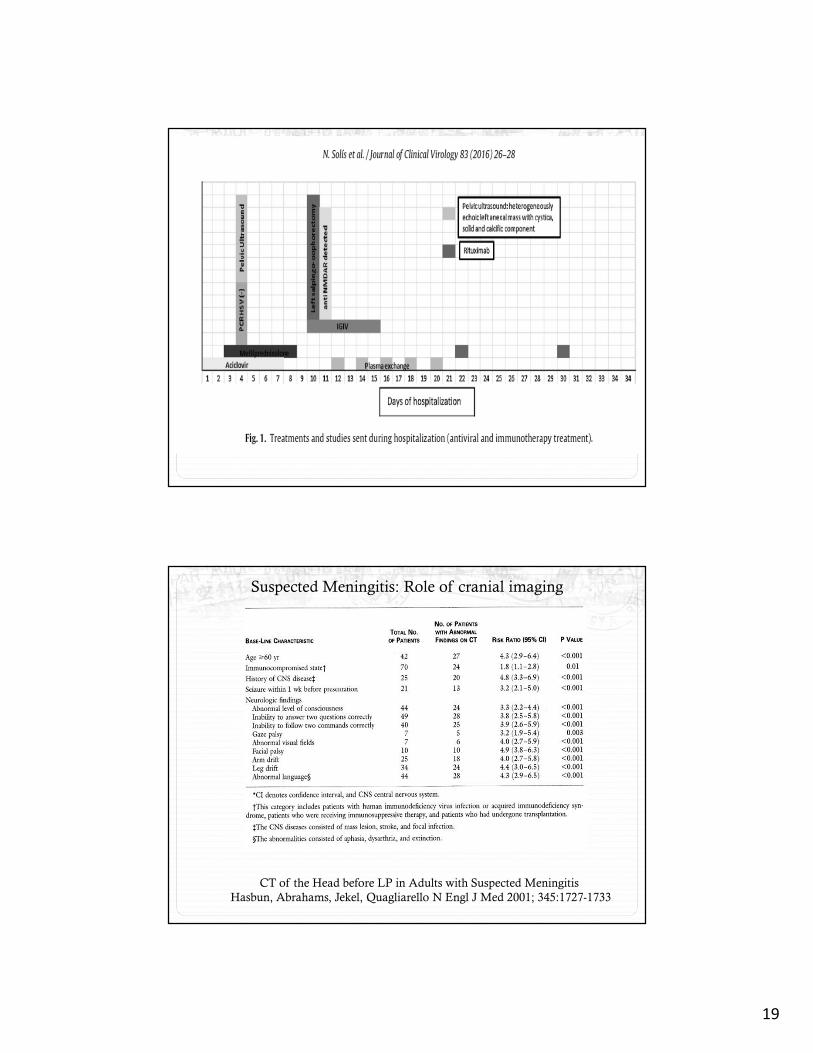
Suspected Meningitis: Role of cranial imaging
CT of the Head before LP in Adults with Suspected Meningitis
Hasbun, Abrahams, Jekel, Quagliarello N Engl J Med 2001; 345:1727-1733

20
IDSA Practice Guidelinesfor the Managementof BacterialMeningitisClin Infec Dis 2004;39:1267-1284

21
22
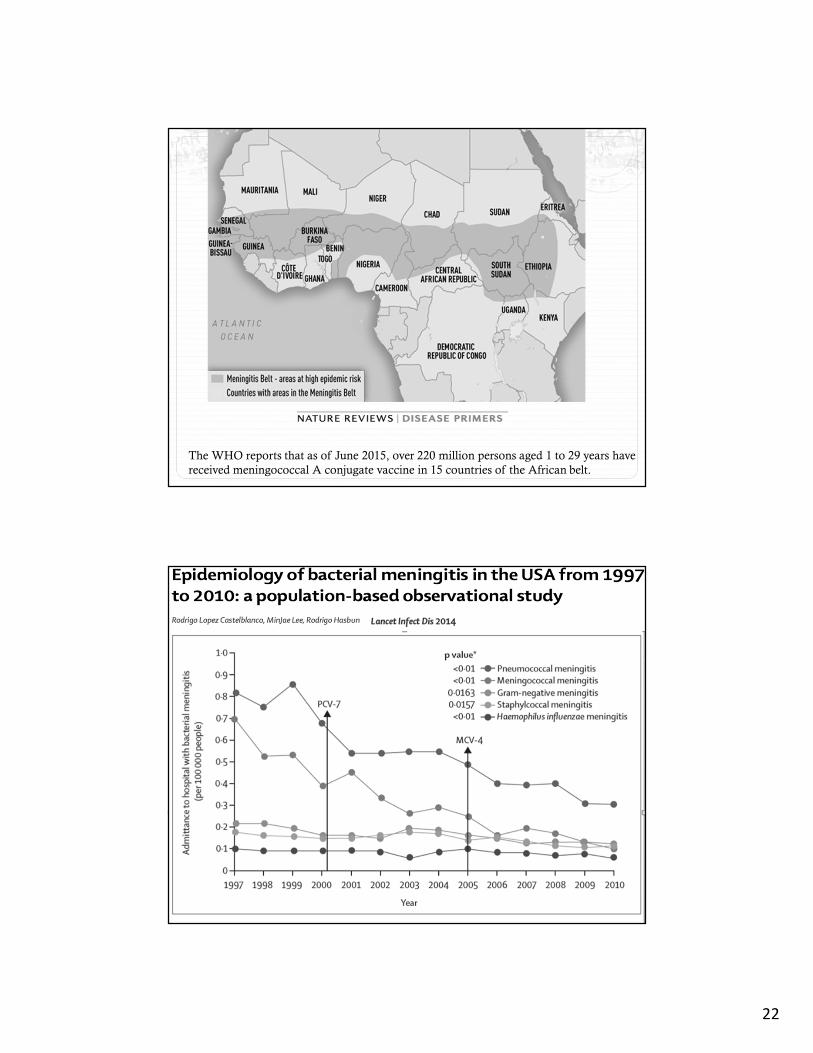
The WHO reports that as of June 2015, over 220 million persons aged 1 to 29 years have
received meningococcal A conjugate vaccine in 15 countries of the African belt.
23

24
Bacterial Meningitis: Mortality
& Antibiotics
Swartz MN. Bacterial meningitis-a view of the past 90 years. N Engl J Med. 2004 Oct 28;351(18):1826-8
Mo
rtali
ty (
%)
S. pneumoniae
N. meningitidis
H. influenzae
Adjunctive dexamethasone� Steroids are the only adjunctive therapy shown to decrease
mortality and hearing loss in high income countries.1,2
� In a European multicenter study, overall mortality decreased from 15% to 7%.3
� In patients with pneumococcal meningitis, mortality decreased from 34% to 14%.3
2M. Glimåker et al. Clinical Microbiology and Infection, 2016
3J.De Gans et al. N Engl J Med, 2002
25
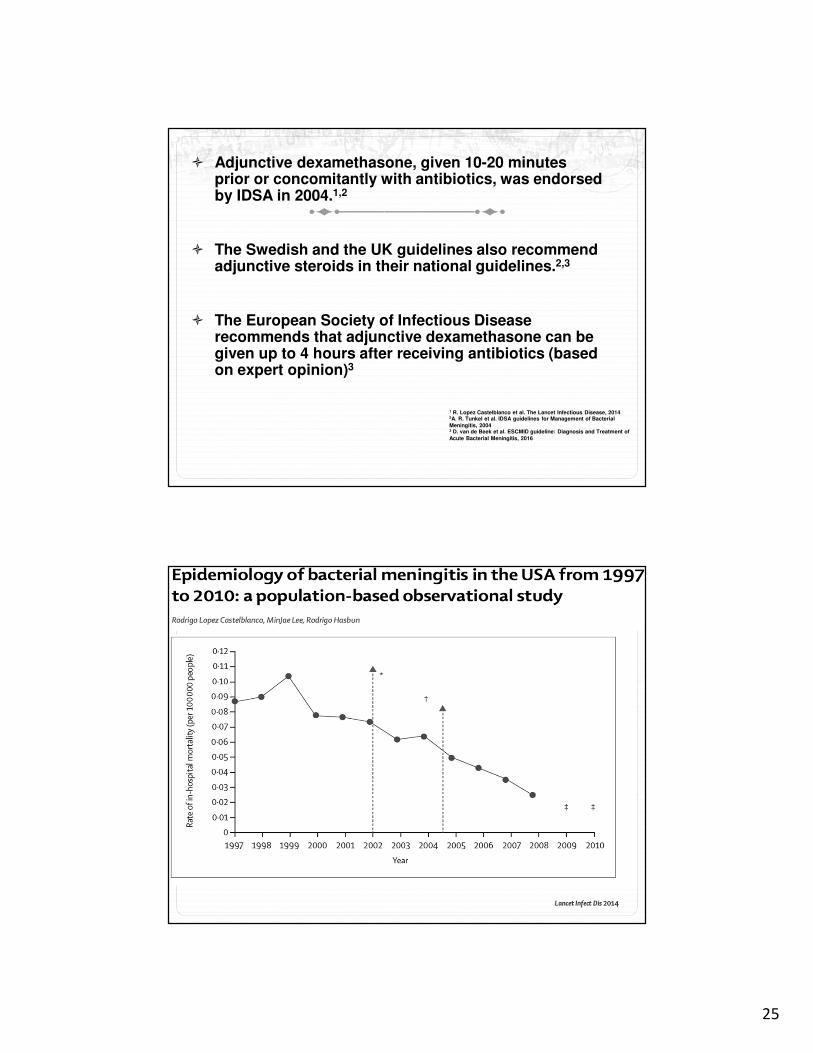
� Adjunctive dexamethasone, given 10-20 minutes prior or concomitantly with antibiotics, was endorsed by IDSA in 2004.1,2
� The Swedish and the UK guidelines also recommend adjunctive steroids in their national guidelines.2,3
� The European Society of Infectious Disease recommends that adjunctive dexamethasone can be given up to 4 hours after receiving antibiotics (based on expert opinion)3
1 R. Lopez Castelblanco et al. The Lancet Infectious Disease, 20142A. R. Tunkel et al. IDSA guidelines for Management of Bacterial Meningitis, 20043 D. van de Beek et al. ESCMID guideline: Diagnosis and Treatment of Acute Bacterial Meningitis, 2016

26
Netherlands1 Sweden2 Denmark3 USA4
Studyduration
2006-2014 1995-2014 2003-2010 2011-2014
Number of patients
1391 1746 147 3692
Overall Steroid use
(%)
89% 56.6% 73%* 30.36%
Steroids ** 78% unk unk unk
1M. Bijlsma et al. The Lancer Infectious Disease, 2016
**steroids given before of with first dose of antibiotics
2M. Glimåker, Clinical Microbiology and Infection, 2016
4Hasbun et al, Clinical Infectious Disease 2017
3G Baunbæk-Knudsen, Infectious Diseases 2016
*steroids given within 1 hour

27
Concerns with use of steroids� Can adequate levels of vancomycin in CSF be obtained in those
treated with steroids? Yes1
� Increased hippocampal apoptosis in rats. On autopsy, no difference was seen in patients who had received dexamethasone and those who did not.2
� Delayed cerebral thrombosis (DCT)
� One study found a 1% incidence of DCT.3
� Possible mechanisms include increased C5a and C5b-9 levels in CSF and increased tissue factor/factor VII pathway3,4
1 J.D Ricard et al, Clinical Infectious Disease 2007
3 M. J. Lucas et al, Intensive Care Med, 20134E.S. Schut et al, Neurology 2009
2 J.Y Engelen-Lee et al Acta Neuropathologica Communications, 2016
Results
� 48 out of 120 (40%) patients were given steroids within 4 hours of antibiotic administration.
� 17 out of 120 (14.1%) received steroids 10-20 minutes prior or at the same time as antibiotics as per the IDSA 2004 guidelines.
� The median duration of steroids was 4 days.

28
Delayed Cerebral Thrombosis (DCT)
� DCT was seen in 5/120 (4.1%) of our patients
� S pneumoniae (3), MRSA (1), Listeria (1).
� 5/5 (100%) of patients with DCT and 43/115 (37.4%) of patients without DCT received steroids within 4 hours of antibiotics. p= 0.01.
� 4/5 patients had an adverse clinical outcome with 2 deaths.
ID Week 2017
ID Week 2017
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5
Sex Female Male Male Female Male
Age 49 63 26 69 31
Organism Streptococcus
pneumoniae
Streptococcus
pneumoniae
Streptococcus
pneumoniae
MRSA Listeria
monocytogenes
Steroids Dexamethasone Dexamethasone/Methylprednisolone
Dexamethasone Dexamethasone Dexamethasone
Timing of thrombosis (days)
12 7 10 5 12
Initial Imaging CT and MRI without evidence of infarction
CT- No acute abnormalities.Encephalomalacia
CT- cerebral edema with no evidence of ischemia
CT and MRI without acuteabnormalities
MRI without evidence ofinfarction
Repeat Imaging MRI- Left frontal cortical vein thrombosis
MRI- multiple acute infarcts in bilateral hemispheres
MRI- multiple acute infarcts in left hemisphere and brain stem
MRI- acute stroke in caudate and anterior internal capsule
Left occipital lobe infarct
Outcome 5 (normal)
1 (death)
3 (severe disability)
1 (death)
4 (moderatedisability)

29
Suspect meningitis in patients with recent neuro-
surgical procedures with new fever, headache,
altered mental status, meningismus, seizures
CSF Profile may be unreliable (e.g., chemical
meningitis)
CSF lactate and procalcitonin level may help
Empiric therapy should be vancomycin and
antipseudomonal cephalosporin/meropenem
Intrathecal therapy should be used for patients
not responding to IV therapy
Removal of devices are very important.
30
Open Forum
ID 2016
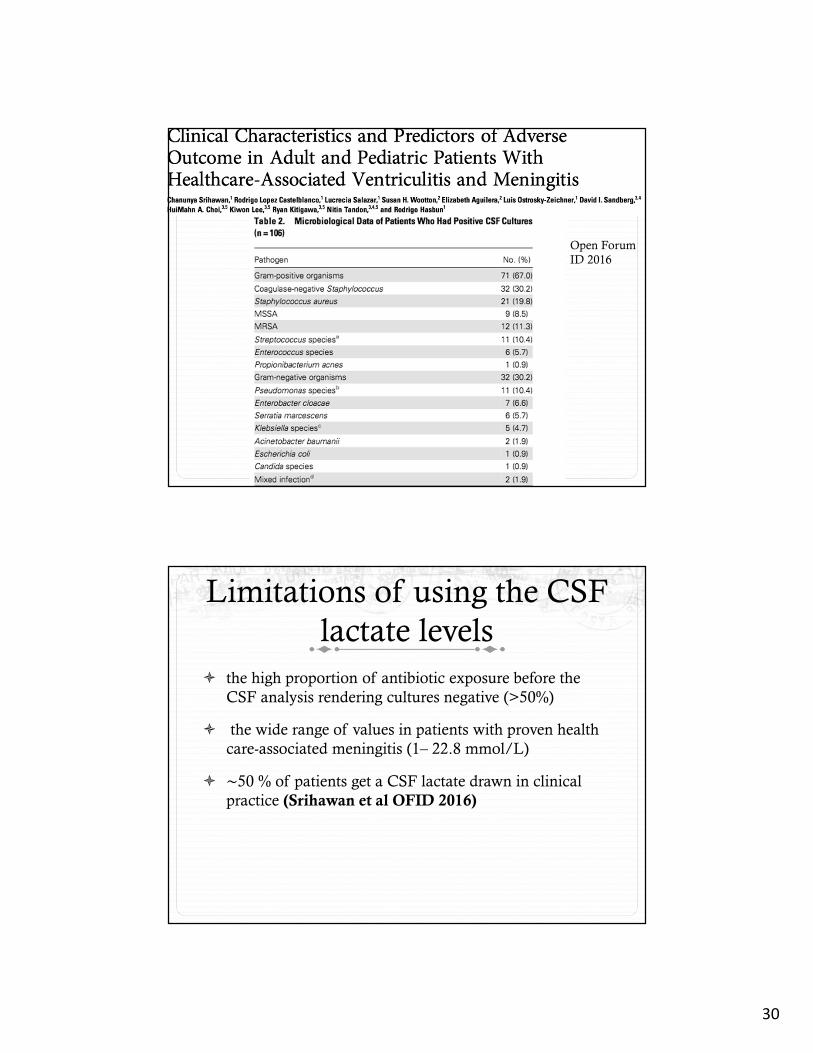
Limitations of using the CSF
lactate levels
� the high proportion of antibiotic exposure before the
CSF analysis rendering cultures negative (>50%)
� the wide range of values in patients with proven health
care-associated meningitis (1– 22.8 mmol/L)
� ∼50 % of patients get a CSF lactate drawn in clinical
practice (Srihawan et al OFID 2016)

31
Removal of devices
� Removal of the infected CSF shunt, external ventricular
drain, intrathecal infusion pump, or deep brain stimulator
with re-implantation of the device once repeat negative
CSF cultures is key.
� In CSF shunt infections, lack of removal of the shunt is
associated with a successful outcome only in 35 % of
patients with high mortality, immediate shunt removal and
reinsertion in 65–75 %, and shunt removal with a delayed
reimplementation in more than 85 % of patients. (J Hosp
Infect. 2016;93(4):323–8)
OFID 2016

32
This study included 120 patients with ICH; 40 patients also had HCAMV,
whereas 80 patients had ICH with no evidence of HCAMV.