
Medin Amyloid in Human Arteries and its Association with ...167986/FULLTEXT01.pdf · ACTA...
56
ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2006 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 129 Medin Amyloid in Human Arteries and its Association with Arterial Diseases SIWEI PENG ISSN 1651-6206 ISBN 91-554-6507-2 urn:nbn:se:uu:diva-6700
Transcript of Medin Amyloid in Human Arteries and its Association with ...167986/FULLTEXT01.pdf · ACTA...

ACTA
UNIVERSITATIS
UPSALIENSIS
UPPSALA
2006
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 129
Medin Amyloid in Human Arteriesand its Association with ArterialDiseases
SIWEI PENG
ISSN 1651-6206ISBN 91-554-6507-2urn:nbn:se:uu:diva-6700

���������� �������� �� ������ �������� � �� �������� ������� � ������� ����� ����������� ��������� ������� ��������� ����� !� ""# �� "$%�& '� ��� ��(��� ' ���� ')������� *+������ ' ,������-. ��� �������� /��� �� ������� � 0(����.
��������
)�(� 1. ""#. ,��� ������ � ���� �������� �� ��� �������� /��� �������� ��������.���� ����������� ���������. ������� ��� � ���� ����� � � ������� ���� ��������� �� ������� � � ����� � $. 2" ��. ������. 3145 $�6&&26#&"!6 .
������ �� � '�� ' ������ ����� �((��(��� /���� ��� ����( ���. ,������ ��������� ���� � �(� '������. ����� �� ��� �������( ������� ���� ������� ���6�������((��(���� ����� ������ ���� �''���� � �����. � ���� & ��''���� ������ ��� �/ � ������ ������ ������� � ���� �������� �����(� � ��� ' ����� ������ ��� �/ � ����������� /��� ������� ��������.���� ������ ����� /��� ��� ���� ��� '�� ' ������ �����7�� � ��� �������� �����.
��� '����� ����� ������ 8����9 /�� �����'��� � �$$$. ,��� �� � &" ��� ���� ������������� '��(��� ' ��� �������� ����� ����������. ����������� '���� '�� � ���� ������� ��������� � ������ ������� ���� �� ������ ���������� *������( ��������-� �������(���� ����. ��� '���� ' ��� ����� �� � �/ ��� �� ��� ������� '������ �����.����� �� � 0+: ���� ����� ������( � �:�6��;����� � ��� 56������� ���� ' ����������. ��� �6������� ���� ������ ' �� �� � ��(����� '���� < �� <333 ���������. ,��� �� '�� /���� ��� � ����. ���� ��(� �� ��((����� � �� ������ ������������ ����� ����(� ������� � ���(������ ' ������� �����.,��� ������ /�� ��(����� ��������� '�� ������� ' ��� ����. 3� �� ��/ ���� ����
������� ��� ��� /����� ������ �� �� �� '�� � ��� ���(� ��������� ������������ /������� ����� ���� ' ��� ���. ��� ��������� ' ���� ������ �������� /��� �(� �� ���������� '��� � � ������ ��(���� � ��������� ������ ���� ��� �(� ' #" �����. ��� ������ ��� �� '�� ��������������� ��� ������������ ������� ��� ��� ����. ������ �� ���������������� /��� ������� ����� � �������� /���� '�� ��/ ��(� ' '��(������.:��� ��� �����7��� ' ������ � ������� ���������� ' ��� �������� ������ ����� ��''����
�������� �������� /��� �������% ������� *(��� ����- ���������� ������� ����� ������� ��������� ����� ��������. ,��� ������ /�� '�� � ������� �������� /��� �� /������'�������. 3 �'����� ��������� ������ /�� ����� ������ ��( ��� ���� ������������� �����. ,��� /�� ��� ���������� /���� (��� �����. 3� �� ��((����� ���� ���� ����� � ���(� ���((���( �������� (��� ���� ���������. 3 ��� ����� ' ������� ������������� �� ���������� /� '�� ��(�'���� ���� ���� ������ � �������� ����� �������������� /��� � ���� ��������. = ��� ���� ���� ������������ ����� ������� � �������� ' ��(����� �((��(����� /�� ��(������ '�� � �������� /��� �������� ����������� ��� � � ��� ���� ��������. 3� �� ��((����� ���� ���� ��(���� ����� �����''���� ���� ������ ����� /���� ��� ���� � /�����( ' ��� �������� /��� /���������� � �������� �� � ���;����.
� ������ ������� ,���� ����������� �������� ����� ��������� ������� ����������������� :��� ����� )��6�((��(���.
��� � � ��� � ���� �� � � ���� ��� �������� !��" �#��"����� �� ����������� ������ �$%&'()' �������� �� � �
> 1�/�� )�( ""#
3115 �#&�6# "#3145 $�6&&26#&"!6 ��%�%��%��%����6#!"" *����%??��.��.��?������@��A��%�%��%��%����6#!""-

To my family


List of Papers
This thesis is based on the following papers, which will be referred to in the text by their Roman numerals.
I. Peng, S., Westermark, T.G., Näslund, J., Häggqvist, B., Glennert, J., Westermark, P. (2002) Medin and medin-amyloid in ageing inflamed and non-inflamed temporal arteries. Journal of Pathology, 196: 91-6
II. Peng, S., Glennert, J., Westermark, P. (2005) Medin-amyloid: a recently characterized age-associated arterial amyloid form affects mainly arteries in the upper part of the body. Amyloid, 12: 96-102
III. Peng, S., Persson, A., Wassberg, E., Gerwins, P., Thelin,S., Westermark, P. Medin and medin-amyloid in thoracic aortic aneurysm and dissection. (manuscript)
IV. Peng, S., Wassberg, E., Gerwins, P., Thelin, S., Westermark, P. Intracellular amyloid-like medin peptide aggregation in the aging human thoracic aorta.(manuscript)
Reprints were made with the permission of the publishers.


Contents
Introduction ..........................................................................................13Protein folding and misfolding ...........................................................15Amyloid in general............................................................................16Amyloid pathogenesis .......................................................................16
Extracellular amyloid formation hypothesis ....................................16Intracellular amyloid formation hypothesis .....................................17Prefibril aggregation and toxicity ...................................................18
How do amyloid deposits develop and spread?....................................19Classification and diagnosis of amyloid diseases .................................19Amyloid in human arterial walls .........................................................20
Amyloid in aortic intima associated with atherosclerotic plaques......21Amyloid in the aortic media ...........................................................21
Lactadherin and the nature of the amyloid in the aortic media ...............22Formation of medin ...........................................................................23The human artery..............................................................................23Cardiovascular diseases.....................................................................24
Temporal arteritis ..........................................................................24Thoracic aorta aneurysm and aorta dissection..................................25
Aims of present investigation .................................................................27
Materials ...............................................................................................28Tissues .............................................................................................28
Medin amyloid in the temporal artery (paper I) ...............................28Medin amyloid deposition in different arteries in the human body (paper II)......................................................................................28Medin amyloid in human thoracic aorta aneurysms and dissections (paper III + paper IV)....................................................................28Antibodies against lactadherin .......................................................29
Methods ................................................................................................30Demonstration of amyloid..................................................................30Immunological methods .....................................................................30Electron microscopy ..........................................................................31Protein pur ification............................................................................31Electrophoresis and western blotting...................................................31

In situ hybridization...........................................................................32
Results and Discussion...........................................................................33Medin amyloid in temporal artery and its association with giant cell arteritis (paper I)................................................................................33Medin amyloid distribution (paper II) .................................................34Importance of medin in the pathogenesis of thoracic aortic aneurysm and dissection (paper III)..........................................................................35Intracellular amyloid (papers II-IV)....................................................36
General discussion and future perspectives..............................................38
Acknowledgements ...............................................................................40
References ............................................................................................42

Abbreviations
AA Amyloid protein AAANF Amyloid atrial natriuretic factorAApoA-I Amyloid apolipoprotein A-IAApoA-II Amyloid apolipoprotein A-IIABri Amyloid Bri polypeptideAß Amyloid betaAß2M Amyloid ß2-microglobulinACal Amyloid procalcitoninACys Amyloid cystatin CAFib Amyloid fibrinogen a -chainAGel Amyloid gelsolinAH Amyloid heavy chainAIAPP Amyloid islet amyloid polypeptideAIns Amyloid insulinAKep Amyloid keratoepithelinAL Amyloid light chainALys Amyloid lysozymeAMed Amyloid medinApoE Apolipoprotein EAPro Amyloid prolactinAPrP Amyloid prion proteinATTR Amyloid transthyretinBNF Buffered neutral formalinDTT DithiothreitolEGF Epidermal growth factorER Endoplasmic reticulumESRF End-stage renal failurekDa kilo DaltonMFG-E8 Milk fat globule-EGF (epidermal growth Factor) 8MMP Matrix metalloproteinasePAGE Polyacrylamide gel electrophoresisRGD Arginine-glycine-aspartic acidSAA Serum amyloid ASAP Serum amyloid P componentSDS Sodium dodecylsulfate


13
Introduction
With increasing longevity, aging problems and diseases are coming more into focus. Amyloidosis is one of the most common senile pathological con-ditions found in association with many age-associated diseases, and can affect different organs. The various forms of amyloidosis represent a group of protein conformational diseases, characterized by aggregation of small protein molecules in a ß-sheet anti-parallel organization.1,2 In medicine, the term ‘amyloid’ was first used by the German pathologist Rudolf Virchow in18543 when he used iodine staining to identify cellulose-like materials at autopsies. Obviously Virchow realized that the iodine-reacting material he found was not cellulose or starch, since he used the name amyloid, which means starch-like. Since then, the knowledge of amyloid grew slowly until 1959, when it was shown that all types of amyloid are actually fine, non-branching protein fibrils.4 In the early 70’s, there came a real break-throughin understanding the nature of amyloid. First, it was shown that the amyloid fibril consists of protein molecules, arranged in cross-ß-sheets. Second, sev-eral of these amyloid proteins were characterized. The first two amyloid proteins characterized were protein AA5,6 (in secondary systemic amyloido-sis) and protein AL7 (in primary and myeloma-associated amyloidosis), fol-lowed by calc itonin and transthyretin. Later, some amyloid proteins known to be associated with some important diseases such as Alzheimer’s disease and type 2 diabetes were characterized.8-12 Todate, more than 25 proteins have been found to form amyloid fibrils in human (Table 1),13 and the num-ber keeps increasing, although not all of them have been shown to be clin i-cally important.

14
Table 1. Nomenclature and classification of amyloidoses.Amyloid protein Precursor Distribution Syndrome(s)
AL Ig light chain (?, ?) G, L Primary, or associated with myeloma
AH Ig heavy chain (?) G, L Primary, or associated with myeloma
AA ApoSAA G (secondary) Infec-tions,chronic inflammation, tumors,familial Mediterra-nean fever,Muckle–Wellssyndrome
ATTR Mutant transthyretin G HereditaryATTR Normal transthyretin G Senile systemic amyloidosisAß 2M ß2-microglobulin G Associated with chronic
ESRFAApoA-I Apolipoprotein A-I G, L Hereditary aortic intimaAApoA-II Apolipoprotein A-II G HereditaryAGel Gelsolin G HereditaryALys Lysozyme G HereditaryACys Cystatin C G Hereditary cerebral
hemorrhageAß Aß precursor protein
(AßPP)L Alzheimer's disease, trisomy
21 angiopathy, hereditary or sporadic cerebral amyloido-sis
APrP PrP L Spongiformencephalopathies
ACal Procalcitonin L Thyroid medullary cancerAANF Atrial natriuretic factor L Isolated atrial amyloidosisAIAPP Islet amyloid
polypeptideL Diabetes type 2, insulinoma
AIns Insulin L IatrogenicAFib Fibrinogen a-chain G HereditaryAPro Prolactin L Senile hypophyseal;
prolactinomaABri ABriPP L Familial British dementiaAKer Keratoepithelin L Lattice dystrophies of the
corneaA-Pin Un-named protein L Odontogenic (Pindborg)
tumorsAMed Lactadherin L Aortic (media)ALac Lactoferrin L Cornea FamilialG: Generalized; L: Localized, ESRF: End-Stage Renal Failure

15
Protein folding and misfoldingIn the human body, there are about 50,000 heterogeneous functional pro-teins according to the Human Genome Sequencing Project.14,15 Proteins are one of the most fundamental elements involved in the lifecycle. Their bio-logical functions depend on their correct native structures which, in general, are complex 3-D structures. Correct folding, as well as clearance of mis-folded proteins, is crucial steps for living organisms of all kinds.
Proteins are first assembled on ribosomes according to the mRNA code. After being modified in the endoplasmic reticulum (ER) or Golgi, these proteins remain or are released from the cells, to exert their biological func-tions. Protein folding procedures normally take place in the ER. Specific amino acid sequences determine protein folding structure,16 but the whole procedure follows protein kinetic and thermodynamic stability laws.17-19
When abnormal proteins are formed, they normally are cleared and de-graded. Factors such as aging and environmental stress may make chaper-one systems insufficient, allowing proteins to misfold and aggregate. Simi-larly, proteins outside cells can also be controlled by chaperone systems. Insufficient chaperone systems may result in accumulation of misfolded proteins which may subsequently form amyloid aggregation, as shown in Figure 1.
Figure 1. Protein processing procedure.

16
Amyloid in generalMutations associated with amino acid substitutions, as well as misfolding of wild type proteins, can make the proteins less soluble under physiological conditions, and induce aggregation and amyloid formation in certain tissues or organs. Amyloid proteins are heterogeneous, nevertheless they form the same ß-sheet rich fibrils and these fibrillar aggregates share certain specific characteristics including: 1. Tinctorial properties. Amyloid can be stained with the diazo dye Congo red and subsequently shows green birefringence when examined with polarized light. This property is usually used for clin i-cal diagnostic work. Amyloid can also be stained with the fluorescent dye thioflavin-T.20 2. In the electron microscope, all amyloid deposits are char-acterized by the presence of long, straight, unbranched fibrils which usually are around 100Å in diameter.1,2,4,21-24 3. Amyloid fibrils have a characteristic cross ß-sheet X-ray diffraction pattern.25 The mature amyloid fibril is usu-ally composed of 4-6 parallel protofilaments, and the protofilament is com-posed of the ß-strands oriented perpendicularly to the fiber axis.24,26,27 4. Amyloid deposits contain several common components such as serum amy-loid P component (SAP), apolipoprotein E (apoE) and heparin sulphate pro-teoglycan. Amyloid fibrils are very resistant to proteolysis and all of the above common components are claimed to be involved in the amyloid fibril stability as well as acceleration of amyloid formation.28-33
Amyloid pathogenesis
Extracellular amyloid formation hypothesisAmyloid is classically defined as being extracellular. The mechanisms by which proteins assemble into amyloid fibrils have been studied intensively during the last two decades. When full-length precursor proteins with an ordered secondary and tertiary structure (e.g. lysozyme and transthyretin) are involved in fibrillogenesis, it is believed that intermediates in the folding process constitute the aggregation-prone species.26,34,35 Such species exposesurfaces that may bind to a surface from another identical molecule.36-39 An important mechanism in fibrillogenesis in many amyloid forms is partial proteolysis, which can release a peptide which may be prone to aggregateinto amyloid fibrils.40,41 A classical example of this is the Aß peptide, which is an internal cleavage product of the large precursor protein APP. The Aßpeptide is a 40-42 peptide which is highly fibrillogenic and which is formed by the action of two proteases, the α and ? secretases.41-43 For Aß amyloi-dogenesis, these cleavages are necessary. Many other amyloid fibril proteins are also the result of partial proteolytic processing. Thus, protein AA and
17
protein AL are both usually missing a substantial part of the C-terminal ends of their precursor proteins, serum AA (SAA) and immunoglobulin light chain, respectively.44,45 With these two proteins, however, it is uncertain whether cleavage comes before or after fibrillogenesis.46,47 Thus, it is oftennot clear whether cleavage is important in the fibrillogenic process.
Somehow during the accumulation of the misfolded protein additional molecules are also probably involved in amyloid formation. There are at least three amyloid co-components that are found in the extracellular amy-loid: serum amyloid P component, apolipoprotein E and heparan sulfate proteoglycan. The importance of these in amyloidogenesis is still incom-pletely understood but they are believed to be involved in acceleration of the amyloid formation.27,29,48,49 There is some experimental support for this con-clusion. Mice, not expressing SAP have a delay in the development of ex-perimentally induced AA-amyloidosis50 and over-expression of heparanase, an enzyme which degrades heparan sulfate, also leads to marked reductionin the amount of amyloid in the same type of murine amyloidosis.32
Massive extracellular amyloid deposits conquer the normal structure of a tissue or organ and may result in organ failure. Such alterations can be found in most systemic amyloid diseases and include for example heart or renal failure in AL amyloidosis and heart failure in TTR amyloidosis.
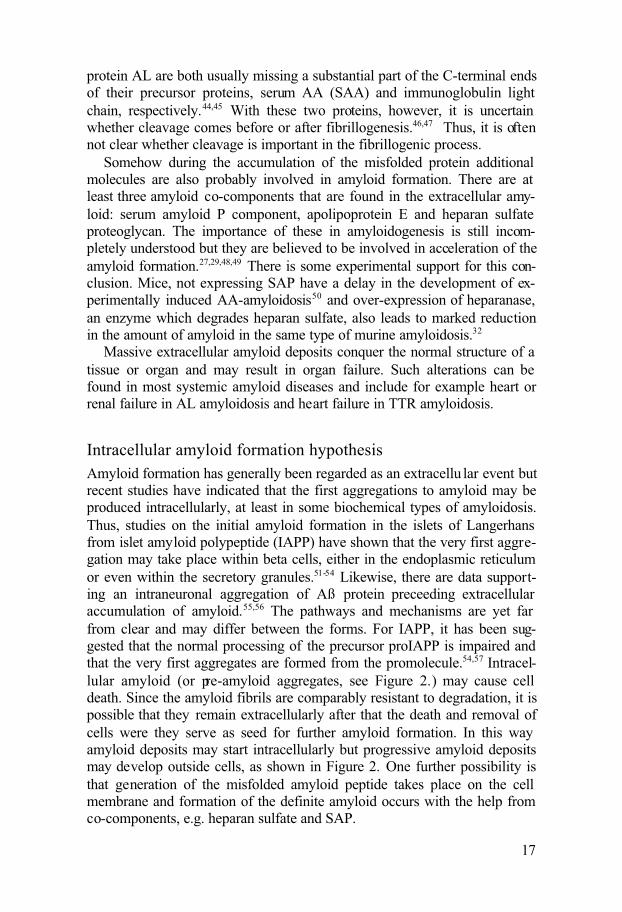
Intracellular amyloid formation hypothesisAmyloid formation has generally been regarded as an extracellu lar event but recent studies have indicated that the first aggregations to amyloid may be produced intracellularly, at least in some biochemical types of amyloidosis. Thus, studies on the initial amyloid formation in the islets of Langerhans from islet amyloid polypeptide (IAPP) have shown that the very first aggre-gation may take place within beta cells, either in the endoplasmic reticulum or even within the secretory granules.51-54 Likewise, there are data support-ing an intraneuronal aggregation of Aß protein preceeding extracellular accumulation of amyloid.55,56 The pathways and mechanisms are yet far from clear and may differ between the forms. For IAPP, it has been sug-gested that the normal processing of the precursor proIAPP is impaired and that the very first aggregates are formed from the promolecule.54,57 Intracel-lular amyloid (or pre-amyloid aggregates, see Figure 2.) may cause cell death. Since the amyloid fibrils are comparably resistant to degradation, it is possible that they remain extracellularly after that the death and removal of cells were they serve as seed for further amyloid formation. In this way amyloid deposits may start intracellularly but progressive amyloid deposits may develop outside cells, as shown in Figure 2. One further possibility is that generation of the misfolded amyloid peptide takes place on the cell membrane and formation of the definite amyloid occurs with the help from co-components, e.g. heparan sulfate and SAP.

18
Figure 2. Amyloid processing procedure.
Prefibril aggregation and toxicityA modern concept is that before amyloid fibrils form, the (misfolded) sub-unit peptides accumulate and assemble into oligomers (or ‘protofibrils’)which are cytotoxic and the direct cause of cell damage.
In the folding-unfolding process that proteins undergo, intermediates may form which are prone to adopt a high degree of beta structure and assemble. Aggregation-prone protein species may also develop from normal peptides with little secondary structure, e.g. IAPP and from peptides hidden in larger molecules and which are released by protease cleavage. Initially, in the pathway towards fully developed fibrils, soluble but still not very well de-fined oligomeric assemblies occur. These oligomers, often referred to as ‘protofibrils’ are now attracting much attention since they may be the spe-cies that are most deleterious to cells. The mature amyloid fibril has instead been suggested to reflect a protective mechanism to take care of and stabi-lize the highly toxic aggregates.58-61 This possibility has important implica-tions for therapeutic strategies since dissolution of fibrils may create more oligomers. How oligomeric assemblies exert their toxicity is still insuffi-ciently understood. They interact with cell membranes and may cause per-meabilization through formation of abnormal pores. Generation of oxidative stress is also probably important. These various mechanisms appear to be universal and shared by many (if not all) oligomeric amyloid fibril protein assemblies and consequences in the different amyloid syndromes depend on which cells are exposed to the aggregates.

19
Much of our knowledge about amyloid protein cytotoxicity is based on studies of the Aß peptide. In addition to induction of toxicity when added to cells in vitro, it has been suggested that Aß may accumulate intracellu larlyin neurons and cause mitochondrial dysfunction and cell death. In addition to Aß , cytotoxic effects of amyloid protein aggregates have been shown for IAPP on beta cells, transthyretin on neuroblastoma cells (in vitro), ADan on neurons and medin on smooth muscle cells.62-66
How do amyloid deposits develop and spread?The initial step in fibril formation is nucleation, i.e. the production of a nu-cleus from which fibrils are elongated.26,36,67 The nature(s) of the nucleus is poorly understood. Some amyloid precursor proteins may, over a variable period of time, form amyloid-like fibrils in vitro. This process is dependent on sufficient concentration and other conditions such as ionic strength and pH. This is the lag phase. If a small amount of pre-formed fibrils are added, the lag phase may be dramatically shortened or almost abolished. Exactly how the added fibrils influence (‘seed’) the protein molecules in solution is not well understood but they may act as a template. It is believed that new, misfolded molecules are added to the ends of the preformed fibrils. Thus, the proposed mechanism resembles that of how prions act.
Most probably, seeding is also the mechanism by which amyloid deposits are spread in the body. Although not shown so far, it is possible that small oligomeric aggregates are transported from one site to another. For the sys-temic amyloidoses, the blood should serve as a spreading medium. Interest-ingly, under certain circumstances and at least experimentally, amyloid is transferable from one animal to another.68-70 When an acute but persistent inflammation is induced in mice, systemic AA-amyloidosis may develop after a lag phase of several weeks. If a tiny amount of an extract of AA-amyloid is given to a mouse at the time of induction of inflammation, amy-loidosis develops within days. The active principle, previously referred to as ‘amyloid enhancing factor’ seems to be the amyloid fibril itself. The same phenomenon has been shown also with another mouse model of systemic amyloidosis (apolipoprotein AII-amyloidosis).71
Classification and diagnosis of amyloid diseasesThere are several ways to classify the amyloidoses. Most commonly, the amyloid forms are grouped as systemic or localized amyloidosis. Systemic amyloidosis, just as its name implies, affects more than one organ of the living body and the deposits are often widely spread. Heart, kidney, liverand peripheral nerves are often affected. These disorders are often lethal.

20
Localized amyloidosis affects only one organ in the body but the amyloid itself has the same appearance as in systemic amyloidosis. Currently, the different types are categorized according to the specific amyloid fibril pro-tein involved. Consequently the former designation ‘primary and myeloma associated amyloid’ is now called AL-amyloidosis (A for amyloid and L for immunoglobulin light chain). Instead of secondary amyloidosis, the name AA-amyloidosis is used (the second A for amyloid protein A). Whether the amyloidosis is systemic or not should also be stated. The different designa-tions are given in Table 1.13
The only safe way to obtain a diagnosis clinically is by identification of amyloid in a biopsy. For systemic amyloidoses, a biopsy from a site, known to contain deposits in most cases is most commonly chosen. Rectal or sub-cutaneous adipose tissue biopsies are usually chosen. Sections of tissue ma-terial or smears of aspiration biopsies are then stained with Congo red and studied in polarized light for green birefringence. There are some alternative staining methods, e.g. with Thioflavine-T or S but these are regarded as less specific and are not commonly used in clinical practice.
Amyloid in human arterial wallsAmyloid inf iltration of blood vessels, particularly arteries, is a hallmark of almost all systemic forms of amyloidosis. Amyloid may also occur as local-ized vascular deposits. Probably most well-known is Aß-amyloid infiltration in brain vessels (sometimes referred to as Congophilic angiopathy), which is one hallmark of Alzheimer’s disease but which also is a common accidental finding in association with ageing. Aß also constitutes the Alzheimer plaque amyloid fibril, which is involved in the cytotoxicity to neurons.72-75 Aß-amyloid may make the vessel wall vulnerable and cause cerebral hemor-rhage.76-79 Intracranial vascular amyloid deposits are also apparent in some other forms of amyloidosis, e.g. amyloidosis derived from cystatine C. This amyloidosis occurs as a familial amyloidosis, first described from Ice-land.80,81
Vascular and particularly arterial deposits are often pronounced in the three most common systemic amyloid forms, AL-, AA- and ATTR- amyloi-doses. These deposits are usually not associated with conspicuous symptoms (if glomeruli are excluded) but may lead to bleedings, e.g. in the skin in AL-amyloidosis and from the urinary bladder in AA-amyloidosis.82,83
Occurrence of small aortic amyloid deposits, not being part of any sys-temic disease, was described decades ago. Deposits were found both in the intima and in the media, and were usually regarded as one entity.84 Later studies showed, however, that the aortic amyloid in the media is a specific entity85 which is biochemically different from amyloid found in the intima.

21
This latter form is mainly seen in conjunction with severe atherosclero-sis.86,87
Amyloid in aortic intima associated with atherosclerotic plaquesThis is a type of localized amyloid which specifically affects atherosclerotic arterial walls. Amyloid deposits do not occur in early plaques but are com-monly seen associated with more advanced atherosclerotic plaques compli-cated with necrosis and calcification.88 In one patient, this amyloid was characterized to be derived from apolipoprotein A1 although it is still not certain that it always has this biochemical composition.87 Whether or not amyloid (or pre-amyloid) is involved in the pathogenesis of atherosclerosis is not known. Interestingly, apolipoprotein A1 gives rise to a common amy-loid form of pulmonary vessels in dogs.87,89
Amyloid in the aortic mediaIt was noted earlier that aortic amyloid deposits were usually restricted to media.21,90,91 In spite of its extreme prevalence, affecting most individuals above a certain age,88,92 this type of amyloid has attracted very little attention. A reason for this little interest is that no functional effects have been attrib-uted to this localized form of amyloidosis. Thus, there are no previous re-ports of an association of medin- amyloid with any clinical disease and aor-tic media amyloid seems not to be associated with atherosclerosis.85,87,90
Aortic media amyloid is found predominantly in the inner part of the me-dia layer.85,88 Battaglia and Trentini noted that media amyloid is more com-monly seen in the thoracic part of the aorta than in the abdominal part and concluded that amyloid starts in the thoracic part and then spreads.93 It has been described as spotted, not fusing and only microscopically visible.93 The amyloid occurs in close association with elastic lamellae in the form of small nodules or thin linear deposits.85,88 Apparent intracellular amyloid in smooth muscle cells may also occur, often in close association with nuclei. 93, (PAPER IV)
Aortic media amyloid is a very prevalent amyloid form in association with aging. It is usually not found before the age of 40, but is demonstrated in almost all individuals over the age of 55.85,88,90,94 The prevalence figuresvary in different studies, however, and Wright and Calkins found aortic amyloid deposits in only 68% of individuals over 60 years of age.95 These variations most likely depend on differences in the sensitivity of the screen-ing methods.
22
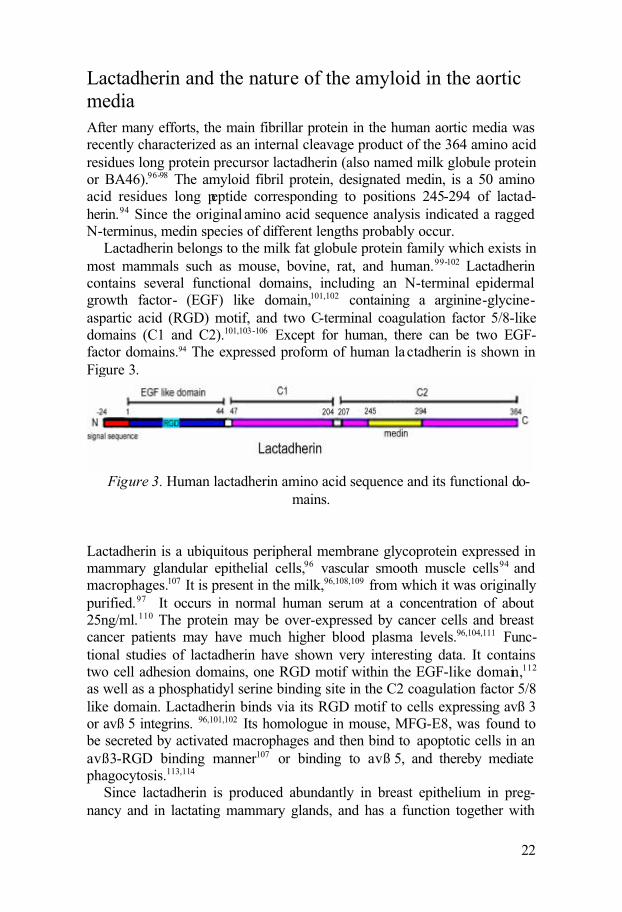
Lactadherin and the nature of the amyloid in the aortic mediaAfter many efforts, the main fibrillar protein in the human aortic media was recently characterized as an internal cleavage product of the 364 amino acid residues long protein precursor lactadherin (also named milk globule protein or BA46).96-98 The amyloid fibril protein, designated medin, is a 50 amino acid residues long peptide corresponding to positions 245-294 of lactad-herin.94 Since the original amino acid sequence analysis indicated a ragged N-terminus, medin species of different lengths probably occur.
Lactadherin belongs to the milk fat globule protein family which exists in most mammals such as mouse, bovine, rat, and human.99-102 Lactadherin contains several functional domains, including an N-terminal epidermal growth factor- (EGF) like domain,101,102 containing a arginine-glycine-aspartic acid (RGD) motif, and two C-terminal coagulation factor 5/8-likedomains (C1 and C2).101,103-106 Except for human, there can be two EGF-factor domains.94 The expressed proform of human lactadherin is shown in Figure 3.
Figure 3. Human lactadherin amino acid sequence and its functional do-mains.
Lactadherin is a ubiquitous peripheral membrane glycoprotein expressed in mammary glandular epithelial cells,96 vascular smooth muscle cells94 and macrophages.107 It is present in the milk,96,108,109 from which it was originally purified.97 It occurs in normal human serum at a concentration of about 25ng/ml.110 The protein may be over-expressed by cancer cells and breast cancer patients may have much higher blood plasma levels.96,104,111 Func-tional studies of lactadherin have shown very interesting data. It contains two cell adhesion domains, one RGD motif within the EGF-like domain,112
as well as a phosphatidyl serine binding site in the C2 coagulation factor 5/8 like domain. Lactadherin binds via its RGD motif to cells expressing avß 3 or avß 5 integrins. 96,101,102 Its homologue in mouse, MFG-E8, was found to be secreted by activated macrophages and then bind to apoptotic cells in an avß3-RGD binding manner107 or binding to avß 5, and thereby mediate phagocytosis.113,114
Since lactadherin is produced abundantly in breast epithelium in preg-nancy and in lactating mammary glands, and has a function together with

23
integrin avß 3 (which is present preferably in new vessels but not mature ones), it has been suggested to be involved in neoangiogenesis.115 Lactad-herin may have an important role as being protective against rota virus in-fections.105,116-118 Furthermore, recent data indicate that it may be active in regulation of coagulation.103
From recent studies in our group, it has been shown that lactadherin is an elastin-binding protein, and we believe that it may be important for the con-nection between smooth muscle cells and the elastic lamina in media layer of artery.119 Lactadherin is produced by smooth muscle cells in the media, and is probably exported and has its biological function extracellularly.119,
(PAPER I)
Formation of medinThe medin sequence is located within the C2 domain of lactadherin.94
Available amino acid sequence data indicate that medin is a somewhat het-erogeneous cleavage product of the precursor protein and has a ragged N-terminus. While the major part of medin starts at position 245 of lactadherin, minor medin species start at positions 241 and 250.94 Whether this heteroge-neity depends on a non-specific cleavage from lactadherin at the formation of medin or a post-cleavage trimming is not known. The enzymes responsi-ble for cleavage are unknown. The anatomical site of the cleavage, i.e. whether medin is generated intracellularly and exported or formed extracel-lularly, is not known. Furthermore, it is not known whether medin is a pathological product or a biologically important polypeptide.
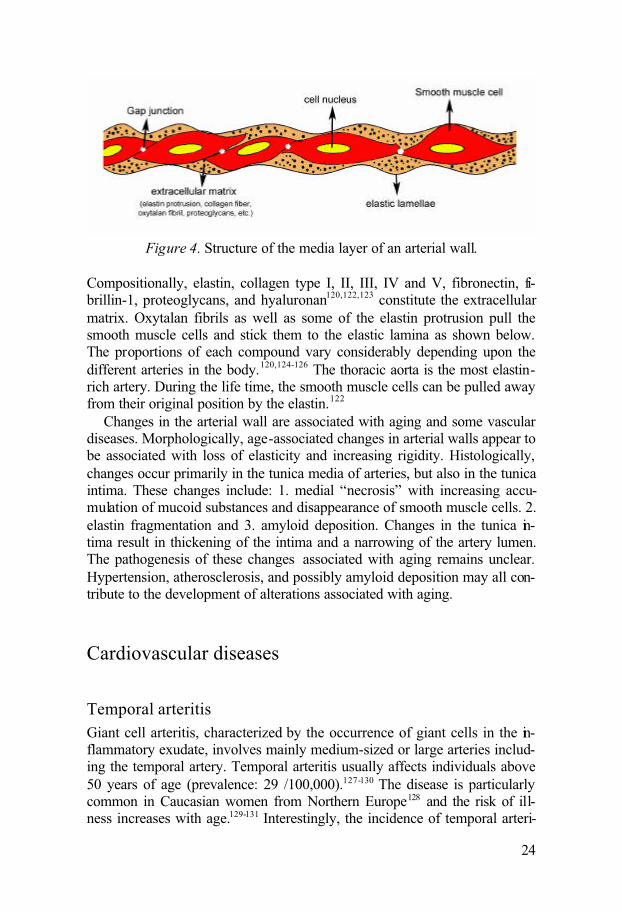
The human arteryArteries have very vital functions to transport oxygen and nutrients to the whole body. In order to do so, arteries must be elastic and able to maintain a suitable blood pressure. Mammalian arteries are composed of three layers: tunica intima, tunica media and tunica adventitia (from internal lumen to the outside). The tunica media is important in giving strength, elasticity and tone to the arterial wall. It is rich in smooth muscle cells as well as extracel-lular matrix. The muscle cells are arranged in a certain way, ensuring the function as well as the structure of the artery. Principally, two layers of the elastic lamellae pinch one layer of smooth muscle cells into a sandwich-likesubunit. Approximately 60 layers of elastic lamellae stretch longitudinally along the aortic wall.120,121 They separate and embed smooth muscle cells oriented in the same direction. Other elastic fibrils and collagen run circum-ferentially around the smooth muscle cells, connecting them to the elastic lamellae (shown below).
24
Figure 4. Structure of the media layer of an arterial wall.
Compositionally, elastin, collagen type I, II, III, IV and V, fibronectin, fi-brillin-1, proteoglycans, and hyaluronan120,122,123 constitute the extracellular matrix. Oxytalan fibrils as well as some of the elastin protrusion pull the smooth muscle cells and stick them to the elastic lamina as shown below. The proportions of each compound vary considerably depending upon the different arteries in the body.120,124-126 The thoracic aorta is the most elastin-rich artery. During the life time, the smooth muscle cells can be pulled away from their original position by the elastin.122
Changes in the arterial wall are associated with aging and some vascular diseases. Morphologically, age-associated changes in arterial walls appear to be associated with loss of elasticity and increasing rigidity. Histologically, changes occur primarily in the tunica media of arteries, but also in the tunica intima. These changes include: 1. medial “necrosis” with increasing accu-mulation of mucoid substances and disappearance of smooth muscle cells. 2. elastin fragmentation and 3. amyloid deposition. Changes in the tunica in-tima result in thickening of the intima and a narrowing of the artery lumen. The pathogenesis of these changes associated with aging remains unclear. Hypertension, atherosclerosis, and possibly amyloid deposition may all con-tribute to the development of alterations associated with aging.
Cardiovascular diseases
Temporal arteritisGiant cell arteritis, characterized by the occurrence of giant cells in the in-flammatory exudate, involves mainly medium-sized or large arteries includ-ing the temporal artery. Temporal arteritis usually affects individuals above 50 years of age (prevalence: 29 /100,000).127-130 The disease is particularly common in Caucasian women from Northern Europe128 and the risk of ill-ness increases with age.129-131 Interestingly, the incidence of temporal arteri-

25
tis follows a regular cyclic pattern which suggests involvement of an envi-ronment factor.128 A patient with temporal arteritis usually suffers fromheadache, accompanied by fever, anorexia and stiffness of the neck. A defi-nite diagnosis is obtained by an arterial biopsy showing characteristic histo-pathologic alterations. Corticosteroids are used as treatment of the vasculitis and this helps to suppress the inflammation of the arteries. Involvement of ocular arteries is not rare and delayed treatment can lead to loss of vision. Consequently, treatment is usually implemented even before the histological diagnosis and is based on clinical symptoms.
The pathogenesis of giant cell arteritis is not well delineated but the dis-ease is regarded as an autoimmune disorder with involvement of cellular immunity. Following the triggering of unknown antigen(s), arteries show a typical inflammatory cell infiltration where macrophages and CD4 T cells penetrate both the intimal and medial layers of affected arteries.132,133 Thepathological changes are also characterized by a fragmented internal elastic lamina and an inflammatory exudate with the presence of giant cells derived from monocytes, thickening of the intima and sometimes thrombosis.
There are two main puzzles in the pathogenesis of temporal arteritis: 1. There is a possible genetic factor. As discussed earlier, Scandinavianwomen are particularly affected by this vasculitis. The incidence does not change with the movement of a population. 2. The antigen(s) which trigger the inflammation remain(s) unknown.
This antigen(s) can lead to activation of the monocytes of the inflamma-tory exudate and enable them to release cytokines which may induce the intimal proliferation and thrombosis.134,135 Antigen(s) may also induce dif-ferentiation of some macrophages into metalloproteinase secretory cells136,137
which, in turn, may lead to more macrophage production. MMPs released from macrophages may be important in the digestion of the arterial wall which leads to fragmentation of the elastic lamina.
Resolution of these questions and relationships will not only help to un-derstand the pathogenesis of giant cell arteritis but can also lead to methods to prevent the development of disease.
Thoracic aorta aneurysm and aorta dissectionAortic aneurysm and dissection are types of arterial diseases associated with weakened arterial walls. Different regions of the aorta may be involved, and also some major vessels such as the renal and cerebral arteries may also be affected. The pathogenesis can differ between regions. Generally, thoracic aortic aneurysm and dissection are amongst the most life threatening aortadiseases and their pathogenesis is unclear. A characteristic pathologic change is cystic medial degeneration of the aortic wall. This was first de-scribed by Erdheim as ‘Medionecrosis aortae idiopathica cystica’ ,138,139
where patchy distribution of mucoid substances replace the normal structure.

26
Fragmented elastic laminas, instead of normal continuous elastic lamina, as well as loss of smooth muscle cells are also seen. The pathogenesis of the cystic degeneration is far from clear and it is not even known whether the degeneration itself is a cause or a consequence of disease. Members the matrix metalloprotease (MMP) family, especially MMP2 and MMP9 are claimed to cause fragmentation of the elastic lamina.140,141
Thoracic aortic aneurysm can occur in the ascending aorta, the aortic arch or the descending aorta. Rupture can occur once the aortic wall dilatation reaches a certain size, which is a catastrophe to the patient. Some factors that are suggested to be associated with thoracic aorta aneurysms are:
1. Genetic disorders, such as Marfan syndrome and Ehlers-Danlos syn-drome.
2. Atherosclerosis may be the main cause of abdominal aortic aneurysm, however atherosclerosis is not the leading cause for thoracic aortic an-eurysm.
3. Infection. Syphilis used to be the dominate cause to thoracic aorta aneu-rysm decades ago but is now much more rare.
4. Giant cell arteritis is proposed to be another potential cause. Patients who have suffered from temporal arteritis have a higher risk to develop thoracic aortic aneurysm. 142
5. Trauma.
Thoracic aortic dissection is also a form of aortic wall weakening disease, where the inner layer tears into the media layer and a false lumen is formed for passing blood flow. It is also associated with cystic media necrosis. The pathogenesis of thoracic aortic dissection is also unclear. In addition to the causes mentioned for aneurysm, hypertension is also known to be one major factor involved.143-145
27
Aims of present investigation
1. To study the distribution of medin amyloid in human arteries in the body
2. To investigate the possible pathogenetic importance of medin amyloid and related peptides in several human vascular diseases
3. To define the location of medin peptide pre-aggregation and aggregation

28
Materials
Tissues
Medin amyloid in the temporal artery (paper I)Temporal artery biopsies from 47 patients (35 females and 12 males) were available in our laboratory archives. Signs of giant cell arteritis were present in 22 of these patients. The biopsies had been fixed in buffered neutral 4 % formaldehyde solution (BNF) and were embedded in paraffin.
Medin amyloid deposition in different arteries in the human body (paper II)At routine clinical autopsies, pieces of arteries from the following locations were fixed in BNF and then embedded in paraffin: A. ascending thoracic aorta (3-5cm above the valves); B. lower thoracic aorta (about 3cm above the renal artery); C. abdominal aorta (about 3 cm above the bifurcation); D. basilar artery; E. left coronary artery; F. superior mesenteric artery; G. pul-monary artery; H. inferior vena cava. Materials from 18 individuals (6 fe-males and 12 males) were studied.
Medin amyloid in human thoracic aorta aneurysms and dissections (paper III + paper IV)A total of 27 (age range: 49-81) thoracic aortic aneurysms and 11 (age range: 33-74) thoracic aortic dissections were studied. All of the aortic specimens were obtained at thoracic aortic surgery. All tissue specimens were from the thoracic ascending aorta. For comparison, 29 (age range: 33-81) thoracic aortic biopsies from the same region of the aorta were taken from patients undergoing coronary artery bypass surgery (punch biopsies) or aortic valve replacement surgery. As soon as the tissue material was taken from the body, the specimens were kept on ice until further treatment. Biopsy material used for light microscopy was fixed in BNF and embedded in paraffin. For elec-tron microscopy, small aortic samples were fixed in 2% paraformalde-

29
hyde/0.25% glutaraldehyde in 0.05 M sodium phosphate buffer, pH 7.4, containing 0.15 M NaCl and embedded in epon. The remainder of the mate-rial was stored at -20°C for later protein extraction.
Antibodies against lactadherinRabbit antisera A-177 and A-172 were raised against synthetic peptides corresponding to positions 245-256 and positions 286-293 of lactadherin both of which are within the medin domain. Since our supply of antiserum A-177 was relatively low, we had a new one (antibody A-179) produced against same peptide as A-177. Rabbit antiserum A-180 was raised against asynthetic peptide C-terminal of medin at positions 310-322 of lactadherin.
30
Methods
Demonstration of amyloidTissues were stained with alkaline Congo red solution after deparaffiniza-tion, and were then analyzed with a polarization microscope. Medin- amy-loid normally shows comparably weak red staining with this method and green birefringence is also sometimes difficult to detect.88,91,146 These facts make an exact measurement of the amount of amyloid difficult. In addition, one has to be aware of the risk of nonspecific staining of non-amyloid struc-tures with Congo red. Particularly elastin can easily take the stain. Congo red is also a fluorescent dye and therefore useful in fluorescence microscopy (see below).
Immunological methodsAntibody A-177 or A-179, used for immunohistochemistry was diluted 1:4000 while the dilution of A-172 was 1:2000. For antigenic retrieval, sev-eral methods were tried. The method of pouring boiling 0.02 M sodium citrate buffer, pH 9.6 was found to give the best and most reproducible re-sults. For light microscopy, immunohistochemistry was performed using the biotin-streptavidine method with diaminobenzidine as chromogen. Some sections were stained with Congo red B solution after the immunohisto-chemical procedure for simultaneous demonstration of Congophilicity and immunoreactivity.
For detail histological study, immunofluorescent methods were per-formed. After the first antibody incubation (the same as for normal immu-nostaining), Alexa fluor 633 anti rabbit IgG secondary antibody was ap-plied followed by Hoechst nuclear staining. The sections were studied in a confocal microscope.

31
Electron microscopySmall pieces of temporal arteries or thoracic aorta containing amyloid de-posits (which were originally fixed in BNF) were embedded in the hydro-philic resin Unicryl which allows better immune electron microscopical results. Ultrathin sections were put on formvar-coated nickel grids and were labeled with antiserum A-179. Binding was visualized with 10 nm gold particles, labeled with protein A.
Protein purificationHuman aortic tissue contains various proteins. Our aim was to extract pro-teins from the media layer to examine medin and its precursor protein lac-tadherin. After removal of intimal and adventitial layers, medial samples (about 200 mg) were cut into small pieces and homogenized on ice in 0.15M NaCl containing 0.05 M dithiothreitol (DTT) and protease inhibitors.Specimens were centrifuged at 15,000 rpm (Beckman centrifuge equipped with a JA-20 rotor) at +4°C for 30 minutes. This procedure was repeated 4 times. The supernatants were combined, dialyzed against distilled water to remove salt and then lyophilized. In order to dissolve more proteins, includ-ing amyloid, the pellet material was treated with 6 M guanidine-HCl in 0.1 M Tris HCl, pH 8.0, containing 0.1 M DTT and 0.2 M EDTA over night at room temperature. After centrifugation, the solution was dialyzed against distilled water and lyophilized. All the harvested materials were kept in room temperature until further investigation. Adventitial, medial and intimal layers from some specimens were homogenized separately and both super-natant and pellet materials were saved as above.
Electrophoresis and western blottingWater soluble and non-soluble proteins from the tissue extractions were re-dissolved in sample buffer containing 4% sodium dodecylsulfate (SDS). The proteins were reduced with DTT and aklkylated by the addition of io-doacetamide in order to block the cysteine recombination. SDS polyacryla-mide gel electrophoresis (PAGE) was performed using a Tris tricine sys-tem147 which is suitable for small protein molecules. Antiserum A-177 or A-179 was used as the primary antibodies in the western blotting step.

32
In situ hybridizationIn situ hybridization was performed to detect lactadherin mRNA expression in the cells of the arterial wall. Paraffin embedded specimens from both temporal arteritis arteries and non- arteritis arteries were studied, and a di-goxygenin labeled RNA probe was used in the in situ hybridization. Tissue sections were hybridized with the antisense-RNA probe and a sense-RNAprobe was used as negative control.

33
Results and Discussion
Medin amyloid in temporal artery and its association with giant cell arteritis (paper I)Temporal artery biopsies from 47 patients were studied and 22 of these showed histological signs of giant cell arteritis. In 14 of these (63%), amy-loid deposits were found (which is similar to the finding in non-inflamedarteries (25 cases; 84%)). The amyloid always reacted with the antibody A-177. The amyloid nearly always was found in close contact with the internal elastic lamina.
In inflamed arteries, the internal elastic lamina was fragmented andfragments were often found engulfed by multinuclear giant cells. Material strongly immunolabelled by A-177 was also seen in these giant cells but Congo-red pos itive material was rarely seen.
Electron microscopically, positive gold labeling along the internal elastic lamina was evident which was identical with the observation of Congo red staining on the same material. It was also clear that small amyloid accumu-lations were intermingled with elastic material. The elastic material itself was not labeled. No immunolabelled material was found within smooth muscle cells.
In situ hybridization studies using both giant cell arteritis and non-inflamed arteries showed that smooth muscle cells express lactadherinmRNA evenly and abundantly. However, inflamed arteries often showed a more uneven labeling. These findings strongly indicate that medin in the amyloid originates from production close to the inflammation.
Giant cell arteritis is recognized to be a T- cell dependent inflammatory disease in arteries that may affect temporal arteries as well as other bigger arteries.132,148-150 Most giant cell arteritis patients are above 50 years old 151
and the causes remain unknown. The antigen that triggers the immune- reac-tion is far from clear. With giant cell arteritis, the typical pathologic changes are associated with the triggering of T cells, the formation of giant cells along the internal elastic lamina, and the fragmentation of elastic lamina.152
From the findings above we suggest that medin may be an important antigen in the pathogenesis of temporal arteritis. The possibility that medin and me-

34
din-amyloid is involved in the pathogenesis of giant cell arteritis may seem provocative. Although we so far have only the spatial relationship betweenthe amyloid and the inflammation as evidence, this relationship may indi-cate that the amyloid is involved in the pathogenesis. It is interesting to notethat vascular inflammation with giant cells occurred in a transgenic mouse model of Aß-amyloid angiopathy.153 Further studies on the possible impor-tance of medin for giant cell arteritis are important.
Medin amyloid distribution (paper II)Given the high frequency of medin-amyloid in biopsies from the temporal artery in an elderly population, we studied the distribution of this form of amyloid in vessels in other parts of the body. Medin-amyloid is probably the most common form of human amyloidosis but, paradoxically, one of the least studied amyloid types. It was previously known as a localized amyloid of the aortic media,85,90,91,95,145 although in those studies the biochemical na-ture was not known and the characterization only performed with Congo red or Thioflavine-S. In this medin-amyloid distribution study, we collected 7 different vessels from 18 autopsy cases age 57-88 (6 females, 12 males). In addition to these 18 individuals, we studied material from a 33-year-oldindividual in whom no amyloid at all was detected (unpublished result). Immunohistochemistry results with antiserum against medin were compared with Congo-red amyloid staining result. Both methods gave identical infor-mation and showed that antibody A-177 labeled nothing but medin-amyloid.Failure to label elastic lamina indicates that the antiserum does not reactwith the precursor protein lactadherin. The most affected artery was theaorta, since 100% of the biopsies from both ascending and descending tho-racic aorta and nearly 72% of the biopsies of the abdominal aorta contained medin-amyloid. A semiquantitative estimation of the amount of amyloid showed that the abdominal aorta contained significantly less amyloid com-pared with the two upper parts. This is in agreement with earlier studies, only based on Congo red.93 In this latter paper, it was suggested that the amyloid starts in the thoracic part and then spreads to the abdominal part. However, our recent demonstration of the interaction between lactadherin (and medin) and elastin (Persson et al. in press) rather points to the impor-tance of elastin for the formation of medin-amyloid. Therefore, the elastin-rich thoracic aorta may be more prone to form medin-amyloid. This is also a part of the body with the highest blood pressure.
In the addition to the aorta, small medin-amyloid deposits were alsofound in other arteries in 12 of the patients. The second most affected artery was the basilar artery was deposits were seen in 8 out of 17 studied cases. The only vein that we studied (inferior vena cava) was not involved in any of the cases. Taken together with earlier results, including those with the

35
temporal artery, we concluded that medin-amyloid is a previously unrecog-nized arterial amyloidosis particularly affecting the upper part of the body. Although medin-amyloid deposits may be found in arteries in different parts of the body, this amyloid is probably best regarded as a localized form of amyloidosis rather than systemic. This is, however, a matter of definition.
Western blot results indicated that the medin precursor protein, lactad-herin, was also present in both soluble and non-soluble materials extracted from amyloid-rich aortic material. However, medin was present only in the non-soluble amyloid pellet material. Although not proven, this finding may indicate that medin is not a normally occurring fragment of lactadherin. However, it is also possible that non-aggregated medin appears at a concen-tration below our detection limits.
Importance of medin in the pathogenesis of thoracic aortic aneurysm and dissection (paper III)The pathogenesis of thoracic aortic aneurysm and dissection remains un-known. Both diseases involve degeneration of the medial layer and deposi-tion of a glycosaminoglycan-rich material, characteristic of the ‘cystic me-dial necrosis’. In this investigation, where we studied aortic material from 27 patients with thoracic aortic aneurysm, 11 with thoracic aortic dissection and 29 control patients, a method was developed to study cystic degenera-tion and depos ition of amyloid simultaneously. A routine staining profile for the aortic wall, which included Alcian blue, aldehyde fuchsine and picric acid, was combined with Congo red. This allowed us to study the relation-ship between amyloid deposition and other structures of the aorta. There was no spatial relationship between cystic degeneration and amyloid depos-its observed in this study.
As expected from previous studies, medin-amyloid deposits were very prevalent and the degree of amyloid infiltration showed a significant corre-lation with age (r=0.34 for the combined three materials). Interestingly, the correlation was particularly strong for the control material (r=0.66) but was weaker for the aneurysm and dissection materials (r=39 and 0.37, respec-tively). Unexpectedly, the amount of medial amyloid (measured as number of amyloid particles) was significantly higher in the control material as compared to the aneurysm group (p=0.03) and the dissection group (p=0.02). Therefore, it seems unlikely that the amyloid by itself is a cause of thoracic aortic aneurysm and dissection. This situation may be similar to that in Alz-heimer’s disease and type 2 diabetes where it is believed that it is not the mature amyloid that is a cause of loss of neurons and ß-cells, respec-tively.154-156 Instead, it has become increasingly clear that small protein ag-gregates, with a high degree of ß -sheet structure can exert toxic effects by

36
direct contact with cells.157 This mechanism could possibly be more impor-tant than a direct mass-effect of amyloid, particularly in disorders with mul-tiple small amyloid deposits.
Amyloid deposits were evenly labeled with antiserum raised against me-din but, as expected, they failed to stain with an antiserum raised against a peptide located within the C-terminus of lactadherin but outside medin. In controls, there was a strong correlation between the amount of amyloid (measured as number of amyloid particles) and the immunoreactive area (r=0.91). This finding serves as an indication that the two methods to meas-ure the amount of amyloid are relevant and reliable in this type of material. The medin-antiserum (A179) does not label normal, full-length lactadherin in tissues although it labels this protein in Western blots. The reason for this behavior is not fully understood but it is probable that the medin-domain is not exposed in the normally folded lactadherin. It is interesting to note that in most of the materials from individuals with aortic aneurysm and dissec-tion, medin-immunoreactive areas (without presence of amyloid) werewidely spread. This was rarely seen in the aortic tissue of the control group and is different from the findings in paper II. For this reason there was no significant correlation between number of amyloid particles and immu-nolabeled area in the aneurysm material (r=0.08) or the dissection material (r=0.33). One important possible explanation is that the non-amyloid medin immunolabeling depends on occurrence of small pre-amyloid, oligomeric protein aggregates. Such types of aggregates are known to be formed with other types of amyloid and are described as ‘soluble’.158 In Western blot analysis of water-soluble extracts of aneurysmatic tissue not containing any amyloid, an immunoreactive band of medin size was demonstrated, as well as bands of higher molecular masses. Although more studies are necessary, this finding may indicate presence of oligomeric medin in these tissues. For this reason, we propose that medin-aggregates in a prefibrillar state are toxic to smooth muscle cells and important in the pathogenesis of thoracic aortic aneurysm and dissection.
In two of the thoracic aortic aneurysm cases, typical epitheloid granulo-mas were found in the aorta. In one of these cases, the extent of granuloma formation was conspicuous. There was no evidence of granulomatous dis-ease such as tuberculosis or sarcoidosis in either of the two individuals. Interestingly, there is an increased risk for individuals with temporal arteritis to develop thoracic aortic aneurysm.159 However, as far as known, none of the patients had suffered from peripheral arteritis.
Intracellular amyloid (papers II-IV)Intracellular amyloid may seem a contradictory designation since, by his-torical definition, amyloid represents an extracellular deposition.13 However,

37
protein aggregates consistent with amyloid may occur intracellularly160 andin addition, intracellular deposits are sometimes found in association with large amyloid deposits.161 In the present studies we often observed (by con-ventional light microscopy) medin-amyloid deposits which seemed to be located within myocytes. Similar findings have been noted by others.93 A notable amount of amyloid deposits were found intracellularly and these often encircled nuclei in a ring-like fashion. We therefore wished to deter-mine the apparent intracellular location by techniques other than conven-tional microscopy. Confocal microscopy confirmed the intracellular occur-rence of medin amyloid. Also, studies in which we used wheat germ agglu-tinin for demonstration of membranes, intracellular amyloid (sometimes in close contact with Golgi) was evident. It was not possible to determine with certainty which cellular compartment contained the amyloid deposits.
The importance of these small intracellular deposits is unknown. It is possible that they may lead to death of the affected cells. Since amyloid fibrils are comparatively stable and difficult to dissolve using normal degra-dation mechanisms, fibrils may reside extracellularly after that the remain-der of the cell has been degraded.162 In this way an originally intracellular deposit may act as a seed for further extracellular amyloid formation.

38
General discussion and future perspectives
This thesis describes a form of arterial amyloidosis which previously was regarded to be restricted to the aorta. However, as shown here, deposits can also be found in the walls of many other arteries. It is a matter of definition as to whether medin-amyloid should be classified as being systemic or lo-calized. On one hand, it occurs in many different organs including the brain but on the other hand it is always restricted to arterial walls. For this latter reason, it is perhaps better to include medin-amyloid in the group of local-ized amyloidosis.
Medin is a polypeptide cleaved from the internal region of a much larger protein precursor. Whether medin is a normal or an abnormal product is not known. If it is a normal product the function of this polypeptide is unknown. We have not found medin in Western blot studies of extracts of normal ves-sels, but this does not exclude the possibility that medin is present inamounts below the limits of detection. Also, enzymes responsible for the generation of medin are unknown and need to be identified.
During the last several years it has become increasingly evident that pro-tein misfolding and aggregation is involved as a disease mechanism in many neurodegenerative disorders. These include Alzheimer’s disease, transmis-sible spongioform encephalopathies, Parkinson’s disease, amyotrophic la t-eral sclerosis and many others. Not all of these diseases are characterized by deposition of typical amyloid fibrils, but small aggregates of misfolded pro-teins (believed to be toxic to cells) are considered to be important in the pathogenesis of all of these diseases. Such toxicity appears to be a generic type of effect, i.e. resulting more or less irrespective of the biochemical composition of the aggregated protein. It is therefore our hypothesis that aggregated medin also has toxic effects on cells, especially medial smooth muscle cells. These studies of medin aggregates in thoracic aortic aneurysm and dissection support this hypothesis, although no full proof could be ob-tained. One big obstacle was that the tissues available to us for study repre-sent end-points of the disease processes, i.e. aneurysms or dissections that have required surgery based on the clinical severity of the disease condition. Ideally, tissue samples taken early in the disease process should be studied. However, this was not possible in this study. An animal model would obvi-ously be of great value. Since a spontaneously occurring animal model is not known, the creation of a transgenic mouse strain overexpressing human lactadherin or medin may be useful for further studies.

39
Medin-amyloid was often found in an intracellular location in our studies, although the cellular compartment was not elucidated. It is possible that aggregated intracellular medin is also deleterious to cells. Experiments with transfection of medin or lactadherin to smooth muscle cells may thus also be of interest.
Lactadherin is obviously normally expressed in medial smooth muscle cells but its vascular function is still unknown. This protein has an integrin-binding motif in its N-terminal region. We have recently shown that both lactadherin and medin bind to elastin.119 Therefore, it seems very feasible that one normal function of lactadherin is to anchor medial smooth muscle cells to the elastic laminae. Theoretically, medin may compete with lactad-herin at the binding sites on the elastic laminae. If this is true, binding of medin to elastic laminae could feasibly disturb the integrity of the vascular structures and the vessel wall per se weakened. Studies of the importance of lactadherin as an anchor between elastin and smooth muscles cells are yet to be performed.
The other disease which was studied in this thesis is temporal arteritis.We have hypothesized in this study that medin or its precursor may be in-volved in autoimmune mechanisms associated with this disease. Studies of plasma and of immune cells from patients with temporal arteritis wereplanned (in order to find antibodies or immune cells reacting with lactad-herin and medin). However, for reasons out of our control, these studies were never possible to accomplish. Such studies should, however, be per-formed in the future.

40
Acknowledgements
This work was carried out in the most successful scientific laboratory, Insti-tute of Genetic and Pathology, Uppsala University. Financial support was kindly provided by the Swedish Research Council, the Swedish Heart Lung Foundation, the Swedish Society of Medical Research, the Medical Faculty of Uppsala University and Stiftelsen för Gamla Tjänarinnor.
Here, I wish to thank peoples who have companied me through this happy, frustrating, and successful period.
Per Westermark, my supervisor, the first person led me into this interestingfield. Thank you for the guidance and your insight throughout the research. No words can express my great thanks from my deep heart.
Gunilla T. Westermark, thank you for the great and kindly help with my experiments, especially at the beginning when I started here.
To Anders Rane, my pre-supervisor, you accepted me into your group,taught me various advanced techniques, I can not get this degree without your education.
To Folk sjökvist, the first Swedish scientist I met in China. Your kindness and erudition impressed me very much and made me never regret of study-ing in Sweden.
Joakim, we have companied each other almost whole our Ph.D studies, Lots of memorable things. It is nice to have you as a friend and colleague.
Annika, Stina and Eva. Your coming to the group brought the real Swedishroutine laboratory life, strict and relaxing, it is very nice to work with you and be friends with you.
To Jan Gravé , thank you for your great help with confocal microscope and all the other help with fluorescent techniques.
Erik Wassberg and Stefan Thelin, collected materials for the study for 3 years.

41
Thank Ken Johnson, for his quick linguistic check of my thesis within so short time.
To Pä r Garvins, Jan Näslund, Bo Häggqvist, Erik Wassberg, Stefan Thelin, and Johanna Glennert the co-authors of thesis work. Thank for your kindlyhelp and support.
To my family, my daddy, mama, my sister, thank you for your motivationand patience.
To Xiaoqun, my best friend, who supported me when I fell and cheered for me when I succeed
The last but not the least, to my husband, Yanwu, for your company, your support and your love, here, I just wish you the same good luck as me.
To all my friends in Sweden, especially, Mi jia,Cheng shi,Shixiaochun,友情客串试验助手。thank you for your great friendship. And wish you all good luck!

42
References
1. Cohen AS, Connors LH: The pathogenesis and biochemistry of amyloidosis. J Pathol 1987, 151:1-10
2. Glenner GG: Amyloid deposits and amyloidosis. The beta-fibrilloses. N Engl J Med 1980, 302:1333-1343
3. Virchow R: Zur cellulosefrage. Virchows Arch. Pathol Anat Physiol 1854:416-426.
4. Cohen AS, Calkins E: Electron microscopic observations on a fibrous component in amyloid of diverse origins. Nature 1959, 183:1202-1203
5. Benditt EP, Eriksen N, Hermodson MA, Ericsson LH: The major proteins of human and monkey amyloid substance: Common properties including unusual N-terminal amino acid sequences. FEBS Lett 1971, 19:169-173
6. Husby G, Sletten K, Michaelsen TE, Natvig JB: Alternative, non- immunoglobulin origin of amyloid fibrils. Nat New Biol 1972, 238:187
7. Glenner GG, Terry W, Harada M, Isersky C, Page D: Amyloid fibril proteins: proof of homology with immunoglobulin light chains by sequence analyses. Science 1971, 172:1150-1151
8. Glenner GG, Wong CW: Alzheimer's disease and Down's syndrome: sharing of a unique cerebrovascular amyloid fibril protein. Biochem Biophys Res Commun 1984, 122:1131-1135
9. Glenner GG, Wong CW: Alzheimer's disease: initial report of the purification and characterization of a novel cerebrovascu-lar amyloid protein. Biochem Biophys Res Commun 1984, 120:885-890
10. Westermark P, Wernstedt C, Wilander E, Sletten K: A novel peptide in the calcitonin gene related peptide family as an amyloid fibril protein in the endocrine pancreas. Biochem Biophys Res Commun 1986, 140:827-831
11. Hull RL, Westermark GT, Westermark P, Kahn SE: Islet amy-loid: a critical entity in the pathogenesis of type 2 diabetes. J Clin Endocrinol Metab 2004, 89:3629-3643

43
12. Hoppener JW, Nieuwenhuis MG, Vroom TM, Ahren B, Lips CJ: Role of islet amyloid in type 2 diabetes mellitus: conse-quence or cause? Mol Cell Endocrinol 2002, 197:205-212
13. Westermark P, Benson MD, Buxbaum JN, Cohen AS, Fran-gione B, Ikeda S, Masters CL, Merlini G, Saraiva MJ, Sipe JD: Amyloid: toward terminology clarification. Report from the Nomenclature Committee of the International Society of Amyloidosis. Amyloid 2005, 12:1-4
14. Venter JC AM, Zhu X, et al: The sequence of the human ge-nome. Science 2001, 291:1304-1351
15. Lander ES, Linton LM, Birren B, Nusbaum C, Zody MC, al e:Initial sequencing and analysis of the human genome. Nature 2001, 409:860-921
16. Anfinsen CB: Principles that govern the folding of protein chains. Science 1973, 181:223-230
17. Szyperski T, Vandenbussche G, Curstedt T, Ruysschaert JM, Wuthrich K, Johansson J: Pulmonary surfactant-associatedpolypeptide C in a mixed organic solvent transforms from a monomeric alpha-helical state into insoluble beta-sheet aggre-gates. Protein Sci 1998, 7:2533-2540
18. Dobson CM: Principles of protein folding, misfolding and aggregation. Semin Cell Dev Biol 2004, 15:3-16
19. Vendruscolo M, Paci E, Karplus M, Dobson CM: Structures and relative free energies of partially folded states of proteins. Proc Natl Acad Sci U S A 2003, 100:14817-14821
20. Westermark GT, Johnson KH, Westermark P: Staining meth-ods for identification of amyloid in tissue. Meth Enzymol 1999, 309:3-25
21. Storkel S, Bohl J, Schneider HM: Senile amyloidosis: princi-ples of localization in a heterogeneous form of amyloidosis. Virchows Arch B Cell Pathol Incl Mol Pathol 1983, 44:145-161
22. Zerovnik E: Amyloid-fibril formation. Proposed mechanisms and relevance to conformational disease. Eur J Biochem 2002,269:3362-3371
23. Serpell LC, Sunde M, Benson MD, Tennent GA, Pepys MB, Fraser PE: The protofilament substructure of amyloid fibrils. J Mol Biol 2000, 300:1033-1039
24. Sunde M, Serpell LC, Bartlam M, Fraser PE, Pepys MB, Blake CC: Common core structure of amyloid fibrils by syn-chrotron X-ray diffraction. J Mol Biol 1997, 273:729-739

44
25. Eanes ED, Glenner GG: X-ray diffraction studies on amyloid filaments. J Histochem Cytochem 1968, 16:673-677
26. Rochet JC, Lansbury PT, Jr.: Amyloid fibrillogenesis: themesand variations. Curr Opin Struct Biol 2000, 10:60-68
27. Blake CC, Serpell LC, Sunde M, Sandgren O, Lundgren E: A molecular model of the amyloid fibril. Ciba Found Symp 1996, 199:6-15; discussion 15-21, 40-16
28. Tomiyama T, Corder EH, Mori H: Molecula r pathogenesis of apolipoprotein E-mediated amyloidosis in late-onset Alz-heimer's disease. Cell Mol Life Sci 1999, 56:268-279
29. Fukuchi K, Hart M, Li L: Alzheimer's disease and heparan sulfate proteoglycan. Front Biosci 1998, 3:d327-337
30. Pepys MB: Pathogenesis, diagnosis and treatment of systemic amyloidosis. Philos Trans R Soc Lond B Biol Sci 2001, 356:203-210; discussion 210-201
31. Hoshii Y, Kawano H, Cui D, Takeda T, Gondo T, Takahashi M, Kogishi K, Higuchi K, Ishihara T: Amyloid A protein amyloidosis induced in apolipoprotein-E-deficient mice. Am J Pathol 1997, 151:911-917
32. Li JP, Galvis ML, Gong F, Zhang X, Zcharia E, Metzger S, Vlodavsky I, Kisilevsky R, Lindahl U: In vivo fragmentation of heparan sulfate by heparanase overexpression renders miceresistant to amyloid protein A amyloidosis. Proc Natl Acad Sci U S A 2005, 102:6473-6477
33. Snow AD, Bramson R, Mar H, Wight TN, Kisilevsky R: A temporal and ultrastructural relationship between heparan sul-fate proteoglycans and AA amyloid in experimental amyloi-dosis. J Histochem Cytochem 1991, 39:1321-1330
34. Serag AA, Altenbach C, Gingery M, Hubbell WL, Yeates TO: Arrangement of subunits and ordering of beta-strands in an amyloid sheet. Nat Struct Biol 2002, 9:734-739
35. Horwich A: Protein aggregation in disease: a role for folding intermediates forming specific multimeric interactions. J Clin Invest 2002, 110:1221-1232
36. Modler AJ, Gast K, Lutsch G, Damaschun G: Assembly of amyloid protofibrils via critical oligomers--a novel pathway of amyloid formation. J Mol Biol 2003, 325:135-148
37. Harper JD, Wong SS, Lieber CM, Lansbury PT: Observation of metastable Abeta amyloid protofibrils by atomic force mi-croscopy. Chem Biol 1997, 4:119-125

45
38. Lashuel HA, Lai Z, Kelly JW: Characterization of the transthyretin acid denaturation pathways by analytical ultra-centrifugation: implications for wild-type, V30M, and L55P amyloid fibril formation. Biochemistry 1998, 37:17851-17864
39. Lashuel HA, Wurth C, Woo L, Kelly JW: The most patho-genic transthyretin variant, L55P, forms amyloid fibrils under acidic conditions and protofilaments under physiological con-ditions. Biochemistry 1999, 38:13560-13573
40. Buxbaum JN: The systemic amyloidoses. Curr Opin Rheuma-tol 2004, 16:67-75
41. Jolly-Tornetta C, Wolf BA: Regulation of amyloid precursor protein (APP) secretion by protein kinase calpha in human ntera 2 neurons (NT2N). Biochemistry 2000, 39:7428-7435
42. Passer B, Pellegrini L, Russo C, Siegel RM, Lenardo MJ, Schettini G, Bachmann M, Tabaton M, D'Adamio L: Genera-tion of an Apoptotic Intracellular Peptide by gamma-SecretaseCleavage of Alzheimer's Amyloid beta Protein Precursor. J Alzheimers Dis 2000, 2:289-301
43. Saftig P, Hartmann D, De Strooper B: The function of prese-nilin-1 in amyloid beta-peptide generation and brain develop-ment. Eur Arch Psychiatry Clin Neurosci 1999, 249:271-279
44. Bellotti V, Mangione P, Merlini G: Review: immunoglobulin light chain amyloidosis--the archetype of structural and patho-genic variability. J Struct Biol 2000, 130:280-289
45. Bell AW, Chan SL, Ali-Khan Z: N-terminal sequence analysis of SAA-derivatives purified from murine inflammatory macrophages. Amyloid 1999, 6:31-36
46. Kisilevsky R: Review: amyloidogenesis-unquestioned an-swers and unanswered questions. J Struct Biol 2000, 130:99-108
47. Westermark P: Aspects on human amyloid forms and their fibril polypeptides. FEBS J 2005, 272:5942-5949
48. Pepys MB, Herbert J, Hutchinson WL, Tennent GA, Lachmann HJ, Gallimore JR, Lovat LB, Bartfai T, Alanine A, Hertel C, Hoffmann T, Jakob-Roetne R, Norcross RD, Kemp JA, Yamamura K, Suzuki M, Taylor GW, Murray S, Thomp-son D, Purvis A, Kolstoe S, Wood SP, Hawkins PN: Targeted pharmacological depletion of serum amyloid P component for treatment of human amyloidosis. Nature 2002, 417:254-259
49. Miklossy J, Taddei K, Martins R, Escher G, Kraftsik R, Pille-vuit O, Lepori D, Campiche M: Alzheimer disease: curly fi-

46
bers and tangles in organs other than brain. J Neuropathol Exp Neurol 1999, 58:803-814
50. Botto M, Hawkins PN, Bickerstaff MC, Herbert J, BygraveAE, McBride A, Hutchinson WL, Tennent GA, Walport MJ, Pepys MB: Amyloid deposition is delayed in mice with tar-geted deletion of the serum amyloid P component gene. Nat Med 1997, 3:855-859
51. Westermark P, Eizirik DL, Pipeleers DG, Hellerstrom C, Andersson A: Rapid deposition of amyloid in human islets transplanted into nude mice. Diabetologia 1995, 38:543-549
52. Yagui K, Yamaguchi T, Kanatsuka A, Shimada F, Huang CI, Tokuyama Y, Ohsawa H, Yamamura K, Miyazaki J, Mikata A, et al.: Formation of islet amyloid fibrils in beta-secretorygranules of transgenic mice expressing human islet amyloid polypeptide/amylin. Eur J Endocrinol 1995, 132:487-496
53. Hiddinga HJ, Eberhardt NL: Intracellular amyloidogenesis by human islet amyloid polypeptide induces apoptosis in COS-1cells. Am J Pathol 1999, 154:1077-1088
54. Paulsson JF, Westermark GT: Aberrant processing of human proislet amyloid polypeptide results in increased amyloid for-mation. Diabetes 2005, 54:2117-2125
55. Wirths O, Multhaup G, Bayer TA: A modified beta-amyloidhypothesis: intraneuronal accumulation of the beta-amyloidpeptide--the first step of a fatal cascade. J Neurochem 2004, 91:513-520
56. Takahashi RH, Nam EE, Edgar M, Gouras GK: Alzheimer beta-amyloid peptides: normal and abnormal localization. His-tol Histopathol 2002, 17:239-246
57. Marzban L, Trigo-Gonzalez G, Verchere CB: Processing of pro-islet amyloid polypeptide in the constitutive and regulated secretory pathways of beta cells. Mol Endocrinol 2005, 19:2154-2163
58. Stefani M, Dobson CM: Protein aggregation and aggregate toxicity: new insights into protein folding, misfolding diseases and biological evolution. J Mol Med 2003, 81:678-699
59. Bucciantini M, Calloni G, Chiti F, Formigli L, Nosi D, Dob-son CM, Stefani M: Prefibrillar amyloid protein aggregates share common features of cytotoxicity. J Biol Chem 2004, 279:31374-31382
60. Kirkitadze MD, Bitan G, Teplow DB: Paradigm shifts in Alz-heimer's disease and other neurodegenerative disorders: the

47
emerging role of oligomeric assemblies. J Neurosci Res 2002, 69:567-577
61. Klein WL, Stine WB, Jr., Teplow DB: Small assemblies of unmodified amyloid beta-protein are the proximate neurotoxin in Alzheimer's disease. Neurobiol Aging 2004, 25:569-580
62. Janson J, Ashley RH, Harrison D, McIntyre S, Butler PC: The mechanism of islet amyloid polypeptide toxicity is membrane disruption by intermediate-sized toxic amyloid particles. Dia-betes 1999, 48:491-498
63. Andersson K, Olofsson A, Nielsen EH, Svehag SE, Lundgren E: Only amyloidogenic intermediates of transthyretin induce apoptosis. Biochem Biophys Res Commun 2002, 294:309-314
64. Olofsson A, Ostman J, Lundgren E: Amyloid: morphology and toxicity. Clin Chem Lab Med 2002, 40:1266-1270
65. Austen B, el-Agnaf O, Nagala S, Patel B, Gunasekera N, Lee M, Lelyveld V: Properties of neurotoxic peptides related to the BRI gene. Biochem Soc Trans 2002, 30:557-559
66. Persson A, Peng S, Gerwins P, Fu X, Westermark P: Effects of lactadherin and medin on smooth muscle cells in amyloid and amyloidosis. CRC Press, Boca, USA 2004:454-456
67. Jiang X, Smith CS, Petrassi HM, Hammarstrom P, White JT, Sacchettini JC, Kelly JW: An engineered transthyretin mono-mer that is nonamyloidogenic, unless it is partially denatured. Biochemistry 2001, 40:11442-11452
68. Lundmark K, Westermark GT, Nystrom S, Murphy CL, Solomon A, Westermark P: Transmissibility of systemic amy-loidosis by a prion- like mechanism. Proc Natl Acad Sci U S A 2002, 99:6979-6984
69. Ganowiak K, Hultman P, Engstrom U, Gustavsson A, Westermark P: Fibrils from synthetic amyloid-related peptides enhance development of experimental AA-amyloidosis in mice. Biochem Biophys Res Commun 1994, 199:306-312
70. Hardt F, Claesson MH: Casein- induced amyloidosis in the nude mouse. I. Acceleration of amyloidosis in recipients of spleen grafts from casein-sensitized donor mice. II. Transfer of amyloidosis by spleen cells. Acta Pathol Microbiol Scand [B] Microbiol Immunol 1974, 82:403-408
71. Korenaga T, Fu X, Xing Y, Matsusita T, Kuramoto K, Syu-miya S, Hasegawa K, Naiki H, Ueno M, Ishihara T, Hoso-kawa M, Mori M, Higuchi K: Tissue distribution, biochemical

48
properties, and transmission of mouse type A AApoAII amy-loid fibrils. Am J Pathol 2004, 164:1597-1606
72. Behl C, Sagara Y: Mechanism of amyloid beta protein in-duced neuronal cell death: current concepts and future per-spectives. J Neural Transm Suppl 1997, 49:125-134
73. Niikura T, Hashimoto Y, Tajima H, Nishimoto I: Death and survival of neuronal cells exposed to Alzheimer's insults. J Neurosci Res 2002, 70:380-391
74. Yan SD, Roher A, Chaney M, Zlokovic B, Schmidt AM, Stern D: Cellular cofactors potentiating induction of stress and cyto-toxicity by amyloid beta-peptide. Biochim Biophys Acta 2000, 1502:145-157
75. Hu J, Igarashi A, Kamata M, Nakagawa H: Angiotensin-converting enzyme degrades Alzheimer amyloid beta-peptide(A beta ); retards A beta aggregation, deposition, fibril forma-tion; and inhibits cytotoxicity. J Biol Chem 2001, 276:47863-47868
76. Yamada M: Cerebral amyloid angiopathy: an overview. Neu-ropathology 2000, 20:8-22
77. Maat-Schieman ML, van Duinen SG, Bornebroek M, Haan J, Roos RA: Hereditary cerebral hemorrhage with amyloidosis-Dutch type (HCHWA-D): II--A review of histopathological aspects. Brain Pathol 1996, 6:115-120
78. Prior R, D'Urso D, Frank R, Prikulis I, Pavlakovic G: Loss of vessel wall viability in cerebral amyloid angiopathy. Neurore-port 1996, 7:562-564
79. Auerbach ID, Sung SH, Wang Z, Vinters HV: Smooth muscle cells and the pathogenesis of cerebral microvascular disease ("angiomyopathies"). Exp Mol Patho l 2003, 74:148-159
80. Jensson O, Palsdottir A, Thorsteinsson L, Arnason A, Abra-hamson M, Olafsson I, Grubb A: Cystatin C mutation causing amyloid angiopathy and brain hemorrhage. Biol Chem Hoppe Seyler 1990, 371 Suppl:229-232
81. Levy E, Lopez-Otin C, Ghiso J, Geltner D, Frangione B: Stroke in Icelandic patients with hereditary amyloid angiopa-thy is related to a mutation in the cystatin C gene, an inhibitor of cysteine proteases. J Exp Med 1989, 169:1771-1778
82. Kyle RA, Greipp PR: Amyloidosis (AL). Clinical and labora-tory features in 229 cases. Mayo Clin Proc 1983, 58:665-683

49
83. Okada K, Takahashi S, Horiuchi K, Nagura Y, Hatano M: A case of primary systemic amyloidosis with AA protein. Nip-pon Jinzo Gakkai Shi 1991, 33:529-531
84. Schwartz AB: Amyloidosis, cause and manifestation of senile deterioration. Springfield 1ll 1970
85. Mucchiano G, Cornwell GG, 3rd, Westermark P: Senile aortic amyloid. Evidence for two distinct forms of localized deposits. Am J Pathol 1992, 140:871-877
86. Mucchiano GI, Haggqvis t B, Sletten K, Westermark P: Apoli-poprotein A-1-derived amyloid in atherosclerotic plaques of the human aorta. J Pathol 2001, 193:270-275
87. Westermark P, Mucchiano G, Marthin T, Johnson KH, Sletten K: Apolipoprotein A1-derived amyloid in human aortic atherosclerotic plaques. Am J Pathol 1995, 147:1186-1192
88. Cornwell GG, 3rd, Murdoch WL, Kyle RA, Westermark P, Pitkanen P: Frequency and distribution of senile cardiovascu-lar amyloid. A clinicopathologic correlation. Am J Med 1983, 75:618-623
89. Johnson KH, Sletten K, Hayden DW, O'Brien TD, Roertgen KE, Westermark P: Pulmonary vascular amyloidosis in aged dogs. A new form of spontaneously occurring amyloidosis de-rived from apolipoprotein AI. Am J Pathol 1992, 141:1013-1019
90. Iwata T, Kamei T, Uchino F, Mimaya H, Yanagaki T, Etoh H: Pathological study on amyloidosis--relationship of amyloid deposits in the aorta to aging. Acta Pathol Jpn 1978, 28:193-203
91. Cornwell GG, 3rd, Westermark P, Murdoch W, Pitkanen P: Senile aortic amyloid. A third distinctive type of age-relatedcardiovascular amyloid. Am J Pathol 1982, 108:135-139
92. Ishii T, Hosoda Y, Ikegami N, Shimada H: Senile amyloid deposition. J Pathol 1983, 139:1-22
93. Battaglia S, Trentini GP: Aortenamyloidose im Erwachsene-nalter. Virchows Arch A Pathol Anat Histol 1978, 378:153-159
94. Haggqvist B, Naslund J, Sletten K, Westermark GT, Muc-chiano G, Tjernberg LO, Nordstedt C, Engstrom U, Wester-mark P: Medin: an integral fragment of aortic smooth muscle cell-produced lactadherin forms the most common humanamyloid. Proc Natl Acad Sci U S A 1999, 96:8669-8674

50
95. Wright JR, Calkins E: Relationship of amyloid deposits in the human aorta to aortic atherosclerosis. A postmortem study of 100 individuals over 60 years of age. Lab Invest 1974, 30:767-773
96. Taylor MR, Couto JR, Scallan CD, Ceriani RL, Peterson JA: Lactadherin (formerly BA46), a membrane-associated glyco-protein expressed in human milk and breast carcinomas, pro-motes Arg-Gly-Asp (RGD)-dependent cell adhesion. DNA Cell Biol 1997, 16:861-869
97. Giuffrida MG, Cavaletto M, Giunta C, Conti A, Godovac-Zimmermann J: Isolation and characterization of full and trun-cated forms of human breast carcinoma protein BA46 from human milk fat globule membranes. J Protein Chem 1998, 17:143-148
98. Cavaletto M, Giuffrida MG, Giunta C, Vellano C, Fabris C, Bertino E, Godovac-Zimmermann J, Conti A: Multiple forms of lactadherin (breast antigen BA46) and butyrophilin are se-creted into human milk as major components of milk fat glob-ule membrane. J Dairy Res 1999, 66:295-301
99. Carmon L, Bobilev-Priel I, Brenner B, Bobilev D, Paz A, Bar-Haim E, Tirosh B, Klein T, Fridkin M, Lemonnier F, Tze-hoval E, Eisenbach L: Characterization of novel breast carci-noma-associated BA46-derived peptides in HLA-A2.1/D(b)-beta2m transgenic mice. J Clin Invest 2002, 110:453-462
100. Shi J, Heegaard CW, Rasmussen JT, Gilbert GE: Lactadherin binds selectively to membranes containing phosphatidyl-L-serine and increased curvature. Biochim Biophys Acta 2004, 1667:82-90
101. Andersen MH, Graversen H, Fedosov SN, Petersen TE, Ras-mussen JT: Functional analyses of two cellular binding do-mains of bovine lactadherin. Biochemistry 2000, 39:6200-6206
102. Andersen MH, Berglund L, Petersen TE, Rasmussen JT: An-nexin-V binds to the intracellular part of the beta(5) integrin receptor subunit. Biochem Biophys Res Commun 2002, 292:550-557
103. Shi J, Gilbert GE: Lactadherin inhibits enzyme complexes of blood coagulation by competing for phospholipid-bindingsites. Blood 2003, 101:2628-2636

51
104. Kruger W, Lohner R, Jung R, Kroger N, Zander AR: Expres-sion of human milk fat globulin proteins in cells of haemopoi-etic origin. Br J Cancer 2000, 83:874-879
105. Peterson JA, Scallan CD, Ceriani RL, Hamosh M: Structural and functional aspects of three major glycoproteins of the hu-man milk fat globule membrane. Adv Exp Med Biol 2001, 501:179-187
106. Ortel TL, Quinn-Allen MA, Keller FG, Peterson JA, Larocca D, Kane WH: Localization of functionally important epitopes within the second C-type domain of coagulation factor V us-ing recombinant chimeras. J Biol Chem 1994, 269:15898-15905
107. Garin J, Diez R, Kieffer S, Dermine JF, Duclos S, Gagnon E, Sadoul R, Rondeau C, Desjardins M: The phagosome pro-teome: insight into phagosome functions. J Cell Biol 2001, 152:165-180
108. Newburg DS: Human milk glycoconjugates that inhibit patho-gens. Curr Med Chem 1999, 6:117-127
109. Peterson JA, Hamosh M, Scallan CD, Ceriani RL, Henderson TR, Mehta NR, Armand M, Hamosh P: Milk fat globule gly-coproteins in human milk and in gastric aspirates of mother's milk-fed preterm infants. Pediatr Res 1998, 44:499-506
110. Andersen MH, Berglund L, Rasmussen JT, Petersen TE: Bo-vine PAS-6/7 binds alpha v beta 5 integrins and anionic phos-pholipids through two domains. Biochemistry 1997, 36:5441-5446
111. Larocca D, Peterson JA, Urrea R, Kuniyoshi J, Bistrain AM, Ceriani RL: A Mr 46,000 human milk fat globule protein that is highly expressed in human breast tumors contains factor VIII-like domains. Cancer Res 1991, 51:4994-4998
112. Couto JR, Taylor MR, Godwin SG, Ceriani RL, Peterson JA: Cloning and sequence analysis of human breast epithelial an-tigen BA46 reveals an RGD cell adhesion sequence presented on an epidermal growth factor- like domain. DNA Cell Biol 1996, 15:281-286
113. Hanayama R, Tanaka M, Miwa K, Shinohara A, Iwamatsu A, Nagata S: Identification of a factor that links apoptotic cells to phagocytes. Nature 2002, 417:182-187
114. Akakura S, Singh S, Spataro M, Akakura R, Kim JI, Albert ML, Birge RB: The opsonin MFG-E8 is a ligand for the al-phavbeta5 integrin and triggers DOCK180-dependent Rac1

52
activation for the phagocytosis of apoptotic cells. Exp Cell Res 2004, 292:403-416
115. Silvestre JS, Thery C, Hamard G, Boddaert J, Aguilar B, Del-cayre A, Houbron C, Tamarat R, Blanc-Brude O, Heeneman S, Clergue M, Duriez M, Merval R, Levy B, Tedgui A, Ami-gorena S, Mallat Z: Lactadherin promotes VEGF-dependentneovascularization. Nat Med 2005, 11:499-506
116. Newburg DS, Peterson JA, Ruiz-Palacios GM, Matson DO, Morrow AL, Shults J, Guerrero ML, Chaturvedi P, Newburg SO, Scallan CD, Taylor MR, Ceriani RL, Pickering LK: Role of human-milk lactadherin in protection against symptomatic rotavirus infection. Lancet 1998, 351:1160-1164
117. Black ME, Armstrong D: Human-milk lactadherin in protec-tion against rotavirus. Lancet 1998, 351:1815-1816
118. Peterson JA, Patton S, Hamosh M: Glycoproteins of the hu-man milk fat globule in the protection of the breast- fed infant against infections. Biol Neonate 1998, 74:143-162
119. Persson A, Peng S, Persson H, Rosenbloom J, Abrams W, Wassberg E, Thelin S, Sletten K, Gerwins P, Westermark P: Lactadherin binds to elastin-a starting point for medin amyloid formation? Amyloid 2006, in press
120. Silver FH, Horvath I, Foran DJ: Viscoelasticity of the vessel wall: the role of collagen and elastic fibers. Crit Rev Biomed Eng 2001, 29:279-301
121. Nakashima Y, Shiokawa Y, Sueishi K: Alterations of elastic architecture in human aortic dissecting aneurysm. Lab Invest 1990, 62:751-760
122. Dingemans KP, Teeling P, Lagendijk JH, Becker AE: Ex-tracellular matrix of the human aortic media: an ultrastructural histochemical and immunohistochemical study of the adult aortic media. Anat Rec 2000, 258:1-14
123. Drake CJ, Hungerford JE, Little CD: Morphogenesis of the first blood vessels. Ann N Y Acad Sci 1998, 857:155-179
124. Gay S, Balleisen L, Remberger K, Fietzek PP, Adelmann BC, Kuhn K: Immunohistochemical evidence for the presence of collagen type III in human arterial walls, arterial thrombi, and in leukocytes, incubated with collagen in vitro. Klin Wochenschr 1975, 53:899-902
125. McCullagh KG, Duance VC, Bishop KA: The distribution of collagen types I, III and V (AB) in normal and atherosclerotic human aorta. J Pathol 1980, 130:45-55

53
126. Bigi A, Ripamonti A, Roveri N: X-ray diffraction and scan-ning electron microscopy of bovine media aortic wall. Con-nect Tissue Res 1977, 5:37-39
127. Salvarani C, Gabriel SE, O'Fallon WM, Hunder GG: The in-cidence of giant cell arteritis in Olmsted County, Minnesota:apparent fluctuations in a cyclic pattern. Ann Intern Med 1995, 123:192-194
128. Salvarani C, Crowson CS, O'Fallon WM, Hunder GG, Gabriel SE: Reappraisal of the epidemiology of giant cell arteritis in Olmsted County, Minnesota, over a fifty-year period. Arthritis Rheum 2004, 51:264-268
129. Baldursson O, Steinsson K, Bjornsson J, Lie JT: Giant cell arteritis in Iceland. An epidemiologic and histopathologic analysis. Arthritis Rheum 1994, 37:1007-1012
130. Noltorp S, Svensson B: High incidence of polymyalgia rheu-matica and giant cell arteritis in a Swedish community. Clin Exp Rheumatol 1991, 9:351-355
131. Hunder GG: Giant cell arteritis. Lupus 1998, 7:266-269132. Brack A, Geisler A, Martinez-Taboada VM, Younge BR,
Goronzy JJ, Weyand CM: Giant cell vasculitis is a T cell-dependent disease. Mol Med 1997, 3:530-543
133. Weyand CM, Goronzy JJ: Arterial wall injury in giant cell arteritis. Arthritis Rheum 1999, 42:844-853
134. Weyand CM, Goronzy JJ: Pathogenic mechanisms in giant cell arteritis. Cleve Clin J Med 2002, 69 Suppl 2:SII28-32
135. Goronzy JJ, Weyand CM: Cytokines in giant-cell arteritis. Cleve Clin J Med 2002, 69 Suppl 2:SII91-94
136. Sorbi D, French DL, Nuovo GJ, Kew RR, Arbeit LA, Gruber BL: Elevated levels of 92-kd type IV collagenase (matrix met-alloproteinase 9) in giant cell arteritis. Arthritis Rheum 1996, 39:1747-1753
137. Rodriguez-Pla A, Bosch-Gil JA, Rossello-Urgell J, Huguet-Redecilla P, Stone JH, Vilardell-Tarres M: Metalloproteinase-2 and -9 in giant cell arteritis: involvement in vascular remod-eling. Circulation 2005, 112:264-269
138. Erdheim VJ: Medionecrosis aortae idiopathica. Virchows Arch 1929:454-479
139. Erdheim VJ: Medionecrosis aortae idiopathica cystica. Vir-chows Arch 1930:186-229
140. Kowalewski R, Sobolewski K, Malkowski A, Wolanska M, Gacko M: Evaluation of enzymes involved in proteoglycan

54
degradation in the wall of abdominal aortic aneurysms. J Vasc Res 2006, 43:95-100
141. Taketani T, Imai Y, Morota T, Maemura K, Morita H, Haya-shi D, Yamazaki T, Nagai R, Takamoto S: Altered patterns of gene expression specific to thoracic aortic aneurysms: mi-croarray analysis of surgically resected specimens. Int Heart J 2005, 46:265-277
142. Nuenninghoff DM, Hunder GG, Christianson TJ, McClelland RL, Matteson EL: Mortality of large-artery complication (aor-tic aneurysm, aortic dissection, and/or large-artery stenosis) in patients with giant cell arteritis: a population-based study over 50 years. Arthritis Rheum 2003, 48:3532-3537
143. Larson EW, Edwards WD: Risk factors for aortic dissection: a necropsy study of 161 cases. Am J Cardiol 1984, 53:849-855
144. Klein DG: Thoracic aortic aneurysms. J Cardiovasc Nurs 2005, 20:245-250
145. Neri E, Toscano T, Civeli L, Capannini G, Tucci E, Sassi C: Acute dissecting aneurysm of the ascending thoracic aorta causing obstruction and thrombosis of the right pulmonary ar-tery. Tex Heart Inst J 2001, 28:149-151
146. Muckle TJ: Giant cell inflammation compared with amyloido-sis of the internal elastic lamina in temporal arteries. Arthritis Rheum 1988, 31:1186-1189
147. Schagger H, von Jagow G: Tricine-sodium dodecyl sulfate-polyacrylamide gel electrophoresis for the separation of pro-teins in the range from 1 to 100 kDa. Anal Biochem 1987, 166:368-379
148. Martinez-Taboada V, Hunder NN, Hunder GG, Weyand CM,Goronzy JJ: Recognition of tissue residing antigen by T cells in vasculitic lesions of giant cell arteritis. J Mol Med 1996, 74:695-703
149. Blockmans D, Maes A, Stroobants S, Nuyts J, Bormans G, Knockaert D, Bobbaers H, Mortelmans L: New arguments for a vasculitic nature of polymyalgia rheumatica using positron emission tomography. Rheumatology (Oxford) 1999, 38:444-447
150. Gravanis MB: Giant cell arteritis and Takayasu aortitis: mor-phologic, pathogenetic and etiologic factors. Int J Cardiol 2000, 75 Suppl 1:S21-33; discussion S35-26
151. Kobayashi S, Yano T, Matsumoto Y, Numano F, Nakajima N, Yasuda K, Yutani C, Nakayama T, Tamakoshi A, Kawamura

55
T, Ohno Y, Inaba Y, Hashimoto H: Clinical and epidemi-ologic analysis of giant cell (temporal) arteritis from a nation-wide survey in 1998 in Japan: the first government-supportednationwide survey. Arthritis Rheum 2003, 49:594-598
152. Weyand CM, Goronzy JJ: Pathogenic principles in giant cell arteritis. Int J Cardiol 2000, 75 Suppl 1:S9-S15; discussion S17-19
153. Anders KH, Wang ZZ, Kornfeld M, Gray F, Soontornniyom-kij V, Reed LA, Hart MN, Menchine M, Secor DL, Vinters HV: Giant cell arteritis in association with cerebral amyloid angiopathy: immunohistochemical and molecular studies. Hum Pathol 1997, 28:1237-1246
154. McLean CA, Cherny RA, Fraser FW, Fuller SJ, Smith MJ, Beyreuther K, Bush AI, Masters CL: Soluble pool of Abeta amyloid as a determinant of severity of neurodegeneration in Alzheimer's disease. Ann Neurol 1999, 46:860-866
155. Lue LF, Kuo YM, Roher AE, Brachova L, Shen Y, Sue L, Beach T, Kurth JH, Rydel RE, Rogers J: Soluble amyloid beta peptide concentration as a predictor of synaptic change in Alzheimer's disease. Am J Pathol 1999, 155:853-862
156. Ma Z, Westermark GT, Li ZC, Engstrom U, Westermark P:Altered immunoreactivity of islet amyloid polypeptide (IAPP) may reflect major modifications of the IAPP molecule in amy-loidogenesis. Diabetologia 1997, 40:793-801
157. Roher AE, Chaney MO, Kuo YM, Webster SD, Stine WB, Haverkamp LJ, Woods AS, Cotter RJ, Tuohy JM, Krafft GA, Bonnell BS, Emmerling MR: Morphology and toxicity of Abeta-(1-42) dimer derived from neuritic and vascular amy-loid deposits of Alzheimer's disease. J Biol Chem 1996, 271:20631-20635
158. Kayed R, Head E, Thompson JL, McIntire TM, Milton SC, Cotman CW, Glabe CG: Common structure of soluble amy-loid oligomers implies common mechanism of pathogenesis. Science 2003, 300:486-489
159. Evans JM, O'Fallon WM, Hunder GG: Increased incidence of aortic aneurysm and dissection in giant cell (temporal) arteritis. A population-based study. Ann Intern Med 1995, 122:502-507
160. Eriksson L, Westermark P: Age-related accumulation of amy-loid inclusions in adrenal cortical cells. Am J Pathol 1990, 136:461-466

56
161. O'Brien TD, Butler AE, Roche PC, Johnson KH, Butler PC: Islet amyloid polypeptide in human insulinomas. Evidence for intracellular amyloidogenesis. Diabetes 1994, 43:329-336
162. Westermark GT, Steiner DF, Gebre-Medhin S, Engstrom U, Westermark P: Pro islet amyloid polypeptide (ProIAPP) im-munoreactivity in the islets of Langerhans. Ups J Med Sci 2000, 105:97-106


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 129
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-6700
ACTA
UNIVERSITATIS
UPSALIENSIS
UPPSALA
2006


















