mbbs ims msu
67
Mediated Transport System Passage of large molecule and some ions are mediated by integral membrane proteins known as transporters Transport solute bind by specific site on the transporter Change of the shape of transporter Molecules can move in either direction. The oscillation in conformation occur continuously.
-
Upload
mbbs-ims-msu -
Category
Health & Medicine
-
view
763 -
download
0
description
physiology
Transcript of mbbs ims msu

Mediated Transport System
Passage of large molecule and some ions are mediated by integral membrane proteins known as transporters
Transport solute bind by specific site on the transporter
Change of the shape of transporter Molecules can move in either direction. The oscillation in conformation occur
continuously.

Two typesFacilitated diffusionActive transport Facilitated diffusion uses transporter
to move solute downhill from higher to lower concentration.
Active transporter uses energy to move solute uphill across the membrane
Mediated Transport System

Diffusion Through the Plasma Membrane

Facilitated Diffusion From high to low concentration until the
concentration on the two side of the membrane equal
No energy required Facilitated diffusion such as those transport
glucoseThe transporter differs in their affinity of their binding sites for glucoseTheir maximal rates of transport when saturatedModulation of their transport activity by various chemical signals

When the concentration of x molecules outside the cell is low, the transport rate is low because it is limited by the number of molecules available to be transported.
When more molecules are present outside the cell, as long as enough carrier proteins are available, more molecules can be transported; thus, the transport rate increases.
The transport rate is limited by the number of carrier proteins and the rate at which each carrier protein can transport solutes. When the number of molecules outside the cell is so large that the carrier proteins are all occupied, the system is saturated and the transport rate cannot increase.
Saturation of a Carrier Protein

Facilitated Diffusion
Passive process, i.e. no ATP usedSolute binds to receptor on carrier protein
Changes shape then releases solute on other side of membraneSubstance moved down its concentration gradient

Active Transport
Require energy to move substance uphill across the membrane
Require binding substance to the transporter
They referred as pumps Exhibits specificity and saturation

Two means of energy flow:1. The direct use of ATP in primary
active transport2. The use of ion concentration
difference across membrane to drive the process secondary active transport
Active Transport

Primary Active Transport
1. Na,K-ATPase2. Ca-ATPase3. H-ATPase4. H,K-ATPase

Na,K-ATPase: Present in all plasma membrane The pumping activity leads to distribution of
high intracellular K and low intracellular Na relative to their extracellular concentration.
Ca-ATPase Found in the plasma membrane and several
organelle membranes In plasma membrane the direction from
cytosol to the extracellular fluid. In organelle membrane from cytosol into the organelle lumen
Primary Active Transport

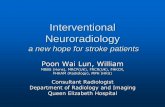
Primary active transport (Na+/K+ ATPase pump)3 Na+’s out, 2 K+’s in, 1 ATP hydrolyzed

Effect of Na+/K+ ATPase pump
fig 4-12

Extracellular fluid
Binding of cytoplasmic Na+ to the pump protein stimulates phosphorylation by ATP.
Phosphorylation causes the protein to change its shape.
Concentration gradients of K+ and Na+
The shape change expels Na+ to the outside, and extracellular K+ binds.
K+ binding triggers release of the phosphate group.
Loss of phosphate restores the original conformation of the pump protein.
K+ is released and Na+ sites are ready to bind Na+ again; the cycle repeats.
Sodium-Potassium Pump

H-ATPase In the plasma membrane and several
organelle membranes Moves hydrogen ions out of the cell H,K-ATPase In the plasma membrane of acid
secreting cells It moves one hydrogen ion out of the
cell and moves one potassium in.
Primary Active Transport

Secondary Active Transport
Uses ion concentration gradient across membrane as energy source
Having binding site for ion and actively transported solute

Secondary active transport
fig 4-13

1. A sodium-potassium
exchange pump maintains a concentration of Na that is higher outside the cell than inside. Active transport.
2. Na moves back into the cell by a carrier protein that also moves glucose. The concentration gradient for Na provides the energy required to move glucose against its concentration gradient.
Secondary Active Transport

The movement of Na is always from high extracellular concentration into the cell where the concentration is lower
The movement of solute can be into the cell (same direction as Na) cotransport or out of the cell (opposite direction of Na movement) is called countertransport
Secondary Active Transport

Composition of extracellular and
intracellular fluidsExtracellular Con. mM
Intracellular Con. mM
Na 145 15
K 4 150
Ca 1 1.5
Cl 110 10
ATP 0 4
Protein 0.2 4

FacilitatedDiffusion
Primary Active Transport
Secondary Active Transport
Use of integral membrane protein
Yes Yes Yes
Typical molecules using pathway
Polar: Glucose
IonsNa, K ,Ca , H
Polar:A.A, Glucose , some ions
Chemical specificity
Yes Yes Yes
Major characteristics of mediated transport

Epithelial Transport
Epithelial cells line hollow organ regulate absorption of substance
One surface faces a hollow refers to luminal membrane of the epithelium
The plasma membrane opposite surface refers to basolateral membrane

Two pathways:1. Paracellular pathway: diffusion
between the adjacent cell2. Transcellular pathway: movement
into the epithelial cell across either luminal
Epithelial Transport

Paracellular is limited by the presence of tight junctions
Transcellular: movement of molecule occur via the pathways.
Transport characteristics of the luminal and basolateral membrane are not the same
Epithelial Transport

Diffusion Summary
Diffusion is the movement of molecule from one location to another by random thermal motion
The net flux between the two compartments always proceed from higher to lower concentration
Diffusion equilibirum is reached when the two concentration become equal

Nonpolar molecule diffuse rapidly than do polar or ionized molecules
Mineral ions diffuse across membranes by passing through ion channels formed by integral proteins
Diffusion of ions across membrane depends on both concentration difference and the membrane potential.
The flux of ions across a membrane can be altered by opening and closing ion channels
Diffusion Summary

Osmosis Summary
Water crosses membranes by (1) diffusion through lipid by layer and (2) diffusing through protein channels in the membrane
Osmosis is the diffusion of water from higher water concentration to lower water concentration. Osmolarity total solute concentration in the solution. The higher osmolarity of a solution the lower the water concentration.

Osmosis across membrane permeable to water but impermeable to solute leads to increase volume in the compartment that initially had higher osmolarity.
Application to a solution of sufficient pressure will prevent the osmotic flow of water into the solution from the compartment of pure water. This pressure is osmotic pressure.
Osmosis Summary

Permeable to water,Not permeable to solutes
Presence of a membraneImpermeable to soluteThat leads to the volumeChanges associated withOsmosis.

Tonicity
Describes the behavior of a cell when it is placed in a solution
Depends not only on the number of particles in solution, but also on the NATURE of the solute

Water diffuses inWater diffuses out

-osmotic vs. -tonic
Example: 1L solution containing 300 mOsm of non-penetrating NaCl and 100 mOsm of urea, which can cross the membrane would have a total osmolarity of 400 mOsm and would be hyperosmotic. However, it would be an isotonic solution producing no change in the equilibrium volume of cells immersed in it.

Therapies Based on Two Basic Principles
Water moves rapidly across cell membranes: Osmolarities of ICF and ECF remain almost exactly equal
Cell membranes are almost completely impermeable to many solutes: the number of osmoles in the ECF or ICF remains constant unless solutes are added or lost from the ECF compartment

Transport, the big picture
fig 4-15

Facilitated diffusion (properties)
Passive, carrier mediated
Examples: glucose into most cells (not luminal membrane of kidney or intestine), urea, some amino acids
Kinetics:
shows: passive shows: carrier mediated

Non-mediated vs. mediated transport
fig 4-9

Primary active transport (Na+/K+ ATPase pump)3 Na+’s out, 2 K+’s in, 1 ATP hydrolyzed
fig 4-11

Primary active transport kinetics
shows active transport shows carrier mediated

Secondary active transport properties
Active (energy from ion gradient, usually Na+)
Carrier mediated
Can be cotransport (symport) or countertransport (antiport)
Examples (many):Na+/amino acids, Na+/glucose (luminal membrane kidney, GI tract), *Na+/H+ kidney, *Ca++/3Na+ muscle, *Cl-/HCO3
- red cell. (* = countertransport)
Kineticssee primary active transport graphs

Sodium Reabsorption: Primary Active Sodium Reabsorption: Primary Active TransportTransport
Sodium Sodium reabsorption is almost always by reabsorption is almost always by active active transporttransport NaNa++ enters the tubule cells at the luminal enters the tubule cells at the luminal
membranemembrane Is actively transported out of the tubules by a Is actively transported out of the tubules by a
NaNa++-K-K++ ATPase pump ATPase pump From there it moves to peritubular capillaries due to:From there it moves to peritubular capillaries due to:
Low hydrostatic pressureLow hydrostatic pressure High osmotic pressure of the bloodHigh osmotic pressure of the blood
NaNa++ reabsorption provides the energy and the means reabsorption provides the energy and the means for reabsorbing most other solutesfor reabsorbing most other solutes

Electrolytes-SodiumElectrolytes-Sodium Major Major cation in ECFcation in ECF (positively charged)(positively charged) Responsible for Responsible for 90-9590-95% of extracellular % of extracellular
osmotic pressureosmotic pressure Regulated by Regulated by aldosterone and the aldosterone and the
kidneyskidneys Increases sodium reabsorption in DCT of Increases sodium reabsorption in DCT of
nephronnephron Also regulates K+ (secretion)Also regulates K+ (secretion)
Normal serum concentration in ECF Normal serum concentration in ECF ranges from 135-146 mEq/Lranges from 135-146 mEq/L

Sodium FunctionsSodium Functions
Sodium maintains ECF osmolality, ECF Sodium maintains ECF osmolality, ECF volume, and volume, and influences water influences water distributiondistribution (where salt goes water (where salt goes water follows)follows)
It affects the concentration, secretion, It affects the concentration, secretion, and adsorption of potassium and and adsorption of potassium and chloride ions, and can combine with chloride ions, and can combine with bicarbonate ions and chloride ions to bicarbonate ions and chloride ions to help regulate acid/base balancehelp regulate acid/base balance
It also help aid the impulse It also help aid the impulse transmission of nerve and muscle fiberstransmission of nerve and muscle fibers

Sodium Recycling: Sodium Recycling: Recycling and ExcretionRecycling and Excretion
Ascending loop of HenleAscending loop of Henle HH22O impermeableO impermeable NaNa++ Active Transport Active Transport
To ECF To ECF GradientGradient Diffuses to bloodDiffuses to blood
Collecting Duct:Collecting Duct: Aldosterone regulatesAldosterone regulates NaNa++ recycled or excreted recycled or excreted

Aldosterone: steroid H from adrenal cortexAldosterone: steroid H from adrenal cortex Stimulates NaStimulates Na+ + uptake (& Kuptake (& K++ secretion) secretion) channel synthesischannel synthesis
Mechanism of NaMechanism of Na++ Selective Selective Reabsorption in Collecting DuctReabsorption in Collecting Duct

Mechanism of NaMechanism of Na++ Selective Selective Reabsorption in Collecting DuctReabsorption in Collecting Duct
Figure 20-12: Aldosterone action in principal cells

ImbalancesImbalances Hyponatremia Hyponatremia (less than 130 mEq/L)-low (less than 130 mEq/L)-low
sodium level-may cause seizures, headache, sodium level-may cause seizures, headache, tachycardia, hypotension, cramps, muscle tachycardia, hypotension, cramps, muscle twitching, irritability, decreased body temp, twitching, irritability, decreased body temp, nausea, vomiting, and possible coma nausea, vomiting, and possible coma (polyuria due to diabetes insipidis may be (polyuria due to diabetes insipidis may be one cause), one cause),
HypernatremiaHypernatremia (more than 150 mEq/L) -high (more than 150 mEq/L) -high sodium level-usually indicates water deficit in sodium level-usually indicates water deficit in ECF-symptoms include thirst, tachycardia, ECF-symptoms include thirst, tachycardia, dry sticky tongue, disorientation, dry sticky tongue, disorientation, hallucination, lethargy, seizures, coma, hallucination, lethargy, seizures, coma, hypotension, agitation, low feverhypotension, agitation, low fever

Artial Natruretic Peptide: Regulates Artial Natruretic Peptide: Regulates NaNa++ & H2O Excretion & H2O Excretion
Hormone from myocardial cellsHormone from myocardial cells Stimulates: hypothalamus, kidney, Stimulates: hypothalamus, kidney,
adrenal, & medullaadrenal, & medulla

Artial Natruretic Peptide: Regulates Artial Natruretic Peptide: Regulates NaNa++ & H & H22O ExcretionO Excretion
Figure 20-15: Atrial natriuretic peptide

Potassium Balance: Potassium Balance: Critical for Excitable Heart & Critical for Excitable Heart &
Nervous TissuesNervous Tissues
Hypokalemia – low [KHypokalemia – low [K++] in ECF, ] in ECF, Hyperkalemia - high [KHyperkalemia - high [K++] ]
Reabsorbed in Ascending Loop, Reabsorbed in Ascending Loop, secreted in Collecting ductsecreted in Collecting duct

Potassium Balance: Potassium Balance: Critical for Excitable Heart & Critical for Excitable Heart &
Nervous TissuesNervous Tissues
Figure 20-4: Osmolarity changes as fluid flows through the nephron

Potassium Balance: Potassium Balance: Critical for Excitable Heart & Critical for Excitable Heart &
Nervous TissuesNervous Tissues
Figure 20-12: Aldosterone action in principal cells

Thirst & "salt craving", or avoidance behaviorThirst & "salt craving", or avoidance behavior Integrated circulatory & excretory reflexesIntegrated circulatory & excretory reflexes
Response to Dehydration & Response to Dehydration & Osmolarity ImbalanceOsmolarity Imbalance

Response to Dehydration & Response to Dehydration & Osmolarity ImbalanceOsmolarity Imbalance

Acidosis: Acidosis: plasma pH plasma pH Protein damageProtein damage CNS depressionCNS depression
Alkalosis: Alkalosis: plasma pH plasma pH HyperexcitabilityHyperexcitability CNS & heartCNS & heart
Buffers: HCOBuffers: HCO33-- & proteins & proteins
HH++ input: diet & metabolic input: diet & metabolic HH++ output: lungs & kidney output: lungs & kidney
Acid/Base Homeostasis: OverviewAcid/Base Homeostasis: Overview

Acid/Base BalanceAcid/Base Balance
Homeostasis of hydrogen ion contentHomeostasis of hydrogen ion content Body fluids are classified as either acids or Body fluids are classified as either acids or
bases depending on H ion concentrationbases depending on H ion concentration Acid is an H donor Acid is an H donor and elevates the and elevates the
hydrogen ion content of the solution to hydrogen ion content of the solution to which it is addedwhich it is added
Base is an H acceptor Base is an H acceptor and can bind and can bind hydrogen ionshydrogen ions
Concentration is expressed as Concentration is expressed as pHpH Normal pH of blood is 7.35-7.45 Normal pH of blood is 7.35-7.45 (alkaline)(alkaline) pH below 6.8 or above 7.8 is incompatible pH below 6.8 or above 7.8 is incompatible
with lifewith life

AcidsAcids
During the process of cellular metabolism During the process of cellular metabolism acids are continually being formed and acids are continually being formed and excess hydrogen ions must be eliminated excess hydrogen ions must be eliminated
There are two types of acids formed: volatile There are two types of acids formed: volatile acids are excreted by the lungs and acids are excreted by the lungs and nonvolatile acids are excreted by the kidneynonvolatile acids are excreted by the kidney
Volatile acids can be excreted from the body Volatile acids can be excreted from the body as gas. as gas. Carbonic acid produced by the Carbonic acid produced by the hydration of carbon dioxide hydration of carbon dioxide is a volatile acid is a volatile acid
Normally carbon dioxide is excreted by the Normally carbon dioxide is excreted by the lungs as fast as metabolism produces it, so lungs as fast as metabolism produces it, so carbonic acid is carbonic acid is not allowed to accumulatenot allowed to accumulate and alter pHand alter pH

Non-volatile acidsNon-volatile acids
Cannot be eliminated by the lungs and Cannot be eliminated by the lungs and must be eliminated by the kidneys must be eliminated by the kidneys
All metabolic acids except carbolic are All metabolic acids except carbolic are non-volatile acidsnon-volatile acids
These include sulfuric acid, These include sulfuric acid, phosphoric acid, lactic acid, ketoacids phosphoric acid, lactic acid, ketoacids like acetoacetic acid and beta like acetoacetic acid and beta hydroxybutyric acid, and small hydroxybutyric acid, and small amounts of other inorganic and amounts of other inorganic and organic acidsorganic acids

Regulation of pHRegulation of pH
Three methods control pHThree methods control pH 1. 1. chemical buffers-whenchemical buffers-when Hydrogen Hydrogen
is removed a buffer replaces itis removed a buffer replaces it 2. 2. regulation of carbon dioxideregulation of carbon dioxide by by
respiratory systemrespiratory system 3. 3. regulation of plasma bicarbonateregulation of plasma bicarbonate
concentration by the kidneys-concentration by the kidneys-slower, second line of defenseslower, second line of defense

Chemical buffersChemical buffers
These are These are the first line of defensethe first line of defense against changes in pHagainst changes in pH
Act within a fraction of a second for Act within a fraction of a second for immediate defenseimmediate defense against H+ shiftagainst H+ shift
These are a mixture of 2 or more These are a mixture of 2 or more chemicals that minimize changes in chemicals that minimize changes in pHpH
Convert strong acids into weak acids Convert strong acids into weak acids and strong bases into weak basesand strong bases into weak bases

Buffers continuedBuffers continued
Carbonic acid-bicarbonate system is Carbonic acid-bicarbonate system is most most important extracellular bufferimportant extracellular buffer because it because it can be regulated by both lungs and kidneyscan be regulated by both lungs and kidneys
Carbonic acid/bicarbonate ratio is usually Carbonic acid/bicarbonate ratio is usually 1:201:20
COCO2 2 + H+ H22O↔HO↔H2 2 COCO 3 3 ↔H↔H+ + + HCO+ HCO33--
Phosphates act as a buffer like the Phosphates act as a buffer like the bicarbonate system does and protein bicarbonate system does and protein buffers are the most abundant buffers in buffers are the most abundant buffers in body cells and bloodbody cells and blood

Regulation of pH through kidneysRegulation of pH through kidneys
Tubular secretion of H+ from convoluted Tubular secretion of H+ from convoluted tubules and collecting ducts so extra is tubules and collecting ducts so extra is excreted in urineexcreted in urine
Helps regulate sulfuric acid and Helps regulate sulfuric acid and phosphoric acid, and other organic acids phosphoric acid, and other organic acids in body fluids as a result of metabolismin body fluids as a result of metabolism
Diets high in protein generate more acid, Diets high in protein generate more acid, so kidneys respond by secreting more so kidneys respond by secreting more hydrogen ion. (Atkins Diet)hydrogen ion. (Atkins Diet)
In urine, hydrogen ion is buffered by In urine, hydrogen ion is buffered by phosphate and ammoniaphosphate and ammonia

Acid/Base Homeostasis: OverviewAcid/Base Homeostasis: Overview
Figure 20-18: Hydrogen balance in the body

HH+ + & NH& NH44++ secreted into lumen and excreted secreted into lumen and excreted
HCOHCO33- - is reabsorbed is reabsorbed
Kidney Hydrogen Ion Balancing: Kidney Hydrogen Ion Balancing: Proximal TubuleProximal Tubule

Kidney Hydrogen Ion Balancing: Kidney Hydrogen Ion Balancing: Proximal TubuleProximal Tubule
Figure 20-21: Proximal tubule secretion and reabsorption of filtered HCO3-

Type A Intercalated cells excrete HType A Intercalated cells excrete H++ absorb HCO absorb HCO33--
Type B intercalated cells absorb HType B intercalated cells absorb H++ secrete HCO secrete HCO33--
Kidney Hydrogen Ion Balancing: Kidney Hydrogen Ion Balancing: Collecting DuctCollecting Duct

Kidney Hydrogen Ion Balancing: Kidney Hydrogen Ion Balancing: Collecting DuctCollecting Duct
Figure 20-22: Role of the intercalated cell in acidosis and alkalosis

AmmoniaAmmonia
Ammonia (NH3) is a weak base Ammonia (NH3) is a weak base produced in cells of renal tubule by produced in cells of renal tubule by removal of amine group from some removal of amine group from some amino acids amino acids (deamination)(deamination)
It diffuses into the tubule and It diffuses into the tubule and accepts hydrogen ions to become accepts hydrogen ions to become NH4+ which is trapped in the tubule NH4+ which is trapped in the tubule and excretedand excreted

SummarySummary
Electrolyte balance depends on integration of circulatory, Electrolyte balance depends on integration of circulatory, excretory and behavioral physiologyexcretory and behavioral physiology
Water recycling and ECF/plasma balance depends on Water recycling and ECF/plasma balance depends on descending loop of Henle and vasopressin regulated descending loop of Henle and vasopressin regulated collecting duct for conservationcollecting duct for conservation
Osmolarity depends on aldosterone and angiotensin pathway Osmolarity depends on aldosterone and angiotensin pathway to regulate CNS & endocrine responsesto regulate CNS & endocrine responses
Along with respiration, proximal tubule and collecting duct Along with respiration, proximal tubule and collecting duct cells reabsorb or excrete Hcells reabsorb or excrete H++ & HCO & HCO33
-- to balance pH to balance pH