
Mattheus W. Vischer Kathrin Vischer ENT clinic Audiology ... · Mattheus W. Vischer Kathrin Vischer...
11
TRANSTYMPANIC VENTILATION TUBES IN TODDLERS AND SMALL TUBES IN TODDLERS AND SMALL CHILDREN CHILDREN Mattheus W. Vischer Kathrin Vischer ENT clinic Audiology and pediatric audiology Gümligen Bern Switzerland Gümligen Bern Switzerland CONDUCTIVE HARING LOSS CONDUCTIVE HARING LOSS otitis media with effusion cleft palate atelectasis of the middle ear cleft palate atelectasis of the middle ear cleft palate perforation of the ear drum middle ear dysplasia otosclerosis fracture of the temporal bone C it l hl t t Congenital cholesteatoma Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
Transcript of Mattheus W. Vischer Kathrin Vischer ENT clinic Audiology ... · Mattheus W. Vischer Kathrin Vischer...

TRANSTYMPANIC VENTILATION TUBES IN TODDLERS AND SMALL TUBES IN TODDLERS AND SMALL
CHILDRENCHILDREN
Mattheus W. Vischer
Kathrin Vischer
ENT clinic
Audiology and pediatric audiology
Gümligen Bern SwitzerlandGümligen Bern Switzerland
CONDUCTIVE HARING LOSSCONDUCTIVE HARING LOSS
otitis media with effusion cleft palate atelectasis of the middle ear cleft palate atelectasis of the middle ear cleft palate perforation of the ear drum middle ear dysplasia otosclerosis
fracture of the temporal boneC it l h l t t Congenital cholesteatoma
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23

PEDIATRIC AUDIOLOGY - DIAGNOSTICSPEDIATRIC AUDIOLOGY DIAGNOSTICS
anamnesis, history of hearing loss ear microscopyear microscopy tympanometry
b h i l di t behavioural audiometry objective audiometry:
– TEOAEABR– ABR
– Stapedial reflex
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
BEHAVIOUR AUDIOMETRY
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23

BEHAVIOUR AUDIOMETRY
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
TEOAE: PRESENT OR ABSENT?
if TEAOE absent:
estmated HL
b t 35 dB
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
about 35 dB

ABR - BRAINSTEM AUDIOMETRY
NEWBORNup to 3 months: as a rule no sedation
After nursingAfter nursingawake or in
t lVischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
spontaneous sleep
ABR – BRAINSTEM AUDIOMETRY
Right ear Left earRight ear Left ear
dB
85
65
55
45
35
25
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23

MILD HEARING LOSSMILD HEARING LOSS
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
OTITIS MEDIA WITH EFFUSIONOTITIS MEDIA WITH EFFUSION
EFFUSION
Middle ear partiallyp yaerated
Prognosis favorable Prognosis favorable
Milde hearing loss
Ventilation of theEustachian tube withOtoventTM Ballons
NO GROMMETS
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
NO GROMMETS

ATELEKTASIS 1st GRADE
Tympanon aerated
Fixed retraction pockets Fixed retraction pockets
Mild conductive HL
Ventilation with OtoventTM
balloons
Consider long term drainage
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
ATELEKTASIS 1st GRADE
left right
T t di t i d t hi d
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
Tympano stapediopexy, tympano incudopexy, atrophic ear drum
CONDUCTIVE HEARING LOSSCONDUCTIVE HEARING LOSS
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
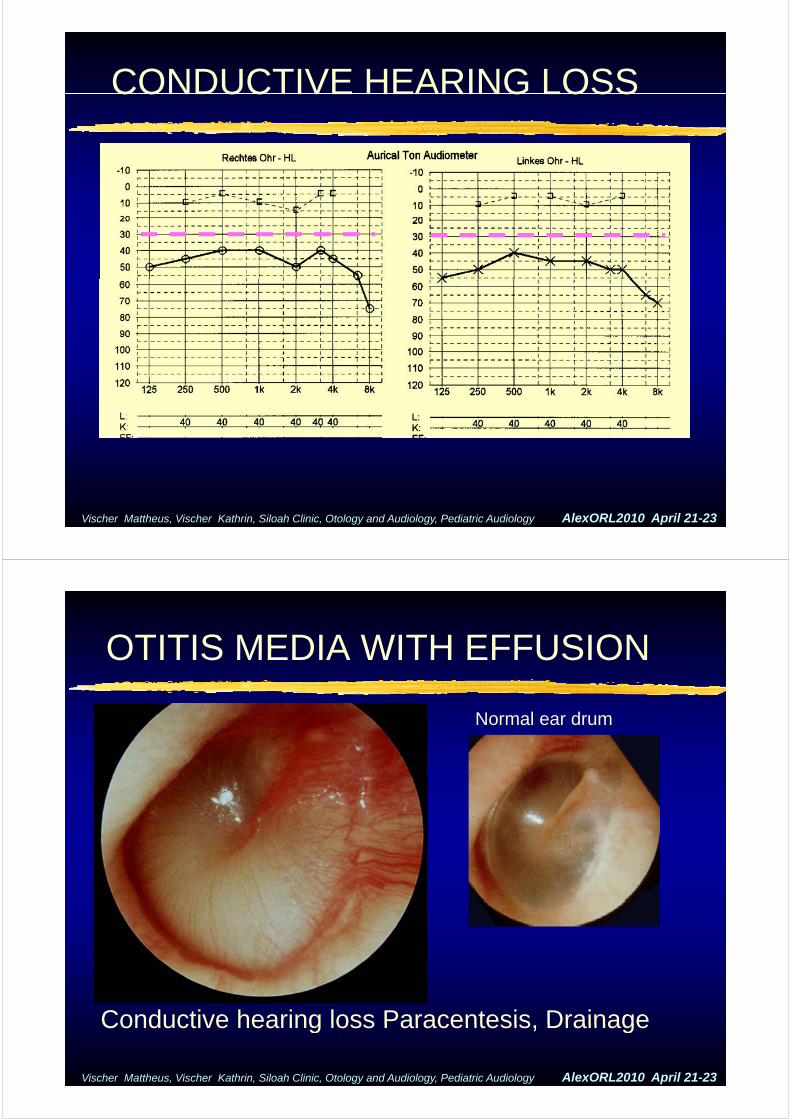
OTITIS MEDIA WITH EFFUSIONOTITIS MEDIA WITH EFFUSION
N l dNormal ear drum
Conductive hearing loss Paracentesis Drainage
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
Conductive hearing loss Paracentesis, Drainage

VENTILATION TUBESVENTILATION TUBES
Ch i f th t f t A f th hildChoice of the type of grommets: Age of the child, cooperative behaviour, Duration of ventilation
mostly T tubes in every case in cleft ypalate: 2 to 4 years often in OMC with effusion: 3 to 4 monthseffusion: 3 to 4 months
Rarely Tübinger tubes In very young children
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
short term
GOOD T TUBE
• Longterm grommet• Good T tubes• Good T tubes
Micromedics• Very soft• Gentle extraction in• Gentle extraction in
the ENT chair
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23

GROMMETS
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
GROMMETSGROMMETS
COMPLICATIONS• Eventually infections with otorhea• Eventually infections with otorhea• Short acting local treatment with antibiotics
• Otosporin or other Aminoglycoside• Frequent recurrent otitis media• Frequent recurrent otitis media• In a few cases: early extraction or change to
an other product was necessary
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23

FOLLOW UP WITH GROMMETS
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
LONG LASTING GROMMETS
Complication of T tubes:persistent perforationpersistent perforation
2 cases:2 cases:no problemsno infectionsno infectionsaudiologically not significant1 child of ophthalmologist1 child of ophthalmologist
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23

CLINICALLY NORMAL HEARING
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23
[email protected]@hin.ch
Vischer Mattheus, Vischer Kathrin, Siloah Clinic, Otology and Audiology, Pediatric Audiology AlexORL2010 April 21-23


















