Manger Et Al-2002-The Journal of Clinical Hypertension
11
THE JOURNAL OF CLINICAL HYPERTENSION VOL. IV NO. I JANUARY/FEBRUARY 2002 62 Pheochromocytoma, a relatively rare (<0.05% of hypertensives), catecholamine-secreting tumor, is almost always lethal unless recognized and ap- propriately treated. Clinical and biochemical manifestations are mainly caused by excess circu- lating catecholamines and hypertension. Manifes- tations mimic many conditions, which may result in erroneous diagnoses and improper treatment. Sustained or paroxysmal hypertension associated with headaches, sweating, or palpitations, occurs in 95% of patients, but at least 5% are nor- motensive. All patients with manifestations of hypercatecholaminemia or coexisting neoplasms should be investigated for pheochromocytoma. Plasma free metanephrines and fractionated uri- nary metanephrines are the most sensitive (≈100%) chemical tests for diagnosing sporadic and familial pheochromocytomas; plasma and urinary catecholamines and total metanephrines are fairly sensitive for identifying sporadic cases but are less sensitive for familial tumors. The clonidine suppression test helps exclude other conditions that may elevate plasma and urinary catecholamines and their metabolites. Magnetic resonance imaging is more sensitive than com- puted tomography for localizing pheochromocy- tomas; iodine-131-metaiodobenzylguanidine ( 131 I-MIBG) tumor uptake confers specificity. Surgical resection is successful in 90% of cases, but 10% of tumors are malignant. Pheochromo- cytomas <5 cm in diameter can be removed la- paroscopically; larger tumors should be removed by open surgery. Drug treatment prior to and during surgery is mandatory; drug treatment, chemotherapy, and radiation therapy are used to treat malignant lesions. (J Clin Hypertens. 2002;4:62–72) © 2002 Le Jacq Communications, Inc. T he key to diagnosing pheochromocytoma is first to think of it! Since this deceptive tumor poses great risk of death or severe complications, early diagnosis and prompt treatment of this “phar- macologic bomb” are crucial. The peril of missing the diagnosis is strikingly revealed by a Mayo Clin- ic report of 54 autopsied patients whose pheochro- mocytomas contributed to 55% of deaths and was not suspected in 75% of cases! 1 Fortunately, pheochromocytomas can be success- fully removed in 90% of cases, and a diagnosis should be established in almost all cases with cur- rent diagnostic modalities. However, because of its many manifestations, it may mimic a large variety of conditions. This can challenge the physician’s acu- men and sometimes result in an erroneous diagnosis. No tumor or disease is capable of causing more di- versified manifestations than pheochromocytoma. 2 About 85% of pheochromocytomas occur in the adrenal medulla, whereas up to 18% have been re- ported in extra-adrenal locations, 3 e.g., the organ of Zuckerkandl (at the bifurcation of the aorta), the urinary bladder (<1%), and paraganglionic chro- maffin cells, which are found in association with sympathetic nerves in the abdomen and pelvis. Oc- casionally, tumors occur in the chest (<2%) and neck (<0.1%) and, rarely, in other locations, e.g., How to Diagnose, How to Treat Pheochromocytoma Robert A. Phillips, MD, PhD Section Editor William M. Manger, MD, PhD; 1,2 Ray W. Gifford, Jr., MD 1,3 From the National Hypertension Association; 1 Departments of Medicine, New York University Med- ical Center and Columbia University, New York, NY; 2 and the Department of Internal Medicine, Ohio State University College of Medicine and Department of Nephrology & Hypertension, Cleveland Clinic, Cleveland, OH 3 Address for correspondence/reprint requests: William M. Manger, MD, PhD, National Hyper- tension Association, 324 East 30th Street, New York, NY 10016
-
Upload
mehtaalberka83 -
Category
Documents
-
view
8 -
download
0
description
Jurnal kesehatan dalam bahasa inggris yang membahas mengenai kelainan pada kelenjar adrenal => Pheocromocytoma
Transcript of Manger Et Al-2002-The Journal of Clinical Hypertension
-
THE JOURNAL OF CLINICAL HYPERTENSION VOL. IV NO. I JANUARY/FEBRUARY 200262
Pheochromocytoma, a relatively rare (
-
the base of the skull, middle ear, and spermaticcord. Extra-adrenal pheochromocytomas (paragan-gliomas) are more frequent in children (30%) thanadults (15%).
Pheochromocytoma is a relatively rare tumor, oc-curring in fewer than 0.05% of patients with dias-tolic hypertension. About 45% of tumors cause onlyparoxysmal hypertension, and a small percentage ofpatients remain normotensive. Tumors occur at anyage, but most often in the 4th and 5th decades.
PATHOPHYSIOLOGY2Pheochromocytoma is a catecholamine-secretingtumor that can cause severe morbidity and/or lethalcomplications (e.g., cerebrovascular and/or cardio-vascular) from effects of excess circulating cate-cholamines and hypertension. Tumors usuallysecrete norepinephrine and epinephrine, but pre-dominantly norepinephrine; some secrete only nor-epinephrine or epinephrine, and very rarely dopaand dopamine are secreted. It is not known whysome pheochromocytomas secrete catecholaminesintermittently and cause paroxysmal hypertension,while others cause sustained hypertension by con-stantly secreting catecholamines. Hypovolemia oc-curs in the majority of patients, primarily thosewith sustained hypertension, and this may con-tribute to orthostatic hypotension in some patientswith this tumor.
About 10% of pheochromocytomas are malig-nant (evident from metastases or invasion of adja-cent tissues). Malignancy occurs in 30%40% ofextra-adrenal pheochromocytomas, i.e., three to15times more commonly than in adrenal tumors(2.4%11%); however, one cannot differentiate be-nign from malignant tumors by histopathology.
Many substances, mostly peptides, have beenidentified in some pheochromocytomas; these in-clude a potent vasodilator, vasoactive intestinalpeptide; adrenocorticotropic hormone; neuropep-tide Y (a potent vasoconstrictor); atrial natriureticfactor; growth hormone-releasing factor; somato-statin; parathyroid hormone-related peptides; calcitonin; serotonin; and others. Some of thesesubstances may be released into the circulation andcause physiologic and/or pharmacologic effectswith diverse manifestations and syndromes.
CLINICAL PRESENTATION2Because it secretes catecholamines, often episodical-ly, pheochromocytoma frequently presents dramati-cally and explosively with numerous and diversemanifestations that mimic many diseases. Of greatdiagnostic importance is the presence of sustainedor paroxysmal hypertension. Manifestations or at-
tacks suggesting hypercatecholaminemia withouthypertension are highly atypical. Rarely, hyperten-sion will be absent; this is most common whenpheochromocytoma is familial.
One or more symptomatic attacks occur weekly in75% of patients; attacks may occur several times dailyor only every few months. Attacks occur abruptly andsubside slowly; they last less than 1 hour in 80% ofpatients, but may last less than 1 minute or persist for1 week. They may be precipitated by palpation of thetumor, postural changes, exertion, anxiety, trauma,pain, ingestion of foods or beverages containing tyra-mine (certain cheeses, beers, and wines), use of certaindrugs (histamine, glucagon, tyramine, phenothiazine,metoclopramide, adrenocorticotropic hormone), intu-bation, induction of anesthesia, operative chemother-pay manipulation, and micturition or bladderdistention (with bladder tumors).
The symptoms and signs of pheochromocytoma(Table I) are mainly due to hypercatecholaminemiaand hypertension. Headaches occur in any part of thehead; they may be mild but are usually severe andthrobbing (especially during paroxysmal hyperten-sion) and are often accompanied by nausea and vom-iting. Generalized sweating (sometimes drenching)and palpitations with tachycardia (or reflex bradycar-dia) occur frequently. Acute anxiety with fear ofdeath is often experienced. Since most patients withhypertension have few symptoms, the occurrence ofheadaches, palpitations, and sweating in a personwith hypertension should alert the physician to con-sider the diagnosis of pheochromocytoma.
Hypermetabolism may cause considerable weightloss, but some patients, especially those with parox-ysmal hypertension, may remain obese. Severe constipation or pseudo-obstruction may occur in pa-tients with sustained hypertension because cate-cholamines inhibit peristalsis. Ischemic enterocolitiswith intestinal necrosis may complicate intensemesenteric artery vasoconstriction caused by hyper-catecholaminemia. Secretion of vasoactive intestinalpeptide, serotonin, or calcitonin by some pheochro-mocytomas may cause diarrhea. Severe Watery Diar-rhea may be accompanied by Hypokalemia andHypochlorhydria or Achlorhydria (Verner-MorrisonWDHH or WDHA syndrome).2 Marked systolicand diastolic hypertension usually accompaniesparoxysmal attacks, which occur in 45% of patients;rarely, paroxysms will convert to sustained hyperten-sion. With sustained hypertension, which occurs in50% of patients, blood pressures may fluctuatewidely, and paroxysms may result from variations incirculating catecholamines. Very rarely, hypertensionalternates with hypotension (with predominantly ep-inephrine-secreting tumors).
VOL. IV NO. I JANUARY/FEBRUARY 2002 THE JOURNAL OF CLINICAL HYPERTENSION 63
-
At least 5% of patients remain normotensive, es-pecially those with familial pheochromocytoma.Patterns of hypertension in familial disease remainconsistent (i.e., family members have either sus-tained or paroxysmal hypertension).
Orthostatic hypotension in untreated hyperten-sive patients suggests pheochromocytoma. Whenthis occurs, blood pressure usually decreases to nor-motensive levels; rarely, the blood pressure falls toshock levels and is accompanied by tachycardia.Resistance to antihypertensive therapy, paradoxicalblood pressure increases during treatment with blockers, or marked pressor responses to conditionsmentioned above that may precipitate attacksshould suggest pheochromocytoma.
Pallor and tachycardia (or reflex bradycardia) fre-quently occur, and, rarely, flushing is observed duringhypertensive paroxysms. Retinopathy is not infrequentwhen hypertension is severe and sustained, but it
rarely occurs when hypertension is paroxysmal. Occa-sionally, a fine tremor and Raynauds phenomenonare noted. Slight temperature elevation is commonand severe hyperpyrexia may rarely occur.
In children, polydipsia, polyuria, and convulsionsmay occur. Attacks of pheochromocytoma may beaggravated or may subside during pregnancy andcan be confused with eclampsia; shock may occurwith labor or after delivery and may mimic a rup-tured uterus. Tumors in the bladder may cause pain-less hematuria, and attacks may occur duringmicturition or bladder distention.
Other manifestations of hypercatecholaminemiaand/or hypertension include such complications ascongestive heart failure with or without cardiomy-opathy, myocardial infarction or arrhythmias, cere-brovascular accident, encephalopathy, shock,hemorrhagic necrosis within a pheochromocytoma,and dissecting aneurysm.
THE JOURNAL OF CLINICAL HYPERTENSION VOL. IV NO. I JANUARY/FEBRUARY 200264
Table I. Most Common Symptoms and Signs in Patients (Almost All Adults) With Pheochromocytoma AssociatedWith Paroxysmal or Persistent Hypertension
SYMPTOMS PAROXYSMAL PERSISTENTN=37 N=39
% %
Headaches (severe) 92 72Excessive sweating (generalized) 65 69Palpitations with or without tachycardia 73 51Anxiety, nervousness, fear of impending death, or panic 60 28Tremulousness 51 26Pain in chest, abdomen (usually epigastric), lumbar regions, lower abdomen, or groin 48 28Nausea with or without vomiting 43 26Weakness, fatigue, prostration 38 15Weight loss (severe) 14 15Dyspnea 11 18Warmth or heat intolerance 13 15
Noteworthy are painless hematuria, urinary frequency, nocturia, and tenesmus in pheochromocytoma of the urinary bladder.
SIGNS
Hypertension with or without wide fluctuations (rarely paroxysmal hypotension or hypertension alternating with hypotension, or hypertension absent)
Hypertension induced by physical maneuver such as exercise, postural change, or palpation and massage of flank or mass elsewhere
Orthostatic hypotension with or without postural tachycardia Paradoxical blood pressure response to certain antihypertensive drugs; marked pressor response with induction of anesthesia
SweatingTachycardia or reflex bradycardia, very forceful heartbeat, arrhythmiaPallor of face and upper part of body (rarely flushing)Anxious, frightened, troubled appearanceLeanness or underweightHypertensive retinopathy
Modified from Clinical and Experimental Pheochromocytoma.2
-
LABORATORY AND ELECTROCARDIO-GRAPHIC ABNORMALITIESLaboratory abnormalities are sometimes caused bypheochromocytoma and coexisting endocrine con-ditions, e.g., multiple endocrine neoplasia andCushings syndrome. Hyperglycemia and increasedtriglyceride concentrations may result from hyper-catecholaminemia; hyperglycemia (without diabetesmellitus) is a frequent occurrence and a clue to thepresence of pheochromocytoma. Rarely, pheochro-mocytomas (or an associated cerebellar heman-gioblastoma) secrete erythropoietin and causepolycythemia.2
Severe catecholamine-induced ischemia involv-ing multiple organs may result in lactic acidosis andelevations of pancreatic, hepatic, and cardiac en-zymes. Hypertension may be exacerbated by elevat-ed plasma concentrations of renin, angiotensin II,and aldosterone resulting from catecholamine stim-ulation of renal 1-adrenergic receptors or, rarely,from renal artery spasm or compression by apheochromocytoma or coexisting neurofibroma.2
Arrhythmias or electorcardiograph (EKG) changessuggesting myocardial ischemia, damage, or leftventricular strain may develop. Their transient ap-pearance during paroxysms suggests pheochromo-cytoma in the absence of other causes. PermanentEKG changes can result from hypertension, myocar-dial ischemia, or catecholamine cardiomyopathy.2
FAMILIAL PHEOCHROMOCYTOMAIt is important to recognize that 10%15% ofpheochromocytomas are familial; these are associ-ated with multiple endocrine neoplasms (MEN),Von Hippel-Lindau disease (VHL), carotid body tumors, or neurofibromatosis type 1. Coexis-tence of pheochromocytoma with medullary thy-roid carcinoma (MTC) or C-cell hyperplasia, andsometimes with parathyroid neoplasms or hyper-plasia, constitutes MEN type 2a. Coexistence ofpheochromocytoma with MTC, mucosal neuro-mas, thickened corneal nerves, alimentary tractganglioneuromatosis, and often a marfanoid habi-tus constitutes MEN type 2b. Hyperparathyroidismoccurs in 50% of patients with MEN type 2a butrarely in type 2b. Calcitonin, serotonin, andprostaglandin may be released from MTC andcause severe diarrhea. Patients with pheochromocy-toma should be screened for MTC or premalignantC-cell hyperplasia, which may occur many yearsbefore pheochromocytoma.2 One large study ofpheochromocytoma coexisting with the MEN 2syndrome revealed that MTC always preceded the occurrence of pheochromocytomas.4 Hypercal-citonemia suggests MTC or C-cell hyperplasia;
however, hypercalcitonemia occurs in other condi-tions and occasionally in pheochromocytoma with-out MTC. Similarly, hypercalcemia may notindicate MEN, since it may result from a parathy-roid-like hormone released from some pheochro-mocytomas. Therefore, re-evaluation for MENshould be performed after pheochromocytomaremoval.2
Von Recklinghausens neurofibromatosis, oftenwith caf au lait spots, coexists in 5% of patientswith pheochromocytoma, whereas pheochromocy-toma occurs in 1% of persons with neurofibromato-sis. Pheochromocytomas coexist in about 14% ofpatients with hemangioblastoma of the cerebellum(or other portions of the central nervous system)and retinal angioma, i.e., VHL. Therefore, patientswith pheochromocytoma should be screened for evi-dence of MTC, hyperparathyroidism, and VHL; pa-tients with the latter diseases or neurofibromatosis(if hypertension exists) should also be screened forpheochromocytoma.2,5 If familial disease is estab-lished, then first-degree relatives should be inter-viewed, examined, and investigated for geneticmutations, e.g., receptor tyrosine kinase proto-onco-gene (RET) on chromosome 10 for MEN type 2a or2b, on chromosome 3p for VHL, and on chromo-some 11q for carotid body paragangliomas.2,6Those with these genetic alterations should bescreened for presence of a pheochromocytoma withappropriate biochemical tests and imaging studies. Itis noteworthy that familial VHL may coexist notonly with pheochromocytoma but commonly withrenal and pancreatic cysts, renal carcinoma, andcystadenoma of the epididymis; very rarely, VHLmay be associated with MTC, carcinoid, pituitaryadenoma, neuroblastoma, and angiomas and cystselsewhere.7 Mutation of chromosome 17q occurs infamilial Von Recklinghausens disease.
DIFFERENTIAL DIAGNOSISTable II lists conditions that may suggest pheochro-mocytoma. Many of these conditions can be ex-cluded clinically. It is important to note that manytypes of stress can also significantly elevate concen-trations of plasma and urinary catecholamines andtheir metabolites, but few conditions increase themto levels that occur with pheochromocytoma.2
Pheochromocytoma should be considered incases of unexplained shock,8 especially if accompa-nied by abdominal pain, pulmonary edema, or in-tensive mydriasis unresponsive to light. If a patientpresents with multiple-system organ failure, highfever, encephalopathy, severe hypertension or hy-potension, and lactic acidosis (i.e., pheochromocy-toma multisystem crisis),9 pheochromocytoma
VOL. IV NO. I JANUARY/FEBRUARY 2002 THE JOURNAL OF CLINICAL HYPERTENSION 65
-
should also be considered. Rarely, hemorrhagicnecrosis in a pheochromocytoma presents as anacute abdomen or cardiovascular crisis.
Consumption of certain illegal substances (am-phetamine, cocaine, phencyclidine, lysergic acid diethylamide, and some prescription and nonpre-scription drugs containing phenylpropanolamine orephedrine) may cause manifestations mimickingpheochromocytoma. Factitious production of mani-festations (pseudo-pheochromocytoma) should beconsidered in emotionally disturbed persons withaccess to prescription or illicit drugs.2
Physicians must forever recall that pheochromo-cytoma wears many disguises. We know of twowomen who were thought to have cerebral vasculi-tis because of neurologic deficits and segmental nar-rowing of cerebral arteries on angiography.Subsequently, pheochromocytomas were found tobe responsible for these manifestations.2
Unrecognized pheochromocytoma in pregnancycarries a high risk of maternal and fetal mortality.Manifestations may first appear in pregnancy, remitafter delivery, and return in a subsequent pregnan-cy. Missing the diagnosis of pheochromocytomamay be responsible for a patients sudden death.Therefore, it is crucial that the differential diagnosisbe carefully considered. Conditions listed in TableII are discussed in detail elsewhere.2
DIAGNOSISAbout 95% of patients experience headache, sweat-ing, or palpitations, and all patients with sustainedor paroxysmal hypertension who have manifesta-tions suggesting pheochromocytoma should bescreened for the tumor. Asymptomatic patients withhypertension of unknown cause should be screenedif they have laboratory or EKG abnormalitiescaused by hyper-catecholaminemia, radiographic ormagnetic resonance imaging (MRI) evidence sug-gesting pheochromocytoma, or diseases sometimesco-existing with pheochromocytomas. Screeningshould be performed by measuring plasma freemetanephrines or catecholamines and 24-hour urinefractionated metanephrines. Urinary catecholamines,total metanephrines, and vanillylmandelic acid(VMA) measurements are less reliable.6 Blood shouldbe collected from patients in a basal state, as recom-mended for plasma catecholamine measurements.2(Currently, plasma metanephrine measurements arecommercially available only at the Mayo Clinic.)
Biochemical and Pharmacologic Tests. Plasma free(unconjugated) metanephrines and catecholamines,and urinary catecholamines and metanephrines are al-most invariably elevated with sustained or paroxysmalhypertension due to pheochromocytoma. Plasma andurinary catecholamines and urinary metanephrinesmay, however, occasionally be normal during nor-motensive periods. Therefore, it is imperative in somepatients to obtain blood during spontaneous or pro-voked hypertension or to collect urine following a hy-pertensive episode. Recent experience6 in a large,multicenter study revealed that normal concentrationsof plasma free metanephrines (metanephrine andnormetanephrine), even in the absence of hyperten-sion, virtually eliminate the presence of sporadic andfamilial pheochromocytomas, with a test sensitivity of100% and 97%, respectively. This high degree of sen-sitivity for detecting pheochromocytomas with plasmafree metanephrines has also been reported by Raber etal.10 Concentrations of plasma normetanephrine andmetanephrine greater than 2.5 pmol (458 pg)/mL and0.9 pmol (177 pg)/mL, respectively, always indicatedthe presence of a pheochromocytoma. Plasma cate-
THE JOURNAL OF CLINICAL HYPERTENSION VOL. IV NO. I JANUARY/FEBRUARY 200266
Table II. Differential Diagnosis of Pheochromocytoma2
All hypertensive patients (sustained and paroxysmal)when diagnosis is unknown
Anxiety, panic attacks, psychoneurosis, tension statesHyperthyroidismParoxysmal tachycardiaHyperdynamic -adrenergic circulatory stateMenopauseVasodilating headache (migraine and cluster headaches)Coronary insufficiency syndromeRenal parenchymal or renal arterial disease with hypertension
Focal arterial insufficiency of the brain; cerebral vasculitis
Intracranial lesions (with or without increased intracranial pressure)
Autonomic hyper-reflexiaDiencephalic seizure; Pages syndrome; dopaminesurges
Preeclampsia (or eclampsia with convulsions)Hypertensive crises associated with monoamine oxidase inhibitors
HypoglycemiaNeuroblastoma; ganglioneuroblastoma; ganglioneuroma
Acute infectious disease; acute abdomen(cardiovascular catastrophe)
Unexplained shockNeurofibromatosis (with hypertension)Rare causes of paroxysmal hypertension (adrenalmedullary hyperplasia; acute porphyria; clonidinewithdrawal; baroreflex failure; pseudopheochromo-cytoma: factitiousinduced by certain illegal, pre-scription, and nonprescription drugs); fatal familialinsomnia
Conditions in italics may increase the excretion ofcatecholamines and/or metabolites.
-
cholamines were 93% sensitive for detecting sporadicpheochromocytoma; however, sensitivity for familialtumors was only 66%. Fractionated urinarymetanephrines, measured by high-pressure liquidchromatography, was almost as sensitive as plasmafree metanephrines, whereas urinary catecholamines,total metanephrines (measured by spectrophotome-try), and VMA were progressively less sensitive, espe-cially for detection of familial disease (93%, 89%, and83%, respectively, for sporadic and 75%, 60%, and43% for familial tumors) (Dr. Graeme Eisenhofer,personal communication, 2002). When available,plasma free metanephrines and normetanephrines orfractionated urine metanephrines should be deter-mined to detect pheochromocytoma because of theirremarkable sensitivity. However, since none of thesebiochemical tests is totally specific (especially for spo-radic pheochromocytomas), repeating a combinationof these tests may help to exclude or establish the pres-ence of a tumor.
A small number of patients with essential hyper-tension or neurogenic hypertension and manifesta-tions simulating pheochromocytoma have borderlineor moderate elevations of plasma catecholamines(i.e., 6002000 pg/mL at basal conditions). Theclonidine suppression test is quite safe and excep-tionally reliable in differentiating neurogenic hyper-tension from pheochromocytic hypertension;11,12clonidine suppresses sympathetic nerve activity andplasma norepinephrine by more than 50% or to nor-mal concentrations in neurogenic hypertension, butnot in patients with pheochromocytoma. Epineph-rine changes, however, are not reliable diagnostical-ly; sometimes, significant increases in epinephrineconsistent with pheochromocytoma occur duringclonidine suppression. Beta blockers must be avoidedfor at least 48 hours before testing, since they mayprevent suppression of catecholamines and also ag-gravate clonidine-induced hypotension and brady-cardia.2 False-positive clonidine tests have beenreported in patients taking diuretics or tricyclic anti-depressants.13,14
Catecholamine assay of blood drawn from an in-dwelling catheter in patients recumbent for 1 houroften differentiates neurogenic from pheochromo-cytic hypertension; we reserve clonidine suppressiontesting for those whose catecholamines remain ele-vated despite 1-hour recumbency. Few drugs otherthan those containing catecholamines, i.e., isopro-terenol, methyldopa, levodopa, Levophed, tricyclicantidepressants, and phenoxybenzamine, may causeactual or spurious plasma catecholamine elevationsdetermined radioenzymatically; however, thesedrugs and certain other drugs (e.g., labetalol, benzo-diazepines, or acetaminophen) may interfere with
high-pressure liquid chromatographic assays of plas-ma and urinary catecholamines or their metabolites.Monoamine oxidase inhibitors can elevate urinaryand plasma metanephrines and decrease VMA lev-els. Sudden cessation of clonidine treatment may elevate plasma and urinary catecholamines and theirmetabolites, whereas metyrosine can decrease cate-cholamine production and sometimes reduce urinecatecholamines and their metabolites to normal concentrations. Radio-opaque media containingmethylglucamine can obscure elevations of totalmetanephrines. (Physicians should familiarize them-selves with drugs that may increase plasma cate-cholamines.) Finally, it must be appreciated that avariety of stressful conditions (e.g., strenuous exer-cise, myocardial infarction, congestive heart failure,hypoglycemia, hypotension, increased intracranialpressure, hypoxia, acidosis, surgery, trauma, someillicit, nonprescription and prescription drugs) maystimulate the sympathetic nervous system and in-crease catecholamine secretion.2
Only very rarely is a glucagon provocative test,combined with plasma catecholamine quantitation,required to establish the presence of a paroxysmallysecreting pheochromocytoma. This test should beperformed with precautions to counteract hyperten-sive crises, arrhythmias, or hypotension. Inductionof -adrenergic blockade prior to testing prevents ahypertensive response without influencing a diag-nostic rise in plasma catecholamines.2
Preoperative Localization. Although significant ele-vation of plasma or urinary epinephrine or itsmetabolite (metanephrine) suggests pheochromocy-toma in the adrenal, in the organ of Zuckerkandl,and rarely in other extra-adrenal sites, imagingmust establish the tumor location. Preoperative lo-calization is essential for the surgeon.
Current imaging techniques are almost alwayscapable of localizing pheochromocytomas. Conse-quently, a variety of surgical approaches can oftenbe utilized for tumor excision without abdominalexploration. Computerized tomography (CT) iden-tifies 95% of adrenal pheochromocytomas that are1 cm or greater; it can localize about 90% of extra-adrenal abdominal lesions greater than 2 cm.6 Oraland i.v. contrast is necessary for optimal interpreta-tion. CT is reliable in demonstrating chest lesions,although intrapericardial pheochromocytomas maybe missed.15
MRI is an extremely valuable modality for detect-ing pheochromocytomas and it is more sensitive andmore specific than CT. Signal intensity on MRI maybe fairly characteristic for pheochromocytoma;16only rarely will other benign or malignant lesions re-
VOL. IV NO. I JANUARY/FEBRUARY 2002 THE JOURNAL OF CLINICAL HYPERTENSION 67
-
semble a pheochromocytoma.17 MRI is noninvasiveand CT artifacts caused by surgical clips are not en-countered; it appears superior to CT in detectingextra-adrenal abdominal and pelvic lesions, andsome cardiac18 and familial adrenal pheochromocy-tomas.2 It is ideal for imaging children and pregnantpatients suspected of having a pheochromocytoma,since no radiation is involved.
The radiopharmaceutical agent 131I-meta-iodoben-zylguanidine (MIBG) concentrates in 81% 85% ofpheochromocytomas; it is highly specific for diagnosisand localization,19,20 and it may be helpful in identify-ing adrenal medullary hyperplasia and in detectingmetastases, very small tumors, or those in unusualextra-adrenal (e.g., intrapericardial) locations.2,21MIBG uptake may also occur in neuroblastomas,medullary thyroid carcinomas, carcinoids, and smallcell lung carcinomas; uptake may be inhibited by cer-tain drugs (e.g., labetalol, reserpine, calcium channelblockers, tricyclic antidepressants, sympathomimetics,cocaine, adrenergic neuron blockers, tranquilizers)and they should be discontinued 1 week beforescintigraphy.2,22
123I-MIBG offers superior image quality and ap-pears especially useful for detecting recurrent andmetastatic tumors and those in unusual locations,2,6but is not generally available in the United States.Bone scanning with technetium (Tc) 99m maydemonstrate metastatic lesions missed by MIGB.Liver metastases are best detected with MRI or CT(metastases frequently involve lymph nodes, liver,lung, and bone, but not brain).
111Indium octreotide is another radiopharmaceu-tical agent taken up by some pheochromocytomas,but it detects only 25% of benign tumors; however,it may occasionally localize metastatic lesions thatare missed by 123I-MIBG.23
Imaging studies are usually indicated only afterbiochemical determinations have established thepresence of a pheochromocytoma; occasionally,however, in some subjects suspected of having fa-milial pheochromocytoma it is justifiable to per-form imaging studies even without biochemicalevidence of the tumor, since some familial tumorsmay be identified before they secrete significantamounts of catecholamines.
Although CT and MRI are both highly accuratefor localizing pheochromocytomas, we prefer initi-ating studies with MRI of the abdomen and pelvis,since a bright signal imparted by T2-weighted images strongly suggests pheochromocytoma; fur-thermore, small extra-adrenal tumors are more eas-ily identified by MRI than CT. If a tumor isidentified, the high specificity of MIBG uptake bypheochromocytomas can help confirm the diagno-
sis. If MRI and CT fail to identify a tumor in theabdomen or pelvis, we recommend MRI of thechest and neck and a whole-body MIBG scan.
Incidentally recognized adrenal masses (inciden-talomas) are encountered in 3%4% of patients examined by CT; an MRI and MIBG can be especially useful in determining whether an inciden-taloma is a pheochromocytoma. However, mea-surement of plasma and urinary catecholaminesand their metabolites is essential to establish the di-agnosis. A large survey24 revealed that 4.2% of in-cidentalomas were pheochromocytomas, but only43% of these patients were hypertensive, despiteurinary catecholamine elevations in 86%.
If efforts to locate a pheochromocytoma fail, sam-pling blood for catecholamine and free metanephrineand normetanephrine assay from various sites in thevena cava, with fluoroscopic guidance, may localizepheochromocytomas in abdominal, pelvic, intratho-racic, or cervical areas. Adrenal vein catheterizationmay stimulate catecholamine secretion from normalglands and is less reliable for tumor localization.Also, paroxysmal or variable tumor secretion of cate-cholamines during vena caval blood sampling mayprevent accurate tumor localization.2
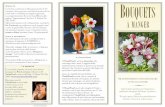
When pheochromocytoma is suspected, the algo-rithm in Table III can be followed.
TREATMENTPheochromocytoma requires a physician, surgeon,and anesthetist who are experienced in its manage-ment. If not contraindicated, surgical removal, theonly curative procedure, should be performed expe-ditiously.
MTC, C-cell hyperplasia, hyperparathyroidism,and VHL should be considered in all patients withpheochromocytoma and in their relatives. Diagno-sis and treatment of these conditions should be de-layed until after pheochromocytoma removal.
Malignant hypertension, acute cardiovascular orabdominal complications (e.g., hemorrhagic necrosisin a pheochromocytoma), or acceleration in frequen-cy and severity of hypertensive crises may necessitateimmediate medical or surgical therapy, or both.
If the patient has very severe hypertension, arapid i.v. bolus of phentolamine (5 mg) is usuallyeffective in reducing pressure; if there is no re-sponse, the dose can be repeated every 2 minutesuntil blood pressure is adequately reduced. The ef-fect of phentolamine is brief; therefore, repeated hy-pertensive crises are best controlled by infusingsodium nitroprusside, nitroglycerine, or phento-lamine2,25 at a rate that normalizes blood pressure.Nitroprusside can cause thiocyanate toxicity if theinfusion is prolonged or if renal insufficiency exists.
THE JOURNAL OF CLINICAL HYPERTENSION VOL. IV NO. I JANUARY/FEBRUARY 200268
-
VOL. IV NO. I JANUARY/FEBRUARY 2002 THE JOURNAL OF CLINICAL HYPERTENSION 69
Figure. MRI=magnetic resonance imaging; CT=computed tomography; MIBG=131I-metaiodobenzylguanidineAdapted with permission from Manger WM, Gifford RW Jr. Pheochromocytoma. In: Laragh JH, Brenner BM, LaplanNM, eds. Endocrine Mechanisms in Hypertension. New York, NY: Raven Press; 1989:16391659.
-
THE JOURNAL OF CLINICAL HYPERTENSION VOL. IV NO. I JANUARY/FEBRUARY 200270
If immediate surgery is necessary, hypovolemiais corrected by infusion of appropriate fluid and/orblood within 18 hours preoperatively to minimizepostoperative hypotension.
Abdominal palpation and stressful proceduresshould be performed cautiously with drugs avail-able to combat hypertensive crises, hypotension, orarrhythmias. Morphine and phenothiazines shouldbe avoided, since they may precipitate hypertensivecrises or hypotension and shock.
Adrenergic Blockade. Preoperative 1 and 2 block-ade with phenoxybenzamine (1030 mg twice daily)or 1 blockade with prazosin (starting with 1 mgand increasing to 1 or 2 mg two or three times daily)for 1 week or more and continued until surgery usu-ally prevents severe preoperative clinical manifesta-tions, reverses hypovolemia, and promotes smoothanesthetic induction and relatively stable blood pres-sure during surgery. Other 1-adrenergic antagonists(e.g., terazosin or doxazosin) and calcium channelblockers (e.g., nifedipine, nicardipine, diltiazem, ver-apamil) have effectively controlled pheochromocytichypertension. Metyrosine (which blocks synthesis ofcatecholamines) alone or in combination with adren-ergic or calcium antagonists may also be helpful inthe preoperative control of blood pressure.2,26 Com-plete blockade (with orthostatic hypotension) is con-traindicated, since it prevents blood pressureelevations during intra- abdominal palpation (whichcan aid the surgeon in identifying some tumors diffi-cult to locate) or prevents recognition of additionaltumors (ordinarily indicated by persistence of hyper-tension after tumor removal).
Preoperative 1 blockade (e.g., long-acting meto-prolol 50150 mg once daily or other cardioselec-tive blockers), if not contraindicated, is used toprevent or treat supraventricular arrhythmias andtachycardia, or if angina occurs. For rapid controlof ventricular tachycardia due to atrial fibrillationor flutter, i.v. esmolol (a short-acting, cardioselec-tive 1 blocker) may be effective. Ventricular ar-rhythmias are treated with lidocaine (50100 mgi.v. bolus). Beta blockers should never be givenwithout first creating blockade, since blockadealone can cause marked hypertension. This is par-ticularly apt to occur with nonselective blockers(e.g., propranolol or nadolol), since they inhibit anyvasodilating effect of epinephrine by blocking 2receptors and thus enhance vasoconstriction. A relatively cardioselective 1 blocker (e.g., metopro-lol, bisoprolol, or atenolol) is more appropriate,since it has less vascular effect.
Combined - and 1-adrenergic blockade andmetyrosine may be effective in combating severe
constipation and the rare complication of intesti-nal pseudo-obstruction that results from impairedintestinal motility due to excess catecholamines.27Labetalol (an and blocker) may effectivelycontrol hypertension and other manifestations ofpheochromocytomas; however, we do not use it,since it sometimes causes hypertension.2
Preoperative, Operative, and Postoperative Man-agement. Preoperatively, diazepam, secobarbital, ormeperidine should be given to allay anxiety, whichmay trigger release of tumor catecholamines. Fen-tanyl and droperidol are avoided, since they mayalso trigger release of catecholamines. Atropine isavoided, since it may enhance tachycardia causedby hypercatecholaminemia. A muscle relaxantshould be administered before endotracheal intuba-tion to minimize a hypertensive response, and arter-ial pressure, EKG, and arterial blood gases shouldbe monitored. Isoflurane is the most popular anes-thetic, although enflurane is also suitable forpheochromocytoma removal.2
During intubation and surgery, prompt treat-ment of hypertensive crises with i.v. nitroprusside,phentolamine, or nitroglycerine and control of ar-rhythmias with i.v. esmolol and/or lidocaine iscrucial. Generous intraoperative volume replace-ment of significant blood loss is essential to pre-vent postoperative hypotension.2
Prior to 1996, there was general agreement thatan anterior transperitoneal incision was mandatoryto remove intra-abdominal pheochromocytomas,since tumors may be multiple and extra-adrenal.However, with the remarkable improvement ofimaging techniques and with increasing experiencewith laparoscopic removal of adrenal and someextra-adrenal pheochromocytomas, open surgicalexploration is now indicated only when tumors aremultiple, large, or particularly difficult to removelaparoscopically. The adrenal vein is usually easierto locate in pheochromocytomas that are relativelysmall, and prompt vein ligation can prevent hyper-tensive episodes during laparoscopic removal.28,29
Some recommend that only adrenal pheochromo-cytomas less than 5 cm in diameter should be removedlaparoscopically.29 At the Mayo Clinic, Dr. John vanHeerden (personal communication, 2002) believes la-paroscopic removal of a pheochromocytoma shouldbe limited to a diameter of 4 cm, since they are usuallyeasy to remove without tumor fracture, which couldleave tumor cells in the peritoneal cavity. Laparoscop-ic tumor removal causes less postoperative pain, ashorter hospitalization, and a better cosmetic result.
Neumann et al.30 reported successful preserva-tion of adrenocortical function after laparoscopic
-
VOL. IV NO. I JANUARY/FEBRUARY 2002 THE JOURNAL OF CLINICAL HYPERTENSION 71
bilateral adrenal-sparing surgery for hereditarypheochromocytoma. This avoids lifelong steroidreplacement, which is required when bilateraladrenalectomy is indicated in MEN syndromes.Patients with hypercalcitonemia and/or hypercal-cemia should be re-evaluated after pheochromocy-toma removal, since return of these elevations tonormal eliminates MEN as the cause of these bio-chemical abnormalities.
Pheochromocytomas of the chest, neck, and uri-nary bladder require special surgical procedures;otherwise, management is similar to that of abdom-inal tumors. Pheochromocytomas discovered dur-ing pregnancy should be removed, but if pregnancyis carried to term, a cesarian section is advisable toavoid the stress of labor and vaginal delivery.
Close postoperative observation is mandatory.Hypovolemia and hemorrhage at operative sitescan cause hypotension requiring volume replace-ment. Hypertension may result from fluid overload,pain, urinary retention, hypoxia, hypercarbia, orresidual pheochromocytoma. Inadvertent renalartery ligation may cause hyper-reninemia, but hy-pertension would probably not occur for severaldays or weeks postoperatively.2
Severe, transient hypoglycemia with centralnervous system manifestations and coma mayoccur within 2 hours following operation. Hypo-glycemia results from increased insulin secretion,which blockers may augment by reducing inhi-bition of catecholamines on insulin secretion. Betablockers can impair recovery from hypoglycemiaby reducing gluconeogenesis and glycogenolysis,and can mask hypoglycemic signs by preventingtachycardia and tremor; sweating may also be impaired.31 Blood glucose should be repeatedlyanalyzed for several hours postoperatively and hypoglycemia treated promptly. Initiating an infu-sion of 5% dextrose in water immediately follow-ing tumor removal and continuing it for severalhours will prevent hypoglycemia.
About 25% of patients remain hypertensive fol-lowing tumor removal. This is possibly due to coex-isting essential hypertension. Five-year survival forpatients with benign pheochromocytoma is 95%,but varies from 36%50% with malignant tumors.In medical centers with extensive experience in treat-ing pheochromocytomas, operative mortality hasbeen low (0%3.3%).2 Expertise is essential!
Long-Term Medical Management. If a malignantpheochromocytoma cannot be totally removed, asmuch as possible should be resected to minimizefunctioning tumor tissue. Radiation therapy ofmetastases in bone may be effective. Irradiation with
radioactive MIBG may temporarily reduce the sizeand catecholamine secretion in about 25% of tu-mors, but inevitably all patients relapse within 2years; this therapy is rarely used in the UnitedStates.2
When patients with metastatic disease becomesymptomatic and tumors appear especially aggres-sive, combination i.v. chemotherapy with cy-clophosphamide, vincristine, and dacarbazine isindicated, since it will reduce tumor mass, cate-cholamine excretion, and symptomatology in 50%of patients.32 Antihypertensive medication shouldbe increased before treatment, and one should beprepared to treat hypertensive crises, sincechemotherapy will damage tumor cells, resultingin the release of catecholamines.2
Alpha and blockers may control symptomatologyand blood pressure for many years in patients withmetastatic tumors. Beta blockers may also prevent cat-echolamine cardiomyopathy. Metyrosine can marked-ly inhibit catecholamine synthesis and reducesymptomatology, and it may be helpful in the treat-ment of catecholamine cardiomyopathy. As malignantmetastases continue to grow, larger doses of metyro-sine are usually required to minimize hypercate-cholaminemia and delay its detrimental effects;however, large doses may cause undesirable side ef-fects, e.g., crystalluria and renal damage, psychic dis-turbance, and occasionally a Parkinson-like syndrome.
An occasional patient with metastatic pheochromo-cytoma will develop a hypersecretory disorder with se-vere diarrhea that may respond to i.v. somatostatin.
Finally, it is noteworthy that some beneficial resultsin treating metastatic pheochromocytomas in the liverwith radiofrequency ablation have been observed inseveral patients treated at the Mayo Clinic (Dr.William F. Young, personal communication, 2002). Aprobe, which is passed percutaneously into an hepaticmetastatic lesion, delivers sufficient heat to destroy themetastasis and replace it with an empty cyst.
CONCLUSIONPheochromocytoma is a rare and treacheroustumor, since, if not recognized and treated appro-priately, it is invariably fatal. Physicians must beespecially alert to recognize and diagnosticallyevaluate all patients with sustained or paroxysmalhypertension associated with headaches, sweating,or palpitations. Biochemical and imaging studiescan almost always confirm or refute the diagnosisof this catecholamine-secreting tumor. Surgical re-moval is usually curative. Pheochromocytomasthat are malignant may often be treated for pro-longed periods with antihypertensive drugs andchemotherapy.
-
THE JOURNAL OF CLINICAL HYPERTENSION VOL. IV NO. I JANUARY/FEBRUARY 200272
Acknowledgment: This report was supported by the NationalHypertension Association. We wish to thank Alla Krayko andRuth Johnston for their expert secretarial assistance.
REFERENCES1 Sutton M, Sheps SG, Lie JL. Prevalence of clinically unsus-
pected pheochromocytoma;review of a 50-year autopsy se-ries. Mayo Clin Proc. 1981;56:354360.
2 Manger WM, Gifford RW Jr. Clinical and experimentalpheochromocytoma. Cambridge, MA: Blackwell Science; 1996.
3 Whalen RK, Althausen AF, Daniels GH. Extra-adrenalpheochromocytoma. J Urol. 1992;147:110.
4 Nguyen L, Niccoli-Sire P, Caron P, et al., and the FrenchCalcitonin Tumors Study Group (GETC). Pheochromocy-toma in multiple endocrine neoplasia type 2: a prospectivestudy. Eur J Endocrinol. 2001;144:3744.
5 Neumann HPH, Berger DP, Sigmund G, et al. Pheochromocy-tomas, multiple endocrine neoplasia type 2 and Von Hippel-Lindau disease. N Engl J Med. 1993;329:15311538.
6 Pacak K, Linehan WM, Eisenhofer G, et al. Recent advances ingenetics, diagnosis, localization, and treatment of pheochromo-cytoma. Ann Intern Med. 2001;134:315329.
7 Neuman HPH, Dinkel E, Brambs H, et al. Pancreatic le-sions in the Von Hippel-Lindau syndrome. Gastroenterol-ogy. 1991;101:465471.
8 Bergland BE. Pheochromocytoma presenting as shock. AmJ Emerg Med. 1989;7:4448.
9 Newell KA, Prinz RA, Pickleman J, et al. Pheochromocy-toma multisystem crisis: a surgical emergency. Arch Surg.1988;123:956959.
10 Raber W, Raffesberg W, Bischof M, et al. Diagnostic efficacyof unconjugated plasma metanephrines for detection ofpheochromocytoma. Arch Intern Med. 2000;160:29572963.
11 Bravo EL, Tarazi RC, Fouad FM, et al. Clonidine suppres-sion test: a useful aid in the diagnosis of pheochromocy-toma. N Engl J Med. 1981;305:623626.
12 Karlberg BE, Hedman L. Value of clonidine suppressiontest in the diagnosis of pheochromocytoma. Acta MedScand. 1986;714 (suppl):1521.
13 Sjoberg RJ, Simcic KJ, Kidd GS. The clonidine suppressiontest for pheochromocytoma. A review of its utility and pit-falls. Arch Intern Med. 1992;152:11931197.
14 Hui TP, Krakoff LR, Felton K, et al. Diuretic treatment al-ters clonidine suppression of plasma norepinephrine. Hy-pertension. 1986;8:272276.
15 Jebara VA, Uva MS, Farge A, et al. Cardiac pheochromo-cytomas. Ann Thorac Surg. 1992;53:356361.
16 Fink IJ, Reinig JW, Dwyer AJ, et al. MR imaging of pheochro-mocytomas. J Comput Assist Tomogr. 1985;9:454458.
17 Baker EM, Spritzer C, Blinder R, et al. Benign adrenal le-
sions mimicking malignancy on MR imaging: report oftwo cases. Radiology. 1987;163:669671.
18 Stowers SA, Gilmore P, Stirling M, et al. Cardiacpheochromocytoma involving the left main coronaryartery presenting with exertional angina. Am Heart J.1987;114:423427.
19 Sisson JC, Frager MS, Valk TW, et al. Scintigraphic localiza-tion of pheochromocytoma. N Engl J Med. 1981;305:1217.
20 Jalil ND, Pattou FN, Combemale F, et al. Effectivenessand limits of preoperative imaging studies for the localiza-tion of pheochromocytomas and paragangliomas: a reviewof 282 cases. Eur J Surg. 1998;164:2328.
21 Saad MF, Frazier OH, Hickey RC, et al. Intrapericardialpheochromocytoma. Am J Med. 1983;75:371376.
22 Khafagi FA, Shapiro B, Fig LM, et al. Labetalol reducesiodine-131 MIBG uptake by pheochromocytoma and nor-mal tissue. J Nucl Med. 1989;30:481489.
23 van der Harst E, de Herder WW, Bruining HA, et al.[123I] Metaiodobenzylguanidine and [111In] octreotideuptake in benign and malignant pheochromocytomas. JClin Endocrinol Metab. 2001;86:685693.
24 Mantero F, Massimo T, Arnoldi G, et al. A survey onadrenal incidentaloma in Italy. J Clin Endocrinol Metab.2000;85:637644.
25 Boutros AR, Bravo EL, Zanettin G, et al. Perioperativemanagement of 63 patients with pheochromocytoma.Cleve Clinic J Med. 1990;57:613617.
26 Bravo EL. Pheochromocytoma. In: Bardin CW, ed. Cur-rent Therapy in Endocrinology and Metabolism. 6th ed.St. Louis, MO: Mosby; 1997:195197.
27 Mullen JP, Cartwright RC, Tisherman SE, et al. Case re-port: pathogenesis and pharmacologic management ofpseudo-obstruction of the bowel in pheochromocytoma.Am J Med Sci. 1985;290:155158.
28 Janetschek G, Finkenstedt G, Gasser R, et al. Laparoscopicsurgery for pheochromocytoma: adrenalectomy, partial resec-tion, excision of paragangliomas. J Urol. 1998;160: 330334.
29 Salomon L, Rabii R, Soulie M, et al. Experience withretroperitoneal laparoscopic adrenalectomy for pheochro-mocytoma. J Urol. 2001;165:18711874.
30 Neumann HPH, Reincke M, Bender BU, et al. Preservedadrenocortical function after laparoscopic bilateral adrenalsparing surgery for hereditary pheochromocytoma. J ClinEndocrinol Metab. 1999;84:26082610.
31 Meeke RI, O'Keeffe JD, Gaffney JD. Phaeochromocytomaremoval and postoperative hypoglycemia. Anaesthesia.1985;40:10931096.
32 Averbush SD, Steakley CS, Young RC, et al. Malignantpheochromocytoma: effective treatment with a combina-tion of cyclophosphamide, vincristine, and dacarbazine.Ann Intern Med. 1988;109:267273.