Managing Pain With Therapeutic Modalities - Kiky
31
MANAGING PAIN WITH THERAPEUTIC MODALITY Rezki Amalia Nurshal Pembimbing : Prof. DR. dr. Angela BM Tulaar, Sp.KFR-K
-
Upload
rezki-amalia-nurshal -
Category
Documents
-
view
20 -
download
2
Transcript of Managing Pain With Therapeutic Modalities - Kiky
MANAGING PAIN WITH THERAPEUTIC MODALITY
Rezki Amalia Nurshal
Pembimbing : Prof. DR. dr. Angela BM Tulaar, Sp.KFR-K

1. PAIN
2. THERAPEUTICAL MODALITIES
3. PAIN MANAGEMENT
OVERVIEW

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
PAIN
• Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage (International Association for the Study of Pain)
• The most chief complain• Subjective sensation
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
PAIN
Warning ProtectionCan persist after its no
longer useful
Enhancing disability
Inhibiting efforts to
rehabilitate
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
PAIN
Acute : tissue damage and after injury.
Chronic : lasting for
more than 6 months.
Persistent : Pain that
defies intervention
from conditions
where continuing (persistent)
pain is a symptom of a
treatable condition
Referred : pain that is
perceived to be in an area that seems to
have little relation to the existing pathology
Radiating pain : irritation of nerve root can cause radiating
pain.
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
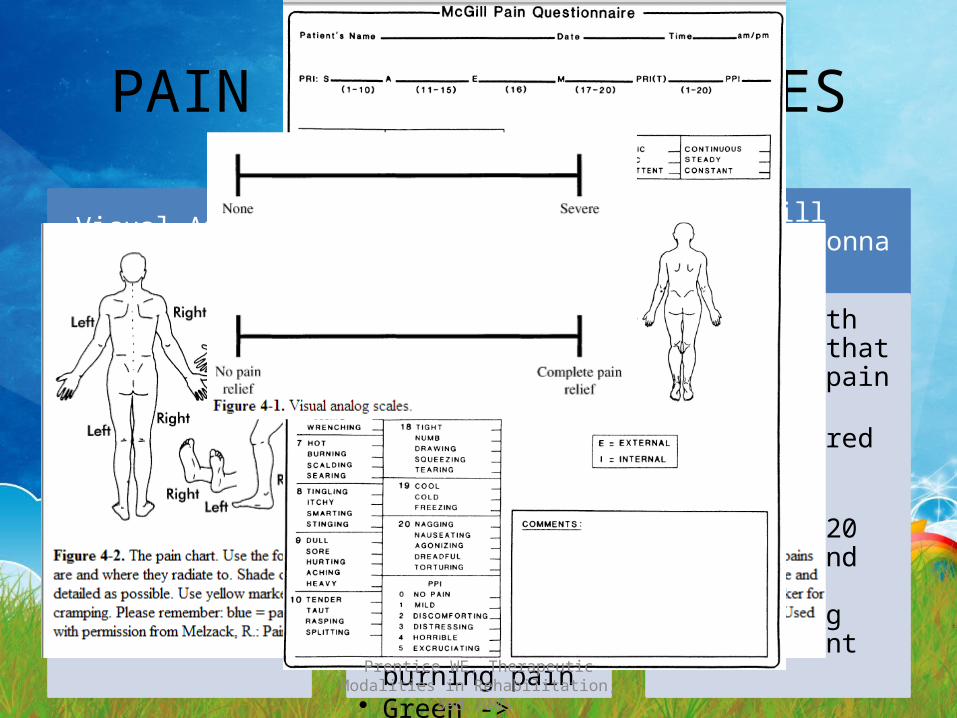
PAIN ASSESMENT SCALES
Visual Analog Scales
• Using a line : 1 - 10• 1 -> NO PAIN• 10 -> SEVERE PAIN
Pain Charts
• To asses the location of pain and a number of subjective components.
• Blue -> aching pain• Yellow ->
numbness or tingling
• Red -> burning pain• Green -> cramping
pain
McGill PainQuestionnaire
• A tool with 78 words that describe pain
• Commonly administered to LBP patients.
• May take 20 minutes and often frustating the patient
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
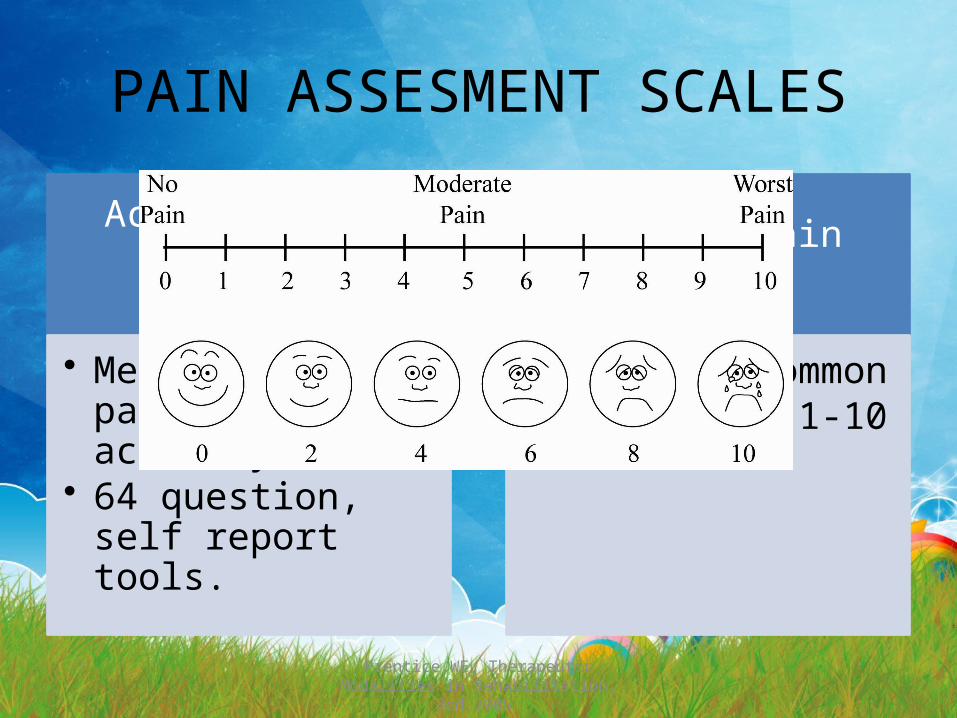
PAIN ASSESMENT SCALES
Activity Pain Indicators Profile
• Measures patient activity.
• 64 question, self report tools.
Numeric Pain Scales
• The most common• Pain scale 1-10

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
PAIN PERCEPTION
Sharp (tajam)
Dull (tumpul)
Aching (nyeri)
Throbbing (berdenyut)
Burning (terbakar)
Piercing (menusuk)
subjective
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
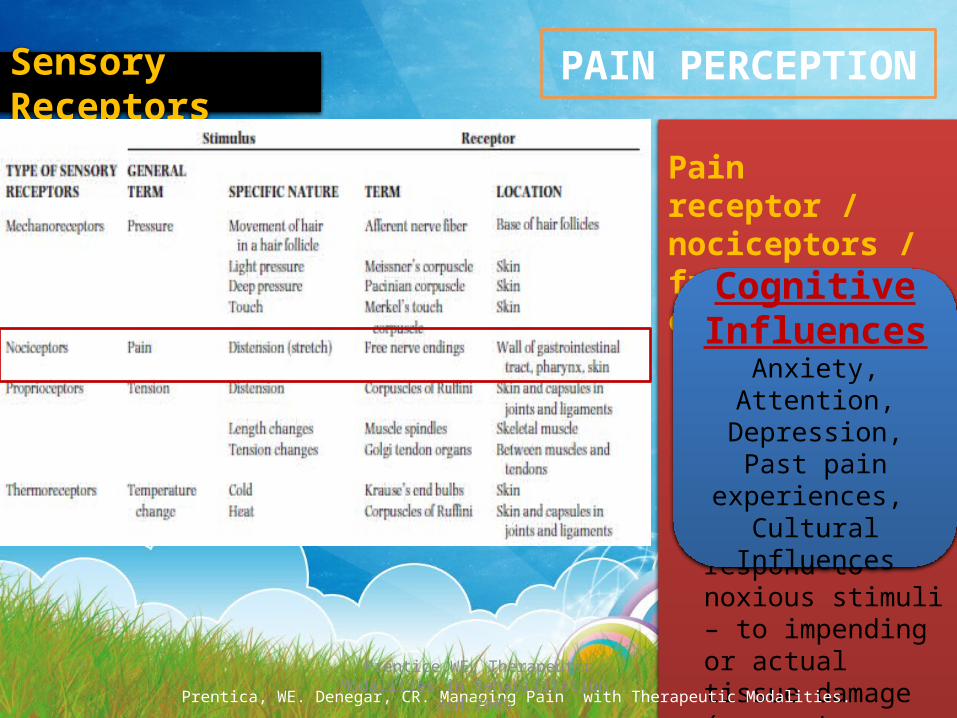
PAIN PERCEPTION
Pain receptor / nociceptors / free nerve endings
noxious stimuli = extreme mechanical, thermal, chemical energy respond to noxious stimuli – to impending or actual tissue damage (e.g cuts, burns, sprains, etc)-> superficial heat, cold, analgesic balms, massage
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
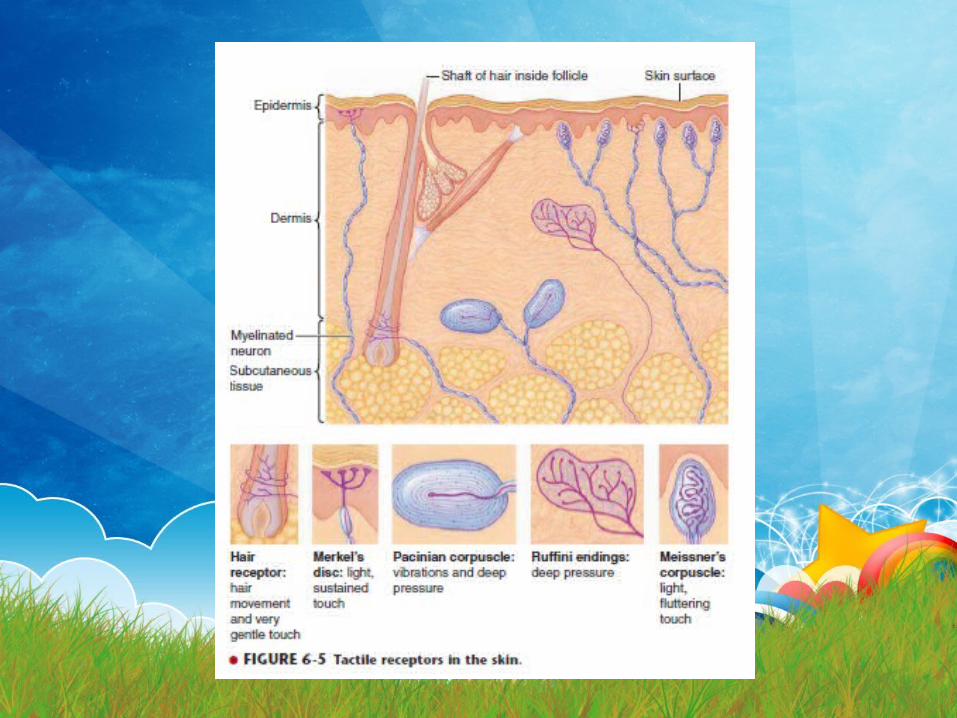
Sensory Receptors
Cognitive Influences
Anxiety, Attention, Depression, Past pain
experiences, Cultural Influences
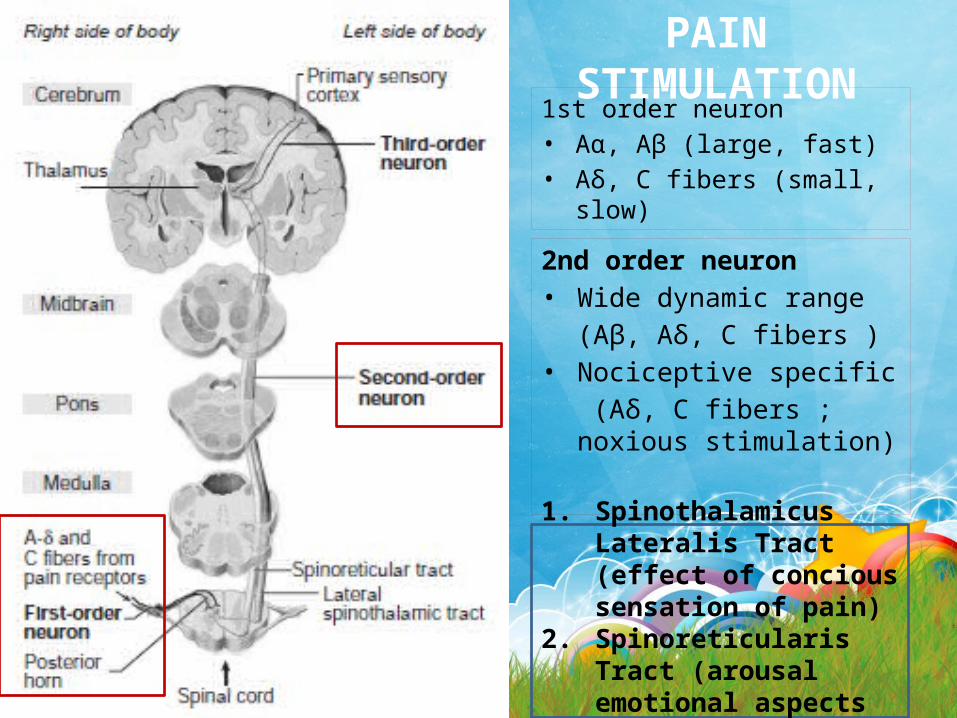
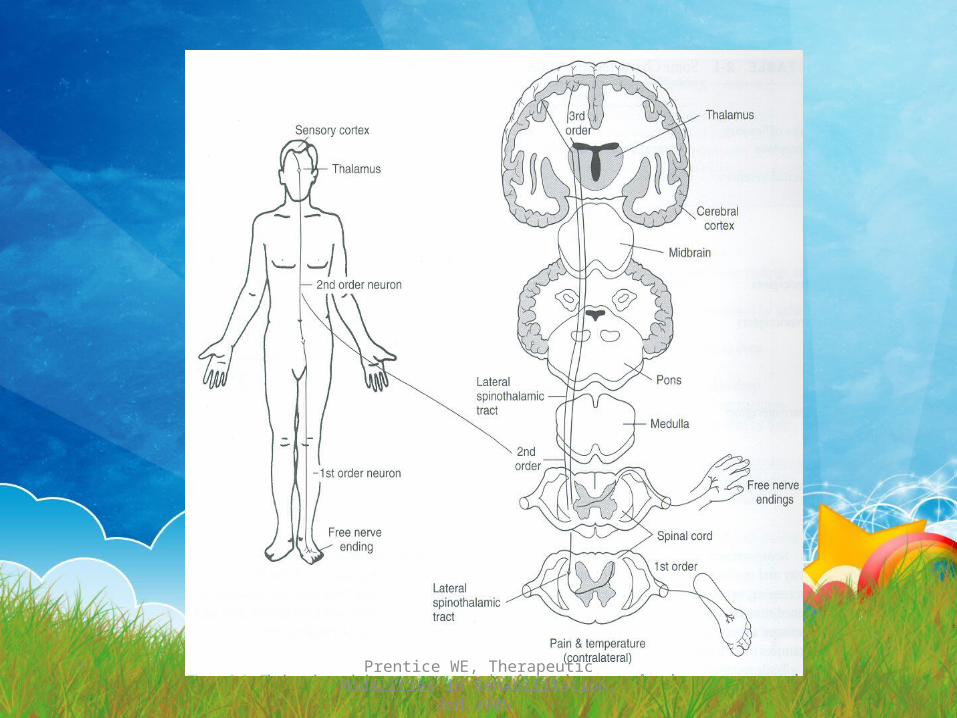
PAIN STIMULATION1st order neuron• Aα, Aβ (large, fast)• Aδ, C fibers (small, slow)
2nd order neuron• Wide dynamic range
(Aβ, Aδ, C fibers )• Nociceptive specific
(Aδ, C fibers ; noxious stimulation)
1. Spinothalamicus Lateralis Tract (effect of concious sensation of pain)
2. Spinoreticularis Tract (arousal emotional aspects of pain)
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
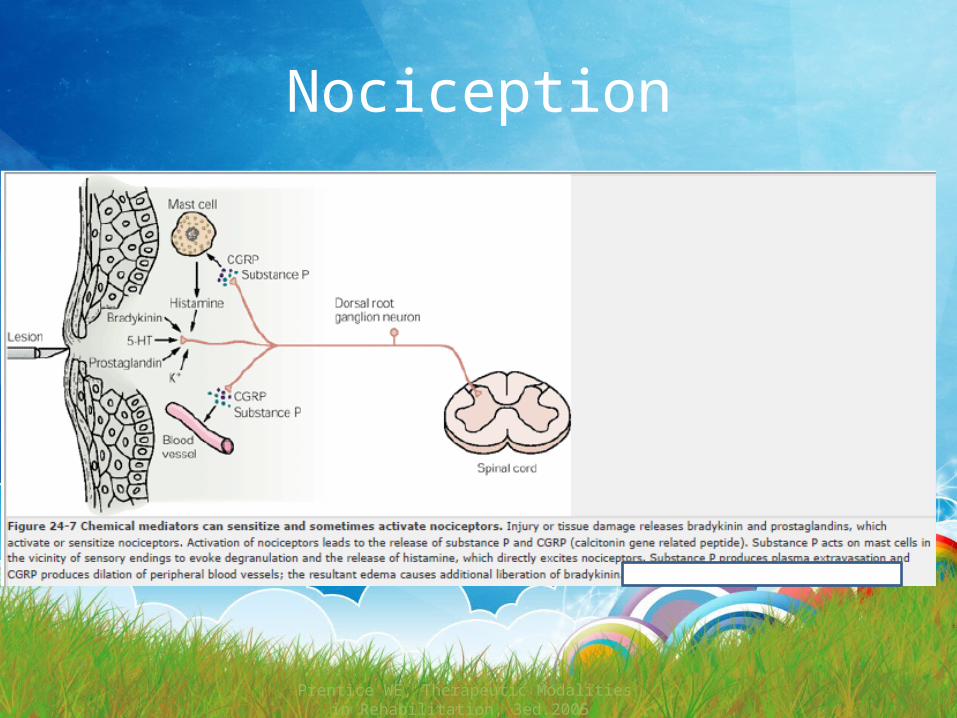
Nociception
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
SYNAPTIC TRANSMISSION
• Neuroactive peptides can facilitate or inhibit synaptic activity ◦ Enkephalin ◦ Serotonin ◦ Norepinephrine ◦ β-endorphine ◦ Dynorphin

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
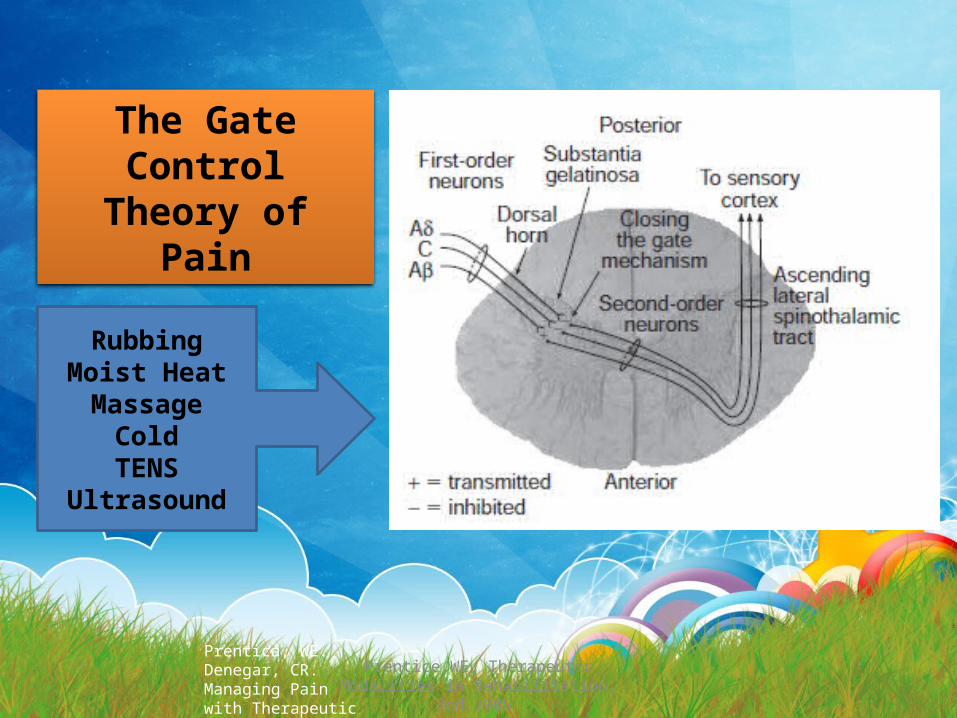
PAIN CONTROL(Melzack, Wall and Castle)
The Gate Control Theory of Pain
Descending Pain Control
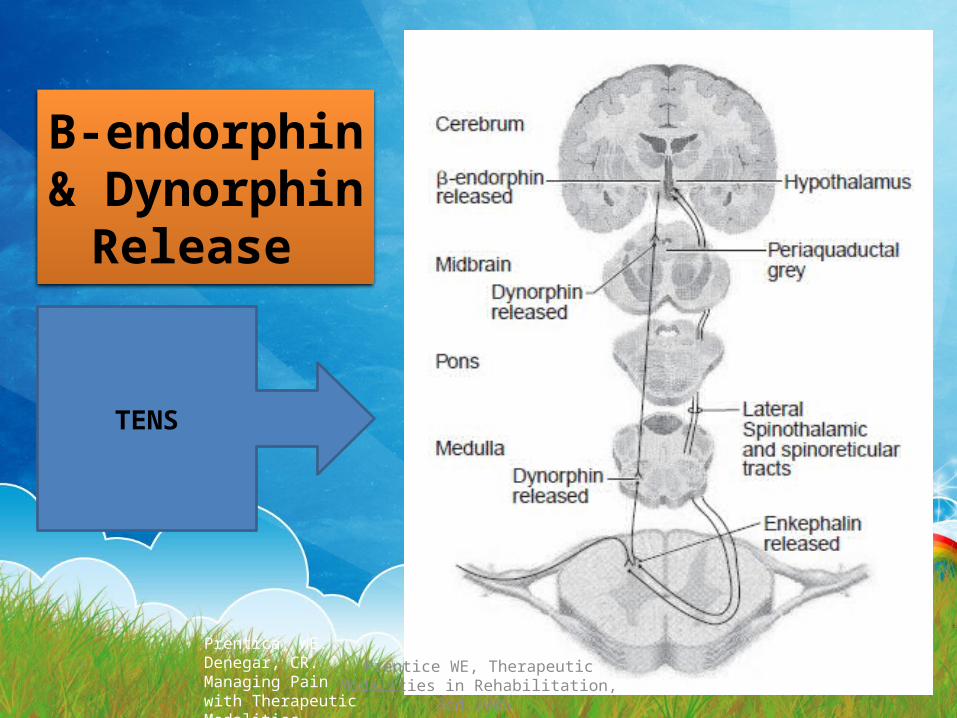
Β-endorphin & Dynorphin
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
The Gate Control
Theory of Pain
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
RubbingMoist Heat
MassageColdTENS
Ultrasound
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
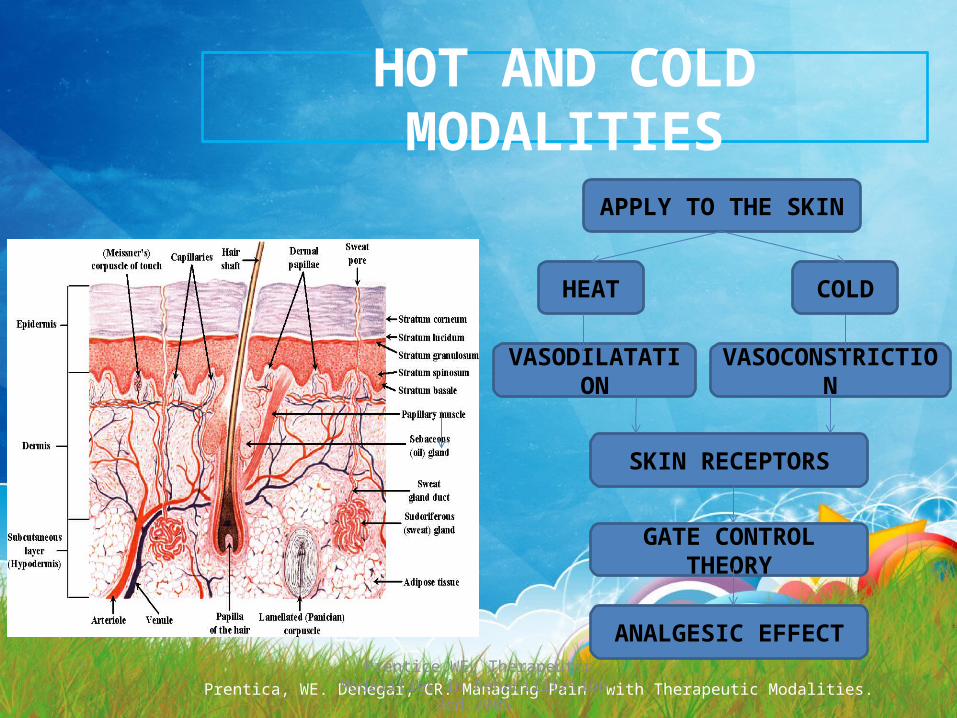
HOT AND COLD MODALITIES
HEAT COLD
APPLY TO THE SKIN
VASODILATATION VASOCONSTRICTION
GATE CONTROL THEORY
ANALGESIC EFFECT
SKIN RECEPTORS
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
Descending Pain Control
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
TENS
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
Β-endorphin & Dynorphin
Release
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
TENS
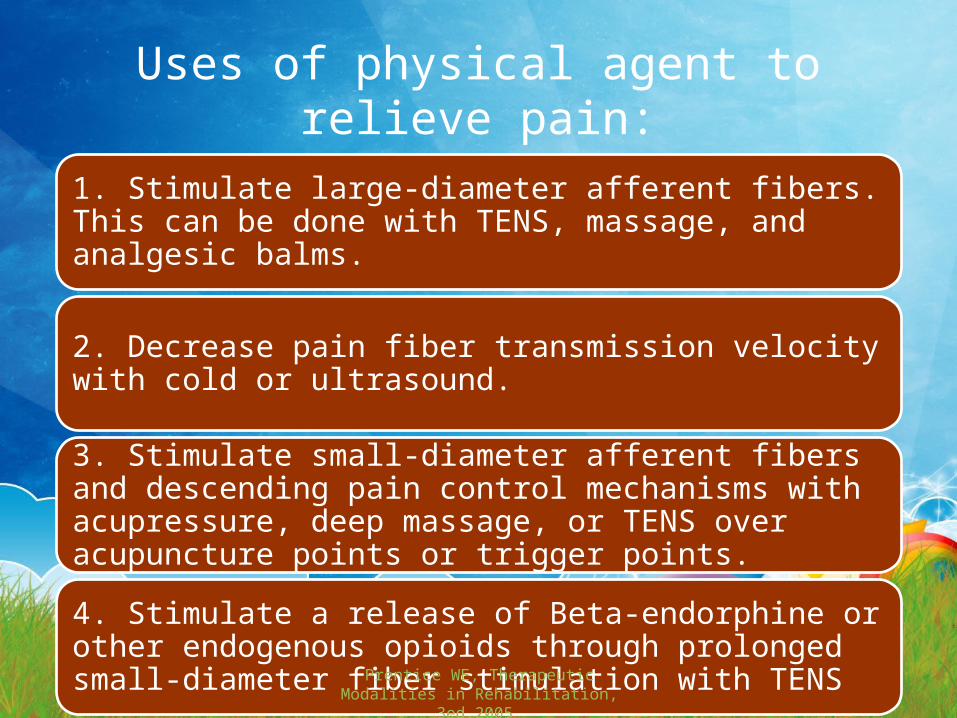
Uses of physical agent to relieve pain:
1. Stimulate large-diameter afferent fibers. This can be done with TENS, massage, and analgesic balms.
2. Decrease pain fiber transmission velocity with cold or ultrasound.
3. Stimulate small-diameter afferent fibers and descending pain control mechanisms with acupressure, deep massage, or TENS over acupuncture points or trigger points.
4. Stimulate a release of Beta-endorphine or other endogenous opioids through prolonged small-diameter fiber stimulation with TENS Prentice WE, Therapeutic Modalities in
Rehabilitation, 3ed.2005
Other pain control strategy1.Encourage central biasing through cognitive processes, such as motivation, tension diversion, focusing, relaxation techniques, positive thinking, thought stopping, and self-control.
2. Minimize the tissue damage through the application of proper first aid and immobilization.
3. Maintain a line of communication with the patient. Let the patient know what to expect following an injury.
4. Recognize that all pain, even psychosomatic pain, is very real to the patient.
5. Encourage supervised exercise to encourage blood flow, promote nutrition, increase metabolic activity, and reduce stiffness and guarding if the activity will not cause further harm to the patient.Prentice WE, Therapeutic Modalities in
Rehabilitation, 3ed.2005

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
PAIN MANAGEMENT
CHOOSING THERAPEUTICAL MODALITIES :
1. ACUTE PAINa. Cold Therapeutical Modalitiesb. TENS
2. SUBACUTE AND CHRONIC PAINa. Hot Therapeutical Modalitiesb. MWD, SWDc. Laserd. Ultrasound
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
CRYOTHERAPYINDICATIONS• Acute pain• Acute swelling (controlling
hemorrhage and edema)• Myofascial trigger points• Muscle guarding• Muscle spasm• Acute muscle strain• Acute ligament sprain• Acute contusion• Bursitis, Tenosynovitis, Tendinitis• Delayed onset muscle soreness
CONTRAINDICATIONS
• Impaired circulation (i.e., Raynaud’s phenomenon)
• Peripheral vascular disease• Hypersensitivity to cold• Skin anesthesia• Open wounds or skin conditions (cold
whirlpools and• contrast baths)• Infection
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
THERMOTHERAPYIndications
• Subacute and chronic inflammatory conditions and pain
• Decreased ROM• Resolution of swelling• Myofascial trigger points• Muscle guarding• Muscle spasm• Subacute muscle strain• Subacute ligament sprain• Subacute contusion• Infectio
Contraindications
• Acute musculoskeletal conditions• Impaired circulation• Peripheral vascular disease• Skin anesthesia• Open wounds or skin conditions (cold
whirlpools• and contrast baths
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
UltrasoundINDICATIONS• Soft tissue healing and repair• Scar tissue• Joint contracture• Chronic inflammation• Increase extensibility of collagen• Reduction of muscle spasm• Pain modulation• Increase blood flow• Soft tissue repair• Bone healing• Repair of nonunion fractures• Inflammation associated with myositis
ossificans• Myofascial trigger points
CONTRAINDICATIONS• Acute conditions• Areas of decreased temperature sensation• Areas of decreased circulation• Vascular insufficiency• Thrombophlebitis• Eyes• Reproductive organs• Pelvis immediately following menses• Pregnancy• Pacemaker• Malignancy• Epiphyseal areas in young children• Total joint replacements• Infection
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
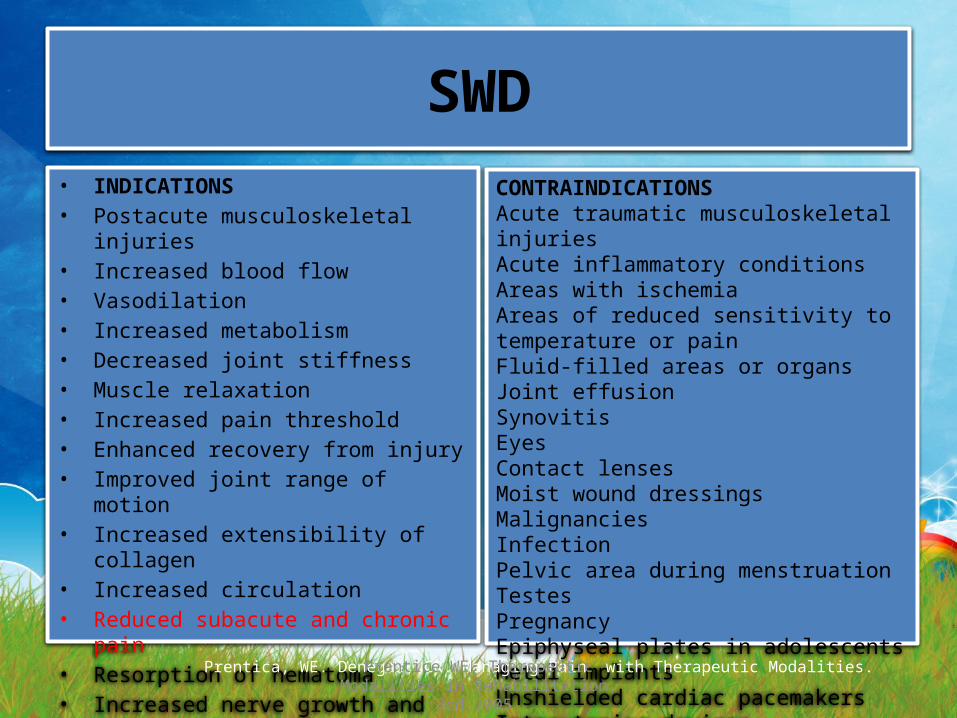
SWD• INDICATIONS• Postacute musculoskeletal injuries• Increased blood flow• Vasodilation• Increased metabolism• Decreased joint stiffness• Muscle relaxation• Increased pain threshold• Enhanced recovery from injury• Improved joint range of motion• Increased extensibility of collagen• Increased circulation• Reduced subacute and chronic pain• Resorption of hematoma• Increased nerve growth and repair
CONTRAINDICATIONSAcute traumatic musculoskeletal injuriesAcute inflammatory conditionsAreas with ischemiaAreas of reduced sensitivity to temperature or painFluid-filled areas or organsJoint effusionSynovitisEyesContact lensesMoist wound dressingsMalignanciesInfectionPelvic area during menstruationTestesPregnancyEpiphyseal plates in adolescentsMetal implantsUnshielded cardiac pacemakersIntrauterine devicesWatches or jewelry
Prentica, WE. Denegar, CR. Managing Pain with Therapeutic Modalities.
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
Mechanisms of Pain Control
• The theories presented are only models
• Pain control is the result of overlapping mechanisms
• Useful in conceptualizing the perception of pain and pain relief

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
Summary
• The goal of rehabilitation programs is to encourage early, pain-free exercise while promoting optimal healing processes

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
THANK YOU

Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005
Noxious Mediator
Prentice WE, Therapeutic Modalities in Rehabilitation, 3ed.2005