
Management of Acute Necrotizing Pancreatitis Dr Joyce WT Ng Tseung Kwan O Hospital.
29
Management of Acute Management of Acute Necrotizing Necrotizing Pancreatitis Pancreatitis Dr Joyce WT Ng Dr Joyce WT Ng Tseung Kwan O Hospital Tseung Kwan O Hospital
-
Upload
javier-burley -
Category
Documents
-
view
218 -
download
1
Transcript of Management of Acute Necrotizing Pancreatitis Dr Joyce WT Ng Tseung Kwan O Hospital.

Management of Acute Management of Acute Necrotizing PancreatitisNecrotizing Pancreatitis
Dr Joyce WT NgDr Joyce WT Ng
Tseung Kwan O HospitalTseung Kwan O Hospital

Prophylactic antibioticsProphylactic antibiotics ERCPERCP Nutritional supportNutritional support Inhibition of pancreatic secretionInhibition of pancreatic secretion Surgical interventionSurgical intervention
IndicationIndication TimingTiming ModalitiesModalities

IntroductionIntroduction
Severe pancreatitisSevere pancreatitis Acute pancreatitis associated with the Acute pancreatitis associated with the
presence of organ failure or presence of organ failure or pancreatic/peri-pancreatic complications, pancreatic/peri-pancreatic complications, or bothor both
Pancreatic necrosisPancreatic necrosis Diffuse or focal areas of non-viable Diffuse or focal areas of non-viable
pancreatic parenchyma, typically pancreatic parenchyma, typically associated with peri-pancreatic fat necrosisassociated with peri-pancreatic fat necrosis
A clinically based classification system for acute pancreatitis. Summary of the A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, 1992. International Symposium on Acute Pancreatitis, Atlanta, 1992.
Bradley EL et al. Arch Surg 1993Bradley EL et al. Arch Surg 1993

Surgical Surgical InterventionIntervention- Indications- Indications- Timing- Timing- Modalities- Modalities

Surgical Surgical InterventionIntervention- - IndicationsIndications- Timing- Timing- Modalities- Modalities

Indications: Infected Indications: Infected NecrosisNecrosis
Infected pancreatic necrosis is a Infected pancreatic necrosis is a uniformly accepted indication for uniformly accepted indication for surgical interventionsurgical intervention
Acute Pancreatitis: Who Needs an Operation?Acute Pancreatitis: Who Needs an Operation?Beger HG et la. J Hepatobiliary Pancreat Surg 2002Beger HG et la. J Hepatobiliary Pancreat Surg 2002
UK Guidelines for the Management of Acute PancreatitisUK Guidelines for the Management of Acute PancreatitisUK Working party on Acute Pancreatitis. Gut 2005UK Working party on Acute Pancreatitis. Gut 2005
Acute Necrotizing Pancreatitis: Acute Necrotizing Pancreatitis: Treatment Strategy According to the Status of InfectionTreatment Strategy According to the Status of Infection
Buchler MW et la. Ann Surg 2000Buchler MW et la. Ann Surg 2000

Indications: Sterile Indications: Sterile NecrosisNecrosis
Over 90% of patients with sterile Over 90% of patients with sterile necrosis can be successfully treated necrosis can be successfully treated without surgical interventionwithout surgical intervention
Acute Necrotiziing Pancreatitis:Acute Necrotiziing Pancreatitis: Treatment Strategy According to the Status of Infection. Treatment Strategy According to the Status of Infection.
Buchler MW et la. Ann Surg 2000Buchler MW et la. Ann Surg 2000
Surgical treatment of sterile necrosis Surgical treatment of sterile necrosis appears to have a higher mortality appears to have a higher mortality rates (11.9%, CI: 5.3-22.2) than the rates (11.9%, CI: 5.3-22.2) than the conservative treatment (2.3%, CI: 0.3-conservative treatment (2.3%, CI: 0.3-8.2) in patients with sterile necrosis8.2) in patients with sterile necrosis
Evidence-Based Treatment of Acute Pancreatitis. Evidence-Based Treatment of Acute Pancreatitis. A look at Established Paradigms. A look at Established Paradigms.
Heinrich S et la. Ann Surg 2006Heinrich S et la. Ann Surg 2006

Indications: Sterile Indications: Sterile NecrosisNecrosis
Small group of sterile necrosis still Small group of sterile necrosis still warrants surgical interventionswarrants surgical interventions Deteriorating condition despite Deteriorating condition despite
maximal supportmaximal support
Evidence-Based Treatment of Acute Pancreatitis. Evidence-Based Treatment of Acute Pancreatitis.
A look at Established Paradigms. A look at Established Paradigms.
Heinrich S et la. Ann Surg 2006Heinrich S et la. Ann Surg 2006
JPN Guidelines for the Management of Acute Pancreatitis: JPN Guidelines for the Management of Acute Pancreatitis:
Surgical ManagementSurgical Management
Isaji S et la. J Hepatobiliary Pancreat Surg, 2006Isaji S et la. J Hepatobiliary Pancreat Surg, 2006

Surgical Surgical InterventionIntervention- Indications- Indications- - TimingTiming- Modalities- Modalities

TimingTiming
First RCT First RCT Early (<72hrs, n=25) Vs Late (>12 days, n=15)Early (<72hrs, n=25) Vs Late (>12 days, n=15) Indication: MOF with clinical deterioration despite Indication: MOF with clinical deterioration despite
maximal intensive caremaximal intensive care Intervention: open packing with staged Intervention: open packing with staged
necrosectomynecrosectomy Mortality: 56% (early) Vs 27% (Late)Mortality: 56% (early) Vs 27% (Late) Prematurely terminated because of very high Prematurely terminated because of very high
mortality for early surgery group (odd ratio: 3.4)mortality for early surgery group (odd ratio: 3.4)
Early versus Late Necrosectomy in Severe Necrotizing Pancreatitis.
The American Journal of Surgery 1997 Feb;173(2):71-5.J Mier, E. Leon, A. Castillo, F Robledo, R Blanco

TimingTiming
.
Timing of Surgical Intervention in Necrotizing PancreatitisBesselink MG et al. Arch Surg 2007
•Systemic review of 11 series•Review of 1136 patients•Only 1 RCT

TimingTiming
Not recommended early surgical Not recommended early surgical interventionintervention
Late interventionLate intervention Separation of viable from non-viable Separation of viable from non-viable
tissuetissue Reduced bleeding Reduced bleeding Removal of less normal pancreasRemoval of less normal pancreas Operate on a more hemodynamically Operate on a more hemodynamically
stable patientstable patient
Analysis of the delayed approach to the management of infected Analysis of the delayed approach to the management of infected pancreatic necrosis. pancreatic necrosis. Nilesh D et al. Word J Gastro 2011Nilesh D et al. Word J Gastro 2011

TimingTiming
However, there was no consensus However, there was no consensus about the length of time that about the length of time that conservative treatment should be conservative treatment should be applied before surgical applied before surgical intervention should be consideredintervention should be considered
It is generalized accepted that at It is generalized accepted that at least 3-4 weeks of conservative least 3-4 weeks of conservative management is desirablemanagement is desirable
JPN Guideline for the Management of Acute Pancreatitis: JPN Guideline for the Management of Acute Pancreatitis: surgical Management. surgical Management. Isaji S. et al. J Hepatobiliary Pancreat Isaji S. et al. J Hepatobiliary Pancreat
Surg 2006Surg 2006

Surgical Surgical InterventionIntervention- Indications- Indications- Timing- Timing- - ModalitiesModalities
ModalitiesModalities
Open necrosectomyOpen necrosectomy Minimally invasive necrosectomyMinimally invasive necrosectomy
PercutaneousPercutaneous EndoscopicEndoscopic Laparoscopic assistedLaparoscopic assisted

Open necrosectomyOpen necrosectomy
Classical modality over the past Classical modality over the past decadesdecades
Principles: control septic fociPrinciples: control septic foci Debridement of the necrotic tissueDebridement of the necrotic tissue Post-operative lavage: removal of Post-operative lavage: removal of
retroperitoneal debris and exudatesretroperitoneal debris and exudates Mortality rate: 13-43%Mortality rate: 13-43%
Surgery in the Treatment of Acute Pancreatitis – Open Surgery in the Treatment of Acute Pancreatitis – Open Pancreatic Necrosectomy. Pancreatic Necrosectomy. Werner J et la. Scand J Surg 2005Werner J et la. Scand J Surg 2005

Open necrosectomyOpen necrosectomy
4 principle techniques:4 principle techniques:1.1. Opening packingOpening packing
2.2. Planned, staged relaparotomies Planned, staged relaparotomies with repeated lavagewith repeated lavage
3.3. Necrosectomy with continuous Necrosectomy with continuous lavage of the lesser sac and lavage of the lesser sac and retroperitoneumretroperitoneum
4.4. Necrosectomy with closed packingNecrosectomy with closed packing

Open necrosectomyOpen necrosectomy
Single necrosectomy with post-Single necrosectomy with post-operative lavage without planned operative lavage without planned relaparotomies seems to be less relaparotomies seems to be less harmful harmful More complications (e.g. fistula, More complications (e.g. fistula,
incisional hernia, local bleeding) incisional hernia, local bleeding) were seen in repeated laparotomieswere seen in repeated laparotomies
Surgery in the Treatment of Acute Pancreatitis – Open Pancreatic Surgery in the Treatment of Acute Pancreatitis – Open Pancreatic Necrosectomy. Necrosectomy. Werner J et la. Scand J Surg 2005Werner J et la. Scand J Surg 2005
Acute Pancreatitis at the beginning of the 21Acute Pancreatitis at the beginning of the 21stst century: The state of century: The state of the art. the art. Tonsi AF et al. World J Gastroenterol 2009 Tonsi AF et al. World J Gastroenterol 2009

Minimally Invasive Minimally Invasive NecrosectomyNecrosectomy
Developed in recent 2 decadesDeveloped in recent 2 decades It is generally accepted to have It is generally accepted to have
comparable results with open comparable results with open necrosectomynecrosectomy
No randomized studies for No randomized studies for comparisoncomparison
Approaches:Approaches: PercutanoeusPercutanoeus Endoscopic Endoscopic Laparoscopic-assistedLaparoscopic-assisted

1. Percutaneous 1. Percutaneous NecrosectomyNecrosectomy
An endoscope is inserted into the An endoscope is inserted into the retroperitoneal space under GAretroperitoneal space under GA Utilize CT guided placement of Utilize CT guided placement of
small calibre percutanous drain small calibre percutanous drain into retroperitoneuminto retroperitoneum
Mainly over left flank Mainly over left flank The tract is then dilated for The tract is then dilated for
passage of the scopepassage of the scope Remove debris by lavage and Remove debris by lavage and
piecemeal extraction of necrotic piecemeal extraction of necrotic debrisdebris
Post operative continuous lavagePost operative continuous lavage
NICE Guideline for Percutaneous Pancreatic NecrosectomyNICE Guideline for Percutaneous Pancreatic Necrosectomy
1. Percutaneous 1. Percutaneous NecrosectomyNecrosectomy
Potential advantages:Potential advantages: Less postoperative physiological Less postoperative physiological
disturbancedisturbance Reduced need for intensive careReduced need for intensive care Fewer complicationsFewer complications
Limitations:Limitations: May not have feasible route for necrosis May not have feasible route for necrosis
in head or uncinate regionin head or uncinate region May require multiple sessions May require multiple sessions
(subsequent session can be done under (subsequent session can be done under LA)LA)
Minimal Access Retroperitoneal Pancreatic NecrosectomyMinimal Access Retroperitoneal Pancreatic NecrosectomyImprovement in Morbidity and Mortality With a Less Invasive Improvement in Morbidity and Mortality With a Less Invasive
Approach.Approach.Raraty MGT et la. Ann Surg 2010Raraty MGT et la. Ann Surg 2010

2. Endoscopic 2. Endoscopic NecrosectomyNecrosectomy
Usually under LA with sedationUsually under LA with sedation Localize the collection with EUSLocalize the collection with EUS Transgastric/ transduodenal punctureTransgastric/ transduodenal puncture Tract is dilatedTract is dilated and scope enter cavityand scope enter cavity Necrosectomy under direct vision with Necrosectomy under direct vision with
irrigation, use of forceps or snaresirrigation, use of forceps or snares Placement of multiple nasocystic Placement of multiple nasocystic
drains for post-operative drainagedrains for post-operative drainagePeroral Transgastric/ Transduodneal Necrosectomy. Peroral Transgastric/ Transduodneal Necrosectomy.
Success in the Treatment of Infected Pancreatic Necrosis. Success in the Treatment of Infected Pancreatic Necrosis. Escourrou J et al. Ann Surg 2008Escourrou J et al. Ann Surg 2008

2. Endoscopic 2. Endoscopic NecrosectomyNecrosectomy
Potential advantagesPotential advantages Comparable results with open necrosectomyComparable results with open necrosectomy Less postoperative physiological disturbanceLess postoperative physiological disturbance Reduced need for intensive careReduced need for intensive care Providing diagnostic and therapeutic option for Providing diagnostic and therapeutic option for
biliary pathologies at the same sessionbiliary pathologies at the same session LimitationsLimitations
Highly skilled experienced interventional Highly skilled experienced interventional endoscopistendoscopist
Transient aggravation of sepsis and hemorrhageTransient aggravation of sepsis and hemorrhage Cannot deal with extended necrosis to paracolic Cannot deal with extended necrosis to paracolic
guttergutter Limited ability to evacuate large cavitiesLimited ability to evacuate large cavities Multiple sessions were requiredMultiple sessions were required
Peroral Endoscopic Drainage/ Debridement of Walled-off Peroral Endoscopic Drainage/ Debridement of Walled-off Pancreatic Necrosis. Pancreatic Necrosis. Papachristou GI. Ann Surg 2007Papachristou GI. Ann Surg 2007

3. Laparoscopic-assisted 3. Laparoscopic-assisted NecrosectomyNecrosectomy
2-5 ports2-5 ports +/- hand ports+/- hand ports Mainly with infra colic approachMainly with infra colic approach
3. Laparoscopic- assisted 3. Laparoscopic- assisted NecrosectomyNecrosectomy
Potential advantagesPotential advantages Decrease the trigger of systemic Decrease the trigger of systemic
cytokine-mediated immune responsecytokine-mediated immune response Better exposureBetter exposure
Possible complicationsPossible complications Spreading of infection to infracolic Spreading of infection to infracolic
compartmentscompartments Similar morbidity rate compared with Similar morbidity rate compared with
open surgeryopen surgery
Laparoscopic-Assisted Pancreatic Necrosectomy.Laparoscopic-Assisted Pancreatic Necrosectomy.A new Surgical Option for Treatment of Severe Necrotizing A new Surgical Option for Treatment of Severe Necrotizing
Pancreatitis.Pancreatitis.Parekh D. Arch Surg 2006 Parekh D. Arch Surg 2006

First RCT First RCT Multi-centre (20 hospitals in Holland)Multi-centre (20 hospitals in Holland) Step-up Approach (45) Vs Open Step-up Approach (45) Vs Open
necrosectomy (43)necrosectomy (43) Primary end-point: major complications/ Primary end-point: major complications/
deathdeath
A Step-up Approach or Open Necrosectomy for Necrotizing
Pancreatitis(PANTER trial: Pancreatitis, Necrosectomy versus
sTEp up appRoach)Santvoot HC et la. N Engl J Med 2010 Apr 22. 362(16): 1491-502
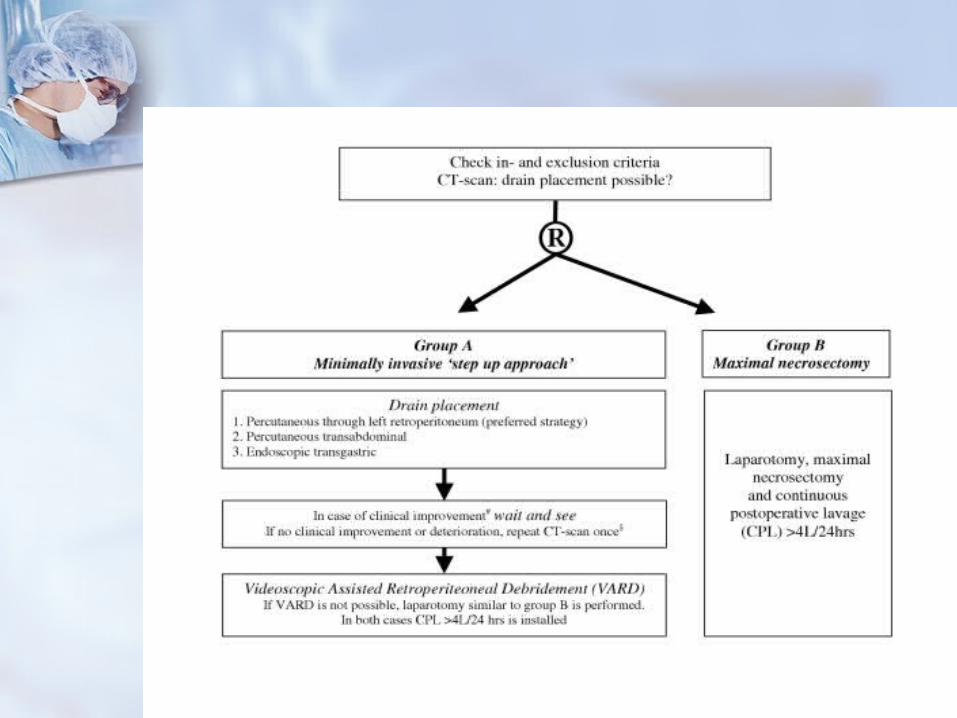

Major complication: 12% (step-up) Major complication: 12% (step-up) Vs 40% (open), p= 0.002Vs 40% (open), p= 0.002
Mortality: 19% (step-up) Vs 16% Mortality: 19% (step-up) Vs 16% (open), p= 0.7(open), p= 0.7
Primary end-point: 40% (step-up) Primary end-point: 40% (step-up) Vs 69% (open), p= 0.006Vs 69% (open), p= 0.006
Conclusion: The minimally invasive Conclusion: The minimally invasive step-up approach reduced the rate step-up approach reduced the rate of the composite end point of major of the composite end point of major complications or deathcomplications or death

Conservative treatment
MOFIntensive Care
Infected Necrosis Sterile Necrosis
Failed
3-4weeks
1. Favourable condition
2. Available experts
Surgery
MIS approach Open necrosectomy


















