Malattia HER-2 positiva Terapia per la fase metastatica Cosa sapremo presto: nuovi farmaci U.O. di...
26
Malattia HER-2 positiva Malattia HER-2 positiva Terapia per la fase metastatica Terapia per la fase metastatica Cosa sapremo presto: nuovi farmaci Cosa sapremo presto: nuovi farmaci U.O. di Oncologia Medica “Sandro Pitigliani” Dipartimento di Oncologia USL 4 Prato Angelo Di Leo
-
Upload
mae-malone -
Category
Documents
-
view
214 -
download
0
Transcript of Malattia HER-2 positiva Terapia per la fase metastatica Cosa sapremo presto: nuovi farmaci U.O. di...

Malattia HER-2 positivaMalattia HER-2 positivaTerapia per la fase metastaticaTerapia per la fase metastatica
Cosa sapremo presto: nuovi farmaciCosa sapremo presto: nuovi farmaci
U.O. di Oncologia Medica “Sandro Pitigliani”Dipartimento di Oncologia
USL 4 Prato
Angelo Di Leo

Ongoing – Future strategies
• Complete HER-2 receptor blockade
• Inhibiting HER-2 dimerization
• Multi-targeted bio-therapy without chemotherapy
• A more potent trastuzumab : TDM-1

Lapatinib 1000 mg qd +
continuation of trastuzumab 2 mg/kg qw
(n=148)
MBC HER2-positive (IHC 3+ / FISH positive) Progression on prior Herceptin-based regimena
(n=296)
Lapatinib 1500 mg qd(n=148)
R
EGF104900: study design
aPatients received a median of 3 prior lines of trastuzumabor 4-5 prior lines of chemotherapy; IHC, immunohistochemistry; FISH, fluorescence in situ hybridisation; qd, every day; qw, every week; PD, progression of disease
Crossover if PD after 4 weeks of therapy(77 patients)
Blackwell K et al, J Clin Oncol 28: 1124-30, 2010

Probability of PFS
0 2 4 6 8Time (months)
0.0
0.2
0.4
0.6
0.8
1.0
10 12
EGF104900: PFS
2.8a1.9a
trastuzumab+ lapatinib (n=146)
Lapatinib (n=145)
HR=0.73; p=0.008
aMedian PFS in months
148148
7353
4221
2713
85
20
Blackwell K et al, J Clin Oncol 28: 1124-30, 2010

EGF104900: Updated OS (SABCS2009)
0.0
0.2
0.4
0.6
0.8
1.0
0 10 20 25Time (months)
5 15 30 35
148148
8865
4328
12513
6447
121102
Probability of survival
14.0a 9.5a
aMedian OS in months
trastuzumab+ lapatinib (n=146)
Lapatinib (n=145)
HR=0.74; p=0.026
Blackwell K et al, J Clin Oncol 28: 1124-30, 2010

EGF104900: results
ORR, %
CBR, %
Median PFS, months
Median OS, months
Lapatinib
6.9
12.4
1.9
9.5
Lapatinib + Herceptin
10.3
24.7
2.8
14.0
p value
0.46
0.01
0.008
0.026
HR
0.73
0.74
Blackwell K et al, J Clin Oncol 28: 1124-30, 2010

EGF104900: safety profile
Grade 3/4, diarrhoea, n (%)
Symptomatic LVEF decline (LV dysfunction ≥ grade 3 or LVEF decrease ≥20% and below LLN), n (%)
Cardiac-related deaths, n (%)
Lapatinib
10 (7)
3 (2)
0 (0)
Lapatinib + Herceptin
12 (8)
10 (7)
1 (0.7)a
LLN, lower limit of normalaDeath due to pulmonary thromboembolism
Blackwell K et al, J Clin Oncol 28: 1124-30, 2010

Complete HER-2 receptor blockade : key message
Concomitant inhibition of the HER-2 external domain and the HER-2 tyrosine kinase more active than single inhibition either as upfront or as a further-line treatment

BO17929: A multicentre Phase II trial of trastuzumab + pertuzumab in HER2-positive MBC that progressed during trastuzumab-based therapy
• Primary endpoint:– Response rate and clinical benefit rate (response rate + disease stabilisation)
HER2-positive MBC progressing on trastuzumab
+ chemotherapy (Cohort 1, n=24; Cohort 2, n=42)
Pertuzumab+ trastuzumab
16 patients receivedpertuzumab + trastuzumab
HER2-positive MBC progressing on trastuzumab
+ chemotherapy (n=29)
PertuzumabPD
MBC = metastatic breast cancer; PD = progressive disease1. Baselga et al. J Clin Oncol 2010;28:1138–1144;
2. Baselga et al. SABCS 2009. Abstract 5114
Cohorts 1 and 21
Cohort 3 (added after protocol amendment)2
Inhibiting HER-2 / HER-3 dimerization: Pertuzumab

BO17929 (cohorts 1 and 2): The combination of pertuzumab and trastuzumab demonstrates
encouraging efficacy
Response n (%)(n=66)
Complete responsea,b 4 (6.1)
Partial responsea,b 12 (18.2)
Objective response rate 16 (24.2)
Stable disease for 8 cycles or ~6 months 17 (25.8)
Clinical benefit rate (CR + PR + SD ≥6 months) 33 (50.0)
Progressive disease 33 (50.0)
Baselga et al. J Clin Oncol 2010;28:1138–1144Cortes J et al. J Clin Oncol 2010;28(7S):Abstract 1066
aMedian duration of response was 5.8 months (2.9–15.3 months);bOne patient was reclassified from a CR to a PR CR = complete response; PR = partial response; SD = stable disease

BO17929 (cohorts 1 and 2): Adverse events were generally grade 1/2
• The most frequent adverse events were grade 1/2 and included diarrhoea, fatigue, nausea, and rash
• Only 4 of 66 patients had treatment-related adverse events grade 3
• Grade 3 adverse events were:
Adverse event n (%) Outcome Treatment continued
Diarrhoea 2 (3) Resolved Yes
Central line infection
1 (2) Resolved Yes
Pruritic rasha 1 (2) Resolved Yes
aOne patient had a grade 3 pruritic rash following injection of contrast before receiving pertuzumabSAE = serious adverse event; NR = Not reported Baselga et al. J Clin Oncol 2010;28:1138–1144

BO17929: A multicentre Phase II trial of trastuzumab + pertuzumab in HER2-positive MBC that progressed during trastuzumab-based therapy
• Primary endpoint:– Response rate and clinical benefit rate (response rate + disease stabilisation)
1. Baselga et al. J Clin Oncol 2010;28:1138–1144;2. Baselga et al. SABCS 2009. Abstract 5114MBC = metastatic breast cancer; PD = progressive disease
HER2-positive MBC progressing on trastuzumab
+ chemotherapy (Cohort 1, n=24; Cohort 2, n=42)
Pertuzumab+ trastuzumab
16 patients receivedpertuzumab + trastuzumab
HER2-positive MBC progressing on trastuzumab
+ chemotherapy (n=29)
PertuzumabPD
Cohorts 1 and 21
Cohort 3 (added after protocol amendment)2

BO17929: Pertuzumab plus trastuzumab demonstrated encouraging efficacy
Response, n (%)Cohorts 1 and 21,2
(n=66)
Cohort 32 (pertuzumab)
(n=29a)
Cohort 32
(pertuzumab + trastuzumab)
(n=16b)
Complete response 4 (6.1)c 0 (0.0) 0 (0.0)
Partial response 12 (18.2)c 1 (3.4) 3 (21.4)
Objective response rate 16 (24.2) 1 (3.4) 3 (21.4)
Stable disease for 8 cycles (6 months)
17 (25.8) 2 (6.9) 3 (21.4)
Clinical benefit rate 33 (50.0) 3 (10.3) 6 (42.8)
Progressive disease 33 (50.0) 24 (82.8) 8 (57.1)
aOnly 27 patients are evaluable: 1 patient did not progress on pertuzumab monotherapy before moving on to combination therapy and 1 patient’s tumour was unassessable after Cycle 2bn=14 as at data cut-off; 1 patient had not reached overall best response endpoint (8 cycles of assessment during this phase) and 1 patient died before efficacy assessmentcOne patient was reclassified from a CR to a PR
1. Baselga et al. J Clin Oncol 2010;28:1138–1144;2. Cortes J et al. J Clin Oncol 2010;28(7S):Abstract 1066
3. Baselga et al. SABCS 2009. Abstract 5114

BO17929 (cohort 3): Pertuzumab monotherapy and combination therapy with trastuzumab were both well tolerated
Pertuzumab (n=29)n (%)
Pertuzumab + trastuzumab (n=16)n (%)
Adverse event Any gradea Grade 3/4 Any gradea Grade 3/4
Diarrhoea 14 (48) 1 (3) 5 (31) 1 (6)
Nausea 10 (34) - 5 (31) -
Vomiting 7 (24) - 4 (25) -
Fatigue 5 (17) 1 (3) 4 (25) 1 (6)
Asthenia 5 (17) - 2 (13) -
Back pain 5 (17) - 2 (13) 1 (6)
Rash 3 (10) - 3 (19) -
Chills - - 3 (19) -
Weight decrease - - 3 (19) -
Baselga et al. SABCS 2009. Abstract 5114aAdverse event occurring in 15% patients

BO17929: Conclusions
• The combination of trastuzumab and pertuzumab is active in patients with HER2-positive breast cancer who have experienced progression during:
– Prior trastuzumab therapy1
– Prior sequential treatment with single-agent trastuzumab and pertuzumab2
• Pertuzumab monotherapy and combination therapy with trastuzumab were well tolerated and there were no significant cardiac events1,2
• The partnership of pertuzumab and trastuzumab may offer an effective new treatment option for patients with HER2-positive MBC
1. Baselga et al. J Clin Oncol 2010;28:1138–1144; 2. Baselga et al. SABCS 2009. Abstract 5114MBC = metastatic breast cancer

• Trastuzumab-DM1 (T-DM1) is a novel anti-HER2 antibody drug–conjugate in development for the treatment of HER2-positive metastatic breast cancer (MBC)1,2
– Combines the HER2-targeting properties of trastuzumab3 with targeted delivery of a highly potent anti-microtubule derivative, DM13-5
– After binding to HER2, T-DM1 undergoes receptor-mediated internalization,6 resulting in intracellular release of DM1
1. Krop I, et al. J Clin Oncol 2008. 28:2698-27042. Burris HA, et al. J Clin Oncol, 2010, in press 20103. Lewis Phillips, et al. Cancer Res. 2008. 68:9280-90.
4 . Junttila TT, et al. Breast Cancer Res Treat, 2010, epub ahead of press5. Remillard S, et al. 1975. Science 189:1002–1005.3. 6. Austin CD, et al. 2004. Mol Biol Cell 15(12):5268–5282.
A more potent trastuzumab: TDM 1

TDM4258g TDM4374g
N=112 N=110
ORR, % 25.9% 32.7%
Clinical benefit rate, % 39.3% 48.2%Median Duration of Response (95% CI)
NR(6.2, NE)
NR (4.6, NE)
Median PFS (95% CI) 4.6 m(3.9, 8.6)
6.9 m(4.2, 9.5)
ORR in patients with retrospectively confirmed HER2+ 32.1% 40.3%
Studies TDM4374g and TDM4258g: Antitumor Activity by IRF Assessment

T-DM1 ISS AE Summary
• The majority of AEs were grade (Gr) 1−2 • Most common AEs (≥ 20% pts) of all grades were fatigue (63.3%), nausea (43.9%), and
headache (31.2%) • 109 pts (46.0%) experienced at least one Gr ≥ 3 AE
– Most common Gr ≥ 3 AEs: thrombocytopenia (7.6%), hypokalaemia (4.6%), fatigue (4.2%), cellulitis (3.4%)
• SAE were reported in 61 pts (25.7%)– Most common SAEs : cellulitis (3.4%), convulsion (2.5%), pneumonia (2.5%), and
dyspnoea (1.7%)• 20/237 (8%) patients discontinued treatment for adverse events• 5 total deaths within 30 days of last protocol therapy
– 4 patients attributable to progressive disease or underlying disease
– 1 due to Grade 5 AE (Hepatotoxicity)

• Randomized, phase II, international, open-label study• HER2+, measurable disease required• Stratification factors:
– World region, prior adjuvant trastuzumab therapy, disease-free interval • Key Primary endpoint: PFS by INV• Key Secondary endpoints: ORR, CBR, OS
TDM4450g: Study Design
HER2-positive, recurrent locally advanced BC or MBC (n=137)
Previously untreated
T-DM13.6 mg/kg Q3W until PD
Trastuzumab 8 mg/kg loading dose; 6 mg/kg Q3W
+ Docetaxel 75 or 100 mg/m2 Q3W
CrossoverT-DM1PD
Hurvitz SA et al, proc. ESMO/ECCO 2011, abstr. 5.001

Objective Response by Investigator Patients With Measurable Disease at Baseline
Trastuzumab + docetaxel
(n=69)a
T-DM1 (n=67)
Patients with an objective response,b n (%) 40 (58.0) 43 (64.2)
95% CI 45.5–69.2 51.8–74.8
Objective responses, n (%)
Complete response 3 (4.3) 7 (10.4)
Partial response 37 (53.6) 36 (53.7)
Stable disease 23 (33.3) 13 (19.4)
Progressive disease 4 (5.8) 8 (11.9)
Unable to evaluate or missing 2 (2.9) 3 (4.5)
Patients with clinical benefit,c n (%) 56 (81.2) 50 (74.6)
95% CI 70.7–89.1 63.2–84.2
aOne patient was not included in the efficacy analysis due to study site withdrawal.bDefined as complete or partial response based on RECIST 1.0 determined on 2 consecutive tumor assessments at least 4 weeks apart.cDefined as objective response any time during the study or maintained stable disease for at least 6 months from randomization.

Time (months)Time (months)
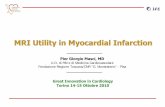
Progression-Free Survival by InvestigatorRandomized Patients
Pro
por
tion
prog
ress
ion
-fre
e P
rop
ortio
n pr
ogre
ssio
n-f
ree
1.0
0.8
0.6
0.4
0.2
0.0
1.0
0.8
0.6
0.4
0.2
0.00 2 4 6 8 10 12 14 16 18 200 2 4 6 8 10 12 14 16 18 20
Number of patients at risk
T+D 70 66 63 53 43 27 12 4 2 2 0T-DM1 67 60 51 46 42 35 22 15 6 3 0
Number of patients at risk
T+D 70 66 63 53 43 27 12 4 2 2 0T-DM1 67 60 51 46 42 35 22 15 6 3 0
Hazard ratio and log-rank P value were from stratified analysis.
Trastuzumab + docetaxel (n=70)T-DM1 (n=67)
Trastuzumab + docetaxel (n=70)T-DM1 (n=67)
Median
PFS, mos
Hazard ratio 95% CI
Log-rank P value
9.2
14.20.594
0.364– 0.968
0.0353

Incidence of Hematologic Adverse Events: ≥30% (All Grade) and/or ≥5% (Grade ≥3) of Patientsa
Green represents those AEs with ≥20% difference between treatment arms.
aIn either treatment arm.bNo adverse events listed were grade 5.cTwo patients mistakenly received a dose of T-DM1 and were thus included in the T-DM1 arm for safety analyses.dIncludes 3 patients who received at least 1 dose of trastuzumab alone or trastuzumab plus docetaxel.e Neutropenia includes events classified as MedDRA preferred terms neutropenia or neutrophil count decreased; thrombocytopenia includes
events classified as MedDRA preferred terms thrombocytopenia, platelet count decreased or heparin-induced thrombocytopenia; leukopenia includes events classified as MedDRA preferred terms leukopenia or white blood cell count decreased.
fAll of these events were grade 3.
Green represents those AEs with ≥20% difference between treatment arms.
aIn either treatment arm.bNo adverse events listed were grade 5.cTwo patients mistakenly received a dose of T-DM1 and were thus included in the T-DM1 arm for safety analyses.dIncludes 3 patients who received at least 1 dose of trastuzumab alone or trastuzumab plus docetaxel.e Neutropenia includes events classified as MedDRA preferred terms neutropenia or neutrophil count decreased; thrombocytopenia includes
events classified as MedDRA preferred terms thrombocytopenia, platelet count decreased or heparin-induced thrombocytopenia; leukopenia includes events classified as MedDRA preferred terms leukopenia or white blood cell count decreased.
fAll of these events were grade 3.
AE
All grade, n (%) Grade ≥3b, n (%)
Trastuzumab + docetaxel (n=66)c
T-DM1 (n=69)c,d
Trastuzumab + docetaxel (n=66)c
T-DM1 (n=69)c,d
Neutropeniae 42 (63.6) 12 (17.4) 40 (60.6) 4 (5.8)Febrile neutropenia 9 (13.6) 0 9 (13.6) 0Thrombocytopeniae 4 (6.1) 21 (30.4) 2 (3.0)f 6 (8.7)f
Leukopeniae 18 (27.3) 6 (8.7) 17 (25.8) 0

Incidence of Nonhematologic Adverse Events: ≥30% (All Grade) and/or ≥5% (Grade ≥3) of Patientsa
Green represents those AEs with ≥20% difference between treatment arms.
aIn either treatment arm.bNo adverse events listed were grade 5.cTwo patients mistakenly received a dose of T-DM1 and were thus included in the T-DM1 arm for safety analyses.dIncludes 3 patients who received at least 1 dose of trastuzumab alone or trastuzumab plus docetaxel.eNational Cancer Institute Common Terminology Criteria for Adverse Events v.3 only categorizes alopecia as grade 1 or grade 2; there is no grade ≥3 for this AE.
AE
All grade, n (%) Grade ≥3b, n (%)
Trastuzumab + docetaxel (n=66)c T-DM1 (n=69)c,d
Trastuzumab + docetaxel (n=66)c T-DM1 (n=69)c,d
Alopecia 44 (66.7) 3 (4.3) e e
Fatigue 30 (45.5) 34 (49.3) 3 (4.5) 3 (4.3)
Nausea 29 (43.9) 33 (47.8) 0 2 (2.9)Diarrhea 30 (45.5) 11 (15.9) 2 (3.0) 0
Peripheral edema 29 (43.9) 7 (10.1) 3 (4.5) 0Increased AST 4 (6.1) 27 (39.1) 0 6 (8.7)
Pyrexia 15 (22.7) 27 (39.1) 1 (1.5) 0Headache 12 (18.2) 25 (36.2) 0 0
Back pain 20 (30.3) 18 (26.1) 3 (4.5) 1 (1.4)Increased ALT 4 (6.1) 16 (23.2) 0 6 (8.7)
Pneumonia 1 (1.5) 6 (8.7) 0 4 (5.8)

Cardiac Safety
• Cardiac function was assessed locally and centrally based on cardiac ECHO/MUGA
• Prior anthracycline in the adjuvant setting was 44.8% and 48.6% in the T-DM1 and trastuzumab + docetaxel arms, respectively
• Asymptomatic LV dysfunction
• There were no clinically significant cardiac events reported
LVEF assessment Trastuzumab + docetaxel T-DM1
Local assessment
Patients assessed 65 67
Patients with post-baseline LVEF ≤40% 2a 0
Central assessment
Patients assessed 60 65
Patients with post-baseline LVEF ≤40% 1b 0
aBoth patients had prior anthracycline therapy in the adjuvant setting; 1 patient received prior trastuzumab therapy in the adjuvant setting.bThis patient did not receive prior treatment with an anthracycline.
aBoth patients had prior anthracycline therapy in the adjuvant setting; 1 patient received prior trastuzumab therapy in the adjuvant setting.bThis patient did not receive prior treatment with an anthracycline.

The future: Do we need more anti-HER-2 compounds or more bio-markers driving our treatment choices?
• Anti-HER-2 sensitive population:
Trastuzumab alone vs. combination
• Anti-HER-2 partially sensitive/resistant population:
Trastuzumab in combination with agents such as
• Anti-HER-2 ± chemotherapy
• If Trastuzumab with chemotherapy
lapatinib
pertuzumab
PI3K inhibitors
HSP 90 inhibitors
anti IGF-1R inhibitors
which regimen
taxaneanthracyclines
TDM1
others (DNA damaging agents, vinorelbine,….)