Makerere School of Public Health Maternal and Newborn...
12
Makerere School of Public Health Maternal and Newborn Health Symposium 2014 Sharing Experiences & Learning from Stakeholders 2014 Inside this Issue Editorial ................................................................................................... 2 • MANIFEST: Working with Districts and the Community to improve maternal & • newborn health...................................................................................................3 MANEST: Innovations for Increasing Access to Integrated safe delivery...............4 • EQUIP: Using Information Power to improve maternal and newborn health..........7 • The FIGO Save the Mothers Initiative in Kiboga...............................................8 • Health Cooperatives: Increased Access to Care....................................................8 • Key Reactions....................................................................................................9 • Discussion...................................................................................................10 •
Transcript of Makerere School of Public Health Maternal and Newborn...

Maternal and Newborn Health Symposium 2014 1
Makerere School of Public Health Maternal and Newborn Health Symposium 2014
Sharing Experiences & Learning from Stakeholders
2014Inside this Issue
Editorial...................................................................................................2•MANIFEST: Working with Districts and the Community to improve maternal &•newborn health...................................................................................................3MANEST: Innovations for Increasing Access to Integrated safe delivery...............4•EQUIP: Using Information Power to improve maternal and newborn health..........7•The FIGO Save the Mothers Initiative in Kiboga...............................................8•Health Cooperatives: Increased Access to Care....................................................8•Key Reactions....................................................................................................9•Discussion...................................................................................................10•

Maternal and Newborn Health Symposium 2014 2
The Makerere University School of Public Health (MakSPH) has conducted several maternal health related projects over the years. Interaction with a diversity of key stakeholders has majorly been at the beginning and at the end
of these studies. However, under the auspices of two projects under the Future Health Systems Research Consortium (Maternal and Neonatal Implementation for Equitable Systems study - MANIFEST and the Maternal and Newborn Study - MANEST) and the EQUIP study, MakSPH held a Maternal and Newborn Health symposium on May 14, 2014 in Kampala to herald a new beginning in dealing with key stakeholders.
The main focus of the symposium was for the MakSPH study team to share MANIFEST, MANEST and EQUIP progress (early successes, lessons and challenges) to date, but at the same time also get experiences from stakeholders who are implementing or have implemented similar interventions.
In addition to hearing from the three MakSPH projects, the symposium was also graced with presentations from HealthPartners Uganda and the Association of Obstetricians andGynaecologistsofUganda.Itistheday’sfivepresentationsthatformedthebasisfor the symposium discussions. However, a poem titled The Man in the Land Cruiser andopeningremarksfromthefirsttwochairswereagoodstartertothesymposiumand set the scene for the presenters of the day.
Contextualizing the MNH Symposium
By Catherine Ruhweza
The man in the Land Cruiser! Sorry. I saw your Land Cruiser passing by. I saw the crowd running up to you. Sorry I could not lift my hand to wave. Actually I tried to wave but the baby kicked my naval. So I stopped halfway. But the crowd looked so good. It looked so big. So I guess, you are having a good time.
I guess you are happy. By the way, do you remember me? Can you recall my name? I am the woman who danced lame at your victory party. I am the woman who fought with her husband during your campaigns. I am the woman who neglected her shamba following your trail. I am the woman who carried loads of soap, distributed quarter kilos of sugar.
I am the woman who recited your promises like a creed. I am the woman now heading to the hospital. I need to hear your voice. Say something to me. This is more important to me than sugar; more important than soap. Didn’t you promise to give me a better deal? I remember you said our mothers shouldn’t die giving birth to life. But now answer me; will I find someone at the hospital to delivermy baby?
The Man in the Land Cruiser
EDITORIAL
“Uganda is not doing well when we compare the health of mothers and newborns to that of older children. However my usual message is that older children can get vaccines, we can buy medicine but mother and newborns need a system that delivers quality care. Recently, a publication in the Lancet by the Institute for Health Metrics and Evaluation showed that the Maternal Mortality Ratio in Uganda was still very high. The UN published another one. In fact according to that report, MMR in Uganda by 2013 is estimated to be 360, within a range of 230 to 580. So they [publications] are all the same if you look at the confidence interval. Butboth reports say Uganda is among the top ten countries in the world that contribute to maternal deaths. This makes this meeting very relevant.” - Dr Peter Waiswa, Principal Investigator of MANEST
Dr Peter Waiswa
By Catherine Ruhweza
“We at Makerere University are always producing knowledge. We would like you to tell us the most important key questions that we may be missing out. You are going to give us feedback to stimulate us to think about these problems. People from universities tend to think about complicated things, but it is important to listen to stakeholders. And that could make a huge impact in terms of outcomes.” - Prof. David Serwadda, immediate
former dean MakSPH
Prof. David Serwada

Maternal and Newborn Health Symposium 2014 3
EXPERIENCES
From the duo, the symposium learnt that the study is in three districts (Kamuli, Pallisa and Kibuku) in eastern Uganda and is using a Participatory Action Research approach. PAR was chosen to encourage local ownership, use of local resources, and ensure stakeholder participation. Ultimately, this is expected to build local district capacity for sustainability, empower communities to make a contribution towards improving their health outcomes and increase chances of program scale up.
Approach
Expected outcomesImproved awareness of maternal and•newborn care seekingImproved awareness of maternal•newborn care and care seekingImproved access and use of savings and•transport mechanismsImproved maternal and newborn care•practicesIncreased number of skilled attended•deliveries, antenatal care and postnatalcare.Improved skills among health workers•and managers
Early ResultsThe early results from the project are indicated in the table below:
Experiences from Implementation: Working with Districts & Community to improve maternal & newborn health
Early lessons• Existing community structuressuchasfinancialnetworks,community health workers
(VHTs) and private transporters should be ‘exploited’ to increase access to MNH;
• Useoflocalstakeholders
as implementers empowers the community to solve local problems and also builds local capacity for sustainability purposes;• Implementationrequiresclosemonitoring and mentoring; • Theflexibilityprovidedbytheparticipatory action research (PAR) approach allows implementers to learn and make adjustments that can promote successful implementation; • Thedistrictsreportedimprovedmanagement skills demonstrated throughconstructiveconflictresolution, improved accountability and transparency, team work and more evidence based decision
making.
ChallengesCommunity mobilization and empowerment component
Dependency culture with a community•that is used to free thingsPoor saving culture•Slow process of creating linkages•between transporters and saving groupsLow VHT literacy levels - where•selection guidelines are not followed,and where literacy levels are generallylowPoor• mobilization for CommunityDialogues
Health systems component Health worker shortage•Poor infrastructure in some health•facilitiesPoor referral systems•Drugs and supplies shortages•Poor health worker attitudes•
“Participatory approaches can empower local implementers to identify and solve local challenges that hinder the utilization and delivery of MNH services.”
Mr. Moses Tetui the study coordinator of MANIFEST (maternal and neonatal implementation for equitable systems) together with Dr. Ahmed Bumba the DHO of one of the implementing districts (Kibuku) shared the experiences of researchers working with district stakeholders and communities to improve maternal and newborn health.
3
• Training in health services managment: Resource mobilisationand allocation, information use,mentoring and supervision, PAR approach
• Promoting birth preparedness
• Sensitisation by CHWs• Linkages with FSNs• Linking transporters with FSNs
• Provision of non financial incentives: basic training, basic supplies, performance recognition, supervision
•MNH campaigns by districtand community leaders
•Community dialogues•Media campaigns• Linking communities with FSNs • Linking transporter with FSNs
CommunitiesImproved routine and referral
transport to support MNH service uptake
More male involvement in MNH Better participation in ensuring
accountability from health service providers
Health ProvidersMotivated to provide better quality servicesBetter use of available MNH resourcesSupport to VHTs to sensitise communitiesSupervision of VHTs to ensure performance
District leadersImproved planning and Mgt for MNH servicesBetter support supervision to health providersMore advocating for resources for MNH service
HouseholdsImproved Maternal and newborn care practicesSaving for MNH related
needs such as birth items and transport.
increased use of transport services
Improved uptake of MNH services
How can maternal and newborn lives be
saved through strengthening health service provision and
linkages between transporters, commu
nities, health providers and district
leaders?
Improved maternal and newborn outcomes:
Reduced maternal and newborn deaths
TECH
NIC
AL SU
PPOR
T BY
MA
KSPH
AN
D O
THER
PA
RTN
ERS
TEC
HN
ICA
L SU
PPO
RT
BY
MA
KSP
H A
ND
OTH
ER
PAR
TNER
S
Our approach 6
Initial results and experiences
Indicator Baseline LQAS 1 LQAS2 Target
ANC 4 time attendance
43% 53% 68.4% 63%
Deliveries from the Health Facilities
66% 76% 84% 81%
Mr. Moses Tetui and Dr. Ahmed Bumba
7
Improved knowledge among women
Indicator Baseline LQAS 2 Target
Pregnancy Danger signs* 28% 50.3% 80%
Delivery/Labor Danger signs * 13% 30% 80%
Women danger signs after birth* 22% 33% 80%
Child danger signs after birth * 41% 26% 70%
Birth Plan Knowledge ** 8% 13% 70%
Women received at least 2 visitswhile pregnant
0% 54.7% 80%
Women received 2 visits after delivery
0% 32.6% 60%
*at least three danger signs mentioned ** at least three birth items mentioned
8
Improved Maternal and newborn Care practices
Indicator Baseline LQAS2 Target
Newborns that are initiated on breastfeeding in the first 24hours of birth
60% 96% 70%
Newborns who had nothing put on their Cord
17% 56.8% 47%
Newborns whose 1st bath is delayed beyond the first 24 hours
14% 14% 44%
Women with essential birth items
84% 95.6% 95%
9
Improved access to savings and transport support for MNH services
Indicator Baseline LQAS2 Target
Women Saving with groups 25% 33% --
Women Saving for MNH services 10% (was not captured) %
40%
Women accessed Money from the Saving groups
0% 7.7%*7.2%**
25%
Women used community organized transport
0 8.2% 20%
*Accessed money to pay for transport**Accessed money to pay medical bills
Maternal and Newborn Health Symposium 2014 4
EXPERIENCES
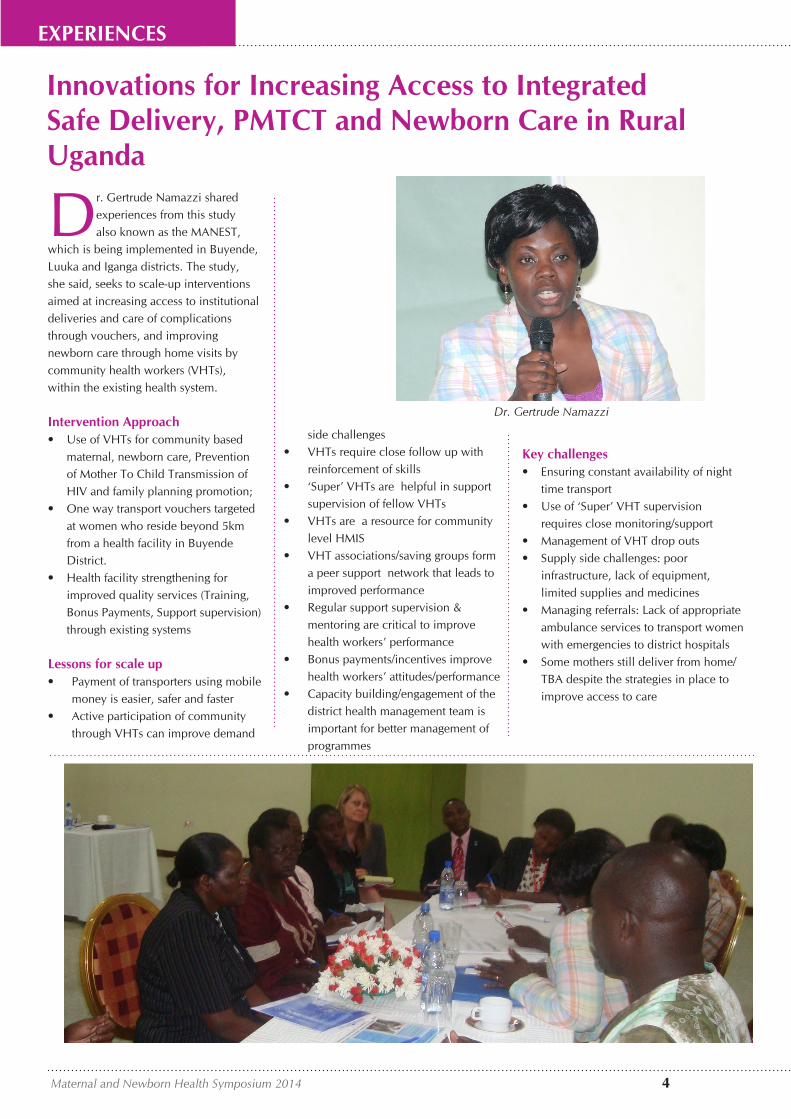
Dr. Gertrude Namazzi sharedexperiences from this study also known as the MANEST,
which is being implemented in Buyende, Luuka and Iganga districts. The study, she said, seeks to scale-up interventions aimed at increasing access to institutional deliveries and care of complications through vouchers, and improving newborn care through home visits by community health workers (VHTs), within the existing health system.
Intervention Approach• UseofVHTsforcommunitybased
maternal, newborn care, Preventionof Mother To Child Transmission ofHIV and family planning promotion;
• Onewaytransportvoucherstargetedat women who reside beyond 5kmfrom a health facility in BuyendeDistrict.
• Healthfacilitystrengtheningforimproved quality services (Training,Bonus Payments, Support supervision)through existing systems
Lessons for scale upPayment of transporters using mobile•money is easier, safer and fasterActive participation of community•through VHTs can improve demand
side challengesVHTs require close follow up with•reinforcement of skills‘Super’ VHTs are helpful in support•supervision of fellow VHTsVHTs are a resource for community•level HMISVHT associations/saving groups form•a peer support network that leads toimproved performanceRegular support supervision &•mentoring are critical to improvehealth workers’ performanceBonus payments/incentives improve•health workers’ attitudes/performanceCapacity building/engagement of the•district health management team isimportant for better management ofprogrammes
Innovations for Increasing Access to Integrated Safe Delivery, PMTCT and Newborn Care in Rural Uganda
Key challenges• Ensuringconstantavailabilityofnight
time transport• Useof‘Super’VHTsupervision
requires close monitoring/support• ManagementofVHTdropouts• Supplysidechallenges:poor
infrastructure, lack of equipment,limited supplies and medicines
• Managingreferrals:Lackofappropriateambulance services to transport womenwith emergencies to district hospitals
• Somemothersstilldeliverfromhome/TBA despite the strategies in place toimprove access to care
Dr. Gertrude Namazzi

Maternal and Newborn Health Symposium 2014 5
EXPERIENCES
While making her presentation, Dr. Monica Okuga said the main objective of this study conducted in Mayuge District was “to assess the feasibility, cost and community effectiveness of an innovative approach of expanded quality management using information power that links communities and health facilities to increase the quality and utilization of health care services in order to improve maternal and newborn health in rural Uganda.”
EQUIP was a two arm study which included:
• Quality Improvement (QI) where thekey intervention included the use ofPlan-Do-Study-Act cycles at 3 levels ofdistrict, health facility and community.
• Continuous surveys to collect highquality data in 3 rounds/year- 4 monthseach from household and healthfacility census
Lessons learnt• Engagingthedistricthealthteamto
lead with support from the project iscritical for successful implementation.
• Itisimportanttostrengthenlinkagesbetween VHTs and health workers.
• Itispossibletorapidlyintegratematernal newborn and child health intoexisting QI interventions within thedistrict
• QIishinderedbykeybottlenecksthatinclude drug stock outs and humanresource shortages
• IntegratingQIintotheactivitiesofVHTs is possible but this is hindered byunderstaffingatfacilitylevel.
Challenges during implementation
General:• Theapproachisdemandingintermsof
coordination• Adequatefinancialresourcesare
required for mentorship• Identifyingappropriatewaysto
motivate QI teams is a challenge
District level: • ToomanycompetingactivitiesmakingitdifficulttoimplementregularQImeetings
Health facility level:• Inadequateskilledstaff• Frequentstockoutsofdrugsand
supplies
Community level:• Slowuptakebecauseitwasanew
concept• Lowliteracylevels
“QI is very feasible at the 3 levels we have seen –district management, health facility and community level- and we need it at all these levels- Dr. Monica Okuga
Expanded Quality Management Using Information Power to Improve Maternal and Newborn Health
Study designIntervention Districts
ComparisonDistricts
HF
HFHFHF
HFHF
C
C
C
C
C
C
C
C
C
Cluster-based data collection: household and linked health
facility surveys for: Report cards
&Effect evaluation
Cluster-based data collection: household and linked health
facility surveys for:
Effect evaluation
EQUIP InterventionQuality management at
community, health facility, and district level empowered by
Report cards from cluster-based data+
Policy briefs
C
C: Community; HF: Health facility6/7/2014 8
EQUIP (Expanded Quality Management Using Information Power) is one of those projects that takes down the quality improvement approach from the conventional health facility district manager’s level to a very unconventional community level.
Dr. Monica Okuga
Maternal and Newborn Health Symposium 2014 6
PICTORIAL
A cross section of participants attending the Maternal and Newborn Health Symposium 2014

Maternal and Newborn Health Symposium 2014 7
PICTORIAL
A cross section of participants attending the Maternal and Newborn Health Symposium 2014

Maternal and Newborn Health Symposium 2014 8
EXPERIENCES
The FIGO (International Federation for Gynaecology and Obstetrics) Save the Mothers Project was conducted in the district of Kiboga from 1999-2004. It aimed at reducing maternal mortality and morbidity in the district by promoting the availability, access and utilization of emergency obstetric care (EOC) services for women.
It was conducted jointly by the Society of Obstetricians and Gynaecologists of Canada (SOGC) and the Association of Obstetricians and Gynaecologists of Uganda (AOGU), in collaboration with the district health team.
Dr Jolly Beyeza shared the experiences of implementation as indicated below:
The intervention entailed recruiting midwives, enhancing EOC skills of midwives & doctors, supportive supervision, provision of equipment & accountability, providing birth registers, community mobilisation, and emergency transport
Use of partnershipsThe use of partnerships enabled: • Solicitingsupportfromthepolitical
leaders.• DialoguewithLocalCouncils
to advocate for skilled birthattendance.
• Seekingsupportforemergencytransportation at community level.
ConstraintsThe project had a couple of challenges like lack of fuel for ambulances but abject poverty stood out because it affected the community’s use of skilled services. To try and minimize this problem, the project adapted Plan International’s Village Savings and Loan Association (VSLA) model. The main objective here was to establishemergencyfinancingforsafemotherhood at community level to reduce the delays to access emergency obstetric care (EMOC) using the VSLA) model of income generation.
How it was done• Savingsrange500Ushsto
2500Ushs (20 US cents to1.20USD) per week
• Welfarefundmandatorysavings200-500Ushs (5-20 US Cents) perweek
• Welfarefundforborrowingforhealth care with no service charge
• Provided100,000Ushs(50USD)asa startup capital revolving fund
Why VSLA?• Lackoffinancialresourcesusually
results in delay in access to qualitymaternal care. The major costs foraccess to care include transport,procurement of sundries for theclean delivery, “under the table”payments to health workers. Mostof the funds used are obtained fromfamily resources
• Ruralwomendonotaccessorcontrol family resources. It istherefore important to empowerwomen and communities to savemoney for emergency preparedness
Impact“Mothers are no longer dying because of lack of transport. There are no more cases of malnourished children, deaths in the area have generally reduced and so many things. Thank you to the initiators.” IDI woman, group 19
Assessment of 2013 by an MBA student
Dr Nakiwala Regina Stella shared how Health Partners Uganda, a nationally registered cooperative, is helping communities establish health cooperatives in Western Uganda. This, she said, is done by empowering groups and providers to develop partnerships that meet their health needs. Training, tools and technical support are also provided.
Why Cooperatives for Health?They [Coops] empower members to improve their health;offerfinancialsolutionstoincreaseaccessto care; are 100 percent sustainable by local partners and; do not need reinsurance or subsidies.
How do Health Coops work?• Groups sign MOUs with health providers• MemberspaypremiumsandgetIDcards• Memberspayasmallcopaywhentheygoforcare• Thereisrisksharing• Notallmembersfallsickatthesametime
Linking MNCH to CooperativesBetween 2008 and 2012 implemented a project of malaria communities program with funding from USAID. The focus was on helping pregnant women and children. The following success was registered.
The percentage of pregnant women using•long lasting insecticide treated nets (LLINs)increased from 5.5% to 51.9%The percentage of children under 5 using•LLINs increased from 6.5% to 42%
• Thepercentageofpregnantwomenseekingantenatal care increased from 16.2% to 31.3%
• Thepercentageofsickchildrenwhoreceivedmalaria treatment within 24 hours of onset offever increased from 1.1% to 29.5% 1.1% to29.5%
The FIGO Save the Mothers Initiative in Kiboga
Health Cooperatives: Increased Access to Care
Local Partnerships
Dr Jolly Beyeza
Dr Nakiwala Regina Stella

Maternal and Newborn Health Symposium 2014 9
KEY REACTIONS
“I would like to throw a challenge to Makerere and other institutions of higher learning. Why isn’t Government using your data? Could it be that perhaps some of the data that is coming out from these studies are things that Government is already doing? I will take the example of the quality improvement strategies. And I know that since the 90s the same exert strategies have been applied in Government health centres. Those who are as old as I am or perhaps older, might have heard of the yellow star program. The yellow star program has used these strategies at scale and many of them have been replicated elsewhere. So perhaps we need something new.We have also talked of improvement in hospital deliveries but that is not what will change maternal survival. What will change maternal survival is the coverage of skilled delivery, not delivery in a health unit. You have all seen hospitals, labour units manned by nursing assistants. Even if you get 500 hospital deliveries up from 5 in a month you are not making an impact because those deliveries are attended by an unskilled person. So as a university perhaps you can help us, these increases we are lauding in hospital deliveries, are they actual increases in skilled delivery? Do some analysis that will inform implementation of some maternal health strategies.”- Dr. Angela Akol - Country Director, FHI360
“These are very good innovations. This beingaveryhighpoweredscientificbodyof researchers you need to form partnership with advocacy groups. When I was at university we were never taught advocacy skills although we have some of them now. I think the ministry needs some other people to push it. I think I would have loved to have in this meeting the Uganda National Health Consumers Organisation and other advocacy groups so that we can advocate for fund allocation. And there are peoplewhocaninfluencehowtheministryof Health works. I would have liked the parliamentarians see some of these results
“What I learn from Dr. Beyeza’s presentation is that it was done long ago and we are now hearing of durable effects. The other presentations were looking at people still working intensively in the short term. We are not sure if they are building durable effects in the long term.
The question I would like to throw to the panel is, how are the things we are doing going look like 10 or 20 years down the road from now? Because, I think we have a lot of short term capital intensive efforts, which actually do not lead to long term. And we as academics are not interested in going back to look at what happened for the big push we had.
A pick of key reactions to the 5 presentations
so that when they are in their various groups in Parliament can help us to advocate and lobby for more funds.” - Dr. Anthony Mugasa -Consultant MoH
I think the issue is what can we do now that can lead to auto-pilot? In other words the things we leave in the system working. And I think right now we see that at community level there are some effects – things that can remain in auto pilot.
“The third point I want to make is that everybody is rushing to the community downstream to pilot things but no one is looking upstream to see what it takes to sustain those efforts. You are playing roles that should be played by upstream institutions during implementation. We are not looking at these institutions to see if they can provide that level of effort, level of funding, level of supervision, and level of design and babysitting the design? In other words, our research is missing a key aspect. We actually don’t look at upstream capacity to sustain downstream innovations. How can we improve on that?
As I end we are looking at universal coverage, how do we take these things from small islands of excellence so that the Uganda map looks a like?” - Dr. Freddie Ssengooba – Associate Professor at MakSPH
Dr. Freddie Ssengooba
Dr. Anthony Mugasa
Dr. Angela Akol

Maternal and Newborn Health Symposium 2014 10
Group 1: Mobilizing and sensitizing communities: Using VHT’s and community meetings
Strategies for sustaining the use of VHTs • Trainingandstrengtheninghealthunit
management committees that would help in strengthening the linkage between the VHTs and the Health workers
• OrganizingVHTsingroupsandstrengtheningthese groups through trainings in income generating activities for example by giving them seed grants, linking them to other partners,
• PuttinginplaceaplatformforVHTstosharesuccess stories
• AttachVHTstothehealthfacilitieswherethey can be supervised by health workers
• RecognitionofVHTsatvariouslevels-forexample at the health facilities, the health workers should make sure VHTs receive Health services without any disturbances
• OrganizeinteractivegroupdiscussionswhereVHTs performance and success/challenges can be shared
Thematic Sessions In order to improve ongoing studies and interventions, MakSPH put to participants 3 thematic questions and below are the views from the three groups:
Strategies for improving community dialogue meetings
1. Strengthen the relationship between local leaders and VHTs. Local leaders like LC 1 chairperson play a key role in mobilizing people to attend community meetings
2. Utilize dance and drama as one way of mobilizing and sensitizing the community-this is because the community is more interested in watching rather than listening to
messages. For example the community canbeinterestedinwatchingfilms,games, and traditional wrestling.
3. There is need to utilize other community days like market days, as one way of reaching a larger group of people.
4. There is need to target areas where more people gather for example Trading Centers, Facilities during ANC days, Outreaches like Immunization, e.t.c.
Group 2: Increasing financial access and transport for maternal and newborn health services
How to improve access to transport services using public and private transport systems
Public transport system • Efficientmotorisedtransportisrequiredfor
transporting mothers who have emergencies. Therefore the Ministry of health and districts should continuously lobby for ambulances at the different referral levels through politicians (MP), donors, increased allocation to the health sector, among others. Districts should have a reserve fund for fuel •for the ambulance. This could be provided through community credit schemes, district allocations etc. Drivers for facility ambulances should also reside at the health facility. Improvedfleetmanagementforpublic•ambulances is recommended e.g. vehicle maintenance, close supervision and
monitoring of vehicle use, and recruitingqualifieddrivers.Communication between lower •levels and upper levels of referral should be improved
.Local transport systems
Work with associations of •transporters if they exist.Sign agreements that clearly •indicate the duties of the transporters and terms of payment
if a third party will be responsible for payment in order to minimise confusion. Separate payment rates for the night and the day should be agreed upon, since the rates are higher at night. Provide basic training so that •transporters know what to do in case a mother delivers enroute to the health facilitiesPlan for communication between •
DISCUSSIONS

Maternal and Newborn Health Symposium 2014 11
Group 3: Improving the quality of maternal and newborn health services
Good practices in support supervision and mentoring of health workers• Trainingleadershipatvariouslevels
(i.e. District Health Team, Health Sub -
District, and Health units)
• Trainingsshouldbeonsite,continuous
and part of continuing medical
education. The participants should be
able to practice on site.
• Usechampionswithinaunit.Ahealth
unit team secretary can document the
trainings and identify areas that need
training.
• Thechampionsshouldbemanagers.
This is because in some institutions if
the top management is not on board
there is usually no response.
• Thechampionsincludingmanagers
should create demand for services and
improve the quality of services.
Improving referral of patients from lower level to higher-level facilities• Somedistrictshavesetupreferral
protocols at the health units.
• :Thehigherlevelfacilitiesshouldgive
feedback to the referring facilities to
complete the loop.
• Improvedocumentationbyusing
referral notes
• Providecommunicationgadgets
and networking facilities
• Healthworkersshouldescort
seriously ill patients
• Somecostsharingshouldbe
introduced for sustainability.
DISCUSSIONS
the transporters and the community. This may include the use of mobile phones or even word of mouth Plan how to increase access to•the transport services by posting telephone numbers of transporters on the facility walls, giving VHT’s the numbers of transporters etc Payment of transporters may be done•by a third party group in order to ensure cash is available when it is needed; therefore links with a local accessiblefinancialnetworkthatcanplay this role may be important.Locally existing groups such as VHT’s•andotherfinancialsocialnetworkscan purchase their own motorbike that can be used to provide emergency transport free or at subsidized rates. Such motorbikes can also be used to generate extra income for the groupMultisectoral action to ensure the•roads are in good condition is requiredWhere the number of transporters•are inadequate it will be necessary to identify innovative ways of attracting people to provide transport services Mapping of the area is necessary to•understand areas that have transport constraints.
The local community should be•involved in the management ofthe transport system to ensuresustainabilityA monitoring and evaluation•system is important for tracking useof the system and its effectiveness,accidents, etc.
Challenges that may be encountered Lack of associations•Getting buy in from local transporters•to provide transport services undersuch a systemOver charging third party payers•Safety at night•Multiple visits incase of false labour•Record keeping•
Good practices for working with Saving/Financial networks
The groups should use multiple•channels for mobilizing funds. These may include:
a. Promoting involvement inincome generating activities by partnering with different groups that exist within the community, and encouraging them to add a component that allows the group to help mothers save money for
maternal and newborn healthb. Lobbying politicians (MPs and
aspiring candidates) and well wishers to contribute money to such schemes
Use locally existing saving groups or•financialnetworksthataretrustedbythe local community e.g. VSLA, small local saving groups, circles, health cooperativesEnsure good management to minimise•losses/embezzlement through the following:Traintheleadersinfinancial1.managementChoose trusted local leaders2.Encouragegoodfinancialpractices3.e.g. checks and balances, bankingbig sums of money etcTransparency through sharing4.information during meetingsUse existing government5.structures to supervise andregister groupsPut in place measures for dealing6.with misuse of fundsEncourage groups to have7.constitutions and to follow them
Maternal and Newborn Health Symposium 2014 12
Acknowledgments
Special thanks go out to our sponsors Comic Relief, UKaid through the Future Health Systems Research Consortium, the World Health Organisation, and the European Union.
We also thank HealthPartners Uganda and Dr Jolly Beyeza for accepting to join the symposium with interesting presentations.
Special thanks also go out to all those who managed to attend the symposium.
And with the industrious efforts of the organizing committee of (Mr. Kakaire Ayub Kirunda, Mrs. Josephine Adikini Oketch, Mr. Moses Tetui, Dr. Elizabeth Ekirapa – Kiracho, Ms Stella Kakeeto, and Mr. David Mutibwa) we were able to hold thesymposium.
This report was compiled by Mr. Kakaire Ayub Kirunda and designed by Mr. Vincent Akumu
Makerere University College of Health Sciences| School of Public Health |MakSPH Building| New Mulago Hospital Complex| Kampala, Uganda
For any comments and questions, send mail to [email protected]
WRAP UP PLENARY: CLOSING REMARKS“Most of our mothers die at the time of delivery and post delivery period. If you work at that level, you save a lot of lives and I thank these projects for trying to work around that period. We learn those best practices from these projects and scale them up.
Our out of pocket expenditure on reproductive health is high. So we are coming up with a National health insurance scheme. So we shall pull together resources and deliver quality health services. We want to harness improvements in delivery through insurance.
Regarding referral, together with our development partners, we have purchased ambulances. They are there but in different
functional states. Some are on stones, some are lacking a tyre, some are lacking fuel, and others are working where community mobilisation has taken place like Yumbe. The community took over those ambulances and they are working. So other districts should learn from Yumbe.
But we are also not sitting down. We are developing guidelines to see how efficientlythesecanbemanaged.
Definitelyfacilitieshavefailedtomanagethem because we have also failed to give them the means. They should have their own vote and be managed moreefficiently.Butweneedtoconsultwidely to see how we can improve the management of these ambulances.”-Dr. Collins Tusingwire – Asst. Commissioner for RH at MoH
Dr. Collins Tusingwire
Note: Look out soon for the entire audio recording of the symposium on the You Tube channel Maternal & Newborn Health @MakSPH
1
secivreS htlaeH erutuFehtrof
POLICY BRIEF No.1, October 2011www.futurehealthsystems.org
IMPROVING SKILLED DELIVERIES THROUGH VOUCHERS: Implications For Policy
BACKGROUNDMillennium Development Goal (MDG) No.5 is to reduce maternal mortality by 75percent. In Uganda the maternal mortalityhas reduced to 435 per 100,000 live birthsover the ten years preceding the 2005survey. There is evidence to show thatattendance of delivery by skilled healthpersonnel reduces maternal mortality, bututilization of maternal health services haspersistently remained low with only 47percent of women attending 4 AntenatalCare visits, 41.1 percent delivering inhealth facilities and 23 percent receivingpostnatal care.
The literature shows that the main reasonsfor not delivering in a health facility includefinancial limitations, long distances tohealth facilities coupled with lack of accessto transport facilities, lack of decisionmaking power among women, preferencefor traditional child birth practises andsettings and poor quality of care reflectedin the frequent shortages of drugs andsupplies as well as the poor attitude ofhealth workers who are underpaid andoverworked.
Most interventions implemented by thegovernment of Uganda and otherstakeholders address the supply sideconstraints but not the demand sideconstraints. Recent literature suggests thatdemand side financing may have thepotential to increase access of targetedservices to vulnerable groups such aspregnant women, however evidence aboutthe use of demand side financing in subSaharan Africa is still limited.
INTERVENTION
Against this backdrop, the SafeDeliveries Study project team under theFuture Health Systems ResearchConsortium and the MakerereUniversity John Hopkins UniversityTwining Programme have beenimplementing an intervention thatcomprises both demand (vouchers fortransport and maternal services) andsupply side initiatives (training healthworkers and provision of essentialequipment, drugs and supplies) togenerate evidence that can contributeto reducing maternal mortality andinform the designing andimplementation of similar schemes.
The vouchers facilitate access tomaternal health services by reducingthe cost of transport and improving theprovision of services by contributing toimprovements in the availability ofskilled motivated health workers andavailability of the required supplies andequipment. This intervention waspiloted in Budiope Health Sub District(Now Buyende district) between Dec2009 and March 2010.
The intervention was then implementedusing a quasi experimental design fromJune 2010 in Buyende and Pallisadistricts (intervention districts) andKamuli and Kibuku districts (controldistricts). The intervention will becompleted in December 2011.
Policy PointersCommunities could beeconomically empoweredso that they can contributeto the financing of healthservices through voucherschemes that targetmaternal health services.
Remuneration of healthworkers needs to beincreased, to reducepractises such asabsenteeism and “under thetable payments” to healthworkers.
Health facilities must beequipped with adequateessential items such asequipment, sundries, drugs,protective gear andstationary if they are todeliver quality services.
Photo: A new mother isintroduced to visitingresearchers at Kamuge HealthCentre in Pallisa District
Future Health Systems Uganda
MATERNALAND NEONATALIMPLEMENTATION FOREQUITABLE SYSTEMS(MANIFEST)
LEARNING QUESTIONSThe following questions are being used to guide the research process:
Do the community mobilisation and empowerment 1.strategies (use of community health workers, community dialogue meetings, media, and linkage with financial networks) lead to increased birth preparedness?Does improving availability of transport services by 2.promoting linkages with commercial transporters and increasing financial preparedness lead to increased access to transport services for maternal and newborn services?Does providing a package of training; supportive 3.supervision and mentorship improve the quality of maternal and newborn health services?
If the answers to these learning questions are in the affirmative, this study will go a long way in emphasizing the need to seek community solutions to solvecommunity problems in the area of maternal and newborn health. Our evidence will further emphasize the increasingly popular paradigm -in development circles- of the need to include local communities in planning for their wellbeing in moving towards a more sustainable future.
Seeking Sustainable Maternal & Child HealthInterventions for Uganda
Background
Future Health Systems (FHS) is a research consortium working to improve access, affordability and quality of health services for the poor and socially marginalised groups. We are a partnership of leading research institutes from across the globe working in a variety of contexts: in low-income countries (Bangladesh, Uganda), middle-income countries (China, India) and fragile states (Afghanistan) to build resilient health systems for the future. After a successful first phase from 2006-2011, we are now in a new six-year phase of research, funded mainly by the UK Department of International Development (DFID).
Consortium-wide research questions
1. Unlocking community capabilities:How can the wide range of resources available at the community be systematically identified and used to improve the quality and impact of health services, particularly for disadvantaged groups?
2. Stimulating Innovations: How can new technologies and organisational innovations be used to improve the quality, coverage and affordability of healthcare in resource-poor settings?
3. Learning by doing in complex adaptive systems: How can models for systematic learning-by-doing be best used by providers, beneficiaries, officials and key local actors to improve the delivery of health services in complex and dynamic settings?
FHS Uganda Focus
The FHS Uganda team is undertaking several activities to generate not only transformative, informative research but also to build the capacity of young researchers at Makerere University School of Public Health.
Contact Us:Dr. Elizabeth Ekirapa - Kiracho, Team Leader
MANIFEST,Tel: +256 772 408 134,
Email: [email protected]
Mr. Moses Tetui, Study CoordinatorMANIFEST
Tel: +256 392 840 142 Email: [email protected]
Dr. Godfrey Mulekwa District Health Officer, Pallisa District
Tel: +256 772 452 479 Email: [email protected]
Dr. Dinah NakigandaDistrict Health Officer Kamuli District
Tel: +256 702 677 192 Email: [email protected]
Dr. Bumba AhmedAg. District Health Officer, Kibuku District
Tel: +256 701 147 720 Email: [email protected]
OUR PARTNERSComic Relief: The funders of the study
Future Health Systems: The FHS consortium funded bythe UK Department for International Development is providing technical support to the study.
managerial skills. Others are improving support supervision and mentoring of health workers to ensure continued growth of health workers and recognizing outstanding health workers through newspaper articles, provision of basic equipment and health symposia as a way of motivating them.
Throughout our study period, stakeholder engagements at different levels shall be encouraged as a way of fostering linkages, sustainability and scale up of the intervention.
MAN I F EST
!"#$%&'()*+,-.'/'0
,1
2)-%.