MADHYA PRADESH HEALTH SECTOR REFORM PROGRAMME Programme Memorandum Government of ... · ·...
27
1 Flag A MADHYA PRADESH HEALTH SECTOR REFORM PROGRAMME Programme Memorandum Government of Madhya Pradesh Government of India DFID, UK May 2007
Transcript of MADHYA PRADESH HEALTH SECTOR REFORM PROGRAMME Programme Memorandum Government of ... · ·...

1
Flag A
MADHYA PRADESH
HEALTH SECTOR REFORM PROGRAMME
Programme Memorandum
Government of Madhya Pradesh
Government of India
DFID, UK
May 2007

2
Table of Contents
Abbreviations and Acronyms
1. Summary
2. Project Details
2.1 Programme Description
2.2 Programme Appraisal
2.3 Lessons and Evaluation
3. Implementation
3.1 Management arrangements
3.2 Timing
3.3 Funding
3.4 Contracting and Procurement
3.5 Accounting and Audit
3.6 Monitoring and Reporting
4. Risks
5. Conditionality
Annex 1: Madhya Pradesh Health Sector Reform Strategy
Annex 2: Policy Milestones Matrix
Annex 3: Consultation record
Annex 4: Fiduciary risk assessment
Annex 5: Procurement Reform Plan
Annex 6: Project Header Sheet
Annex 7: Innovative practices in health introduced by the GoMP
Annexes on Economic, Social, Institutional and Political Appraisals are available on
request, as is the Medium Term Expenditure Framework.

3
Abbreviations and Acronyms
ANM Auxiliary Nurse Midwife
AWW Anganwadi Worker
ASHA Accredited Social Health Activists
BCC Behaviour Change Communication
BJP Bharatiya Janata Party
CAP Country Assistance Plan
CBP Capacity Building Plan
CHC Community Health Centre
CSSs Centrally Sponsored Schemes
CM Chief Minister
DEA Department of Economic Affairs
DFID Department for International Development (UK)
DWCD Department of Women and Child Development
EAG Empowered Action Group (referring to the states with the poorest social
indicators)
EC European Community
GoMP Government of Madhya Pradesh
GoI Government of India
GSDP Gross State Domestic Product
HMIS Health Management Information System
HRM/D Human Resource Management/Development
HSRS Health Sector Reform Strategy
HSS Health Sector Strategy
IMEP Infection Management and Environment Plan
JBIC Japanese Bank for International Cooperation
MPHSRP Madhya Pradesh Health Sector Reform Strategy
MTEF Medium Term Expenditure Framework
MDG Millennium Development Goals
M&E Monitoring and evaluation
MoF Ministry of Finance
MMR Maternal Mortality Rate (or Ratio)
MP Madhya Pradesh
4
NACP 3 National AIDS Control Programme Phase 3
NFHS National Family and Health Survey
NRHM National Rural Health Mission
PHC Primary Health Care (or Centre)
PHED Public Health Engineering Department
PPP Public Private Partnerships
PH&FWD Public Health and Family Welfare Department
PRD Panchayati Raj Department
PRI Panchayati Raj Institutions
RCH Reproductive and Child Health
RKS Rogi Kalyan Samiti (Patients Welfare Society)
SRS Sample Registration System
SWAp Sector-wide approach
TA Technical Assistance
TFR Total Fertility Rate
VAT Value Added Tax

5
1. Summary
1.1. Madhya Pradesh (MP) is one of the poorest states in India with over 37% of its
total population of 60 million living below the poverty line. Scheduled Castes (SCs)
and Scheduled Tribes (STs), two of the most marginalised groups, constitute 35% of
the population and account for 60% of the poor. Gender-based discrimination is
reflected in the unequal sex ratio (916/1,000) against an already worrying national
average of 933/1,000 in 20011) and lower human development indicators for women.
Despite progress in recent years, MP still has among the highest rates of maternal and
infant mortality of all states in India. Total fertility rate and incidence of vector-borne
and communicable diseases are also much higher than average. Recently published
national statistics (National Family Health Survey (NFHS 3) indicated that MP had
the highest rates of under nourishment in children under 3 years (60%) in the country.
1.2. DFID has been working in MP since early 2000 and has a diverse portfolio of
programmes. DFID started working in the health sector in MP in 2004 through the
District Health Management and Sector Reform Programme (2004 – 2006). A recent
evaluation of this programme indicated that it has led to a number of gains including
encouraging innovative practices such as the Janani Express (emergency transport
scheme for expecting mothers) and the Completely Observed Meal Programme
(COMP) for pregnant women; promoting decentralised planning of resources and
closer working with other government departments and schemes.
1.3. This earlier project also led to the development of a comprehensive Health Sector
Strategy (Annex 1) for the Health Department, covering a period of 5 years, starting
from 2007. The main objectives of this strategy are reduction in: infant mortality,
maternal mortality, total fertility rate, making health outcomes and utilisation of
services more equitable, addressing malnutrition among children and reducing
morbidity and mortality from common communicable diseases such as malaria,
leprosy and tuberculosis.
1.4. The Madhya Pradesh Health Sector Reform Programme (MPHSRP) will support
six key elements of this reform strategy: improving equitable access to quality public
1 Indian census 2001

6
healthcare services, accountability of staff, organisational development and human
resource management, adequacy of financial allocation and effectiveness of
expenditure, participation and regulation of the private sector and integrated service
delivery to reduce malnutrition. Progress milestones for each area, agreed with the
GoMP are at Annex 2.
1.5. The performance of the public health delivery system in MP faces several
constraints: vacancies of staff and infrastructure gaps, particularly in the poorest 10
districts and tribal areas; lack of drugs and other essential supplies at local levels;
weak implementation and monitoring systems; poor accountability of staff and low
staff motivation and management capacity. The poor quality and low funding of the
public health system has resulted in the growth of an unregulated and poor quality
private sector. For poor households, use of the private sector has led to high out-of-
pocket expenditures (often pushing people further into poverty).
1.6. The GoMP has taken a number of steps in the recent past to improve the
functioning of the health system and facilities, which have been recognised by the
Government of India’s (GoI’s) central line ministry, the Ministry of Health and
Family Welfare (MoHFW). MP has set the example for other Indian states in
promoting decentralised planning under MoHFW’s flagship programme, the National
Rural Health Mission (NRHM). MP has already signed a memorandum of
understanding (MoU) with the GoI, committing itself to: increasing public
expenditure on health, increased decentralization and community participation,
providing funding for community level health workers and granting functional
autonomy to local health facilities. MPHSRP will enable GoMP to meet some of
these critical commitments by reducing the resource gap.
1.7. It is proposed that a total of up to £60 million be provided to GoMP as sector
poverty reduction budget support (PRBS), including £56 million in financial aid and
£4 million as technical cooperation (TC) funds. The support (which amounts to 7%
of the state health budget) will be made available over five years starting in 2007/8.
This will help GoMP to undertake a series of critical measures such as upgrading the
health infrastructure, particularly in the 10 poor districts and tribal areas, increasing
the supply of essential drugs, augmenting staff resources, building staff capacity and

7
financing innovative schemes such as vouchers for emergency transport and other
schemes for the poorest groups, encouraging public private partnerships, introducing
health insurance for the poor, establishing Auxiliary Nurse Midwife (ANM) schools
in tribal areas and developing Anganwadi’s (village nutrition centres) into Village
Health Centres.
1.8. The first annual tranche will be of £ 6 million to be disbursed in 2007-08;
subsequent annual disbursements will be in the range of £ 10 m - £ 12.5 m and based
on the projected financial need against the agreed milestones for the coming year. In
order to absorb any likely future adjustments in resources available to the programme,
we propose that 80% of each annual tranche be designated as core and 20% as
indicative. The core and indicative components of DFIDI’s disbursements for the
coming years will be communicated to GoMP by November in the preceding year, in
time for the state budget session. The tranches will be disbursed as follows:
2007 – 08 £ 6.0 million
2008 – 09 £ 12.5 million
2009 – 10 £ 12.5 million
2010 – 11 £ 12.5 million
2011 – 12 £ 12.5 million
1.9. GoMP has committed to a minimum of 10% year on year increase in public
expenditure on health until 2012. This would be supplemented further by support
from GoI programmes and other donor support. The Medium Term Expenditure
Framework (MTEF), recently finalised by the state, forecast a resource requirement of
£9262 million over the next five years to implement the health sector strategy. DFID’s
contribution to this will be approximately 5.5%.
1.10. The goal of MPHSRP is to improve the health status of people in Madhya
Pradesh – especially the poorest. The purpose is “increased use of quality health
services, especially by the poorest people and in underserved areas”. The purpose of
the project is consistent with DFID India’s Country Assistance Plan (CAP), the Asia
2 £926 million includes the State’s funds plus those received from Government of India for centrally sponsored schemes in health

8
Director’s Delivery Plan and with Public Service Agreement (PSA) objective 2. It
forms an important part of DFID’s strategy to meet the health and gender related
MDGs in India. The programme will also complement DFID’s existing work in MP
on public sector reform, rural and urban livelihoods.
1.11. We judge that the MPHSRP is a well-conceived and realistic plan for health
sector reform in MP. DFID support in the form of untied budget support provides
much needed flexibility to deploy resources across the health sector thereby
increasing the effectiveness of overall public health spending, including particularly
central schemes such as Reproductive and Child Health Phase 2 (RCH2), and
ensuring greater allocation of resources for poorer districts and populations. Expected
outcomes include: reduction in maternal mortality from 379 to 220 per 100, 000 live
births and of infant mortality from 70 to 60 per 1000 live births; increased
institutional deliveries from 30 to 75%; increased childhood immunisation coverage
from 40 to 75%; reduction in total fertility rates from 3.1 to 2.1; reduction in under
nutrition rates in children under 3 years from 60% to 35%; and reduction in the
burden of communicable diseases, particularly malaria, TB and HIV.
1.12. The programme is rated as medium risk, with potential high impact. Key risks
include: weak planning and implementation capacity, non availability of critical
medical staff particularly for remote areas, staff resistance to change, lack of political
commitment, and medium fiduciary risk. We judge that these risks are manageable
due to: presence of strong political and bureaucratic commitment to health reforms,
realistic GoMP plans for strengthened financial systems and capacity building, and
agreed actions from a Fiduciary Risk Assessment (FRA). The potential returns of this
intervention are also high, in terms of enhanced outcomes for some of India’s most
vulnerable people.
2. Programme Details
2.1. Programme Description and Approach
2.1.1. The goal of the MPHSRP is to improve the health status of people in MP,
especially the poor and the underserved, and thereby accelerate the state’s progress
towards the MDGs. The purpose is to increase use of quality health services

9
especially by the poorest people and in underserved areas. The MPHSRP has been
jointly designed by GoMP and DFID.
Problems to be addressed
2.1.2. Health and poverty indicators in MP are amongst the worst in India. 37% of the
population of 60 million people are below the poverty line. MP has the second
highest infant mortality rate of all states in India of 70 deaths per 1000 live births.
Maternal mortality is 379/100,000 live births compared to the national average of
300/100,000; 60% of children under 3 years are undernourished compared to the
national figure of 46%. The health outcomes of SC/ST populations and girls/women
are worse than those for other groups. MP is currently off track on the maternal and
child mortality MDGs.
Table 1: Health Outcomes: Madhya Pradesh in Comparative Perspective
Maternal
Mortality (per
100,000)
Infant Mortality
(per 1,000)
% of
Institutional
Deliveries
Undernourished
children under 3
All India 300 57 41 46
Madhya Pradesh 379 70 30 60
Maharashtra3 149 38 66 40
Kerala 110 14 100 29
Source: SRS/NFHS III data
2.1.3. Regional and social disparities within the state are striking. The rural infant
mortality rate (IMR) is 80 per 1000 live births, compared to 54 per 1000 in urban
areas and figures for SCs and STs are much worse (NFHS-2). The tribal areas
concentrated in the south east and south west, have worse indicators due to
remoteness and lack of access to medical facilities. Table 2 sets out health indicators
for specific population groups.
Table 2: Health Indicators for specific population groups (number of cases per
1000 live births
Background characteristic Neonatal
mortality
Infant
mortality
Child
mortality
Under five
mortality
3 Maharashtra is a medium performing state and Kerala is the best performing state in India, on health indicators.
10
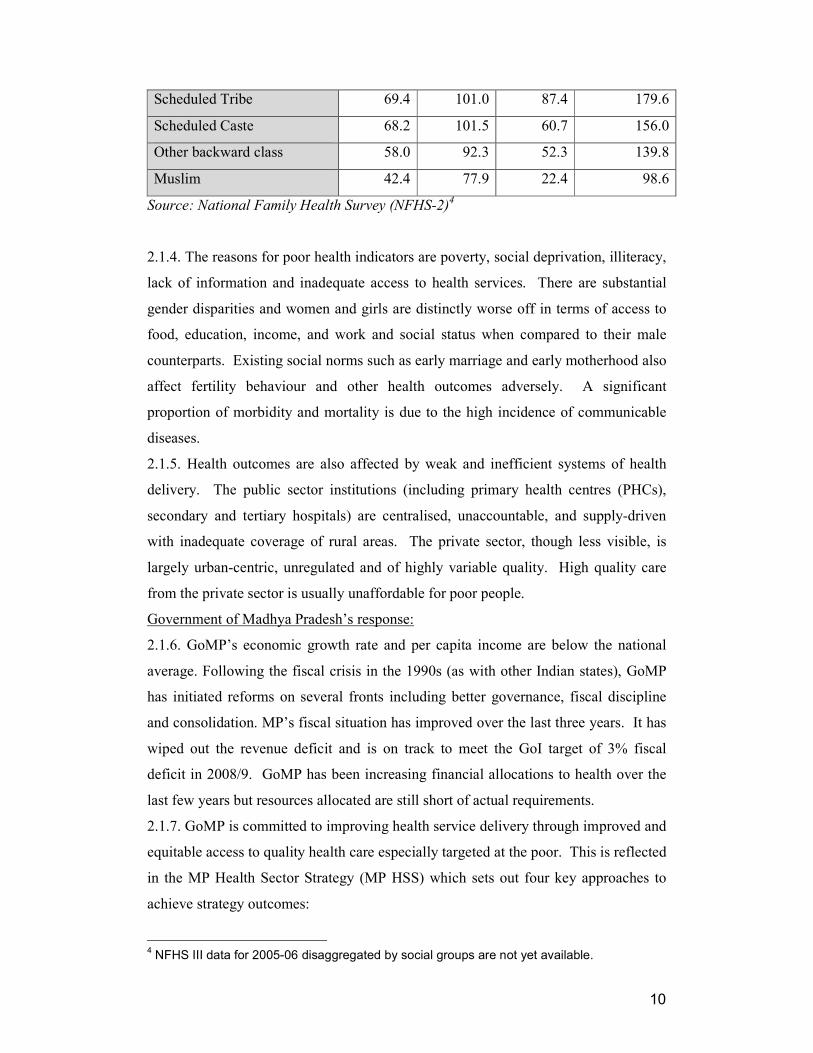
Scheduled Tribe 69.4 101.0 87.4 179.6
Scheduled Caste 68.2 101.5 60.7 156.0
Other backward class 58.0 92.3 52.3 139.8
Muslim 42.4 77.9 22.4 98.6
Source: National Family Health Survey (NFHS-2)4
2.1.4. The reasons for poor health indicators are poverty, social deprivation, illiteracy,
lack of information and inadequate access to health services. There are substantial
gender disparities and women and girls are distinctly worse off in terms of access to
food, education, income, and work and social status when compared to their male
counterparts. Existing social norms such as early marriage and early motherhood also
affect fertility behaviour and other health outcomes adversely. A significant
proportion of morbidity and mortality is due to the high incidence of communicable
diseases.
2.1.5. Health outcomes are also affected by weak and inefficient systems of health
delivery. The public sector institutions (including primary health centres (PHCs),
secondary and tertiary hospitals) are centralised, unaccountable, and supply-driven
with inadequate coverage of rural areas. The private sector, though less visible, is
largely urban-centric, unregulated and of highly variable quality. High quality care
from the private sector is usually unaffordable for poor people.
Government of Madhya Pradesh’s response:
2.1.6. GoMP’s economic growth rate and per capita income are below the national
average. Following the fiscal crisis in the 1990s (as with other Indian states), GoMP
has initiated reforms on several fronts including better governance, fiscal discipline
and consolidation. MP’s fiscal situation has improved over the last three years. It has
wiped out the revenue deficit and is on track to meet the GoI target of 3% fiscal
deficit in 2008/9. GoMP has been increasing financial allocations to health over the
last few years but resources allocated are still short of actual requirements.
2.1.7. GoMP is committed to improving health service delivery through improved and
equitable access to quality health care especially targeted at the poor. This is reflected
in the MP Health Sector Strategy (MP HSS) which sets out four key approaches to
achieve strategy outcomes:
4 NFHS III data for 2005-06 disaggregated by social groups are not yet available.

11
• Programmatic – choice of basic package with focus on needs of the poor
and vulnerable, provision of physical infrastructure and drugs, especially
in poorer regions, effective referral system, approaches to resource
allocation, communication strategies, and contracting for service
provision.
• Governance – Changing institutional arrangements (decentralization,
community participation, hospital autonomy, public private mix) to
improve responsiveness and accountability, improved capabilities for
policy making, planning, financial management and procurement, health
information systems, convergence with other determinants of health, and
stewardship of the private sector.
• Organisational – Reorganising of health services at the state and field
level, skill-mix and skill upgrading, human resource development,
adequacy of manpower.
• Health Financing - raising public expenditure on health, reducing
financial barriers to accessing basic health services, risk pooling
mechanisms for the poor and better targeting of resources.
2.1.8. MP was one of the first states to give limited financial autonomy to hospitals by
permitting them to retain user fees. The money thus collected is used by the Rogi
Kalyan Samiti (RKS – ‘patient welfare society’), which includes the senior medical
officials and local representatives, for better maintenance of facilities.
DFID Approach and Use of Resources:
2.1.9. To support GoMP in this programme of reforms, DFID will focus financial and
technical support on six priority outputs of GoMP’s health strategy:
i) Equitable access to quality public healthcare services improved
2.1.10. GoMP will ensure that the infrastructure and staffing requirements are met to
agreed standards, especially in 10 of the poorest districts and tribal blocks. GoMP has
initiated innovative approaches to recruit local talent to resource health centres and is
considering incentive mechanisms to retain talent. ANM training schools will be
established in tribal areas to encourage recruitment of tribal women into the ANM
cadre, with innovative financing mechanisms to attract participation of tribal
communities in this process. Support to participatory planning for health and related

12
services, will lead to more appropriate and responsive service delivery. A
comprehensive monitoring and evaluation system will be established with
disaggregated data to track progress of the reforms, particularly in remote areas and
groups such as the SCs and STs.
2.1.11. Financial barriers to accessing health services have been identified as a major
constraint in MP. GoMP plans to test out ways to provide financial protection to the
poor to cover their large out-of-pocket expenses. DFID will work with GoMP to find
ways of supporting this.
ii) Accountability of health services improved
2.1.12. Systems will be developed for health service planning and monitoring,
together with mechanisms to make services more accountable to the population
groups they serve. Health committees will be set up at village, block and district
levels to ensure increased local ownership and accountability. Special efforts will be
made to ensure representation of the poorest groups and women in these committees.
GoMP will provide capacity building support to these health committees.
iii) Organisational development & human resource management systems
strengthened
2.1.13. A Strategic Planning Cell will be established within GoMP’s Department of
Public Health & Family Welfare. Human resource management systems (HRM) will
be strengthened through activities such as establishing a comprehensive database of
existing staff, institutionalising a transparent staff transfer and posting policy and
undertaking a cadre review. GoMP will also implement detailed reforms on
procurement and other issues as outlined in the Fiduciary Risk Assessment (FRA) risk
mitigation plan.
iv) Adequacy of financial allocation and effectiveness of expenditure
improved
2.1.14. Improved financial management systems will be developed to ensure
alignment of actual spend with budgeted expenditure, to keep the focus of spend as
planned on primary and secondary care, and to develop and implement criteria and
mechanisms to target resources to remote and under-served areas. The districts will
be mapped based on a composite health index (CHI) and the worst performing 10
districts will be selected for special focus for the next five years.
v) Participation and regulation of private providers in achieving public
health goals

13
2.1.15. Dependence on the private sector for both minor and major ailments is high in
MP, particularly in rural areas. GoMP will focus on strengthening the regulation and
quality of services provided by the private sector, and will enhance the role of elected
local bodies in monitoring and holding providers to account for delivering better
quality services to the poor. The existing pilots for public-private partnerships (PPP)
in emergency transport and other services will be expanded to other areas. A PPP Cell
will be established within the Public Health and Family Welfare Department
(PH&FWD) to act as a focal point for managing PPPs.
vi) Integrated service delivery to reduce malnutrition and improve child
health.
2.1.16. GoMP will strengthen working between the Department of Women and Child
Development (DWCD), PH&FWD and the Panchayati Raj Department (PRD) at all
levels. DFID will provide technical assistance to DWCD to upgrade skills of, and
establish career progression for, Anganwadi Workers (AWW – village nutrition
workers) to develop into Auxiliary Nurse Midwives (ANMs). A Monitoring and
Evaluation System will also be set up. During the first year, GoMP will develop a
three year Action Plan based on its recently published state nutrition policy including
a Medium Term Expenditure Framework. Based on the outcome of these plans, DFID
will consider broadening the scope of our investment programme to cover DWCD
from the second year onwards.
Beneficiaries:
2.1.17. The programme will directly benefit the entire population of 60 million people
in MP, but in particular the 23 million poor and disadvantaged who suffer the greatest
burden of ill health. There will be a special focus on improving the health outcomes
for population groups located in the 10 poorest districts, and for scheduled castes and
tribes whose health outcomes are the worst.
2.2. Programme/Technical Appraisal
Background
2.2.1. Over the last few years, GoMP has taken a number of steps to improve the
functioning of the health system and facilities, which have been recognised by
Government of India’s (GoI’s) central line ministry, the Ministry of Health and
Family Welfare (MoHFW). MP has set the example for other Indian states in
promoting decentralised planning under MoHFW’s flagship programme covered
under the National Rural Health Mission (NRHM). MP has already signed a

14
memorandum of understanding (MoU) with the GoI, committing itself to: increasing
public expenditure on health, increased decentralization and community participation,
training and funding community level health workers (ASHAs). This programme will
support GoMP to deliver these targets.
Fit with Government of India (GoI) policy
2.2.2. The reform strategy of MPHSRP is closely aligned with the key directions of
the Government of India’s National Rural Health Mission (NRHM) and the National
Health Policy. This includes increased public funding for the health sector,
decentralised village and district level planning involving Panchayati Raj Institutions,
convergence of vertical health programmes, and a stronger focus on equity in resource
allocation for health.
2.2.3. HIV prevalence in MP is currently low, but there is risk of greater transmission
of the virus. MPHSRP will help MP to implement the framework set by GoI’s
National AIDS Control Programme Phase 3 (NACP3) which is supported by DFID at
the national level and implemented through the MP State AIDS Control Society. In
particular, the MPHSRP will support MP to strengthen linkages between NACP3 and
broader health services, for example through provision of HIV testing for people with
TB, provision of treatment for sexually transmitted infections, and promotion of HIV
behaviour change counselling and HIV testing through health services.
Fit with DFID policy
2.2.4. This programme is consistent with DFID India’s CAP and contributes towards
meeting health and gender-related MDGs in India and DFID PSA objectives. The
approach responds to White Paper 3 in enabling the State service providers to address
key challenges and accelerate progress towards the MDGs. DFID India’s Health
Information Note (approved by the PUSS in November 2006) sets out the rationale
for our policy of working through both national and state governments.
Working with other development partners
2.2.5. GoMP and DFID have worked closely to build consensus amongst various
stakeholders within the state to develop the health sector reform programme. The
functional group of Development Partners (‘Donor Partner Technical Assistance
Group’), consisting of members from UNFPA, UNICEF, JICA and EC were
consulted during the design process.
Approach

15
2.2.6. Experience from various sector reform programmes by DFID and other
development partners in other countries suggest a need to move away from inputs and
focus more on outputs and outcomes. MPHSRP, designed on the basis of an agreed
health strategy, a milestones matrix and an MTEF, has a clear focus on outputs.
Sector Budget Support is a relatively new aid instrument for GoMP. However, key
officials in the government recognise the merits of this instrument and welcome the
flexibility of use that goes with it.
2.2.7. The Health Sector Strategy (HSS) provides the overarching context within
which DFID will provide this five year support. On going policy dialogue with
GoMP will help ensure a programme focus towards the poor, especially in remote and
interior areas. Other areas of focus will include governance issues, health sector
management systems and convergence with nutrition, water and sanitation.
2.2.8. DFID’s technical support will be used to strengthen capacity, accountability
and responsiveness at state and district levels to implement and sustain reforms.
DFID support will also be used to strengthen M&E systems and improve human
resource and financial management systems. MPHSRP will play a key role in
supporting GoMP to evaluate and scale up various innovative schemes piloted in the
state. The Strategic Planning Cell that will be set up within the department and the
State Health Systems Resource Centre will also be supported through this programme.
2.2.9. The HSS recommends prioritisation of resources not only in terms of activities
but also poorer regions and districts. PH&FWD will develop a resource allocation
framework to allocate resources to districts based on the Composite Health Index and
absorptive capacity.
Key stakeholders involved in design
2.2.10. MPHSRP has been developed through wide ranging consultations with
GoMP’s PH &FWD, the state’s finance department and the DWCD. DFID also
consulted civil society organisations such as the Urban Resource Centre and
development partners through the Donor Partner Technical Assistance Group.
Economic Appraisal
2.2.11. MP has grown at 4% over 1993-2006, less than the national average of 6%.
GoMP enacted the Fiscal Responsibility and Budget Management Act in August
2005. It has reduced its revenue deficit and is on track to bring down its fiscal deficit
to 3% of GSDP by 2008-09, in line with GoI guidelines. However, the resource base

16
in MP is low and competing demands from other sectors reduce GoMP’s ability to
raise health expenditure, which is currently (2005/6) 3.5% of public expenditure and
0.93% of GSDP. Per-capita public health expenditure is around INR 132 or less than
4 US$: one of the lowest in the country. Not surprisingly, National Health Accounts
for 2001/2, show private health out of pocket expenses at 85% of the total expenditure
incurred on health. There is scope for significant increases in volumes as well as
effectiveness and efficiency of public expenditure. The fragmented institutional health
framework constrains GoMP’s ability to comprehensively plan, budget and judge
overall effectiveness.
2.2.12. MPHSRP will support reforms not funded through other sources. GoMP’s
MTEF, which will be revised annually, estimates a sustainable resource envelope and
matches this to the costed health strategy. It shows health expenditure increasing to
4.3% of public expenditure by 2011-12. GoMP will increase budgetary allocation to
health from its own resources by 10% year on year, with an additional increase for
each percentage above 5% in inflation. GoI allocations will increase, mostly off-
budget, through national programmes such as the NRHM and NACP III.
2.2.13. The percentage of public health expenditure going to primary services is
appropriate at 57% and will be maintained. However, there are issues that undermine
effectiveness and efficiency of expenditure, such as significant absenteeism of staff in
public health facilities, especially in remote and tribal areas, and inadequate planning
and budgeting capacity. The MP HSS proposes to deal with the burden of out-of-
pocket expenses on the poor by financing of emergency referrals (by meeting
transportation costs) and assisting poor people through insurance cover for health
services. More generally, an improved public health service across the board should
result in much reduced out of pocket expenses for private healthcare.
Social Appraisal
2.2.14. In MP and in India a disproportionate number of deaths occur amongst girls,
ST and SC communities. MPHSRP will address inequities in health outcomes and
health provision by focusing on the 10 poorest districts and tribal blocks and by
targeting the marginalised groups within all districts. National NFHS3 data shows that
girls, tribals and dalits have worse infant and child mortality indicators than other
groups. Three out of every four tribals in India are estimated to be in the poorest two
economic quintiles. Tribal human development indicators have been compared with
those of the poorest countries in Sub Saharan Africa. Analysing trends in NSS data,

17
the Human Development Institute predicts that in 2015 the incidence of poverty
amongst tribals will be 37.9% which is the same as the all India figure was in 1993-
94.
2.2.15. The programme will have a significant impact on the tribal districts, most of
which count amongst the poorest in MP. The programme will address the problem of
non-availability of staff and medical facilities in these areas by strengthening the
infrastructure and developing ANM Training Schools in these Districts. This strategy
will increase the accessibility, encourage local recruitment and enhance retention of
staff and reduction of absenteeism. It will also provide much needed jobs, incomes
and status for women from tribal communities. The long distances from functioning
health facilities mean that tribal women currently face higher costs in accessing
emergency obstetric care than their counterparts. There is a strong case for exploring
ways to increase the Janani Suraksha Yojana (JSY) allowance to women in remote
under served locations to compensate for increased transportation costs.
2.2.16 Dalits (SCs) and girl children in MP have poorer health indicators than the rest
of the population but are more evenly distributed geographically. The adverse sex
ratio indicates discrimination at household level. Girls are less likely to be well
nourished or bought for life saving treatment than their brothers. NFHS3 shows that
only 35% of Dalit women had institutional deliveries nationally. Dalit children are
also less likely to be immunised than their non SC/ST counterparts and are less likely
to have received life saving treatments. The reasons for their exclusion from health
services are more complex than remote location and require attention to provider
attitudes and behaviours. Issues of “untouchability” still influence provider
behaviour. The reform programme will strengthen the monitoring and evaluation
system to ensure that progress on various process and outcome indicators is tracked
and disaggregated by sex and socio-economic groups.
2.2.17. Two key challenges for this programme will be: first to reallocate scarce
resources to districts and blocks that are at present deprived and under served and
secondly to increase access for the poorest women, girls, dalits and tribals to health
services. This will require representation of underserved communities on decision
making committees at the District, Block and Gram Panchayat level. PRIs and SC/ST
and women members of PRIs, in particular, will need training if they are to be
empowered to monitor and hold staff to account. Development of risk pooling

18
mechanisms and social insurance schemes are important components of the
programme.
Institutional Appraisal
2.2.18. The MPHSRP is sound and is implementable in the current institutional and
policy context. The policy context for reforms in the health sector is set by:
• Political acceptance that health and education sectors should get priority in
resource allocation.
• Increased emphasis on devolution of powers to decentralized governance
structures, and
• A realization within government that the major problem with the working of
the public health system is related to the overall governance of the sector.
2.2.19. MPHSRP is fully aligned with NRHM and RCH2, with an emphasis on
improving the overall governance of the public health system to make it more
responsive and accountable. The programme rightly focuses on organisational
restructuring, reform of human resource management systems, improved monitoring
and evaluation, strengthening public health infrastructure in focus districts and closer
working with DWCD and water and sanitation departments. Successful
implementation of these measures will require buy-in of all stakeholders and careful
sequencing. The organisational reforms and changes in deep rooted HR practices will
be slow and may invite opposition of staff and political classes. As such, the
programme will need to be led by the top political leadership.
2.2.20. The poor institutional capacity to plan and manage complex reforms will be a
constraint. The programme, however, makes provisions for strengthening capacity at
all levels. It will support reorganisation at the state level to bring in requisite skills for
strategic policy making and for overall management. State level training institutions
will be strengthened (and new schools set up) to ensure staff at all levels receive
training. District offices will be reorganised and strengthened for better planning and
management of health facilities and technical assistance will be provided for
preparation of evidence based and responsive district health plans. The programme
will support capacity building of Panchyati Raj Institutions (PRIs) at all levels.
2.2.21. We assess that critical governance issues have been adequately addressed and,
if implemented successfully, will result in delivering a responsive, efficient and
accountable health system in the state.

19
Political Appraisal
Political Support for Reforms
2.2.22. The state is currently ruled by the Bharatiya Janta Party (BJP), one of the two
major national parties. The Chief Minister is young and dynamic and has strong
support from the central party leadership and from the state legislature. This increases
the prospect of political stability. Elections to the state assembly are due in 2008. The
current government is committed to enhancing expenditure on development. Public
expenditure on social services (including health, education and social welfare) has
increased from 5.27% of GDP in 2003/4 to 5.82% in 2005/6, reflecting the
development orientation of the government.
2.2.23. Overall, the political dynamic of the state is favourable to reform of the health
sector. However, changing the political mind-set to base resource allocation decisions
on rigorous performance data will take continuous engagement. It could be difficult to
ensure that resource allocation priorities are altered in favour of poorer districts as this
may weaken the ability of the political levels to offer patronage. Many proposed
changes in HR policies (transparent transfer policy, Cadre reviews, performance
linked career progression) could face political resistance. Continued support from the
highest political levels will be required to ensure implementation of these difficult
reform measures.
Voices of the Poor and the Policy Processes
2.2.24. The programme will support involving the community in planning for and in
management of service delivery at the local level. The PRIs or locally elected
governments, will be involved in preparations of district health plans which should
help in making these more responsive to local needs. Community monitoring of
services and client satisfaction surveys will improve the accountability of the system
and service providers and should also generate demand for services. However, the
policy making processes at the state level are still exclusive with very little
consultation with civil society.
2.2.25. Overall, the policy context at the national level, fiscal stability, the demand for
performance improvements in public expenditure, and the grain of state level politics
are all key forces that support the reform programme.

20
Environmental Appraisal
2.2.26. Environmental impacts will be widely variable in a programme of this scale and
design. Health and environmental risks arise out of poor infection control and
insufficient environmental management practices. Health risks include the need for
potable water, better air quality, improved sanitation, reduction of mosquitoes, other
disease vectors; all of which impact on the morbidity and mortality profile. The Health
sector reform plan has initiated fundamental analysis of the causes of morbidity and
mortality in the population and has explored multi-disciplinary and multi-institutional
mechanisms by which these issues will be addressed.
2.2.27. Environmental risks include the impact of project-supported interventions, such
as treatment and disposal of bio-medical waste, design and construction of basic health
infrastructure, environmental contamination from medicines/treatment processes, and
sensitisation of human resources to environmental concerns. Appropriate sensitisation
and education can prevent or mitigate these problems. The environmental health
scoping study has been integrated within the GoI’s Infection Management and
Environment Plan (IMEP). IMEP envisages baseline data on medical products, medical
facilities and surveillance systems for mitigating all relevant solid and liquid waste
streams from health facilities through the effective application of GoI’s Biomedical
Waste Management Rules. It also looks at opportunities for green housekeeping and
reduction of environmental impact in health sector facilities.
2.2.28. GoMP proposes to adopt IMEP in the state to cover all health care facilities for
effective management of health and environmental risks in these facilities. The MP
State Health Mission will appoint an IMEP nodal officer and ensure that budgetary
support for IMEP is integrated in the Programme Implementation Plan. Training needs
assessments and awareness building workshops will be conducted in districts.
2.3. Lessons & Evaluation
2.3.1. DFID supported GoMP’s District Health Management and Sector Reform
Programme from 2004 to 2006. The project had three distinct and complementary
components (a) development of coherent and pro-poor sector strategy approved by
GoMP; (b) implementation of district planning process through out the state; and (c)
improved access to basic services affecting health. A recent evaluation of this
programme indicated that it has led to a number of gains including encouraging
innovative practices such as the Janani Express (emergency transport scheme for

21
expecting mothers) and the Completely Observed Meal Programme (COMP) for
pregnant women promoting decentralised planning of resources and stronger working
with other government departments and schemes. GoMP has successfully
implemented a number of innovations under this programme (details are at Annex 7).
The support also helped GoMP to prepare a comprehensive Medium Term Health
Sector Strategy and Medium Term Expenditure Framework, both prerequisites for
MPHSRP.
2.3.2. In designing MPHSRP, DFIDI has taken into account its experience in
implementing the Health Sector Budget Support programme in West Bengal. The first
two years of this programme have demonstrated strong ownership and oversight of
the health sector by the Government of West Bengal, and better donor coordination in
support of the reform process.
3. IMPLEMENTATION
3.1. Management arrangements
3.1.1. The strategic leadership for the programme will be provided by GoMP’s
Finance Department. The Principal Secretary (PH&FWD) in GoMP will lead on
operationalising the Programme. S/he will be assisted by the Commissioner,
Directorate of Health Services, PH&FWD and a core group. A Strategic Planning
Cell (Core Group) headed by a Commissioner will be set up to support the Principal
Secretary to manage implementation, and bring together Development Partners.
DFID will support PH&FWD to contract in additional management and technical
support to implement the strategy. Progress against the milestones will be tracked
through joint annual reviews, with participation from the GoI, DFID, Unicef, UNFPA,
JBIC and others.
3.1.2. A Task Force, chaired by the Chief Secretary, GoMP, and with Principal
Secretaries of the Finance Department, PH &FWD, DWCD, Public Health
Engineering Department (PHED), PRD and Tribal Welfare Department as members,
will provide oversight of convergence activities and monitor outcomes of the
MPHSRP.

22
3.2 Timing
3.2.1. The programme will be effective from the date of Exchange of Letters (EOL).
The programme aims to provide support in five annual tranches beginning Financial
Year (FY) 2007/08, ending FY 2011/2012.
3.3 Funding
3.3.1. A total of up to £60m is being sought as DFID support for MPHSRP. This
will consist of up to £56 million of financial aid and £4 million of Technical Co-
operation funds.
3.3.2. Of the FA component, £2 million will be used by PH&FWD to procure local
consultants. DFID financial aid will pass from the GoI Department of Economic
Affairs to GoMP’s Finance Department and then to the budget of the PH&FWD.
Annual tranches will be separately assessed and disbursed by DFID based on approval
by the Director, South Asia. GoI will appoint Crown Agents Financial Services
Limited to manage the financial arrangements in respect of this FA component.
3.3.3. The Technical Co-operation funds will be available to support implementation
of the strategy, specifically to fund areas where PH&FWD, are unable to identify
resources locally. During the first year, DFID, and PH&FWD will agree upon an
action plan on the utilisation of this TA prior to incurring expenditure.
3.3.4. Based on our assessment of needs and available aid framework, we propose the
following schedule of tranches, which will be revised annually based on progress, and
estimate of need.
Table 7 : Annual DFID tranches (to be revised annually)
Tranches Year I Year II Year III Year IV Year V Total
FA: Core 6m 10 10 10 10 £46m
FA: Indicative 2.5 2.5 2.5 2.5 £10m
TA £4 million over five years £4m
Total £60m
3.3.5. There will be no DFID-funded assets under the programme.

23
3.4. Contracting and Procurement
3.4.1. For the financial aid components, contracting and procurement will be
undertaken by PH&FWD in line with GoMP norms. The Fiduciary Risk Assessment
Study (Annex 4) reviewed GoMP’s contracting and procurement procedures and
DFID India’s Contracts and Procurement Advisory Section (CaPAS) have advised on
the procurement reform plan to strengthen these systems. GoMP has agreed to the
action plan (Annex 5) and the Madhya Pradesh Laghu Udyog Nigam (MP Small
Scale Industries Corporation responsible for health procurement) will be further
strengthened and will function as the nodal agency responsible for the procurement of
drugs and equipment.
3.4.2. DFID will manage the TC fund component through a contracted arrangement,
and procure any technical assistance required using standard DFID procedures.
3.5 Accounting and Auditing
3.5.1. GoMP will account for the financial aid through standard GoMP procedures,
including annual audits conducted by the Comptroller and Auditor General, whose
reports are presented to the legislative assembly. A fiduciary risk assessment has been
carried out as part of the current support to the MPHSRP. This has indicated that
auditing systems within the state and PH&FWD will need to be strengthened. GoMP
will undertake the following activities, laid out in the milestone matrix:
• An internal assessment of under spending and implementation measures to
address these;
• Implementation of the IT Enabled Financial System Plan developed for
improved financial management of on and off-budget items at the state and
district levels;
• Training on improved financial management for state and district level staff.
3.5.2. GoI/GoMP will exempt UK Government and the Programme from the costs of
any taxes, fees, VAT, import or customs duties imposed directly or indirectly by
GoMP on all goods and services provided.
Any providers of Technical Assistance will account for funds they manage in
accordance with DFID accounting rules for consultants.

24
3.6. Monitoring and Reporting
3.6.1. Overall progress will be tracked against the targets set out in the Health Sector
Strategy. The table below sets out the targets for key health indicators:
Table 8: Madhya Pradesh progress on key health indicators and targets for 2012,
compared to all-India targets.
HEALTH
INDICATOR
SRS/ NFHS
II
1998-99
Baseline
SRS/NFHS
III
2005-06
Strategy
outcome
2011-12
India 10th
Plan/NPP/M
DG Targets
and years
1. Maternal mortality
Ratio (per 100,000 live
births)
498
379 (SRS
2003)
220
109 (2015)
2. % Institutional
Deliveries
22 30 75 (2009) 80 (2010)
3. % Deliveries with
Skilled Birth Attendant
28.9 37.1 90
4. Infant Mortality Rate
(per 1000 live births)
88 70 60 30 (2010)
5. Malnutrition among
children (under 3) in %
54 60 35
6. % Children
immunized against 6
diseases
23 40 75 100 (2010)
7. Total Fertility Rate
(TFR)
3.4 3.1 2.1 2.1 (2010)
3.6.2. In addition to overall progress in the State on the key indicators in Table 8,
disaggregated data will be produced regularly to monitor progress amongst the most
disadvantaged groups including ST and SC. This will be used to inform planning and
investment in subsequent years to ensure a narrowing of the inequities in health
between these and other population groups.

25
3.6.2. The policy Milestones Matrix will form the basis on which overall progress will
be assessed at annual joint reviews. Development Partners will also be invited to join
review missions. The purpose of these reviews will be to monitor progress made
against common milestones, and to agree milestones for subsequent tranches. At the
block and district level, the monitoring role of the District and the Panchayat Health
Committee will be strengthened. This will result in PHCs and CHCs being regularly
supervised, and should enhance public participation.
4. Risks
4.1. The programme is judged to be of medium risk with the potential of high return.
Key risks include: fiduciary, weak planning and implementation capacity, non
availability of critical medical staff particularly for remote areas, staff resistance to
change and potential change to GoI policies.
4.2. We judge that these risks are manageable due to: presence of strong political and
bureaucratic commitment to health refoms, realistic GoMP plans for strengthened
financial systems and capacity building, and agreed actions from a Fiduciary Risk
Assessment (FRA).
A. Fiduciary risk
4.2.1. Medium probability, high impact: The programme of support is viewed to be
of medium risk. Key risks revolve around quality and targeting of expenditure,
monitoring, accounting and auditing of funds, procurement, and internal government
controls. The detailed assessment is at Annex 4.
4.2.2. Mitigation measures have been agreed with the government to address these
risks. Many of these mitigation measures are already a part of the larger reforms that
are being undertaken by GoMP to improve the working of the Public Financial
Management and Accountability (PFMA) system in the state as a whole. These
measures include preparation of performance budgets, preparation of a budget manual
and IT based Financial Monitoring and Information System (FMIS), strengthening
staffing of accounts and finance functions in the health department at all levels. The
GoMP will also focus on standardization of financial procedures in health societies,
enactment of a procurement law and establishment of an oversight body. Institutional
mechanisms for follow up on audit reports will be strengthened. Fiduciary risks will
be reviewed regularly through out implementation.
B. Inadequate implementation capacity to address critical reforms

26
4.2.3. Medium probability, high impact: There is a risk that GoMP will not be able
to build/deploy adequate capacity to implement reforms. However, DFID will be
supporting GoMP in strengthening planning and implementation capacity by
providing support for the district planning process, promoting Public Private
Partnerships and encouraging better human resource management systems particularly
in 10 focus districts. Capacity building of staff will be taken up as a priority. There is
a high degree of political commitment to health sector reforms.
C. GoMP commitment to Health Sector Strategy priorities is not sustained
4.2.4. Low probability, high impact: The likelihood of PH&FWD meeting its
Strategic Objectives will depend on prioritised system improvements, strengthened
service delivery and sector reforms identified in the HSS and MTEF. If the
HSS/MTEF priorities are not kept central to future planning, budgeting and donor
partner activity, chances of reverting back to ad hoc and piecemeal planning will
increase significantly. Given the high degree of political and bureaucratic
commitment to reforms, this risk is low probability. We will review this risk through
the annual review process.
D. Staff obstruction to reforms
4.2.5. Medium probability, medium impact: PH&FWD has a large complement of
organised staff, including doctors and nurses. PH&FWD commitments to policy and
strategic reform may be resisted, especially in human resource restructuring. Again,
this risk will be monitored through the annual reviews. The current high degree of
political and bureaucratic commitment to reforms reduces the probability and impact
of this risk.
E. Continued exclusion of disadvantaged areas/groups
4.2.6. Medium probability, high impact: There is a risk that services continue to fail
to reach the poor in 10 focus districts and therefore that inequity in health outcomes
persists. However, much of MPSRP is aimed at reducing this risk. For example,
addressing gaps in infrastructure and redeployment/recruitment of staff to fill vacant
posts in 10 focus districts, provision of untied funds at district level and a
disaggregated participatory monitoring framework all seek to ensure progress towards
equity outcomes. Residual risk is medium probability, high impact.
F. Change in GoI policies and commitment

27
4.2.7. Low probability, medium impact: There is a risk of GoI changing its policies
and commitment to the health sector. This could adversely affect the financing plan
since GoI contributes 18% of the resources. However, this risk is low probability, and
medium impact for the reform programme. GoI continues to show strong commitment
to investment in the health sector and NRHM promises to bring more money into the
sector. There is also a consensus across the political spectrum to increase public
investment in health.
Table 8: Risk Matrix
Probability
Impact
Low Medium High
Low F C
Medium D A, B, E
High
5. Conditionality
5.1. GoMP will monitor MPHSRP implementation using the Policy Milestones
Matrix in consultation with DFID and other development partners. The present
Milestones Matrix includes prior actions for 2006-07, definite actions for 2007-08,
draft matrix for 2008-9 and expected outcomes by 2012. The actions for 2008-9 will
be revised at the time of the first annual review. Milestones for later years will be
developed annually during review missions between the Government and
development partners.
5.2. In order to absorb any likely future adjustments in resources available to the
programme, we propose that 80% of each annual tranche be designated as core and
20% as indicative. The core and indicative components of DFIDI’s disbursements for
the coming years will be communicated to GoMP by November in the preceding year,
in time for the state budget session..