
Luxation Injuries World Health Organization Classification.
25
Luxation Injuries Luxation Injuries World Health World Health Organization Organization Classification Classification
-
Upload
isabel-iredale -
Category
Documents
-
view
219 -
download
1
Transcript of Luxation Injuries World Health Organization Classification.

Luxation InjuriesLuxation Injuries
World Health World Health Organization Organization ClassificationClassification

Great Threat to Pulp VitalityGreat Threat to Pulp Vitality(Luxations)(Luxations)
• Traumatizes supporting structures of Traumatizes supporting structures of the periodontiumthe periodontium
• Potentially severs pulpal blood Potentially severs pulpal blood supply entering the apical foramensupply entering the apical foramen
• WHO recognizes five main types of WHO recognizes five main types of luxation injuriesluxation injuries

Luxation InjuriesLuxation Injuries
• ConcussionConcussion
• SubluxationSubluxation
• Extrusive luxationExtrusive luxation
• Lateral luxationLateral luxation
• Intrusive luxationIntrusive luxation

ConcussionConcussion
• Clinical findings: tender to touch, not Clinical findings: tender to touch, not displaced no increased mobility. displaced no increased mobility. Sensitivity test are most likely positiveSensitivity test are most likely positive
• Radiographic findings: No Radiographic findings: No abnormalitiesabnormalities
• Treatment: No treatment is need but Treatment: No treatment is need but it is essential to monitor pulpal it is essential to monitor pulpal condition for one yearcondition for one year

Concussion: follow up
• Follow up: clinical and radiographic Follow up: clinical and radiographic examination at, 4 weeks, 8 weeks, 1 year with examination at, 4 weeks, 8 weeks, 1 year with clinical and radiographic examinationclinical and radiographic examination
• Favorable outcome: Asymptomatic, positive Favorable outcome: Asymptomatic, positive pulp tests, can have false negative up to 3 pulp tests, can have false negative up to 3 months, continued root development, intact months, continued root development, intact lamina duralamina dura
• Unfavorable outcome: Symptomatic, negative Unfavorable outcome: Symptomatic, negative pulp test, can have false neg for 3 months no pulp test, can have false neg for 3 months no continuing root development, signs of PAP, endo continuing root development, signs of PAP, endo tx appropriate for stage of root developmenttx appropriate for stage of root development

Subluxation• Clinical findings: tender to touch or tap, Clinical findings: tender to touch or tap,
increased mobility, not displaced. Bleeding increased mobility, not displaced. Bleeding from the gingival crevice. May have from the gingival crevice. May have negative pulp test initially indicating negative pulp test initially indicating transient pulpal damage.transient pulpal damage.
• Monitor pulpal response until a definitive Monitor pulpal response until a definitive pulpal diagnosis can be madepulpal diagnosis can be made
• Radiographic findings: Abnormalities are Radiographic findings: Abnormalities are usually not foundusually not found
• Treatment: no treatment is needed. Treatment: no treatment is needed. Monitor pulpal status for one yearMonitor pulpal status for one year

Subluxation:Subluxation: follow up follow up
• Follow up at 2 weeks, 4 weeks, 8 weeks 6 Follow up at 2 weeks, 4 weeks, 8 weeks 6 months and one year with clinical and months and one year with clinical and radiographic examinationradiographic examination
• Favorable outcome: asymptomatic, positive Favorable outcome: asymptomatic, positive pulp test. Can have false negative up to 3 pulp test. Can have false negative up to 3 months. Continued root development of months. Continued root development of immature teeth. Intact lamina dura.immature teeth. Intact lamina dura.
• Unfavorable outcome: Symptomatic, Unfavorable outcome: Symptomatic, negative pulp tests, external inflammatory negative pulp tests, external inflammatory resorption, arrested root development, PAP, resorption, arrested root development, PAP, endo tx appropriate for stage of root endo tx appropriate for stage of root development.development.

Extrusive Extrusive LuxationsLuxations

ExtrusiveExtrusive LuxationLuxation• Clinical Findings: Tooth appears elongated Clinical Findings: Tooth appears elongated
and is excessively mobile. Sensitivity test and is excessively mobile. Sensitivity test give negative resultsgive negative results
• Radiographic findings: Increased periodontal Radiographic findings: Increased periodontal ligament space apicallyligament space apically
• Treatment: Reposition tooth by gently re-Treatment: Reposition tooth by gently re-inserting it into the socket. Stabilize for 2 inserting it into the socket. Stabilize for 2 weeks with a flexible splint. In mature tooth weeks with a flexible splint. In mature tooth pulp necrosis is expected. With immature pulp necrosis is expected. With immature teeth watch for signs and symptoms of pulpal teeth watch for signs and symptoms of pulpal necrosis. Endodontic therapy indicated.necrosis. Endodontic therapy indicated.

Extrusive Luxation: Extrusive Luxation: follow upfollow up
• Remove splint in 2 weeks. Perform clinical and Remove splint in 2 weeks. Perform clinical and radiographic exam at 2 weeks, 4 weeks, 8 weeks, radiographic exam at 2 weeks, 4 weeks, 8 weeks, 6 months, then yearly6 months, then yearly
• Favorable outcome: Asymptomatic, clinical and Favorable outcome: Asymptomatic, clinical and radiographic signs of healed periodontium, radiographic signs of healed periodontium, positive pulp tests (false neg up to 3 mos), positive pulp tests (false neg up to 3 mos), marginal bone height maintained, continued root marginal bone height maintained, continued root development development
• Unfavorable outcome: Symptoms and Unfavorable outcome: Symptoms and radiographic signs of apical periodontitis, radiographic signs of apical periodontitis, negative response to pulp tests, if breakdown of negative response to pulp tests, if breakdown of marginal bone is noted splint for an additional 4 marginal bone is noted splint for an additional 4 weeks, signs of external inflammatory root weeks, signs of external inflammatory root resorption, endodontic therapy appropriate for resorption, endodontic therapy appropriate for root development.root development.
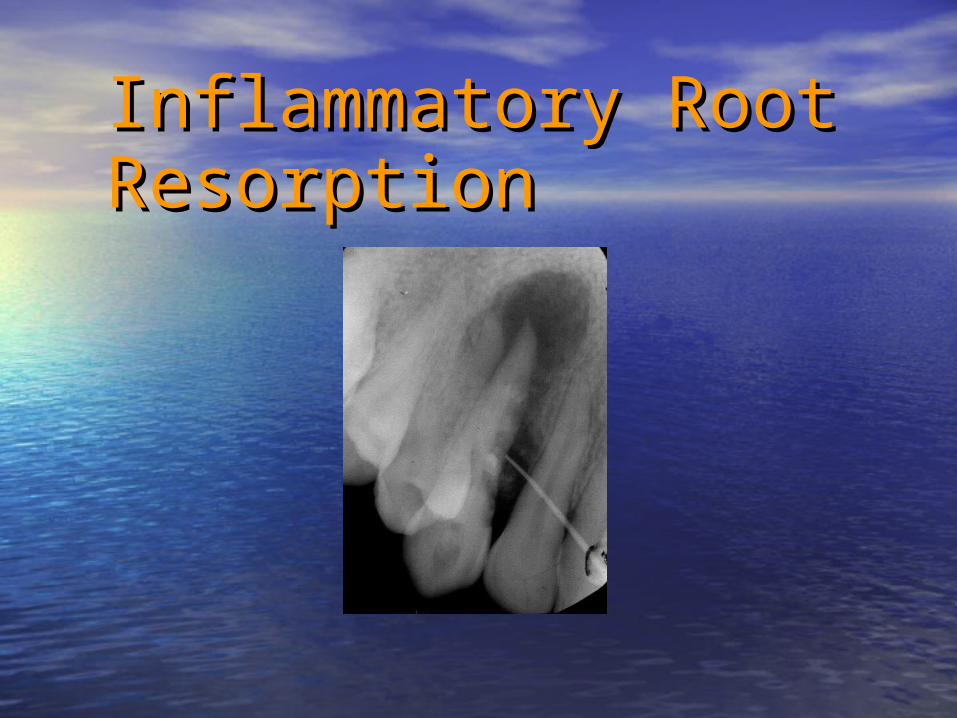
Inflammatory Root Inflammatory Root ResorptionResorption

Lateral LuxationsLateral Luxations• Clinical findings: displacement usually Clinical findings: displacement usually
palatal/lingual direction. Often immobile and palatal/lingual direction. Often immobile and percussion gives metallic sound. percussion gives metallic sound. Fracture of Fracture of alveolar process is present. alveolar process is present. Negative pulp Negative pulp tests.tests.
• Radiographic findings: widen PDL, best seen Radiographic findings: widen PDL, best seen on occlusal exposureon occlusal exposure
• Treatment: Reposition digitally to disengage Treatment: Reposition digitally to disengage from its boney lock and gently reposition to from its boney lock and gently reposition to original location. Stabilize 4 weeks with flexible original location. Stabilize 4 weeks with flexible splint. Monitor vitality. If necrotic endodontic splint. Monitor vitality. If necrotic endodontic therapy is indicated to prevent root resorptiontherapy is indicated to prevent root resorption

Lateral LuxationsLateral Luxations

Lateral LuxationsLateral Luxations

Lateral LuxationsLateral Luxations

Lateral LuxationsLateral Luxations

LateralLateral LuxationsLuxations

Lateral Luxation: Lateral Luxation: follow upfollow up
• Follow up: 2 weeks splint removal, 2-4-6weeks, Follow up: 2 weeks splint removal, 2-4-6weeks, 6-12 months and yearly for 5 years clinical and 6-12 months and yearly for 5 years clinical and radiographic exam.radiographic exam.
• Favorable outcome: asymptomatic, clinical and Favorable outcome: asymptomatic, clinical and radiographic signs of normal periodontium. radiographic signs of normal periodontium. Positive pulp tests. Potential false neg. for 3 Positive pulp tests. Potential false neg. for 3 months. No loss of marginal bone height. months. No loss of marginal bone height. Continued root development in immature teeth.Continued root development in immature teeth.
• Unfavorable outcome: Symptomatic with Unfavorable outcome: Symptomatic with radiographic PAP. Negative vitality. (False radiographic PAP. Negative vitality. (False negative up to 3 months) If marginal bone is negative up to 3 months) If marginal bone is breaking down splint for additional 4 weeks. breaking down splint for additional 4 weeks. External inflammatory root resorption or External inflammatory root resorption or replacement resorption. Endodontic therapy replacement resorption. Endodontic therapy appropriate for root development stage.appropriate for root development stage.

Intrusive LuxationIntrusive Luxation
• Clinical findings: tooth displaced axially into Clinical findings: tooth displaced axially into the alveolar bone. Immobile with metallic the alveolar bone. Immobile with metallic sound to percussion (ankylotic). Negative to sound to percussion (ankylotic). Negative to vitality tests.vitality tests.
• Radiographic findings: PDL absent. CEJ more Radiographic findings: PDL absent. CEJ more apical then adjacent non-injured teeth.apical then adjacent non-injured teeth.
• Treatment: contingent on root development. Treatment: contingent on root development. Teeth with incomplete root development vs Teeth with incomplete root development vs teeth with complete root formationteeth with complete root formation

Intrusive LuxationsIntrusive Luxations

Intrusive Luxation: Intrusive Luxation: treatmenttreatment• Incomplete root formation: Allow eruption with no Incomplete root formation: Allow eruption with no
intervention. If no movement within three weeks intervention. If no movement within three weeks initiate orthodontic repositioning. If tooth was initiate orthodontic repositioning. If tooth was intruded more than 7 mm immediately reposition intruded more than 7 mm immediately reposition surgically or orthodontically.surgically or orthodontically.
• Complete root formation: allow eruption if Complete root formation: allow eruption if intruded less than 3 mm. If no movement in 3 intruded less than 3 mm. If no movement in 3 weeks reposition surgically or orthodontically weeks reposition surgically or orthodontically before ankylosis sets in. More extensive intrusions before ankylosis sets in. More extensive intrusions promptly reposition surgically.promptly reposition surgically.
• Pulpal necrosis likely initiate endodontic therapy Pulpal necrosis likely initiate endodontic therapy with CAOH 2 weeks after surgery.with CAOH 2 weeks after surgery.
• Once repositioned surgically or orthodontically Once repositioned surgically or orthodontically stabilize with flexible splint for 4-8 weeksstabilize with flexible splint for 4-8 weeks

Intrusive Luxation: Intrusive Luxation: Follow upFollow up
• 2 weeks splint removal. Clinical and 2 weeks splint removal. Clinical and radiographic exam. Then continue checking radiographic exam. Then continue checking at 4 weeks 8 weeks 6 months and yearly for at 4 weeks 8 weeks 6 months and yearly for 5 years.5 years.
• Favorable outcome: tooth erupting or in Favorable outcome: tooth erupting or in place. Intact lamina dura. No sign of place. Intact lamina dura. No sign of resorption. Continued root development.resorption. Continued root development.
• Unfavorable outcome: Tooth locked in place Unfavorable outcome: Tooth locked in place (ankylotic) Apical periodontitis. External (ankylotic) Apical periodontitis. External inflammatory root resorption or replacement inflammatory root resorption or replacement resorption. Endodontic therapy appropriate resorption. Endodontic therapy appropriate for stage of root development.for stage of root development.

Intrusive Luxation Intrusive Luxation Immature Immature

Re-eruptingRe-erupting

Replacement Replacement ResorptionResorption(Ankylosis)(Ankylosis)


















