Sports Injury Classification - University of...
16
Classification of Injuries Sports Injury Classification Acute / Traumatic • extrinsic causes: direct blow, collision, impact • intrinsic causes: muscle forces, joint loadings Acute vs Overuse Injuries v increasing frequency of overuse injuries v acute injuries: high velocity uncontrolled impacts macro-trauma
Transcript of Sports Injury Classification - University of...

Classification of Injuries
Sports Injury Classification
Acute / Traumatic
• extrinsic causes: direct blow, collision, impact
• intrinsic causes: muscle forces, joint loadings
Acute vs Overuse Injuriesv increasing frequency of
overuse injuries
v acute injuries:high velocityuncontrolled impacts macro-trauma
Classic Ankle Inversion Sprain
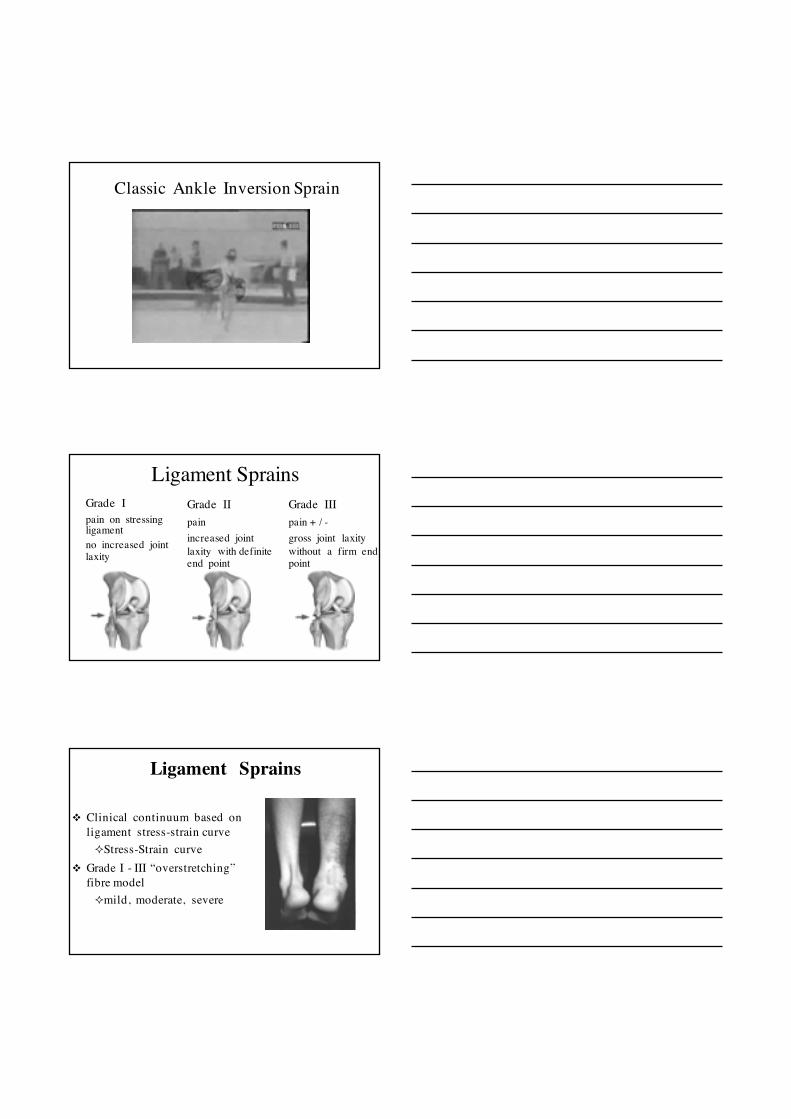
Ligament SprainsGrade Ipain on stressing ligament no increased joint laxity
Grade IIpainincreased joint laxity with definite end point
Grade IIIpain + / -gross joint laxity without a firm end point
v Clinical continuum based on ligament stress-strain curve ²Stress-Strain curve
v Grade I - III “overstretching” fibre model²mild, moderate, severe
Ligament Sprains

Stress - Strain Curve
Rupture of Joint Capsule / Ligaments(AC Injury Examination under Anesthesia)
vAC Injuries: Type I - VI(Rockwood classification)
v joint capsulevacromioclavicular lig’svcoracoclavicular lig’s
trapezoidconoid
v single, debilitating episode ²e.g., Knee²ACL²ACL + L/MCL²ACL + L/MCL + Meniscus²ACL + PCL
Ligament Sprains

v multiple, debilitating episodes(chronic on acute)
²e.g., Ankle²ATFL²ATFL+CFL+PTFL²Syndesmosis²ATFL+CFL+PTFL+Deltoid
Ligament Sprains
v Clinical premise -“hypermobility”, assessed by multi-joint “laxity”, predisposes to subluxation / dislocation injuries
Joint Dislocations & Subluxations
Joint Action ROM ScoreElbow extension > 10° 1 1Knee extension >10° 1 1Thumb apposition to ant forearm 1 15th finger ext >90° 1 1Forward flexion Palms flat on floor 1
/ knees straight
Total maximum possible score 9
Beighton Score
Joint Dislocations & Subluxations
v dislocation: complete dissociation of the articulating joint surfaces
v subluxation: articulating surfaces remain partially in contact

Tendon Subluxation – Acute / Chronic
Diastasis - Tibiofibular Syndesmosis
AP Xray>6mm overlap
v Distal separation of the tibia & fibula due to tear / rupture of syndesmosis
v “high” ankle sprain
Biomechanics & Anatomy in Joint Injuries
v direct impactsv distracting forces

Biomechanics & Anatomy in Joint Injuries
v injury to surrounding joint capsule and structures with luxations
v luxation / laxity predispose to impingement (e.g., acromionprocess) and recurrent injury
Meniscal Injuries – Knee Joint
Acute tears shear stress with knee in flexion & compression with femoral rotation (twisting with planted foot)
medial meniscus at greater risk of injury (less mobile) than lateral meniscus
Acute Meniscus Injuries
v Joint line painv +ve McMurray’s testv Joint effusion / swellingv Popping or clicking within joint v Giving way sensation / lockingv Arthroscopic surgery

Acute Joint Injuries – Joint Effusion
vincreased intra-articularfluid
vtraumatic ligament, bone or meniscalinjuries
Acute Joint Injuries – Joint Effusion
vsynovial fluidvbloody effusion: hemarthrosis
Acute Articular Cartilage Injuriesv fragments sheared from articular
surfaces (luxations) v chondral & osteochondral
fractures common v osteoarthritis linkv typical changes seen on X-ray
include: joint space narrowing, subchondral sclerosis, subchondralcyst formation, and osteophytes
v better detection (MRI, CT) v arthroscopic surgery

Chondral Injuries
acute chondral / osteochondralinjuries from high compressive / shearing forces“poor healing” – limited regenerative / repair capacityrange of injury severity
v among most common sporting injuries
v muscle fibres fail under imposed demands
v recurrent (particularly hamstrings)
Muscle Strains
“Classic” Muscle Strain Classification
Grade Ismall # fibres ruptured, pain localised, no strength lossGrade IIlarge # fibres ruptured, reduced strength, swelling & pain limited movementGrade IIIcomplete tear of muscle, muscle-tendon junction, significant strength loss, obvious visual defect
Tears of muscle at muscle-tendon junction – tendinous interfaces

“Evolving” Muscle Strain Classification
1. Small Injuries (tears)2. Moderate Injuries (tears)3. Extensive Tears4. Complete Tears
a) myofascialb) within muscle at MTJc) extends into tendon
Pollock et al. 2014
Classification by anatomical location & type/s of tissue involved
Biceps femoris strain with central tendon disruption – 72 days recoveryBiceps femoris strain without central tendon disruption – 21 days recovery
v sudden acceleration or deceleration
v neural innervation
Biomechanical & Anatomical Factors in Muscle Strains
v eccentric action mode²force velocity curve
v biarticular muscles pre-disposed²hamstrings²rectus femoris²medial gastrocnemius
vHigher proportion of fast twitch fibres
Biomechanical & Anatomical Factors in Muscle Strains

Applying Exercise Physiology KnowledgeDraw a Force-Velocity Curve on the Graph below
0eccentric concentric
100%
200%
Contraction Velocity
Contraction Force
Sarcomeres lengtheningunder load
Sarcomeres shorteningunder load
v agonist-antagonist imbalance(e.g., quad - ham ratio)
v muscle-tendon interfaces(e.g., semitendinosus)
v elasticity (cc, sec, pec)
Biomechanical & Anatomical Factors in Muscle Strains
Hamstring Strain Classification
v“Type I”
²Biceps Femoris Long Head
²High Speed Running
²Proximal Muscle Tendon Junction
v“Type II”
²Semimembranosus
²Stretching – Slow Speed
²Proximal Tendon / Ischial Tuberosity

Muscle Strains & Haematomas
vIntramuscular haematoma²More painful
²More restrictive
vIntermuscular haematoma²Generally more evident
Biceps Femoris InjuryMRI Visualization
Muscle Contusions
“Corks”v forceful impact
v localised (blunt) trauma
v “common” (superficial) sites
v vastus lateralis / biceps brachii
v “other” (medial) sites
v thigh adductors / med. gastroc
Muscle Contusions“Corks”vmild - severe bruising
vlocal fibre damage & bleeding
vedema & hematoma
vICE not HARM
v place in pain free stretched position

Myositis Ossificans Traumaticavheterotrophic ossification (bone deposition 2-4 wks)v cause - local factors (reserve of Ca++ in adjacent skeletal tissue; vascular stasis tissue hypoxia; mesenchymal cells with osteoblasticactivity) / unknown systemic factors. vmechanism - differentiation of fibroblasts into osteoblasts
Tendon Rupture
vPartial RuptureSmall to large # ruptured fibres, pain and limited function (equivalent to Grade I / II sprain)
vComplete RuptureTotal rupture of tendon, pain and non-function of specific muscle-tendon unit (Grade III equivalent)
Biomechanics & Anatomy in Tendon Rupture
vsudden accelerationv jumping / landingvunexpected loadingvstretch-shortening action

Biomechanics & Anatomy in Tendon Rupture
v in vivo loading patternvexcessive stiffnessvmuscle-tendon “imbalance”
(e.g., Achilles tendon)
Tendon “Avulsions”
vdetachment of tendonvmallet finger
(extensor mechanism)vjersey finger
(flex digit profundus)
Bone Fractures
²blow / collision
²twisting
vcommon sporting injuryvdirect trauma
²blow / collisionvindirect trauma
²twistingvsplint / stabilizevmedical referral

Bone Fracturesvclosed fracturesvopen fractures
²(compound)
vnerve damagevvessel damagevbleeding / shockvinfection
Simple & Complex Fractures

Peak Fracture Prevalence in Adolescence
Collés Fracture
Biomechanics & Anatomy in FracturesAvulsion fractureslinternal forceslyounger athletes
Stress fractureslrepetitive forceslpars interarticularis
Greenstick fractureslincomplete breaklyounger athletes
Bone “Bruising”
• Microtrabecular fracture /haemorrhage / oedema in bone following traumatic insult
• MRI shows bone marrow oedema• Evident for 12 - 14 weeks• Interosseous bruise - bleeding inside bone
marrow is located. • Subchondral bruise – between cartilage
and bone beneath, causing cartilage to separate from bone
• Subperiosteal hematoma - bleeding beneath periosteum.

Periosteal Contusion
• Sub-periosteal haematoma• Development of palpable lump• Periosteum is raised, inflammed,
irritated and painful on palpation or muscle contraction
• Maybe associated with damage to surrounding structure e.g., clunealnerve in “hip pointer”
• Protective padding e.g., shin pads, hip guards
Growth Plate Injuries
Salter & HarrisSalter & Harris
Type I - epiphysis (E) completely separated from metaphysis (M) Type II - E + growth plate (GP) separated from metaphysis MType III - Fx thru E separates part of E & GP from MType IV - Fx thru E, across GP and into MType V - GP compressed / crushed (prognosis poor)