CUTANEOUS LUPUS ERYTHEMATOSUS; EPIDEMIOLOGY, ASSOCIATION WITH SLE

Lupus erythematosus: systemic andcutaneous manifestations
Naomi Rothfield, MDa,*, Richard D. Sontheimer, MDb,d, Megan Bernstein, MDc
aDivision of Rheumatology, Department of Medicine, University of Connecticut Health Center, Farmington, CT 06030, USAbDepartment of Dermatology and Residency Training Program, University of Oklahoma Health Sciences Center,
Oklahoma City, OK 73104, USAcUniversity of Connecticut Health Center, Farmington, CT 06030, USA
Abstract Skin and joint involvements are the most commonly occurring manifestations of systemic
lupus erythematosus. There are 3 forms of cutaneous lupus: chronic cutaneous (discoid) lupus, subacute
cutaneous lupus, and acute cutaneous lupus. Joint manifestations are usually not associated with warmth
of the joints and may be only associated with pain and swelling. Painful or swollen joints respond
rapidly to small or moderate doses of corticosteroids, whereas cutaneous manifestations usually respond
to antimalarial drugs. Anti-Ro is associated closely with a photosensitive rash and with subacute lupus.
D 2006 Elsevier Inc. All rights reserved.
Introduction
Systemic lupus erythematosus (SLE) is a multisystem
disease of unknown cause that is characterized by the
presence of multiple autoantibodies. Typically, it affects
the skin, joints, kidneys, lungs, nervous system, serous
membranes, and other systems. The autoantibodies are
typically antinuclear antibodies. The clinical course is
extremely variable and ranges from life-threatening to mild
diseases that never require hospitalization. The disease is
predominantly present in women, especially those who are
in their 20s and 30s, but it may occur in children and in
elderly individuals.
0738-081X/$ – see front matter D 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.clindermatol.2006.07.014
* Corresponding author. Tel.: +1 860 679 3604, +1 860 679 2160;
fax: +1 860 679 1287.
E-mail addresses: [email protected] (N. Rothfield)8
[email protected] (R.D. Sontheimer)8 [email protected]
(M. Bernstein).d Tel.: + 1 405 271 4662; fax: +1 405 271 7216.
Cutaneous manifestations of SLE are present in 85% of
patients during the course of the disease, and musculoskel-
etal abnormalities are present in approximately 95%.1 Joint
and skin manifestations thus occur in nearly all patients with
SLE. The disease tends to mimic the manifestations present
at onset during subsequent exacerbations.
Musculoskeletal manifestations
Musculoskeletal manifestations are the most common
feature of SLE.1 Arthritis with objective evidence of pain on
motion, tenderness, effusion, or periarticular soft-tissue
swelling is present at the time of diagnosis in 88% of
patients. Some patients develop arthritis after the diagnosis
had been made, such that 89% of patients have arthritis
during the disease. Other patients have arthralgia without
objective evidence of arthritis, such that 95% of patients
have either arthritis or arthralgia.
In some patients, arthralgia or arthritis may precede the
onset of multisystem disease by many years. The most
common joints involved are the proximal interphalangeal
Clinics in Dermatology (2006) 24, 348–362

Manifestations of lupus erythematosus 349
joints (present in 82% of patients). The distribution is nearly
always symmetrical. The knees are involved in 76% of
patients, followed by the wrists and metacarpophalangeal
joints. The ankles, elbows, and shoulders are involved less
frequently. Knee effusions can be moderately severe.
Aspiration reveals a clear fluid with less than 3000 white
blood cells per microliter. Most cells are small lymphocytes,
and there is a low protein level. Antinuclear antibodies and
lupus erythematosus (LE) cells may be found in the fluid.
Serum complement proteins are usually low, reflecting
similarly low levels in the serum. Synovial histopathology is
nonspecific with diffuse proliferation of lining cells and
some perivascular mononuclear cells, enlarged endothelial
cells, and thrombi. The arthritis disappears completely
within a few days after treatment with corticosteroids for
systemic diseases.
If a patient presents with a single swollen or painful
joint, one should suspect an alternate diagnosis, such as
infectious or crystalline arthritis, for which appropriate
diagnostic (eg, joint aspiration) and therapeutic measures
should be instituted.
During the course of the disease, patients may develop
deformities, but these are not related to joint destruction.
Typical swan-neck deformities with ulnar deviation of the
fingers develop after 3 to 4 years of disease in approxi-
mately 10% of patients who continue to have mild inter-
mittent joint pains. Radiographs of the hands reveal no bony
erosion or loss of joint space. Joint subluxation is a result of
involvement of the tendons and spasm of the small muscles
of the fingers.
Morning stiffness is present in 50% of patients, and
typical subcutaneous nodules occur in 10%. Tenosynovitis
occurs in approximately 10% of patients, with some
patients experiencing rupture of the infrapatellar, deltoid,
or Achilles tendons.
Avascular necrosis occurs in approximately 15% of
patients after prolonged treatment with high doses of
corticosteroids. Avascular necrosis is most common in the
femoral heads and presents as anterior groin pain, trochan-
teric bursal pain, or anterior thigh pain. Radiographs may be
negative early after the onset of pain, but magnetic
resonance imaging may allow early diagnosis.
Muscle pain is present in approximately 30% of patients,
with enzyme abnormalities occurring in approximately 20%
of patients before treatment.
Fibromyalgia is common in patients with SLE and must
be distinguished from the joint and muscle pain associated
with the disease.
Cutaneous manifestations
Pathophysiology
The pathophysiologic mechanisms of LE-specific skin
disease continue to be elucidated.2 It is thought that
development of skin disease is related to the same
autoimmune abnormalities responsible for the systemic
components of LE. Current theories discuss the relationship
between genetic susceptibility, autoimmune induction and
subsequent expansion, and injury to the immune system.3
Genetic susceptibility is probably related to genes that
decrease the threshold for self-reactivity and allow a
sustained immune response after the first response or to
the type and extent of end-organ damage.4 Case-control
studies have demonstrated that the major histocompatibility
complex class II alleles DRB and DQA are associated with
SLE in human beings.5 The autoimmune induction phase
refers to the development of self-reactive T cells that
demonstrate loss of self-tolerance.2 Mechanisms of induc-
tion may include molecular mimicry induced by infectious
antigens, abnormal expression of human leukocyte antigen
DR, malfunction of thymic or peripheral tolerance, and
presentation of cryptic peptides during apoptosis. The
expansion phase involves the progressive development of
abnormal autoimmune clonal expansions of B and T cells
that have self-recognition capabilities. The final injury phase
results in clinical disease and is likely related to autoanti-
bodies and immune complexes causing tissue damage.
Mechanisms likely include direct cell death, activation of
the complement system, opsonization, and the inhibiting
function of target molecules.2
Clinical characteristics
The cutaneous manifestations of lupus are categorized
according to the Gilliam classification of LE skin disease.6
This system divides lupus skin diseases into LE-specific
skin diseases, which show distinctive histologic changes of
LE, and LE-nonspecific skin diseases, which include man-
ifestations that can be seen in lupus and in other diseases.
Characteristic histopathologic skin changes of LE-specific
skin disease include hyperkeratosis; atrophy of the epider-
mis; liquefactive degeneration of the basal epidermis; and an
infiltrate of mononuclear cells in the perivascular, perifol-
licular, and dermal-epidermal junction, perivascular areas,
and perifollicular areas.7 Other characteristic changes
include epidermal basement membrane thickening and
melanin pigment incontinence.2 Varying mosaics of these
features are seen in the 3 major categories of LE-specific
disease: acute cutaneous LE (ACLE), subacute cutaneous
LE (SCLE), and chronic cutaneous LE (CCLE).
Acute cutaneous LE
Acute cutaneous LE is categorized as localized ACLE or
generalized ACLE. Localized ACLE is characterized by
erythema over the malar eminences of the face and bridge
of the nose (butterfly blush). The nasolabial folds are
typically spared. This distribution resembles the shape of a
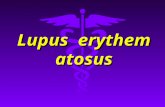
butterfly. Acute cutaneous LE is often associated with
active SLE (Fig. 1). The rash may have a fine surface scale
and be associated with edema. When especially severe,

Fig. 1 Acute cutaneous LE. In addition to the butterfly areas
(malar eminences and nose bridge), the forehand and chin areas
can also be affected in severe cases such as this. Note sparing of the
nasolabial folds and areas of sun-protected skin (eg, upper eyelids).
N. Rothfield et al.350
ACLE produces vesiculobullous skin changes. The butter-
fly rash has been noted in 52% of patients with SLE at the
time of diagnosis.1 The clinical activity of ACLE typically
cycles in parallel with the activity of the underlying SLE.
Acute cutaneous LE is frequently associated with exposure
to sunlight or artificial sources of UV light. The lesions
typically heal well without scarring. In darkly pigmented
individuals, however, postinflammatory hyperpigmentation
and/or hypopigmentation can remain long after the red-
dened inflammatory component of ACLE had resolved.
Acute cutaneous LE may be confused with seborrheic
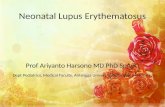
Fig. 2 Subacute cutaneous LE. Left panel, Annular morphological s
panel, Papulosquamous/psoriasiform subtype. Note the retiform array pr
with either subtype.
dermatitis or acne rosacea; the former condition involves
the nasolabial folds, whereas the latter condition is
characterized by the presence of papules and pustules that
are not found in the facial rash of SLE unless secondary
infection is present.
Generalized ACLE is described as a diffuse or papular
erythema of the face, upper trunk, or extremities that
resembles a viral exanthem or drug eruption. One study
reported generalized ACLE in 35% of patients with SLE.8
Lesions develop quickly and last for hours to days. The
development of this rash is most often associated with
systemic disease activity and is usually related to sun
exposure. Facial involvement can be extensive. The rash
spares the distal interphalangeal, proximal interphalangeal,
and metacarpophalangeal joints, an important differentiating
feature from dermatomyositis, which can otherwise resemble
ACLE. Complications of ACLE include postinflammatory
hyperpigmentation, especially in darker-skinned individuals.
HistopathologyThe histopathology of ACLE is less striking than that of
SCLE and of discoid LE (DLE). Acute cutaneous LE demons-
trates a sparse dermal cellular infiltrate, focal liquefactive
degeneration of the basal epidermis, and upper dermal edema.
Epidermal necrosis can be noted in the most severe forms of
ACLE and may resemble toxic epidermal necrolysis.2
Subacute cutaneous LE
Subacute cutaneous LE is subdivided into 2 morpholog-
ical variants—annular SCLE and papulosquamous SCLE.
Annular SCLE has also been referred to as lupus margin-
ubtype. Note the polycyclic array formed as lesions merge. Right
oduced as lesions merge. There was no dermal scarring associated

Table 1 Drugs implicated in triggering the clinical expression
of SCLE (listed alphabetically within groups)
Diuretics
Hydrochlorothiazidea
Spironolactonea
Calcium-channel blockers
Diltiazema
Nifedipinea
Nitrendipine
Angiotensin-converting enzyme inhibitors
Captoprila
Cilazapril
Acid blockers
Lansoprazole
Omeprazoleb
Ranitidinea,b
Nonsteroidal antiinflammatory agents
Naproxena
Piroxicama
b-blockersAcebutolol
Oxprenolol
Lipid-lowering agents
Pravastatina
Simvastatina
Antimicrobials
Griseofulvina
Terbinafinea
Antihistamines
Cinnarizine/triethylperazine
Anticonvulsants
Phenytoina
Antimalarials
Hydroxychloroquinea
Sulfonylureas
Glyburidea
Chemotherapy
Taxotere (docetaxel)a
Tamoxifen
Others
Bupropiona
Etanercept/infliximaba
Interferon alfaa
Insecticides
d-Penicillamineb
Procainamide
Leflunomidea
Tetracycline derivatives (COL-3)a
Tiotropium (inhaled)
Reproduced with publisher’s permission from Reference 67.a Reported to be capable of producing photosensitive skin reactions
in individuals without SCLE.b Unpublished personal observation by the authors of SCLE
induction with drug in question.
Manifestations of lupus erythematosus 351
atus, symmetrical erythema centrifugum, autoimmune an-
nular erythema, and LE gyratum repens.
Subacute cutaneous LE presents with erythematous mac-
ules and papules that subsequently develop into papulosqu-
amous or annular plaques. Most patients tend to develop
predominantly one type of lesion, although some will display
the elements of both simultaneously. Subacute cutaneous LE
is highly photosensitive, with lesions being seen most
commonly on the V area of the neck and upper chest, upper
back, shoulders, extensor surfaces of the arms and forearms,
and dorsum of the hands (the knuckles are typically spared)
(Fig. 2). Interestingly, the face and scalp are much less
commonly involved. Subacute cutaneous LE occurs infre-
quently below the waist. Less-common presentations of SCLE
include appearance simulating erythema annulare centrifu-
gum,2 erythema multiforme,9 and Rowell’s syndrome (lesions
resembling erythema multiforme with La/SS-B antibodies).2
Progression of annular SCLE lesions may include develop-
ment of vesicles and crusting.2,9-11 Subacute cutaneous LE has
been reported to occasionally produce a clinical picture
resembling toxic epidermal necrolysis.12 Other rare variants
of SCLE include exanthematous,9 pityriasiform,9,13 follicular
erythematous,2 acral annular presentation,14 and exfoliative
erythroderma.15 Lesions resolve without scarring; however,
there can be vitiligolike leukoderma that may last for a
significant amount of time and can be permanent.2
A growing number of drugs have been noted to induce
SCLE (Table 1). These medications include phenytoin,
diltiazem, thiazides, tumor necrosis factor inhibitors,
terbinafine, and antihistamines, among others. Interestingly,
systemic medications used to treat SLE, including hydrox-
ychloroquine and quinacrine, have also been implicated in
the development or worsening of cutaneous LE lesions.16
Drug-induced LE classically cannot be differentiated from
idiopathic cutaneous LE lesions based on histopathology
alone. Possible clues to drug-induced lupus include blood
or tissue eosinophilia and histologic findings of lymphocyte
migration into the acrosyringium as well as palisading
granulomatous inflammation in the interstitium.16,17 Dis-
continuation of the causative drug can but does not always
result in resolution of lesions.18
Patients with SCLE often have mild systemic disease
activity associated with the cutaneous outbreak. This
systemic activity is most commonly musculoskeletal with
associated serologic evidence of disease activity, most
commonly including 70% that are anti-Ro (SS-A).19 Anti-
Ro/SS-A has been associated with photosensitivity in 90%
of patients with SCLE.20 Severe central nervous system,
progressive renal, and severe systemic vasculitis are
uncommon in association with SCLE, occurring in no more
than 10% of SCLE cases.
HistopathologyThe histopathology of SCLE is of LE-specific skin disease
but cannot always be differentiated from the lupus-specific
skin diseases ACLE and DLE. The classic findings of
LE-specific skin disease, such as hyperkeratosis, degenera-
tion of the basal cell layer, and a mononuclear cell infiltrate in
the dermal-epidermal junction and dermis, are seen in
varying degrees in SCLE, ACLE, and DLE.

N. Rothfield et al.352
Focal liquefactive degeneration, sparse mononuclear
infiltrates in the upper one third of the dermis (usually in
the perivascular and adnexal areas), dermal edema, and
infrequent necrosis of the epidermis are seen in SCLE.21
The epidermis may be mildly atrophic, and there may be
vesicular changes at the active border.10,11,22 Typically,
SCLE lesions have less follicular plugging, hyperkeratosis,
adnexal mononuclear cell infiltrates, and dermal melanoph-
ages as compared with DLE lesions.2
Chronic cutaneous LE
Chronic cutaneous LE is subdivided into classic DLE,
hypertrophic/verrucous DLE, LE profundus/LE pannicu-
litis, mucosal DLE, lupus tumidus, chilblains lupus, lichen
DLE, and other rare variants.
Classic DLE is the most common form of CCLE and
occurs in 20% of patients with SLE.1 Most patients
having classic DLE lesions never develop features of
SLE, however. The disease presents as a well-demarcated
red-purple macule or a papule with a superficial scale.
This lesion increases in size into a coin-shaped, or
discoid, plaque with peripheral hyperpigmentation sec-
ondary to inflammation. There are increased adherent
scales with extension into dilated hair follicles. The center
of the lesion becomes depressed with scarring, depigmen-
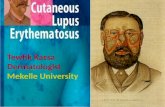
tation, and telangiectasia. In some cases, the plaques
extend into adjacent plaques, forming large disfiguring
lesions (Fig. 3).
Fig. 3 Chronic cutaneous LE. Left panel, An early lesion showing ker
standing lesion showing dermal scarring and disfiguring pigmentary cha
The hair follicle becomes plugged by thick scales.
Peeling the back of the scale of a DLE lesion can reveal
keratotic spikes protruding from the undersurface. These are
referred to as a carpet tack sign. Progression of follicular
involvement can result in scarring alopecia.
These DLE lesions are most commonly on the scalp,
face, ears, V region of the neck, and extensor surfaces of the
arms. As does ACLE, DLE spares the nasolabial folds.
Discoid LE lesions can occasionally occur anywhere on the
body, including areas that are not exposed to the sun.2 The
scalp as well as the external canal and conchal bowl of
the ears are common locations of DLE lesions that are not
related to sunlight exposure.
Scalp involvement occurs in approximately 60% of
patients with DLE, and the scalp can be the only involved
region in approximately 10%.23 Permanent scarring alopecia
occurs secondary to follicular destruction and has been
noted in 34% of patients in one study.24 In contrast, DLE
lesions occurring solely below the neck are much less
common; they are typically seen on the extensor surfaces of
the hands, forearms, and arms.2 Patients exhibiting classic
DLE lesions above and below the neck (generalized DLE)
have a somewhat higher risk of developing clinically
significant SLE as compared with those having lesions only
above the neck (localized DLE).
Nail involvement in DLE is also common.25,26 Nail plate
dystrophy is a manifestation of the DLE lesion in the nail
plate itself. Other nail involvements secondary to other
types of cutaneous lupus can also occur and may include
atotic follicular plugging and dermal atrophy. Right panel, A long-
nges.

Manifestations of lupus erythematosus 353
pitting, leukonychia striata, onycholysis, clubbing, nail bed
erythema, and telangiectasia.2,25
Variants of DLE include palmoplantar and follicular
DLE. Painful palmoplantar DLE is an erosive variant
that can be difficult to manage.2,27,28 Follicular DLE is
characterized by approximately 1-cm follicular papules that
are most commonly located in the elbow region.
The Koebner phenomenon (isomorphic response) is
defined as the tendency for skin lesions of a disease to
develop in areas of nonlesional skin that have undergone
trauma. It is seen in patients with cutaneous LE.2,29 Trauma;
exposure to UV, cold, and X ray; infection; diathermy;
chemical burns; various types of dermatitis; and scars have
been noted as triggers to outbreak of DLE lesions.2,29,30
Ueki29 noted a latent period of 4 weeks after the trauma
toward development of cutaneous LE lesions. Sunlight
exposure is a trigger for DLE lesions, although not as
significantly as for ACLE and SCLE lesions. It has been
noted that UV-B is a trigger for DLE lesion outbreak,
although there are evidence that long-wave UV-A is a
trigger as well.2,31-34 Recent evidence postulate that there is
a UV-induced cycle that leads to an amplified production of
chemokines, apoptosis, and necrosis, subsequently causing
autoimmune T-cell activation, as well as plasmacytoid
dendritic cells, which produce interferon alfa. It is thought
that this increases subsequent chemokine production
and invasion of leukocytes, which may lead to cutaneous
LE manifestations.35
Hypertrophic, or verrucous, DLE is a variant in which
the hyperkeratotic element of DLE is the predominant
feature. The lesions are most commonly noted on the
face, upper back, extensor surfaces of the arms,3 as well
as the palms and soles. Lupus planus has been the term
used to describe the lesion with overlapping features of
hypertrophic LE and lichen planus. In addition, a rare
variant of hypertrophic DLE, referred to as LE hyper-
trophicus et profundus, produces a facial lesion with
violet-red, thick, and rolled edges as well as significant
central atrophy.3
Lupus erythematosus profundus, also referred to as LE
panniculitis when there is solely subcutaneous involve-
ment,3 is a rare form of CCLE that has been reported in
1% to 3% of patients with cutaneous LE.36-38 There is
involvement of the deep dermis and subcutaneous fat.
Lesions are firm mobile 1 to 3-cm nodules with adherent
overlying skin creating superficial depression in the skin.3,39
The most common locations include the head, trunk,
breasts, proximal extremities, and buttocks.3 Approximately
50% of patients with lupus panniculitis will also have
overlying skin changes of classic DLE or classic DLE
lesions elsewhere on their bodies.
Diagnosis of LE profundus can be challenging because it
can often mimic other lesions. A recent study by Massone
et al36 demonstrated that histopathologic differentiation can
be used to distinguish it from subcutaneous panniculitis–like
T-cell lymphoma. The histopathologic criteria of LE
profundus recommended for use in differentiation include
presence of epidermal involvement, lymphoid follicles with
reactive germinal centers, mixed cell infiltrates with
significant plasma cells, and groupings of B lymphocytes.
In addition, polyclonal T-cell receptor–c gene rearrange-
ment is another feature of LE profundus that could
distinguish it from malignant lesions.36 Significant facial
involvement can mimic lipatrophy.3 Lupus erythematosus
panniculitis lesions within breast tissue can resemble breast
carcinoma clinically and radiographically. This has been
referred to as lupus mastitis.3,39
Mucosal DLE presents as an erythematous papule in the
oral, nasal, conjunctival, or genital mucosa that progresses
into a chronic plaque. The oral mucosa is the most common
site, with the buccal mucosa being the most frequent oral
site. Chronic plaques are sharply demarcated with irregular
white borders with peripheral telangiectasia and radiating
white striae. Lesions can mimic lichen planus.3 Superficial
palatal lesions can have a honeycomb appearance. Compli-
cations include painful ulceration and malignant transfor-
mation to squamous cell carcinoma.3
Lupus tumidus (urticarial plaque cutaneous LE variant)
demonstrates erythematous beefy and indurated plaques
with minimal superficial change. Histopathologically, there
are increased deposition of mucin and inflammation of the
superficial periadnexal and perivascular areas.3 Evidence
supporting lupus tumidus as a subset of CCLE have been
noted in case and cohort studies.3,40,41
Chilblains lupus (periodic LE) is a variant of CCLE in
which red-purple papules and plaques develop in response to
cold temperatures and humidity. The lesions can evolve
over time into atrophic plaques with scarring and telangiec-
tasia that are indistinguishable from chronic DLE lesions.
Lesions typically occur on the fingers, toes, and face.
These lesions are similar clinically and histologically to
idiopathic chilblains.
HistopathologyClassic DLE demonstrates hyperkeratosis and follicular
plugging. There is characteristic loss of organized basal
epidermis, whereas the spinous layer of the epidermis may
be atrophic. Other changes in the basal layer of the epidermis
include edema, liquefactive degeneration, epidermal base-
ment membrane thickening, increased formation of melanin
pigment, and pigment incontinence. There is a mononuclear
cell infiltrate of macrophage and T lymphocytes in the
dermis, with plasma cells in chronic lesions at times leading
to significant mucin deposition. The inflammatory infiltrate
can extend deeper as compared with ACLE and SCLE
lesions, with invasion into the reticular dermis.2
Lupus erythematosus–nonspecific skin disease
Lupus erythematosus–nonspecific skin disease includes
many skin changes that are frequently associated with LE
but are not specific to the disease itself. The lesions most
commonly occur in association with SLE.

N. Rothfield et al.354
Nonscarring alopecia occurs in various forms in associ-
ation with LE. Lupus hair is the term for thin hair and
nonscarring alopecia that is typically in the peripheral scalp
during disease flares.2,3 Telogen effluvium can occur in the
context of SLE as a transient phenomenon, also occurring
during increased LE activity.2 Alopecia areata occurs more
rarely in association with LE. Nonscarring alopecia can also
result from drugs that are used to treat systemic LE activity
(eg, methotrexate, cyclophosphamide).
Vasculitis lesions typically present in the skin of patients
with LE as small-vessel leukocytoclastic vasculitis. Clini-
cally, dependent palpable purpura or urticarial vasculitis
lesions result. Less commonly, larger vessels in the deep
dermis and subcutaneous tissue are affected, producing
periarteritis nodosa–like lesions resulting in nodules and/or
ulceration. Cutaneous vasculitis has been reported in 20%
to 70% of patients with SLE.3 Other vascular lesions such
as Degos’ disease–like lesions, livedo reticularis, and
secondary atrophie blanche may occur in association with
the antiphospholipid antibody syndrome.42 Periungual
telangiectasia occurs in 10% to 15% of patients with
SLE43 but is seen more often and more prominently in
those with dermatomyositis and systemic sclerosis. Ray-
naud’s phenomenon has been reported in 18% to 46% of
patients with SLE.3
Other lesions that have been noted in association with
LE include rheumatoid nodules, sclerodactyly, bullous
lesions, calcinosis cutis, thrombophlebitis, urticaria, eryth-
romelalgia, papulonodular mucinosis, cutis laxis/aneto-
derma, acanthosis nigricans, erythema multiforme, leg
ulcers, and lichen planus.
Cutaneous manifestations have been associated with the
antiphospholipid antibody syndrome. The antiphospholipid
syndrome denotes the clinical association between the
presence of antiphospholipid antibodies and a syndrome
of hypercoagulability. The syndrome may occur in certain
infectious diseases or in the absence of any disease; it may
occur in patients with SLE. The hypercoagulability results
in arterial and venous thromboses. It is also associated
with a high proportion of pregnancy losses after 10 weeks
of gestation. Livedo reticularis is seen in patients with
SLE with and in those without the antiphospholipid
antibody syndrome. It is seen in 11% to 22% of
patients with the antiphospholipid syndrome.44,45 Splinter
hemorrhages, leg ulcers, blue toe syndrome, and skin
infarcts may also be seen. The pathology involves the
presence of thrombotic microangiopathy, and true vascu-
litis is not seen.
Immunopathology/Lupus band test
The lupus band test is commonly discussed in reference to
the systemic and cutaneous manifestations of SLE. Immu-
noglobulins and complement proteins were first identified on
the dermal-epidermal junction of LE lesional skin biopsy
specimens, and this phenomenon has been referred to as the
lupus band.46 Although initially thought to be specific for LE,
the lupus band has been found in other skin diseases.47
Immunoreactant deposits in the nonlesional skin of
patients with LE were first noted by Burnham and Fine.48
Similar deposits in normal skin have been reported in
patients with rheumatoid arthritis, Sjfgren’s syndrome,
scleroderma, Raynaud’s syndrome, polydermatomyositis,47
and lepromatous leprosy.49
Because there has been controversy about the terminol-
ogy of this test, it has been proposed that using the terms
lesional lupus band test and nonlesional lupus band
test would minimize confusion between the types of test
being studied.2
The strongest association of a positive nonlesional lupus
band test finding has been with SLE. It is therefore also
logical that patients with DLE without extracutaneous
disease have negative lupus band test findings.23 One
study reported that 25% of patients with SLE who have
DLE lesions had positive nonlesional lupus band test
findings.23 There is controversy about the diagnostic
specificity of the nonlesional lupus band test. It has been
shown that there is a very high diagnostic specificity with
the presence of 3 or more immunoreactants.2,47,50 It is
important to note that sun-damaged skin can have a false-
positive nonlesional lupus band test result; therefore, the
greatest specificity is in nonlesional skin from sun-
protected regions with 3 or more immunoreactants pres-
ent.2,47 Serial studies on nonlesional skin showed an
association between the presence of immunoglobulins as
well as complement proteins and the clinical as well as
serologic disease activity of the systemic disease.51
There are few published studies on direct immunofluo-
rescence in ACLE. One study noted 5 of 5 ACLE lesional
skin biopsy specimens to have positive lesional lupus band
test results.2
In SCLE, DLE, and ACLE, more than 60% of patients
have proteins in their lesional skin.22 In biopsy specimens of
lesional skin, therefore, the presence of bandlike granular
deposits on direct immunofluorescence does help confirm
the diagnosis of SLE, but a negative test finding does not
rule out the diagnosis of lupus.
The diagnosis of SLE should never depend on the
presence of immune deposits in the dermal-epidermal
junction of either involved or normal skin.
Other clinical manifestations
General features
Fatigue is present in nearly all patients with SLE during
periods of disease activity and can precede the appearance
of rashes or joint swelling. Fever is present in approximately
80% of patients at the time of diagnosis and may be of low
grade or spiking. Fever in a treated patient with SLE should
be considered to be a result of infection until proven

Manifestations of lupus erythematosus 355
otherwise. Weight loss is present in approximately 85% of
patients at the time of diagnosis unless the nephrotic
syndrome is present.
Cardiovascular manifestations
Clinically evident pericarditis is present in approximately
25% of patients. Pericardial tamponade is unusual. Myocar-
dial disease may cause myocardial infarction as a result of
arteritis early in the course of the disease in younger patients.
Myocardial infarction in corticosteroid-treated patients is an
important cause of death late in the course of the disease.
Raynaud’s phenomenon is present in approximately 20% of
patients and may precede the development of multisystem
disease. Cryoglobulinemia is commonly present in patients
with an onset of Raynaud’s phenomenon at the time of
diagnosis. Such patients also may have nephritis. Raynaud’s
phenomenon may disappear with treatment of the systemic
disease. Thrombotic episodes occur in patients with the
lupus anticoagulant (see discussion on the antiphospholipid
antibody syndrome).
Pulmonary manifestationsPleural involvement occurs in 40% of patients, and the
effusions are usually small or moderate. The fluid is a
transudate that contains the same immunoglobulins and com-
plement proteins as does the peripheral blood. An unusual
manifestation is lupus pneumonitis characterized by dyspnea,
rales, and areas of platelike atelectasis. This diagnosis should
be made only after a rigorous search for an infectious agent.
Pathologic abnormalities are common in autopsied lungs and
are usually nonspecific. Pulmonary hemorrhage caused by
pulmonary vasculitis is a rare but life-threatening manifesta-
tion. Pulmonary hypertension occurs rarely.
Renal diseaseClinical evidence of renal disease occurs in 50% of
patients, but pathologic abnormalities are present in
additional patients. Immunofluorescent studies on biopsy
specimens of autopsy material from nearly all patients
reveal deposits of immunoglobulins or complement pro-
teins. Mesangial immune deposits are present in nearly all
patients with and those without clinical evidence of lupus
nephritis. The type and severity of the renal disease bear no
relation to the presence of other manifestations of the
disease, which may be either severe or mild. The pathologic
diagnosis is made by performing renal biopsy, which may
reveal mesangial nephritis, diffuse proliferative nephritis, or
membranous nephritis. Sclerosing nephritis is seen in end-
stage renal disease. Interstitial nephritis may be found
frequently. The prognosis is good in patients who have focal
nephritis and in those with a serum creatinine level lower
than 1.3. Male patients have a poorer prognosis.
Nervous system disease
Peripheral neuropathy occurs in 14% of patients and is
usually sensory, but a mixed sensory-motor disturbance is
seen in approximately 5% of patients with typical asymmet-
ric involvement of mononeuritis multiplex. The episodes
occur during periods of disease activity in other systems.
Less commonly, a picture suggestive of the presence of the
Guillain-Barre syndrome is present. Cranial nerve signs
occur in approximately 16% of patients. Optic neuritis may
be one of the presenting manifestations, as well as transverse
myelitis. I am currently caring for 2 patients with SLE who
have developed classic multiple sclerosis. Central nervous
system involvement occurs most often as organic brain
syndrome and seizures. Seizures occur in approximately
15% of patients, usually at the onset of the disease rather than
late in its course. Grand mal seizures are most common, but
chorea, jacksonian fits, petit mal, and temporal lobe seizures
also occur. Organic brain disease characterized by impair-
ment of orientation, perception, and ability to calculate may
occur usually during the first year after diagnosis and usually
occurs in the setting of disease activity in other systems.
Severe headaches may occur along with other manifestations
of the disease. Cerebrovascular accidents occur in the
antiphospholipid antibody syndrome (see below).
Psychologic problems
Depression and anxiety are common in patients with SLE
and should be neither considered to be a part of the disease
nor treated with increasing corticosteroid doses. Patients
need reassurance and may require treatment with antide-
pressants and antianxiety medications.
Gastrointestinal manifestations
Abdominal pain is the most common symptom and may
be a result of mesenteric arteritis. Perforation of the small or
large intestines may occur. This manifestation occurs in
patients with disease activity in other systems. Pancreatitis
occurs rarely. Hepatomegaly is present in approximately
30% of patients and is more common in children. Liver
enzyme elevations may occur.
Spleen and lymph nodesSplenomegaly is present in 20% of patients and is more
common in children. Lymphadenopathy is present in
approximately 50% of patients with active disease.
Ocular manifestationsFifteen percent of patients have conjunctivitis or epis-
cleritis. Both manifestations are more common in patients
with extensive cutaneous manifestations. Retinal arteritis
may occur.
Parotid gland enlargement and Sjogren’s syndrome
Enlarged parotid glands may occur in approximately 8%
of patients, most of whom do not have xerostomia.
Associated Sjfgren’s syndrome may be present with a
positive Schirmer’s test finding in 20% of patients, a
positive parotid scan finding in 58%, and a positive lip
biopsy finding in 50%.52

N. Rothfield et al.356
Menstrual abnormalities and pregnancy
Cessation of menses during the initial 3 to 6 months of
treatment occurs frequently. Stillbirths and spontaneous
abortions are common in untreated patients with active
disease and are associated with the antiphospholipid
antibody syndrome (see below). Children may be born with
congenital heart block by mothers with SLE who have anti-
Ro antibodies.
Laboratory findings
One or more hematologic abnormalities are present in
nearly all patients with SLE who have active disease. Most
commonly, mild to moderate normocytic and normochro-
mic anemia is present. Coombs’ test–positive hemolytic
anemia occurs in approximately 10% of patients. Mild to
moderate leukopenia is present in 17% of patients, and
lymphopenia is also usually present during disease activity.
Mild thrombocytopenia is present in approximately one
third of patients, but less than 100,000 platelets/mm3 is
present in only 5%. Qualitative thrombocyte defects are
also common.53 The erythrocyte sedimentation rate is
elevated in nearly all patients with SLE and usually falls
to normal levels when the disease becomes inactive. Serum
C-reactive protein levels are elevated during disease
activity and in infected patients. Cryoglobulins of the
mixed IgG-IgM type are found in 10% of patients. Elevated
serum gamma globulin is present in 80% of patients with
active disease. Rheumatoid factor is present in 14% of
patients. Serum complement levels are depressed in active
disease in most patients.
Autoantibodies
Patients with SLE always have a positive antinuclear
antibody test finding; this test is an excellent screening test.
A titer of 1:160 is significant, but that of 1:40 may be found
in approximately 30% of healthy individuals. In addition,
the antinuclear antibody test finding is positive in many
other rheumatic diseases and is not diagnostic of SLE. A
negative antinuclear antibody test finding essentially rules
out the disease. Anti–double-stranded DNA is present in
approximately 70% of patients with SLE and is highly
specific for SLE. Anti-Sm antibodies are also highly
specific for SLE but are found in only 25% of patients.
Anti-DNA antibodies correlate with disease activity and
may disappear when the disease goes into remission,
whereas anti-Sm antibodies are present throughout the
course of the disease. Other autoantibodies such as anti-La
and anti-Ro are found in patients with SLE, those with
Sjfgren’s syndrome, and those with subacute cutaneous
lupus. Anti-Ro antibodies occur in patients with SLE who
have babies with congenital heart block or congenital SLE;
thus, it is important to determine whether anti-Ro is present
in all patients with SLE so that anti-Ro–positive patients can
be followed closely during a pregnancy. Antiribonucleo-
protein is found in SLE and systemic sclerosis. Antiphos-
pholipid antibodies, lupus anticoagulant, and a VDRL
(Venereal Disease Research Laboratories) test should be
ordered, and, if the results are positive, the patients should
be treated with a daily aspirin.
Complement proteins
C3 and C4 are frequently low during periods of active
disease and return to normal levels during disease remissions.
Precipitating factors
Sun exposure may induce the onset of SLE and cause
exacerbations of the disease. Infections, especially bacterial
infections, may occur before the onset of the disease or
cause an exacerbation. Infections especially occur before
clotting episodes in patients with antiphospholipid anti-
bodies. Surgery or any trauma that induces necrosis of tissue
and the release of nuclear antigens may cause an exacerba-
tion of SLE. Pregnancy is associated with the onset of lupus
during the last trimester or the postpartum period. Thera-
peutic abortions may also be followed by exacerbation of
the disease, especially in patients with active disease at the
time of the therapeutic abortion.
Treatment: systemic manifestations
Conventional agents
Systemic glucocorticoids are the standard form of
treatment for patients with SLE. Some patients require very
low doses of prednisone (V10 mg) to alleviate manifestations
of the disease. Patients with nephritis, central nervous system
lupus, or pulmonary hemorrhage may require very high
doses, and intravenous therapy is frequently recommended
to them. Cyclophosphamide and mycophenolate may be
used in conjunction with high doses of glucocorticoids.
Author, Naomi Rothfield, treats patients with rising anti-
DNA levels associated with falling complement levels with
an increased dose of prednisone because of experience with
onset of lupus nephritis in patients who were not treated so.
The newer agents in the treatment of severe SLE have
recently been reviewed.54 In patients with seizures, organic
brain disease, or transverse myelitis, intravenous bolus
glucocorticoids are used along with cyclophosphamide.
Significantly in patients whose renal biopsy specimens show
more than focal lupus nephritis, cyclophosphamide or
mycophenolate is given with corticosteroids. In systemic
vasculitis and pulmonary hemorrhage, intravenous bolus
glucocorticoids and cyclophosphamide are also used.
Antimalarials are effective in the treatment of cutaneous
manifestations of the disease and help in the treatment of
arthralgias, arthritis, and fatigue. They may also prevent
major damage to the kidneys and central nervous system.55

Manifestations of lupus erythematosus 357
We have shown that patients taking antimalarials have a
significantly higher bone density as compared with those
not taking antimalarials when all other factors are taken into
consideration.56
Nonsteroidal antiinflammatory drugsNonsteroidal antiinflammatory drugs may be effective in
the treatment of musculoskeletal manifestations of the
disease, but the risk of renal insufficiency is high and
I avoid the use of these agents.
Experimental agents
Stem cell transplantation preceded by high-dose chemo-
therapy has been studied in patients with severe SLE who
did not respond to corticosteroids plus intravenous cyclo-
phosphamide57 Fifteen patients were followed for 3 years
and had improvement. The European registry of autologous
stem cell transplantation cases reported remissions in 33 of
50 patients, in addition to 10 relapses and 12 deaths.58 A
report on immunoablation alone without stem cell support
described 14 patients with moderate to severe SLE
unresponsive to corticosteroids and immunosuppressive
therapy.59 The patients received 50 mg/kg of cyclophos-
phamide; all had improved at 10 to 47 months of follow-up,
and no death had occurred. Complete responses were
reported in 5 of the 14 patients.
Anti–B-cell antibodies have been used in SLE, and good
results have been reported in uncontrolled observational
studies.60-66 The largest study was on 90 patients who have
refractory SLE with a 3- to 40-month follow-up.61 A
decrease in disease activity was noted in 80% of the
patients, and the infusions were well tolerated, with adverse
events caused by hypersensitivity to the chimeric antibody
occurring in 10%. At present, there are a number of
multicenter double-blind clinical trials of anti–B-cell anti-
bodies in SLE being carried out. Dehydroepiandrosterone
has been studied in a multicenter double-blind clinical trial
that used pharmaceutical-grade dehydroepiandrosterone.
There was no sufficient evidence of efficacy to warrant
US Food and Drug Administration approval.65,66 Over-the-
counter dehydroepiandrosterone products vary extensively
in potency and purity and are not recommended.
Treatment: cutaneous manifestations
Comments here will be directed at the treatment of LE-
specific skin diseases such as SCLE and CCLE. The second
author (RDS) has recently addressed this subject more
comprehensively elsewhere.67,68 Acute cutaneous LE (eg,
facial butterfly-shaped erythema reactions) and LE-nonspe-
cific skin lesions (eg, cutaneous vasculitis) are typically
seen in the context of active SLE. The systemic immuno-
modulatory/immunosuppressive treatments required to con-
trol the SLE activity will typically in a parallel fashion be of
benefit to the ACLE- and LE-nonspecific skin lesions.
Before beginning active treatment of LE skin disease,
one should consider the possibility of drug-induced cutane-
ous LE, especially drug-induced SCLE.69 Over the past
15 years, it has become increasingly clear that SCLE skin
lesions accompanied by circulating Ro/SS-A autoantibodies
can be found to be triggered by medications from a number
of drug classes.70-73 As such, recognition of this association
and withdrawal of the offending triggering drug can within
several months result in complete resolution of SCLE skin
disease activity without other active treatments. Table 1
shows an outline of the drugs that have been reported or
observed to be triggers for drug-induced SCLE.67,68
The initial management of all LE-specific skin diseases
should include education regarding protection from sunlight
and artificial sources of UV light and the avoidance if
possible of potentially provocative photosensitizing drugs
such as those indicated in Table 1. With regard to specific
medical therapy, local/topical measures should be maxi-
mized first and systemic agents should then be used if
significant disease activity continues.
Protection from UV light
Issues relating to photoprotection in patients with LE
have been discussed elsewhere in depth by one of the
authors.74
Physical protectionPatients should be advised to avoid direct sun exposure,
particularly during the midday hours and during the summer
months when the UV component of sunlight is least
attenuated by the atmosphere. Tightly woven clothing and
hats should be worn in conjunction with broad-spectrum
sunscreens to achieve maximal shielding from sunlight. The
use of broad-brimmed hats should be encouraged. Several
clothing lines offering maximized protection from UV light
are currently being marketed. Ultraviolet-light blocking
films can be applied to home and automobile windows.
Plastic/acrylic shields can be placed over fluorescent light
tubes to block the small amount of UV-B and UV-A
radiation that can leak from such sources.
Chemical sunscreensThe use of chemical sunscreens has been shown in
phototesting studies to be able to block the induction of
cutaneous LE lesions.75 Patients should select broad-
spectrum sunscreens that contain agents that block UV-B
with a sun protection factor (SPF) of 30 or greater. Under
everyday use conditions, the actual SPF of the product is
much lower than the advertised SPF. This is mainly because
patients tend to use much less of the product on their skin
than that used during the initial laboratory determination of
the SPF value for the product. In the United States,
preparations containing avobenzone (Parsol 1789), zinc
oxide, and titanium dioxide provide the broadest degree
of UV-A protection. Sunscreen products that contain the
highly effective chemical UV-A blocker, mexoryl SX

N. Rothfield et al.358
(eg, Anthelios L, La Roche-Posay Laboratoire), are cur-
rently available outside the United States. Mexoryl SX is
more resistant to photodegradation than the formulations of
avobenzone/Parsol 1789 that have previously been available
in the United States. Sunscreen products containing a
photostabilized form of avobenzone provided by the Helio-
plex technology have recently been introduced in the United
States (eg, Neutrogena Ultra Sheer Dry-Touch Sunblock
SPF 55), however.
Sunscreen products that are most resistant to being
washed off by sweating or bathing should also be selected.
Sunscreens should be applied at least 30 minutes be-
fore sun exposure and reapplied after bathing or apprecia-
ble perspiration.
Opaque corrective camouflage cosmetic products (eg,
Dermablend, Covermark) are designed to optimally conceal
pigmentary changes and scarring. These products offer the
dual benefit of being highly effective physical sunscreens
and aesthetically pleasing cosmetic masking agents for
patients suffering psychologically from chronic disfiguring
skin disease as a result of cutaneous LE.76 The proper use of
such products can improve the quality of life of patients.77
Local corticosteroids
TopicalInitial treatment usually includes daily application of a
formulation containing a medium-strength topical cortico-
steroid (eg, triamcinolone acetonide 0.1%). If this does not
provide adequate relief, more potent topical corticosteroids
such as clobetasol propionate 0.05%, betamethasone dipro-
pionate 0.05%, diflorasone diacetate 0.05%, and amcino-
nide 0.1% can be tried. Daily application of these products
to lesional skin for 2 weeks followed by a 2-week rest
period off treatment can lower the risk of local complica-
tions such as steroid atrophy and telangiectasia and that of
systemic absorption. Cutaneous LE represents one of the
very few clinical situations in which such potent topical
fluorinated corticosteroids can be recommended for use on
atrophy-prone areas such as the face because the alternatives
are disfiguring skin disease and risk of side effects from
systemic therapy. Unfortunately, topical corticosteroids
alone do not provide adequate improvement for most
patients with cutaneous LE.
IntralesionalIntralesional corticosteroid therapy (triamcinolone hex-
acetonide using a 30-G needle) is practical in some settings
such as localized DLE. Side effects are dose dependent and
include subcutaneous atrophy and leukoderma at the
injection sites. Patients with SCLE typically have too many
lesions for this approach to be tolerated, however.
OralIt is a good policy to avoid oral corticosteroid therapy as
much as possible in patients having isolated forms of
cutaneous LE because of the risks of side effects (eg,
avascular bone necrosis). Burst and taper oral pred-
nisone therapy can be of benefit, however, while waiting
for slower-acting agents such as antimalarials to become
fully effective.
Local calcineurin inhibitors
Several topical formulations of the calcineurin inhibitors
tacrolimus and pimecrolimus have been examined in
cutaneous LE, including SCLE.78-80 It has been one of the
authors’ personal experience (RDS) that LE lesions on facial
skin can respond to these preparations better than LE skin
lesions on other parts of the body can. It is hoped that
higher-strength formulations of tacrolimus/pimecrolimus
that are currently being developed will have greater clinical
efficacy in cutaneous LE, as has been observed anecdotally
with compounded formulations.79
Antimalarials
Although a number of systemic medications have been
reported anecdotally to be of benefit to patients with
cutaneous LE, by far, those having the highest safety-
benefit ratios are the aminoquinoline antimalarial agents. In
addition, hydroxychloroquine is one of the few drugs that
have been proven by controlled clinical trials to be of
benefit in cutaneous LE.81,82 There is general agreement
within the academic dermatology community that approx-
imately 75% of patients with SCLE will respond to single-
agent or combination antimalarial therapy. The 3 agents
most frequently prescribed in the United States for patients
with SCLE are hydroxychloroquine sulfate (Plaquenil,
Sanofi-Synthelabo), chloroquine phosphate (Aralen,
Sanofi-Synthelabo), and quinacrine (currently available in
the United States only as a compounded formulation of
the dihydrochloride salt that must be encapsulated). In
general, hydroxychloroquine is best tolerated with the least
side effects.
Therapy with hydroxychloroquine alone should be tried,
initially starting at 6.5 mg/kg per day in 2 divided doses
(~400 mg/d for the average-sized person). Hydroxychlor-
oquine reaches steady-state levels in 6 to 8 weeks, and its
full clinical efficacy cannot be judge before then. Its full
clinical effects can take even longer. If there is no significant
improvement by 2 to 3 months, 100 mg/d of quinacrine can
be added to the hydroxychloroquine.83-86 If the response is
inadequate after 4 to 6 weeks of combined hydroxychlor-
oquine and quinacrine therapy, 250 mg/d of chloroquine can
be substituted for the hydroxychloroquine in this combina-
tion because an occasional patient with cutaneous LE will
respond better to chloroquine than to hydroxychloroquine.
Hydroxychloroquine and chloroquine should not be used
concurrently because of the enhanced risk of developing
retinopathy. Once disease activity is controlled, the hydrox-
ychloroquine can be decreased to 200 mg/d for mainte-
nance. Authorities recommend a treatment period of 1 to
2 years to fully suppress cutaneous LE activity. As noted

Manifestations of lupus erythematosus 359
previously, there is evidence that cigarette smoking through
unknown mechanisms can interfere with the efficacy of
antimalarials in cutaneous LE and/or directly exacerbate
cutaneous LE activity.
It should also be realized that the aminoquinoline
antimalarials, especially hydroxychloroquine, are being
increasingly recognized to have a salutary effect on the
extracutaneous manifestations of SLE (Canadian Hydroxy-
chloroquine Study Group, 1991; Molad, 2002). The
malaise, fatigue, and arthralgia that patients with cutaneous
LE can experience can thus respond to antimalarials
that have been given to control cutaneous LE disease
activity. As with the cutaneous LE disease activity, the
musculoskeletal manifestations of patients with cutaneous
LE will take several months to be fully impacted after
starting antimalarials.
When using either hydroxychloroquine or chloroquine,
ophthalmologic monitoring is required to minimize the risk
of retinal toxicity (quinacrine is not retinopathic). A baseline
ophthalmologic evaluation should be obtained before
starting antimalarial therapy to document any preexisting
change that might otherwise be attributed to the medication.
The frequency with which patients are subsequently
monitored has been debated. The most recent set of
guidelines published by the American Academy of Oph-
thalmology in April 200287 suggests that this should be
repeated at yearly intervals in complicated patients (ie, those
taking antimalarials for N5 years; those taking larger-than-
recommended daily doses; those having high body fat
levels; those having concomitant kidney or liver disease;
and those who are N60 years old). These guidelines have
indicated that uncomplicated patients should have repeat
ophthalmologic examinations every 5 years.
This ophthalmologic evaluation should at minimum
include a funduscopic examination, visual field testing
(including central fields with a red object), and visual
acuity testing. Use of the self-administered Amsler grid at
home to detect the earliest evidence of visual field defects
has become popular. Retinal changes can become irrevers-
ible if not detected early. It has been suggested that the risk
of retinal toxicity is minimized when the total daily dose of
hydroxychloroquine does not exceed 6.5 mg/kg per day
(3.5 mg/kg per day for chloroquine). There does not appear
to be an upper limit on the safe total lifetime dose of these
drugs if these daily maximum dosing recommendations are
not exceeded.
Periodic assessments of hematologic and hepatic func-
tion are carried out by most dermatologists during
the hydroxychloroquine and chloroquine therapy to identify
the occasional patient who will suffer an idiosyncratic
reaction. It should be noted however that when using
hydroxychloroquine for rheumatoid arthritis, the American
College of Rheumatology guidelines indicate that no such
routine hematologic monitoring is necessary.88 It should be
noted that full-dose hydroxychloroquine or chloroquine
therapy in an individual having subclinical porphyria
cutanea tarda can produce an acute hepatotoxic reaction
that can in turn produce symptoms simulating an acute
surgical abdomen. Quinacrine hydrochloride is more likely
to induce hemolysis in glucose-6-phosphate dehydroge-
nase–deficient patients than is hydroxychloroquine or
chloroquine, and routine hematologic monitoring should
be carried out with this agent. Neurotoxicity and muscular
toxicity (including cardiotoxicity) can occur with the
aminoquinoline antimalarials but were much more of a
problem in the past when much higher daily doses of these
drugs were used.
Antimalarial agents can induce a number of dermato-
logic changes. All can cause a blue-black pigmentation of
the skin (particularly in sun-exposed areas), palatal mucosa,
nails, and pretibial surfaces. They can also rarely cause
bleaching of lightly pigmented hair, although this is rare
with currently recommended daily doses. Quinacrine
frequently causes diffuse yellowing of the skin, sclera,
and bodily secretions that are fully reversible on discon-
tinuation of the drug. On occasion, quinacrine produces a
lichenoid drug reaction that can be the harbinger of severe
bone marrow toxicity if the drug is not discontinued.89 The
lichenoid drug eruptions that can be produced by all of the
aminoquinoline antimalarials can simulate the appearance
of cutaneous LE lesions, including SCLE, resulting in a
highly confusing clinical setting.16
Other systemic antiinflammatory agents
Other systemic antiinflammatory drugs that might be
considered in an antimalarial-refractory patient with cuta-
neous LE include dapsone 90-92; isotretinoin (Accutane) and
acitretin (Soriatane) 82,93; thalidomide 94,95; gold (auranofin;
Ridaura, aurothiomalate; aurothioglucose) 96; and clofazi-
mine.97 With rare exception, however, it should be noted
that these agents had been used only anecdotally in
cutaneous LE. Among these agents, thalidomide is probably
the most uniformly beneficial and rapidly acting agent. This
drug carries a number of risks other than its well-known
teratogenicity (eg, sensory neuropathy, hyperacoagulable
state induction in the setting of antiphospholipid antibody
production, secondary amenorrhea), however.
Experimental therapy
Ultraviolet-A1 phototherapyPreliminary animal work has suggested that UV-A (320-
400 nm) irradiation might dampen the autoimmune abnor-
malities in experimental murine models of SLE.98 In
addition, small controlled trials from 2 groups of inves-
tigators have suggested that patients with SCLE might
actually benefit from very low doses of whole-body UV-A1
irradiation (340-400 nm).99-101 The true value of this
somewhat controversial form of treatment remains to be
confirmed by controlled studies in larger groups of patients,
however. Caution should be taken in interpreting these data

N. Rothfield et al.360
in view of the evidence that UV-A, including long-wave
UV-A1, can play an exacerbating role in the cutaneous
manifestations of SLE.102
Recombinant biologic response modifiersVariant tumor necrosis factor–a gene expression has been
implicated as a predisposing genetic factor for SCLE. This
and the remarkable efficacy of thalidomide, a known
inhibitor of tumor necrosis factor–a expression, in SCLE
and other forms of cutaneous LE have suggested the
possibility that the recombinant tumor necrosis factor–ainhibitors (eg, etanercept, infliximab, and adalimumab)
might potentially be of benefit to patients with SCLE. A
drug-induced form of cutaneous LE, including SCLE, has
now been recognized as a potential complication of
treatment with this class of biologics. Despite this, there
exists an anecdotal report describing rapid improvement of
SCLE in a patient with rheumatoid arthritis who was treated
with etanercept.103
In addition, other recombinant biologics that interfere
with antigen-presenting cell/T-cell interaction that have
proven to be of benefit in psoriasis (alefacept, Amevive;
efalizumab, Raptiva) theoretically could be of benefit in
other T-cell–dependent autoimmune skin diseases such as
cutaneous LE. There is one recently published case of a
therapeutically refractory patient with SCLE who appeared
to have responded quickly and remarkably well to efalizu-
mab (Raptiva).104
B-cell–depleting recombinant biologics acting through
CD20, such as rituximab (Rituxan), have been recently
reported in preliminary studies to be of possible benefit in
humoral autoimmune diseases such as SLE and pemphi-
gus.105-109 It would be interesting to know what their impact
might be on cutaneous LE.
Acknowledgment
Dr Sontheimer’s contribution to the preparation of this
work was supported by the Richard and Adeline Fleischaker
Chair in Dermatology Research of the University of
Oklahoma Health Sciences Center.
References
1. Rothfield NF. Systemic lupus erythematosus: clinical aspects and
treatment. In: McCarthy EJ, editor. Arthritis and allied conditions: a
textbook of rheumatology. 11th ed. Philadelphia7 Lea & Febiger;
1989. p. 1022-48.
2. Costner MI, Sontheimer RD, Provost TT. Lupus erythematosus.
In: Sontheimer RD, Provost TT, editors. Cutaneous manifestations
of rheumatic diseases. 2nd ed. Philadelphia7 Lippincott Williams
and Wilkins; 2004. p. 15-64.
3. Costner MI, Sontheimer RD. Lupus erythematosus. In: Freedberg IM,
Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors.
Fitzpatrick’s dermatology in general medicine. 6th ed. New York7
McGraw-Hill; 2003. p. 1677-93.
4. Peterson KS, Wincester RJ. Systemic lupus erythematous: pathogen-
esis. In: Kooperman WJ, editor. Arthritis and allied conditions.
Philadelphia7 Lipincott Williams & Wilkins; 2000. p. 1.
5. Reveille JD, Moulds JM, Ahn C, et al. Systemic lupus erythematosus
in three ethnic groups: I. The effects of HLA class II, C4, and CR1
alleles, socioeconomic factors, and ethnicity at disease onset.
LUMINA Study Group. Lupus in minority populations, nature versus
nurture. Arthritis Rheum 1998;41:1161-72.
6. Sontheimer RD. The lexicon of cutaneous lupus erythematosus—a
review of personal perspective on the nomenclature and classifica-
tion of the cutaneous manifestations of lupus erythematosus. Lupus
1997;6:84-95.
7. Pinkus H. Lichenoid tissue reactions: a speculative review of the
clinical spectrum of epidermal basal cell damage with special
reference to erythema dyschromicum perstans. Arch Dermatol 1973;
107:840-6.
8. Cervera R, Khamashta MA, Font J, et al. Systemic lupus erythema-
tosus: clinical and immunologic patterns of disease expression in a
cohort of 1,000 patients. Medicine 1993;72:113-24.
9. Sontheimer RD. Subacute cutaneous lupus erythematosus. Clin
Dermatol 1985;3:58-68.
10. Grant JM. Annular vesicular lupus erythematosus. Cutis 1981;28:
90 -2.
11. Wechsler HL, Stavrides A. Systemic lupus erythematosus with anti-
Ro antibodies: clinical, histologic and immunologic findings. J Am
Acad Dermatol 1982;6:73-83.
12. Bielsa I, Herrero C, Font J, Mascaro JM. Lupus erythematosus and
toxic epidermal necrolysis. J Am Acad Dermatol 1987;16:1265-7.
13. Hymes SR, Russell TJ, Jordon RE. The anti-Ro antibody system.
Int J Dermatol 1986;25:1 -7.
14. Scheinman PL. Acral subacute cutaneous lupus erythematosus: an
unusual variant. J Am Acad Dermatol 1994;30:800-1.
15. DeSpain J, Clark DP. Subacute cutaneous lupus erythemato-
sus presenting as erythroderma. J Am Acad Dermatol 1988;19:
388 -92.
16. Geraminejad P, Stone MS, Sontheimer RD. Antimalarial lichenoid
tissue reactions in patients with pre-existing lupus erythematosus.
Lupus 2004;13:473-7.
17. Magro MC, Crowson AN, Schapiro BL. The interstitial granuloma-
tous drug reaction: a distinctive and pathologic entity. J Cutan Pathol
1988;2:72-8.
18. Werth VP. Clinical manifestations of cutaneous lupus erythematosus.
Autoimmun Rev 2005;4:296-302.
19. Sontheimer RD, Maddison PJ, Reichlin M, Jordan RE, Stasny P,
Gilliam JN. Serologic and HLA associations in subacute cutaneous
lupus erythematosus, a clinical subset of lupus erythematosus. Ann
Intern Med 1982;97:664 -71.
20. Mond CB, Peterson MG, Rothfield NF. Correlation of anti-Ro
antibody with photosensitivity rash in systemic lupus erythematosus
patients. Arthritis Rheum 1989;32:202-4.
21. Bangert JL, Freeman RG, Sontheimer RD, Gilliam JN. Subacute
cutaneous lupus erythematosus and discoid lupus erythematosus.
Comparative histopathologic findings. Arch Dermatol 1984;120:
332 -7.
22. Herrero C, Bielsa I, Font J, et al. Subacute cutaneous lupus
erythematosus: clinicopathologic findings in thirteen cases. J Am
Acad Dermatol 1988;19:1057-62.
23. Prystowsky SD, Herndon JH, Gilliam JN. Chronic cutaneous lupus
erythematosus (DLE): a clinical and laboratory investigation of
80 patients. Medicine (Baltimore) 1975;55:183 -91.
24. Wilson CL, Burge SM, Dean D, Dawber RPR. Scarring alopecia in
discoid lupus erythematosus. Br J Dermatol 1992;126:307-14.
25. Sontheimer RD. Clinical manifestations of cutaneous lupus eryth-
ematosus. In: Wallace DJ, Hahn BH, editors. Dubois’ lupus
erythematosus. 4th ed. Philadelphia7 Lea & Febiger; 1993. p. 285.
26. Kanwar J, Dhar S, Ghosh S. Involvement of nails in discoid lupus
erythematosus. J Assoc Phys India 1993;41:543.

Manifestations of lupus erythematosus 361
27. Ashinoff R, Werth VP, Franks Jr AG. Resistant discoid lupus
erythematosus of palms and soles: successful treatment with
azathioprine. J Am Acad Dermatol 1988;19:961 -5.
28. Parrish LC, Kennedy RJ, Hurley HJ. Palmar lesions in lupus
erythematosus. Arch Dermatol 1967;96:273-6.
29. Ueki H. Koebner phenomenon in lupus erythematosus with special
consideration of clinical findings. Autoimmun Rev 2005;4:219-23.
30. Rowell NR, Goodfield MJD. The bconnective tissue diseasesQ. In:Champioin RH, Burton JL, Ebling FJG, editors. Textbook of
dermatology. London7 Blackwell Scientific Publications; 1992.
p. 2163.
31. Wolska H, Blaszczyk M, Jablonska S. Phototests in patients
with various forms of lupus erythematosus. Int J Dermatol 1989;28:
98 -103.
32. Velthuis PJ, Van Weelden H, Van Wichen D, De la Faille HB.
Immunohistopathology of light-induced skin lesions in lupus eryth-
ematosus. Acta Derm Venereol (Stockh) 1990;70:93 -8.
33. Lehmann P, Holzle E, Kind P, Goerz G, Plewig G. Experimental
reproduction of skin lesions in lupus erythematosus by UVA and
UVB radiation. J Am Acad Dermatol 1990;22(2 Pt 1):181-7.
34. Nived O, Johansen PB, Sturfelt G. Standardized ultraviolet-A
exposure provokes skin reaction in systemic lupus erythematosus.
Lupus 1993;2:247 -50.
35. Meller S, Winterberg F, Gilliet M, et al. Ultraviolet radiation–induced
injury, chemokines, and leukocyte recruitment. An amplification cycle
triggering cutaneous lupus erythematosus. Arthritis Rheum 2005;52:
1504-16.
36. Massone C, Kodama K, Salmhofer W, et al. Lupus erythematosus
panniculitis (lupus profundus): clinical, histopathological and molec-
ular analysis of nine cases. J Cutan Pathol 2005;32:396-404.
37. Requena L, Sanchez Yus E. Panniculitis (Part II). Mostly lobular
panniculitis. J Am Acad Dermatol 2001;45:325.
38. Caproni M, Palleschi GM, Papi C, Fabbri P. Discoid lupus
erythematosus lesions developed on lupus erythematosus profundus
nodules. Int J Dermatol 1995;34:357-9.
39. Carducci M, Mussi A, Lisi S, Muscardin L, Solivetti FM. Lupus
mastitis: a 2-year history of a single localization of lupus erythema-
tosus mimicking breast carcinoma. J Eur Acad Dermotol Venereol
2005;19:260-2.
40. Ruiz H, Sanchez JL. Tumid lupus erythematosus. Am J Dermatopa-
thol 1999;21:356-60.
41. Kuhn A, Sonntag M, Richter-Hintz D, et al. Phototesting in lupus
erythematosus tumidus—review of 60 patients. Photochem Photobiol
2001;73:532-6.
42. Diogenes MJ, Diogenes PC, de Morais Carneiro RM, Neto CC,
Duarte FB, Holanda RR. Cutaneous manifestations associated with
antiphospholipid antibodies. Int J Dermatol 2004;43:632 -7.
43. Weinstein C, Miller MH, Axtens R, Littlejohn GO, Dorevitch AP,
Buchman R. Lupus and nonlupus cutaneous manifestations in
systemic lupus erythematosus. Aust N Z J Med 1987;17:501 -6.
44. Asherson RA, Khamashta MA, Ordi-Ros J, et al. The bprimaryQantiphospholipid syndrome: major clinical and serological features.
Medicine (Balitimore) 1989;68:366-74.
45. Alarcon-Segovia D, Perez-Vazquez ME, Villa AR, Drenkard C,
Cabiedes J. Preliminary classification criteria for the antiphospholipid
syndrome within systemic lupus erythematosus. Semin Arthritis
Rheum 1992;21:275-6.
46. Burnham TK, Neblett JR, Fine G. The application of fluorescent
antibody technique to the investigation of lupus erythematosus and
various dermatoses. J Invest Dermatol 1963;41:451.
47. Smith CD, Marino C, Rothfield NF. The clinical utility of the lupus
band test. Arthritis Rheum 1984;27:382-7.
48. Burnham TK, Fine G. The immunofluorescent band test for LE: III.
Employing clinically normal skin. Arch Dermatol 1971;103:24 -32.
49. Bullock WE, Callerame ML, Panner BJ. Immunohistologic alterna-
tional skin and ultrastructural changes in glomerular membrane in
leprosy. Am J Trop Med Hyg 1974;23:78 -86.
50. Font J, Cervera R, Navarro M, et al. Systemic lupus erythematosus in
men: clinical and immunological characteristics. Ann Rheum Dis
1992;51:1050-2.
51. Rothfield N, Marino C. Studies of repeat skin biopsies of nonlesional
skin in patients with systemic lupus erythematosus. Arthritis Rheum
1982;25:624 -30.
52. Matsopoulis HM, et al. Correlative histologic and serologic findings
of sicca syndrome in patients with systemic lupus erythematosus.
Arthritis Rheum 1980;23:36 -40.
53. Laurence J, Nachman R. Hematologic aspects of systemic lupus
erythematosus. In: Lahita RG, editor. Systemic lupus erythematosus.
New York7 John Wiley & Sons, Inc; 1987. p. 721-90.
54. Ginzler EM, Dvorkina O. Newer therapeutic approaches for
systemic lupus erythematosus. Rheum Dis Clin North Am 2005;31:
315 -28.
55. Fessler BJ, Alarcon GS, McGwin Jr G, et al. Systemic lupus
erythematosus in three ethnic groups: XVI. Association of hydroxy-
chloroquine use with reduced risk of damage accrual. Arthritis Rheum
2005;52:1473.
56. Lakshiminarayanan S, Walsh S, Mohanraj M, Rothfield N. Factors
associated low bone mineral density in female patients with systemic
lupus erythematosus. J Rheumatol 2001;28:102-8.
57. Traynor AE, Barr WG, Rose RM, et al. Hematopoietic stem cell
transplantation for severe and refractory lupus. Analysis after five
years and fifteen patients. Arthritis Rheum 2002;46:2917.
58. Jayne D, Tyndall A. Autologous stem cell transplantation for systemic
lupus erythematosus. Lupus 2004;13:359.
59. Petri M, Jones RG, Brodsky RA. High-dose cyclophosphamide
without stem cell transplantation in systemic lupus erythematosus.
Arthritis Rheum 2003;48:166.
60. Leandro MJ, Edwards JC, Cambridge G, et al. An open study of
B lymphocyte depletion in systemic lupus erythematosus. Arthritis
Rheum 2002;46:2673.
61. Sfikakis PP, Boletis JN, Tsokos GC. Rituximab anti–B-cell therapy in
systemic lupus erythematosus: pointing to the future. Curr Opin
Rheumatol 2005;17:550.
62. Leandro MJ, Cambridge G, Edwards JC, et al. B-cell depletion in
the treatment of patients with systemic lupus erythematosus:
a longitudinal analysis of 24 patients. Rheumatology (Oxford)
2005:44:1542.
63. Looney RJ, Anolik JH, Campbell D, et al. B cell depletion as a novel
treatment for systemic lupus erythematosus: a phase I/II dose-
escalation trial of rituximab. Arthritis Rheum 2004;50:2580.
64. Sfikakis PP, Boletis JN, Lionaki S, et al. Remission of proliferative
lupus nephritis following B cell depletion therapy is preceded by
down-regulation of the T cell costimulatory molecule CD40 ligand: an
open-label trial. Arthritis Rheum 2005;52:501.
65. Chang DM, Lan JL, Lin HY, Luo SF. Dehydroepiandrosterone
treatment of women with mild-to-moderate systemic lupus eryth-
ematosus: a multicenter randomized, double-blind, placebo-controlled
trial. Arthritis Rheum 2002;46:2924.
66. Petri MA, Mease PJ, Merrill JT, et al. Effects of prasterone on disease
activity and symptoms in women with active systemic lupus
erythematosus. Arthritis Rheum 2004;50:2852.
67. Sontheimer RD. Subacute cutaneous lupus erythematosus: a quarter
century’s perspective. In: Sarzi-Puttini P, Doria A, Girolomoni G,
Kuhn A, editors. The skin in systemic autoimmune diseases.
Amsterdam7 Elsevier; 2006. p. 65-86.
68. Sontheimer RD. Subacute cutaneous lupus erythematosus: 25-year
evolution of a prototypic subset (subphenotype) of lupus erythema-
tosus defined by characteristic cutaneous, pathological, immunolog-
ical, and genetic findings. Autoimmun Rev 2005;4:253 -63.
69. Reed BR, Huff JC, Jones SK, et al. Subacute cutaneous lupus
erythematosus associated with hydrochlorothiazide therapy. Ann
Intern Med 1985;103:49 -51.
70. Farhi D, Viguier M, Cosnes A, et al. Terbinafine-induced subacute
cutaneous lupus erythematosus. Dermatology 2006;212:59-65.

N. Rothfield et al.362
71. Matthes T, Hagedorn M. Terbinafine-induced subacute cutaneous
lupus erythematosus. Case report and review of the literature
[German]. Hautarzt 2004;55:653-7.
72. Srivastava M, Rencic A, Diglio G, et al. Drug-induced, Ro/SSA-
positive cutaneous lupus erythematosus. Arch Dermatol 2003;139:
45 -9.
73. Shapiro M, Sosis AC, Junkins-Hopkins JM, et al. Lupus erythema-
tosus induced by medications, ultraviolet radiation, and other
exogenous agents: a review, with special focus on the development
of subacute cutaneous lupus erythematosus in a genetically predis-
posed individual. Int J Dermatol 2004;43:87 -94.
74. Ting WW, Sontheimer RD. Local therapy for cutaneous and systemic
lupus erythematosus: practical and theoretical considerations. Lupus
2001;10:171-84.
75. Herzinger T, Plewig G. Use of sunscreens to protect against ultraviolet
induced lupus erythematosus. Arthritis Rheum 2004;50:3045-6.
76. Kaye ET, Levin JA, Blank IH, et al. Efficiency of opaque
photoprotective agents in the visible light range. Arch Dermatol
1991;127:351 -5.
77. Boehncke WH, Ochsendorf F, Paeslack I, et al. Decorative cosmetics
improve the quality of life in patients with disfiguring skin diseases.
Eur J Dermatol 2002;12:577-80.
78. Yoshimasu T, Ohtani T, Sakamoto T, et al. Topical FK506
(tacrolimus) therapy for facial erythematous lesions of cutaneous
lupus erythematosus and dermatomyositis. Eur J Dermatol 2002;12:
50 -2.
79. Walker SL, Kirby B, Chalmers RJG. The effect of topical tacrolimus
on severe recalcitrant chronic discoid lupus erythematosus. Br J
Dermatol 2002;147:405 -6.
80. Kreuter A, Gambichler T, Breuckmann F, et al. Pimecrolimus 1%
cream for cutaneous lupus erythematosus. J Am Acad Dermatol
2004;51:407-10.
81. Jessop S, Whitelaw D, Jordaan F. Drugs for discoid lupus
erythematosus. Cochrane Database Syst Rev 2001;CD002954.
82. Ruzicka T, Sommerburg C, Goerz G, et al. Treatment of cutaneous
lupus erythematosus with acitretin and hydroxychloroquine. Br J
Dermatol 1992;127:513 -8.
83. Toubi E, Rosner I, Rozenbaum M, et al. The benefit of combining
hydroxychloroquine with quinacrine in the treatment of SLE patients.
Lupus 2000;9:92-5.
84. Chung HS, Hann SK. Lupus panniculitis treated with a combination
therapy of hydroxychloroquine and quinacrine. J Dermatol 1997;24:
569 -72.
85. Lipsker D, Piette J-C, Cacoub P, et al. Chloroquine-quinacrine
association in resistant cutaneous lupus. Dermatology 1995;190:
257 -8.
86. Feldmann R, Salomon D, Saurat J-H. The association of the two
antimalarials chloroquine and quinacrine for treatment-resistant
chronic and subacute cutaneous lupus erythematosus. Dermatology
1994;189:425-7.
87. Marmor MF, Carr RE, Easterbrook M, et al. Recommendations on
screening for chloroquine and hydroxychloroquine retinopathy:
a report by the American Academy of Ophthalmology. Ophthalmol-
ogy 2002;109:1377 -82.
88. Anonymous. Guidelines for monitoring drug therapy in rheumatoid
arthritis. American College of Rheumatology Ad Hoc Committee on
Clinical Guidelines. Arthritis Rheum 1996;39:723-31.
89. Wallace DJ. The use of quinacrine (Atabrine) in rheumatic diseases:
a re-examination. Semin Arthritis Rheum 1989;18:282-97.
90. Holtman JH, Neustadt DH, Klein J, et al. Dapsone is an effective
therapy for the skin lesions of subacute cutaneous lupus erythema-
tosus and urticarial vasculitis in a patient with C2 deficiency.
J Rheumatol 1990;17:1222-5.
91. Fenton DA, Black MM. Low-dose dapsone in the treatment of
subacute cutaneous lupus erythematosus. Clin Exp Dermatol
1986;11:102-3.
92. McCormack LS, Elgart ML, Turner ML. Annular subacute cutaneous
lupus erythematosus responsive to dapsone. J Am Acad Dermatol
1984;11:397-401.
93. Furner BB. Subacute cutaneous lupus erythematosus response to
isotretinoin. Int J Dermatol 1990;29:587 -90.
94. Volc-Platzer B, Wolff K. Treatment of subacute cutaneous lupus
erythematosus with thalidomide. Hautarzt 1983;34:175-8.
95. Naafs B, Bakkers EJM, Flinterman J, et al. Thalidomide treatment of
subacute cutaneous lupus erythematosus. Br J Dermatol 1982;107:
83 -6.
96. Dalziel K, Going G, Cartwright PH, et al. Treatment of chronic
discoid lupus erythematosus with an oral gold compound (auranofin).
Br J Dermatol 1986;115:211 -6.
97. Mackey JP, Barnes J. Clofazimine in the treatment of discoid lupus
erythematosus. Br J Dermatol 1974;91:93-6.
98. McGrath Jr H, Bak E, Michalski JP. Ultraviolet-A light pro-
longs survival and improves immune function in (New Zealand
Black � New Zealand White) F1 hybrid mice. Arthritis Rheum 1987;
30:557-61.
99. McGrath Jr H. Prospects for UV-A1 therapy as a treatment modality
in cutaneous and systemic LE. Lupus 1997;6:209 -17.
100. Mcgrath H, Martinez-Osuna P, Lee FA. Ultraviolet-A1 (340-400 nm)
irradiation therapy in systemic lupus erythematosus. Lupus 1996;
5:269-74.
101. Polderman MC, Huizinga TW, Le Cessie S, et al. UVA-1 cold light
treatment of SLE: a double blind, placebo controlled crossover trial.
Ann Rheum Dis 2001;60:112-5.
102. Nived O, Johansen PB, Sturfelt G. Standardized ultraviolet-A
exposure provokes skin reaction in systemic lupus erythematosus.
Lupus 1993;2:247-50.
103. Fautrel B, Foltz V, Frances C, et al. Regression of subacute cutaneous
lupus erythematosus in a patient with rheumatoid arthritis treated with
a biologic tumor necrosis factor alpha–blocking agent: comment on
the article by Pisetsky and the letter from Aringer et al. Arthritis
Rheum 2002;46:1408-9.
104. Clayton TH, Ogden S, Goodfield MD. Treatment of refractory
subacute cutaneous lupus erythematosus with efalizumab. J Am Acad
Dermatol 2006;54:892 -5.
105. Saito K, Nawata M, Nakayamada S. Successful treatment with anti-
CD20 monoclonal antibody (rituximab) of life-threatening refractory
systemic lupus erythematosus with renal and central nervous system
involvement. Lupus 2003;12:798 -800.
106. Cooper HL, Healy E, Theaker JM, et al. Treatment of resistant
pemphigus vulgaris with an anti-CD20 monoclonal antibody (ritux-
imab). Clin Exp Dermatol 2003;28:366-8.
107. Herrmann G, Hunzelmann N, Engert A. Treatment of pemphigus
vulgaris with anti-CD20 monoclonal antibody (rituximab). Br J
Dermatol 2003;148:602 -3.
108. Perrotta S, Locatelli F, La Manna A, et al. Anti-CD20 monoclonal
antibody (rituximab) for life-threatening autoimmune haemolytic
anaemia in a patient with systemic lupus erythematosus. Br J
Haematol 2002;116:465-7.
109. Heizmann M, Itin P, Wernli M, et al. Successful treatment of
paraneoplastic pemphigus in follicular NHL with rituximab: report of
a case and review of treatment for paraneoplastic pemphigus in
NHL and CLL. Am J Hematol 2001;66:142-4.