Lung Microvessel Injury from Peritoneal Abscesses and Gram-Negative Bacteremia
17
MICROVASCULAR RESEARCH 52, 84–100 (1996) ARTICLE NO. 0046 BRIEF COMMUNICATION Lung Microvessel Injury from Peritoneal Abscesses and Gram-Negative Bacteremia 1 ROSEMARY JONES* AND ORLANDO C. KIRTON *Department of Anesthesia, Molecular and Cell Biology Laboratory, Massachusetts General Hospital- East, 149 Thirteenth Street, Charlestown, Massachusetts; Harvard Medical School, Boston, Massachusetts; and Department of Surgery/Division of Trauma, University of Miami School of Medicine, P.O. Box 016960 (D-40) Miami, Florida 33101 Received October 20, 1995 To analyze the effect of an extrathoracic focus of infection on lung vessel wall structure, we produced peritoneal abscesses in the rat, over a period of 3 to 7 weeks, by implanting capsules containing live gram-negative bacteria (3.0 1 10 7 Escherichia coli and 5.0 1 10 7 Bactercides fragilis) with an adjutant. We document here by arteriography, morphometric analysis, and high resolution microscopy, microvessel cell injury, and wall remodeling. In the sepsis-injured lung, both dilated and thick-walled microvessels are present. The walls of dilated vessels are disrupted by extensive endothelial and precursor smooth muscle cell injury. In thick-walled vessels these cells are hypertrophied, and the precursor smooth muscle cells express filaments, demonstrating a shift toward a contractile phenotype. Infiltrating monocytic cells focally consolidate alveolar regions. In the residual nonconsolidated regions, alveolar-capillary membrane cells are attenuated and the capillaries dilated. Vessel changes after 7 weeks are similar to those after 3 weeks but alveolar-capillary membrane injury is more extensive. These structural changes, including the development of precursor smooth muscle cells, may contribute to the known increase in reactivity of these lung vessels to challenge by vasoactive agents. q 1996 Academic Press, Inc. INTRODUCTION Gram-negative septicemia is a known cause and complication of the adult respiratory distress syndrome (ARDS). 2 As many as 30–40% of patients with ARDS develop sepsis syndrome or gram-negative sepsis, and the mortality rate of this group then doubles that of the ARDS group without sepsis [1]. Lung vascular injury is an im- portant feature of ARDS, regardless of etiology [2, 3]. 1 Supported by NHLBI ARF SCOR 23591 and by unrestricted funds from the Department of Anesthesia, MGH. 2 Abbreviations used: PMN, polymorphonuclear leukocyte; ARDS, adult respiratory distress syndrome; ED, external diameter; E. coli, Escherichia coli; B. fragilis, Bactercides fragilis; CFU, colony forming units; M, muscular; PM, partially muscular; NM, nonmuscular; PSMC, precursor smooth muscle cell; TNFa, tumor necrosis factor a; IL-1 and IL-8, interleukin 1 and 8. 84 0026-2862/96 $18.00 Copyright q 1996 by Academic Press, Inc. All rights of reproduction in any form reserved.
-
Upload
rosemary-jones -
Category
Documents
-
view
214 -
download
0
Transcript of Lung Microvessel Injury from Peritoneal Abscesses and Gram-Negative Bacteremia

MICROVASCULAR RESEARCH 52, 84–100 (1996)ARTICLE NO. 0046
BRIEF COMMUNICATION
Lung Microvessel Injury from Peritoneal Abscesses andGram-Negative Bacteremia1
ROSEMARY JONES* AND ORLANDO C. KIRTON
*Department of Anesthesia, Molecular and Cell Biology Laboratory, Massachusetts General Hospital-East, 149 Thirteenth Street, Charlestown, Massachusetts; Harvard Medical School, Boston,
Massachusetts; and Department of Surgery/Division of Trauma, University of MiamiSchool of Medicine, P.O. Box 016960 (D-40) Miami, Florida 33101
Received October 20, 1995
To analyze the effect of an extrathoracic focus of infection on lung vessel wall structure, weproduced peritoneal abscesses in the rat, over a period of 3 to 7 weeks, by implanting capsulescontaining live gram-negative bacteria (3.0 1 107 Escherichia coli and 5.0 1 107 Bactercidesfragilis) with an adjutant. We document here by arteriography, morphometric analysis, and highresolution microscopy, microvessel cell injury, and wall remodeling. In the sepsis-injured lung,both dilated and thick-walled microvessels are present. The walls of dilated vessels are disruptedby extensive endothelial and precursor smooth muscle cell injury. In thick-walled vessels thesecells are hypertrophied, and the precursor smooth muscle cells express filaments, demonstratinga shift toward a contractile phenotype. Infiltrating monocytic cells focally consolidate alveolarregions. In the residual nonconsolidated regions, alveolar-capillary membrane cells are attenuatedand the capillaries dilated. Vessel changes after 7 weeks are similar to those after 3 weeks butalveolar-capillary membrane injury is more extensive. These structural changes, including thedevelopment of precursor smooth muscle cells, may contribute to the known increase in reactivityof these lung vessels to challenge by vasoactive agents. q 1996 Academic Press, Inc.
INTRODUCTION
Gram-negative septicemia is a known cause and complication of the adult respiratorydistress syndrome (ARDS).2 As many as 30–40% of patients with ARDS developsepsis syndrome or gram-negative sepsis, and the mortality rate of this group thendoubles that of the ARDS group without sepsis [1]. Lung vascular injury is an im-portant feature of ARDS, regardless of etiology [2, 3].
1 Supported by NHLBI ARF SCOR 23591 and by unrestricted funds from the Department of Anesthesia,MGH.
2 Abbreviations used: PMN, polymorphonuclear leukocyte; ARDS, adult respiratory distress syndrome;ED, external diameter; E. coli, Escherichia coli; B. fragilis, Bactercides fragilis; CFU, colony formingunits; M, muscular; PM, partially muscular; NM, nonmuscular; PSMC, precursor smooth muscle cell;TNFa, tumor necrosis factor a; IL-1 and IL-8, interleukin 1 and 8.
84
0026-2862/96 $18.00Copyright q 1996 by Academic Press, Inc.All rights of reproduction in any form reserved.
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

85BRIEF COMMUNICATION
Widespread occlusion and obliteration both are common, as are dilated and tortuousvessels, especially in the microcirculation. Systemic release of gram-negative bacterialproducts, endotoxins, and other membrane fragments, acting directly or indirectlythrough proinflammatory mediators [4–6], are known to injure lung cells [7, 8] andto give rise to permeability edema, but structural changes in the microvessels of thelung, while long suspected, have not been demonstrated. In this study we demonstratethe effect on lung microvascular wall structure of episodes of bacteremia arising froman extrathoracic source, in a model of subacute gram-negative infection in the rat [9].
We used known concentrations of live aerobic and anaerobic organisms, and anadjuvant, to create multiple, small, peritoneal abscesses, and recurrent bacteremia,over a period of several weeks [9–11]. Since sepsis often is associated clinically withmajor abdominal surgery, or follows penetrating abdominal injury, an intraabdominalabscess model is appropriate to study [12]. Furthermore, the use of live organisms toproduce injury that progresses from a focus of infection more closely follows theclinical course of sepsis and so is preferable to the use of bolus intravenous injectionsof bacteria or endotoxin [1, 13]. As the criteria of peritoneal sepsis, we used a risein body temperature, culture from blood and abscesses of the implanted gram-negativeorganisms, and peripheral leukocytosis to monitor the course of bacteremia and toassess the repeatability of our model.
Increased permeability, and leukocyte infiltration, but not microvascular wall injuryand remodeling, has been reported in earlier studies of subacute lung injury fromsepsis induced either by inoculation of cecal contents into the peritoneal cavity or byinjection of bacteria [12, 14–17]. After cecal ligation and perforation, injury in theform of a thrombotic lesion in the wall of a large pulmonary artery has been described[18]. We have reported hemodynamic measurements, blood thromboxane B2, andprostacyclin levels and briefly described injury to the alveolar-capillary membrane inthis model [9]. Here, we describe structural changes in pre- and postcapillary vesselsegments (£100 mm in external diameter (ED)) and capillaries. While short (õ1 cm),these segments are numerous (Ç3001 106 alveoli each withÇ1000 capillary segmentsare present in human lung) and so represent an important site of injury.
MATERIALS AND METHODS
Implantation of capsules into rats. Male (250–300 g) Sprague–Dawley viral anti-body-free rats (Charles River Breeding Laboratories, Kingston, NY) were maintainedin accordance with Institutional guidelines. E. coli (0 serotype-054) from rat cecum(Dr. AB Onderdonk, State Laboratories, Boston, MA) and B. fragilis (23745 ATCC,Rockville, MD), with an adjuvant (filtered and autoclaved cecal contents from ratsfed chow for 2 weeks (n Å 20)), were mixed with an equal volume of tryptic soybroth to which barium sulfate (10% weight/vol) was added [19]. B. fragilis is essentialfor the formation of abscesses, its capsular polysaccharides reducing clearance byphagacytosis [20]. Organisms were recovered from log-phase growth (when theircapsule polysaccharides and lipopolysaccharide content were high). Their virulenceis enhanced by the addition of sterile cecal contents and their clearance from theperitoneum is slowed by the presence of barium [10, 19].
Double gelatin capsules containing 3.0 1 107 CFU/ml of E. coli and 5.0 1 107
CFU/ml B. fragilis suspended in an equal volume of adjuvant (total volume 0.5 ml/
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

86 BRIEF COMMUNICATION
capsule) were implanted into the abdominal cavity of anesthetized rats (3 mg/100 gbody weight sodium pentobarbital, i.p.). In 32 rats, the first capsule was implantedand thereafter an additional capsule was implanted weekly for 3 weeks (i.e., 4-implantswere placed over a 3-week period). Some of these rats were used for bacteriologicmonitoring (n Å 12). Similarly, in 6 animals a total of 8 capsules were implantedover 7 weeks. In this study we examine the effect on lung vessels of the products oflive bacteria and their associated endotoxins; the control rats were untreated (n Å24). We have previously confirmed that vascular findings in rats receiving capsulescontaining only sterile fecal content and barium (i.e., surgery and a relatively lowdose of endotoxin) are the same as for untreated rats [21]. Positive E. coli and B.fragilis cultures from blood drawn by cardiac puncture from anesthetized rats thathad received 1–4 implants confirmed that each caused a bacteremia that lasted 48 hr.There were thus 4 or 8 episodes of bacteremia, each lasting 2 days, with 5-day intervalsbetween. We isolated only E. coli and B. fragilis from blood and from peritonealabscesses (multiple abscesses õ1 mm were found in all sepsis rats at autopsy). Thetotal white blood cell count increased (from 12.2 { 1.2 1 103/mm3 to 19.18 { 2.01 103 after 4-implants and to 25.50 { 1.0 1 103/mm3 after 8-implants). The relativenumber of polymorphonuclear leukocytes (PMNs) increased after the 4th and 8thimplant (Px
2£ 0.05 and Px2£ 0.001, respectively). Body temperature fell immediately
after the first 2 implants and rose after the next 2 (P £ 0.01 versus the control valuefor rats receiving 4- or 8-implants on each occasion). Twenty-four hours after eachimplant body temperature returned to normal.
Lung preparation for arteriography and structural studies. Twenty-four hours afterthe last implant, rats were anesthetized (30 mg/100 g body weight sodium pentobarbi-tal, i.p.) and the thoracic block was excised. For arteriography, and morphometricstudies, the pulmonary arteries were injected (100 cm H2O) with a barium-gelatinsuspension [22, 23] via a catheter in the right ventricle (4-implants, n Å 10; controls,n Å 9); filling arteries from the lung hilum to periphery (i.e., §15 mm ED). Theairways were distended with 1% glutaraldehyde–4% formaldehyde (at 23 cm H2O)until the pleural surface was tense, and the lungs immersed in the same fixative for48 hr [22, 23]. Because of the limited number of lungs available from rats receiving8-implants none were available for this procedure. In all other lungs, the vascular bedand airways were similarly distended with fixative (4-implants, n Å 4; controls, n Å9). Lung sections (5 mm) were stained with hematoxylin and eosin or with an elastic-van Gieson, to demonstrate elastin, muscle, and collagen fibers [3]. For high resolutionstudies the vessels and airways were simultaneously distended with 2% glutaraldehydein 0.1 M cacodylate buffer (pH 7.2) as described (4-implants, n Å 6; 8-implants,n Å 6; controls, n Å 6). Thick lung sections (1 mm) were stained with 1% toluidineblue and thin sections (70 nm) with uranyl acetate and lead citrate.
Vessel analysis. We located arteries by their associated airway (preacinar—bronchi-olus, terminal bronchiolus; intraacinar—respiratory bronchiolus, alveolar duct, or al-veolar wall) [3, 24] and noted wall structure. We analyzed all preacinar arteries, and100 intraacinar ones, in lungs sections from each rat (4-implants, n Å 8; controls,n Å 6). In rat lung (as in human lung) arteries are fully muscular (M), partiallymuscular (PM), or nonmuscular (NM), the NM ones increasing distally. In consecutivemicroscopy fields (125 or 140 objective and 110 eyepiece), we measured the EDof all arteries and the thickness of the medial layer (MT) of smooth muscle cells in
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

87BRIEF COMMUNICATION
M and PM ones [3]. Results for group data were analyzed by Student’s t test and chi-squared analysis, and a P value £0.05 was considered significant.
In lung sections examined by transmission microscopy, in which the vessels weredistended with fixative, small arteries were not identified from small veins becauseof similar wall structure: We found striking cell changes in the walls of NM vesselsegments that normally consist of endothelial cells, basement membrane, and an elasticlamina, with precursor smooth muscle cells (PSMCs) forming only a thin, discontinu-ous, subendothelial layer. The PSMCs, also called intermediate cells, are consideredmidway between vascular smooth muscle cells and capillary pericytes in location andstructure [25, 26].
RESULTS
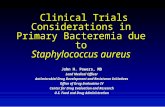
Arteriography. Arteriograms of normal rat lungs showed uniform tapering ofaxial and lateral pathways and even filling of the small arteries seen as a backgroundhaze (Fig. 1a). After 4-implants, the background haze increased centrally, indicat-ing dilatation of small filled arteries, and decreased midway between lateralbranches, and distally, indicating restriction, and nonfilling, of vessels at the edgeof acini (Fig. 1b). The distal axial and lateral arteries also were dilated, as evidencedby obvious widening and by reduced tapering of these vessels between central anddistal lung regions (Fig. 1b).
Vessel wall structure. A mixed pattern of diffuse microvessel injury was evidentin all sepsis lungs. Some segments appeared dilated and thin-walled, and others ap-peared thick-walled. Morphometric analysis indicated dilatation of arteries of all sizesbut showed significant changes in only distal alveolar duct and wall vessels (Figs. 2aand 2b). Analysis of alveolar arteries by size demonstrated dilatation of ones between61 and 120 mm in ED at the expense of ones 21–60 mm (Fig. 2b). The MT of M andPM alveolar duct and wall arteries was reduced, although not significantly so (datanot given), indicating thinning of the muscle layer.
In the thin-walled vessels of the sepsis lung, some cell processes were normal whileothers were disrupted. In the thick-walled vessels, cell size and number were increased,and most cells were hypertrophied, although swollen and disrupted cells also wereevident. Hypertrophic endothelial cells were characterized by extensive organelles—mitochondria, free ribosomes, dilated cisternae, stacked endoplasmic reticulum, anextensive Golgi complex, and micropinocytotic vesicles (Figs. 3a and 3b). Hyperplasiaof these cells was evident from the number of junctional regions (Fig. 3c). Hypertro-phied fibroblasts, and increased collagen deposits, were present in the adjacent intersti-tium (Figs. 3a and 3c). The hypertrophied processes of PSMCs, absent or formingonly a thin subendothelial layer in vessels of the normal lung, thickened the walls ofvessels in the sepsis lung (Figs. 3a–3d). They formed single or multiple layers thatextended completely, or in part, around the vessel circumference. While some lackedthe density of filaments characteristic of smooth muscle cells, in others extensivefilaments indicated progression toward a contractile phenotype (Fig. 4). In vesselswhere cell injury was extensive, endothelial cells were characterized by an intactplasmalemmal membrane and a disrupted, and electron-lucent, cytoplasm, with dilatedcisternae, many micropinocytotic vesicles, and condensed electron-dense bodies (Figs.5a and 5b). Similar changes were evident in adjacent interstitial and epithelial cells
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

88 BRIEF COMMUNICATION
FIG. 1. Pulmonary arteriograms (12.3). (a) Normal lung showing uniform filling of arteries with barium-gelatin. Arteries ú160 mm ED are discerned as separate lines, and ones õ160 mm ED as background haze[3]. (b) Sepsis lung (4-implants) showing dilatation of axial and lateral artery branches (black arrows), withdense background haze centrally and multiple regions of reduced haze focally at the lung periphery (whitearrows).
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

89BRIEF COMMUNICATION
FIG. 2. External diameter and size distribution of distal pulmonary arteries: Normal (n Å 6) and sepsis(n Å 8) lung. (a) External diameter (mean { SEM) of nonmuscular (NM) and partially muscular (PM)alveolar duct and wall arteries. The diameter of NM and PM alveolar duct arteries, and NM alveolararteries, is significantly increased in the sepsis lung (the ED of M alveolar duct arteries was unchanged inthe sepsis lung, and no M alveolar wall arteries were found this distally in either the normal or sepsislung). (b) Distribution of alveolar duct and wall arteries by size (NM, PM, and M arteries being includedin each population). In the sepsis lung the distribution of alveolar duct and wall arteries is significantlydifferent, the number of medium and large ones (61–120 mm in diameter) increasing at the expense ofsmaller ones (21–60 mm).
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

90 BRIEF COMMUNICATION
FIG. 3. Alveolar wall vessels. (a) Thick-walled vessel (ED 48 mm, 14195) in the sepsis lung (4-implants)with hypertrophied intimal endothelial cells (e) and PSMCs (*). Note surrounding interstitium thickenedby hypertrophied fibroblasts (fb) and matrix components; elastic lamina (el). (b, inset) Vessel of similarsize in normal lung shown for comparison (ED 49 mm, 15650); alveolus (alv). (c) Higher magnification(15884) of vessel wall in (a) (at double arrow indicating endothelial cell): Note developing PSMC processes(*) and increased interstitial collagen deposits. Numerous electron-dense endothelial cell junctions areevident (small arrows) as compared to the number of these in vessels of a similar size in normal lung. (d)Higher magnification (120,998) of the vessel wall in (a) (at single arrow), showing nucleated PSMC (*)abluminal to the endothelial cell basement membrane (arrows) and adluminal to an elastic lamina.
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

91BRIEF COMMUNICATION
FIG. 3—Continued
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

92 BRIEF COMMUNICATION
FIG. 4. Alveolar wall vessel (ED 30 mm, 126,228) in the sepsis lung (4-implants). The processes of twoPSMCs (*) lie abluminal to an endothelial cell (e). Dense microfilaments are aligned parallel to the adluminalmargin of the PSMC closest to the endothelium (double arrows). Alveolus (alv); basement membrane (bm,indicated by thick arrows).
(Fig. 5a). In vessels where the endothelium appeared relatively normal, adjacent PSMCprocesses were swollen and disrupted (Fig. 6). Retracted endothelial cells were seendirectly over fibrin deposits lying between the endothelial basement membrane andthe margins of adjacent PSMCs or interstitial cells.
Alveolar-capillary membrane structure. In all sepsis lungs, the interstitial com-ponents of the alveolar-capillary membrane were thicker and more cellular thannormal or disrupted. After 4-implants, marked areas of intraalveolar collapse wereevident. Regions of consolidation, caused by intraalveolar accumulations of in-flammatory cells were common. Similar cells were seen infiltrating alveolar walls.Monocytes were seen infiltrating the interstitium around small vessels and adjacentalveolar spaces. In nonconsolidated regions, alveolar-capillary membrane cellswere attenuated and the capillary lumen expanded (Figs. 7a and 7b). In othercapillary segments, the plasmalemmal membrane of endothelial cells, interstitialfibroblasts, and epithelial type 1 cells was disrupted. After 8-implants, regions ofalveolar consolidation were fewer than after 4-implants, and fewer cells were seeninfiltrating the alveolar wall, but the extent of disruption and thickening of the
FIG. 5. Alveolar vessel in the sepsis lung (4-implants). (a) Note disrupted endothelial cell (e) and disruptedadjacent interstitial fibroblasts (fb) and epithelial type 2 cells (ep2) (114,276). (b) Higher magnification(163,202) of endothelial cell shown at arrow in (a). The plasmalemmal membrane is intact but organellesare sparse and irregularly scattered throughout the cytoplasm. Note electron-dense mitochondrial bodieswithout cristae (m), pinocytotic vesicles (small arrows), and clusters of ribosomes (small double arrows).
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

93BRIEF COMMUNICATION
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

94 BRIEF COMMUNICATION
FIG. 6. Alveolar wall vessel in the sepsis lung (4-implants, 151,260). The processes of two PSMCs (*)lie abluminal to endothelial cells (e). The PSMC with filaments distributed throughout the cytoplasm (arrow)is separated from the endothelium by the process of a PSMC with an electron-lucent and disrupted cytoplasm.
alveolar-capillary membrane was greater. Degranulated PMNs were adherent toendothelial cell surfaces, and, in addition to lumen dilatation and attenuation ofalveolar-capillary membrane cells, the normally apposing epithelial and endothelialmembrane surfaces were separated. Extensive disruption of endothelial cells, epi-thelial type 1 cells and interstitial fibroblasts was evident (Fig. 8a). Focally, hyper-trophied processes of interstitial fibroblasts, epithelial and endothelial cells, andextensive collagen deposits thickened the membrane (Fig. 8b).
DISCUSSION
The findings of this study demonstrate striking microvessel injury and remodelingin the lungs of rats with peritoneal sepsis. We recovered only the implanted organismsfrom peritoneal abscesses and blood, and, in some of the animals receiving 8-implants,from abscesses on the pleural surface. Albeit rarely, we have also identified gram-negative organisms in the lung. From these findings, and from the impaired regulationof body temperature and peripheral leukocytosis in the sepsis animals, it would seemjustified to propose that a proinflammatory response to the contents of the implantedcapsule (including live organisms and associated endotoxins) causes the lung mi-crovessel injury reported here. The presence of infiltrating cells and alveolar-capillarymembrane injury after subacute episodes of bacteremia is consistent with the changesafter acute injury caused by an intravenous bolus infusion of organisms or by therelease of cecal contents after cecal ligation and perforation [18, 27–29]. To our
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

95BRIEF COMMUNICATION
FIG. 7. Alveolar-capillary membrane. (a) Sepsis lung (4-implants, 15079) showing attenuation of alveolarcapillary membrane cells (arrows) and PMNs and platelets within a dilated capillary lumen. (b) Normallung (15255) shown for comparison. Capillary (cap), alveolus (alv), red blood cell (rbc).
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

96 BRIEF COMMUNICATION
knowledge, however, this represents the first report of extensive injury and wallremodeling in lung microvessels in response to an intraabdominal source of infection.The changes described here differ considerably from the vasculitis we reported afterchronic intermittent endotoxemia, and the wall remodeling and pulmonary hyperten-sion after chronic persistent endotoxemia [22, 23].
The aim of the model is the development of small abscesses that shed bacteria andtheir fragments (including outer membrane proteins) and trigger the inflammatory andimmunogenic response that typifies the course of sepsis in ARDS patients. An acuteinflammatory response is likely as the capsule dissolves (within minutes of beingimplanted) and releases its contents into the abdominal cavity. Following this it islikely that there is a sustained release of blood-borne products from the pool oforganisms within the peritoneum. While the first two implants produce circulatorycollapse and fall in body temperature—the response typical of an unprimed immunesystem—the later implants are associated with an improved clinical state, as well ashyperthermia and leukocytosis [9]. The model has the advantage that it reflects thecourse of human sepsis [1], and, since animals receiving the same number of implantsshow similar clinical and pathological changes, a further advantage is its reliabilityand repeatability. As such it provides a suitable system in which to test the protectiveeffects of antibodies or anti-inflammatory agents and one in which these agents canbe used to dissect underlying mechanisms.
We found that peritoneal abscesses and gram-negative bacteremia resulted in lungmicrovessel dilatation or lumen restriction by wall thickening. Our structural findingssupported the evidence on the arteriogram of dilated vessels and band-like regions ofreduced filling. Even in normal lung, as part of homeostasis, and in response tomediators generated locally, the vessel wall remodels constantly as cells are removedby programmed cell death, proliferate, migrate, or form matrix [30]. In response toinjury, remodeling represents an adaptive process reflecting alterations in the hemody-namics of blood flow as well as mediator levels. Marked changes in lumen size resultfrom small changes in wall thickness as the endothelium, sensing change in shearstress, releases mediators that remodel the wall to adjust lumen size and restore shearstress to an optimal level [30]. Occurring in response to a long-term increase in bloodflow, dilatation is the result of an increase in wall compliance, produced by a decreasein the deposition (or increase in the degradation) of matrix proteins or a change invasoactive mediator levels. In the sepsis-injured lung a flow-mediated change is likelyproduced by vasoactive mediators—by an increase in the release of a vasodilatorsuch as prostacyclin [9] and perhaps nitric oxide. While the vascular bed of normallung is under-perfused, allowing additional vessels to be recruited to accommodateincreased flow, vessel restriction limits recruitment in the injured lung and so increasesblood flow in residual vessels, potentiating wall changes. In the sepsis-injured lung,lumen restriction from the structural changes described here, or from increased produc-tion of a vasoconstrictor such as endothelin-1 [31], may similarly potentiate flow-mediated injury and lumen dilatation.
FIG. 8. Alveolar-capillary membrane: Sepsis lung (8-implants). (a) Expanded and disrupted interstitialspace and the disrupted process of an epithelial type 1 cell (ep1) (15076). (b) Thickened region of alveolar-capillary membrane with extensive interstitial deposits of collagen fibers (16921). Capillary (cap), alveolus(alv), collagen (co), epithelial type 2 cell (ep2).
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

97BRIEF COMMUNICATION
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

98 BRIEF COMMUNICATION
Extensive injury to endothelial and precursor cells, as demonstrated by swellingand fragmentation, and by the loss of vessel and capillary wall integrity, likely reflectsthe cytotoxic effects of circulating bacterial products and the systemic or local releaseof proinflammatory mediators such as tumor necrosis factor (TNFa) and interleukins(IL-1, IL-8) [6, 32, 33]. Hypertrophied cells indicate less extensive injury and anability to adapt to a new level of homeostasis. While it is likely that cytokines releasedin the sepsis lung, by vascular or inflammatory cells, induce endothelial procoagulantactivity [34], we found no evidence of lumen occlusion by platelet or organizingthrombi, although we cannot exclude the possibility that as the lungs were inflatedloosely adherent microthrombi and leukocytes were dislodged. Lack of evidence ofwidespread microthrombi, and of lumen or wall obliteration, indicates that hypertro-phied vascular cells and increased matrix components form the basis of microvascularwall thickening and lumen restriction in the sepsis lung. While mediator interactionsin the vessel wall, and their kinetics, in the sepsis-injured lung are likely complex, asin other injuries [24] the local release of growth factors by vascular cells or by adjacentmacrophages or monocytic cells will induce these changes. Whether these events aretriggered directly by bacterial products, or indirectly by the activation of proinflamma-tory mediators, remains speculative.
Our finding that the PSMCs are not organized into a medial layer by the formationof elastic laminae in the walls of the microvessels in the sepsis-injured lung—a changetypical of injuries associated with pulmonary hypertension—is consistent with thenormal pulmonary artery pressure and resistance measurements in vivo reported inthis model and the lack of right ventricular hypertrophy [9]. In an isolated perfusedlung preparation, however, we found that the vascular bed of the sepsis-injured lungis hyperreactive, with vascular resistance normal at baseline but abnormal in responseto challenge [21]: Angiotensin increases arterial but not venous resistance more thanin normal lung, while free radicals (generated by purine-xanthine oxidase) increasethe resistance of both arterial and venous segments, but especially the latter, indicatinga site-specific injury. The development of PSMCs in distal NM segments, as well asa change in the function of smooth muscle cells in more proximal segments wherethey normally form a medial layer, will contribute to microvessel hyperreactivity inthe sepsis-injured lung.
ACKNOWLEDGMENTS
We thank Karen Rock and Howard Mulhern for their expert technical assistance, and Dr. R. C. MoelleringJr. and Ms Sandy Willy (Department of Medicine, New England Deaconess Hospital, Boston, MA) foradvice in developing the model and for help with bacteriologic techniques.
REFERENCES
1. Cross, A. S., Opal, S. M., Sadoff, J. C., and Gemski, P. (1993). Choice of bacteria in animal models ofsepsis. Infect. Immun. 61, 2741–2747.
2. Tomashefski, J. F., Davies, P., Boggis, C., Greene, R., Zapol, W. M., and Reid, L. (1983). The pulmonaryvascular lesions of the adult respiratory distress syndrome. Am. J. Pathol. 112, 112–126.
3. Jones, R., Tomashefski, J. F., Kobayashi, K., Kirton, O. C., Zapol, W. M., and Reid, L. (1985). PulmonaryVascular Pathology. In ‘‘Acute Respiratory Failure’’ (W. M. Zapol and K. Falke, Eds.), Vol. 24, pp.23–160. Lung Biology in Health and Disease Series (C. Lenfant, ex Ed.), New York/Basel.
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

99BRIEF COMMUNICATION
4. Movat, H. Z., Cybulsky, M. I., Colditz, K. G., Chan, M. K. W., and Dinarello, C. A. (1987). Acuteinflammation in gram-negative infection: endotoxin, interleukin-1, tumor necrosis factor and neutrophils.Fed. Proc. 46, 97–104.
5. Cross, A. S., Sadoff, J. C., Kelly, N., Berton, E., and Gemski, P. (1989). Pretreatment with recombinantmurine tumor necrosis factor alpha/cachectin and murine interleukin-1 alpha protects mice from lethalbacterial infection. J. Exp. Med. 169, 2021–2027.
6. Czuprynski, C. J., and Brown, J. F. (1987). Recombinant murine interleukin-1a enhancement of non-specific antibacterial resistance. Infect. Immun. 55, 2061–2065.
7. Seeger, W., and Suttorp, N. (1987). Role of membrane lipids in the pulmonary vascular abnormalitiescaused by bacterial toxins. Am. Rev. Respir. Dis. 136, 426–466.
8. Danner, R. L., Elin, R. J., Hosseini, J. M., Wesley, R. A., Reilly, J. M., and Parillo, J. E. (1991).Endotoxemia and human septic shock. Chest 99, 169–175.
9. Kirton, O. C., Jones, R., Zapol, W. M., and Reid, L. (1984). The development of a model of subacutelung injury after intraabdominal infection. Surgery 96, 384–394.
10. Sharbaugh, R. J., and Rambo, W. M. (1971). A new model for producing experimental fecal peritonitis.Surg. Gynecol. Obstetr. 133, 843–845.
11. Onderdonk, A. B., Weinstein, W. M., Sullivan, N. M., Bartlett, S. G., and Gorbach, S. L. (1974).Experimental intra-abdominal abscesses in rats: Quantitative bacteriology of infected animals. Infect.Immun. 10, 1256–1259.
12. Witcherman, K. A., Baue, A. E., and Chaudry, I. H. (1980). Sepsis and septic shock—A review oflaboratory methods and a proposal. J. Surg. Res. 29, 189–210.
13. Hurley, J. C. (1993). Reappraisal of the role of endotoxin in the sepsis syndrome. Lancet 341, 1133–1135.
14. Nichols, R. L., Smith, J. W., and Balthazar, E. R. (1978). Peritonitis and intraabdominal abscess: Anexperimental model for evaluation of the human disease. J. Surg. Res. 25, 129–134.
15. Bartlett, J. G., and Gorbach, S. L. (1979). An animal model of intraabdominal sepsis. Scand. J. Infect.Dis. (Suppl) 19, 26–29.
16. Fry, D. E., Garrison, R. N., Rink, R. D., Casey, J., DeCamp, M. M., and Richardson, J. D. (1982). Anexperimental model of intraabdominal sepsis in the rat. Adv. Shock Res. 7, 7–11.
17. Fink, M. P., Gardiner, W. M., Roethel, R., and Fletcher, J. R. (1985). Plasma levels of 6-keto-PGF1a
but not TxB2 increase in rats with peritonitis due to cecal ligation. Cir. Shock 16, 297–305.
18. Craig, I., Judges, D., Gnidec, A., Lefcoe, M., Paterson, N., Finley, R., and Sibbald, W. (1987). Pulmonarypermeability edema in a large animal model of nonpulmonary sepsis. A morphologic study. Am. J.Pathol. 128, 241–251.
19. Weinstein, W. M., Onderdonk, A. B., Bartlett, J. G., and Gorbach, S. L. (1974). Experimental intraab-dominal abscesses in rats: Development of an experimental model. Infect. Immun. 10, 1250–1255.
20. Cross, A. S. (1994). Inducing an abscess. Lancet 343, 248–249.
21. Kirton, O. C., Gore, R. G., Reid, L., and Jones, R. (1992). Recurrent episodes of gram-negativebacteremia or endotoxemia change reactivity of pre- and post-capillary pulmonary segments to angiotensinand free radicals. Int. Care Med. 18, 293–298.
22. Jones, R., Kirton, O. C., Zapol, W. M., and Reid, L. (1986): Rat pulmonary artery wall injury bychronic intermittent infusions of Escherichia coli: Obliterative vasculitis and vascular occlusion. Lab.Invest. 54, 282–294.
23. Kirton, O. C., and Jones, R. (1987). Rat pulmonary artery restructuring and pulmonary hypertensioninduced by continuous Escherichia coli infusion. Lab. Invest. 56, 198–210.
24. Jones, R., and Reid, L. (1995). Vascular Remodeling in the Clinical and Experimental PulmonaryHypertensions. In ‘‘Pulmonary Vasculature Remodeling’’ (J. E. Bishop, J. Reeves, and G. J. Laurent,Eds.), pp. 47–115. Portland Press, London.
25. Meyrick, B., and Reid, L. (1978). The effect of continued hypoxia on rat pulmonary arterial circulation.An ultrastructural study. Lab. Invest. 38, 188–199.
26. Jones, R. (1992). Ultrastructural analysis of contractile cell development in lung microvessels in hyper-
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR

100 BRIEF COMMUNICATION
oxic pulmonary hypertension: Fibroblasts and intermediate cells selectively reorganize nonmuscular vesselsegments. Am. J. Pathol. 141, 1491–1505.
27. Sato, T., Isoyama, T., Tanaka, J., Jones, R. T., Cowley, T. A., and Trump, B. F. (1982). The pathophysiol-ogy of septic shock: Changes in hemodynamics in rats following live E. coli injection. An applicationof the thermodilution method for measurement of cardiac output. Adv. Shock Res. 7, 25–42.
28. Tanaka, J., Sato, T., Jones, R. T., Trump, B. F., and Cowley, R. A. (1983). The pathophysiology ofseptic shock: responses to different doses of live Escheria coli injection in rats. Adv. Shock Res. 9, 101–114.
29. Hangen, D. H., Bloom, R. J., Stevens, J. H., O’Hanley, P., Ranchod, M., Collins, J., and Raffin, T. A.(1987). Adult respiratory distress syndrome. A live E. coli septic primate model. Am. J. Pathol. 126,396–400.
30. Gibbons, G. H., and Dzau, V. J. (1994). The emerging concept of vascular remodeling. N. Eng. J. Med.330, 1431–1438.
31. Oian, O., Wilson, M. A., Yue, Z., Spain, D. A., Chou, M., Matheson, P. J., and Garrison, R. N. (1995).Tissue endothelin-1 gene expression following bacteremia. FASEB J. 9(3), 5165.
32. Said, S. I. (1991). Principles and Strategies in the Pharmacological Modulation of Lung Injury. In ‘‘ThePulmonary Circulation and Acute Lung Injury’’ (S. I. Said, Ed.), 2nd ed, pp. 457–472. Futura, MountKisco, NY.
33. Wakabayashi, G., Gelfand, J. A., Burke, J. F., Thompson, R. C., and Dinarello, C. A. (1991). A specificreceptor antagonist for interleukin-1 prevents E. coli-induced shock in rabbits. FASEB J. 5, 338–343.
34. Ulich, T. (1992). Tumor necrosis factor. In ‘‘Cytokines of the Lung’’ (J. Kelley, Ed.), Vol. 61, pp.307–332. Lung Biology in Health and Disease Series (C. Lenfant, ex Ed.), New York/Basel/Hong Kong.
6z07$$1958 06-12-96 22:07:31 mvras AP: MVR