Low-Income and Blue-Collar Populations Elizabeth Barbeau, ScD, MPH Dana-Farber Cancer Institute...
29
Low-Income and Blue- Collar Populations Elizabeth Barbeau, ScD, MPH Dana-Farber Cancer Institute Harvard School of Public Health
-
Upload
barry-tart -
Category
Documents
-
view
216 -
download
1
Transcript of Low-Income and Blue-Collar Populations Elizabeth Barbeau, ScD, MPH Dana-Farber Cancer Institute...
Low-Income and Blue-Collar Populations
Elizabeth Barbeau, ScD, MPH
Dana-Farber Cancer Institute
Harvard School of Public Health
Question
What are effective strategies for increasing consumer demand for and use of proven individually oriented cessation treatments among low-income and blue-collar populations?
Key points
1. Compared to smokers in higher socioeconomic groups, those in low socioeconomic groups are just as likely to attempt to quit, but less likely to use proven treatments and less likely to succeed in quitting
2. Insurance-based coverage of smoking cessation treatments increases use of treatments (Medicaid and labor-management funds)
3. Little empirical evidence on effectiveness of various strategies to promote use of treatments; suggestions for future research directions
Social class and smoking
• Dimensions of social class– Income– Occupation– Education
• Related but not identical constructs – Providing evidence of their independent effects on
smoking, analyses on NHIS 2000 data indicated that odds ratios for current smoking were attenuated but remained statistically significant for education, occupation, and income when jointly included in a multivariable model. (Barbeau et al, 2004)
Key points
1. Compared to smokers in higher socioeconomic groups, those in low socioeconomic groups are just as likely to attempt to quit, but less likely to use proven treatments and less likely to succeed in quitting
2. Insurance-based coverage of smoking cessation treatments increases use of treatments (Medicaid and labor-management funds)
3. Little empirical evidence on effectiveness of various strategies to promote use of treatments; suggestions for future research directions
Key point #1
• Low SES groups try to quit as often as higher SES groups, BUT…
• Low SES groups are less likely to succeed in quit attempts
• And less likely to use proven cessation treatments
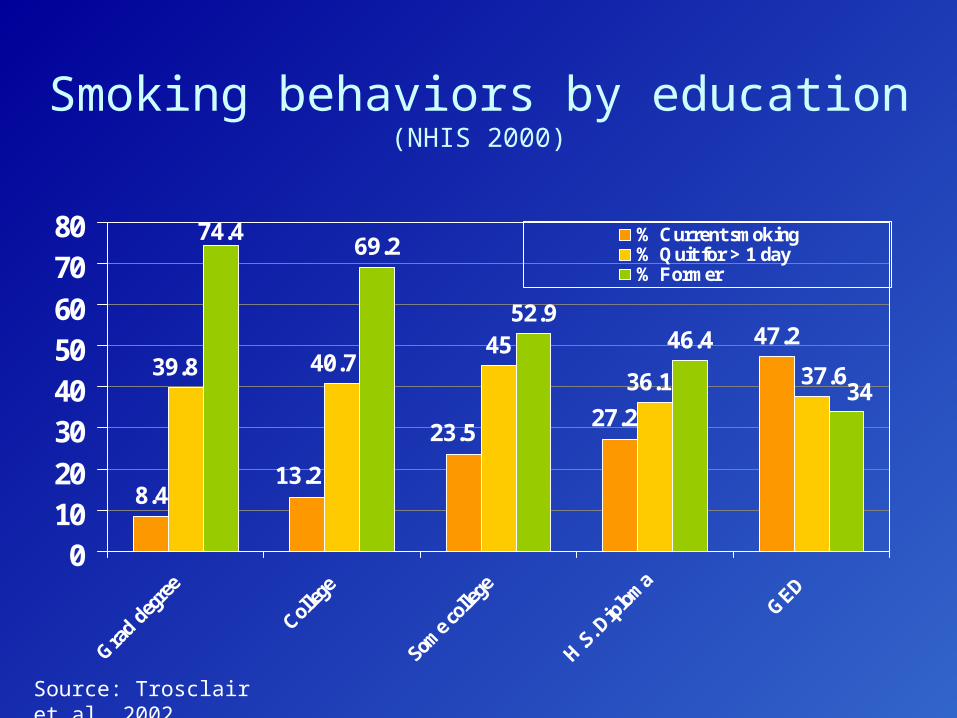
Smoking behaviors by education (NHIS 2000)
8.4
47.245
69.2
52.946.4
13.2
23.527.2
39.8 40.7 37.636.1
74.4
34
01020
30405060
7080
Gra
d deg
ree
Colleg
e
Some c
olleg
e
H.S
. Dip
loma
GED
% Current smoking% Quit for > 1 day% Former
Source: Trosclair et al, 2002
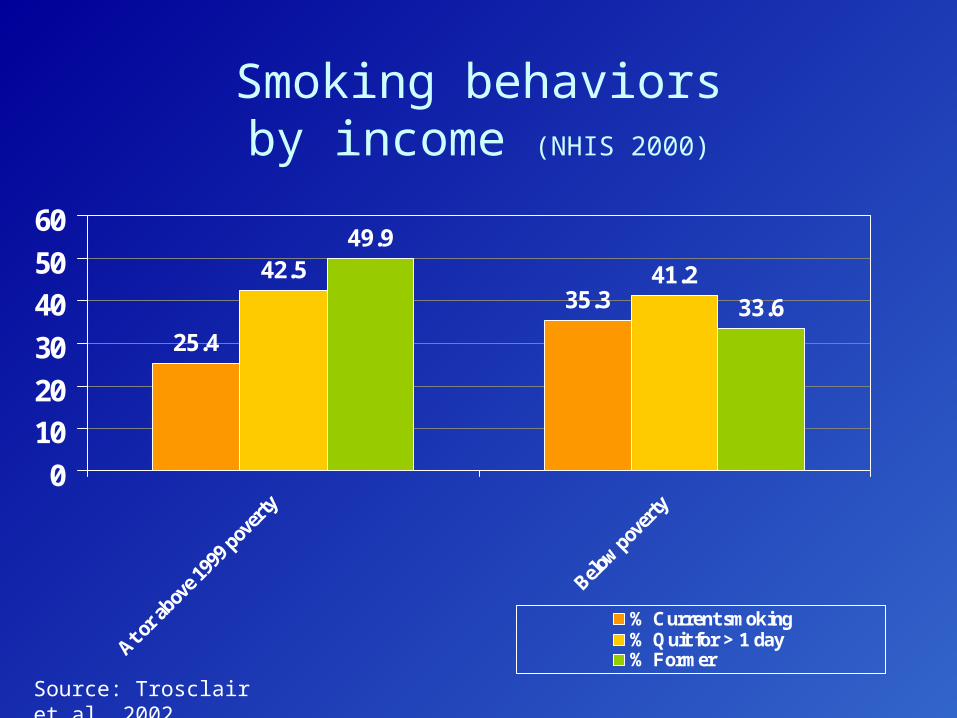
Smoking behaviorsby income (NHIS 2000)
25.4
35.342.5 41.2
49.9
33.6
0
10
20
30
40
50
60
At or a
bove 1
999 p
over
ty
Below p
over
ty
% Current smoking% Quit for > 1 day% Former
Source: Trosclair et al, 2002
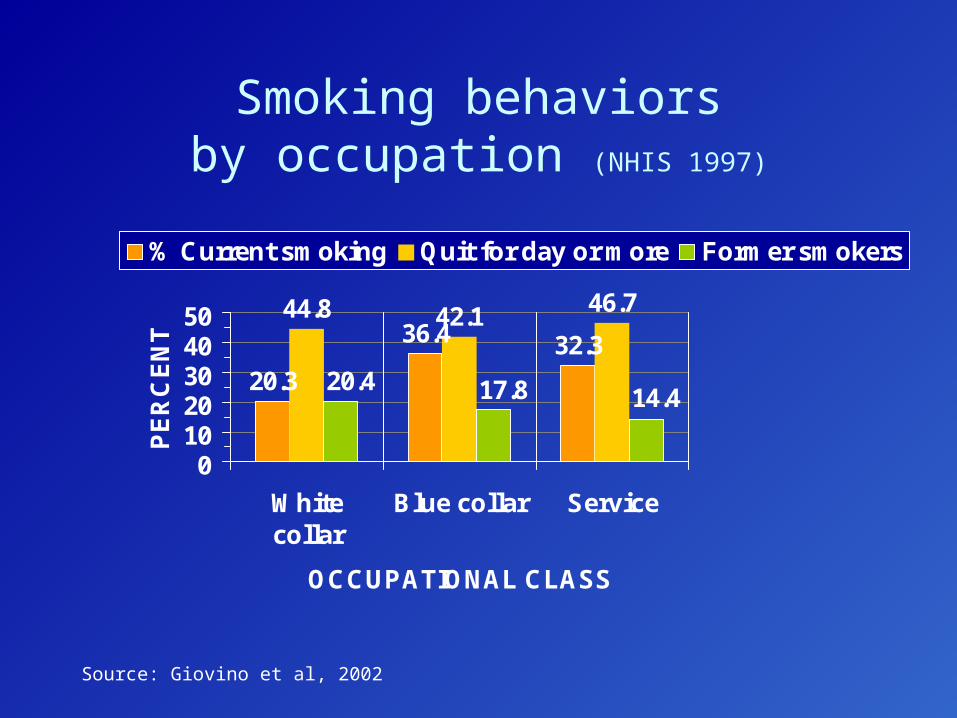
44.8 42.1 46.7
32.336.4
20.314.417.820.4
01020304050
Whitecollar
Blue collar Service
OCCUPATIONAL CLASS
PE
RC
EN
T
% Current smoking Quit for day or more Former smokers
Smoking behaviorsby occupation (NHIS 1997)
Source: Giovino et al, 2002
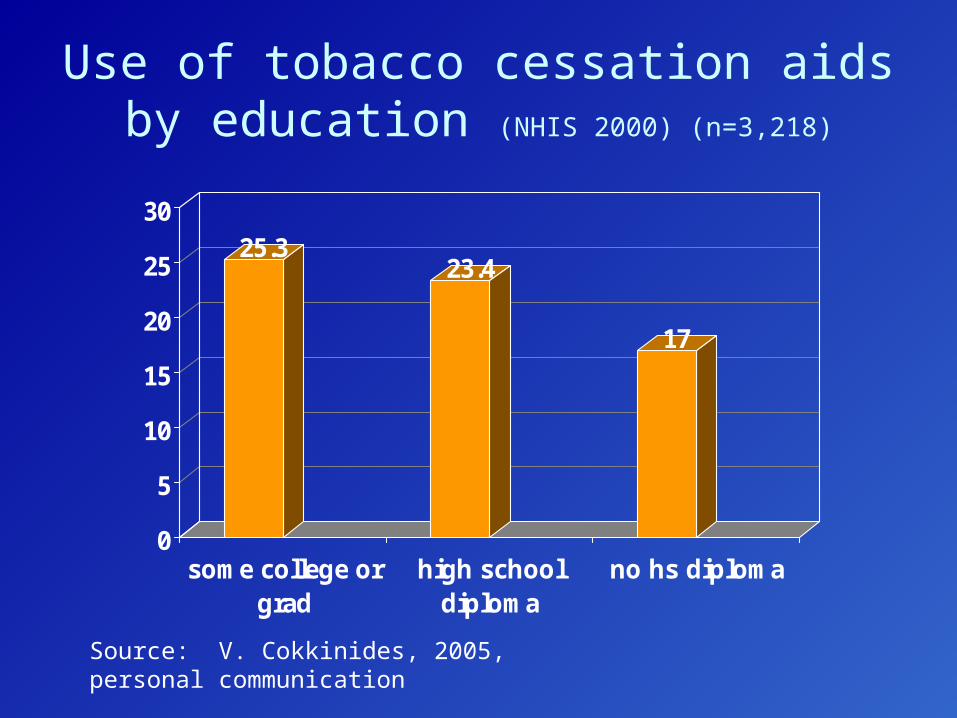
Use of tobacco cessation aids by education (NHIS 2000) (n=3,218)
25.323.4
17
0
5
10
15
20
25
30
some college orgrad
high schooldiploma
no hs diploma
Source: V. Cokkinides, 2005, personal communication
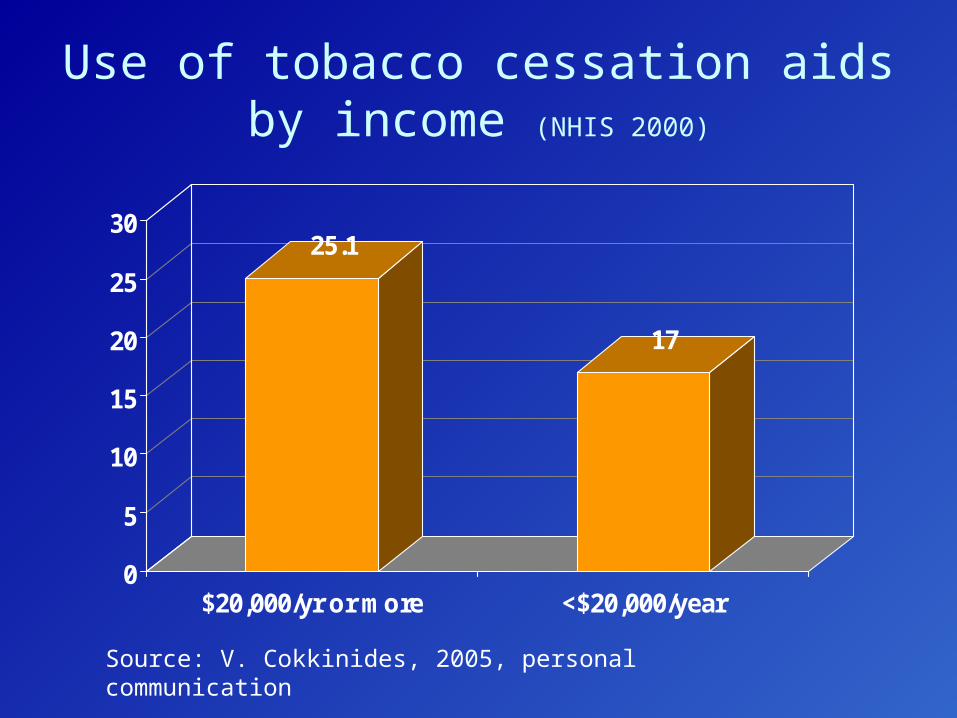
Use of tobacco cessation aidsby income (NHIS 2000)
25.1
17
0
5
10
15
20
25
30
$20,000/yr or more <$20,000/year
Source: V. Cokkinides, 2005, personal communication
Insurance-based coverage for smoking cessation treatments
• Out-of-pocket expenditures can be a barrier to use of counseling and/or pharmacotherapy
• Insurance (private and public)
• Limitation: Not reaching uninsured
Key points
1. Compared to smokers in higher socioeconomic groups, those in low socioeconomic groups are just as likely to attempt to quit, but less likely to use proven treatments and less likely to succeed in quitting
2. Insurance-based coverage of smoking cessation treatments increases use of treatments (Medicaid and labor-management funds)
3. Little empirical evidence on effectiveness of various strategies to promote use of treatments; suggestions for future research directions
Key point #2
• HMO-based study found that the use of all cessation services was greater with full coverage than with cost-sharing plans (11.6% vs. 3.5-3.7%). [Curry et al, 1998]
• RCT (n=1,204 smokers) found higher use of NRT among those receiving fully-covered benefits for NRT and counseling (25%) vs. self-help kit (14%); p=0.001. [Schauffler et al, 2001]
• RCT (n=1,266 smokers) found higher use of treatments among those in the fully-covered benefits arm (10.8%) vs. no coverage arm (4.1%) (OR=2.8, 95% CI 1.8-4.7). [Kaper et al, 2005]
Insurance and low SES smokers
• Medicaid – 36% of Medicaid recipients smoke – Across 20 US communities, among low-income
smokers, nicotine patch use was significantly higher among those who lived in a state where Medicaid included the patch as a benefit (12.1% vs. 7.7%)When full coverage for NRT patch provided, use increased by 57%. [Cummings et al, 1997]
– 37 states cover at least one evidence-based treatment
• Labor-management health & welfare (Taft-Hartley) funds – Coverage is suspected to be low [Barbeau et al, 2000]– Pilot study of coverage demonstrated 13% use of
treatments. [Ringen et al, 2002]
What we know: Insurance-based coverage works
• Small but convincing literature indicates that insurance coverage for full costs of treatments increases their use.
• Medicaid and labor-management insurance vehicles important for low SES groups.
What we don’t know: New research directions
• Need to identify effective intervention strategies – Purchasers, benefits administrators, insurance
consultants– Plan participants
Key points
1. Compared to smokers in higher socioeconomic groups, those in low socioeconomic groups are just as likely to attempt to quit, but less likely to use proven treatments and less likely to succeed in quitting
2. Insurance-based coverage of smoking cessation treatments increases use of treatments (Medicaid and labor-management funds)
3. Little empirical evidence on effectiveness of various strategies to promote use of treatments; suggestions for future research directions
Key point #3
• Channels: Where can we best reach low SES smokers?
• Message: What to say? How to say it?• Messenger: Who should say it?
Potential channels for reaching low SES smokers
• Worksites employing blue-collar and service workers
• Labor unions (largely represent blue-collar and service workers)
• Vocational/trade schools and GED programs• Public assistance programs (e.g., WIC)• Telephone quitlines• Take a page from the tobacco industry
– Bars and night clubs, concerts, car races
• Internet
Blue-collar smokers: Promising channels and messages
WellWorks-2
MassBUILT
WellWorks-2Research question
• Does an intervention integrating health promotion with occupational health and safety result in increases in smoking cessation compared to a standard health promotion intervention?– Secondary aim of evaluating participation levels in
two conditions
• RCT: worksites randomized to HP/OHS vs. HP-only
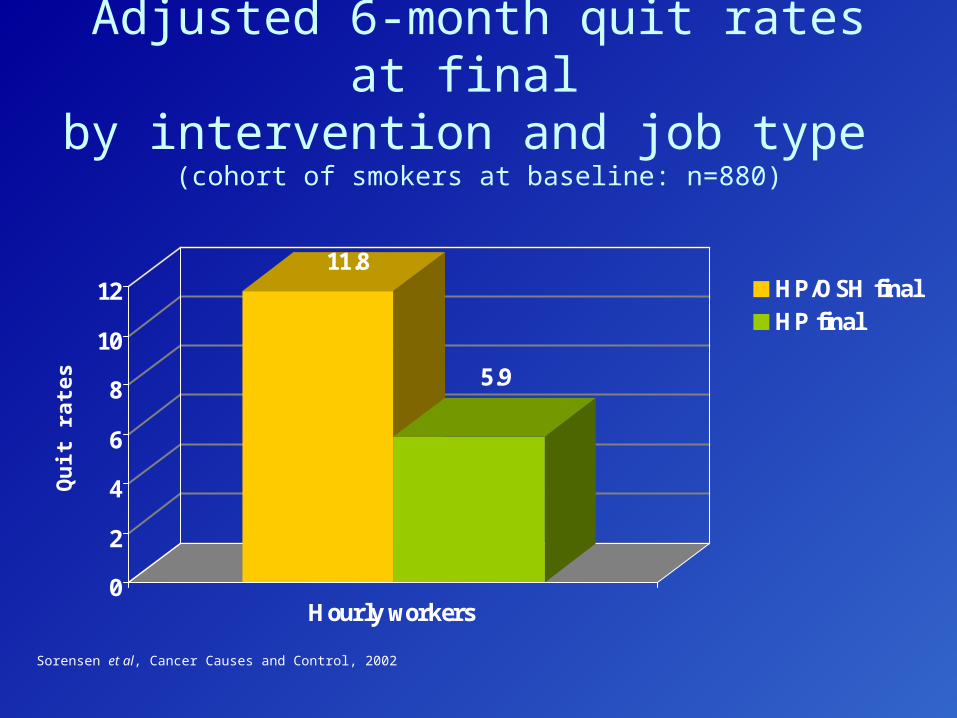
Adjusted 6-month quit rates at final by intervention and job type
(cohort of smokers at baseline: n=880)
11.8
5.9
0
2
4
6
8
10
12
Hourly workers
HP/OSH finalHP final
Sorensen et al, Cancer Causes and Control, 2002
Qu
it r
ates
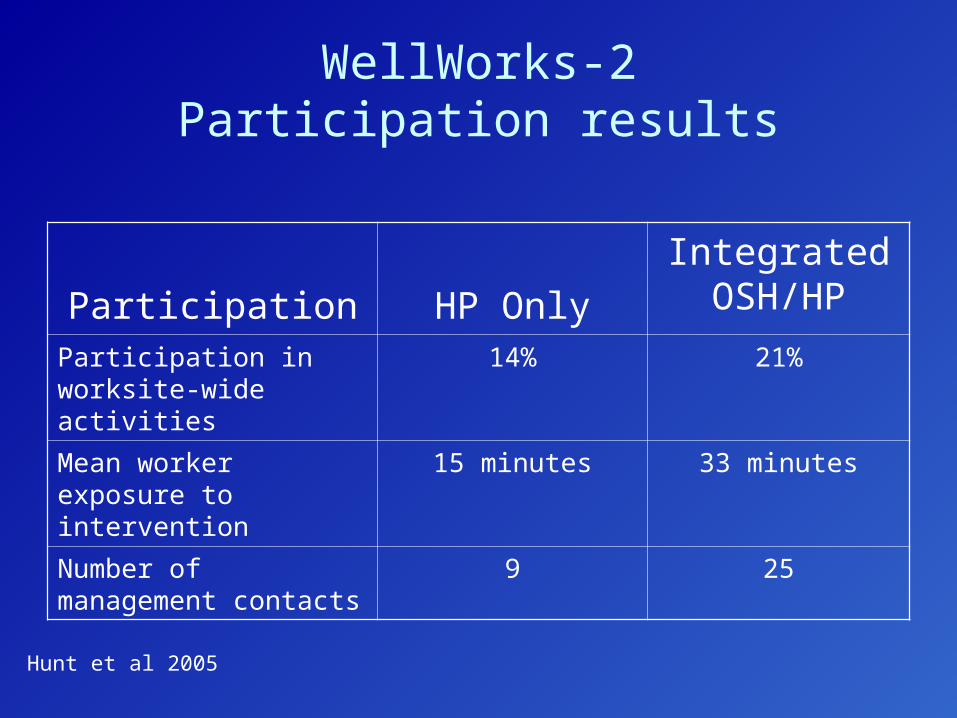
WellWorks-2Participation results
Participation HP Only
Integrated OSH/HP
Participation in worksite-wide activities
14% 21%
Mean worker exposure to intervention
15 minutes 33 minutes
Number of management contacts
9 25
Hunt et al 2005
massbuilt
massBUILTResearch question
• Feasibility and effect of incorporating smoking cessation intervention into health and safety training for building trades apprenticeship programs
• Pilot study: – Baseline smoking prevalence of 41% (n=330). – 19.4% quit rate immediately post-intervention
(Barbeau et al, 2006)
• RCT underway
massbuilt
Channels and messages: State quitlines
• Demonstrated effectiveness• Telephone-based quitlines create theoretically
equal access to cessation counseling • How can we drive more traffic to quitlines?• Could promotions be targeted to low SES
groups?
Channels and messages:Internet
• Digital divide is narrowing• Among smokers, those who use web for
cessation assistance are more highly educated and earn higher incomes than those who do not. [Stoddard and Augustson].
• Research challenges:– Interventions to reduce digital divide and increase
capacity to access health information via internet– Creating websites and testing effectiveness of
attracting low SES smokers and enabling successful quits
Summary
• Low SES smokers are just as likely to attempt to quit as higher SES smokers, but less likely to use proven treatments and to succeed.
• Insurance-based coverage of treatments works, but need additional research on ways to increase coverage and use of services through Medicaid, labor-management funds.
• Research is needed to identify effective messages, channels, and messengers to stimulate increased demand for and use of treatments among low SES smokers.


















