lostridium difficile Clostridium difficile Infection Team ... · PDF fileClostridium difficile...
29
Quality Department Guidelines for Clinical Care 1 Michigan Medicine C. difficile Guideline December 2016 Clostridium difficile Infection Guideline Team Team Leads Tejal N Gandhi MD Infectious Diseases Krishna Rao, MD Infectious Diseases Team Members Gregory Eschenauer, PharmD Pharmacy John Y Kao, MD Gastroenterology Andrea H Kim, MD Internal Medicine Lena M Napolitano, MD Surgery F Jacob Seagull, PhD Leaning Heath Sciences David M Somand, MD Emergency Medicine Kathleen B To, MD Surgery Alison C Tribble, MD Pediatric Infectious Diseases Amanda M Valyko, MPH, CIC Infection Control Michael E Watson Jr, MD, PhD Pediatric Infectious Diseases Consultants: Meghan A. Arnold, MD Pediatric Surgery Daniel H Teitelbaum, MD Pediatric Surgery Laraine Lynn Washer, MD Infection Diseases Initial Release: December 2016 Inpatient Clinical Guidelines Oversight Megan R Mack, MD David H Wesorick, MD F Jacob Seagull, PhD Literature search service Taubman Health Sciences Library For more information: 734- 936-9771 © Regents of the University of Michigan These guidelines should not be construed as including all proper methods of care or excluding other acceptable methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding any specific clinical procedure or treatment must be made by the physician in light of the circumstances presented by the patient. Clostridium difficile Infection in Adults and Children Patient population: Adult and pediatric patients with a primary or recurrent episode of Clostridium difficile infection (CDI) Objectives: 1. Provide a brief overview of the epidemiology of, and risk factors for development of CDI 2. Provide guidance regarding which patients should be tested for CDI, summarize merits and limitations of available diagnostic tests, and describe the optimal approach to laboratory diagnosis 3. Review the most effective treatment strategies for patients with CDI including patients with recurrences or complications Key points for adult patients: Diagnosis • Definitive diagnosis of CDI requires either the presence of toxigenic C. difficile in stool with compatible symptoms, or clinical evidence of pseudomembranous colitis (Table 2, Figure 4). • Once identified, CDI should be classified according to severity ( Table 3). • Although risk factors for CDI (Table 1) should guide suspicion for CDI, testing should be ordered only when indicated (Figure 1). [IC] • Choice of test should be guided by a multi-step algorithm for the rapid diagnosis of CDI ( Figure 2). [IIC] • Single-step PCR testing (not part of the UMHS algorithm) occurs as part of the new Biofire test panel for gastrointestinal pathogens and should not be used if CDI is suspected. [IIIB] However, if C. difficile is detected as part of this panel and the patient’s symptoms are compatible with CDI, then treatment is appropriate and additional testing is unnecessary. [IIC] • Patients who are asymptomatic, actively being treated or completed treatment for CDI with clinical improvement in symptoms, or have post-infectious irritable bowel syndrome after CDI should not undergo testing for CDI. [IIIC] Treatment: (See Figure 3 and Table 4) Mild-Moderate CDI: Patient does not meet criteria for “severe” or “complicated” CDI • metronidazole 500 mg PO TID for 10-14 days [IIB] OR • In patients with metronidazole allergy, pregnant, nursing, or on warfarin therapy: vancomycin 125 mg PO QID for 10-14 days. [IB] Severe CDI: Patients with WBC ≥ 15K, Cr ≥ 1.5x baseline, Age ≥ 65, ANC ≤ 500, Albumin ≤ 2.5, SOT/BMT < 100 days, chronic GVHD (BMT), treatment of rejection in the preceding 2 months (SOT), Small bowel CDI, or inflammatory bowel disease • vancomycin 125 mg PO QID for 10-14 days [IA] Complicated CDI: Patients with septic shock, ileus, toxic megacolon, peritonitis, or bowel perforation • Triple therapy=vancomycin 500 mg PO QID, metronidazole 500 mg IV every 8 hours, and vancomycin enema every 6 hours (in patients with ileus, bowel obstruction or toxic megacolon) [IB] • Consult infectious diseases • Consult surgery to assist in management including possible surgical intervention (Table 4, Figure 5). Recurrent CDI: Recurrent symptoms and positive testing for toxigenic C. difficile within 8 weeks of prior episode First recurrence: • Classify as “mild-moderate” “severe,” or “complicated,” and treat accordingly [IC] Second or multiple recurrences (third or more episode of CDI): • Consult infectious diseases • vancomycin PO (dose, need for concurrent IV metronidazole/vancomycin enemas depends on disease classification as noted above) for 10-14 days then taper to 125 mg PO BID for 7 days, 125 mg PO daily for 7 days, and then pulse with 125 mg PO once every 2-3 days for 2-8 weeks. [IIC] OR • fidaxomicin 200 mg PO BID for 10 days (with approval from the infectious diseases consult service). [IIE] * Strength of recommendation: I = generally should be performed; II = may be reasonable to perform; III = generally should not be performed. Level of evidence supporting a diagnostic method or an intervention: A = systematic reviews of randomized controlled trials with or without meta-analysis, B = randomized controlled trials, C = systematic review of non-randomized controlled trials or observational studies, non-randomized controlled trials, group observation studies (cohort, cross-sectional, case-control), D = individual observation studies (case study/case series), E = expert opinion regarding benefits and harm
Transcript of lostridium difficile Clostridium difficile Infection Team ... · PDF fileClostridium difficile...

Quality Department
Guidelines for Clinical Care
1 Michigan Medicine C. difficile Guideline December 2016
Clostridium difficile
Infection Guideline
Team
Team Leads
Tejal N Gandhi MD
Infectious Diseases
Krishna Rao, MD
Infectious Diseases
Team Members
Gregory Eschenauer, PharmD
Pharmacy
John Y Kao, MD Gastroenterology
Andrea H Kim, MD Internal Medicine
Lena M Napolitano, MD
Surgery
F Jacob Seagull, PhD
Leaning Heath Sciences
David M Somand, MD Emergency Medicine
Kathleen B To, MD
Surgery
Alison C Tribble, MD
Pediatric Infectious
Diseases
Amanda M Valyko, MPH,
CIC
Infection Control
Michael E Watson Jr, MD,
PhD
Pediatric Infectious Diseases
Consultants:
Meghan A. Arnold, MD Pediatric Surgery
Daniel H Teitelbaum, MD
Pediatric Surgery
Laraine Lynn Washer, MD
Infection Diseases
Initial Release:
December 2016
Inpatient Clinical
Guidelines Oversight Megan R Mack, MD
David H Wesorick, MD
F Jacob Seagull, PhD
Literature search service
Taubman Health Sciences
Library
For more information: 734- 936-9771
© Regents of the
University of Michigan These guidelines should not be
construed as including all proper
methods of care or excluding
other acceptable methods of care
reasonably directed to obtaining
the same results. The ultimate
judgment regarding any specific
clinical procedure or treatment
must be made by the physician in
light of the circumstances
presented by the patient.
Clostridium difficile Infection
in Adults and Children
Patient population: Adult and pediatric patients with a primary or recurrent episode of Clostridium difficile infection (CDI)
Objectives:
1. Provide a brief overview of the epidemiology of, and risk factors for development of CDI 2. Provide guidance regarding which patients should be tested for CDI, summarize merits and
limitations of available diagnostic tests, and describe the optimal approach to laboratory diagnosis 3. Review the most effective treatment strategies for patients with CDI including patients with
recurrences or complications
Key points for adult patients:
Diagnosis
• Definitive diagnosis of CDI requires either the presence of toxigenic C. difficile in stool with compatible symptoms, or clinical evidence of pseudomembranous colitis (Table 2, Figure 4).
• Once identified, CDI should be classified according to severity (Table 3). • Although risk factors for CDI (Table 1) should guide suspicion for CDI, testing should be ordered
only when indicated (Figure 1). [IC] • Choice of test should be guided by a multi-step algorithm for the rapid diagnosis of CDI (Figure 2).
[IIC] • Single-step PCR testing (not part of the UMHS algorithm) occurs as part of the new Biofire test
panel for gastrointestinal pathogens and should not be used if CDI is suspected. [IIIB] However, if C. difficile is detected as part of this panel and the patient’s symptoms are compatible with CDI, then treatment is appropriate and additional testing is unnecessary. [IIC]
• Patients who are asymptomatic, actively being treated or completed treatment for CDI with clinical improvement in symptoms, or have post-infectious irritable bowel syndrome after CDI should not undergo testing for CDI. [IIIC]
Treatment: (See Figure 3 and Table 4)
Mild-Moderate CDI: Patient does not meet criteria for “severe” or “complicated” CDI • metronidazole 500 mg PO TID for 10-14 days [IIB]
OR • In patients with metronidazole allergy, pregnant, nursing, or on warfarin therapy: vancomycin 125
mg PO QID for 10-14 days. [IB]
Severe CDI: Patients with WBC ≥ 15K, Cr ≥ 1.5x baseline, Age ≥ 65, ANC ≤ 500, Albumin ≤ 2.5, SOT/BMT < 100 days, chronic GVHD (BMT), treatment of rejection in the preceding 2 months (SOT), Small bowel CDI, or inflammatory bowel disease • vancomycin 125 mg PO QID for 10-14 days [IA]
Complicated CDI: Patients with septic shock, ileus, toxic megacolon, peritonitis, or bowel perforation • Triple therapy=vancomycin 500 mg PO QID, metronidazole 500 mg IV every 8 hours, and
vancomycin enema every 6 hours (in patients with ileus, bowel obstruction or toxic megacolon) [IB]
• Consult infectious diseases • Consult surgery to assist in management including possible surgical intervention (Table 4, Figure 5).
Recurrent CDI: Recurrent symptoms and positive testing for toxigenic C. difficile within 8 weeks of prior episode
First recurrence: • Classify as “mild-moderate” “severe,” or “complicated,” and treat accordingly [IC]
Second or multiple recurrences (third or more episode of CDI): • Consult infectious diseases • vancomycin PO (dose, need for concurrent IV metronidazole/vancomycin enemas depends on
disease classification as noted above) for 10-14 days then taper to 125 mg PO BID for 7 days, 125 mg PO daily for 7 days, and then pulse with 125 mg PO once every 2-3 days for 2-8 weeks. [IIC] OR
• fidaxomicin 200 mg PO BID for 10 days (with approval from the infectious diseases consult service). [IIE]
* Strength of recommendation:
I = generally should be performed; II = may be reasonable to perform; III = generally should not be performed.
Level of evidence supporting a diagnostic method or an intervention: A = systematic reviews of randomized controlled trials with or without meta-analysis, B = randomized controlled trials, C = systematic review of non-randomized controlled trials or observational studies, non-randomized controlled trials, group
observation studies (cohort, cross-sectional, case-control), D = individual observation studies (case study/case series), E =
expert opinion regarding benefits and harm

2 Michigan Medicine C. difficile Guideline December 2016
Key points for pediatric patients ≤ 18 years of age:
Diagnosis • The decision to test children for CDI is complicated given a high rate of asymptomatic carriage, especially in infants <
12 months of age. Although risk factors for CDI should guide suspicion for CDI, testing should be ordered only when indicated (Figure 1). [IC] Indications and contraindications for testing pediatric patients are included in Figure 1, but testing is rarely indicated or recommended for infants < 12 months [IIC] and consultation with pediatric ID is recommended. Children from 12 months to 36 months of age may be diagnosed with CDI if no alternative etiology for diarrhea is identified and with positive diagnostic testing. [IIC]
• Definitive diagnosis of CDI requires either the presence of toxigenic C. difficile in stool with other symptoms, or clinical evidence of pseudomembranous colitis (Table 2). Choice of test should be guided by a multi-step algorithm for the rapid diagnosis of CDI (Figure 2). Single-step PCR testing (not part of the UMHS algorithm) occurs as part of the new Biofire test panel for gastrointestinal pathogens and should not be used if CDI is suspected. [IIIE] However, if C. difficile is detected as part of this panel and the patient’s symptoms are compatible with CDI, then treatment is appropriate and additional testing is unnecessary. [IIC] Patients who are asymptomatic, actively being treated or completed treatment for CDI with clinical improvement in symptoms, or have post-infectious irritable bowel syndrome after CDI should not undergo testing for CDI. [IIIC]
• Once identified, CDI should be classified according to severity (Table 3). Certain pediatric conditions are associated with severe CDI and should be treated as such (see Table 3). [IIC]
Treatment: (See Figure 3 for general strategy and Table 3 for pediatric-specific dosing recommendations)
Mild-Moderate CDI: Patient does not meet criteria for “severe” or “complicated” CDI • metronidazole 7.5 mg/kg/dose PO QID for 10 days, maximum 500 mg/dose [IIC] OR • In patients with metronidazole allergy, pregnant, nursing, or on warfarin therapy, or who fail to improve after 3-5 days
of PO metronidazole therapy: vancomycin 10 mg/kg/dose PO QID, up to maximum 125 mg/dose x 10 days. [IIC] Severe CDI: Pediatric patients with ≥ 2 lab criteria (WBC ≥ 15K, Cr ≥ 1.5x baseline, ANC ≤ 500, Albumin ≤ 2.5) OR ANY
high-risk condition with Hirschsprung’s Disease or other intestinal dysmotility disorder, neutropenia from leukemia or other
malignancy, inflammatory bowel disease, SOT/BMT < 100 days • vancomycin 10 mg/kg/dose PO QID, up to maximum 125 mg/dose x 10 days [IB]
Complicated CDI: Patients with septic shock, ICU admission within 2 days of CDI diagnosis, surgery related to CDI diagnosis, ileus, toxic megacolon, peritonitis, or bowel perforation.
• Triple therapy = vancomycin up to 500 mg PO QID, metronidazole 7.5 mg/kg/dose IV Q6H up to 500 mg/dose, and vancomycin enema 10-20 ml/kg/dose up to 1000 ml/dose every 6 hours of vancomycin 500 mg/L solution [if tolerated, 20 mL/kg/dose every 6 hours is preferred, however in patient with additional administration considerations, a minimum of 10 mL/kg/dose every 8 hours should be used] (in patients with ileus, bowel obstruction or toxic megacolon; bowel perforation is a contraindication to enema therapy) [IC]
• Consult pediatric infectious diseases • Consult pediatric surgery to assist in management including possible surgical intervention (Table 4).
Recurrent CDI: Recurrent symptoms and positive testing for toxigenic C. difficile within 8 weeks of prior episode. First recurrence: • Classify as “mild-moderate” “severe,” or “complicated,” and treat accordingly. [IC] Second or multiple recurrences (third or more episode of CDI): • Consult pediatric infectious diseases • vancomycin PO (dose, need for concurrent IV metronidazole/vancomycin enemas depends on disease classification as
noted above) for 10-14 days then taper to 125 mg PO BID for 7 days, 125 mg PO daily for 7 days, and then pulse with 125 mg PO once every 2-3 days for 2-8 weeks. [IIC]
OR • fidaxomicin 16 mg/kg/dose BID, max 200 mg per dose, for 10 days [IIC]; pediatric ID approval is required for use.

3 Michigan Medicine C. difficile Guideline December 2016
Table 1. Risk Factors for CDI
Past history of CDI
Current or recent antibiotic use (highest risk within 3 months of exposure)
Advanced age (65 or older)
Severe comorbid disease(s)
Hospitalization within 30 days
Inflammatory bowel disease (IBD
Immunosuppressed state and use of immunosuppressive drugs
Acid suppressive therapy (especially, proton pump inhibitors)
Additional risk factors specific to pediatrics
Pediatric patients with history of prematurity, prolonged or frequent
hospitalizations, or history of frequent or recent antimicrobial therapy
Pediatric patients with Hirschsprung’s disease, other intestinal dysmotility disorder,
or history of abdominal surgery, including gastrostomy or jejunostomy tubes
Note: Community-associated CDI1 can be seen in low risk population or in patients without traditional risk factors.
Figure 1. Indications and Contraindications for CDI Testing
CDI: Clostridium difficile infection; IBD: inflammatory bowel disease; ID: infectious disease (service); PCR: polymerase chain
reaction; WBC: white blood cell count.

4 Michigan Medicine C. difficile Guideline December 2016
Table 2. Definition of Clostridium difficile Infection (CDI)
CDI: Clostridium difficile infection; WBC: white blood cell count.
Figure 2. University of Michigan Health System Multistep Algorithm*
for the Rapid Diagnosis of C. difficile Infection
CDI: Clostridium difficile infection; EIA: enzyme immunoassay; GDH: glutamate dehydrogenase; PCR: polymerase chain
reaction.
* Adapted under Creative Commons License from Rao K, Erb-Downward JR, Walk ST, et al. The Systemic Inflammatory
Response to Clostridium difficile Infection. PLoS ONE. 2014;9(3):e92578.
Requires either of the following:
1. A positive laboratory result for presence of toxigenic C. difficile in the stool
PLUS Any of the following symptoms compatible with CDI
Diarrhea (≥3 unformed stools in a 24-hour period without an alternate explanation such
as laxative use)
Radiographic evidence of ileus without alternate explanation (especially if leukocytosis
present [WBC >15,000 cells/mm3])
Abdominal pain with radiographic evidence of bowel thickening
Radiographic evidence of toxic megacolon
OR
2. Colonoscopic or histopathologic evidence of pseudomembranous colitis.

5 Michigan Medicine C. difficile Guideline December 2016
Table 3. Criteria for Severity Classification of Clostridium difficile Infection
Adult* Pediatric*
Severity Treatment Severity Treatment
Mild/ Moderate
• Diagnosis of CDI (see
Table 2)
AND
• None of the criteria in the
“severe” or “complicated”
columns below
Patient does not meet criteria
for “severe” or “complicated”
CDI
• metronidazole 500 mg PO
TID for 10-14 days
OR
Patients with metronidazole
allergy, pregnant, nursing, or
on warfarin therapy:
• vancomycin 125 mg PO
QID for 10-14 days
Mild/ Moderate
• Diagnosis of CDI (see Table 2)
AND
• None of the criteria in the
“severe” or “complicated”
columns below
Patient does not meet criteria for
“severe” or “complicated” CDI
• metronidazole 7.5 mg/kg/dose PO
QID for 10 days, maximum 500
mg/dose
OR
• Patients with metronidazole allergy,
pregnant, nursing, on warfarin
therapy, or who fail to improve after
3-5 days of PO metronidazole
therapy: vancomycin 10 mg/kg/dose
PO QID, up to maximum 125
mg/dose x 10 days
Severe (ANY of the
following)
• Age ≥ 65
• WBC ≥ 15K
• Cr ≥ 1.5x baseline
• ANC ≤ 500
• ALB ≤ 2.5
• SOT/BMT < 100 days
• Small bowel CDI
• Inflammatory Bowel
Disease
• Treatment of rejection in
the preceding 2 months
(SOT)
• Chronic GVHD (BMT)
• vancomycin 125 mg PO QID
for 10-14 days
Severe (at least 2 abnormal lab
values OR at least 1 high-risk
condition)
• WBC ≥ 15K
• Cr ≥ 1.5x baseline
• ANC ≤ 500
• ALB ≤ 2.5
OR
• SOT/BMT < 100 days
• Small bowel CDI
• Inflammatory Bowel Disease
• Hirschsprung’s Disease or other
intestinal dysmotility disorder
• Neutropenia from malignancy
• vancomycin 10 mg/kg/dose PO
QID, up to maximum 125 mg/dose
x 10 days
Complicated (ANY of the
following)
• Septic shock –Sepsis with
persistent hypotension,
requiring vasopressors to
maintain MAP ≥ 65 mm
Hg and having a serum
lactate level > 2 mmol/L
despite adequate fluid
resuscitation
• Severe sepsis –Life-
threatening organ
dysfunction caused by a
dysregulated host response
to infection. Suspected or
documented infection and
an acute increase of ≥ 2
SOFA points
• Ileus or bowel obstruction
• Toxic megacolon
• Peritonitis
• Bowel perforation
• vancomycin 500 mg PO
QID
• metronidazole 500 mg IV
every 8 hours
• vancomycin enema 500 mg
in 1000 mL of normal saline
every 6 hours (in patients
with ileus, bowel
obstruction or toxic
megacolon)
• Consult infectious diseases
and surgery to assist in
management including
possible surgical
intervention (Table 4).
Operative management
strategies for CDI may
include exploratory
laparotomy, diverting loop
ileostomy with lavage, total
or subtotal abdominal
colectomy with end
ileostomy (Figure 5).
Complicated (ANY of the
following)
• Septic shock
• Severe sepsis
• Ileus or bowel obstruction
• Toxic megacolon
• Peritonitis
• Bowel perforation
• vancomycin up to maximum 500
mg/dose PO QID
• metronidazole 7.5 mg/kg/dose IV
every 6 hours, up to maximum 500
mg/dose • vancomycin retention enema (10-20
mL/kg/dose, up to 1000 mL max, of a 500 mg/L solution in normal saline q6h instilled by appropriately sized Foley catheter inserted into rectum with balloon inflated and Foley clamped for 1 hour, in patients with ileus, bowel obstruction or toxic megacolon). Treatment naïve patients should be started at 10 mL/kg/dose and escalated as tolerated up to 20 mL/kg/dose up to a maximum of 1000 mL). Suspected or known bowel perforation is a contraindication for rectal administration.)
• Consult pediatric infectious diseases
and pediatric surgery to assist in
management
ANC: absolute neutrophil count; ALB: albumin; BMT: bone marrow transplant; CDI: Clostridium difficile infection; Cr: serum
creatinine; GVHD: graft versus host disease; SOT: solid organ transplant; WBC: white blood cell count. *Please see text
regarding treatment of second or greater recurrence of CDI and the role of prophylactic oral vancomycin with concomitant
antibiotic use for first or greater CDI episode

6 Michigan Medicine C. difficile Guideline December 2016
Figure 3. Clostridium difficile Infection Treatment Algorithm Overview
Note: Doses indicated are for adult patients. For pediatric-specific dosing recommendations see Table 3.
BID: twice per day; CDI: Clostridium difficile infection; CT: computed tomography; ID: infectious disease (service); IV:
intravenous; PO: by mouth; QID: four times per day; TID: three times per day.

7 Michigan Medicine C. difficile Guideline December 2016
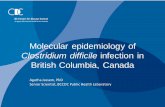
Figure 4. Imaging of “accordion sign” and “target sign”
(Left) Accordion sign in 50-year-old woman with C. difficile colitis. Marked submucosal edema is present in the right colon
(“thumbprint” appearance on longitudinal axis, short arrows). Oral contrast material (arrowhead) is trapped within the lumen.
(image from Macari Balthazar Megibow 1999).
(Right) A 65-yo C. difficile –positive woman with CT through the mid-abdomen showing diffusely thickened colonic wall
appearing as a “target sign” (concentric circles formed by the layers of bowel wall in inflammatory disease) on axial imaging
(arrow) (image from AJR:186, May 2006).
Table 4. Indications for Surgical Consult 2-6
Surgical consultation is appropriate for C. difficile infected patients in these situations:
- Any patient with complicated CDI (see Table 3)
- Any patient with CDI and clinical deterioration attributable to CDI, including the following:
Worsening abdominal distention/pain and/or peritonitis
Bowel obstruction
Intubation
Vasopressor requirement
Mental status changes
New or worsening Acute Kidney Injury
Worsening Lactate > 5mmol/L
Persistent or worsening leukocytosis (WBC ≥35,000 cells/mm3)
Hirschsprung’s disease
- Any patient with failure to improve with standard therapy within 5 days as determined by resolving symptoms and
physical exam, resolving WBC/band count
CDI: Clostridium difficile infection; WBC: white blood cell count.

8 Michigan Medicine C. difficile Guideline December 2016
Figure 5. Operative Management Strategy for CDI
Table 5. Guidance on Preemptive Isolation for Patients with Diarrhea.
Preemptive isolation should be considered if patients have diarrhea (3 or more watery stools in 12 to 24 hours) *not caused by laxative use, chemotherapy, enteral feeds or other medical causes AND AT LEAST ONE of the following:
Current or prior antibiotic use (within 30 days)
Significant abdominal pain, not caused by incisional pain, dyspepsia, or nausea
History of C. difficile
Suspect C. difficile
Place patient in room with curtain or door (NO HALL BEDS)
Place CONTACT PRECAUTIONS-D sign on door/curtain
*1L of colostomy output, >200mL of watery rectal bag output

9 Michigan Medicine C. difficile Guideline December 2016
Clinical Background
Clostridium difficile is a Gram-positive bacillus that can
asymptomatically colonize the gastrointestinal tract or
cause symptomatic disease through the production of
cytotoxins TcdA and TcdB.2 Patients usually develop
Clostridium difficile infection (CDI) after exposure to
antibiotics, and the severity of CDI can range from self-
limited diarrheal illness, to a fulminant, life-threatening
colitis.7 Even among those that recover, recurrent disease is
common.8 Despite being first identified in 1978 as the
causative agent of pseudomembranous colitis9,10 and
subsequently garnering significant attention from the
medical community, attempts to control C. difficile have not
met with much success, especially in hospitals and other
acute care settings.
The past decade has seen a significant increase in the
incidence of CDI in the United States. In hospitals and
nursing homes, there are now at least 450,000 new cases
and 29,000 deaths per year.11-13 The increased burden of
disease is largely attributable to the emergence of several
strains, especially polymerase chain reaction (PCR)
ribotype 027, which led to a worldwide epidemic.14 Though
CDI occurs in all age groups, infection with ribotype 027,
as well as CDI in general, is most common in older adults.15
Thus, as the US population ages, the incidence of CDI and
adverse outcomes will likely increase.15 Ninety-two percent
of CDI-related deaths occur in adults of age 65 or older,
where CDI is the 18th leading cause of mortality.16 The risk
of recurrent CDI is 2-fold higher with each decade of life.8
The annual rate of CDI-related hospitalizations in those
aged >85 years exceeds those of all other age groups
combined.17 All of these epidemiologic trends contribute to
an estimated $1.5 billion in excess healthcare costs each
year due to CDI.18
Rationale for Recommendations
The increased incidence of CDI and its adverse outcomes
among hospitalized patients, coupled with the availability
of new therapies has complicated the management of CDI.
This underscores the need for guidelines that review the
evidence and provide recommendations for the prevention,
diagnosis, and treatment of CDI in hospitalized patients.
Clinical Problem and Management Issues
Causes and Risk Factors
Risk factors for CDI are listed in Table 1 and elaborated
below.
History of CDI. As CDI can be recurrent, a history of
CDI is predictive of CDI in patients presenting with
diarrhea.
Antibiotic Exposure. Antibiotic use is one of the most
significant yet modifiable risk factors for CDI. Number
(dose dependent risk), class, and duration of antibiotic
use (significantly higher risk if > 7 days) impact the risk
for CDI (See Antibiotic Section under Prevention and
Treatment).
Advanced Age. Patients age 65 or older are at several
fold higher risk for CDI.19 Older patients are also at
higher risk for more severe disease with complications,
especially if they have poor preadmission functional
status.
Comorbid Conditions, Severity of Disease and
Hospitalization. Presence of severe underlying
comorbidities has been associated with increased risk of
CDI. Severity of comorbid conditions upon admission,
and longer hospitalization have all been associated with
higher risk for hospital-acquired CDI. Other risk factors
for CDI also include gastrointestinal surgery and the use
of tube feeds.20
Inflammatory Bowel Disease (IBD). Patients with
inflammatory bowel disease (IBD) are at higher risk for
CDI compared to the general population. Thus, all
patients with IBD presenting with diarrhea concerning for
possible IBD flare should also undergo C. difficile
testing, even in the absence of other risk factors for CDI.
In a retrospective study, only 61% of IBD patients with
CDI had antibiotic exposure.21 The risk in IBD patients is
even higher if they have colonic involvement and they
are on immunomodulator therapy.21
Immunosuppression. Immunosuppressed states such as
leukemia, lymphoma, HIV, neutropenia, organ
transplantation, and use of immunosuppressive drugs
significantly increase the risk for CDI. In HIV-infected
patients, CDI is the most common cause for bacterial
diarrhea and risk of CDI correlates with severity of HIV
disease.22,23 Acid Suppressive Therapy. Acid suppressive therapy,
including use of proton pump inhibitors (PPIs), elevates
the risk of CDI. (For expanded explanation, see “Proton
Pump Inhibitors” section on Page 13).
Pediatric Population Risk Factors
Risk factors for acquiring CDI in pediatric populations
include a history of prematurity, prolonged or frequent
hospitalizations, history of antimicrobial therapy, solid
organ transplantation, the presence of gastrostomy or
jejunostomy tubes, and the use of proton pump inhibitors
(see Table 1). Conditions associated with acquisition of
severe CDI are shown in Table 2. Special attention to the
importance of Hirschsprung’s disease, neutropenia from
leukemia and other malignancies, and inflammatory bowel
disease as high-risk factors for severe disease in children
should be noted.24-27

10 Michigan Medicine C. difficile Guideline December 2016
Risks in Community-Associated CDI.
Community-associated CDI has a different risk profile, and
is less likely to be severe CDI. Community-associated CDI
is defined by the Infectious Diseases Society of America as
symptom onset occurring in the community or within 48
hours of hospital admission with no prior hospitalization in
the past 12 weeks. Community-associated CDI affects
populations that were previously thought to be at low risk
such as younger adults without the traditional risk factors
mentioned above. In a US population-based study involving
385 patients with CDI, 41% of cases met the criteria for
community-associated CDI. Patients with community-
associated infection were younger (median age of 50 years
compared with 72 years), had lower comorbid scores, had
less exposure to antibiotics (78% vs 94%), and were less
likely to have severe infection.28
Diagnosis
Testing for C. difficile
Patients with diarrhea and risk factors for CDI should
undergo testing for C. difficile (Figure 1).
The diagnosis of C. difficile infection (CDI) is based on the
combination of both clinical findings (usually diarrhea), as
well as laboratory or histopathological findings (see Table
2) for definition of CDI). Clinical severity can range from
mild diarrhea to severe, fulminant colitis with paralytic
ileus and toxic megacolon. Patients can also have
asymptomatic carriage or colonization of Clostridium
difficile.
The following signs and symptoms suggest patients who
exhibit these features should be tested for the disease. The
most common symptom of CDI is diarrhea, defined as 3 or
more loose or unformed stool in less than 24 hours, without
an alternative cause (e.g., laxative use). The stool may
contain occult blood, but melena and hematochezia are
atypical. Fever and abdominal pain are present in about
50% of patients, and can be markers for increasing disease
severity. Leukocytosis (WBC > 15,000 cells/mm3) occurs
frequently and may actually precede diarrhea or other
clinical symptoms.
The presence of pseudomembranes on lower endoscopy is
essentially pathognomonic for CDI, and occurs in 50% of
cases. Endoscopy is not needed for diagnostics, however, as
stool studies are readily available and active CDI renders a
patient at increased risk for endoscopic complications
including perforation.
Less common signs and symptoms of CDI include
arthralgias and reactive arthritis, as well as severe protein-
wasting diarrhea with resultant hypoalbuminemia, edema
and ascites.
Contraindications to testing for C difficile
Because diarrhea occurs in the majority of patients with
CDI, individuals without diarrhea should usually not be
tested for CDI (Figure 1). The prevalence of asymptomatic
colonization with C. difficile is 10–26% among hospitalized
patients and may approach 50% among patients residing in
long-term care facilities. Test of cure should not be
performed in patients who have finished treatment for CDI
and have experienced clinical improvement in symptoms
because they can have persistent shedding of toxin for up to
6 weeks after completing treatment.29 For the same reason,
there is no indication for testing while an individual is being
actively treated. However, testing can be performed if
symptoms have not resolved following a full treatment
course. Finally, it is important to note that some individuals
may take several weeks after completing therapy for stool
consistency and frequency to become entirely normal. In
addition, some individuals may develop a post-infectious
irritable bowel syndrome after CDI, which can be difficult
to differentiate from true recurrent CDI and clinicians must
use their judgment. In this circumstance, clinicians should
refrain from repeat testing for C. difficile.
Laboratory Testing Algorithms
Two- or three-stage testing algorithms are preferable to
single-step methods.
The optimal rapid laboratory testing algorithm for presence
of toxigenic C. difficile in stool has not been established,
but there is evidence that two- or three-stage testing
algorithms are preferable to single-step methods due to
improved specificity.30
For UMHS testing algorithms See Figures 1 and 2.
When possible, testing should be limited to diarrheal stools
unless the suspicion for CDI is high and an ileus is present.
In select patients (immunocompromised, ileus, or on
empiric therapy) the sensitivity of other rapid tests can be
low and ID consultation and PCR-based testing should be
considered (Appendix A).
The gold standard for organism detection is cytotoxigenic
culture and the corresponding gold standard for toxin
detection is the cell cytotoxicity assay.31 Both methods
require considerable time and expense and are now rarely
performed by clinical laboratories.
An overview of symptoms consistent with CDI is provided
in Figure 1. To avoid false-positive results (e.g., positive C.
difficile testing in the setting of colonization), only diarrheal
stools (those that take the shape of the container) should be
submitted for testing. An exception to this is the case of
patients with suspected CDI and ileus, in which case stool
of any consistency can be considered for testing. If a patient
with ileus and suspected CDI is unable to produce stool, a
rectal swab for tcdB PCR can be sent for after consultation
with ID. If a patient has an ileostomy with higher then
baseline output (without an alternative explanation) then a

11 Michigan Medicine C. difficile Guideline December 2016
stool specimen can be sent for CDI testing. In patients
where there is concern for CDI involving the rectal stump, a
rectal swab for direct tcdB PCR may be sent after
consultation with ID. (For PCR testing at UMHS, after
electronically placing an order for a C. difficile test, phone
the lab to request PCR only from the swab. See Appendix A
for available diagnostic tests for toxigenic C. difficile).
The recommended UMHS testing algorithm consists of two
initial EIA tests (GDH and Toxins A/B), with reflex to a
PCR test for tcdB gene for discordant results (Figure 2).
Data and recent guidelines support the use of multi-step
over single-step testing with EIA for toxigenic C. difficile
due to improved test characteristics, though single-step
testing via PCR also performed well.30-34 This algorithm has
been validated by our clinical laboratory and has a negative
predictive value of 99%.35
There are circumstances when false-negative results can
occur with EIA testing alone. Immunocompromised
patients with symptoms suggestive of CDI (colitis on
imaging, ileus with minimal stool production, and/or WBC
>15,000 cells/µL with diarrhea) and patients receiving
empiric therapy at the time of diagnosis are at risk for a
false-negative EIA test.36 In these patients, if PCR testing
was not performed, an ID consult and direct PCR for tcdB
on stool or via rectal swab should be considered (at UMHS,
ordered separately by phone). Finally, single-step PCR
testing (not part of the UMHS algorithm) occurs as part of
the new Biofire test panel for gastrointestinal pathogens
(FilmArray, BioFire Diagnostics Inc., Salt Lake City, UT).
This test should not be used if CDI is suspected, and
providers should follow the recommendations in Figure 2
and order multi-step testing as indicated. However, if C.
difficile is detected as part of the Biofire panel and the
patient’s symptoms are compatible with CDI, then a
separate order for multi-step testing is unnecessary and
providers should refer to our treatment algorithm (Figure 3)
and begin therapy as indicated.37
Imaging. In patients with abdominal distention and
suspicion for CDI, radiologic evaluation may serve as a
useful diagnostic adjunct. This is especially true if there is a
concern for CDI-induced ileus or toxic megacolon. Plain
film abdominal x-rays may show dilated colon or ileus
pattern. If free air is present on x-ray imaging, emergent
surgical consult is warranted.6,38
In patients who present with abdominal pain, significant
abdominal distention, or other signs of complicated CDI,
computed tomography (CT) of the abdomen and pelvis may
be considered for further evaluation. Findings on CT may
include colonic wall thickening, ascites, megacolon
(distension of the colon of >6 cm in transverse width), ileus
or perforation.4 Overall CT sensitivity for diagnosis of C.
difficile colitis is 52–85%, with specificity of 48–93%.39
The use of enteral, intravenous and rectal contrast is
preferred by UMHS Acute Care Surgery group, unless
otherwise contraindicated. Some institutions advocate a
more rigid adherence to CT scan diagnostic criteria for C.
difficile colitis of colon wall thickening of greater than 4
mm combined with any one or more findings of pericolonic
stranding, colon wall nodularity, the “accordion” sign
(alternating edematous haustral folds separated by
transverse mucosal ridges filled with oral contrast material,
simulating the appearance of an accordion40), or otherwise
unexplained ascites, with a reported sensitivity of 70% and
specificity of 93% 39 (Figure 4).
Patients who have CT findings concerning for severe or
complicated CDI, or who are critically ill with documented
severe CDI warrant early surgical consultation. Specific
findings have not been shown to reliably predict the need
for surgical intervention.39,41 However, early involvement
of a general surgeon may initiate discussions of treatment
options, including consideration for diverting loop
ileostomy for antegrade colonic irrigation. (Refer to section
on surgical management, Figure 5).
Endoscopy. Colonoscopy may be useful in patients with
persistent diarrhea despite negative C. difficile toxin or with
toxin-positive CDI refractory to antibiotics. In patients with
positive stool testing for CDI, a colonoscopy is not
necessary for diagnosis given that pseudomembranes are
present only in 50% of patient with toxin-positive CDI.42
Additional indications to perform a colonoscopy in toxin-
positive CDI patients include the assessment of CDI
severity and the management of severe colonic distension
associated with ileus. It is worth noting that a negative
flexible sigmoidoscopy does not rule out CDI as sparing of
the rectosigmoid colon is common in CDI patients with
pseudomembranes on colonoscopy.43
Colonoscopy is contraindicated, especially for diagnostic
purposes, in patients with hemodynamic instability or with
significant risk for bowel perforation (e.g., fulminant
colitis, recent bowel surgeries, bowel obstruction).
Differential Diagnosis of Diarrhea. C. difficile-toxin
negative patients with persistent diarrhea should be
evaluated further with colonoscopy with random biopsies
and esophagogastroduodenoscopy (EGD), with duodenal
biopsies for inflammatory and non-inflammatory causes of
persistent diarrhea. Inflammatory diarrhea includes
inflammatory bowel disease (ulcerative colitis and Crohn’s
disease), celiac disease, microscopic colitis (collagenous
and lymphocytic colitis), CMV (in immunocompromised
hosts), and routine enteric pathogens when patients have
exposure history or risk factors. Non-inflammatory causes
include, dietary intolerance (lactose, fructose, or rapidly
fermentable, short-chain carbohydrates [“FODMAP”44]) or
small intestinal bacterial overgrowth in patients with
significant abdominal bloating. Functional etiologies
(irritable bowel syndrome) should be considered when
workup is negative for inflammatory and non-inflammatory
diarrhea.
Disease Classification
Criteria for disease classification are summarized in Table
3, and discussed below.

12 Michigan Medicine C. difficile Guideline December 2016
Though risk factors for adverse outcomes after CDI have
been identified, there is no generally accepted and validated
definition for severe CDI. Nonetheless, it is important to
classify the episode as mild-moderate, severe, or
complicated prior to initiation of CDI therapy. It is
imperative to classify CDI by disease severity and whether
the CDI episode represents a recurrence, because it
influences the choice of therapy. Recurrent CDI often
requires a longer duration of therapy, consideration of
adjunctive treatments such as antimicrobial “chasers,” or
fecal microbiota transplantation (FMT).
CDI can range from self-limited disease to severe infection,
sometimes resulting in colectomy or death.7 Even among
those that recover, recurrent disease is common.8 Although
the reasons are incompletely understood, older adults are
disproportionately affected by adverse outcomes.16
Despite these epidemiologic links, no robust, validated
predictive models for the development of adverse outcomes
from CDI or recurrence exist for clinical use. Several
prediction models for severe disease outcomes based on
initial diagnostic criteria have been proposed with variable
sensitivity/specificity. Eight different published scores for
severe disease have been compared at diagnosis to assess if
they predicted complicated CDI in a validation cohort.45
The scores used a variety of clinical variables including
age, medication use, symptoms, vital signs, physical exam
findings, laboratory parameters, and abdominal
radiographic changes. The agreement between predicted
and observed outcomes was variable (Cohen’s κ 0.18–
0.69). The “Hines VA” score had the highest κ but was only
73.7% sensitive. The classification criteria for CDI used in
this guideline are presented in Table 3. These were drafted
after considering published guidelines on CDI,1,4,37,45,46 and
several studies on predictors of adverse outcomes and
recurrence, and the expert opinion of this guideline
committee’s membership.
This guideline’s definition for recurrence follows the CDC
definition. Recurrent disease is defined as the presence of
recurrent symptoms and positive testing within 8 weeks of
initial onset (the index episode), but after the original
symptoms resolved.1 There are situations, however, when
patients will have another episode of CDI soon after this
arbitrary 8-week window has elapsed. In such cases, it may
not be unreasonable to classify these episodes as recurrent
and treat accordingly (Figure 3). This is especially
important in patients with risk factors for further
recurrences, including the need for concurrent therapy with
antimicrobials to treat condition other than CDI, age 65 or
older, and use of proton pump inhibitors.8
Special Populations
Extra-colonic CDI. Small bowel enteritis secondary to C.
difficile is rare, but usually occurs in patients with a partial
or total colectomy. The literature on this topic consists
primarily of case reports,47 making it difficult to
recommend specific treatment strategies. However,
outcomes in small bowel enteritis from CDI can be poor
and, these patients warrant aggressive therapy in most cases
(see severe and complicated CDI arms in Figure 3).
Inflammatory Bowel Disease. There is a high incidence of
CDI in IBD patients.48-51 The most likely explanation is the
shared risk factor of an altered gut microbiota, known as
dysbiosis.52 Thus, workup of patients presenting with signs
and/or symptoms of IBD flare should include testing for
CDI. IBD patients at significant risk for CDI include those
living in nursing homes, with recent or ongoing
hospitalization, with previous broad-spectrum antibiotic
use, and with a surgical pouch.53-56 Other risk factors
include increased severity of colitis and
immunosuppression (especially corticosteroids with 3-fold
risk increase).21,57-60
Pediatric population. CDI may be associated with
significant morbidity and mortality in children.24,61 In
general, the diagnosis of CDI in pediatric patients follows
the same diagnostic criteria and algorithms for adult
patients as discussed above (see Figure 3). However, the
accurate diagnosis of CDI in infants and young children
represents a special challenge given a high rate of
asymptomatic C. difficile colonization in this population.
Treatment decisions in this population should be made in
conjunction with ID consultation. Please note the following
age-specific recommendations for interpretation of testing
results:
1. Testing for CDI in infants < 12 months of age is
generally not recommended. It is recommended to
consult Pediatric ID if CDI is suspected in infants <12
months of age. Testing should be limited to those
symptomatic with frequent diarrhea and/or ileus who
meet one or more of the following conditions:
Have comorbidities associated with severe CDI
(see Table 3)
Have history of multiple antibiotic exposures
C. difficile outbreak situations
Note: Alternative etiologies for diarrhea should always
be considered even in those infants < 12 months of age
with a positive test for CDI (e.g., viral gastroenteritis,
food allergy, carbohydrate malabsorption, immune-
mediated condition, etc.).
2. Children 12 to 36 months of age may have
asymptomatic colonization. A positive test result in a
symptomatic patient indicates possible CDI.
Alternative etiologies for diarrhea should continue to
be considered even in those testing positive for CDI.
3. Children >36 months of age who are symptomatic
with diarrhea and/or ileus, with positive testing results
suggests probable CDI, especially in those with risk
factors including history of antibiotic therapy, use of
proton pump inhibitors, or comorbidities associated
with severe CDI (see Table 1 and Table 3).

13 Michigan Medicine C. difficile Guideline December 2016
Asymptomatic carriage of C. difficile varies significantly by
age. A review of multiple studies of carriage in healthy
infants and young children determined colonization of
neonates up to 1 month of age occurs at an average of 37%,
between 1 to 6 months of age at an average of 30%,
between 6 to 12 months of age at an average of 14%, and
by 36 months of age the carriage rate is similar to that of
healthy, non-hospitalized adults at < 3%.62 Carriage may be
transient, and different strains of C. difficile may colonize
an individual over time as new strains are acquired from the
environment. Breastfed infants have lower C. difficile
carriage rates than do formula-fed infants (14% vs. 30%,
respectively), but these differences decrease after 12
months of age.62 Given the frequency of asymptomatic
colonization, testing for CDI should generally only be
performed in children with diarrhea and other risk factors
for CDI.63 Despite high rates of colonization and significant
amounts of detectable toxin, clinical illness with CDI is
relatively uncommon in children <36 months of age.
Hypotheses regarding the lack of clinical illness in infants
and young children include the possibility that neonates and
infants lack cellular receptors to bind and process C.
difficile toxin, preferential colonization by nontoxigenic or
less-pathogenic strains, and protective factors in breast milk
and the developing microbiota.25,62 Rates of hospitalized
infants and young children with positive CDI testing are
increasing, but again, many studies do not adequately
distinguish CDI disease from asymptomatic
colonization.25,26,64,65 Therefore, it is critical to consider
other etiologies for diarrhea in infants and young children,
even in those with positive CDI testing. Consultation with a
Pediatric Infectious Diseases specialist may be helpful
when considering the need for treatment in young age
groups.25
Pediatric Disease Classification. In pediatric patients, a
diagnosis of CDI may be considered based on a
combination of signs and symptoms, generally involving
frequent diarrhea, and evidence of C. difficile and toxin
present in stool (see age-based interpretation of testing
results above).
1. In pediatric patients CDI is classified as mild to
moderate when lab values are reassuring (e.g., WBC
<15,000 cells/mm3 and serum creatinine <1.5 times
baseline level), similar to adult classification schemes
(see Table 3).
2. In patients failing to improve after 3 to 5 days of
therapy, lab values should be repeated to determine if it
is still appropriate to maintain classification as mild to
moderate, or if the classification should be escalated to
severe.
3. In pediatric patients CDI is determined to be severe
when ≥ 2 lab values are abnormal (e.g., WBC ≥ 15,000
cells/mm3, creatinine >1.5 times baseline level, ANC ≤
500, or ALB ≤ 2.5) OR the presence of high-risk
patient factors for severe CDI exists (e.g.,
Hirschsprung’s disease, neutropenia from leukemia,
IBD). Patients with these high-risk factors should
generally be classified as, and treated for, at least
severe disease (see Table 3).
4. In pediatric patients CDI is determined to be
complicated when evidence exists of sepsis, shock,
ileus, toxic megacolon, peritonitis, bowel perforation,
or other conditions requiring ICU admission within 2
days of CDI diagnosis are present (see Table 3).
5. For pediatric patients meeting severe or complicated
clinical criteria (see Table 4), or having risk factors
associated with severe CDI disease (see Table 3),
testing should be performed as described above (see
Figure 2), and empiric therapy should be strongly
considered while awaiting results.
The majority of CDI in infants and children is of mild to
moderate disease severity criteria.26,27,66 Applying the same
criteria for adult severe disease to pediatric populations
tends to overclassify pediatric disease as severe, hence the
need for 2 or more abnormal lab criteria required to make a
severe diagnosis (or the presence of a high-risk condition).
The frequency of pediatric CDI patients meeting criteria for
severe disease is low (~8%), with similar proportions of
severe disease noted across all pediatric age groups.66
Prevention
Antibiotics and Prevention
Nearly all antimicrobial classes have been associated with
CDI. However, clindamycin and cephalosporins (especially
third-generation cephalosporins) have been consistently
associated with the highest risk of CDI. After the
emergence of the epidemic NAP1/ribotype 027 strain in
2002, fluoroquinolones, have also been associated with a
high risk of CDI.67-69
The risk of CDI is highest during antibiotic therapy and in
the first month after cessation of antibiotics (7 to 10 fold
increased risk compared to patients who did not receive
antibiotics). Risk appears to normalize 3 months after
cessation of antibiotic therapy.70 The use of >14 Defined
Daily Doses (DDDs) of antibiotics in the 3 months prior to
CDI had the strongest association with CDI (OR 8.50;95%
CI 4.56–15.9). Another study found the risk of CDI
increases with cumulative dose and number of antibiotics,
as well as days of antibiotic exposure.71 Poor clinical
outcomes in patients with CDI were independently
associated with concomitant use of non-CDI-related
antimicrobials,72 and are associated with a doubling in risk
of failure of CDI therapy.73 In addition, use of non-CDI-
related antimicrobials within 30 days of an episode of CDI
is associated with a 3-fold increase in CDI recurrence.74
Based on the results of these studies, it is imperative that
providers stop unnecessary antibiotic therapy to reduce the
risk of CDI.
Use of Prophylactic Vancomycin
Recommendations:
1. Consider use of vancomycin prophylaxis in patients that
recently had a first or greater recurrence of CDI and require
antimicrobials for a different infection.

14 Michigan Medicine C. difficile Guideline December 2016
2. The dose of prophylactic vancomycin is 125 mg PO BID
to QID and the duration of prophylaxis should be at least
50% of the expected duration of antibiotic therapy for the
other infection.
There is a paucity of evidence to support the practice of
extending or using vancomycin prophylactically in patients
that recently were diagnosed with CDI and require non-CDI
antibiotics for treatment of a different infection. A recent
retrospective study showed that, for patients where the CDI
episode was a first or greater recurrence, prophylactic
vancomycin reduced the risk of recurrent CDI by nearly
50% when on other antibiotics. Potential downsides of this
strategy include selection for resistant organisms such as
vancomycin-resistant Enterococcus, onset or worsening of
antibiotic-associated diarrhea, and additional expense.
Probiotics
Probiotics are not recommended as primary prevention of
CDI in hospitalized patients. There are conflicting data on
whether probiotics are effective in preventing primary
episodes of CDI in patients receiving antibiotics, with the
largest RCT to-date including over 2,000 patients failing to
replicate possible reductions seen from meta-analyses of
smaller, more heterogeneous trials.75,76 Also, there are
concerns regarding safety in patients with certain comorbid
conditions (immunocompromised- receiving chemotherapy,
recipients of solid organ transplant or bone marrow
transplant) which are common among hospitalized patients.
The literature has noted invasive infections or poor
outcomes with Lactobacillus probiotic use in
immunocompromised patients,77 patients with severe acute
pancreatitis,78 and patients with central venous catheters.79
As such, we do not recommend the use of probiotics in
primary prevention of CDI in hospitalized patients.
Proton Pump Inhibitors (PPIs)
PPIs and acid suppression may increase the risk of CDI and
recurrence of CDI. Unnecessary use of PPIs should be
avoided and acid suppression should be minimized,
especially in patients with a history or current diagnosis of
CDI. A systematic review of case-control and cohort
studies has shown an association between PPIs and
increased risk of CDI.8 Although a causal relationship is not
clear, this finding is similar to prior systemic reviews.80 A
prospective cohort study showed that increasing levels of
acid suppression correlated with increased risk of
nosocomial CDI, with the highest risk in patients receiving
greater than once daily PPI dosing.81
Infection Control Measures
Isolation. Patients with diarrhea and a positive C. difficile
lab test must be placed in Contact Precautions Diarrheal
(CP-D). Patients are placed in either a private room or
cohorted with another patient with CDI. CP-D rooms are
bleach cleaned on a daily basis and upon discharge.
Healthcare personnel must wear an isolation gown and
gloves upon entry to the room. Healthcare personnel must
remove gowns and gloves upon exiting the room and wash
hands with soap and water. Any equipment leaving the
room is disinfected with bleach.
Preemptive Isolation (Initiation of isolation for patients
with diarrhea prior to test results). CP-D is not required, but
may be utilized at the discretion of Infection Prevention &
Epidemiology (IPE) or the provider. (At UMHS, nursing
may initiate this by working through the provider or IPE.)
See Table 5 for further guidance on preemptive isolation.
Disinfection and Hygiene. Both the patient’s immediate
environment and the broader environment have been
implicated in the spread of C. difficile. Quaternary
ammonia-based disinfectants have been shown to be
ineffective against C. difficile spores. Bleach is sporicidal
and has been shown to decrease the bioburden of C. difficile
in the healthcare setting.82-85 An approved hospital
sporicidal (such as bleach) must be used on rooms of
patients with CDI as well as any equipment leaving those
rooms. In locations where bleach is the approved sporicidal,
a bleach wipe or 1:10 bleach solution may be used.
Additionally, patients undergoing inpatient fecal microbiota
transplantation (FMT) should have their rooms cleaned
with an approved hospital sporicidal, with the same rigor as
used in terminal cleaning, prior to them returning to the
room from the endoscopy suite. In addition to using the
appropriate disinfectant, the importance of good mechanical
cleaning with the product should be emphasized to
maximize the mechanical removal of spores.
Alcohol based hand rub is not effective against C.
difficile spores.
Hands are to be cleaned with soap and water upon
exit of a CDI room to ensure mechanical removal of
the spores.86
Duration of Isolation. Patients are to remain in CP-D for
the duration of their hospitalization, as their hospital room
will remain contaminated with C. difficile spores as long as
they inhabit it. Terminal cleaning and decontamination is
not possible with the patient present; spores persist and may
continue to be transmitted. Thus, patients must remain in
CP-D and the room must be terminally cleaned at
discharge. This recommendation for isolation holds even
for FMT recipients after their room has been cleaned with
bleach following the FMT. In special circumstances,
arrangements may be made to move the patient to allow for
a terminal clean and the discontinuation of precautions.
These are determined on a case-by-case basis with IPE and
the clinical team.
Isolation Practices for Readmission. When patients with a
history of CDI are readmitted, they do not need to be placed
in CP-D unless they are readmitted with diarrhea. Patients
with a history of CDI that are readmitted with diarrhea
should be managed in CP-D until CDI has been ruled out.
Visitor/Family Recommendations. For the protection of
family members, it is recommended that family and visitors
wear an isolation gown and gloves when assisting in the
care of a patient with CDI. Family and visitors must wash

15 Michigan Medicine C. difficile Guideline December 2016
hands with soap and water upon leaving the patient room.
Though family and visitors may move about the facility,
they should not utilize the unit nourishment room. There is
no published evidence that visitors contribute to the spread
of CDI in hospitals. Studies have included interventions
such as having visitors comply with wearing cover gowns
and gloves in CDI rooms, but no studies have evaluated the
sole impact of visitors on CDI transmission.
Isolation of Asymptomatic Carriers. Except in special
circumstances, asymptomatic carriers are not placed in CP-
D. At UMHS, the exception to this is the adult bone
marrow transplant unit. Adult Bone-Marrow Transplant
(BMT) patients are screened for C. difficile upon admission
and if positive, placed in CP-D for the duration of their
hospitalization. Patients are placed in CP-D, even if they
don’t currently have symptoms as many of the treatments
for which they are admitted can cause them to become
symptomatic. Because BMT patients are such a vulnerable
population, this protects non-colonized patients from
exposure. Please note this policy does not apply to UMHS
Pediatric BMT units given the high rate of asymptomatic
colonization among young children.
Medical Treatment of C. difficile Infection
The approach to antibiotic treatment for CDI is shown in
Figure 3. Details of the treatment options and
considerations are listed below.
Treatment of asymptomatic carriers is not recommended.
There is no role for prophylactic CDI therapy in
asymptomatic carriers. In a small, randomized placebo
controlled trial, only oral vancomycin (not metronidazole)
was effective in reducing C. difficile carriage. However oral
vancomycin treatment was associated with significantly
higher rates of C. difficile carriage 2 months after
treatment.87 Further study is needed to assess the role of
asymptomatic carriers in C. difficile transmission and the
need for isolation precautions. In a prospective study, 29%
of cases of hospital acquired CDI were associated with
carriers.88
Antimicrobial Treatment Based on Disease
Severity
Antimicrobial treatment for CDI is based on the severity of
the disease:
Mild-Moderate CDI: metronidazole 500 mg PO TID
Severe CDI: vancomycin 125 mg PO QID
Complicated CDI: vancomycin 500 mg PO QID,
metronidazole 500 mg IV every 8 hours, and if ileus,
small bowel obstruction, or toxic megacolon
vancomycin enema every 6 hours.
Two recent, prospective, randomized trials comparing oral
metronidazole and oral vancomycin to tolevamer, found
vancomycin was associated with clinical success even after
adjusting for disease severity.89,90 However, this study was
not designed or powered for this secondary analysis that
pooled data from 2 RCTs.89,90 Another RCT comparing
metronidazole and vancomycin, found vancomycin
treatment was associated with a higher rate of clinical cure
in patients with severe CDI (ZAR 2007). Currently, oral
metronidazole is recommended for the treatment of
mild/moderate CDI (except with ≥2 recurrences; see Figure
3), and oral vancomycin is recommended in severe CDI.37,46
Oral vancomycin is also preferred in pregnant or
breastfeeding patients, those with metronidazole allergy, or
those receiving concomitant warfarin.
The duration of therapy in the above trials was 10 days.
However, some patients may respond slowly to treatment
and IDSA guidelines endorse treatment for 10–14 days.46
Intravenous metronidazole is less efficacious than oral
metronidazole or oral vancomycin in the treatment of CDI,
and should only be utilized when oral or enteral
administration is not feasible.
There is no supportive data for the use of oral vancomycin
doses ≥ 125 mg QID in patients with mild, moderate, or
severe disease without complications. There is an absence
of data regarding the optimal treatment of complicated CDI.
Guidelines currently recommend combination therapy with
administration of intravenous metronidazole and high-dose
oral vancomycin (500mg QID) in patients with complicated
CDI.91,92 Intracolonic administration of vancomycin may be
considered in all patients with complicated CDI, but should
be given in patients with ileus, small bowel obstruction, and
toxic megacolon.92 In the absence of data, longer durations
of therapy (≥ 14 days) may be recommended in patients
with complicated CDI,4,37,46 and final treatment plan should
be formulated in discussion with the infectious diseases
consult team.93
C. difficile Enteritis (small bowel involvement). Patient
with CDI of the small bowel should be treated with oral
vancomycin 125 mg PO QID. Small bowel involvement
with C. difficile is rare but has been reported.47 The
majority of patients with C. difficile enteritis have either
surgically altered intestinal anatomy such as colectomy
with ileostomy and/or inflammatory bowel disease. In a
review of 56 patients with C. difficile enteritis the majority
of patients required ICU management and mortality was
high (32.1%).47 In patients with an ileostomy, fever and
increased ileostomy output should prompt further
evaluation for C. difficile infection. The optimal treatment
of C. difficile enteritis is unknown. However, since these
patients are often refractory to metronidazole therapy,94
often require ICU management, and have a high mortality,47
vancomycin treatment is recommended.
Recurrent C. difficile Infection. The treatment of CDI
recurrence depends on how many recurrences the patient
has experienced.
First recurrence: Classify as mild-moderate, severe, or
complicated and treat accordingly.
Second or multiple recurrences (third or more episode
of CDI):
- vancomycin PO (dose, need for concurrent IV
metronidazole/vancomycin enemas depends on

16 Michigan Medicine C. difficile Guideline December 2016
disease classification as noted in the sections
immediately above) for 10–14 days then taper to
125 mg PO BID for 7 days, 125 mg PO daily for 7
days, and then pulse with 125 mg PO every 2-3
days for 2–8 weeks. Duration of taper should be
determined in conjunction with the infectious
diseases consult services.
OR
- fidaxomicin 200 mg PO BID for 10 days (with
infectious diseases consult service approval).
There is a paucity of data regarding the optimal treatment of
patients with recurrent CDI. Guidelines currently
recommend treatment concordant with severity of disease
for the first recurrence (i.e., metronidazole for mild-
moderate CDI and vancomycin for severe CDI46). Due to
the possibility of peripheral neuropathy with prolonged
exposure to metronidazole, guidelines recommend
vancomycin therapy for second (or further) recurrences.
Tapered or pulsed dosing regimens of vancomycin have
been shown to reduce the risk of further recurrences
compared to placebo in patients with multiple recurrences,
and thus are recommended in patients with a second (or
further) recurrence.4,31,46,95
In a randomized, trial of patients with either a first episode
of CDI or first recurrence, fidaxomicin was non-inferior to
vancomycin in terms of clinical cure rates.96 Recurrence
rates were lower with fidaxomicin, but only in the subset of
patients infected with non-NAP1/027 strains. Due to
uncertain cost-effectiveness (~$300/day) compared to
vancomycin (especially when vancomycin is compounded
from the intravenous formulation),97,98 the role of
fidaxomicin in CDI therapy remains undefined. At UMHS
fidaxomicin requires ID approval and has been reserved for
treatment of CDI in patients with documented recurrent
disease who have failed a recent vancomycin taper.
Fidaxomicin has not been studied in patients with
complicated CDI, and should not be utilized in this
scenario.
Numerous agents (rifaximin or fidaxomicin “chasers,”
which are provided at the end of a vancomycin taper;
tigecycline; IVIG; nitazoxanide; etc.) have been studied in
patients with refractory or recurrent CDI.99-102 The data
supporting their use is limited. Rifaximin or fidaxomicin
chasers can be considered in patients with multiple
recurrences especially in patients who choose not to
perform fecal microbiota transplantation (FMT) or who are
not candidates for FMT.99,100
To our knowledge, there is a paucity of data evaluating
extension of CDI therapy duration for patients receiving
non-CDI antibiotics.103 However, concomitant anti-
microbials in the context of CDI are associated with poor
clinical outcomes, extended time to resolution of diarrhea,
treatment failure, and recurrence of CDI.30,72,73,104 In one
study, the use of non-CDI antimicrobials within 30 days of
an episode of CDI was associated with a 3-fold increase in
CDI recurrence.74 Therefore, it may be advisable in patients
at high risk for recurrent CDI to overlap and extend anti-
CDI therapy beyond the duration of concomitant antibiotic
use. However, there are no data to support providing
secondary prophylaxis for all patients with CDI on
concomitant antibiotic therapy. Consultation with ID is
recommended to determine if the patient would benefit
from this practice.105
Probiotic Treatment
Probiotics as adjunct treatment of CDI is not recommended
in hospitalized patients. There are limited data supporting
the use of Lactobacillus-containing probiotic preparations
in the treatment of CDI, and use is not recommended.
Two randomized, double-blind, placebo-controlled trials
have shown that Saccharomyces boulardii, in conjunction
with standard treatment for CDI, significantly reduces the
number of further episodes of CDI in patients with a history
of recurrent infection.106,107 However, a recent meta-
analysis only showed a modest but non-significant
reduction in recurrent CDI from either S. boulardii or
Lactobacillus species.108 Additionally, the use of
Saccharomyces probiotic preparations has been associated
with invasive infection in patients with central venous
catheters, intestinal disease (abdominal surgery, intestinal
obstruction, ulcerative colitis, neoplasm, bowel or gastric
ulcerations), and critically ill or immunocompromised
patients.109 In the opinion of this committee, these safety
concerns preclude use of S. boulardii for hospitalized
patients with CDI.
In patients with multiple recurrences of CDI, who are not
candidates for FMT, a regimen of staggered and tapered
oral vancomycin in combination with kefir can be
considered. A prospective case series of patients with
multiple recurrences of CDI found that daily administration
of kefir (a probiotic yogurt drink) in combination with a
staggered and tapered oral vancomycin or metronidazole
regimen achieved a treatment success rate of 84%.110
Immunotherapy
Intravenous Gamma globulins (IVIG) can be considered in
patients with hypogammaglobulinemia and recurrent CDI,
but IVIG in all other patient populations is not
recommended. There are no randomized controlled trials on
the use of human IVIG. A retrospective analysis of 18
patients with severe CDI treated with IVIG and standard
therapy found no difference in clinical outcomes compared
with matched controls.111 In patients with recurrent CDI and
hypogammaglobulinemia (<450 mg/dL) in the presence of
a cancer or immune deficiency disorder, IVIG can be
considered on a case by case basis. In a randomized,
double-blind, placebo-controlled Phase II trial, addition of
two neutralizing monocolonal antibodies against C. difficile
toxins A and B to standard therapy did not impact the initial
infection course but did significantly reduce infection
recurrence. This therapy is currently being evaluated in
Phase III trials.4,31,111,112

17 Michigan Medicine C. difficile Guideline December 2016
Recently, two phase-3 studies, MODIFY I and MODIFY II
evaluated the efficacy of two monoclonal antibodies,
actoxumab (ACT) and bezlotoxumab (BEZ), with activity
against TcdA and TcdB, respectively. The study arm with
ACT alone was stopped early due to lack of efficacy in an
interim analysis. The pooled analysis of the 2327 patients
that received either ACT + BEZ or BEZ alone observed
recurrent CDI in 15.4% and 16.5%, respectively, versus
26.6% in the placebo arm (P <.001). The safety profiles in
the interventional arms were similar to the placebo arm.113
Toxin-Binding Polymers and Resins
Therapy with toxin-binding polymers (tolevamer) and
resins (cholestyramine and colestipol) is not recommended.
In two multinational, randomized, controlled trials, clinical
success (defined as resolution of diarrhea and absence of
abdominal discomfort) of tolevamer (a non-antibiotic,
toxin-binding polymer) was inferior to both metronidazole
and vancomycin.89 Regarding toxin-binding resins,
colestipol was found to be no more effective than placebo at
decreasing fecal excretion of C. difficile toxin.114
Cholestyramine, another resin, binds oral vancomycin,
which may lead to decreased concentrations of the
antibiotic,115 and thus concomitant cholestyramine and oral
vancomycin administration should be avoided in patients
with CDI.
Fecal Microbiota transplantation (FMT)
Recommendations: 1. FMT is a good treatment option for multiple
recurrences of CDI (after two or more recurrences of
CDI within one year) and can be considered in patients
with CDI not responsive to standard treatment by day
5, assuming escalation of pharmacologic therapy has
already been attempted (Figure 3).
2. At UMHS, outpatient FMT is initiated in the outpatient
ID clinic and requires a referral. Inpatient FMT is
initiated through consultation of the inpatient ID and
GI consult services, though GI consult is unnecessary if
the patient is already on the GI inpatient service.
3. Conventional therapy should be pursued for the
treatment of primary CDI or first recurrence. There is
insufficient experience with FMT to recommend it as a
primary approach. More longitudinal data on patients
that have undergone FMT are needed; therefore,
judicious use of this treatment modality is warranted.
4. Conventional therapy should be pursued first in
patients with severe CDI, and FMT is contraindicated
in patients with complicated CDI. The safety and
efficacy of FMT for these patients has not been
established.
5. Caution should be exercised with use of FMT in
patients with IBD. Those who undergo FMT for CDI
may be at increased risk of IBD flare.
6. Either frozen or fresh stool can be used for FMT in the
setting of recurrent CDI.
Overview. The human gut microbiome is a diverse
community with thousands of bacterial species116 which
likely protects against invasive pathogens.117,118 The
pathogenesis of CDI is thought to require disruption of the
gut microbiota prior to the onset of symptomatic disease,119
usually through antibiotic exposure.120
Even after recovery from CDI, some patients retain a
susceptible microbiome and can have recurrent CDI.121 This
can occur either from recrudescence of the original
infection or from reinfection with a new C. difficile
strain.122 A small minority of patients (<5%) have difficulty
achieving clinical cure with conventional antibiotic therapy
and will enter a cycle with multiple recurrences,123,124 often
relapsing soon after antibiotics are stopped. Restoration of
the gut microbiome through fecal microbiota
transplantation (FMT) appears to be the most effective
treatment strategy for these patients and has gained
widespread acceptance in the medical community.125
Indications and Summary of Evidence. There is
insufficient experience with FMT to recommend it for the
treatment of primary CDI or first recurrence vs. standard
therapy with either vancomycin or metronidazole.126,127
There is also insufficient evidence for treatment of severe
CDI or complicated CDI with FMT, though several
published case reports suggest that it may be effective.128-131
Based on a wealth of data from case reports, systematic
reviews, and clinical trials,132-144 FMT appears quite
effective for recurrent CDI with cure rates exceeding 85–
90% in most studies.
Thus, the UMHS FMT protocol excludes patients with
primary CDI, first recurrence of CDI, or complicated
disease but other patients become eligible for FMT with
two or more recurrences of CDI (especially within 1 year).
Additionally, patients are eligible for FMT with CDI not
responsive to standard treatment by day 5, assuming
escalation of pharmacologic therapy has already been
attempted (Figure 3).
Often, donors are family members or close friends. Some
studies suggest that related donors are associated with a
higher resolution of CDI than unrelated donors, 93% vs.
84%, respectively. However, the results of a meta-analysis
indicated that there was no significant difference between
outcomes from related and unrelated donors.145
Furthermore, a randomized non-inferiority trial conducted
in patients with recurrent CDI found that the use of frozen
stool for FMT resulted in a rate of clinical resolution of
diarrhea that was no worse than that obtained with fresh
stool for FMT (per-protocol analysis revealing ,83.5% vs.
85.1%; difference, −1.6% [95% CI, −10.5% to ∞];
P=0.01).146

18 Michigan Medicine C. difficile Guideline December 2016
Protocol. The optimal parameters for FMT, including stool
preparation, infusion amount, and infusion route, are not
known, but FMT appears highly effective regardless of
variability in these specifics.132 There are three formulations
of stool available at UMHS through the non-profit stool
bank OpenBiome (Somerville, MA): oral fecal capsules
(outpatient only), upper GI (for G- or J-tubes only;
nasogastric or Dobhoff tube routes are not available), and
lower GI (sigmoidoscopy- or colonoscopy-delivered, in the
medical procedures unit). The upper and lower GI infusions
can also utilize stool from a directed donor (related or
unrelated), selected by the patient and/or their family.
OpenBiome has a rigorous donor selection process that
entails thorough screening questionnaires and testing of
donors and donor stool in order to ensure safety. The oral
capsule formulation has specific exclusion criteria and
lower efficacy compared to lower delivery of FMT.142,147
The efficacy of capsules is 70% with one administration
and 94% with multiple administrations.148
Outpatient FMT requires the patient be seen in the
infectious diseases (ID) clinic, so the protocol is initiated
through a referral to the ID clinic and the ID provider will
coordinate the process from that point onward. Inpatient
FMT requires consults to be placed to both the ID and
gastroenterology (GI) services, if GI is not already the
primary service for the patient. The ID/GI inpatient services
will coordinate the process from that point onward.
Preparation of the recipient ideally involves cessation of all
antibiotics, including those used to treat CDI, 48 hours prior
to FMT. In recipients undergoing FMT via colonoscopy a
standard colonoscopy bowel preparation usually must also
be administered. The ID and GI physicians coordinating the
FMT will make any final determinations about exceptions
to these criteria or modifications in the FMT preparations.
Safety. FMT is generally safe and effective for most
patients with recurrent CDI in the short term (1-2 years).93
Among most immunocompromised patients, FMT also
appears safe.140 However, patients with IBD may be at
increased risk for disease flare, fever, and/or elevation in
inflammatory markers following FMT.140,149-151 Though
several case reports exist, there is insufficient data on safety
or efficacy to support the use of FMT for severe CDI.128-131
Of particular concern is a case of toxic megacolon that
resulted in death of a patient that received FMT for severe
CDI, though it is undetermined whether FMT itself or
withdrawal of antibiotics for CDI following FMT
contributed to the outcome.152
There are few data on long-term safety of FMT, but the
intestinal microbiota has been associated with colon cancer,
diabetes, obesity, and atopic disorders such as asthma.153
One study following patients for 3-68 months (mean 17
months) after FMT154 noted the development of new
conditions, including autoimmune disease, ovarian cancer,
myocardial infarction, and stroke, though a causal
mechanism cannot be inferred from these data. Thus, more
longitudinal data on patients that have undergone FMT are
needed and at present, judicious use of this treatment
modality is warranted.
Avoid Anti-Motility Agents
Anti-motility agents in the initial treatment or treatment
adjunct of CDI are not recommended as they can mask
symptoms and increase risk of toxic megacolon.46 In a
literature review of 55 patients, 31% of patients who
received anti-motility agents without initial treatment of C.
difficile developed toxic megacolon or colonic dilatation.155
No significant difference in complications was noted in
patients who received anti-motility agents along with
treatment of C. difficile.155 Further study is needed to assess
role of anti-motility agents to control diarrhea in patients
with mild-to moderate CDI who are already being treated
for CDI.
Treatment Response
Treatment response generally occurs after 3–5 days of
therapy and is characterized by a decrease in stool
frequency, improvement in stool consistency, and
improvement in laboratory, radiologic and physiologic
parameters.
For patients with mild to moderate CDI with no
improvement or worsening of symptoms after 3–5 days of
metronidazole therapy, escalation to vancomycin therapy is
indicated.
Recurrence of CDI after the initial episode occurs in is
approximately 19–25% of patients.8,132 Approximately 25-
64.7% of patients have another recurrence of CDI after first
or multiple recurrences.8,132
Surgical Treatment
In patients who have severe, complicated (fulminant) CDI
and clinical deterioration despite maximal medical therapy,
surgery may confer mortality benefit However, in advanced
fulminant CDI, surgical mortality can be up to 80% (range
19–80%).5,156
The optimal timing for surgical intervention is not well
defined, with only expert opinion supporting
recommendations. Early surgical involvement may be
warranted in patients who are critically ill from CDI.6
While not every patient requires surgical intervention,
patients with complicated CDI (Table 4) warrant early
surgical consultation.2,45 Indications for surgical
consultation and potential considerations for surgery6 are
listed in Table 4.
Delayed surgical intervention may result in increased
morbidity and mortality.2,3 Prior studies indicate higher
mortality rates if surgical intervention occurred after
evidence of end-organ failure (e.g. intubation for
respiratory failure, vasopressor therapy for hemodynamic
instability, or acute renal failure). In one study evaluating
timing of surgical intervention for fulminant pseudo-

19 Michigan Medicine C. difficile Guideline December 2016
membranous colitis, patients who survived received
surgical consult at a mean of 3.2 days from admission (or
onset of symptoms for those already in the hospital), as
compared to the nonsurvivors who received surgical consult
at a mean of 5.4 days after admission or symptom onset.157
Likewise, an analysis of the National Inpatient Sample
(NIS) database suggested that surgical intervention more
than 3 days after admission for CDI may be associated with
increased mortality.5
Surgical options include total or subtotal colectomy with
end ileostomy (total abdominal colectomy, or TAC).158
Partial colectomy is contraindicated: in one
retrospective analysis, partial colectomy carried a
mortality rate of 100% when compared to TAC.159
In patients with peritonitis, prior abdominal surgeries
with adhesions, or frank perforation, exploratory
laparotomy with TAC may be warranted.
Diverting loop ileostomy with antegrade colonic lavage
may be associated with reduced mortality when
compared to a historical population of patients
undergoing total abdominal colectomy,2 and the
majority of patients undergoing the former intervention
(93%) achieved colonic preservation. This may also
allow for earlier surgical intervention on CDI patients,
before the development of end-organ failure and shock
progression. However, more research is needed before
this can be universally adopted as standard of care.
In patients who are poor surgical candidates, or who are in
refractory end-stage septic shock, with continued clinical
decline, the risk for morbidity and mortality may be
prohibitively high, and a frank discussion with the patient
and/or the patient’s family may be warranted regarding
goals of care, including the risks and benefits involved with
an aggressive attempt at surgery vs. continued nonoperative
management with maximal medical therapy.
Special Populations - Pediatric Treatment
For pediatric patients, treatment guidelines generally follow
those outlined above for adults (see Figure 3). Ideally,
discontinuation of antimicrobial agents is the first step in
treating CDI and may suffice to resolve symptoms in mild
cases. Antiperistaltic medications are not recommended for
pediatric patients as these may mask symptoms and
precipitate complications, including toxic megacolon.
1. For pediatric patients with mild to moderate disease
(see Table 3) who lack significant pediatric risk factors
associated with severe disease (see Table 3),
metronidazole (7.5 mg/kg/dose QID, orally, maximum
500 mg/dose x 10 days) is the preferred therapy for
initial treatment of first episode of CDI.
2. For pediatric patients with criteria meeting severe
disease (Table 3), including those with risk factors
associated with severe disease (see Table 3),
metronidazole allergy, pregnancy/ breastfeeding, or
without symptom resolution after 3 to 5 days of oral
metronidazole, oral vancomycin is the preferred
therapy (10 mg/kg/dose QID, up to maximum 125
mg/dose x 10 days).
3. Combination therapy with vancomycin, both oral and
by retention enema, and intravenous metronidazole, or
second-line agents, may be considered in complicated
high-risk cases with sepsis, shock, ileus, small bowel
obstruction, peritonitis, or toxic megacolon (see Triple
Therapy in Figure 3). Do not use enema if concern of
colonic perforation. Intracolonic vancomycin
administered by retention enema (10-20 mL/kg/dose,
up to 1000 ml max, of a 500 mg/L solution in normal
saline q6h instilled by appropriately-sized Foley
catheter inserted into rectum with balloon inflated and
Foley clamped for 1 hour; treatment naïve patients
should be initiated at 10 mL/kg/dose and escalated as
tolerated to a maximum of 20 mL/kg/dose or 1000
mL), and high-dose oral vancomycin (minimum
10mg/kg/dose up to 500 mg/dose QID) in combination
with IV metronidazole should be administered. For
patients receiving combination therapy including PO,
IV, and PR vancomycin or in patient at high risk for
systemic absorption, serum vancomycin concentrations
should be considered to evaluate for elevated serum
concentrations.
4. For pediatric patients with first recurrence of CDI, that
is mild to moderate, oral metronidazole is the preferred
therapy.
5. For pediatric patients with prolonged or recurrent CDI,
metronidazole should not be used for chronic therapy
due to possible neurotoxicity. Oral vancomycin is
recommended for second or multiple recurrences (10
mg/kg/dose QID, maximum 500 mg/dose, x 10 days),
and pulsed or tapered regimens may be beneficial in
difficult cases (see adult section above).
6. Criteria for optimal use of second-line agents in
recurrent CDI, including nitazoxanide, fidaxomicin,
and rifaximin, do not exist in children, and consultation
with a Pediatric Infectious Diseases specialist is
recommended if considering these options. Pediatric
dosing for fidaxomicin is 16 mg/kg/dose BID, max 200
mg per dose; Peds ID approval is required for use of
fidaxomicin.
7. Fecal microbiota transplantation (FMT) may be
considered in children <18 years old as an outpatient to
help prevent recurrence of CDI; consultation with a
Pediatric Infectious Disease specialist is recommended.
There are currently no mechanisms in place to provide
FMT to children <18 years old as an inpatient.
8. Probiotics are not routinely recommended for either
prevention or treatment of CDI in infants and children,
due to a lack of sufficient evidence in infants and
children and a theoretical risk of bacteremia due to gut
translocation.
Summary of Evidence. It should be recognized that oral
vancomycin is the only FDA-approved medication for the
treatment of CDI in children; however, metronidazole is
currently the accepted first-line medication in otherwise
healthy infants and children with mild to moderate
disease.24,27 Prospective trials evaluating the use of
metronidazole or vancomycin for longer than 10 to 14 days
in children are lacking.26 Data does not support a clear
benefit for combination therapy vs. oral vancomycin

20 Michigan Medicine C. difficile Guideline December 2016
monotherapy for treatment of severe CDI.160 Experience
with FMT in pediatrics is limited, but growing evidence
suggests that FMT is effective and safe for treatment of
chronic CDI in children.161 An FMT program for inpatients
<18 years old is currently unavailable at UMHS;
consultation with Pediatric Infectious Diseases is suggested
if considering FMT as an option as an outpatient procedure
to prevent future recurrences. The American Academy of
Pediatrics (AAP) does not currently recommend probiotics
for prevention or treatment of CDI in infants and children
citing insufficient data.25 However, a recent Cochrane
Database review of 23 randomized controlled trials found
moderate quality evidence to suggest that short-term use of
probiotics in healthy, immunocompetent adults and children
was safe and effective in the prevention of CDI.162 UMHS
guidelines reflect the recommendation of the AAP and do
not recommend probiotic use for prevention or treatment of
CDI in this patient population.
Special Populations - Inflammatory Bowel Disease
In IBD patients with concomitant CDI and mild IBD flare,
antibiotics for CDI should be started without corticosteroids
(patient should be maintained on home immunosuppression
medications). This recommendation is based on evidence
suggesting worse outcomes in IBD patients with CDI on
immunosuppression,141,142 and a reduction of corticosteroids
dose is associated with a lower colectomy rate.14 However,
with a lack of symptom improvement after 48 hours of CDI
therapy or in severe IBD flare with concomitant CDI,
antibiotics and corticosteroids co-therapy is advised. This
strategy is based on clinical data indicating a more severe
IBD course (i.e., an increased colectomy rate and mortality)
in IBD patients with CDI vs IBD patients without
CDI.50,143,144 The recommended practice of IBD experts at
UMHS is to use CDI therapy and corticosteroids when IBD
patients with concomitant CDI present with a severe IBD
flare defined as >6 bloody stools/day and one or more of:
Temp>37.5, Pulse >90, Hgb<10.5, ESR>30.
Vancomycin is preferred over metronidazole for the
treatment of CDI in IBD patients based on a retrospective
study showing fewer readmissions and shorter lengths of
stay when IBD patients are treated with vancomycin-
containing regimen relative to those treated with
metronidazole alone.163
Related National/International Guidelines
The UMHS Clinical Guideline on CDI is generally
consistent with other guidelines published nationally and
internationally, including:
1. Clinical Practice Guidelines for Clostridium difficile
Infection in Adults: 2010 Update by the Society for
Healthcare Epidemiology of America (SHEA) and the
Infectious Diseases Society of America (IDSA). Infect
Control Hosp Epidemiol 2010; 31(5):431-455.
2. Guidelines for Diagnosis, Treatment, and Prevention of
Clostridium difficile Infections. Am J Gastroenterol
2013; 108:478–498.
3. European Society of Clinical Microbiology and
Infectious Diseases: update of the treatment guidance
document for Clostridium difficile infection. Clin
Microbiol Infect 2014; 20 (Suppl. 2): 1–26
Notable differences in recommendations: Our guideline
deviates from the above guidelines in the way that it
classifies "mild-to-moderate" vs. "severe" vs. "severe and
complicated" disease (see Table 3). The change in
classification criteria was undertaken to better reflect
additional factors we identified in the literature that can
predispose patients to developing complicated C. difficile or
more severe manifestations of C. difficile.
Guideline Development Methodology
Funding
The development of this guideline was funded by the
University of Michigan Health System.
Guideline Development Team and Disclosures
The multidisciplinary guideline development team
consisted of:
Primary care physicians: Andrea H Kim, MD, Internal
Medicine
Specialists: Meghan A Arnold, MD, Pediatric Surgery,
Gregory Eschenauer, PharmD, Pharmacy, Tejal N
Gandhi, MD, Infectious Diseases, John Y Kao, MD,
Gastroenterology, Lena M Napolitano, MD Surgery,
Krishna Rao, MD, Infectious Diseases, David M.
Somand, MD, Emergency Medicine, Daniel H
Teitelbaum, MD, Pediatric Surgery, Kathleen B To,
MD, Surgery, Alison C Tribble, MD, Pediatric
Infectious Diseases, Amanda M Valyko, MPH, CIC,
Infection Control, Laraine L Washer, MD Infection
Diseases, Michael E Watson, Jr., MD, PhD, Pediatric
Infectious Diseases
A guideline development methodologist: F. Jacob
Seagull, PhD, Learning Health Sciences.
Literature search services were provided by
informationists at the Taubman Health Sciences Library,
University of Michigan Medical School.
The University of Michigan Health System endorses the
Guidelines of the Association of American Medical
Colleges and the Standards of the Accreditation Council for
Continuing Medical Education that the individuals who
present educational activities disclose significant
relationships with commercial companies whose products
or services are discussed. Disclosure of a relationship is not
intended to suggest bias in the information presented, but is
made to provide readers with information that might be of
potential importance to their evaluation of the information.
No relevant personal financial relationships with
commercial entities: Meghan A Arnold, Gregory
Eschenauer, PharmD, Tejal N Gandhi MD, John Y Kao,

21 Michigan Medicine C. difficile Guideline December 2016
MD, Andrea H Kim, MD, Lena M Napolitano, MD,
Krishna Rao, MD, F Jacob Seagull, PhD, David M Somand,
MD, Daniel H Teitelbaum, MD, Kathleen B To, MD,
Alison C Tribble, MD, Amanda M Valyko, Laraine Lynn
Washer, MD, Michael E Watson Jr, MD, PhD.
Strategy for Literature Search
Within the Medline (Ovid) database, the following search
strategy was used for most of the search topics, except for
the searches on suppurative thrombosis, endocarditis, and
vascular infection. The search below is identified as Main
in the search strategies document. Because the appropriate
indexing terms either do not exist or were applied
inconsistently, the main search uses keywords in addition to
MeSH terms to arrive at the following main strategy.
1. exp *Clostridium difficile/ or exp *enterocolitis/ or exp
*Clostridium Infections/
2. exp *Hirschsprung Disease/
3. limit 2 to "all child (0 to 18 years)"
4. 1 or 3
5. exp animals/ not (exp animals/ and humans/)
6. 4 not 5
7. limit 6 to (english language and yr="2013 -Current")
8. remove duplicates from 7. The searches on suppurative
thrombosis, endocarditis, and vascular infection used the
first 3 searches of the main search strategy. The MEDLINE
In-Process search was based entirely on keywords.
Results were limited to: English, and 2013 to present. The
Main search retrieved 893 references. When the search
hedges for Guidelines, Clinical Trials, and Cohort Studies
were added, the base results are as follow:
C-Diff -Guidelines, total results were 8
C-Diff -Clinical Trials, total results were 27
C-Diff -Cohort Studies, total results were 59
The search was conducted in components each keyed to a
specific causal link in a formal problem structure (available
upon request). The search was supplemented with very
recent clinical trials known to expert members of the panel.
Negative trials were specifically sought. The search was a
single cycle.
Level of evidence supporting a diagnostic method or an
intervention:
A = systematic reviews of randomized controlled trials with
or without meta-analysis,
B = randomized controlled trials,
C = systematic review of non-randomized controlled trials
or observational studies, non-randomized controlled
trials, group observation studies (cohort, cross-
sectional, case-control),
D = individual observation studies (case study/case series),
E = expert opinion regarding benefits and harm
Search details and evidence tables available at
http://www.uofmhealth.org/provider/clinical-care-
guidelines.
Recommendations
Guideline recommendations were based on prospective
randomized controlled trials if available, to the exclusion of
other data; if RCTs were not available, observational
studies were admitted to consideration. If no such data were
available for a given link in the problem formulation, expert
opinion was used to estimate effect size. The “strength of
recommendation” for key aspects of care was determined
by expert opinion.
The strength of recommendations regarding care were
categorized as:
I = Generally should be performed
II = May be reasonable to perform
III = Generally should not be performed
Review and Endorsement
Drafts of this guideline were reviewed in clinical
conferences and by distribution for comment within
departments and divisions of the University of Michigan
Medical School to which the content is most relevant:
Family Medicine, General Medicine, Department of
Surgery, Infectious Diseases Division, Gastroenterology
Division. Pediatrics and Communicable Diseases and the
Division of Pediatric Infectious Diseases. The Executive
Committee for Clinical Affairs of the University of
Michigan Hospitals and Health Centers endorsed the final
version.
References
1. McDonald LC, Coignard B, Dubberke E, et al.
Recommendations for surveillance of clostridium difficile-
associated disease. Infect Control Hosp Epidemiol.
2007;28(2):140-145.
2. Neal MD, Alverdy JC, Hall DE, Simmons RL,
Zuckerbraun BS. Diverting loop ileostomy and colonic
lavage: An alternative to total abdominal colectomy for the
treatment of severe, complicated clostridium difficile
associated disease. Ann Surg. 2011;254(3):423-7;
discussion 427-9.
3. Halabi WJ, Nguyen VQ, Carmichael JC, Pigazzi A,
Stamos MJ, Mills S. Clostridium difficile colitis in the
united states: A decade of trends, outcomes, risk factors for
colectomy, and mortality after colectomy. J Am Coll Surg.
2013;217(5):802-812.
4. Surawicz CM, Brandt LJ, Binion DG, et al. Guidelines
for diagnosis, treatment, and prevention of clostridium
difficile infections. Am J Gastroenterol. 2013;108(4):478-
98; quiz 499.

22 Michigan Medicine C. difficile Guideline December 2016
5. Ferrada P, Velopulos CG, Sultan S, et al. Timing and
type of surgical treatment of clostridium difficile-associated
disease: A practice management guideline from the eastern
association for the surgery of trauma. The Journal of
Trauma and Acute Care Surgery. 2014;76(6):1484-1493.
6. To KB, Napolitano LM. Clostridium difficile infection:
Update on diagnosis, epidemiology, and treatment
strategies. Surg Infect (Larchmt). 2014;15(5):490-502.
7. Kuijper EJ, Coignard B, Tull P, ESCMID Study Group
for Clostridium difficile, EU Member States, European
Centre for Disease Prevention and Control. Emergence of
clostridium difficile-associated disease in north america and
europe. Clin Microbiol Infect. 2006;12 Suppl 6:2-18.
8. Abou Chakra CN, Pepin J, Sirard S, Valiquette L. Risk
factors for recurrence, complications and mortality in
clostridium difficile infection: A systematic review. PLoS
One. 2014;9(6):e98400.
9. Bartlett JG, Moon N, Chang TW, Taylor N, Onderdonk
AB. Role of clostridium difficile in antibiotic-associated
pseudomembranous colitis. Gastroenterology.
1978;75(5):778-782.
10. Bartlett JG, Chang TW, Gurwith M, Gorbach SL,
Onderdonk AB. Antibiotic-associated pseudomembranous
colitis due to toxin-producing clostridia. N Engl J Med.
1978;298(10):531-534.
11. Campbell RJ, Giljahn L, Machesky K, et al. Clostridium
difficile infection in ohio hospitals and nursing homes
during 2006. Infect Control Hosp Epidemiol.
2009;30(6):526-533.
12. Tabak YP, Zilberberg MD, Johannes RS, Sun X,
McDonald LC. Attributable burden of hospital-onset
clostridium difficile infection: A propensity score matching
study. Infect Control Hosp Epidemiol. 2013;34(6):588-596.
13. Lessa FC, Mu Y, Bamberg WM, et al. Burden of
clostridium difficile infection in the united states. N. Engl.
J. Med. Feb 26 2015;372(9):825-834.
14. He M, Miyajima F, Roberts P, et al. Emergence and
global spread of epidemic healthcare-associated clostridium
difficile. Nat Genet. 2013;45(1):109-113.
15. Louie TJ, Miller MA, Crook DW, et al. Effect of age on
treatment outcomes in clostridium difficile infection. J Am
Geriatr Soc. 2013;61(2):222-230.
16. Lessa FC, Gould CV, McDonald LC. Current status of
clostridium difficile infection epidemiology. Clin Infect
Dis. 2012;55 Suppl 2:S65-70.
17. Keller JM, Surawicz CM. Clostridium difficile infection
in the elderly. Clin Geriatr Med. 2014;30(1):79-93.
18. Zimlichman E, Henderson D, Tamir O, et al. Health
care-associated infections: A meta-analysis of costs and
financial impact on the US health care system. JAMA Intern
Med. 2013;173(22):2039-2046.
19. Pepin J, Valiquette L, Alary ME, et al. Clostridium
difficile-associated diarrhea in a region of quebec from
1991 to 2003: A changing pattern of disease severity.
CMAJ. 2004;171(5):466-472.
20. Bliss DZ, Johnson S, Savik K, Clabots CR, Willard K,
Gerding DN. Acquisition of clostridium difficile and
clostridium difficile-associated diarrhea in hospitalized
patients receiving tube feeding. Ann Intern Med.
1998;129(12):1012-1019.
21. Issa M, Vijayapal A, Graham MB, et al. Impact of
clostridium difficile on inflammatory bowel disease. Clin
Gastroenterol Hepatol. 2007;5(3):345-351.
22. Sanchez TH, Brooks JT, Sullivan PS, et al. Bacterial
diarrhea in persons with HIV infection, united states, 1992-
2002. Clin Infect Dis. 2005;41(11):1621-1627.
23. Haines CF, Moore RD, Bartlett JG, et al. Clostridium
difficile in a HIV-infected cohort: Incidence, risk factors,
and clinical outcomes. AIDS. 2013;27(17):2799-2807.
24. Sammons JS, Toltzis P, Zaoutis TE. Clostridium
difficile infection in children. JAMA Pediatr.
2013;167(6):567-573.
25. Schutze GE, Willoughby RE, Committee on Infectious
Diseases, American Academy of Pediatrics. Clostridium
difficile infection in infants and children. Pediatrics.
2013;131(1):196-200.
26. Kim J, Smathers SA, Prasad P, Leckerman KH, Coffin
S, Zaoutis T. Epidemiological features of clostridium
difficile-associated disease among inpatients at children's
hospitals in the united states, 2001-2006. Pediatrics.
2008;122(6):1266-1270.
27. McFarland LV, Ozen M, Dinleyici EC, Goh S.
Comparison of pediatric and adult antibiotic-associated
diarrhea and clostridium difficile infections. World J
Gastroenterol. 2016;22(11):3078-3104.
28. Khanna S, Baddour LM, Huskins WC, et al. The
epidemiology of clostridium difficile infection in children:
A population-based study. Clinical Infectious Diseases.
2013;56(10):1401-1406.
29. Fekety R, Silva J, Kauffman C, Buggy B, Deery HG.
Treatment of antibiotic-associated clostridium difficile

23 Michigan Medicine C. difficile Guideline December 2016
colitis with oral vancomycin: Comparison of two dosage
regimens. Am J Med. 1989;86(1):15-19.
30. Bagdasarian N, Rao K, Malani PN. Diagnosis and
treatment of clostridium difficile in adults: A systematic
review. JAMA. 2015;313(4):398-408.
31. Debast SB, Bauer MP, Kuijper EJ, Committee.
European society of clinical microbiology and infectious
diseases: Update of the treatment guidance document for
clostridium difficile infection. Clinical Microbiology &
Infection. 2014;20(Suppl 2):1-26.
32. Bignardi GE, Hill K, Berrington A, Settle CD. Two-
stage algorithm for clostridium difficile: Glutamate-
dehydrogenase-positive toxin-negative enzyme
immunoassay results may require further testing. J Hosp
Infect. 2013;83(4):347-349.
33. Finch LS, Duncan CM. Molecular test to determine
toxigenic capabilities in GDH-positive, toxin-negative
samples: Evaluation of the portrait toxigenic C. difficile
assay. Br J Biomed Sci. 2013;70(2):62-66.
34. Walkty A, Lagace-Wiens PR, Manickam K, et al.
Evaluation of an algorithmic approach in comparison with
the illumigene assay for laboratory diagnosis of clostridium
difficile infection. J Clin Microbiol. 2013;51(4):1152-1157.
35. Brown NA, Lebar WD, Young CL, Hankerd RE,
Newton DW. Diagnosis of clostridium difficile infection:
Comparison of four methods on specimens collected in
cary-blair transport medium and tcdB PCR on fresh versus
frozen samples. Infect Dis Rep. 2011;3(1):e5.
36. Sunkesula VC, Kundrapu S, Muganda C, Sethi AK,
Donskey CJ. Does empirical clostridium difficile infection
(CDI) therapy result in false-negative CDI diagnostic test
results?. Clinical Infectious Diseases. 2013;57(4):494-500.
37. Debast SB, Bauer MP, Kuijper EJ, European Society of
Clinical Microbiology and Infectious Diseases. European
society of clinical microbiology and infectious diseases:
Update of the treatment guidance document for clostridium
difficile infection. Clin Microbiol Infect. 2014;20 Suppl
2:1-26.
38. Fujitani S, George WL, Murthy AR. Comparison of
clinical severity score indices for clostridium difficile
infection. Infect Control Hosp Epidemiol. 2011;32(3):220-
228.
39. Kirkpatrick ID, Greenberg HM. Evaluating the CT
diagnosis of clostridium difficile colitis: Should CT guide
therapy? AJR Am J Roentgenol. 2001;176(3):635-639.
40. Macari M, Balthazar EJ, Megibow AJ. The accordion
sign at CT: A nonspecific finding in patients with colonic
edema. Radiology. 1999;211(3):743-746.
41. Ash L, Baker ME, O'Malley CM,Jr, Gordon SM,
Delaney CP, Obuchowski NA. Colonic abnormalities on
CT in adult hospitalized patients with clostridium difficile
colitis: Prevalence and significance of findings. AJR Am J
Roentgenol. 2006;186(5):1393-1400.
42. Gerding DN, Olson MM, Peterson LR, et al.
Clostridium difficile-associated diarrhea and colitis in
adults. A prospective case-controlled epidemiologic study.
Arch Intern Med. 1986;146(1):95-100.
43. Tedesco FJ. Antibiotic associated pseudomembranous
colitis with negative proctosigmoidoscopy examination.
Gastroenterology. 1979;77(2):295-297.
44. Gibson PR, Shepherd SJ. Evidence-based dietary
management of functional gastrointestinal symptoms: The
FODMAP approach. J Gastroenterol Hepatol.
2010;25(2):252-258.
45. Fujitani S, George WL, Murthy AR. Comparison of
clinical severity score indices for clostridium difficile
infection. Infect Control Hosp Epidemiol. 2011;32(3):220-
228.
46. Cohen SH, Gerding DN, Johnson S, et al. Clinical
practice guidelines for clostridium difficile infection in
adults: 2010 update by the society for healthcare
epidemiology of america (SHEA) and the infectious
diseases society of america (IDSA). Infect Control Hosp
Epidemiol. 2010;31(5):431-455.
47. Kim JH, Muder RR. Clostridium difficile enteritis: A
review and pooled analysis of the cases. Anaerobe.
2011;17(2):52-55.
48. Rodemann JF, Dubberke ER, Reske KA, Seo da H,
Stone CD. Incidence of clostridium difficile infection in
inflammatory bowel disease. Clin Gastroenterol Hepatol.
2007;5(3):339-344.
49. Issa M, Ananthakrishnan AN, Binion DG. Clostridium
difficile and inflammatory bowel disease. Inflamm Bowel
Dis. 2008;14(10):1432-1442.
50. Ananthakrishnan AN, McGinley EL, Saeian K, Binion
DG. Temporal trends in disease outcomes related to
clostridium difficile infection in patients with inflammatory
bowel disease. Inflamm Bowel Dis. 2011;17(4):976-983.
51. Kelsen JR, Kim J, Latta D, et al. Recurrence rate of
clostridium difficile infection in hospitalized pediatric
patients with inflammatory bowel disease. Inflamm Bowel
Dis. 2011;17(1):50-55.

24 Michigan Medicine C. difficile Guideline December 2016
52. Kostic AD, Xavier RJ, Gevers D. The microbiome in
inflammatory bowel disease: Current status and the future
ahead. Gastroenterology. 2014;146(6):1489-1499.
53. Li Y, Qian J, Queener E, Shen B. Risk factors and
outcome of PCR-detected clostridium difficile infection in
ileal pouch patients. Inflamm Bowel Dis. 2013;19(2):397-
403.
54. Shen B, Goldblum JR, Hull TL, Remzi FH, Bennett AE,
Fazio VW. Clostridium difficile-associated pouchitis. Dig
Dis Sci. 2006;51(12):2361-2364.
55. Causey MW, Spencer MP, Steele SR. Clostridium
difficile enteritis after colectomy. Am Surg.
2009;75(12):1203-1206.
56. Lundeen SJ, Otterson MF, Binion DG, Carman ET,
Peppard WJ. Clostridium difficile enteritis: An early
postoperative complication in inflammatory bowel disease
patients after colectomy. J Gastrointest Surg.
2007;11(2):138-142.
57. Ananthakrishnan AN, Issa M, Binion DG. Clostridium
difficile and inflammatory bowel disease. Gastroenterol
Clin North Am. 2009;38(4):711-728.
58. Jen MH, Saxena S, Bottle A, Aylin P, Pollok RC.
Increased health burden associated with clostridium
difficile diarrhoea in patients with inflammatory bowel
disease. Aliment Pharmacol Ther. 2011;33(12):1322-1331.
59. Jodorkovsky D, Young Y, Abreu MT. Clinical
outcomes of patients with ulcerative colitis and co-existing
clostridium difficile infection. Dig Dis Sci. 2010;55(2):415-
420.
60. Schneeweiss S, Korzenik J, Solomon DH, Canning C,
Lee J, Bressler B. Infliximab and other immunomodulating
drugs in patients with inflammatory bowel disease and the
risk of serious bacterial infections. Aliment Pharmacol
Ther. 2009;30(3):253-264.
61. Sammons JS, Localio R, Xiao R, Coffin SE, Zaoutis T.
Clostridium difficile infection is associated with increased
risk of death and prolonged hospitalization in children.
Clinical Infectious Diseases. 2013;57(1):1-8.
62. Jangi S, Lamont JT. Asymptomatic colonization by
clostridium difficile in infants: Implications for disease in
later life. J Pediatr Gastroenterol Nutr. 2010;51(1):2-7.
63. Leibowitz J, Soma VL, Rosen L, Ginocchio CC, Rubin
LG. Similar proportions of stool specimens from
hospitalized children with and without diarrhea test positive
for clostridium difficile. Pediatr Infect Dis J.
2015;34(3):261-266.
64. Nylund CM, Goudie A, Garza JM, Fairbrother G,
Cohen MB. Clostridium difficile infection in hospitalized
children in the united states. Arch Pediatr Adolesc Med.
2011;165(5):451-457.
65. Zilberberg MD, Tillotson GS, McDonald C.
Clostridium difficile infections among hospitalized
children, united states, 1997-2006. Emerg Infect Dis.
2010;16(4):604-609.
66. Wendt JM, Cohen JA, Mu Y, et al. Clostridium difficile
infection among children across diverse US geographic
locations. Pediatrics. 2014;133(4):651-658.
67. Owens RC,Jr, Donskey CJ, Gaynes RP, Loo VG, Muto
CA. Antimicrobial-associated risk factors for clostridium
difficile infection. Clin Infect Dis. 2008;46 Suppl 1:S19-31.
68. Slimings C, Riley TV. Antibiotics and hospital-acquired
clostridium difficile infection: Update of systematic review
and meta-analysis. J Antimicrob Chemother.
2014;69(4):881-891.
69. Goorhuis A, Debast SB, Dutilh JC, et al. Type-specific
risk factors and outcome in an outbreak with 2 different
clostridium difficile types simultaneously in 1 hospital. Clin
Infect Dis. 2011;53(9):860-869.
70. Hensgens MP, Goorhuis A, Dekkers OM, Kuijper EJ.
Time interval of increased risk for clostridium difficile
infection after exposure to antibiotics. J Antimicrob
Chemother. 2012;67(3):742-748.
71. Stevens V, Dumyati G, Fine LS, Fisher SG, van
Wijngaarden E. Cumulative antibiotic exposures over time
and the risk of clostridium difficile infection. Clin Infect
Dis. 2011;53(1):42-48.
72. Pop-Vicas A, Shaban E, Letourneau C, Pechie A.
Empirical antimicrobial prescriptions in patients with
clostridium difficile infection at hospital admission and
impact on clinical outcome. Infect Control Hosp Epidemiol.
2012;33(11):1101-1106.
73. Modena S, Gollamudi S, Friedenberg F. Continuation of
antibiotics is associated with failure of metronidazole for
clostridium difficile-associated diarrhea. J Clin
Gastroenterol. 2006;40(1):49-54.
74. Drekonja DM, Amundson WH, Decarolis DD,
Kuskowski MA, Lederle FA, Johnson JR. Antimicrobial
use and risk for recurrent clostridium difficile infection. Am
J Med. 2011;124(11):1081.e1-1081.e7.
75. Ehrhardt S, Guo N, Hinz R, et al. Saccharomyces
boulardii to prevent antibiotic-associated diarrhea: A
randomized, double-masked, placebo-controlled trial. Open
Forum Infect Dis. 2016;3(1):ofw011.

25 Michigan Medicine C. difficile Guideline December 2016
76. Lau CS, Chamberlain RS. Probiotics are effective at
preventing clostridium difficile-associated diarrhea: A
systematic review and meta-analysis. Int J Gen Med.
2016;9:27-37.
77. Luong ML, Sareyyupoglu B, Nguyen MH, et al.
Lactobacillus probiotic use in cardiothoracic transplant
recipients: A link to invasive lactobacillus infection?
Transpl Infect Dis. 2010;12(6):561-564.
78. Besselink MG, van Santvoort HC, Buskens E, et al.
Probiotic prophylaxis in predicted severe acute pancreatitis:
A randomised, double-blind, placebo-controlled trial.
Lancet. 2008;371(9613):651-659.
79. Snydman DR. The safety of probiotics. Clin Infect Dis.
2008;46 Suppl 2:S104-11; discussion S144-51.
80. Deshpande A, Pant C, Pasupuleti V, et al. Association
between proton pump inhibitor therapy and clostridium
difficile infection in a meta-analysis. Clin Gastroenterol
Hepatol. 2012;10(3):225-233.
81. Howell MD, Novack V, Grgurich P, et al. Iatrogenic
gastric acid suppression and the risk of nosocomial
clostridium difficile infection. Arch Intern Med.
2010;170(9):784-790.
82. Mayfield JL, Leet T, Miller J, Mundy LM.
Environmental control to reduce transmission of
clostridium difficile. Clin Infect Dis. 2000;31(4):995-1000.
83. Hacek DM, Ogle AM, Fisher A, Robicsek A, Peterson
LR. Significant impact of terminal room cleaning with
bleach on reducing nosocomial clostridium difficile. Am J
Infect Control. 2010;38(5):350-353.
84. Wilcox MH, Fawley WN, Wigglesworth N, Parnell P,
Verity P, Freeman J. Comparison of the effect of detergent
versus hypochlorite cleaning on environmental
contamination and incidence of clostridium difficile
infection. J Hosp Infect. 2003;54(2):109-114.
85. Weber DJ, Anderson DJ, Sexton DJ, Rutala WA. Role
of the environment in the transmission of clostridium
difficile in health care facilities. Am J Infect Control.
2013;41(5 Suppl):S105-10.
86. Pepin J, Saheb N, Coulombe MA, et al. Emergence of
fluoroquinolones as the predominant risk factor for
clostridium difficile-associated diarrhea: A cohort study
during an epidemic in quebec. Clin Infect Dis.
2005;41(9):1254-1260.
87. Johnson S, Homann SR, Bettin KM, et al. Treatment of
asymptomatic clostridium difficile carriers (fecal excretors)
with vancomycin or metronidazole. A randomized, placebo-
controlled trial. Ann Intern Med. 1992;117(4):297-302.
88. Curry SR, Muto CA, Schlackman JL, et al. Use of
multilocus variable number of tandem repeats analysis
genotyping to determine the role of asymptomatic carriers
in clostridium difficile transmission. Clin Infect Dis.
2013;57(8):1094-1102.
89. Johnson S, Louie TJ, Gerding DN, et al. Vancomycin,
metronidazole, or tolevamer for clostridium difficile
infection: Results from two multinational, randomized,
controlled trials. Clin Infect Dis. 2014;59(3):345-354.
90. Zar FA, Bakkanagari SR, Moorthi KM, Davis MB. A
comparison of vancomycin and metronidazole for the
treatment of clostridium difficile-associated diarrhea,
stratified by disease severity. Clin Infect Dis.
2007;45(3):302-307.
91. Bolton RP, Culshaw MA. Faecal metronidazole
concentrations during oral and intravenous therapy for
antibiotic associated colitis due to clostridium difficile. Gut.
1986;27(10):1169-1172.
92. Olson MM, Shanholtzer CJ, Lee JT,Jr, Gerding DN.
Ten years of prospective clostridium difficile-associated
disease surveillance and treatment at the minneapolis VA
medical center, 1982-1991. Infect Control Hosp Epidemiol.
1994;15(6):371-381.
93. Apisarnthanarak A, Razavi B, Mundy LM. Adjunctive
intracolonic vancomycin for severe clostridium difficile
colitis: Case series and review of the literature. Clin Infect
Dis. 2002;35(6):690-696.
94. Seril DN, Shen B. Clostridium difficile infection in
patients with ileal pouches. Am J Gastroenterol.
2014;109(7):941-947.
95. McFarland LV, Elmer GW, Surawicz CM. Breaking the
cycle: Treatment strategies for 163 cases of recurrent
clostridium difficile disease. Am J Gastroenterol.
2002;97(7):1769-1775.
96. Crook DW, Walker AS, Kean Y, et al. Fidaxomicin
versus vancomycin for clostridium difficile infection: Meta-
analysis of pivotal randomized controlled trials. Clin Infect
Dis. 2012;55 Suppl 2:S93-103.
97. Bartsch SM, Umscheid CA, Fishman N, Lee BY. Is
fidaxomicin worth the cost? an economic analysis. Clin
Infect Dis. 2013;57(4):555-561.
98. Nathwani D, Cornely OA, Van Engen AK, Odufowora-
Sita O, Retsa P, Odeyemi IA. Cost-effectiveness analysis of
fidaxomicin versus vancomycin in clostridium difficile
infection. J Antimicrob Chemother. 2014;69(11):2901-
2912.

26 Michigan Medicine C. difficile Guideline December 2016
99. Johnson S, Gerding DN. Fidaxomicin "chaser" regimen
following vancomycin for patients with multiple
clostridium difficile recurrences. Clin Infect Dis.
2013;56(2):309-310.
100. Johnson S, Schriever C, Galang M, Kelly CP, Gerding
DN. Interruption of recurrent clostridium difficile-
associated diarrhea episodes by serial therapy with
vancomycin and rifaximin. Clin Infect Dis. 2007;44(6):846-
848.
101. Herpers BL, Vlaminckx B, Burkhardt O, et al.
Intravenous tigecycline as adjunctive or alternative therapy
for severe refractory clostridium difficile infection. Clin
Infect Dis. 2009;48(12):1732-1735.
102. Musher DM, Logan N, Mehendiratta V, Melgarejo
NA, Garud S, Hamill RJ. Clostridium difficile colitis that
fails conventional metronidazole therapy: Response to
nitazoxanide. J Antimicrob Chemother. 2007;59(4):705-
710.
103. Rao K, Micic D, Natarajan M, et al. Clostridium
difficile ribotype 027: Relationship to age, detectability of
toxins A or B in stool with rapid testing, severe infection,
and mortality. Clin Infect Dis. 2015;61(2):233-241.
104. Mullane KM, Miller MA, Weiss K, et al. Efficacy of
fidaxomicin versus vancomycin as therapy for clostridium
difficile infection in individuals taking concomitant
antibiotics for other concurrent infections. Clin Infect Dis.
2011;53(5):440-447.
105. Stranges PM, Hutton DW, Collins CD. Cost-
effectiveness analysis evaluating fidaxomicin versus oral
vancomycin for the treatment of clostridium difficile
infection in the united states. Value Health.
2013;16(2):297-304.
106. McFarland LV, Surawicz CM, Greenberg RN, et al. A
randomized placebo-controlled trial of saccharomyces
boulardii in combination with standard antibiotics for
clostridium difficile disease. JAMA. 1994;271(24):1913-
1918.
107. Surawicz CM, McFarland LV, Greenberg RN, et al.
The search for a better treatment for recurrent clostridium
difficile disease: Use of high-dose vancomycin combined
with saccharomyces boulardii. Clin Infect Dis.
2000;31(4):1012-1017.
108. McFarland LV. Probiotics for the primary and
secondary prevention of C. difficile infections: A meta-
analysis and systematic review. Antibiotics (Basel).
2015;4(2):160-178.
109. Enache-Angoulvant A, Hennequin C. Invasive
saccharomyces infection: A comprehensive review. Clin
Infect Dis. 2005;41(11):1559-1568.
110. Bakken JS. Staggered and tapered antibiotic
withdrawal with administration of kefir for recurrent
clostridium difficile infection. Clin Infect Dis.
2014;59(6):858-861.
111. Juang P, Skledar SJ, Zgheib NK, et al. Clinical
outcomes of intravenous immune globulin in severe
clostridium difficile-associated diarrhea. Am J Infect
Control. 2007;35(2):131-137.
112. Lowy I, Molrine DC, Leav BA, et al. Treatment with
monoclonal antibodies against clostridium difficile toxins.
N Engl J Med. 2010;362(3):197-205.
113. Wilcox M, Gerding D, Poxton Iea. Bezlotoxumab
(BEZ) alone and with actoxumab (ACT) for prevention of
recurrent C. difficile infection (rCDI) in patients on
standard of care (SoC) antibiotics: Integrated results of 2
phase 3 studies (MODIFY I and MODIFY II). ID Week.
2015(October 7-11).
114. Mogg GA, George RH, Youngs D, et al. Randomized
controlled trial of colestipol in antibiotic-associated colitis.
Br J Surg. 1982;69(3):137-139.
115. Pantosti A, Luzzi I, Cardines R, Gianfrilli P.
Comparison of the in vitro activities of teicoplanin and
vancomycin against clostridium difficile and their
interactions with cholestyramine. Antimicrob Agents
Chemother. 1985;28(6):847-848.
116. Yatsunenko T, Rey FE, Manary MJ, et al. Human gut
microbiome viewed across age and geography. Nature.
2012;486(7402):222-227.
117. van der Waaij D, Berghuis-de Vries JM, Lekkerkerk
L. Colonization resistance of the digestive tract in
conventional and antibiotic-treated mice. J Hyg (Lond).
1971;69(3):405-411.
118. Vollaard EJ, Clasener HA. Colonization resistance.
Antimicrob Agents Chemother. 1994;38(3):409-414.
119. Britton RA, Young VB. Role of the intestinal
microbiota in resistance to colonization by clostridium
difficile. Gastroenterology. 2014;146(6):1547-1553.
120. Theriot CM, Koenigsknecht MJ, Carlson PE,Jr, et al.
Antibiotic-induced shifts in the mouse gut microbiome and
metabolome increase susceptibility to clostridium difficile
infection. Nat Commun. 2014;5:3114.
121. Figueroa I, Johnson S, Sambol SP, Goldstein EJ,
Citron DM, Gerding DN. Relapse versus reinfection:
Recurrent clostridium difficile infection following
treatment with fidaxomicin or vancomycin. Clin Infect Dis.
2012;55 Suppl 2:S104-9.

27 Michigan Medicine C. difficile Guideline December 2016
122. Eyre DW, Babakhani F, Griffiths D, et al. Whole-
genome sequencing demonstrates that fidaxomicin is
superior to vancomycin for preventing reinfection and
relapse of infection with clostridium difficile. J Infect Dis.
2014;209(9):1446-1451.
123. Borody TJ, Warren EF, Leis SM, Surace R, Ashman
O, Siarakas S. Bacteriotherapy using fecal flora: Toying
with human motions. J Clin Gastroenterol. 2004;38(6):475-
483.
124. Bakken JS. Fecal bacteriotherapy for recurrent
clostridium difficile infection. Anaerobe. 2009;15(6):285-
289.
125. Bakken JS, Polgreen PM, Beekmann SE, Riedo FX,
Streit JA. Treatment approaches including fecal microbiota
transplantation for recurrent clostridium difficile infection
(RCDI) among infectious disease physicians. Anaerobe.
2013;24:20-24.
126. Lofgren ET, Moehring RW, Anderson DJ, Weber DJ,
Fefferman NH. A mathematical model to evaluate the
routine use of fecal microbiota transplantation to prevent
incident and recurrent clostridium difficile infection.
Infection Control & Hospital Epidemiology. 2014;35(1):18-
27.
127. Rao K, Young VB, Aronoff DM. Fecal microbiota
therapy: Ready for prime time? Infect Control Hosp
Epidemiol. 2014;35(1):28-30.
128. You DM, Franzos MA, Holman RP. Successful
treatment of fulminant clostridium difficile infection with
fecal bacteriotherapy. Ann Intern Med. 2008;148(8):632-
633.
129. Gallegos-Orozco JF, Paskvan-Gawryletz CD, Gurudu
SR, Orenstein R. Successful colonoscopic fecal transplant
for severe acute clostridium difficile pseudomembranous
colitis. Rev Gastroenterol Mex. 2012;77(1):40-42.
130. Neemann K, Eichele DD, Smith PW, Bociek R,
Akhtari M, Freifeld A. Fecal microbiota transplantation for
fulminant clostridium difficile infection in an allogeneic
stem cell transplant patient. Transpl Infect Dis.
2012;14(6):E161-5.
131. Trubiano JA, Gardiner B, Kwong JC, Ward P, Testro
AG, Charles PG. Faecal microbiota transplantation for
severe clostridium difficile infection in the intensive care
unit. Eur J Gastroenterol Hepatol. 2013;25(2):255-257.
132. Gough E, Shaikh H, Manges AR. Systematic review of
intestinal microbiota transplantation (fecal bacteriotherapy)
for recurrent clostridium difficile infection. Clin Infect Dis.
2011;53(10):994-1002.
133. Hamilton MJ, Weingarden AR, Sadowsky MJ,
Khoruts A. Standardized frozen preparation for
transplantation of fecal microbiota for recurrent clostridium
difficile infection. Am J Gastroenterol. 2012;107(5):761-
767.
134. Kassam Z, Hundal R, Marshall JK, Lee CH. Fecal
transplant via retention enema for refractory or recurrent
clostridium difficile infection. Arch Intern Med.
2012;172(2):191-193.
135. Kassam Z, Lee CH, Yuan Y, Hunt RH. Fecal
microbiota transplantation for clostridium difficile
infection: Systematic review and meta-analysis. Am J
Gastroenterol. 2013;108(4):500-508.
136. van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal
infusion of donor feces for recurrent clostridium difficile. N
Engl J Med. 2013;368(5):407-415.
137. Dutta SK, Girotra M, Garg S, et al. Efficacy of
combined jejunal and colonic fecal microbiota
transplantation for recurrent clostridium difficile infection.
Clin Gastroenterol Hepatol. 2014;12(9):1572-1576.
138. Emanuelsson F, Claesson BE, Ljungstrom L, Tvede
M, Ung KA. Faecal microbiota transplantation and
bacteriotherapy for recurrent clostridium difficile infection:
A retrospective evaluation of 31 patients. Scand J Infect
Dis. 2014;46(2):89-97.
139. Friedman-Moraco RJ, Mehta AK, Lyon GM, Kraft
CS. Fecal microbiota transplantation for refractory
clostridium difficile colitis in solid organ transplant
recipients. Am J Transplant. 2014;14(2):477-480.
140. Kelly CR, Ihunnah C, Fischer M, et al. Fecal
microbiota transplant for treatment of clostridium difficile
infection in immunocompromised patients. Am J
Gastroenterol. 2014;109(7):1065-1071.
141. Sha S, Liang J, Chen M, et al. Systematic review:
Faecal microbiota transplantation therapy for digestive and
nondigestive disorders in adults and children. Aliment
Pharmacol Ther. 2014;39(10):1003-1032.
142. Youngster I, Sauk J, Pindar C, et al. Fecal microbiota
transplant for relapsing clostridium difficile infection using
a frozen inoculum from unrelated donors: A randomized,
open-label, controlled pilot study. Clinical Infectious
Diseases. 2014;58(11):1515-1522.
143. Cammarota G, Masucci L, Ianiro G, et al. Randomised
clinical trial: Faecal microbiota transplantation by
colonoscopy vs. vancomycin for the treatment of recurrent
clostridium difficile infection. Aliment Pharmacol Ther.
2015;41(9):835-843.

28 Michigan Medicine C. difficile Guideline December 2016
144. Lagier JC, Delord M, Million M, et al. Dramatic
reduction in clostridium difficile ribotype 027-associated
mortality with early fecal transplantation by the nasogastric
route: A preliminary report. Eur J Clin Microbiol Infect
Dis. 2015.
145. Zanella Terrier MC, Simonet ML, Bichard P, Frossard
JL. Recurrent clostridium difficile infections: The
importance of the intestinal microbiota. World J
Gastroenterol. 2014;20(23):7416-7423.
146. Lee CH, Steiner T, Petrof EO, et al. Frozen vs fresh
fecal microbiota transplantation and clinical resolution of
diarrhea in patients with recurrent clostridium difficile
infection: A randomized clinical trial. JAMA.
2016;315(2):142-149.
147. Kassam Z, Lee CH, Yuan Y, Hunt RH. Fecal
microbiota transplantation for clostridium difficile
infection: Systematic review and meta-analysis. Am J
Gastroenterol. 2013;108(4):500-508.
148. Fischer M, Allegretti JR, Smith M, et al. A multi-
center, cluster randomized dose-finding study of fecal
microbiota transplantation capsules for recurrent
clostridium difficile infection. United European
Gastroenterology Week 2015 (oct 24-28, 2015);.
2015;OP054-LB703.
149. Angelberger S, Reinisch W, Makristathis A, et al.
Temporal bacterial community dynamics vary among
ulcerative colitis patients after fecal microbiota
transplantation. Am J Gastroenterol. 2013;108(10):1620-
1630.
150. De Leon LM, Watson JB, Kelly CR. Transient flare of
ulcerative colitis after fecal microbiota transplantation for
recurrent clostridium difficile infection. Clin Gastroenterol
Hepatol. 2013;11(8):1036-1038.
151. Kump PK, Grochenig HP, Lackner S, et al. Alteration
of intestinal dysbiosis by fecal microbiota transplantation
does not induce remission in patients with chronic active
ulcerative colitis. Inflamm Bowel Dis. 2013;19(10):2155-
2165.
152. Solari PR, Fairchild PG, Noa LJ, Wallace MR.
Tempered enthusiasm for fecal transplant. Clin Infect Dis.
2014;59(2):319.
153. Sekirov I, Russell SL, Antunes LC, Finlay BB. Gut
microbiota in health and disease. Physiol Rev.
2010;90(3):859-904.
154. Brandt LJ, Aroniadis OC, Mellow M, et al. Long-term
follow-up of colonoscopic fecal microbiota transplant for
recurrent clostridium difficile infection. Am J
Gastroenterol. 2012;107(7):1079-1087.
155. Koo HL, Koo DC, Musher DM, DuPont HL.
Antimotility agents for the treatment of clostridium difficile
diarrhea and colitis. Clin Infect Dis. 2009;48(5):598-605.
156. Pepin J, Vo TT, Boutros M, et al. Risk factors for
mortality following emergency colectomy for fulminant
clostridium difficile infection. Dis Colon Rectum.
2009;52(3):400-405.
157. Ali SO, Welch JP, Dring RJ. Early surgical
intervention for fulminant pseudomembranous colitis. Am
Surg. 2008;74(1):20-26.
158. Bhangu A, Nepogodiev D, Gupta A, Torrance A,
Singh P, West Midlands Research Collaborative.
Systematic review and meta-analysis of outcomes following
emergency surgery for clostridium difficile colitis. Br J
Surg. 2012;99(11):1501-1513.
159. Lipsett PA, Samantaray DK, Tam ML, Bartlett JG,
Lillemoe KD. Pseudomembranous colitis: A surgical
disease? Surgery. 1994;116(3):491-496.
160. Bass SN, Bauer SR, Neuner EA, Lam SW.
Comparison of treatment outcomes with vancomycin alone
versus combination therapy in severe clostridium difficile
infection. J Hosp Infect. 2013;85(1):22-27.
161. Kelly CR, Kahn S, Kashyap P, et al. Update on fecal
microbiota transplantation 2015: Indications,
methodologies, mechanisms, and outlook.
Gastroenterology. 2015;149(1):223-237.
162. Goldenberg JZ, Ma SS, Saxton JD, et al. Probiotics for
the prevention of clostridium difficile-associated diarrhea in
adults and children. Cochrane Database of Systematic
Reviews. 2013;5:006095.
163. Horton HA, Dezfoli S, Berel D, et al. Antibiotics for
treatment of clostridium difficile infection in hospitalized
patients with inflammatory bowel disease. Antimicrob
Agents Chemother. 2014;58(9):5054-5059.

29 Michigan Medicine C. difficile Guideline December 2016
Appendix A. Available diagnostic tests for toxigenic C. difficilea
Methods Test Target(s) Notes on Testing
Reference Tests
Cytotoxigenic Culture Toxigenic C. difficile Expertise required
Takes 24-48 hours
Cultures C. difficile and determines if isolate
can produce toxin in vitro
Cell Cytotoxicity Assay Toxins A or Ba Highly sensitive for toxin production
Expertise required
Takes 24-48 hours
Rapid Tests
EIAc
GDH
Must be paired with a test for toxinb
Sensitivity and specificity vary considerably by
manufacturer
EIAc Toxins A or Ba Sufficient for diagnosis alone
Sensitivity and specificity vary considerably by
manufacturer
NAAT More expensive than EIA
Sensitive and specific for presence of toxigenic
C. difficile
Possible increase in false positive rate if used
alone without specimen screening: increases
detection of colonization
RT-PCRc tcdBc or tcdC genes tcdA and tcdB are the genes for toxins A and B,
respectively
tcdB presence is necessary for disease
tcdC is a regulatory gene for toxin production
LAMP tcdA or tcdB genes Strains that are tcdA-positive / tcdB-negative do
not cause disease; thus false negative results
can occur with tcdA testing alone by LAMP
CDI, Clostridium difficile infection; EIA, enzyme immunoassay; GDH, glutamate dehydrogenase; LAMP, loop-mediated
isothermal amplification; NAAT, nucleic acid amplification testing; RT-PCR, real-time polymerase chain reaction. a C. difficile can produce toxin A and/or toxin B. Although both play a role in clinical disease, it is not known if strains producing
only toxin A are associated with symptomatic infection in humans. b Non-toxigenic C. difficile strains also exist, do not cause disease, and will be GDH positive. c Test available at University of Michigan (EIA for GDH, EIA for toxin A, and RT-PCR)