Long-Term Outcomes With Use of Intravascular Ultrasound for the Treatment of Coronary Bifurcation...
6
Long-Term Outcomes With Use of Intravascular Ultrasound for the Treatment of Coronary Bifurcation Lesions Yogesh Patel, MD, Jeremiah P. Depta, MD, Eric Novak, MS, Michael Yeung, MD, Kory Lavine, MD, PhD, Sudeshna Banerjee, MD, C. Huie Lin, MD, PhD, Alan Zajarias, MD, Howard I. Kurz, MD, John M. Lasala, MD, PhD, Richard G. Bach, MD, and Jasvindar Singh, MD* Percutaneous coronary intervention (PCI) of bifurcation lesions remains challenging with a higher risk of adverse outcomes. Whether adjunctive intravascular ultrasound (IVUS) imaging improves outcomes of PCI of bifurcation lesions remains unclear. This study sought to determine the long-term clinical outcomes associated with using IVUS for percutaneous treatment of coronary bifurcation lesions. From April 2003 through August 2010, 449 patients with 471 bifurcation lesions underwent PCI with (n 247) and without (n 202) the use of IVUS. Clinical outcomes (death, myocardial infarction [MI], peripro- cedural MI, stent thrombosis, target vessel revascularization [TVR], and target lesion revascularization [TLR]) were compared between patients undergoing PCI with and with- out IVUS using univariate and propensity score-adjusted analyses. Most patients (61%) presented with acute coronary syndrome and 89% of bifurcations lesions were Medina class 1,1,1. After propensity score adjustment, use of IVUS was associated with significantly lower rates of death or MI (odds ratio 0.38, 95% confidence interval 0.20 to 0.74, p 0.005), death (odds ratio 0.40, 95% confidence interval 0.18 to 0.88, p 0.02), MI (odds ratio 0.37, 95% confidence interval 0.14 to 0.98, p 0.04), periprocedural MI (odds ratio 0.45, 95% confidence interval 0.20 to 0.97, p 0.04), TVR (odds ratio 0.28, 95% confidence interval 0.14 to 0.53, p <0.0001), and TLR (odds ratio 0.27, 95% confidence interval 0.14 to 0.53, p 0.0003) compared to no IVUS. In conclusion, IVUS-guided treatment of complex bifurcation lesions was associated with significantly lower rates of adverse cardiac events at late follow-up. Further study is warranted to evaluate the role of IVUS guidance in improving long-term outcomes after PCI of bifurcation lesions. © 2012 Elsevier Inc. All rights reserved. (Am J Cardiol 2012;109:960 –965) Percutaneous coronary intervention (PCI) of coronary bifurcation lesions represent 10% to 15% of PCIs and is technically challenging owing to multiple factors including anatomic variability related to bifurcation site, plaque bur- den and morphology, bifurcation angle, and branch diame- ter. 1–7 Moreover, bifurcation anatomy may have dynamic variability during PCI, with plaque shift or dissection re- quiring adjustments in interventional approach. 3 For any given bifurcation lesion, uncertainty exists in the selection of the most appropriate interventional strategy and of the potential benefit of available adjunctive technologies. Given its ability to more precisely define coronary anatomy, plaque characteristics, and stent dimensions and morphol- ogy compared to angiography, we hypothesized that intra- vascular ultrasound (IVUS) would improve the outcomes of PCI of bifurcation lesions. 8 We compared long-term clinical outcomes of patients with coronary bifurcations lesions who underwent PCI after the availability of drug-eluting stents with and without the use of IVUS. Methods From April 2003 through August 2010, 9,131 patients underwent PCI at our institution. A retrospective analysis identified 482 patients with de novo coronary bifurcation lesions with a visually estimated diameter stenosis 50% involving the main branch at or within 5 mm of the origin of a side branch 1.5 mm in diameter. 9 Patients were separated into groups by use of IVUS or no IVUS. Of the 482 patients, 13 patients (IVUS, n 7; no IVUS, n 6) had no clinical follow-up and could not be contacted by telephone and thus were excluded from the study. In addi- tion, 20 patients were excluded owing to having multiple bifurcation lesions where IVUS was used during PCI on 1 bifurcation lesion but not used on another. The final analysis comprised 449 patients with 471 distinct coronary bifurca- tion lesions. All bifurcation lesions were classified accord- ing to the Medina classification. 9 Baseline patient data were obtained through review of the electronic medical record and/or paper charts. Institutional review board approval was obtained on April 30, 2010 (protocol number 10-0475). Each coronary angiogram was reviewed by an investiga- tor independent of the operator. All patients were treated with aspirin 325 mg before the procedure. A loading dose of Division of Cardiology, Department of Medicine, Washington Univer- sity School of Medicine, St. Louis, Missouri. Manuscript received Sep- tember 8, 2011; revised manuscript received and accepted November 7, 2011. Dr. Singh has received consulting honoraria from Volcano Corp., Rancho Cordova, California. *Corresponding author: Tel: 314-747-4535; fax: 314-747-1417. E-mail address: [email protected] (J. Singh). 0002-9149/12/$ – see front matter © 2012 Elsevier Inc. All rights reserved. www.ajconline.org doi:10.1016/j.amjcard.2011.11.022
-
Upload
yogesh-patel -
Category
Documents
-
view
212 -
download
0
Transcript of Long-Term Outcomes With Use of Intravascular Ultrasound for the Treatment of Coronary Bifurcation...

gopipovP
Long-Term Outcomes With Use of Intravascular Ultrasound forthe Treatment of Coronary Bifurcation Lesions
Yogesh Patel, MD, Jeremiah P. Depta, MD, Eric Novak, MS, Michael Yeung, MD,Kory Lavine, MD, PhD, Sudeshna Banerjee, MD, C. Huie Lin, MD, PhD, Alan Zajarias, MD,
Howard I. Kurz, MD, John M. Lasala, MD, PhD, Richard G. Bach, MD, and Jasvindar Singh, MD*
Percutaneous coronary intervention (PCI) of bifurcation lesions remains challenging witha higher risk of adverse outcomes. Whether adjunctive intravascular ultrasound (IVUS)imaging improves outcomes of PCI of bifurcation lesions remains unclear. This studysought to determine the long-term clinical outcomes associated with using IVUS forpercutaneous treatment of coronary bifurcation lesions. From April 2003 through August2010, 449 patients with 471 bifurcation lesions underwent PCI with (n � 247) and without(n � 202) the use of IVUS. Clinical outcomes (death, myocardial infarction [MI], peripro-cedural MI, stent thrombosis, target vessel revascularization [TVR], and target lesionrevascularization [TLR]) were compared between patients undergoing PCI with and with-out IVUS using univariate and propensity score-adjusted analyses. Most patients (61%)presented with acute coronary syndrome and 89% of bifurcations lesions were Medina class1,1,1. After propensity score adjustment, use of IVUS was associated with significantlylower rates of death or MI (odds ratio 0.38, 95% confidence interval 0.20 to 0.74, p � 0.005),death (odds ratio 0.40, 95% confidence interval 0.18 to 0.88, p � 0.02), MI (odds ratio 0.37,95% confidence interval 0.14 to 0.98, p � 0.04), periprocedural MI (odds ratio 0.45, 95%confidence interval 0.20 to 0.97, p � 0.04), TVR (odds ratio 0.28, 95% confidence interval0.14 to 0.53, p <0.0001), and TLR (odds ratio 0.27, 95% confidence interval 0.14 to 0.53,p � 0.0003) compared to no IVUS. In conclusion, IVUS-guided treatment of complexbifurcation lesions was associated with significantly lower rates of adverse cardiac events atlate follow-up. Further study is warranted to evaluate the role of IVUS guidance inimproving long-term outcomes after PCI of bifurcation lesions. © 2012 Elsevier Inc. All
rights reserved. (Am J Cardiol 2012;109:960–965)Percutaneous coronary intervention (PCI) of coronarybifurcation lesions represent 10% to 15% of PCIs and istechnically challenging owing to multiple factors includinganatomic variability related to bifurcation site, plaque bur-den and morphology, bifurcation angle, and branch diame-ter.1–7 Moreover, bifurcation anatomy may have dynamicvariability during PCI, with plaque shift or dissection re-quiring adjustments in interventional approach.3 For anyiven bifurcation lesion, uncertainty exists in the selectionf the most appropriate interventional strategy and of theotential benefit of available adjunctive technologies. Givents ability to more precisely define coronary anatomy,laque characteristics, and stent dimensions and morphol-gy compared to angiography, we hypothesized that intra-ascular ultrasound (IVUS) would improve the outcomes ofCI of bifurcation lesions.8 We compared long-term clinical
outcomes of patients with coronary bifurcations lesions who
Division of Cardiology, Department of Medicine, Washington Univer-sity School of Medicine, St. Louis, Missouri. Manuscript received Sep-tember 8, 2011; revised manuscript received and accepted November 7,2011.
Dr. Singh has received consulting honoraria from Volcano Corp.,Rancho Cordova, California.
*Corresponding author: Tel: 314-747-4535; fax: 314-747-1417.
E-mail address: [email protected] (J. Singh).0002-9149/12/$ – see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.amjcard.2011.11.022
underwent PCI after the availability of drug-eluting stentswith and without the use of IVUS.
Methods
From April 2003 through August 2010, 9,131 patientsunderwent PCI at our institution. A retrospective analysisidentified 482 patients with de novo coronary bifurcationlesions with a visually estimated diameter stenosis �50%involving the main branch at or within 5 mm of the originof a side branch �1.5 mm in diameter.9 Patients wereseparated into groups by use of IVUS or no IVUS. Of the482 patients, 13 patients (IVUS, n � 7; no IVUS, n � 6)had no clinical follow-up and could not be contacted bytelephone and thus were excluded from the study. In addi-tion, 20 patients were excluded owing to having multiplebifurcation lesions where IVUS was used during PCI on 1bifurcation lesion but not used on another. The final analysiscomprised 449 patients with 471 distinct coronary bifurca-tion lesions. All bifurcation lesions were classified accord-ing to the Medina classification.9 Baseline patient data wereobtained through review of the electronic medical recordand/or paper charts. Institutional review board approval wasobtained on April 30, 2010 (protocol number 10-0475).
Each coronary angiogram was reviewed by an investiga-tor independent of the operator. All patients were treated
with aspirin 325 mg before the procedure. A loading dose ofwww.ajconline.org
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
givenname
Original text:
surname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
givenname
Original text:
surname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname

t(p(e
Iasudmg
AMM
D
A
D
961Coronary Artery Disease/IVUS Use in PCI of Bifurcation Lesions
clopidogrel 300 to 600 mg or 60 mg prasugrel was admin-istered before or at the time of the index procedure. Allpatients received anticoagulation during the procedure, butthe choice of agent and dosage and the addition of glyco-protein IIb/IIIa inhibitors were left to the operator’s discre-
Table 1Baseline clinical characteristics
Variable IVUS p Value
Yes No(n � 247patients)
(n � 202patients)
ge (years) 62.0 � 11.9 65.9 � 12.2 0.0006en 163 (66%) 132 (65%) 0.75edical history
Diabetes mellitus 76 (31%) 77 (38%) 0.89Hypertension 198 (80%) 180 (89%) 0.001Hyperlipidemia 188 (76%) 166 (82%) 0.12Current/former smoker 132 (53%) 107 (53%) 0.92Previous percutaneous
coronaryintervention
57 (23%) 70 (35%) 0.007
Previous coronaryartery bypass graft
46 (19%) 36 (18%) 0.83
Peripheral arterialdisease
17 (7%) 25 (12%) 0.05
Chronic kidneydisease
30 (12%) 24 (12%) 0.93
iagnosis atpercutaneouscoronaryintervention
ST-segment elevationmyocardialinfarction
24 (10%) 18 (9%) 0.77
Non–ST-segmentelevationmyocardialinfarction
78 (32%) 44 (22%) 0.02
Unstable anginapectoris
56 (23%) 55 (27%) 0.27
Stable angina pectoris 50 (20%) 59 (29%) 0.03Asymptomatic/atypical
chest pain39 (16%) 26 (13%) 0.38
ntithrombotic therapyduring intervention
Heparin 116 (47%) 138 (68%) �0.0001Bivalirudin 119 (48%) 61 (30%) 0.0001Glycoprotein IIb/IIIa
inhibitor121 (49%) 123 (61%) 0.01
ischarge medicationsAspirin 247 (100%) 202 (100%)Clopidogrel 242 (98%) 202 (100%) 0.06Prasugrel 5 (2%) 0 (0%) 0.06Cilostazol 5 (2%) 3 (1%) 0.74� Blocker 220 (89%) 183 (91%) 0.60Angiotensin-
converting enzyme/angiotensin receptorblocker
184 (74%) 149 (74%) 0.86
Statin 232 (94%) 193 (96%) 0.45
Values are presented as absolute number (percentage) or mean � SD.
tion. After PCI all patients were prescribed aspirin 81 to 325 S
mg/day indefinitely and clopidogrel 75 mg/day or prasugrel10 mg/day for �12 months.
All PCIs were performed using standard techniques. Theoperator determined the stenting technique and type ofstent(s) used to treat the bifurcation lesion. Final ballooninflation was performed in all cases. Decision to use IVUSwas at the operator’s discretion at the time of PCI. All IVUSstudies were performed using a commercially available sys-tem (20-MHz Eagle Eye gold or platinum IVUS catheter,Volcano Corp., Rancho Cordova, California; 40-MHziCross IVUS catheter, Boston Scientific, Corp., Natick,Massachusetts) after intracoronary administration of nitro-glycerin 100 to 200 �g. IVUS images were obtained usinga manual or automated transducer pullback and were re-corded on digital media. IVUS was performed in selectedpatients in the IVUS group before PCI to identify plaqueburden and composition, vessel size(s), bifurcation angle,and/or mark side branch ostium. After stenting IVUS wasused in all patients in the IVUS group to assess stentposition, lesion coverage, degree of expansion, neocarinaformation, and/or any complications of PCI not apparent byangiography (e.g., edge dissection, plaque shift, stent un-derexpansion).
The primary outcome of the study was a composite ofdeath from any cause or myocardial infarction (MI). Sec-ondary outcomes included individual end points of death,MI, periprocedural MI, target vessel revascularization(TVR), target lesion revascularization (TLR), or stentthrombosis. Patients were followed from the date of indexstenting through December 31, 2010. All outcomes wereadjudicated independently without knowledge of a patient’sIVUS status. MI, periprocedural MI (creatine kinase-MBincrease �3 times the upper reference limit), TVR, andstent thrombosis were defined according to guidelines setforth by the Academic Research Consortium.10 TLR wasdefined as repeat revascularization with stenosis �50%within the stent, within 5-mm adjacent to the stent, or within5-mm of the carina in the main or side branch. For patientswith multiple coronary bifurcation lesions, death, MI, orperiprocedural MI were counted only 1 time and analyzedper patient, whereas TVR, TLR, and stent thrombosis wereanalyzed per bifurcation lesion.
Differences between the IVUS and no-IVUS groupswere analyzed by univariate methods. Categorical variableswere presented as counts and percentages and comparedusing chi-square or Fisher’s exact tests. Continuous vari-ables were presented as mean � SD and compared using tests or Mann–Whitney U tests. Patient-level outcomesdeath or MI, death, MI, and periprocedural MI) were com-ared using Fisher’s exact test. For lesion-level outcomesTLR, TVR, and stent thrombosis), generalized estimatingquations were used to build logistic models.
Propensity scores were created for the IVUS versus no-VUS groups based on patient and lesion characteristicsnd were used as an adjustment factor in a logistic regres-ion model for each outcome. The following variables weresed to calculate the propensity score: age, male gender,iabetes mellitus, hypertension, hyperlipidemia, current/for-er smoker, previous PCI, previous coronary artery bypass
raft(s), peripheral arterial disease, chronic kidney disease,
T-segment elevation MI, non–ST-segment elevation MI,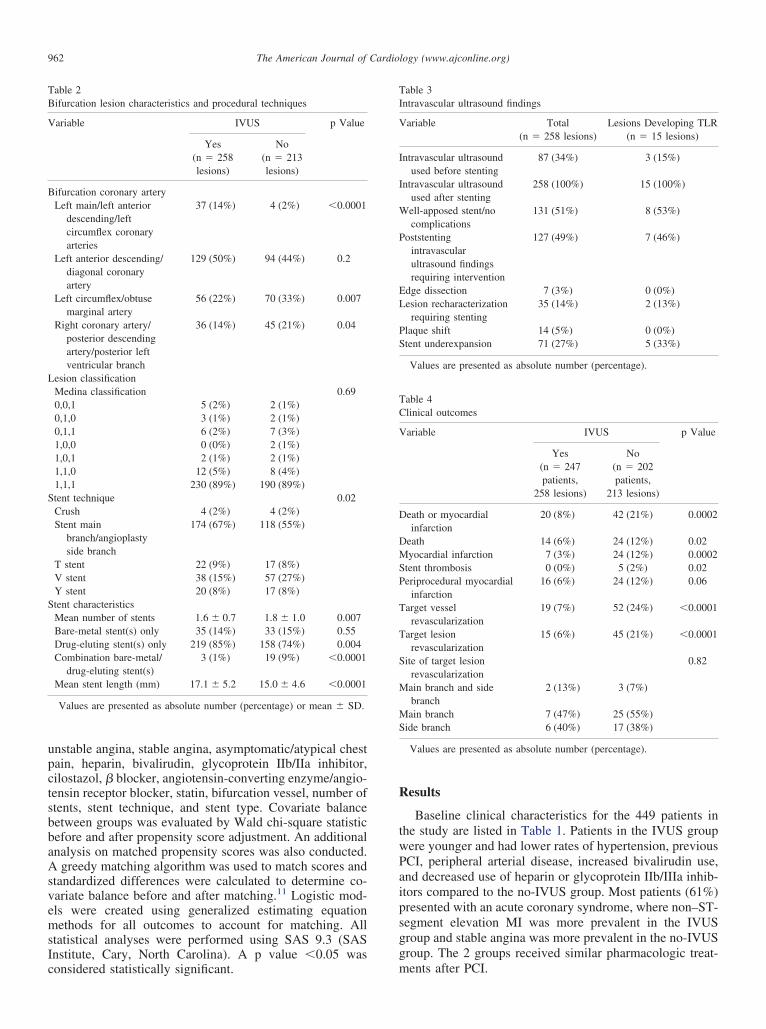
tsbbaAsv
S
962 The American Journal of Cardiology (www.ajconline.org)
unstable angina, stable angina, asymptomatic/atypical chestpain, heparin, bivalirudin, glycoprotein IIb/IIa inhibitor,cilostazol, � blocker, angiotensin-converting enzyme/angio-ensin receptor blocker, statin, bifurcation vessel, number oftents, stent technique, and stent type. Covariate balanceetween groups was evaluated by Wald chi-square statisticefore and after propensity score adjustment. An additionalnalysis on matched propensity scores was also conducted.
greedy matching algorithm was used to match scores andtandardized differences were calculated to determine co-ariate balance before and after matching.11 Logistic mod-
els were created using generalized estimating equationmethods for all outcomes to account for matching. Allstatistical analyses were performed using SAS 9.3 (SASInstitute, Cary, North Carolina). A p value �0.05 was
Table 2Bifurcation lesion characteristics and procedural techniques
Variable IVUS p Value
Yes No(n � 258lesions)
(n � 213lesions)
Bifurcation coronary arteryLeft main/left anterior
descending/leftcircumflex coronaryarteries
37 (14%) 4 (2%) �0.0001
Left anterior descending/diagonal coronaryartery
129 (50%) 94 (44%) 0.2
Left circumflex/obtusemarginal artery
56 (22%) 70 (33%) 0.007
Right coronary artery/posterior descendingartery/posterior leftventricular branch
36 (14%) 45 (21%) 0.04
Lesion classificationMedina classification 0.690,0,1 5 (2%) 2 (1%)0,1,0 3 (1%) 2 (1%)0,1,1 6 (2%) 7 (3%)1,0,0 0 (0%) 2 (1%)1,0,1 2 (1%) 2 (1%)1,1,0 12 (5%) 8 (4%)1,1,1 230 (89%) 190 (89%)
Stent technique 0.02Crush 4 (2%) 4 (2%)Stent main
branch/angioplastyside branch
174 (67%) 118 (55%)
T stent 22 (9%) 17 (8%)V stent 38 (15%) 57 (27%)Y stent 20 (8%) 17 (8%)tent characteristicsMean number of stents 1.6 � 0.7 1.8 � 1.0 0.007Bare-metal stent(s) only 35 (14%) 33 (15%) 0.55Drug-eluting stent(s) only 219 (85%) 158 (74%) 0.004Combination bare-metal/
drug-eluting stent(s)3 (1%) 19 (9%) �0.0001
Mean stent length (mm) 17.1 � 5.2 15.0 � 4.6 �0.0001
Values are presented as absolute number (percentage) or mean � SD.
considered statistically significant.
Results
Baseline clinical characteristics for the 449 patients inthe study are listed in Table 1. Patients in the IVUS groupwere younger and had lower rates of hypertension, previousPCI, peripheral arterial disease, increased bivalirudin use,and decreased use of heparin or glycoprotein IIb/IIIa inhib-itors compared to the no-IVUS group. Most patients (61%)presented with an acute coronary syndrome, where non–ST-segment elevation MI was more prevalent in the IVUSgroup and stable angina was more prevalent in the no-IVUSgroup. The 2 groups received similar pharmacologic treat-
Table 3Intravascular ultrasound findings
Variable Total Lesions Developing TLR(n � 258 lesions) (n � 15 lesions)
Intravascular ultrasoundused before stenting
87 (34%) 3 (15%)
Intravascular ultrasoundused after stenting
258 (100%) 15 (100%)
Well-apposed stent/nocomplications
131 (51%) 8 (53%)
Poststentingintravascularultrasound findingsrequiring intervention
127 (49%) 7 (46%)
Edge dissection 7 (3%) 0 (0%)Lesion recharacterization
requiring stenting35 (14%) 2 (13%)
Plaque shift 14 (5%) 0 (0%)Stent underexpansion 71 (27%) 5 (33%)
Values are presented as absolute number (percentage).
Table 4Clinical outcomes
Variable IVUS p Value
Yes No(n � 247patients,
258 lesions)
(n � 202patients,
213 lesions)
Death or myocardialinfarction
20 (8%) 42 (21%) 0.0002
Death 14 (6%) 24 (12%) 0.02Myocardial infarction 7 (3%) 24 (12%) 0.0002Stent thrombosis 0 (0%) 5 (2%) 0.02Periprocedural myocardial
infarction16 (6%) 24 (12%) 0.06
Target vesselrevascularization
19 (7%) 52 (24%) �0.0001
Target lesionrevascularization
15 (6%) 45 (21%) �0.0001
Site of target lesionrevascularization
0.82
Main branch and sidebranch
2 (13%) 3 (7%)
Main branch 7 (47%) 25 (55%)Side branch 6 (40%) 17 (38%)
Values are presented as absolute number (percentage).
ments after PCI.
Scp
s8bvlvc(
cp(a1
sb
sdsdmPb
963Coronary Artery Disease/IVUS Use in PCI of Bifurcation Lesions
Lesion characteristics and stenting techniques are listedin Table 2. The IVUS group had significantly more lesionslocated at the left main bifurcation, whereas the no-IVUSgroup had more lesions located at the left circumflex/obtusemarginal artery and right coronary artery bifurcations. Thepredominant lesion type was Medina type 1,1,1 (89%). Themost common PCI technique used in the 2 groups wasprovisional stenting of the main branch with angioplasty ofthe side branch, but this technique was employed more oftenin the IVUS group compared to the no-IVUS group. MostPCIs in the 2 groups included implantation of drug-elutingstents, but with a significantly higher frequency in the IVUSgroup compared to the no-IVUS group. Mean stent lengthwas significantly longer in the IVUS group versus the no-IVUS group (17.1 � 5.2 vs 15.0 � 4.6 mm, p �0.0001).
ignificantly fewer stents were placed in the IVUS groupompared to the no-IVUS group (1.6 � 0.7 vs 1.8 � 1.0,� 0.007).IVUS findings observed during the index PCI are pre-
ented in Table 3. IVUS was used in 34% of lesions (n �7) before PCI and in all lesions after PCI. In almost 1/2 ofifurcation lesions, IVUS findings prompted further inter-ention. IVUS prompted a change in PCI strategy for 35esions (14%). Stent underexpansion was observed in 71essels (27%), prompting additional balloon dilation in allases. Lesions with edge dissection (n � 7) or plaque shiftn � 14) also received further therapy. The remaining ves-
sels (n � 131) were considered to have optimal stent di-mensions and well-apposed stent struts. No significant dif-ferences were observed in clinical outcomes in patients whohad IVUS performed before and after PCI compared to afterPCI only.
Clinical follow-up was available for all patients with amean follow-up period of 2.5 � 2.0 years. Clinical out-comes for the study are presented in Table 4. The compositerate of all-cause death or MI was significantly lower in theIVUS group compared to the no-IVUS group (8% vs 21%,p � 0.0002). Compared to no IVUS, IVUS use was asso-iated with a significantly lower rate of death (6% vs 12%,� 0.02), MI (3% vs 12%, p � 0.0002), stent thrombosis
0% vs 2%, p � 0.02), TVR (7% vs 24%, p �0.0001), andtrend toward a lower rate of periprocedural MI (6% vs
2%, p � 0.06). Occurrence of TLR was significantly lessfrequent in the IVUS group compared to the no-IVUSgroup, with an absolute difference of 15% (6% vs 21%,p �0.0001). In the IVUS group, TLR occurred evenly
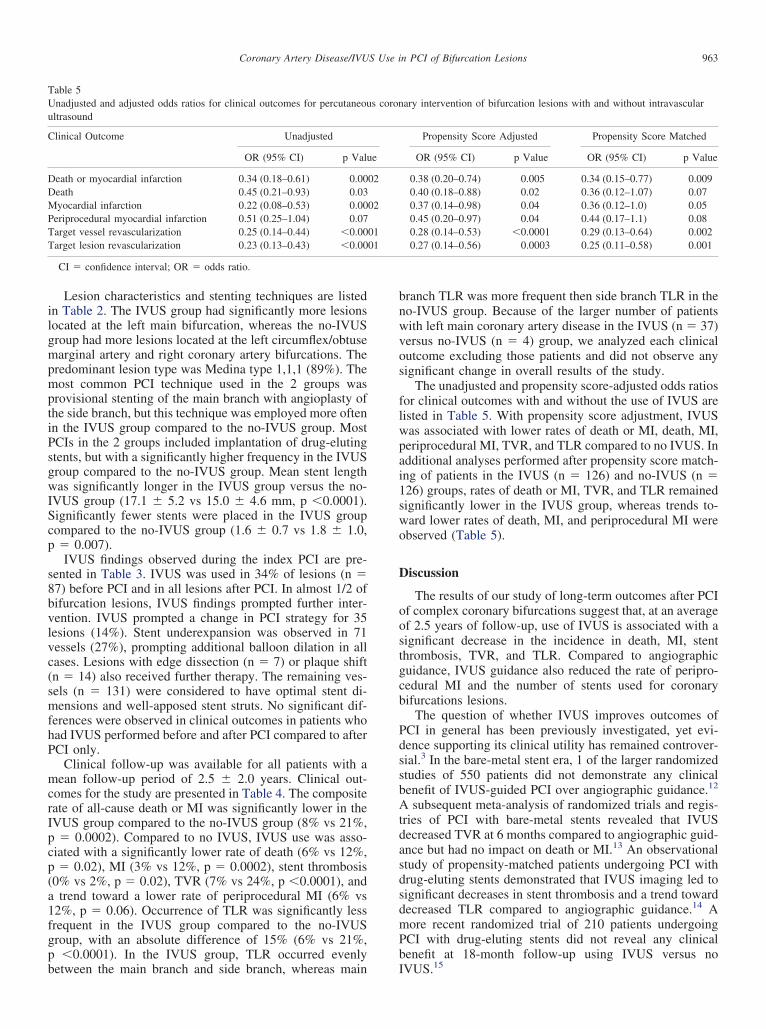
Table 5Unadjusted and adjusted odds ratios for clinical outcomes for percutaneouultrasound
Clinical Outcome Unadjusted
OR (95% CI) p Valu
Death or myocardial infarction 0.34 (0.18–0.61) 0.00Death 0.45 (0.21–0.93) 0.03Myocardial infarction 0.22 (0.08–0.53) 0.00Periprocedural myocardial infarction 0.51 (0.25–1.04) 0.07Target vessel revascularization 0.25 (0.14–0.44) �0.00Target lesion revascularization 0.23 (0.13–0.43) �0.00
CI � confidence interval; OR � odds ratio.
between the main branch and side branch, whereas main I
branch TLR was more frequent then side branch TLR in theno-IVUS group. Because of the larger number of patientswith left main coronary artery disease in the IVUS (n � 37)versus no-IVUS (n � 4) group, we analyzed each clinicaloutcome excluding those patients and did not observe anysignificant change in overall results of the study.
The unadjusted and propensity score-adjusted odds ratiosfor clinical outcomes with and without the use of IVUS arelisted in Table 5. With propensity score adjustment, IVUSwas associated with lower rates of death or MI, death, MI,periprocedural MI, TVR, and TLR compared to no IVUS. Inadditional analyses performed after propensity score match-ing of patients in the IVUS (n � 126) and no-IVUS (n �126) groups, rates of death or MI, TVR, and TLR remainedsignificantly lower in the IVUS group, whereas trends to-ward lower rates of death, MI, and periprocedural MI wereobserved (Table 5).
Discussion
The results of our study of long-term outcomes after PCIof complex coronary bifurcations suggest that, at an averageof 2.5 years of follow-up, use of IVUS is associated with asignificant decrease in the incidence in death, MI, stentthrombosis, TVR, and TLR. Compared to angiographicguidance, IVUS guidance also reduced the rate of peripro-cedural MI and the number of stents used for coronarybifurcations lesions.
The question of whether IVUS improves outcomes ofPCI in general has been previously investigated, yet evi-dence supporting its clinical utility has remained controver-sial.3 In the bare-metal stent era, 1 of the larger randomizedtudies of 550 patients did not demonstrate any clinicalenefit of IVUS-guided PCI over angiographic guidance.12
A subsequent meta-analysis of randomized trials and regis-tries of PCI with bare-metal stents revealed that IVUSdecreased TVR at 6 months compared to angiographic guid-ance but had no impact on death or MI.13 An observationaltudy of propensity-matched patients undergoing PCI withrug-eluting stents demonstrated that IVUS imaging led toignificant decreases in stent thrombosis and a trend towardecreased TLR compared to angiographic guidance.14 Aore recent randomized trial of 210 patients undergoingCI with drug-eluting stents did not reveal any clinicalenefit at 18-month follow-up using IVUS versus no
ary intervention of bifurcation lesions with and without intravascular
Propensity Score Adjusted Propensity Score Matched
OR (95% CI) p Value OR (95% CI) p Value
0.38 (0.20–0.74) 0.005 0.34 (0.15–0.77) 0.0090.40 (0.18–0.88) 0.02 0.36 (0.12–1.07) 0.070.37 (0.14–0.98) 0.04 0.36 (0.12–1.0) 0.050.45 (0.20–0.97) 0.04 0.44 (0.17–1.1) 0.080.28 (0.14–0.53) �0.0001 0.29 (0.13–0.64) 0.0020.27 (0.14–0.56) 0.0003 0.25 (0.11–0.58) 0.001
s coron
e
02
02
0101
VUS.15

b(o
Tbl1fdh
dvwmg
sb
964 The American Journal of Cardiology (www.ajconline.org)
IVUS has potential value during PCI of coronary bifur-cations by virtue of its enhanced vessel and lesion imaging.3
IVUS allows assessment of the bifurcation lesion plaquedistribution and, importantly, can evaluate the extent of sidebranch disease. Accurate anatomic characterization of thebifurcation lesion may improve stent placement, stent di-ameter and length, and stenting technique. After stent de-ployment, IVUS has enhanced sensitivity to detect certainintraprocedural complications (e.g., edge dissection, plaqueshift, or side branch compromise), stent underexpansion, orstent malapposition, factors that have been strongly associ-ated with stent thrombosis.16 Currently, data on the use ofIVUS for PCI of bifurcation lesions remain limited.17
A recent observational study of Korean patients (n �758) who underwent PCI of de novo non-left main coronaryartery bifurcation lesions suggested that IVUS guidancesignificantly decreased all-cause mortality at follow-up andvery late stent thrombosis compared to angiographic guid-ance.18 The benefit of IVUS was limited to patients whoreceived drug-eluting stents compared to bare-metal stents.The study did not observe any decrease in TLR. A subse-quent observational study of the Korean Multicenter Bifur-cation Registry compared 974 propensity score-matchedpatients who underwent PCI with drug-eluting stents for denovo non-left main coronary artery bifurcation lesions andwere followed for 2 years.19 The study showed a significantdecrease in combined death or MI using IVUS compared tono IVUS, which was primarily driven by a trend towarddecreased MI. The study did not observe any change in theincidence of TLR or stent thrombosis between the 2 groups.A recent analysis of 4,314 Italian registry patients withbifurcation lesions who underwent PCI from 2002 through2006 with (n � 226) and without (n � 4,088) IVUS did notshow any clinical benefit.20 However, the study was limitedecause 35% of patients lacked severe bifurcation diseasei.e., main and side branch disease) and IVUS was used innly 5% of cases.20
Our analysis of outcomes after contemporary PCI ofbifurcation lesions demonstrates significant clinical benefitusing IVUS. Our study was distinct from previous reports inseveral respects. The study population included patientswith de novo left main coronary artery bifurcation lesions,whereas previous reports included only non-left main cor-onary artery bifurcations. Lesion complexity was likelygreater in our patient population because nearly 90% of thelesions were Medina class 1,1,1, whereas only 48% ofpatients in 1 of the previous studies had lesions in Medinaclass 1,1,1.19 In this regard, the role of IVUS in deceasing
LR may be heightened in patients with the most complexifurcations lesions. The number of stents implanted wasarger in the IVUS group compared to the no-IVUS group in
previous study, whereas we observed that significantlyewer stents were placed in patients in the IVUS group.18 Aecrease in the number of stents in the IVUS group mayave contributed to fewer TLR events.
A notable observation in our study was the high inci-ence of IVUS findings (49%) that prompted further inter-ention. Stent underexpansion was found in 27% of patientsho underwent bifurcation PCI with IVUS guidance. Re-arkably, in the present study no patients in the IVUS
roup had stent thrombosis. Stent underexpansion is
trongly associated with in-stent restenosis and stent throm-osis.21–24 Given the high incidence of stent underexpan-
sion and lower rates of TLR and stent thrombosis observedin our IVUS group, IVUS may prevent adverse clinicaloutcomes specifically in patients in whom stent underex-pansion is discovered.
Our study has several important limitations that shouldbe considered. It is nonrandomized, retrospective, and ob-servational. The choice to use IVUS was made solely by theoperator at the time of PCI. It is unknown what clinicalfactors led each operator to use IVUS, thus making it verydifficult to control for selection bias. No standardized pre-specified criteria were used to optimize the stenting proce-dure in either group. Although careful analysis was per-formed to account for any significant differences betweenthe IVUS and no-IVUS groups, residual confounders mayhave contributed to differences in clinical outcomes be-tween the 2 groups.
In conclusion, IVUS use in PCI of complex bifurcationlesions is associated with improved long term outcomes thatstrongly support its clinical utility.
Acknowledgment: We are indebted to Tom Holdener forassistance with clinical data abstraction.
1. Myler RK, Shaw RE, Stertzer SH, Hecht HS, Ryan C, Rosenblum J,Cumberland DC, Murphy MC, Hansell HN, Hidalgo B. Lesion mor-phology and coronary angioplasty: current experience and analysis.J Am Coll Cardiol 1992;19:1641–1652.
2. Steigen TK, Maeng M, Wiseth R, Erglis A, Kumsars I, Narbute I,Gunnes P, Mannsverk J, Meyerdierks O, Rotevatn S, Niemelä M,Kervinen K, Jensen JS, Galløe A, Nikus K, Vikman S, Ravkilde J,James S, Aarøe J, Ylitalo A, Helqvist S, Sjögren I, Thayssen P,Virtanen K, Puhakka M, Airaksinen J, Lassen JF, Thuesen L, NordicPCI Study Group. Randomized study on simple versus complex stent-ing of coronary artery bifurcation lesions: the Nordic bifurcation study.Circulation 2006;114:1955–1961.
3. Latib A, Colombo A. Bifurcation disease: what do we know, whatshould we do? JACC Cardiovasc Interv 2008;1:218–226.
4. Al Suwaidi J, Yeh W, Cohen HA, Detre KM, Williams DO, HolmesDR. Immediate and one-year outcome in patients with coronary bifur-cation lesions in the modern era (NHLBI dynamic registry). Am JCardiol 2001;87:1139–1144.
5. Stinis CT, Hu SP, Price MJ, Teirstein PS. Three-year outcome ofdrug-eluting stent implantation for coronary artery bifurcation lesions.Catheter Cardiovasc Interv 2010;75:309–314.
6. Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G,Airoldi F, Chieffo A, Montorfano M, Carlino M, Michev I, Corvaja N,Briguori C, Gerckens U, Grube E, Colombo A. Incidence, predictors,and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005;293:2126–2130.
7. Colombo A, Moses JW, Morice MC, Ludwig J, Holmes DR, SpanosV, Louvard Y, Desmedt B, Di Mario C, Leon MB. Randomized studyto evaluate sirolimus-eluting stents implanted at coronary bifurcationlesions. Circulation 2004;109:1244–1249.
8. Costa RA, Mintz GS, Carlier SG, Lansky AJ, Moussa I, Fujii K,Takebayashi H, Yasuda T, Costa JR, Tsuchiya Y, Jensen LO, CristeaE, Mehran R, Dangas GD, Iyer S, Collins M, Kreps EM, Colombo A,Stone GW, Leon MB, Moses JW. Bifurcation coronary lesions treatedwith the “crush” technique: an intravascular ultrasound analysis. J AmColl Cardiol 2005;46:599–605.
9. Medina A, Suárez de Lezo J, Pan M. [A new classification of coronarybifurcation lesions]. Rev Esp Cardiol 2006;59:183.
10. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA,Steg PG, Morel MA, Mauri L, Vranckx P, McFadden E, Lansky A,
Hamon M, Krucoff MW, Serruys PW; Academic Research Consor-
2
2
2
2
2
965Coronary Artery Disease/IVUS Use in PCI of Bifurcation Lesions
tium. Clinical end points in coronary stent trials: A case forstandardized definitions. Circulation 2007;115:2344–2351.
11. Parsons L. Reducing bias in a propensity score matched-pair sampleusing greedy matching techniques. Available at: http://www2.sas.com/proceedings/sugi26/p214-26.pdf. Accessed March 19, 2011.
12. Mudra H, di Mario C, de Jaegere P, Figulla HR, Macaya C, Zahn R,Wennerblom B, Rutsch W, Voudris V, Regar E, Henneke KH, Schäch-inger V, Zeiher A; OPTICUS (OPTimization with ICUS to reducestent restenosis) Study Investigators. Randomized comparison of cor-onary stent implantation under ultrasound or angiographic guidance toreduce stent restenosis (OPTICUS study). Circulation 2001;104:1343–1349.
13. Casella G, Klauss V, Ottani F, Siebert U, Sangiorgio P, Bracchetti D.Impact of intravascular ultrasound-guided stenting on long-term clin-ical outcome: a meta-analysis of available studies comparing intravas-cular ultrasound-guided and angiographically guided stenting. Cathe-ter Cardiovasc Interv 2003;59:314–321.
14. Roy P, Steinberg DH, Sushinsky SJ, Okabe T, Pinto Slottow TL,Kaneshige K, Xue Z, Satler LF, Kent KM, Suddath WO, Pichard AD,Weissman NJ, Lindsay J, Waksman R. The potential clinical utility ofintravascular ultrasound guidance in patients undergoing percutaneouscoronary intervention with drug-eluting stents. Eur Heart J 2008;29:1851–1857.
15. Jakabcin J, Spacek R, Bystron M, Kvasnák M, Jager J, Veselka J, KalaP, Cervinka P. Long-term health outcome and mortality evaluationafter invasive coronary treatment using drug eluting stents with orwithout the IVUS guidance. Randomized control trial. HOME DESIVUS. Catheter Cardiovasc Interv 2010;75:578–583.
16. Hassan AK, Bergheanu SC, Stijnen T, van der Hoeven BL, Snoep JD,Plevier JW, Schalij MJ, Wouter Jukema J. Late stent malappositionrisk is higher after drug-eluting stent compared with bare-metal stentimplantation and associates with late stent thrombosis. Eur Heart J2010;31:1172–1180.
17. Rogacka R, Latib A, Colombo A. IVUS-guided stent implantation toimprove outcome: A promise waiting to be fulfilled. Curr Cardiol Rev2009;5:78–86.
18. Kim SH, Kim YH, Kang SJ, Park DW, Lee SW, Lee CW, Hong MK,Cheong SS, Kim JJ, Park SW, Park SJ. Long-term outcomes of
intravascular ultrasound-guided stenting in coronary bifurcationlesions. Am J Cardiol 2010;106:612–618.
19. Kim JS, Hong MK, Ko YG, Choi D, Yoon JH, Choi SH, Hahn JY,Gwon HC, Jeong MH, Kim HS, Seong IW, Yang JY, Rha SW, TahkSJ, Seung KB, Park SJ, Jang Y. Impact of intravascular ultrasoundguidance on long-term clinical outcomes in patients treated with drug-eluting stent for bifurcation lesions: data from a Korean multicenterbifurcation registry. Am Heart J 2011;161:180–187.
0. Biondi-Zoccai G, Sheiban I, Romagnoli E, De Servi S, Tamburino C,Colombo A, Burzotta F, Presbitero P, Bolognese L, Paloscia L, RubinoP, Sardella G, Briguori C, Niccoli L, Franco G, Girolamo DD, Piatti L,Greco C, Capodanno D, Sangiorgi G. Is intravascular ultrasoundbeneficial for percutaneous coronary intervention of bifurcation le-sions? Evidence from a 4,314-patient registry. Clin Res Cardiol 2011;100:1021–1028.
1. Kang SJ, Mintz GS, Park DW, Lee SW, Kim YH, Whan Lee C, HanKH, Kim JJ, Park SW, Park SJ. Mechanisms of in-stent restenosis afterdrug-eluting stent implantation: intravascular ultrasound analysis. CircCardiovasc Interv 2011;4:9–14.
2. Fujii K, Carlier SG, Mintz GS, Yang YM, Moussa I, Weisz G, DangasG, Mehran R, Lansky AJ, Kreps EM, Collins M, Stone GW, MosesJW, Leon MB. Stent underexpansion and residual reference segmentstenosis are related to stent thrombosis after sirolimus-eluting stentimplantation: an intravascular ultrasound study. J Am Coll Cardiol2005;45:995–998.
3. Okabe T, Mintz GS, Buch AN, Roy P, Hong YJ, Smith KA, TorgusonR, Gevorkian N, Xue Z, Satler LF, Kent KM, Pichard AD, WeissmanNJ, Waksman R. Intravascular ultrasound parameters associated withstent thrombosis after drug-eluting stent deployment. Am J Cardiol2007;100:615–620.
4. Sonoda S, Morino Y, Ako J, Terashima M, Hassan AH, Bonneau HN,Leon MB, Moses JW, Yock PG, Honda Y, Kuntz RE, Fitzgerald PJ;SIRIUS Investigators. Impact of final stent dimensions on long-termresults following sirolimus-eluting stent implantation: serial intravas-
cular ultrasound analysis from the Sirius trial. J Am Coll Cardiol2004;43:1959–1963.