Local atresia versus congenital coarctation with acquired occlusion: More data required
4
Letters to the Editor Not Congenital Atresia of the Aortic Isthmus, But Acquired Complete Occlusion in Congenital Aortic Coarctation TO THE EDITOR: Joseph et al. [1] have described well the techniques for opening percutaneously the completely occluded aortic isthmus. We would submit, however, that what they have crossed and dilated so well is not congenital atresia of the aortic isthmus, but acquired complete occlusion in con- genital coarctation of the aortic isthmus. Atresia or interruption of the aortic arch as an isolated congenital malformation is extremely rare [2–5]. To find four such patients among 26 undergoing balloon angio- plasty of aortic coarctation would be more than extraor- dinary. Intimal proliferation due to turbulent flow, how- ever, is found at the aortic coarctation site in virtually all patients, tends to progress with age, and not uncommonly completely occludes the lumen [6]. Among 70 aortic coarctations serially sectioned and examined histologi- cally, we found 4 (6%) with complete occlusion of the lumen, and in each the mechanism of occlusion was intimal proliferation (Fig. 1). In most patients with aortic coarctation, blood flow to the descending aorta is primarily via collaterals, and consequently severe stenosis or complete occlusion at the coarctation site presents the same clinical picture. Joseph et al. [1] comment several times that the clinical features of their four patients were similar to those of patients with aortic coarctation, and the reason is that their pa- tients had aortic coarctation. D. Luke Glancy, MD Louisiana State University Health Sciences Center New Orleans, Louisiana William C. Roberts, MD Baylor Cardiovascular Institute Dallas, Texas REFERENCES 1. Joseph G, Mandalay A, Rajendiran G. Percutaneous recanalization and balloon angioplasty of congenital isolated local atresia of the aortic isthmus in adults. Cathet Cardiovasc Intervent 2001;53:535– 541. 2. Roberts WC, Morrow AG, Braunwald E. Complete interruption of the aortic arch. Circulation 1962;26:39 –59. 3. Dische MR, Tsai M, Baltaxe HA. Solitary interruption of the arch of the aorta: clinicopathologic review of eight cases. Am J Cardiol 1975;35:271–277. 4. Milo S, Massini C, Goor DA. Isolated atresia of the aortic arch in a 65-year-old man: surgical treatment and review of published reports. Br Heart J 1982;47:294 –297. 5. Van Mierop LHS, Kutsche LM. Interruption of the aortic arch and coarctation of the aorta: pathogenetic relations. Am J Cardiol 1984;54:829 – 834. 6. Glancy DL, Morrow AG, Simon AL, Roberts WC. Juxtaductal aortic coarctation: analysis of 84 patients studied hemodynami- cally, angiographically, and morphologically after age 1 year. Am J Cardiol 1983;51:537–551. DOI 10.1002/ccd.10153 Published online in Wiley InterScience (www.interscience.wiley.com). Figure 1. See next page. Resected specimens and aortograms in aortic coarctation. In each of the histologic sections (a, b, d), stained by the Verhoff–van Gieson method and magnified 6 to 6.5 times, the proximal aortic lumen (P) is to the left, and the distal lumen (D) is to the right. The invaginated aortic media (darkly staining) of the posterior wall of aorta, seen at the top of a, b, and d, points toward the ligamentum arteriosum, seen at the bottom of each panel. In a, from a 3-year-old boy, intimal thickening (lightly staining) is minimal, and the aortic luminal diameter just distal to the ligamentum arteriosum measures 1.1 mm. In b, from a 35-year-old woman, the invaginated media and striking superimposed intimal thickening narrow the aortic lu- men to < 0.2 mm. In d, from a 27-year-old man, the invaginated posterior wall of the darkly stained aortic media narrows the lumen to < 1.0 mm. Final closure of the aortic lumen is the result of intimal proliferation. In c, the gross specimen of the same coarctation seen in d is viewed from its proximal side before sectioning. The aorta is completely occluded, and di- lated intercostal arteries (i) can be seen on its adventitial sur- face. In the same 27-year-old man, a preoperative lateral film taken 2.2 sec (e) after injection of contrast material into the ascending aorta (A) shows no filling beyond the coarctation (c). The film taken 3.3 sec after injection (f) shows only minimal opacification proximal to the coarctation, seen as a lucent line, but the distal aorta (D) is now opacified via collaterals, some of which can be faintly visualized both anterior and posterior to the aorta. Adapted from Glancy et al. [6]. Catheterization and Cardiovascular Interventions 56:103–106 (2002) © 2002 Wiley-Liss, Inc.
-
Upload
george-joseph -
Category
Documents
-
view
212 -
download
0
Transcript of Local atresia versus congenital coarctation with acquired occlusion: More data required

Letters to the Editor
Not Congenital Atresia of theAortic Isthmus, But AcquiredComplete Occlusion inCongenital Aortic Coarctation
TO THE EDITOR:
Joseph et al. [1] have described well the techniques foropening percutaneously the completely occluded aorticisthmus. We would submit, however, that what they havecrossed and dilated so well is not congenital atresia of theaortic isthmus, but acquired complete occlusion in con-genital coarctation of the aortic isthmus.
Atresia or interruption of the aortic arch as an isolatedcongenital malformation is extremely rare [2–5]. To findfour such patients among 26 undergoing balloon angio-plasty of aortic coarctation would be more than extraor-dinary. Intimal proliferation due to turbulent flow, how-ever, is found at the aortic coarctation site in virtually allpatients, tends to progress with age, and not uncommonlycompletely occludes the lumen [6]. Among 70 aorticcoarctations serially sectioned and examined histologi-cally, we found 4 (6%) with complete occlusion of thelumen, and in each the mechanism of occlusion wasintimal proliferation (Fig. 1).
In most patients with aortic coarctation, blood flow tothe descending aorta is primarily via collaterals, andconsequently severe stenosis or complete occlusion at thecoarctation site presents the same clinical picture. Josephet al. [1] comment several times that the clinical featuresof their four patients were similar to those of patientswith aortic coarctation, and the reason is that their pa-tients had aortic coarctation.
D. Luke Glancy, MDLouisiana State University Health Sciences CenterNew Orleans, LouisianaWilliam C. Roberts, MDBaylor Cardiovascular InstituteDallas, Texas
REFERENCES
1. Joseph G, Mandalay A, Rajendiran G. Percutaneous recanalizationand balloon angioplasty of congenital isolated local atresia of theaortic isthmus in adults. Cathet Cardiovasc Intervent 2001;53:535–541.
2. Roberts WC, Morrow AG, Braunwald E. Complete interruption ofthe aortic arch. Circulation 1962;26:39–59.
3. Dische MR, Tsai M, Baltaxe HA. Solitary interruption of the archof the aorta: clinicopathologic review of eight cases. Am J Cardiol1975;35:271–277.
4. Milo S, Massini C, Goor DA. Isolated atresia of the aortic arch ina 65-year-old man: surgical treatment and review of publishedreports. Br Heart J 1982;47:294–297.
5. Van Mierop LHS, Kutsche LM. Interruption of the aortic arch andcoarctation of the aorta: pathogenetic relations. Am J Cardiol1984;54:829–834.
6. Glancy DL, Morrow AG, Simon AL, Roberts WC. Juxtaductalaortic coarctation: analysis of 84 patients studied hemodynami-cally, angiographically, and morphologically after age 1 year. Am JCardiol 1983;51:537–551.
DOI 10.1002/ccd.10153Published online in Wiley InterScience (www.interscience.wiley.com).
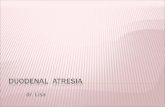
Figure 1. See next page. Resected specimens and aortogramsin aortic coarctation. In each of the histologic sections (a, b, d),stained by the Verhoff–van Gieson method and magnified 6 to6.5 times, the proximal aortic lumen (P) is to the left, and thedistal lumen (D) is to the right. The invaginated aortic media(darkly staining) of the posterior wall of aorta, seen at the top ofa, b, and d, points toward the ligamentum arteriosum, seen atthe bottom of each panel. In a, from a 3-year-old boy, intimalthickening (lightly staining) is minimal, and the aortic luminaldiameter just distal to the ligamentum arteriosum measures 1.1mm. In b, from a 35-year-old woman, the invaginated media andstriking superimposed intimal thickening narrow the aortic lu-men to < 0.2 mm. In d, from a 27-year-old man, the invaginatedposterior wall of the darkly stained aortic media narrows thelumen to < 1.0 mm. Final closure of the aortic lumen is theresult of intimal proliferation. In c, the gross specimen of thesame coarctation seen in d is viewed from its proximal sidebefore sectioning. The aorta is completely occluded, and di-lated intercostal arteries (i) can be seen on its adventitial sur-face. In the same 27-year-old man, a preoperative lateral filmtaken 2.2 sec (e) after injection of contrast material into theascending aorta (A) shows no filling beyond the coarctation (c).The film taken 3.3 sec after injection (f) shows only minimalopacification proximal to the coarctation, seen as a lucent line,but the distal aorta (D) is now opacified via collaterals, some ofwhich can be faintly visualized both anterior and posterior tothe aorta. Adapted from Glancy et al. [6].
Catheterization and Cardiovascular Interventions 56:103–106 (2002)
© 2002 Wiley-Liss, Inc.

Figure 1.
104 Letters to the Editor

Local Atresia Versus CongenitalCoarctation With AcquiredOcclusion: More Data Required
REPLY TO THE LETTER
We thank Dr. Glancy and Dr. Roberts for their com-ments and agree with them that intimal proliferation dueto turbulent flow at the site of congenital aortic coarcta-tion could be responsible for acquired complete occlu-sion. Our reluctance to label these cases as acquiredocclusions is due to the fact that none of our four patients[1], or the four reported by Glancy and Roberts [2], wasseen in an earlier stenotic stage when luminal patencywas identified. The “cross-sectional” data presented byGlancy and Roberts does point to such a sequence ofevents having occurred, but the absence of “longitudinal”data mandates caution before accepting this as a certaintyand as the operative mechanism in all such cases. It isevident from the clinical presentation, angiographic fea-tures, and response to angioplasty in our four patientsthat the predominant underlying pathology is likely to be
the same as that in coarctation of aorta, namely, a pos-terior aortic shelf that exists in utero and leads to post-natal obstruction of the aortic isthmus in association withductal closure [3]. Whether this process by itself is suf-ficient to produce complete obstruction of the lumen(atresia) in some cases, or whether all such cases requireadditional (acquired) intimal proliferation to producecomplete occlusion, is uncertain given the small numberof such cases studied.
George Joseph, MDAsishkumar Mandalay, MDDepartment of CardiologyChristian Medical College HospitalVellore, South India
REFERENCES
1. Joseph G, Mandalay A, Rajendiran G. Percutaneous recanalizationand balloon angioplasty of congenital isolated local atresia of theaortic isthmus in adults. Cathet Cardiovasc Intervent 2001;53:535–541.
2. Glancy DL, Morrow AG, Simon AL, Roberts WC. Juxtaductalaortic coarctation: analysis of 84 patients studied hemodynami-cally, angiographically, and morphologically after age 1 year. Am JCardiol 1983;51:537–551.
3. Talner NS, Berman MA. Postnatal development of obstruction incoarctation of the aorta: role of the ductus arteriosus. Pediatrics1975;56:562–569.
TO THE EDITOR:
We read with interest the recent description of percu-taneous gene transfer using the endocardial substancedelivery (ESD) catheter by Sanborn et al. [1]. We haveused the same catheter to deliver a replication-deficientadenovirus expressing the reporter gene green fluores-cent protein (GFP, 109 pfu/100 �l injection) in pig hearts.Fluorescence microscopy of cryosections 2 days aftertreatment revealed strong fluorescence in virtually allcells up to 5 mm from the needle track. No fluorescencewas seen in sections injected with control adenovirus. Inboth cases, an intense inflammatory response was seen.
We also investigated whether this catheter could beused to deliver naked plasmid DNA. Two animals re-ceived 10 endomyocardial injections of plasmid contain-ing human VEGF165 DNA and 1 received plasmid �-ga-
lactosidase. Plasmids were delivered at a concentrationof 100 �g/100 �l injection. Hearts were harvested 4 dayslater. Inflammation was again observed around all needletracks. No �-galactosidase activity was detectable in the�-galactosidase–treated heart. Immunoperoxidase stain-ing using a polyclonal anti-VEGF primary antibody(A20, Santa Cruz Biotechnology) revealed abundant andspecific VEGF staining around the needle tracks in plas-mid VEGF165- and plasmid �-galactosidase–treatedhearts. Thus, VEGF staining does not depend on thepresence of a VEGF-encoding plasmid and we concludethat this VEGF is of endogenous origin. VEGF localizedpredominantly to infiltrating monocytes, indicating that itis probably induced as part of the inflammatory responseto needle injury. This observation is in agreement withprevious studies documenting that various inflammatorycell types express VEGF, and that VEGF is upregulatedin inflammatory conditions [2,3].
We therefore demonstrated successful adenoviral genetransfer to heart muscle using the ESD catheter, but were
DOI 10.1002/ccd.10155Published online in Wiley InterScience (www.interscience.wiley.com).
DOI 10.1002/ccd.10173Published online in Wiley InterScience (www.interscience.wiley.com).
Letters to the Editor 105

unable to show uptake or expression of plasmid DNA.Needle injury induces inflammation and local endoge-nous VEGF induction, a phenomenon that must be takeninto account when designing studies of local angiogenictherapy.
Peter E. Glennon, MDPeter L. Weissberg, MDDivision of Cardiovascular MedicineAddenbrooke’s HospitalCambridge, U.K.Sarah C. Clarke, MDPeter M. Schofield, MDCardiac UnitPapworth HospitalCambridge, U.K.
Svein Rotavatn, MDJan-Erik Nordrehaug, MDCardiology DepartmentHaukeland SykehusBergen, Norway
REFERENCES
1. Sanborn TA, Hackett NR, Lee LY, El-Sawy T, Blanco I, TarazonaN, Deutsch E, Crystal RG, Rosengart TK. Percutaneous endocar-dial transfer and expression of genes to the myocardium utilizingfluoroscopic guidance. Cathet Cardiovasc Intervent 2001;52:260–266.
2. Taichman NS, Young S, Cruchley AT, Taylor P, Paleolog E.Human neutrophils secrete vascular endothelial growth factor.J Leukoc Biol 1997;62:397–400.
3. Griga T, Tromm A, Spranger J, May B. Increased serum levels ofvascular endothelial growth factor in patients with inflammatorybowel disease. Scand J Gastroenterol 1998;33:504–508.
REPLY TO THE LETTER
We appreciate the opportunity to comment on theobservations of Glennon et al. regarding catheter-basedintramyocardial delivery of adenovirus versus plasmid tothe porcine myocardium. The authors report transgeneexpression in porcine myocardium following catheter-based delivery of an adenovirus (Ad) vector, but theabsence of detectable transgene expression following theadministration of a plasmid vector. They conclude thatendogenous VEGF expression, presumably produced asa component of an inflammatory reaction to the deliveryneedle or the gene transfer vector, must be considered insuch models.
Although we agree that such artifacts must be consid-ered, our prior experience suggests that these are notrelevant concerns. First, we have noted little inflamma-tion (equivalent to that produced by saline injections)following delivery of clinical-grade adenovirus to theporcine myocardium [1]. We believe that the degree ofinflammation noted by Glennon et al. and by other earlyinvestigators may be related to the purity of vector prep-arations in regard to the presence in these preparations ofreplication-competent particles and/or other contami-nants such as endotoxins. Second, we have includedAdNull controls in our early pharmacokinetic studiesassessing Ad-mediated transfer of the VEGF cDNA tothe myocardium [2]. In our hands, VEGF expressionfollowing administration of an Ad vector encodingVEGF was approximately 1 ng/mg protein, compared to
levels of VEGF expression that were indistinguishablefrom background after administration of a vector withoutthe VEGF transgene (AdNull). Taking into account theprior demonstration of plasmid-mediated upregulation ofVEGF expression above that produced by appropriateplasmid controls by other investigators, it must be as-sumed that the plasmid delivery strategy utilized byGlennon et al. was somehow deficient. These data sug-gest that endogenous VEGF expression induced by localinflammation is not an important contributor to Ad-me-diated upregulation of VEGF expression in the myocar-dium, and we conclude that AdVEGF administrationmay be an important means of delivering VEGF to themyocardium for therapeutic applications.
Todd K. Rosengart, MDTimothy A. Sanborn, MDNeil Hackett, PhDRonald G. Crystal, MDDivision of CardiologyEvanston HospitalEvanston, Illinois
REFERENCES
1. Patel SR, Lee LY, Mack CA, Polce DR, El-Sawy T, Hackett NR,Ilercil A, Jones EC, Hahn RT, Isom OW, Rosengart TK, CrystalRG. Safety of direct myocardial administration of an adenovirusvector coding for vascular endothelial growth factor 121. HumGene Ther 1999;10:1331–1348.
2. Lee LY, Patel SR, Hackett NR, Mack CA, Polce DR, El-Sawy T,Hachamovitch R, Zanzonico P, Sanborn TA, Parikh M, Isom OW,Crystal RG, Rosengart TK. Focal angiogen therapy using intramyo-cardial delivery of an adenovirus vector coding for vascular endo-thelial growth factor121. Ann Thorac Surg 2000;69:14–24.
DOI 10.1002/ccd.10172Published online in Wiley InterScience (www.interscience.wiley.com).
106 Letters to the Editor